")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Influence of Personal Factors on Health-Promoting Behavior in College Students: A Structural Equation Modeling Approach
Authors Zambrano Bermeo RN, Estrada Gonzalez C , Guerra EDPH
Received 17 December 2022
Accepted for publication 14 March 2023
Published 5 May 2023 Volume 2023:16 Pages 1259—1270
DOI https://doi.org/10.2147/JMDH.S401870
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rosa Nury Zambrano Bermeo,1,* Catalina Estrada Gonzalez,2,* Eugenia del Pilar Herrera Guerra3,*
1School of Health, Universidad Santiago de Cali, Cali, Colombia; 2School of Health Sciences, Universidad Libre, Sectional Cali, Cali, Colombia; 3School of Health Sciences, Universidad de Córdoba, Montería, Colombia
*These authors contributed equally to this work
Correspondence: Rosa Nury Zambrano Bermeo, Calle 4 # 73-91 apto 514 Cali Valle del Cauca, Colombia, Tel +57 3007760830, Email [email protected]
Purpose: This study aimed to determine how personal factors influence health-promoting behavior in university students using a structural equation modeling approach guided by the Health Promotion Model.
Patients and Methods: An analytical cross-sectional study was conducted. The study included 763 health science students from four universities in Cali, Colombia, who answered a questionnaire on personal factors and Health Promoting Lifestyle Profile II, Spanish version, which was validated in the study population. The direct and indirect relationships between personal factors and health-promoting behaviors were assessed using structural equation modeling. Data analysis was performed using descriptive statistics and structural equation modeling.
Results: A significant relationship was noted between the biological and psychological personal factors of the measurement model (p < 0.05). Psychological personal factors (self-esteem and perceived health status) positively influence health promoting behavior in university students (Hypothesis 2). It’s not possible to demonstrate that health promoting behavior is positively influenced by personal biological factors (Hypothesis 1) and by personal sociocultural factors (Hypothesis 3).
Conclusion: There is a need for interventions that help improve the health-promoting lifestyle profile and are focused on enhancing the self-esteem and perceived health status of university students.
Keywords: healthy lifestyle, health promotion, student health, health‐promoting behavior
Introduction
The Health Promotion Model is a theoretical framework that aims at exploring the complex biopsychosocial processes that motivate people to engage in health-promoting behaviors. Behavioral influences are of immense theoretical significance and need to be studied because they have both direct and indirect effects on health-promoting behaviors. The model used emphasizes the importance of exploring individual characteristics and their experiences, including the prior related behavior and biological, psychological, and sociocultural factors that influence health-promoting behavior.1
Observance of health-promoting lifestyle behaviors is a fundamental component of health maintenance and improvement. Health-promoting lifestyle is a multifactorial pattern of self-initiated behaviors and perceptions that serve to maintain and improve the individual’s level of wellbeing and self-fulfillment.2–5
Unhealthy behaviors, such as unhealthy diets, physical inactivity, and stress, increase the risk for noncommunicable diseases (NCDs), which may manifest as high blood pressure, diabetes mellitus, obesity, and other metabolic risk factors that can lead to early death. The latter jeopardizes the progress toward achieving the sustainable development goals of reducing premature deaths from NCDs by 33% by 2030.6
NCDs mainly affect people in low- and middle-income countries and are responsible for >75% of deaths from NCDs. They affect all age groups and people in all countries and regions but are more associated with older age groups.7 In the Region of the Americas, there are 5.5 million deaths from NCDs each year. Cardiovascular diseases account for the majority of NCD deaths (17.9 million each year), being responsible for >80% of all premature deaths from NCDs, along with cancer, respiratory diseases, and diabetes.8
NCDs during adulthood are associated with behavioral risk factors established early in life,9 and about two-thirds of premature deaths in adults are related to behaviors adopted during adolescence.10 Multidimensional factors affect early adulthood, such as lifestyle habits, emotional wellbeing, interpersonal relationships, family support, and socioeconomic factors, which can pose health risks.11 These multidimensional factors may also predict or mediate their perceived quality of life. Studies found that obesity in young people is associated with poor lifestyle and/or psychosocial health conditions that could result in a lower self-reported quality of life compared with healthy young people.12,13 Furthermore, the Lancet Adolescent Commission determined that tobacco use, alcohol consumption, being overweight/obese, and mental health problems are the main health risks for young people globally, concluding that investing in healthy NCD-related behaviors among adolescents is necessary to prevent the future development of diseases in adulthood.14
Data from the Global School-based Student Health Survey showed that one in three adolescents present lifestyle-related risk factors. This study did not include countries in the European, North American, and Australian regions as the differences in youth health within and outside the region should be considered.15 This limitation did not allow conclusions to be drawn regarding the grouping of risk factors in young people, which should be prioritized when adopting specific preventative measures in each country or region.
A systematic review of the scientific literature on the identification of patterns of eating habits revealed that university students do not practice healthy eating habits. They present unhealthy behaviors characterized by skipping meals due to academic hours, high consumption of fats and sweets, low consumption of fruit, vegetables and milk, which contributes to the risk of suffering from overweight and obesity, as well as the future appearance of NCDs, considering that this negative behavior tends to get worse as students progress through their college studies.16
In Colombia, studies show that university health science students score poorly when evaluating healthy lifestyles, mainly in aspects such as nutrition, physical activity, and health responsibility. Young university health science students exhibit unhealthy behaviors related to nutrition despite their knowledge about food groups that benefit health. Academic schedules and the limited availability of healthy foods and economic resources are some of the reasons.17 On the contrary, students recognize the importance of physical activity to lead a healthy life although they do not practice the required hours weekly.18 In the literature review, no studies were found on the influence of personal factors on health-promoting behaviors in university health science students using the Health Promotion Model (MPS), which originated the development of this study.
The MPS is considered a mid-range theory, therefore, it has a limited number of variables and a limited scope. However, it’s one of the most widely used models due to its usefulness in research and in practice to identify the factors that influence health-promoting behaviors and to help people achieve higher levels of well-being19,20 The research results empirically support the self-efficacy perceived and the benefits and barriers to action as predictors of health-promoting behaviors. They are part of the specific behaviors, cognitions and affect that are the central axis of the revised MPS21–25
The MPS (used) also includes individual characteristics and experiences as predictors of health promotion behaviors, based on the assumption “Individuals in all their biopsychosocial complexity interact with the environment, progressively transforming the environment and transforming themselves over time”.21 However, few studies have used the MPS to investigate personal biopsychosocial factors that influence health-promoting behaviors in college students.
Hence, this study aimed to determine the influence of personal factors on health-promoting behaviors in Colombian university students using a structural equation model (SEM) analysis guided by the Health Promotion Model (HPM).
Materials and Methods
Design and Setting
A cross-sectional analytical study was conducted from February to June 2021 among undergraduate students in the school of health of four universities in Colombia.
Study Sample
The population sample comprised 7808 students from the Faculty of Health Sciences of four universities in Cali, Colombia. A sample of 763 individuals was finally selected using probability sampling stratified by academic programs by considering the following inclusion criteria: (1) undergraduate health science students, (2) ≥18 years of age, (3) voluntary participation. Students enrolled in other faculties offered by universities and postgraduate students and the students with mental health problems were excluded. The sample size ratio required for SEM should not be less than 10:1 (10 cases per parameter); a minimum of 200 SEM participants is recommended.18,26 Thus, it is considered an adequate sample taking into account the parameters to be estimated.
Study Instruments
Personal Factors Questionnaire
Questionnaire developed by the researchers based on the MPS (revised), where individual characteristics are considered unique for each person and are studied based on personal biopsychosocial factors. “Biological factors include: age, body mass index, aerobic capacity, strength, agility, or balance. Psychological factors include self-esteem, and perceived health status. Sociocultural factors include race, ethnicity, education, and socioeconomic status. The MPS seeks to provide flexibility in the identification of the most important variables related to health behavior in the target population.21
Health-Promoting Lifestyle Profile- II
The Health-Promoting Lifestyle Profile II (HPLP-II) questionnaire was used, which comprised 52 items grouped into six subscales: responsibility for health (9 items), physical activity (8 items), nutrition (9 items), spiritual growth (9 items), interpersonal relationships (9 items), and stress management (8 items). A Likert scale with four response options (never, sometimes, frequently and routinely) ranging from 1 to 4 was used. The score was obtained by calculating the mean of the responses to the items both globally and by subscales, which allows comparisons between subscales and identify the areas that must be intervened to improve the lifestyle that promotes global health.27
The dimension responsibility for health implies an active sense of responsibility for one’s own well-being (eg, I report any unusual signs or strange symptoms to a doctor or other health professionals). Physical activity assesses regular participation in light, moderate, and/or vigorous activities for the sake of physical fitness and health (eg, I follow a planned exercise program). The nutrition dimension assesses the informed selection and consumption of foods essential for sustenance, health, and well-being (eg, I choose a diet low in fat, saturated fat, and cholesterol). Spiritual growth focuses on evaluating the development of internal resources and is achieved through transcending, connecting, and developing (eg, I believe that my life has a purpose). Interpersonal relationships involve using communication to achieve a sense of intimacy and closeness within meaningful relationships (eg, I find it easy to show concern, love, and caring for others). Stress management involves identifying and mobilizing resources to effectively control or reduce stress (eg, I maintain balance to prevent fatigue).18,27,28
The HPLP-II original version has validity and reliability,29 as does the HPLP-II Spanish version.18,28 Validity and reliability tests of the Spanish version of the HPLP-II were performed in a sample of the local population before administering it to the study sample (n=763). In the confirmatory factor analysis, the goodness-of-fit indices evidenced an acceptable level of validity (χ2 = 7168.98; gl = 1268; p < 0.001; root mean square error of approximation (RMSEA) = 0.08; normed fit index (NFI) and AGFI = 0.95). The overall reliability results (Cronbach’s alpha 0.94) and the results by subscales (Cronbach’s alpha ranged from 0.68 to 0.89) support the reliability of the data obtained in this study.
Outline of the Proposed Model
A theoretical structural model was designed with four latent variables and their respective observed variables, as shown in Figure 1. To evaluate the relationships between the latent variables, the following hypotheses were proposed:
H1: health-promoting behavior is positively influenced by personal biological factors. H2: health-promoting behavior is positively influenced by personal psychological factors. H3: health-promoting behavior is positively influenced by personal sociocultural factors.
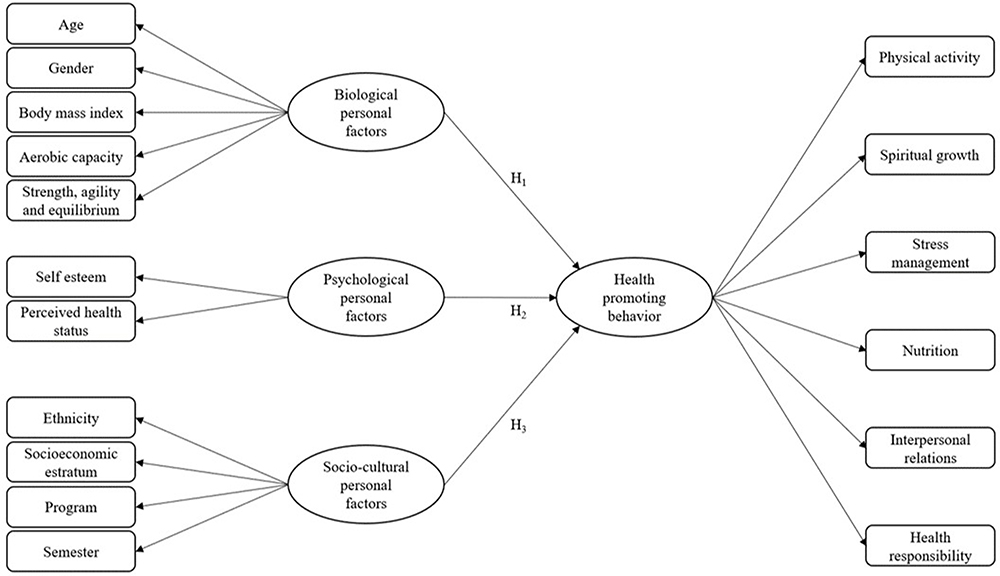 |
Figure 1 Preliminary MET of personal factors related to health-promoting behavior in university students. Notes: The rectangles and ovals indicate observed and latent variables, respectively; arrows connecting the circles represent the relationships between the variables (regression coefficients); the arrows between the circles and rectangles indicate the reliability of the indicators (factor loadings). |
Data Collection
Students were contacted via email guaranteeing anonymity and confidentiality. Voluntary participation was requested, using the informed consent template, where participants could choose the “I agree to participate” or “I do not agree to participate” box. In the case of choosing to accept participation, click “next” to start filling out the forms. In the case of choosing not to accept, the process ends.
The data was collected virtually through the Google Forms form, taking into account the advantages it offers: freedom to express oneself, speed up the process and efficiency of data collection. The forms were sent to 800 students with a response rate of 95%, which allowed the sample to be completed (n=763).
Data Analysis
Descriptive statistics were used to analyze the general characteristics of the participants. Internal reliability tests and factor and correlation analyses were performed. Based on these analyses, SEM was performed to describe the ability of the hypothesized model to predict the mutual relationships between the factors that emerged from the confirmatory factor analysis.
To evaluate the model fit, several indices were used: chi-square test (v2), RMSEA, goodness-of-fit index (GFI), Tucker–Lewis index (TLI), comparative fit index (CFI), and NFI. The model fit is considered to be good if the values of the fit indices for GFI, CFI, NFI, and TLI are >0.90 and if the value for RMSEA is <0.05.30
The robust maximum likelihood estimator was used to determine the SEM. In the hypothetical model, personal biological, psychological, and sociocultural factors were estimated using multiple regression analysis to examine their contribution to health-promoting behavior (HPLP-II) and its aspects (spiritual growth, interpersonal relationships, responsibility toward health, nutrition, physical activity, and stress management). Based on the aforementioned analysis, SEM was performed to assess the relationship between the latent variables and their respective indicators and the accuracy with which the hypothesized model predicted the mutual relationships between the factors. All statistical analyses were performed using the R-project software.
Ethical Considerations
This study complied with international31 and national ethical guidelines.32 The study was approved by the ethics committee of the Universidad Santiago de Cali (2020–2606 Acta N°1). Permission was obtained from the author of the HPLP-II scale, and informed consent was obtained from each participant prior to data collection, guaranteeing anonymity and confidentiality. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki for health research involving human beings.
Results
Sample Characteristics
Seven hundred and sixty-three undergraduate students from the faculty of health of four universities in Colombia participated in this study. The Shapiro–Wilk normality test was used for the variable of the continuous variable age, reporting 0.674. The average age of the participants was 21.7 ± 4.3 years, and most of them were under 21 years of age (59.6%) and of female sex (78.1%). Their average body mass index was 24.2 ± 4.1. Table 1 also presents the personal psychological and sociocultural characteristics of the participants. Most of them had medium self-esteem (48.9%) and were of mestizo ethnicity (56.1%).
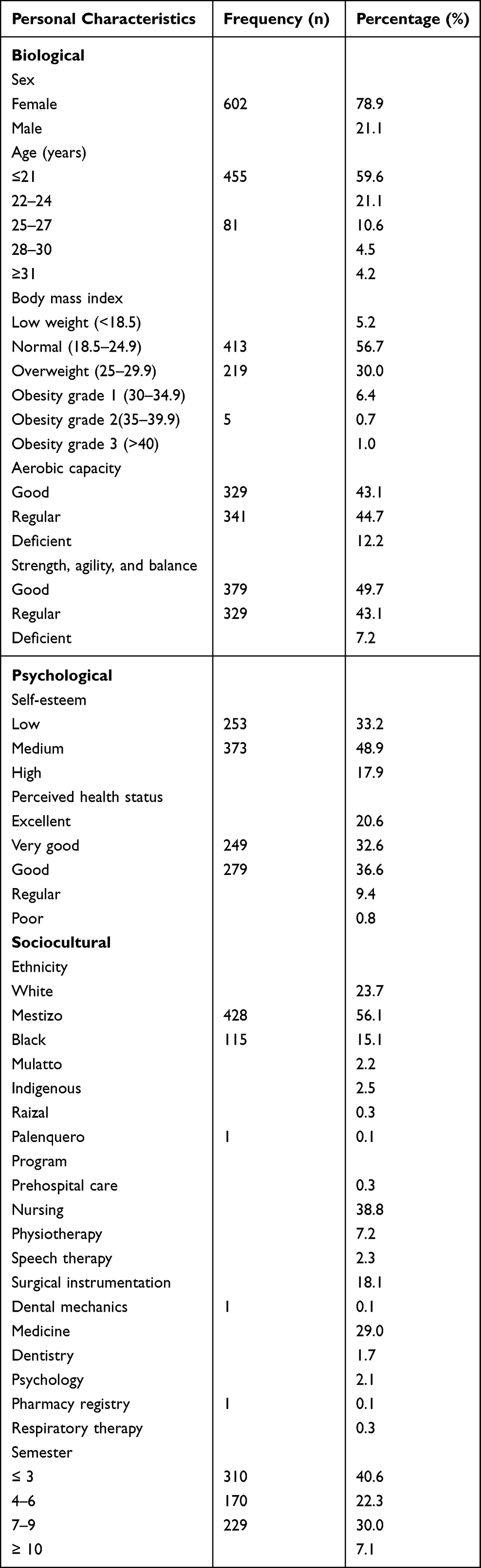 |
Table 1 Distribution of Personal Characteristics of College Students (n = 763) |
Health-Promoting Behavior Lifestyle Profile
The mean scores of the six subscales of HPLP-II were highest for spiritual growth ( : 27.7) and interpersonal relationships (
: 27.7) and interpersonal relationships ( : 25.9). Most participants exhibited inadequate physical activity (
: 25.9). Most participants exhibited inadequate physical activity ( : 18.2) and poor stress management (
: 18.2) and poor stress management ( : 18.9). Table 2.
: 18.9). Table 2.
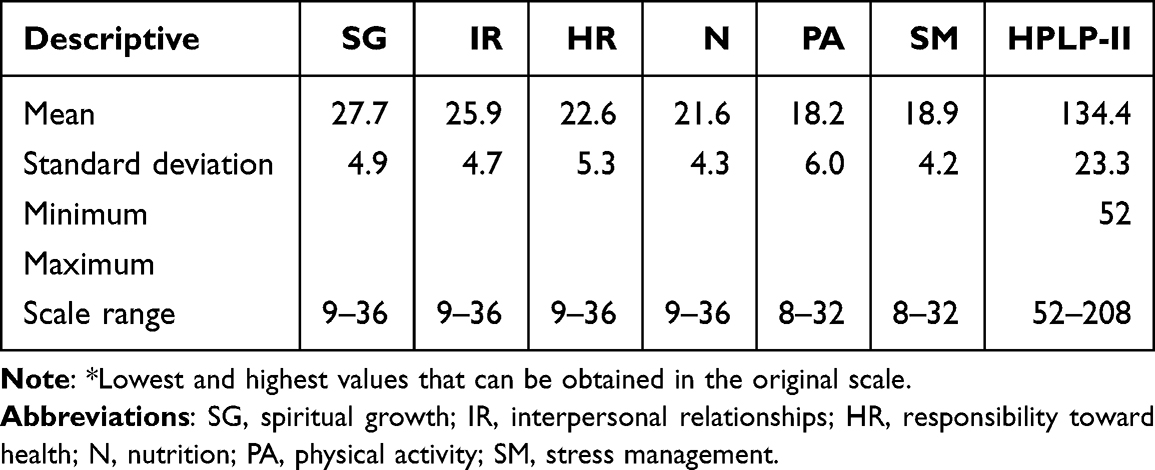 |
Table 2 Total and Subscale Mean Scores of the Health-Promoting Behavior Lifestyle Profile of University Students (n = 763) |
Structural Model
Four latent variables were specified in the measurement model. Analysis of the preliminary measurement model showed that two observed variables (age and semester) were not significant (p > 0.05); hence, they were eliminated from the proposed model. The HPLP variables had loadings ranging from 0.66 to 0.87. Factor loadings for all latent constructs were significant (p < 0.05). The fit indices for the goodness-of-fit tests showed that the final MET fit the data adequately. Table 3.
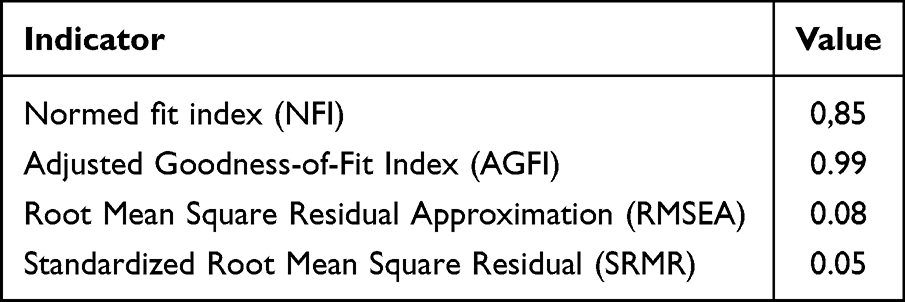 |
Table 3 Goodness-of-Fit Indicators of the SEM Model for Personal Factors and Health-Promoting Behavior in University Students |
The results of the SEM are shown in Table 4 and the structural model in Figure 2. The psychological personal factor had a trajectory or regression coefficient of −0.41, being significant (p<0.05). The factor loadings of the items: perceived state of health, socioeconomic stratum, and academic program are due to the inverted scale of the responses. Biological and sociocultural factors presented almost null and insignificant coefficients (p>0.05). The highest factor loading of the observed variables that measured the personal factors was for the perceived state of health (−0.85) over the psychological personal factor. This indicates that as the assessment score for that variable increases toward excellent, students will have fewer psychological problems. However, personal psychological factors can negatively influence health promoting behavior, that is, low self-esteem, can affect the psychological needs of university students, which leads to less health promoting behavior.
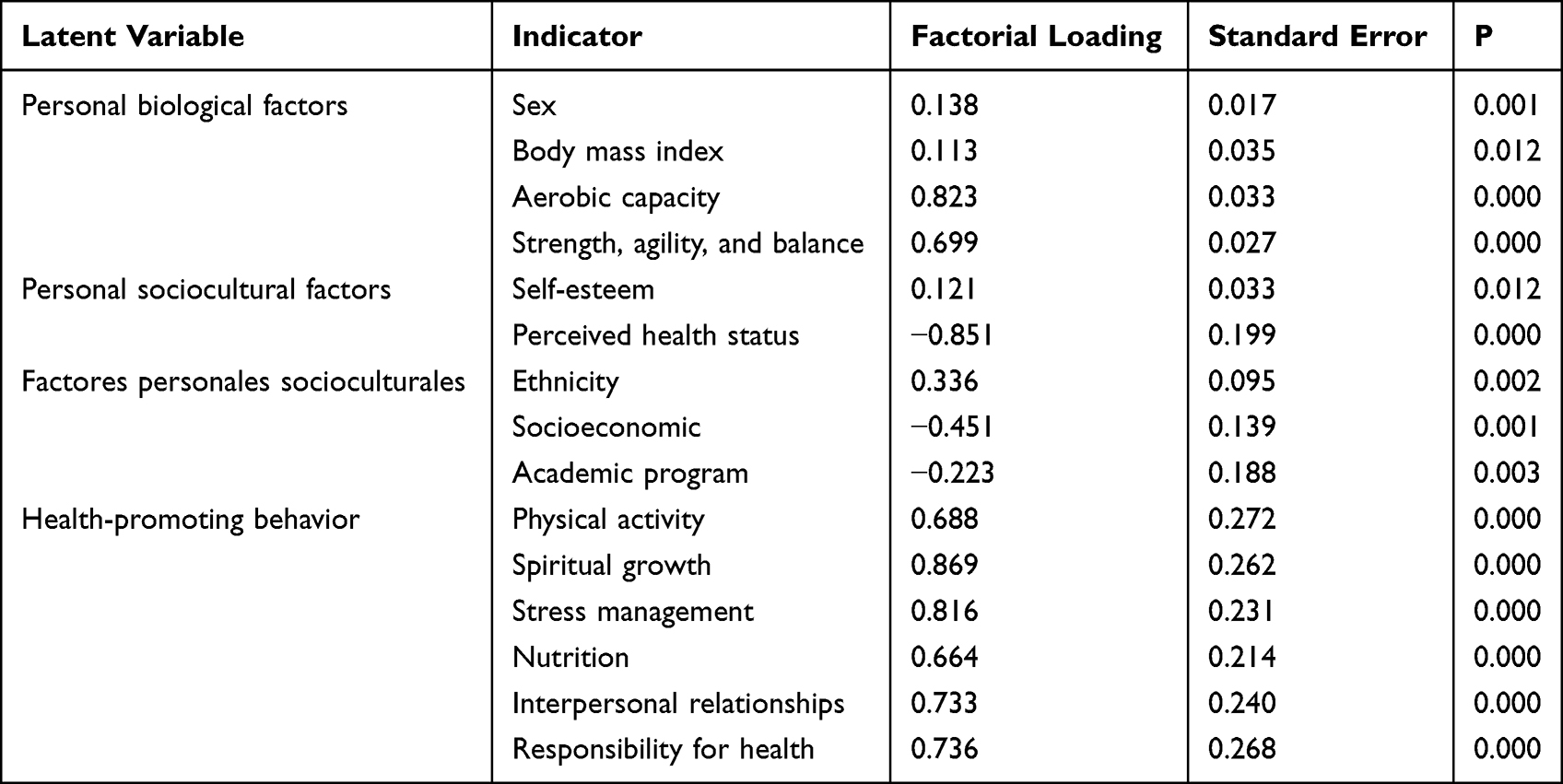 |
Table 4 SEM Results |
 |
Figure 2 Structural model with personal factors related to health promoting behavior in university students. Abbreviation: ns, not significant. Notes: Dashed lines with double arrows indicate covariance between the variables. |
Discussion
This study has shown that Pender’s HPM fits the Colombian university student populations well and could be useful for research on intervention design. Personal psychological factors were identified, which should be considered to help improve the HPLP-II of university students.
Health-Promoting Lifestyle
In this study the mean scores of the subscales of HPLP-II indicate a healthy lifestyle of college students were high for spiritual growth ( :27.7) and interpersonal relationships (
:27.7) and interpersonal relationships ( :25.9). In the case of interpersonal relationships, the results of this study are consistent with recent studies.33–35 It is important to continue cultivating interpersonal relationships and teamwork in students, considering that the use of technologies and social networks alienate people from their immediate environment and cause health problems.
:25.9). In the case of interpersonal relationships, the results of this study are consistent with recent studies.33–35 It is important to continue cultivating interpersonal relationships and teamwork in students, considering that the use of technologies and social networks alienate people from their immediate environment and cause health problems.
Regarding spiritual growth, the results were similar to those obtained by Fashafsheh et al and Polat et al, who also evidenced a high score for spiritual growth. In the case of university students, spiritual growth represents a comprehensive training scenario owing to the fact that spirituality is recognized as a part of wellbeing and quality of life in physical and mental health.36,37
The stress management subscale showed low mean scores ( :18.9), contrary to what was reported in a study in Mexican university students, where the HPLP-II was applied, which demonstrated a significantly healthier lifestyle in terms of stress management in students who attended a brief health promotion intervention to promote a healthy lifestyle, which explains the importance of experimental evidence to establish guidelines for the design of healthier universities.38
:18.9), contrary to what was reported in a study in Mexican university students, where the HPLP-II was applied, which demonstrated a significantly healthier lifestyle in terms of stress management in students who attended a brief health promotion intervention to promote a healthy lifestyle, which explains the importance of experimental evidence to establish guidelines for the design of healthier universities.38
This study had a mean score of 21.6 on the nutrition scale, and physical activity had the lowest mean score of 18.2. Similar results were obtained, using the HPLP-II, by Alzahrani et al, Fashafsheh et al, Hwang & Oh, Mak et al, and Polat et al, who reported a low score for physical activity, as a product of a life style in which psychological, social, cultural aspects that are related, among other factors, personal or acquired behavior patterns converge.34–37,39 Gurusamy et al reported that one of the lowest lifestyle profile scores were obtained for nutrition,33 and Sanchez-Ojeda & De Luna-Bertos, highlighted that the association between poor diet and lack of physical exercise was common among college students.40 Furthermore, other studies, showed that insufficient intake of fruits and vegetables and a lack of physical activity were the most frequent risk factors among young people.41,42 The researchers also found a high prevalence of overweight/obesity that increased during middle adolescence and continued into early adulthood. Other studies indicated that health-promoting behavior in students decreased as academic years advanced owing to the increased workload,33,43,44 thus favoring sedentary lifestyles and the consumption of fast and ultra-processed foods.
Risk factors such as physical inactivity and malnutrition are a global trend among university students, resulting in chronic diseases that require timely interventions to ensure public health. These scenarios illustrate that there is a need to review the current curricula of health programs so that environments that promote healthy lifestyles and focus on interventions based on students’ health needs are strengthened to open up possibilities for future research.
Maintaining healthy lifestyles is essential for promoting health and improving the level of wellbeing, self-fulfillment, and personal development. Health science students will be the future health promoters and educators. Therefore, curricula should encourage, support, and take the lead in promoting healthy lifestyles, incorporating it as a fundamental skill to guide patients.
Current policies in Colombia make it possible to support a healthy lifestyle for university students, through the implementation of individual, collective and population interventions in the educational environment defined in the comprehensive care route for the promotion and maintenance of health, interventions that are focused on health education to promote healthy lifestyles and the well-being of the student population.
Personal Factors Related to Health-Promoting Behavior in College Students
In this study, the estimated SEM showed how each of the latent variables, namely, biological, psychological, and sociocultural personal factors, was measured using its observable variables proposed by the HPM. However, the relationships that were anticipated among biological, psychological, and sociocultural personal factors were not significant when related to each other. The only exception was the correlation between biological and psychological personal factors, which was inconsistent with previous studies.45
Furthermore, the estimated model only contained effects and relationships between personal psychological factors (self-esteem and perceived health status) and health-promoting behavior, showing that it exerted statistically significant direct effects on the health-promoting behavior of the participants. The model assumed that a university student with a high self-esteem and health perception will score high on all six indicators of HPLP-II.
This finding is similar to those from other studies, which also asserted that college students with higher self-esteem and perceived health status exhibit a higher health promotion behavior. Therefore, perceived health status and self-esteem are two dominant variables that influence the health-promoting behavior.46
According to Pender, self-esteem and perceived health status are the personal psychological factors that influence learning and the effect related to health-promoting behavior.47 Huang demonstrated via meta-analysis that the level of self-esteem is closely related to cognition and healthy behavior.48 Another study reported that people with high self-esteem value their health more and take greater responsibility for their health.49 Furthermore, high self-esteem has been shown to promote physical activity,50 regulate the behavior in the process of social adaptation, and foster taking the initiative in interpersonal relationships.51 High self-esteem can help a person manage stressful events, avoid anxiety and depression, maintain optimistic expectations for the future, and adapt to the surrounding environment.52 From a nursing and public health perspective, professionals can increase self-esteem through short interventions that contribute to improving college students’ personal judgment of their self-worth by nudging them toward an overall positive appraisal of themselves by maintaining a positive attitude in different situations that involves believing that they are capable, important, and successful.
Finally, it is worth noting that the combination of the three personal biological, psychological, and sociocultural factors is unique for each person. Therefore, identifying the most important variable(s) in relation to health-promoting behavior is important in the groups of people subject to the intervention as it means being able to recognize the best predictor of future behavior. In this group of university students, personal psychological factors, such as self-esteem and perceived health status, were the main targets for modifying the health-promoting behavior. Hence, they should be taken into consideration when developing future interventions that can help students adopt a health-promoting lifestyle, with a focus on the benefits of individual and collective psychological support.
Conclusion
This study explored the personal factors presented by the HPM. Psychological personal factors were an important mediator in these relationships. Perceived health status and self-esteem were consistently reported as the main determinants of health-promoting behavior. Therefore, it is recommended to consider interventions because it becomes necessary that increase the perceived health status and self-esteem to maintain and improve the health-promoting behavior of these students.
Acknowledgments
The authors wish to acknowledge the cooperation of the health sciences students and their participation in this study. This research has been funded by General Directorate of Investigations of Universidad Santiago de Cali under call No. 02-2023.
Funding
This research has been funded by Dirección General de Investigaciones of Universidad Santiago de Cali under call No. 01-2022.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Pender N, Murdauge C, Parsons MA. Health promotion model. In: Pender N, Murdauge C, Parsons MA, editors. Health Promotion in Nursing Practice.
2. Alpar ŞE, Şenturan L, Karabacak Ü, Sabuncu N. Change in the health promoting lifestyle behaviour of Turkish University nursing students from beginning to end of nurse training. Nurse Educ Pract. 2008;8(6):382–388. doi:10.1016/j.nepr.2008.03.010
3. Edelman CL, Mandle CL. Health Promotion Throughout the Life Span.
4. Esin N. The adaptation of the healthy lifestyle behaviour scale for Turkey. Hems_irelik Bu¨lteni. 1999;12(45):87–96.
5. Hui WH. The health-promoting lifestyles of undergraduate nurses in Hong Kong. J Professional Nursing. 2002;18(2):101–111. doi:10.1053/jpnu.2002.32346
6. World Health Organization (WHO). Non communicable diseases. Available from: http://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
7. Global Burden of Disease (GBD 2019). Institute for Health Metrics and Evaluation. Available from: https://www.healthdata.org/gbd/2019.
8. Enfermedades no transmisibles - OPS/OMS | organización Panamericana de la Salud. PAHO/WHO | Pan American Health Organization. Available from: https://www.paho.org/es/temas/enfermedades-no-transmisibles.
9. Champion KE, Parmenter B, McGowan C, et al. Effectiveness of school-based eHealth interventions to prevent multiple lifestyle risk behaviours among adolescents: a systematic review and meta-analysis. Lancet Digital Health. 2019;1(5):e206–e221. doi:10.1016/s2589-7500(19)30088-3
10. Long KQ, Ngoc-Anh HT, Phuong NH, et al. Clustering Lifestyle Risk Behaviors among Vietnamese Adolescents and Roles of School: a Bayesian Multilevel Analysis of Global School-Based Student Health Survey. Lancet Reg Health West Pac. 2019;30(15):100–225. doi:10.1016/j.lanwpc.2021.100225
11. Berg N Accumulation of disadvantage from adolescence to midlife: a 26-year follow-up study of 16-year old adolescents. Dissertationes Scholae Doctoralis Ad Sanitatem Investigandam Universitatis Helsinkiensis; 2017. Available from: http://urn.fi/URN:ISBN:978-951-51-2870-6.
12. Schwimmer JB, Burwinkle TM, Varni JW. Health-related quality of life of severely obese children and adolescents. JAMA. 2003;289(14):13–19. doi:10.1001/jama.289.14.1813
13. Kistler KD, Molleston J, Unalp A, Abrams SH, Behling C, Schwimmer JB; Nonalcoholic Steatohepatitis Clinical Research Network (NASH CRN). Symptoms and quality of life in obese children and adolescents with non-alcoholic fatty liver disease. Aliment Pharmacol Ther. 2010;31(3):396–406. doi:10.1111/j.1365-2036.2009.04181.x
14. Patton GC, Sawyer SM, Santelli JS, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016;387(10036):2423–2478. doi:10.1016/s0140-6736(16)00579-1
15. Uddin R, Lee EY, Khan SR, Tremblay MS, Khan A. Clustering of lifestyle risk factors for non-communicable diseases in 304,779 adolescents from 89 countries: a global perspective. Prev Med. 2020;131:105955. doi:10.1016/j.ypmed.2019.105955
16. Maza-ávila F, Caneda-Bermejo M, Vivas-Castillo A. Hábitos alimenticios y sus efectos en la salud de los estudiantes universitarios. Una revisión sistemática de la literatura. Psicogente. 2022;25(47):110–140. doi:10.17081/psico.25.47.4861
17. Romero VR, Luque JA, Andrade KN, Henao VA, Bermeo RN, Castillo JA. Estilos de vida promotor de salud en estudiantes de medicina en una universidad privada de Colombia en tiempos de pandemia Covid-19. Studies Health Sci. 2022;3(2):1249–1265. doi:10.54022/shsv3n2-049
18. Laguado E, Gómez M. Estilos de vida saludable en estudiantes de Enfermería en la Universidad Cooperativa de Colombia. Hacia Promoc Salud. 2014;19(1):68–83.
19. Khoshnood Z, Rayyani M, Tirgari B. Theory analysis for Pender’s health promotion model (HPM) by Barnum’s criteria: a critical perspective. Int J Adolesc Med Health. 2018;32(4). doi:10.1515/ijamh-2017-0160
20. Habibzadeh H, Shariati A, Mohammadi F, Babayi S. The effect of educational intervention based on Pender’s health promotion model on quality of life and health promotion in patients with heart failure: an experimental study. BMC Cardiovasc Disord. 2021;21:1–13. doi:10.1186/s12872-021-02294-x
21. Pender NJ, Murdaugh CL, Ann M. Parsons. Health Promotion in Nursing Practice / Nola J. Pender, Carolyn L. Murdaugh, Mary Ann Parsons.
22. Chen H-H, Hsieh P-L. Applying the Pender’s Health Promotion Model to Identify the Factors Related to Older Adults’ Participation in Community-Based Health Promotion Activities. Int J Environ Res Public Health. 2021;18(19):9985. doi:10.3390/ijerph18199985
23. Hepburn M. The variables associated with health promotion behaviors among urban black women. J Nursing Scholarship. 2018;50(4):353–366. doi:10.1111/jnu.12387
24. Stanulewicz N, Knox E, Narayanasamy M, Shivji N, Khunti K, Blake H. Effectiveness of lifestyle health promotion interventions for nurses: a systematic review. Int J Environ Res Public Health. 2019;17(1):17–26. doi:10.3390/ijerph17010017
25. Taghadosi M, Nouri H. The Effect of Education Based on “Pender Health Promotion Model” on Adherence to Treatment of Patients with Hypertension. J Health Promotion Management. 2023;12(1):69–80.
26. Hair J, Black W, Barry B, Rolph A Multivariate Data Analysis: Pearson new international edition (7a ed). New Jersey: Essex: Pearson. 2014. Available from: https://doc1.bibliothek.li/acd/FLMF050541.pdf.
27. Walker SN, Hill-Polerecky DM. Psychometric Evaluation of the Health-Promoting Lifestyle Profile II. Omaha: University of Nebraska Medical Centre; 1996.
28. Serrano-Fernández M, Boada-Grau J, Vigil-Colet A, Gil-Ripoll C. Adaptación española de la escala HPLP-II con una muestra de empleados. Univ Psychol. 2016;15(4):1–14. doi:10.11144/Javeriana.upsy15-4.aeem
29. Walker S, Kerr M, Pender N, Sechrist K. A Spanish language version of the Health Promoting Lifestyle Profile. Nurs Res. 1990;39(5):268–273. doi:10.1097/00006199-199009000-00003
30. Escobedo Portillo MT, Hernández Gómez JA, Estebané Ortega V, Martínez Moreno G. Modelos de ecuaciones estructurales: características, fases, construcción, aplicación y resultados. Ciencia Trabajo. 2016;18(55):16–22. doi:10.4067/s0718-24492016000100004
31. Organización Panamericana de la Salud y Consejo de Organizaciones Internacionales de las Ciencias Médica. Pautas éticas internacionales para la investigación relacionada con la salud con seres humanos, Cuarta Edición. Ginebra: Consejo de Organizaciones Internacionales de las Ciencias Médicas (CIOMS); 2016.
32. Ministerio de salud de Colombia. Normas científicas, técnicas y administrativas para la administración en salud; 1993. Available from: https://www.minsalud.gov.co/salud/Lists/Normatividad%20%20Salud/DispForm.aspx?ID=2110&ContentTypeId=0x0100A08A4A1DF8E9D448BEF600BFAC0E7622.
33. Gurusamy J, Amudhan S, Veerabhadraiah KB, Palaniappan M. Health-promoting behaviours, their relationships and correlates in nursing students: implications for nursing education and practice. J Professional Nursing. 2022;39:69–75. doi:10.1016/j.profnurs.2022.01.001
34. Mak YW, Kao AHF, Tam LWY, Tse VWC, Tse DTH, Leung DYP. Health-promoting lifestyle and quality of life among Chinese nursing students. Prim Health Care Res Dev. 2018;19(6):629–636. doi:10.1017/S1463423618000208
35. Hwang Y, Oh J. Factors Affecting Health-Promoting Behaviors among Nursing Students. Int J Environ Res Public Health. 2020;17(17):6291. doi:10.3390/ijerph17176291
36. Fashafsheh I, Al-Ghabeesh SH, Ayed A, Salama B, Batran A, Bawadi H. Health-Promoting Behaviors among Nursing Students: Palestinian Perspective. INQUIRY. 2021;58:004695802110187. doi:10.1177/00469580211018790
37. Ü P, Ozen S, Kahraman B. Factors affecting health- promoting behaviors in nursing students at a University in Turkey. J Transcultural Nursing. 2016;27(4):413–419. doi:10.1177/1043659615569536
38. Díez U, Fortis AP, Franco SF. Eficacia de una intervención de promoción de la salud para estudiantes universitarios: un ensayo controlado aleatorio. Invest en Enfermería. 2012;61(2):121–132.
39. Alzahrani SH, Azam A, Bashawri J. Health-promoting lifestyle profile and associated factors among medical students in a Saudi university. SAGE Open Med. 2019;7:1–7. doi:10.1177/2050312119838426
40. Sánchez-Ojeda MA, De Luna-Bertos E. Healthy lifestyles of the university population. Nutricion Hospitalaria. 2015;31(5):1910–1919. doi:10.3305/nh.2015.31.5.8608
41. Shayo FK. Co-occurrence of risk factors for non-communicable diseases among in-school adolescents in Tanzania: an example of a low-income setting of sub-Saharan Africa for adolescence health policy actions. BMC Public Health. 2019;19(1). doi:10.1186/s12889-019-7320-1
42. Victora CG, Adair L, Fall C, et al.; Maternal and Child Undernutrition Study Group. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–357. doi:10.1016/S0140-6736(07)61692-4
43. Kara B. Predictors of health behaviors in Turkish female nursing students. Asian Nurs Res. 2016;10(1):75–81. doi:10.1016/j.anr.2015.12.001
44. Nacar M, Baykan Z, Cetinkaya F, et al. Health promoting lifestyle behaviour in medical students: a multicentre study from Turkey. Asian Pacific J Cancer Prevent. 2014;15(20):8969–8974. doi:10.7314/apjcp.2014.15.20.8969
45. Lolokote S, Hidru TH, Li X. Do socio-cultural factors influence college students’ self-rated health status and health-promoting lifestyles? A cross-sectional multicenter study in Dalian, China. BMC Public Health. 2017;17(1). doi:10.1186/s12889-017-4411-8
46. Kim SJ, Yoo IY. Health Promotion Behavior of Chinese International Students in Korea Including Acculturation Factors: a Structural Equation Model. Asian Nurs Res. 2016;10(1):25–31. doi:10.1016/j.anr.2015.10.008
47. Pender NJ, Pender AR. Attitude, subject norms to engage in health behavior. Nurs Res. 1986;35:15–18. doi:10.1097/00006199-198601000-00004
48. Huang C. Mean-Level Change in Self-Esteem from Childhood through Adulthood: meta-Analysis of Longitudinal Studies. Rev General Psychol. 2010;14(3):251–260. doi:10.1037/a0020543
49. Xiaomiao L, Fangfang Z, Xinkai S, Wenbin G. A study on the relationship between lifestyle, self-esteem and life satisfaction of adolescents in China. J Peking Univ. 2010;42:330–334. doi:10.3969/j.issn.1671-167X.2010.03.018
50. Tremblay MS, Inman JW, Willms JD. The relationship between physical activity, self-esteem, and academic achievement in 12-year-old children. Pediatr Exerc Sci. 2000;12:312–323. doi:10.1123/pes.12.3.312
51. Jambor E, Elliott M. Self-esteem and coping strategies among deaf students. J Deaf Stud Deaf Educ. 2005;10:63–81. doi:10.1093/deafed/eni004
52. Fukuya Y, Fujiwara T, Isumi A, Doi S, Ochi M. Association of birth order with mental health problems, self-esteem, resilience, and happiness among children: results from a-child study. Front Psychiatry. 2021;12:638088. doi:10.3389/fpsyt.2021.638088
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.