Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 9 » Issue 1
Influence of diet and obesity on COPD development and outcomes
Authors Hanson C, Rutten E, Wouters E ![]() , Rennard S
, Rennard S
Received 16 January 2014
Accepted for publication 20 February 2014
Published 5 August 2014 Volume 2014:9(1) Pages 723—733
DOI https://doi.org/10.2147/COPD.S50111
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Corrine Hanson,1 Erica P Rutten,2 Emiel FM Wouters,2,3 Stephen Rennard4
1Division of Medical Nutrition Education, School of Allied Health Professions, University of Nebraska Medical Center, Omaha, NE, USA; 2Research and Education, Centre of Expertise for Chronic Organ Failure, Horn, The Netherlands; 3Department of Pulmonary Diseases, University of Maastricht, Maastricht, The Netherlands; 4Division of Internal Medicine, University of Nebraska Medical Center, Omaha, NE, USA
Abstract: The global increase in the prevalence and incidence of obesity has called serious attention to this issue as a major public health concern. Obesity is associated with many chronic diseases, including cardiovascular disease and diabetes, and recently the role of overweight and obesity in lung disease has received new interest. Independently of obesity, diet also plays a role as a risk factor for many chronic diseases, and evidence is accumulating to support a role for diet in the prevention and management of several lung diseases. Chronic obstructive lung disease is the third-leading cause of death globally, and both obesity and diet appear to play roles in its pathophysiology. Obesity has been associated with decreased lung-function measures in population-based studies, with increased prevalence of several lung diseases and with compromised pulmonary function. In contrast, obesity has a protective effect against mortality in severe chronic obstructive pulmonary disease (COPD). Nutrient intake and dietary patterns have also been associated with lung-function measures and the development and progression of COPD. Taken together, this suggests that a focus on obesity and diet should be part of public health campaigns to reduce the burden of lung disease, and could have important implications for clinicians in the management of their patients. Future research should also focus on elucidating these relationships in diverse populations and age-groups, and on understanding the complex interaction between behavior, environment, and genetics in the development and progression of COPD. The goal of this article is to review current evidence regarding the role that obesity and diet play in the development of COPD, and in COPD-related outcomes.
Keywords: diet, obesity, nutrition, lung function, COPD
Introduction to the prevalence of obesity
According to the World Health Organization (WHO), the worldwide prevalence of obesity has nearly doubled since 1980.1 In 2008, more than 1.4 billion adults (35%) around the world were considered overweight, and of these over 200 million (11%) adults were classified as obese.1 Obesity is commonly defined using body mass index (BMI). The WHO classifications of body weight using BMI are given in Table 1. BMI can be used for both sexes and for all ages of adults, therefore providing a useful population-based measure of body habitus. It does, however, have limitations in that it may not represent the same level of fatness in different individuals. For instance, those with increased muscle mass may have elevated BMI in the presence of low-fat mass, and likewise a high BMI could mask a loss of lean body mass.
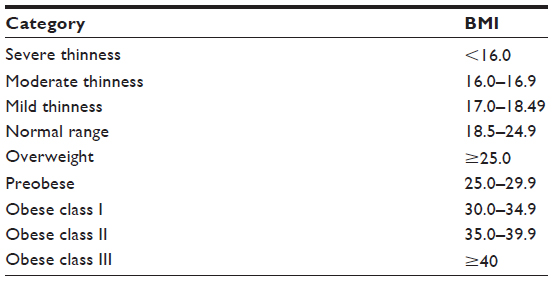 | Table 1 World Health Organization body mass index (BMI) classifications |
National survey data collected in different nations support the increasing prevalence of obesity as a rising public health issue in most developed countries. Most commonly in the US data from the National Health and Nutrition Examination Survey (NHANES) are used to monitor the health and nutrition status of the civilian, noninstitutionalized US population. Data from NHANES in 2009–2010 showed that over a third (35.7%) of all US adults were obese,2 and the rate of increase in the proportion of the population classified as overweight showed an alarming increase from 36.9% in 1976 to 62.0% in 2008.3 Compared to the US, the rate of obesity in Canada is significantly lower (24.1% compared to 34.4% when using 2008 data, P<0.05). However, the rate of increase in obesity in men in Canada of 10% over the last 20 years is comparable to the rate of increase in US men at 12%.4 High prevalence of obesity is also seen in North Africa, the Middle East, Central and Southern Latin America, and southern sub-Saharan Africa, ranging from 27.4% to 31.1%.5
Influence of obesity and diet on the global burden of disease
Overweight and obesity are estimated to be the fifth leading cause of death around the world, which translates into roughly 208 million adults that die each year as a result of overweight or obesity. The WHO also estimates that 44% of the global health burden of diabetes, along with 23% of the ischemic heart burden and between 7% and 41% of the burden of certain cancers, are attributable to overweight and obesity. Increase in BMI is also a major risk factor for degenerative joint conditions, such as osteoarthritis.1
Understanding the contribution of individual risk factors to the overall burden of disease is essential to inform public health initiatives targeting prevention. The Global Burden of Disease (GBD) study provides a global and regional comparative assessment of mortality and disability-adjusted life years (DALYs) attributable to ten major risk factors.6 A category titled “Dietary risk factors and physical inactivity” is one of the ten risk-factor categories, as shown in Table 2. This category is further subdivided into 15 subcategories, 14 of which relate directly to dietary intake. Analysis of the GBD 2010 concluded that dietary risk factors and physical inactivity were responsible for the largest portion of global disease burden, accounting for 10.0% of global DALYs in 2010. Of the individual dietary risk factors, the largest attributable burden was associated with diets low in fruit, followed by diets high in sodium.6 These results also highlighted a dramatic shift in the contribution of risk factors for disease since 1990, from risk factors that mainly cause communicable diseases in children, to risk factors that cause noncommunicable diseases in adults.
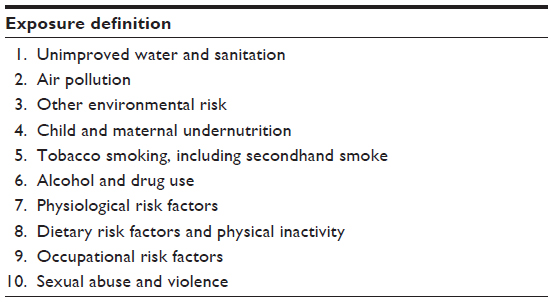 | Table 2 Risk factors for death or disease burden included in Global Burden of Disease Study 2010 |
Chronic obstructive pulmonary disease (COPD) is another condition that is associated with severe morbidity and mortality globally. COPD is characterized by airflow obstruction, and is the umbrella term for two conditions: chronic bronchitis and emphysema, both of which are related to similar etiologies and may coexist. Lung function, which is readily measured by spirometry, is the defining feature of COPD. A low ratio of forced expiratory volume in 1 second (FEV1) to forced vital capacity (FVC) is currently used to define the presence of airflow limitation. Because FVC becomes difficult to measure as disease worsens, measurements of FEV1 are often used as an indicator of disease severity and to describe lung function in epidemiological studies. COPD is currently the third leading cause of death globally.7 A relationship between obesity and COPD is increasingly recognized, though to date remains largely unexplored.
The association between obesity and COPD
The relationship between COPD and body composition has been extensively studied. Most commonly, malnutrition has been examined in relationship to COPD, and it is well accepted that undernutrition in COPD patients contributes to poor outcomes. Underweight and low BMI are independent risk factors for mortality in patients with COPD.8,9 However, given the global increase in risk factors related to development and progression of noncommunicable diseases, recently there has been increased interest in the interrelationship between obesity and COPD.
Data exist to support the coexistence of obesity and COPD.10 In 650,000 subjects evaluated as part of the Canadian National Health Survey, the prevalence of obesity was significantly higher in COPD subjects when compared to those without COPD (24.6% and 17.1%, respectively, P<0.001).11 However, the prevalence of obesity in subjects with self-reported COPD increased by 5% over a 14-year period, while it rose by 38% in non-COPD subjects over the same period.11 Patients with COPD in the Netherlands had an obesity prevalence of 18%, and the highest rates were in patients with milder spirometric disease severity (GOLD [Global initiative for chronic Obstructive Lung Disease] 1 and 2) and was lowest in those with severe disease (GOLD 4) (16%–24% versus 6%).12 An even higher prevalence of obesity was reported in an adult multiethnic cohort of early stage COPD patients in the US.13 In this study, 54% of subjects had BMI measurement of greater than 30, compared to the 20%–24% reported prevalence for the general adult population of that region. These data suggest that obesity is more prevalent in patients with COPD than in the general population; however, not all studies confirm this finding. In a population-based study conducted in five Latin American cities, there were higher proportions of COPD subjects in the underweight and normal-weight categories when compared to non-COPD patients, and a lower proportion in the obese category. There were also no differences in BMI among the GOLD strata. The prevalence of obesity in those with COPD was 23%, compared to 32% in subjects without COPD.14
The role of BMI relative to the risk of impaired lung function has also been investigated. Obesity is known to contribute to other respiratory illnesses, including asthma, sleep apnea, pulmonary embolism, and hypoventilation syndrome,15,16 making it logical to investigate obesity as a risk factor for loss of lung function. Reductions in FEV1 and FVC have been documented in extremely obese subjects, as well as a reduction in lung volume.17,18 Both BMI and weight gain have been associated with declines in lung function in the general population.19–21 A large cross-sectional, population-based study conducted in France concluded that abdominal obesity was the strongest predictor of lung-function impairment (odds ratio [OR] 1.94, 95% confidence interval [CI] 1.80–2.09; and OR 2.1, 95% CI 1.95–2.29; for FEV1 and FVC, respectively).22 Waist circumference and waist-to-hip ratio have been associated with lung function in normal weight, overweight, and obese adults,23,24 suggesting that distribution of fat (ie, subcutaneous versus visceral fat mass or abdominal versus lower-extremity fat mass) may be important. However, conflicting reports exist, as one study did not find any relationship between total lung capacity and truncal fat volume.25 Longitudinal evaluation of age-related changes in lung function relative to BMI found that among healthy young adults, FEV1 and FVC decrease both with higher baseline BMI and with increasing BMI over time, and that those subjects who reduced their BMI also increased these lung-function parameters.20,26 Obesity, however, also has a protective effect on the level of hyperinflation as a consequence of a decreasing static lung volume with increasing BMI.27
Obesity is a complex metabolic condition that influences many physiological systems. Adipose tissue is often considered to be an abundant source of proinflammatory mediators.15,28 Systemic inflammation is considered a hallmark of COPD,29 and increased levels of proinflammatory mediators have been reported in the circulation of COPD patients.29–33 However, not all patients with COPD demonstrate systemic inflammation. In the ECLIPSE (Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints) study, only 16% of patients with COPD had persistent systemic inflammation at baseline.34 However, it is interesting to note that the patients with systemic inflammation in this study were more obese, with a mean BMI of 29.4, compared to a mean BMI of 25.6 in the group without persistent systemic inflammation.34 Increased levels of systemic inflammation had been earlier reported in relation to excessive fat mass in COPD patients. Specifically, tumor necrosis factor-α, interleukin (IL)-6 and leptin plasma levels have been shown to be significantly increased in overweight/obese COPD patients compared with normal-weight patients,35 and the likelihood of having elevated C-reactive protein in COPD patients was found to be 3.3 times higher in obese patients (BMI≥30) compared to normal-weight patients, after adjusting for relevant confounders.36 A study by Rutten et al also demonstrated that abdominal fat mass is positively associated with plasma C-reactive protein levels in patients with COPD.37 Interestingly, it has been shown that nonobese patients with COPD have more visceral fat mass compared to control subjects, and this was associated with increased IL-6 levels.38 Whether this contributes to the pathophysiology of COPD has yet to be determined.
The impact of obesity on COPD outcomes
Patients with COPD are at increased risk for the development of comorbid conditions often associated with obesity, including cardiovascular disease,39 diabetes,40 and metabolic syndrome.41 Metabolic syndrome is a cluster of risk factors (ie, hypertension, dyslipidemia, glucose intolerance) associated with an increased risk for the development of type 2 diabetes and cardiovascular disease.42 Studies investigating the prevalence of metabolic syndrome in patients with COPD have shown increased rates of metabolic syndrome in COPD subjects when compared to those without COPD.43 In a small study of patients with severe COPD referred for pulmonary rehabilitation, 47% of patients fulfilled the diagnostic criteria for metabolic syndrome, compared to 21% in age- and sex-matched controls.44 Similar results were reported in a larger study including patients with chronic bronchitis and COPD.45 In a large cross-sectional population-based study, the risk of metabolic syndrome was 40% higher in subjects with restrictive lung-function impairment compared to subjects with normal lung function.22
It has long been recognized that obese individuals experience increased symptoms of dyspnea and more exercise limitation than nonobese individuals, independently of the presence of airflow limitation.10,46 Because of extrinsic compression of the chest, obesity causes a reduction in vital capacity, which is most marked in the expiratory reserve volume.17,47 Functional residual capacity may approach residual volume with marked obesity.48 The compression of the lung tissue can lead to atelectasis, compromising ventilation–perfusion matching and thus leading to hypoxemia, which may correct with exercise and deeper inhalation. The reduction in lung operating volumes leads to expiratory airflow limitation and dynamic hyperinflation.49,50 In asthma, this worsens with bronchospasm.51 Together with the increased oxygen cost for exercise due to the metabolic cost resulting from the increased weight, this dynamic hyperinflation likely contributes to the dyspnea on exertion noted by obese individuals and particularly those with asthma. In contrast to individuals with normal lungs and with asthma, obese patients with COPD do not experience more dyspnea than normal-weight COPD patients with similar degrees of obstruction at similar work rates.27,52 Recently however, data of the ECLIPSE study showed more dyspnea and lower health status in obese compared to normal-weight COPD patients.53
There have been several studies that have investigated the impact of obesity on mortality in patients with COPD.8,54–59 In the epidemiological Copenhagen City Heart Study, obesity was associated with a 20%–34% increase in the relative risk (RR) of all-cause mortality in patients with mild-to-moderate COPD compared to normal-BMI patients with comparable disease severity.8 However, the relative risk of all-cause mortality and COPD-related mortality was 0.62 and 0.31, respectively, in patients with severe COPD compared to normal-weight patients with severe disease.8 This suggests that obesity may exert different effects depending on disease severity. Other studies investigating the relationship between body weight and mortality in COPD patients have also observed a potential protective effect of obesity in those with severe COPD.54,60 A recent meta-analysis concluded that underweight individuals with COPD were associated with higher mortality (RR 1.34, 95% CI 1.01–1.78), while both overweight and obese people were associated with a decrease in mortality (RR 0.47, 95% CI 0.33–0.68; and RR 0.59, 95% CI 0.38–0.91; respectively) when compared to those with a normal BMI.55 A recent study that enrolled 968 patients hospitalized for acute exacerbation of COPD and followed them for a median time of 3.26 years found that higher BMI was predictive of survival, with each 1 kg/m2 unit increase in BMI associated with 5% lower chance of death (hazard ratio 0.95, 95% CI 0.93–0.97).56 This possible association between obesity and improvement in outcomes in patients with COPD would seem to contrast with the epidemiological data for the general population, in which obesity is usually associated with a decreased life span.61 This phenomenon known as the “obesity paradox”,62 and the reasons for this protective effect of obesity have been extremely difficult to elucidate.63 Studies evaluating the obesity paradox in COPD are shown in Table 3.
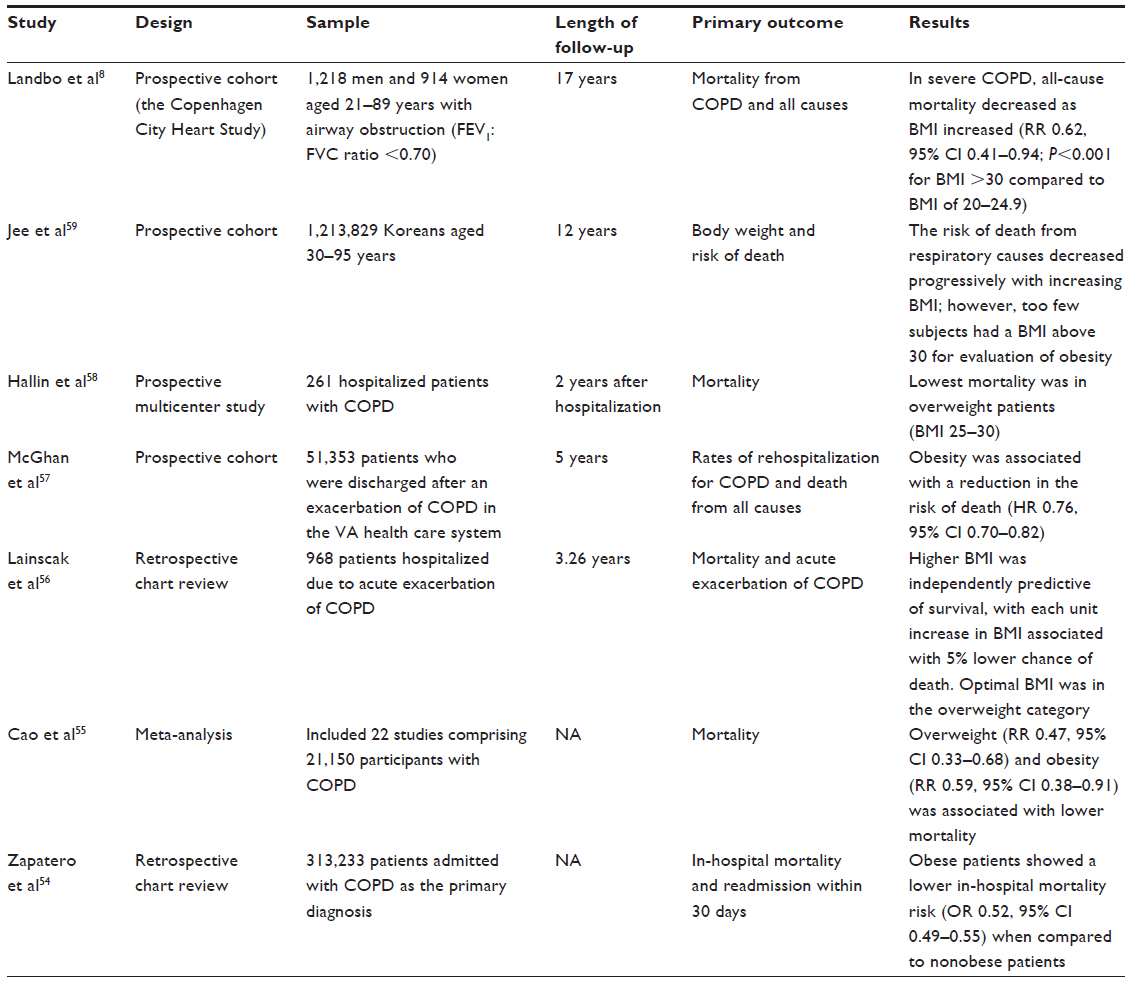 | Table 3 Studies investigating the “obesity paradox” in COPD |
In comparison to mortality outcomes, there are even fewer data assessing the relationships between obesity and other COPD outcomes, such as progression of disease or exacerbations. While there is some evidence supporting a positive effect of obesity on such parameters,64,65 this is an area that requires future research.
Effect of diet on lung function and the development of COPD
Epidemiological studies have documented a relationship between dietary intake and the maintenance of lung function and prevention of COPD. Analysis of NHANES data in the US population has shown that increased intakes of certain nutrients, including vitamin E, vitamin C, and total carotenes were all positively associated with FEV1.66 Epidemiological studies in other parts of the world concur with this finding, including the MORGEN (monitoring project on risk factors and health in the Netherlands) study in Dutch adults, which found higher FEV1 and FVC in those with high intakes of vitamin C and β-carotene,67 and a comparable study in Nottingham, UK, which found that intakes of both vitamins C and E were independently associated with measures of lung function.68 In a cross-sectional study in rural China, Hu et al calculated an increase of 21.6 mL in FEV1 (95% CI −0.4 to 43.5) and of 25 mL for FVC (95% CI 0.2–49.6) for every 100 mg/day greater vitamin C intake.69 Similar results for a relationship between lung function and vitamin E intake have been demonstrated in Finland,70 and vitamin C and β-carotene intake in Scotland.71 It has been speculated that these relationships may be due in part to the antioxidant and anti-inflammatory properties of these nutrients. Indeed, intake of individual nutrients in COPD has been shown to modulate serum markers of oxidative stress. In a study of 267 stable COPD patients, intake of vitamin E was associated with decreased carbonyls (P=0.05), and olive oil (which is high in ω -3 polyunsaturated fatty acids) was associated with an increase in the anti-inflammatory compound glutathione (P=0.01). Intake of vegetables was also related to a decrease in inflammatory compounds in former smokers.72 However, not all studies confirm this relationship. In the Zutphen study, the intake of specific antioxidants was not associated with the development of nonspecific lung disease; however, higher intake of fruits (which are high in antioxidant compounds) was inversely related to disease development.73
Vitamin D status has also been related to measures of lung function;74–76 however, these results remain conflicting.77 Serum 25-hydroxyvitamin D levels are the currently used functional marker of vitamin D status,78 and while vitamin D status is influenced by inputs other than diet, such as sun exposure, it is nonetheless a nutrient of interest in COPD. Intake of low-fat dairy products, but not specifically vitamin D, was associated with less severe measures of emphysema (defined by lung density on computed tomography) in 3,271 subjects enrolled in the MESA (Multi-Ethnic Study of Atherosclerosis) trial (P=0.02 and 0.01 for α, a measure of emphysema, and apical versus basilar distribution of emphysema, respectively).79
Although most studies evaluating the relationship between micronutrient intake and lung function are cross-sectional in nature, there are a small number of longitudinal studies available. In one such study, dietary intake and FEV1 were measured in a cross-sectional study in 2,633 adults. Nine years later, these measures were repeated in 1,346 of the subjects. Higher intakes of vitamin C were associated with higher levels of FEV1 at both points in time, and the decline in FEV1 was lowest among those with higher average vitamin C intake by 50.8 mL/5 years (95% CI 3.8–97.9) for each 100 mg of vitamin C a day.80 Another longitudinal study that followed subjects for 4 years found higher vitamin C intakes and higher intake of fruits and vegetables were associated with an 18 and 24 mL/year slower rate of FEV1 decline when compared to the lower-intake group (P=0.001 and 0.003, respectively).81
Because nutrients do not occur in isolation and are part of an overall diet, studies have also been conducted to determine if an individual’s dietary pattern is related to measures of lung function. Observational studies have shown that adults following a “prudent” diet (defined as diets high in intakes of fruit, vegetables, oily fish, and whole grains) are positively associated with FEV1.82–85 Indeed, prudent diets have also been associated with a significant reduction in the OR for the development of COPD, with reductions in risk ranging from 25% to 54%.82,84,85 In a rare longitudinal study conducted over 5 years to evaluate the effect of dietary patterns, a traditional diet (higher intake of meat and potatoes, lower intake of soy and cereal) was associated with lower FEV1 (P<0.001) and an increased prevalence of COPD, and the highest quintile of the refined-food diet (higher intakes of mayonnaise, salty snacks, candy, high-sugar beverages, white bread) had a significantly greater decline in lung function over 5 years (−48.5 mL, 95% CI −80.7 to −16.3) when compared to the lowest quintile of the refined-food diet.86
Increased consumption of fruits and vegetables has been shown to be inversely associated with the development of COPD in several studies.87–89 Other dietary components have been implicated in COPD as well, including tea and processed meats. Black tea consumption has been shown to be significantly higher in smokers who did not develop COPD, compared to smokers who did develop COPD.90 Tea is considered a rich source of antioxidants due to the high concentration of polyphenols. A high intake of cured meats, which are high in nitrates, has been positively associated with the risk of newly diagnosed COPD and a pattern of obstructive lung disease.91,92
Effect of diet on outcomes in COPD
In addition to lung-function parameters, diet has been shown to play a role in outcomes related to COPD. Indeed, one study showed an inverse trend for 20-year COPD mortality across tertiles of fruit intake,93 with a 100 g increase in fruit intake at baseline associated with a 24% lower COPD mortality risk.93 Analysis of the Seven Countries Study, a population-based cohort of 12,763 men, calculated that fruit and fish intake together explained about 67% of the variation in COPD mortality rates after 25 years.94 In an interventional study of patients with known COPD, 120 subjects were randomized to follow either a diet based on a high consumption of fruit and vegetables, or a usual diet for 3 years. The COPD patients who followed a diet with a high intake of fruits and vegetables showed an annual increase in the percentage predicted FEV1, compared to patients on their usual diet, who showed a decrease in FEV1 over 3 years (P=0.03).95 However, a study of 75 subjects followed for 12 weeks showed that while COPD patients were able to increase their intake of fruits and vegetables, there were no significant changes in systemic or airway markers of inflammation or oxidative stress between groups randomized to increase their fruit and vegetable intake and controls.96 In a study of vitamin D supplementation in COPD, no effect on the rate of exacerbations was seen in the entire population; however, analysis of a subset of patients with severe vitamin D deficiency did show an improvement.97
Implications for treatment
Given the conflicting evidence on the role of diet and lung function, and such phenomena as the obesity paradox with COPD, how should health care providers proceed? It can be suggested that clinicians should consider the possible protective effects of BMI before implementing weight-loss programs in COPD patients, especially in those with severe-lung function impairment. In patients who are overweight or obese, fat-free mass index has been shown to be associated with higher exercise capacity;98 therefore, therapies that promote weight loss without the loss of lean body mass should be considered. Obese patients with COPD can be expected to show improvement in pulmonary rehabilitation programs, and referrals should be made as such.99–101 Furthermore, concurrent comorbidity related to obesity, such as cardiovascular disease, diabetes mellitus type II, and hypertension, should be screened and treated.
Although some results are conflicting, there is a great body of evidence that micronutrient intake is associated with better lung function in the general population and in patients with COPD.66–70 An adequate intake of micronutrients may be of specific concern in obese COPD patients, as poor dietary quality and inadequate intake of micronutrients has been documented in this population.102 As only few intervention studies are available, we are not prone to support micronutrient supplementation for these patients per se.103–105 However, based on the available research, patients with COPD might benefit even more from a healthy diet, and attention should be given to these effects.95
If there is an association between micronutrients and lung function, should clinicians consider supplementation of micronutrients in their patients? In one study, adults at high risk for cardiovascular events received antioxidant vitamins for 5 years (600 mg vitamin E, 250 mg vitamin C, 20 mg β-carotene), and the intervention had no effect on lung function.103 While vitamin A supplementation showed beneficial effects on lung function in a small trial (n=12) of smokers with COPD,104 another large trial showed a significantly higher incidence of lung cancer in current smokers supplemented with α-tocopherol and β-carotene for 5–8 years.105 However, a high intake of β-carotene and vitamin E from food was associated with an improvement in respiratory symptoms.106 The latter study seems to suggest that prevention campaigns should stress the importance of nutrient intake from food, especially in smokers. Supplementation of vitamin D in severely deficient populations (<10 ng/mL) may have a positive impact on rates of exacerbation of COPD;97 however, no impact on exacerbations has been identified in patients with higher 25-hydroxyvitamin D levels. There is evidence that a significant proportion of patients with COPD are vitamin D deficient,75,107 and careful monitoring of vitamin D status in this population may be prudent. There is also some evidence that nutritional factors can reduce the risk for lung disease associated with such factors as pollution and smoking.108–110 Similarly, a recent trial found that vitamin C supplementation during pregnancy improved pulmonary function among newborns of smoking women, particularly among women with genotypes associated with smoking-related lung disease and addiction.111
Conclusion and future directions
A causal relation between obesity, diet, and lung function is not directly proven yet, but the data exist to suggest a link between these factors. Given the growing worldwide problem of obesity in relation to its related comorbidities, strategies for prevention and treatment are essential. Whether treatment of obesity also results in long-term effects in patients with COPD needs further investigation. In addition, the contribution of visceral fat mass, irrespective of total body fat mass, to the pathophysiology of COPD needs to be further explored in future studies.
Lung-function impairment and COPD can be viewed as a complex systemic disease with much comorbidity that may require a more comprehensive approach to its management. The evidence would seem to indicate that nutritional interventions aimed at increasing the intake of certain nutrients and controlling obesity might have beneficial outcomes in both primary prevention and management of lung impairment. Targeting the inflammation associated with COPD with nutrients that have powerful anti-inflammatory effects might be a novel approach to treatment. Current nutritional guidelines for the management of patients with COPD, such as GOLD, do not provide any specific guidance to either patients or health care practitioners other than to avoid weight loss. As the relationships between diet, obesity, and COPD are further elucidated, public health campaigns targeting weight-management strategies and optimal intakes of nutrients with anti-inflammatory properties for improvement in lung function and attenuation of inflammation can be implemented. However, COPD is an extremely heterogeneous disease, and approaches to diet and weight that benefit one subset of COPD patients may not have the same effect in other subsets.
While there does appear to be a relationship between obesity and lung function, it remains unknown if this holds true for diverse populations. Future directions for research could include interventional studies designed to assess if a change in BMI or measures of abdominal obesity results in a corresponding change in lung-function measures, and the effect of these parameters at different points in the life cycle. With a rise in pediatric obesity that is paralleling, or even outpacing, the rise in obesity in the adult population, this becomes an important demographic to study. Diseases like COPD are complex, multifactorial diseases, involving interactions between environmental, genetic, and behavioral factors.
It is always a challenge to separate the direct effect of one lifestyle factor, such as obesity or diet, from other overall effects of associated lifestyle factors. However, given the role of inflammation in the development of COPD, the mechanical and inflammatory effects of obesity,10 and the possible anti-inflammatory effects of certain nutrients, a biological relationship is readily plausible. Given that lung-function measures are an independent predictor of mortality in both the general population and in those with COPD,112,113 public health initiatives targeting obesity and diet could have a profound impact on global health.
Disclosure
SR discloses that he has had or currently has a number of relationships with companies who provide products and/or services relevant to the outpatient management of chronic obstructive pulmonary disease. These relationships include serving as a consultant, advising regarding clinical trials, speaking at continuing medical education programs, and performing funded research at both basic and clinical levels. He does not own any stock in any pharmaceutical companies. Specific companies and institutions with whom he has had relationships to date in 2013 include: (consultant) Align2Action, GlaxoSmithKline, Almirall, HealthStar, Boehringer, Ingelheim, Lek, Under Decision Resources, McKinsey, Dunn Group, Navigant, Easton Associates, Penn Technology, Elevation Pharma, Strategic North, Forest, Synapse, Gerson, and Telecon SC; (speaker) CME Incite, Nuvis, Forest, Pro-iMed, Incite, Takeda, IntraMed (Forest); and (advisory board) AstraZeneca, Pearl, Forest, Pfizer, and Johnson and Johnson. EFMW is a member of the scientific advisory boards for GlaxoSmithKline, Nycomed, and Novartis and received lecture fees from GlaxoSmithKline, AstraZeneca, Nycomed, Numico, and Novartis. The other authors report no conflicts of interest in this work.
References
World Health Organization. Obesity and overweight. 2013. Available from: http://apps.who.int/bmi/index.jsp?introPage=intro_3.html. Accessed December 6, 2013. | |
Ogden CL, Carroll MD, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009–2010. NCHS Data Brief. 2012;(82):1–8. | |
Singh GK, Siahpush M, Hiatt RA, Timsina LR. Dramatic increases in obesity and overweight prevalence and body mass index among ethnic-immigrant and social class groups in the United States, 1976–2008. J Community Health. 2011;36(1):94–110. | |
Shields M, Carroll MD, Ogden CL. Adult obesity prevalence in Canada and the United States. NCHS Data Brief. 2011;(56):1–8. | |
Pérez Rodrigo C. Current mapping of obesity. Nutr Hosp. 2013;28 Suppl 5:21–31. | |
Lim SS, Vos T, Flaxman AD, et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2224–2260. | |
Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. | |
Landbo C, Prescott E, Lange P, Vestbo J, Almdal TP. Prognostic value of nutritional status in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1999;160(6):1856–1861. | |
Chailleux E, Laaban JP, Veale D. Prognostic value of nutritional depletion in patients with COPD treated by long-term oxygen therapy: data from the ANTADIR observatory. Chest. 2003;123(5):1460–1466. | |
Franssen FM, O’Donnell DE, Goossens GH, Blaak EE, Schols AM. Obesity and the lung: 5. Obesity and COPD. Thorax. 2008;63(12):1110–1117. | |
Vozoris NT, O’Donnell DE. Prevalence, risk factors, activity limitation and health care utilization of an obese, population-based sample with chronic obstructive pulmonary disease. Can Respir J. 2012;19(3):e18–e24. | |
Steuten LM, Creutzberg EC, Vrijhoef HJ, Wouters EF. COPD as a multicomponent disease: inventory of dyspnoea, underweight, obesity and fat free mass depletion in primary care. Prim Care Respir J. 2006;15(2):84–91. | |
Eisner MD, Blanc PD, Sidney S, et al. Body composition and functional limitation in COPD. Respir Res. 2007;8:7. | |
Montes de Oca M, Tálamo C, Perez-Padilla R, et al. Chronic obstructive pulmonary disease and body mass index in five Latin America cities: the PLATINO study. Respir Med. 2008;102(5):642–650. | |
Mancuso P. Obesity and lung inflammation. J Appl Physiol (1985). 2010;108(3):722–728. | |
McClean KM, Kee F, Young IS, Elborn JS. Obesity and the lung: 1. Epidemiology. Thorax. 2008;63(7):649–654. | |
Costa D, Barbalho MC, Miguel GP, Forti EM, Azevedo JL. The impact of obesity on pulmonary function in adult women. Clinics (Sao Paulo). 2008;63(6):719–724. | |
Biring MS, Lewis MI, Liu JT, Mohsenifar Z. Pulmonary physiologic changes of morbid obesity. Am J Med Sci. 1999;318(5):293–297. | |
Ubilla C, Bustos P, Amigo H, Oyarzun M, Rona RJ. Nutritional status, especially body mass index, from birth to adulthood and lung function in young adulthood. Ann Hum Biol. 2008;35(3):322–333. | |
Thyagarajan B, Jacobs DR Jr, Apostol GG, et al. Longitudinal association of body mass index with lung function: the CARDIA study. Respir Res. 2008;9:31. | |
Lazarus R, Sparrow D, Weiss ST. Effects of obesity and fat distribution on ventilatory function: the normative aging study. Chest. 1997;111(4):891–898. | |
Leone N, Courbon D, Thomas F, et al. Lung function impairment and metabolic syndrome: the critical role of abdominal obesity. Am J Respir Crit Care Med. 2009;179(6):509–516. | |
Chen Y, Rennie D, Cormier YF, Dosman J. Waist circumference is associated with pulmonary function in normal-weight, overweight, and obese subjects. Am J Clin Nutr. 2007;85(1):35–39. | |
Canoy D, Luben R, Welch A, et al. Abdominal obesity and respiratory function in men and women in the EPIC-Norfolk study, United Kingdom. Am J Epidemiol. 2004;159(12):1140–1149. | |
Watson RA, Pride NB, Thomas EL, Ind PW, Bell JD. Relation between trunk fat volume and reduction of total lung capacity in obese men. J Appl Physiol (1985). 2012;112(1):118–126. | |
Bottai M, Pistelli F, Di Pede F, et al. Longitudinal changes of body mass index, spirometry and diffusion in a general population. Eur Respir J. 2002;20(3):665–673. | |
Ora J, Laveneziana P, Ofir D, Deesomchok A, Webb KA, O’Donnell DE. Combined effects of obesity and chronic obstructive pulmonary disease on dyspnea and exercise tolerance. Am J Respir Crit Care Med. 2009;180(10):964–971. | |
Sood A. Obesity, adipokines, and lung disease. J Appl Physiol (1985). 2010;108(3):744–753. | |
Gan WQ, Man SF, Senthilselvan A, Sin DD. Association between chronic obstructive pulmonary disease and systemic inflammation: a systematic review and a meta-analysis. Thorax. 2004;59(7):574–580. | |
Koehler F, Doehner W, Hoernig S, Witt C, Anker SD, John M. Anorexia in chronic obstructive pulmonary disease – association to cachexia and hormonal derangement. Int J Cardiol. 2007;119(1):83–89. | |
Yasuda N, Gotoh K, Minatoguchi S, et al. An increase of soluble fas, an inhibitor of apoptosis, associated with progression of COPD. Respir Med. 1998;92(8):993–999. | |
Vernooy JH, Kucukaycan M, Jacobs JA, et al. Local and systemic inflammation in patients with chronic obstructive pulmonary disease: soluble tumor necrosis factor receptors are increased in sputum. Am J Respir Crit Care Med. 2002;166(9):1218–1224. | |
Petersen AM, Penkowa M, Iversen M, et al. Elevated levels of IL-18 in plasma and skeletal muscle in chronic obstructive pulmonary disease. Lung. 2007;185(3):161–171. | |
Agusti A, Edwards LD, Rennard SI, et al. Persistent systemic inflammation is associated with poor clinical outcomes in COPD: a novel phenotype. PLoS One. 2012;7(5):e37483. | |
Poulain M, Doucet M, Drapeau V, et al. Metabolic and inflammatory profile in obese patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2008;5(1):35–41. | |
Breyer MK, Spruit MA, Celis AP, et al. Highly elevated C-reactive protein levels in obese patients with COPD: a fat chance? Clin Nutr. 2009;28(6):642–647. | |
Rutten EP, Breyer MK, Spruit MA, et al. Abdominal fat mass contributes to the systemic inflammation in chronic obstructive pulmonary disease. Clin Nutr. 2010;29(6):756–760. | |
van den Borst B, Gosker HR, Wesseling G, et al. Low-grade adipose tissue inflammation in patients with mild-to-moderate chronic obstructive pulmonary disease. Am J Clin Nutr. 2011;94(6):1504–1512. | |
Mannino DM, Thorn D, Swensen A, Holguin F. Prevalence and outcomes of diabetes, hypertension and cardiovascular disease in COPD. Eur Respir J. 2008;32(4):962–969. | |
Feary JR, Rodrigues LC, Smith CJ, Hubbard RB, Gibson JE. Prevalence of major comorbidities in subjects with COPD and incidence of myocardial infarction and stroke: a comprehensive analysis using data from primary care. Thorax. 2010;65(11):956–962. | |
Park SK, Larson JL. Metabolic syndrome and associated factors in people with chronic obstructive pulmonary disease. West J Nurs Res. Epub November 29, 2013. | |
Alberti KG, Zimmet P, Shaw J. The metabolic syndrome – a new worldwide definition. Lancet. 2005;366(9491):1059–1062. | |
Paek YJ, Jung KS, Hwang YI, Lee KS, Lee DR, Lee JU. Association between low pulmonary function and metabolic risk factors in Korean adults: the Korean national health and nutrition survey. Metabolism. 2010;59(9):1300–1306. | |
Marquis K, Maltais F, Duguay V, et al. The metabolic syndrome in patients with chronic obstructive pulmonary disease. J Cardiopulm Rehabil. 2005;25(4):226–232; discussion 233–234. | |
Watz H, Waschki B, Kirsten A, et al. The metabolic syndrome in patients with chronic bronchitis and COPD: frequency and associated consequences for systemic inflammation and physical inactivity. Chest. 2009;136(4):1039–1046. | |
Sin DD, Jones RL, Man SF. Obesity is a risk factor for dyspnea but not for airflow obstruction. Arch Intern Med. 2002;162(13):1477–1481. | |
Wasserman K, Hansen JE, Sue DY, Stringer WW, Whipp B. Principles of Exercise Testing and Interpretation: Including Pathophysiology and Clinical Applications. Philadelphia: Lippincott Williams & Wilkins; 2005. | |
Salome CM, King GG, Berend N. Physiology of obesity and effects on lung function. J Appl Physiol (1985). 2010;108(1):206–211. | |
Ferretti A, Giampiccolo P, Cavalli A, Milic-Emili J, Tantucci C. Expiratory flow limitation and orthopnea in massively obese subjects. Chest. 2001;119(5):1401–1408. | |
Koutsoukou A, Koulouris N, Bekos B, et al. Expiratory flow limitation in morbidly obese postoperative mechanically ventilated patients. Acta Anaesthesiol Scand. 2004;48(9):1080–1088. | |
Sutherland TJ, Cowan JO, Taylor DR. Dynamic hyperinflation with bronchoconstriction: differences between obese and nonobese women with asthma. Am J Respir Crit Care Med. 2008;177(9):970–975. | |
Ora J, Laveneziana P, Wadell K, Preston M, Webb KA, O’Donnell DE. Effect of obesity on respiratory mechanics during rest and exercise in COPD. J Appl Physiol (1985). 2011;111(1):10–19. | |
Rutten EP, Calverley PM, Casaburi R, et al. Changes in body composition in patients with chronic obstructive pulmonary disease: do they influence patient-related outcomes? Ann Nutr Metab. 2013;63(3):239–247. | |
Zapatero A, Barba R, Ruiz J, et al. Malnutrition and obesity: influence in mortality and readmissions in chronic obstructive pulmonary disease patients. J Hum Nutr Diet. 2013;26 Suppl 1:16–22. | |
Cao C, Wang R, Wang J, Bunjhoo H, Xu Y, Xiong W. Body mass index and mortality in chronic obstructive pulmonary disease: a meta-analysis. PLoS One. 2012;7(8):e43892. | |
Lainscak M, von Haehling S, Doehner W, et al. Body mass index and prognosis in patients hospitalized with acute exacerbation of chronic obstructive pulmonary disease. J Cachexia Sarcopenia Muscle. 2011;2(2):81–86. | |
McGhan R, Radcliff T, Fish R, Sutherland ER, Welsh C, Make B. Predictors of rehospitalization and death after a severe exacerbation of COPD. Chest. 2007;132(6):1748–1755. | |
Hallin R, Gudmundsson G, Suppli Ulrik C, et al. Nutritional status and long-term mortality in hospitalised patients with chronic obstructive pulmonary disease (COPD). Respir Med. 2007;101(9):1954–1960. | |
Jee SH, Sull JW, Park J, et al. Body-mass index and mortality in Korean men and women. N Engl J Med. 2006;355(8):779–787. | |
Schols AM, Slangen J, Volovics L, Wouters EF. Weight loss is a reversible factor in the prognosis of chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 1998;157(6 Pt 1):1791–1797. | |
Peeters A, Barendregt JJ, Willekens F, et al. Obesity in adulthood and its consequences for life expectancy: a life-table analysis. Ann Intern Med. 2003;138(1):24–32. | |
Lavie CJ, Ventura HO, Milani RV. The “obesity paradox”: is smoking/lung disease the explanation? Chest. 2008;134(5):896–898. | |
Guenette JA, Jensen D, O’Donnell DE. Respiratory function and the obesity paradox. Curr Opin Clin Nutr Metab Care. 2010;13(6):618–624. | |
Hurst JR, Vestbo J, Anzueto A, et al. Susceptibility to exacerbation in chronic obstructive pulmonary disease. N Engl J Med. 2010;363(12):1128–1138. | |
Watson L, Vonk JM, Lofdahl CG, et al. Predictors of lung function and its decline in mild to moderate COPD in association with gender: results from the Euroscop study. Respir Med. 2006;100(4):746–753. | |
Hu G, Cassano PA. Antioxidant nutrients and pulmonary function: the third national health and nutrition examination survey (NHANES III). Am J Epidemiol. 2000;151(10):975–981. | |
Grievink L, Smit HA, Ocké MC, van’t Veer P, Kromhout D. Dietary intake of antioxidant (pro)-vitamins, respiratory symptoms and pulmonary function: the MORGEN study. Thorax. 1998;53(3):166–171. | |
Britton JR, Pavord ID, Richards KA, et al. Dietary antioxidant vitamin intake and lung function in the general population. Am J Respir Crit Care Med. 1995;151(5):1383–1387. | |
Hu G, Zhang X, Chen J, Peto R, Campbell TC, Cassano PA. Dietary vitamin C intake and lung function in rural China. Am J Epidemiol. 1998;148(6):594–599. | |
Tabak C, Smit HA, Rasanen L, et al. Dietary factors and pulmonary function: a cross sectional study in middle aged men from three European countries. Thorax. 1999;54(11):1021–1026. | |
Chen R, Tunstall-Pedoe H, Bolton-Smith C, Hannah MK, Morrison C. Association of dietary antioxidants and waist circumference with pulmonary function and airway obstruction. Am J Epidemiol. 2001;153(2):157–163. | |
de Batlle J, Barreiro E, Romieu I, et al. Dietary modulation of oxidative stress in chronic obstructive pulmonary disease patients. Free Radic Res. 2010;44(11):1296–1303. | |
Miedema I, Feskens EJ, Heederik D, Kromhout D. Dietary determinants of long-term incidence of chronic nonspecific lung diseases. The Zutphen study. Am J Epidemiol. 1993;138(1):37–45. | |
Black PN, Scragg R. Relationship between serum 25-hydroxyvitamin D and pulmonary function in the third national health and nutrition examination survey. Chest. 2005;128(6):3792–3798. | |
Berg I, Hanson C, Sayles H, et al. Vitamin D, vitamin D binding protein, lung function and structure in COPD. Respir Med. 2013;107(10):1578–1588. | |
Janssens W, Bouillon R, Claes B, et al. Vitamin D deficiency is highly prevalent in COPD and correlates with variants in the vitamin D-binding gene. Thorax. 2010;65(3):215–220. | |
Shaheen SO, Jameson KA, Robinson SM, et al. Relationship of vitamin D status to adult lung function and COPD. Thorax. 2011;66(8):692–698. | |
Food and Nutrition Board, Institute of Medicine of the National Academies. Dietary Reference Intakes: Calcium and Vitamin D. Washington: National Academies; 2011. | |
Jiang R, Jacobs DR, He K, et al. Associations of dairy intake with CT lung density and lung function. J Am Coll Nutr. 2010;29(5):494–502. | |
McKeever TM, Scrivener S, Broadfield E, Jones Z, Britton J, Lewis SA. Prospective study of diet and decline in lung function in a general population. Am J Respir Crit Care Med. 2002;165(9):1299–1303. | |
Bentley AR, Kritchevsky SB, Harris TB, et al. Dietary antioxidants and forced expiratory volume in 1 s decline: the health, aging and body composition study. Eur Respir J. 2012;39(4):979–984. | |
Shaheen SO, Jameson KA, Syddall HE, et al. The relationship of dietary patterns with adult lung function and COPD. Eur Respir J. 2010;36(2):277–284. | |
Tabak C, Smit HA, Heederik D, Ocke MC, Kromhout D. Diet and chronic obstructive pulmonary disease: independent beneficial effects of fruits, whole grains, and alcohol (the MORGEN study). Clin Exp Allergy. 2001;31(5):747–755. | |
Varraso R, Fung TT, Barr RG, Hu FB, Willett W, Camargo CA Jr. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US women. Am J Clin Nutr. 2007;86(2):488–495. | |
Varraso R, Fung TT, Hu FB, Willett W, Camargo CA. Prospective study of dietary patterns and chronic obstructive pulmonary disease among US men. Thorax. 2007;62(9):786–791. | |
McKeever TM, Lewis SA, Cassano PA, et al. Patterns of dietary intake and relation to respiratory disease, forced expiratory volume in 1 s, and decline in 5-y forced expiratory volume. Am J Clin Nutr. 2010;92(2):408–415. | |
Watson L, Margetts B, Howarth P, Dorward M, Thompson R, Little P. The association between diet and chronic obstructive pulmonary disease in subjects selected from general practice. Eur Respir J. 2002;20(2):313–318. | |
Hirayama F, Lee AH, Binns CW, et al. Do vegetables and fruits reduce the risk of chronic obstructive pulmonary disease? A case-control study in Japan. Prev Med. 2009;49(2–3):184–189. | |
Lin YC, Wu TC, Chen PY, Hsieh LY, Yeh SL. Comparison of plasma and intake levels of antioxidant nutrients in patients with chronic obstructive pulmonary disease and healthy people in Taiwan: a case-control study. Asia Pac J Clin Nutr. 2010;19(3):393–401. | |
Celik F, Topcu F. Nutritional risk factors for the development of chronic obstructive pulmonary disease (COPD) in male smokers. Clin Nutr. 2006;25(6):955–961. | |
Varraso R, Jiang R, Barr RG, Willett WC, Camargo CA Jr. Prospective study of cured meats consumption and risk of chronic obstructive pulmonary disease in men. Am J Epidemiol. 2007;166(12):1438–1445. | |
Jiang R, Paik DC, Hankinson JL, Barr RG. Cured meat consumption, lung function, and chronic obstructive pulmonary disease among United States adults. Am J Respir Crit Care Med. 2007;175(8):798–804. | |
Walda IC, Tabak C, Smit HA, et al. Diet and 20-year chronic obstructive pulmonary disease mortality in middle-aged men from three European countries. Eur J Clin Nutr. 2002;56(7):638–643. | |
Tabak C, Feskens EJ, Heederik D, Kromhout D, Menotti A, Blackburn HW. Fruit and fish consumption: a possible explanation for population differences in COPD mortality (the Seven Countries Study). Eur J Clin Nutr. 1998;52(11):819–825. | |
Keranis E, Makris D, Rodopoulou P, et al. Impact of dietary shift to higher-antioxidant foods in COPD: a randomised trial. Eur Respir J. 2010;36(4):774–780. | |
Baldrick FR, Elborn JS, Woodside JV, et al. Effect of fruit and vegetable intake on oxidative stress and inflammation in COPD: a randomised controlled trial. Eur Respir J. 2012;39(6):1377–1384. | |
Lehouck A, Mathieu C, Carremans C, et al. High doses of vitamin D to reduce exacerbations in chronic obstructive pulmonary disease: a randomized trial. Ann Intern Med. 2012;156(2):105–114. | |
Sabino PG, Silva BM, Brunetto AF. Nutritional status is related to fat-free mass, exercise capacity and inspiratory strength in severe chronic obstructive pulmonary disease patients. Clinics (Sao Paulo). 2010;65(6):599–605. | |
Ramachandran K, McCusker C, Connors M, Zuwallack R, Lahiri B. The influence of obesity on pulmonary rehabilitation outcomes in patients with COPD. Chron Respir Dis. 2008;5(4):205–209. | |
Sava F, Laviolette L, Bernard S, Breton MJ, Bourbeau J, Maltais F. The impact of obesity on walking and cycling performance and response to pulmonary rehabilitation in COPD. BMC Pulm Med. 2010;10:55. | |
Greening NJ, Evans RA, Williams JE, Green RH, Singh SJ, Steiner MC. Does body mass index influence the outcomes of a waking-based pulmonary rehabilitation programme in COPD? Chron Respir Dis. 2012;9(2):99–106. | |
van de Bool C, Mattijssen-Verdonschot C, van Melick PP, et al. Quality of dietary intake in relation to body composition in patients with chronic obstructive pulmonary disease eligible for pulmonary rehabilitation. Eur J Clin Nutr. 2014;68(2):159–165. | |
Heart Protection Study Collaborative Group. MRC/BHF heart protection study of antioxidant vitamin supplementation in 20,536 high-risk individuals: a randomised placebo-controlled trial. Lancet. 2002;360(9326):23–33. | |
Paiva SA, Godoy I, Vannucchi H, Favaro RM, Geraldo RR, Campana AO. Assessment of vitamin A status in chronic obstructive pulmonary disease patients and healthy smokers. Am J Clin Nutr. 1996;64(6):928–934. | |
[No authors listed]. The effect of vitamin E and beta carotene on the incidence of lung cancer and other cancers in male smokers. The Alpha-Tocopherol, Beta Carotene Cancer Prevention Study Group. N Engl J Med. 1994;330(15):1029–1035. | |
Rautalahti M, Virtamo J, Haukka J, et al. The effect of alpha-tocopherol and beta-carotene supplementation on COPD symptoms. Am J Respir Crit Care Med. 1997;156(5):1447–1452. | |
Puhan MA, Siebeling L, Frei A, Zoller M, Bischoff-Ferrari H, Ter Riet G. No association of 25-hydroxyvitamin D with exacerbations in primary care patients with COPD. Chest. 2014;145(1):37–43. | |
Romieu I, Meneses F, Ramirez M, et al. Antioxidant supplementation and respiratory functions among workers exposed to high levels of ozone. Am J Respir Crit Care Med. 1998;158(1):226–232. | |
Lange NE, Sparrow D, Vokonas P, Litonjua AA. Vitamin D deficiency, smoking, and lung function in the Normative Aging Study. Am J Respir Crit Care Med. 2012;186(7):616–621. | |
Grievink L, Zijlstra AG, Ke X, Brunekreef B. Double-blind intervention trial on modulation of ozone effects on pulmonary function by antioxidant supplements. Am J Epidemiol. 1999;149(4):306–314. | |
McEvoy C, Hollister-Smith J, Schilling D, et al. Vitamin C improves pulmonary function in newborns of pregnant smoking women: a randomized trial and interaction with maternal nicotinic receptor polymorphisms. Pediatric Academic Society. 2012; abstract. | |
Hole DJ, Watt GC, Davey-Smith G, Hart CL, Gillis CR, Hawthorne VM. Impaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population study. BMJ. 1996;313(7059):711–715; discussion 715–716. | |
Thomason MJ, Strachan DP. Which spirometric indices best predict subsequent death from chronic obstructive pulmonary disease? Thorax. 2000;55(9):785–788. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.