Back to Journals » Cancer Management and Research » Volume 18

Inflammatory, Immune-Metabolic, and Vascular Biomarker Trajectories Across Treatment Modalities and Associations with Treatment-Related Complications in Oral Squamous Cell Carcinoma: A Prospective Study in Taiwan
Authors Chou YF, Huang CH, Chen PR, You SJ
Received 27 January 2026
Accepted for publication 30 April 2026
Published 8 July 2026 Volume 2026:18 599334
DOI https://doi.org/10.2147/CMAR.S599334
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Javier-David Benitez-Fuentes
Yu-Fu Chou,1,2 Chun-Hou Huang,3 Peir-Rong Chen,1,2 Shu-Jheng You4
1Department of Otolaryngology, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan; 2School of Medicine, College of Medicine, Tzu Chi University, Hualien, Taiwan; 3School of Nursing, Tzu Chi University, Hualien, Taiwan; 4Department of Nursing, Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Hualien, Taiwan
Correspondence: Chun-Hou Huang, School of Nursing, Tzu Chi University, No. 701, Sec. 3, Zhongyang Road, Hualien, 970374, Taiwan, Email [email protected]
Background: Oral squamous cell carcinoma (OSCC) is a substantial cancer burden in Taiwan, and multimodality treatment is associated with heterogeneous toxicities. Longitudinal inflammatory, immune-metabolic, and vascular biomarker changes across treatment intensities, and their links with complications, remain insufficiently defined.
Purpose: To characterize biomarker trajectories across OSCC treatment modalities and identify baseline biomarkers associated with treatment-related complications.
Methods: This prospective cohort study included patients with OSCC receiving surgery alone, surgery followed by concurrent chemoradiotherapy (CCRT), or CCRT followed by tegafur–uracil (UFUR) maintenance. Peripheral blood indices and vascular measures, including arterial stiffness index (ASI) and brachial–ankle pulse wave velocity (baPWV), were assessed at baseline and weeks 2, 12, and 24 after surgery. Temporal changes were analyzed using generalized estimating equations, and baseline biomarker associations with complications were examined using multivariable logistic regression.
Results: Among 140 patients, 60 received surgery alone, 40 received CCRT, and 40 received CCRT followed by UFUR maintenance. Patients receiving CCRT showed sustained inflammatory activation, with neutrophil-to-lymphocyte ratio (NLR) peaking at week 12 (β = 4.90, p < 0.001). ASI and baPWV also increased in the CCRT groups at week 12. Elevated baseline NLR (≥ 3.5) was independently associated with postoperative infection (odds ratio [OR] = 1.52, p = 0.026), whereas low prognostic nutritional index (PNI < 40.5) was associated with major complications (OR = 2.85, p = 0.028). Among patients receiving CCRT, low hemoglobin (< 11 g/dL) was associated with febrile neutropenia (OR = 7.10, p = 0.003), while elevated systemic immune-inflammation index (SII ≥ 1100) and uric acid (≥ 5.3 mg/dL) were associated with severe mucositis.
Conclusion: Blood-based and vascular biomarkers showed treatment-specific trajectories and were associated with clinically relevant complications. These exploratory findings may support risk-adapted toxicity monitoring in OSCC, although the proposed cutoffs require external validation.
Keywords: neutrophil-to-lymphocyte ratio, prognostic nutritional index, arterial stiffness, concurrent chemoradiotherapy, treatment-related toxicity
Introduction
Oral squamous cell carcinoma (OSCC) represents a significant global health burden, with particularly high incidence and mortality rates in Asian populations.1 Taiwan exhibits the highest age-standardized incidence among South and Southeast Asian countries.2 While surgical resection remains the cornerstone of treatment, adjuvant cisplatin-based concurrent chemoradiotherapy (CCRT) is indicated for patients with high-risk pathological features.3,4 In Taiwan, approximately 65% of patients present with advanced-stage disease requiring multimodality treatment.5 Recent evidence suggests that one-year maintenance therapy with tegafur–uracil (UFUR; 100 mg tegafur and 224 mg uracil per capsule) following adjuvant chemoradiotherapy may improve survival outcomes in Asian patients with advanced OSCC.6 Because UFUR prolongs systemic 5-fluorouracil exposure, extended treatment may also raise concerns regarding cumulative toxicity.
Treatment-related morbidity is substantial. Surgical complications occur in 20%–50% of cases,7 and clinically significant acute and late toxicities are observed after CCRT.8,9 The clinical challenge is further compounded in populations with high betel quid consumption, such as in Taiwan, where approximately 85% of OSCC cases are associated with betel quid.10 Chronic betel quid exposure induces systemic inflammation, oxidative stress, and endothelial dysfunction,11 potentially amplifying treatment-related inflammatory and vascular injury.12
Peripheral blood-based biomarkers offer accessible means for risk stratification and treatment monitoring. Among blood-derived indices, the neutrophil-to-lymphocyte ratio (NLR), systemic immune–inflammation index (SII), and prognostic nutritional index (PNI) reflect inflammatory, immune, nutritional, and metabolic status, supporting their use as immune-metabolic biomarkers in OSCC. These indices have been associated with treatment tolerance, postoperative complications, and survival outcomes in OSCC.8,13 Hemoglobin further reflects nutritional reserve and oxygen-carrying capacity, and low pretreatment levels have been consistently associated with poor prognosis in OSCC.14,15 Serum uric acid (UA), the terminal product of purine catabolism, may serve as a metabolic marker linking systemic inflammation with adverse outcomes, including distant metastasis in head and neck cancers16 and mortality among patients with cancer who develop chemotherapy-induced febrile neutropenia.17
Vascular function assessment complements these blood-based inflammatory and immune-metabolic markers and directly evaluates cardiovascular risk. Pulse wave velocity (PWV), a validated measure of arterial stiffness, has demonstrated value in cancer populations. Meta-analytic evidence indicates that anticancer therapies significantly increase arterial stiffness,18 and PWV measurements are consistently elevated in patients with cancer relative to age-matched controls.19
Despite the prognostic relevance of individual biomarkers, systematic longitudinal data on inflammatory, immune-metabolic, and vascular responses across multimodality OSCC therapy remain limited. How treatment intensity, from surgery alone to CCRT followed by UFUR maintenance, modulates these biomarkers during acute and extended phases is unclear. Additionally, while anticancer therapies increase arterial stiffness across malignancies, OSCC-specific evidence is limited. This exploratory study aimed to delineate the temporal patterns of these biomarkers across distinct treatment modalities, examine their associations with treatment-related complications, and provide an initial framework for risk-adapted toxicity monitoring in OSCC.
Materials and Methods
Study Design and Participants
Patients with newly diagnosed, pathologically confirmed OSCC at an academic medical center in eastern Taiwan between March 2024 and November 2025 were enrolled in this prospective longitudinal cohort study. Eligible participants were aged ≥ 40 years, had no history of coronary artery bypass surgery, and were able to provide informed consent. Exclusion criteria comprised distant metastasis, previous or concurrent malignancy, second primary tumor, uncontrolled comorbidities, or active infection. The study protocol was approved by the Institutional Review Board of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (IRB Number 112-261-B), and written informed consent was obtained from all participants.
Patients were stratified into three treatment groups based on the intended treatment intensity determined by the multidisciplinary tumor board prior to surgery, considering pathological risk factors and performance status. This classification reflected clinical judgment regarding disease aggressiveness and anticipated treatment needs. The surgery group underwent surgery alone. The CCRT group received surgery followed by CCRT comprising radiotherapy of 60–66 Gy to the primary tumor bed and 54–60 Gy to at-risk nodal regions, with weekly cisplatin at 25–40 mg/m2 based on renal function, performance status, and treatment tolerance as determined by the treating physician. The CCRT with UFUR group received surgery and CCRT as described, followed by initiation of maintenance therapy with oral UFUR at 300–400 mg daily based on body surface area, with planned duration of one year. Although the CCRT and CCRT with UFUR groups received identical treatment during weeks 0–12, the three-group framework was retained to examine whether baseline characteristics associated with planned maintenance therapy influenced biomarker trajectories. All adjuvant treatments commenced within six weeks after surgery. Perioperative antibiotic prophylaxis was administered according to institutional protocol; however, prophylactic antibiotics were not routinely prescribed for treatment-related neutropenia during adjuvant therapy.
Study Procedure
Patients were evaluated at four time points: baseline (T0, before surgery), and 2 (T1), 12 (T2), and 24 (T3) weeks after surgery. The T3 visit corresponded to about 3 months after the start of UFUR maintenance therapy in the CCRT with UFUR group. At each visit, inflammatory and immune-metabolic biomarkers were obtained from routine blood tests, and arterial stiffness parameters, including arterial stiffness index (ASI) and brachial–ankle pulse wave velocity (baPWV), were measured concurrently. Although the CCRT and CCRT with UFUR groups received identical treatment during weeks 0–12, they were pre-specified as separate groups by the multidisciplinary tumor board based on distinct baseline risk profiles, and the T3 assessment was designed to capture the initial three months of UFUR exposure, enabling exploratory detection of early maintenance-related biomarker trajectories.
The primary endpoints were longitudinal trajectories of inflammatory, immune-metabolic, and vascular biomarkers. Secondary analyses explored baseline predictors of postoperative complications, infections, and CCRT-related toxicities with grade ≥ 3. All patients were followed for at least six months.
Sample size was estimated using the lmmPower function of the longpower package (R version 4.3.0), assuming a medium effect size (Cohen’s d = 0.5), four repeated measures, and 80% statistical power. The minimum required number of participants was 96. Considering an anticipated attrition rate of about 32% based on prior study,8 142 participants were targeted. This sample size was considered adequate to capture temporal trends in biomarker changes and to maintain sufficient statistical precision for exploratory subgroup analyses. The allocation ratio of 1.5:1:1 reflected the higher prevalence of early-stage OSCC cases undergoing surgery alone in routine clinical practice.
Variables and Instruments
Baseline Demographics and Clinical Characteristics
Baseline data, including age at diagnosis, gender, lifestyle factors, tumor characteristics, and pathological features, were extracted from electronic medical records. The Charlson Comorbidity Index (CCI) was used to quantify comorbidity burden.20 Nutritional and metabolic parameters assessed within 1–3 days before surgery included body mass index and lipid profile.
Inflammatory and Immune-Metabolic Biomarkers
Serial laboratory data were collected from complete blood count with differential and serum biochemistry panels at all four assessment time points. Albumin, hemoglobin, white blood cell, platelet, and differential leukocyte counts were recorded at each visit. Derived biomarkers were calculated using standard formulas as previously described:13 the neutrophil-to-lymphocyte ratio (NLR) was calculated as the ratio of the absolute neutrophil to lymphocyte counts; the prognostic nutritional index (PNI) was computed as the serum albumin concentration (g/L) plus five times the lymphocyte count (×109/L); and the systemic immune-inflammation index (SII) was defined as the product of the platelet count and the NLR. Serum uric acid was measured from fasting blood samples and analyzed concurrently with other biochemical parameters.
Arterial Stiffness Assessment
Arterial stiffness was measured noninvasively using an oscillometric device (Cardio Vision MS-2000; Osachi, Nagano, Japan). All measurements were performed with patients in the supine position after a 10-minute rest. Systolic, diastolic, and pulse pressures were recorded from the right brachial artery, and the device automatically calculated the ASI from oscillometric waveform analysis. baPWV was measured simultaneously by applying cuffs to both upper arms and ankles. Two consecutive 3-minute recordings were obtained, and the mean value was used for analysis. This oscillometric method correlates strongly with carotid–femoral PWV, the gold standard for central arterial stiffness assessment, and the ASI has been validated as a reliable surrogate marker for atherosclerotic vascular alterations.21
Treatment-Related Adverse Events
Postoperative complications were systematically evaluated using standardized criteria. Systemic complications were graded according to the Clavien–Dindo classification,22 and grade ≥ III was considered major. Postoperative infections were included only when microbiologically confirmed by positive bacterial cultures. Recurrent infections at the same anatomical site were regarded as independent events if separated by at least 14 days and accompanied by documented negative interim cultures. Arterial and venous thromboembolic events were prospectively monitored for 6 months postoperatively.
Acute toxicities during CCRT were assessed weekly using the Common Terminology Criteria for Adverse Events (version 5.0),23 and grade ≥ 3 was defined as severe. Nutritional status was monitored by hospital dietitians who provided individualized dietary counseling. Nasogastric tube feeding was initiated in patients with oral intake < 50% of baseline or with grade ≥ 3 dysphagia refractory to supportive measures for > 48 hours.
Data Analysis
All statistical analyses were performed using SPSS version 28.0 (IBM Corp., Armonk, NY, USA). Continuous variables were expressed as means ± standard deviations and categorical variables as frequencies and percentages. Baseline group differences were assessed using one-way ANOVA or the Kruskal–Wallis test for continuous variables and the chi-square or Fisher’s exact test for categorical variables, as appropriate.
Longitudinal changes in hemoglobin, NLR, SII, PNI, uric acid, ASI, and baPWV were evaluated at baseline and at 2, 12, and 24 weeks after surgery using generalized estimating equation (GEE) models with an exchangeable correlation structure. Interaction terms between treatment group and time were included to assess differential biomarker trajectories. To account for baseline disease severity, clinical stage (III–IV vs. I–II) was included as a covariate in all GEE models.
Binary logistic regression was used to examine factors associated with major postoperative complications, postoperative infections, and grade ≥3 CCRT-related toxicities. Because this was an exploratory study, ROC-derived cutoffs were applied to enhance clinical interpretability rather than to develop a definitive prediction model; thus, all cutoffs should be considered hypothesis-generating and require external validation. Variables significant in univariate analyses (p < 0.05) were further evaluated by ROC analysis using the Youden index, except for hemoglobin, for which a clinically established threshold (11 g/dL) was applied. Significant predictors were subsequently entered into multivariable models. All tests were two-tailed, with p < 0.05 considered statistically significant.
Results
Baseline Characteristics
A total of 198 potentially eligible patients with oral cavity cancer were assessed for eligibility, of whom 160 provided informed consent and were enrolled in this study. Overall, 140 patients completed all follow-up assessments, yielding a retention rate of 87.5%. The attrition rates were 2.5% (T0 to T1), 5.1% (T1 to T2), and 5.4% (T2 to T3). Details of participant recruitment and study flow are presented in Figure 1. Baseline demographic and clinical characteristics are summarized in Table 1.
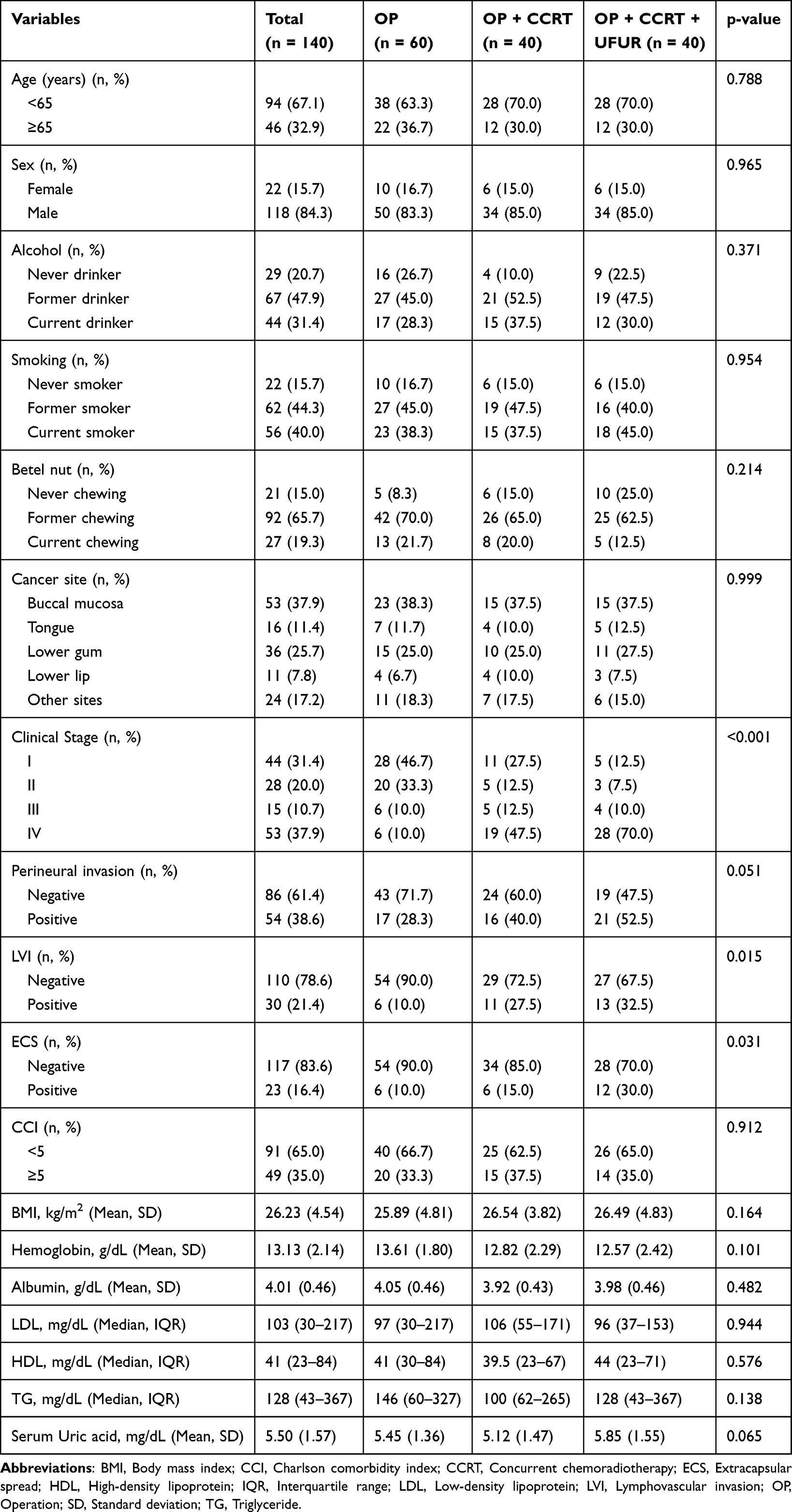 |
Table 1 Patient Characteristics |
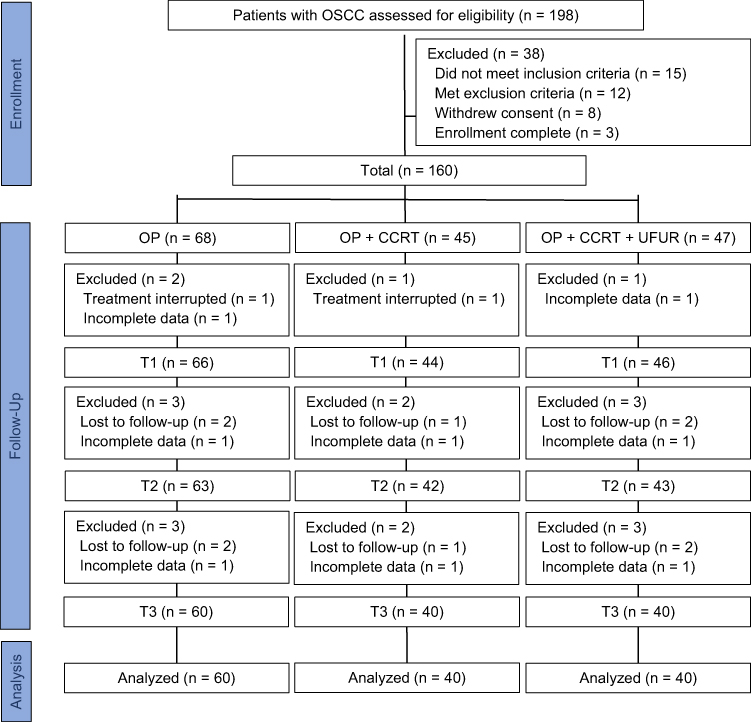 |
Figure 1 Participant Enrollment, Follow-Up, and Analysis Flow. Abbreviations: CCRT, Concurrent chemoradiotherapy; OP, Operation; OSCC, Oral squamous cell carcinoma; T1, 2 weeks post-surgery; T2, 12 weeks post-surgery; T3, 24 weeks post-surgery. |
The mean age of the cohort was 59.5 ± 9.5 years, and males accounted for 84.3% (118/140). The most common primary tumor sites were the buccal mucosa (37.9%), lower gum (25.7%), and tongue (11.4%). Clinical stage distribution differed significantly among treatment groups (p < 0.001), and stage IV disease was observed in 10.0% of the surgery group, 47.5% of the CCRT group, and 70.0% of the CCRT with UFUR group. Pathologic features also varied significantly among groups. Lymphovascular invasion (p = 0.015) and extracapsular spread (p = 0.031) were more frequent in the CCRT with UFUR group. Age, gender, comorbidity burden, and baseline nutritional and metabolic parameters, including body mass index, serum albumin, hemoglobin, lipid profile, and UA, were comparable across the three treatment groups.
Longitudinal Changes in Inflammatory, Immune-Metabolic, and Vascular Biomarkers
In the GEE model (Table 2 and Supplementary Table S1), hemoglobin levels decreased at week 2 across all treatment arms (β = −0.60, 95% CI = −0.95 to −0.25, p < 0.001). At week 12, the surgery group maintained stable hemoglobin levels, whereas both CCRT groups exhibited significant treatment-by-time interactions (CCRT: β = −1.95, 95% CI = −2.64 to −1.26, p < 0.001; CCRT with UFUR: β = −1.85, 95% CI = −2.57 to −1.13, p < 0.001). By week 24, hemoglobin concentrations in all groups approximated baseline values. NLR elevations were observed in both CCRT groups at week 2 (CCRT: β = 1.20, 95% CI = 0.12 to 2.28, p = 0.029; CCRT with UFUR: β = 1.35, 95% CI = 0.21 to 2.49, p = 0.020), with peak values at week 12 (CCRT: β = 4.90, 95% CI = 2.31 to 7.49, p < 0.001; CCRT with UFUR: β = 4.85, 95% CI = 2.14 to 7.56, p < 0.001). SII followed a similar temporal pattern and demonstrated significant treatment-by-time interactions at week 12 (CCRT: β = 890.0, 95% CI = 149.4 to 1630.6, p = 0.019; CCRT with UFUR: β = 980.0, 95% CI = 213.6 to 1746.4, p = 0.012). Both inflammatory markers returned toward baseline by week 24, while the surgery group showed only transient early postoperative changes.
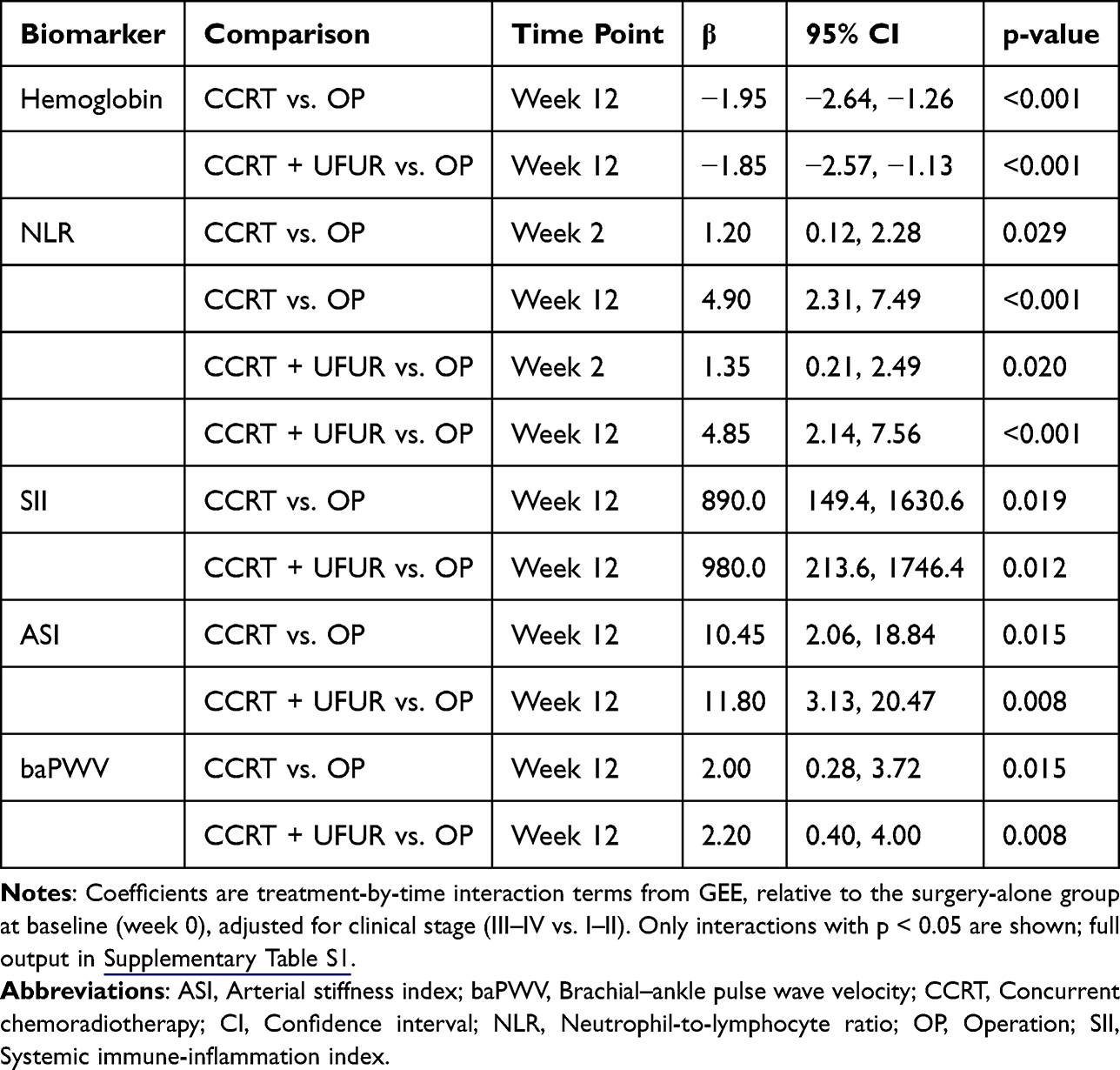 |
Table 2 Generalized Estimating Equation Analysis of Temporal Trends in Inflammatory, Immune-Metabolic, and Vascular Markers |
PNI declined at weeks 2 and 12 (β = −2.15, 95% CI = −3.03 to −1.27, p < 0.001; β = −4.30, 95% CI = −5.47 to −3.13, p < 0.001, respectively) and recovered by week 24 (β = −0.80, 95% CI = −1.90 to 0.30, p = 0.154), and no significant treatment-by-time interactions were detected. Vascular indices showed similar CCRT-related temporal patterns.
ASI showed significant treatment-by-time interactions at week 12 in both CCRT groups (CCRT: β = 10.45, 95% CI = 2.06 to 18.84, p = 0.015; CCRT with UFUR: β = 11.80, 95% CI = 3.13 to 20.47, p = 0.008), as did baPWV (CCRT: β = 2.00, 95% CI = 0.28 to 3.72, p = 0.015; CCRT with UFUR: β = 2.20, 95% CI = 0.40 to 4.00, p = 0.008). The surgery group maintained stable vascular parameters throughout the study period. Because both CCRT groups received identical CCRT during weeks 0–12, their broadly parallel biomarker trajectories during this period were not interpreted as UFUR-specific effects.
Treatment-Related Major Adverse Events and Infections
As summarized in Supplementary Table S2, major postoperative complications were observed across treatment groups, with increasing incidence according to treatment intensity. Postoperative infections, reoperations, and Clavien–Dindo grade ≥ III complications occurred in 20.0%–30.0%, 11.7%–27.5%, and 18.3%–32.5% of patients, respectively.
Among the 80 patients who received CCRT with or without UFUR, the most common grade ≥ 3 acute toxicities were mucositis (62.5%–70.0%), followed by dysphagia (25.0%–30.0%), leukopenia (17.5%–20.0%), anemia (15.0%), and febrile neutropenia (12.5%–15.0%). No thromboembolic events were recorded during the six-month follow-up period.
Predictors of Severe and Infection-Related Treatment Toxicities
Univariate and multivariable analyses of postoperative complications are presented in Table 3. Continuous variables showing significant univariate associations were dichotomized using ROC-derived optimal cutoffs based on the Youden index (Supplementary Table S3 and Supplementary Figure S1). After adjustment for significant univariate predictors, multivariable analysis identified advanced stage (OR = 4.27, 95% CI = 1.37 to 13.37, p = 0.012) and NLR ≥ 3.5 (OR = 1.52, 95% CI = 1.08 to 2.20, p = 0.026) as independent predictors of postoperative infections. For major systemic complications (Clavien–Dindo ≥ III), independent predictors included hemoglobin < 11 g/dL (OR = 3.29, 95% CI = 1.03 to 10.47, p = 0.044) and PNI < 40.5 (OR = 2.85, 95% CI = 1.12 to 7.25, p = 0.028), whereas PNI < 41.4 was also the sole independent predictor of reoperation (OR = 3.20, 95% CI = 1.25 to 8.18, p = 0.015).
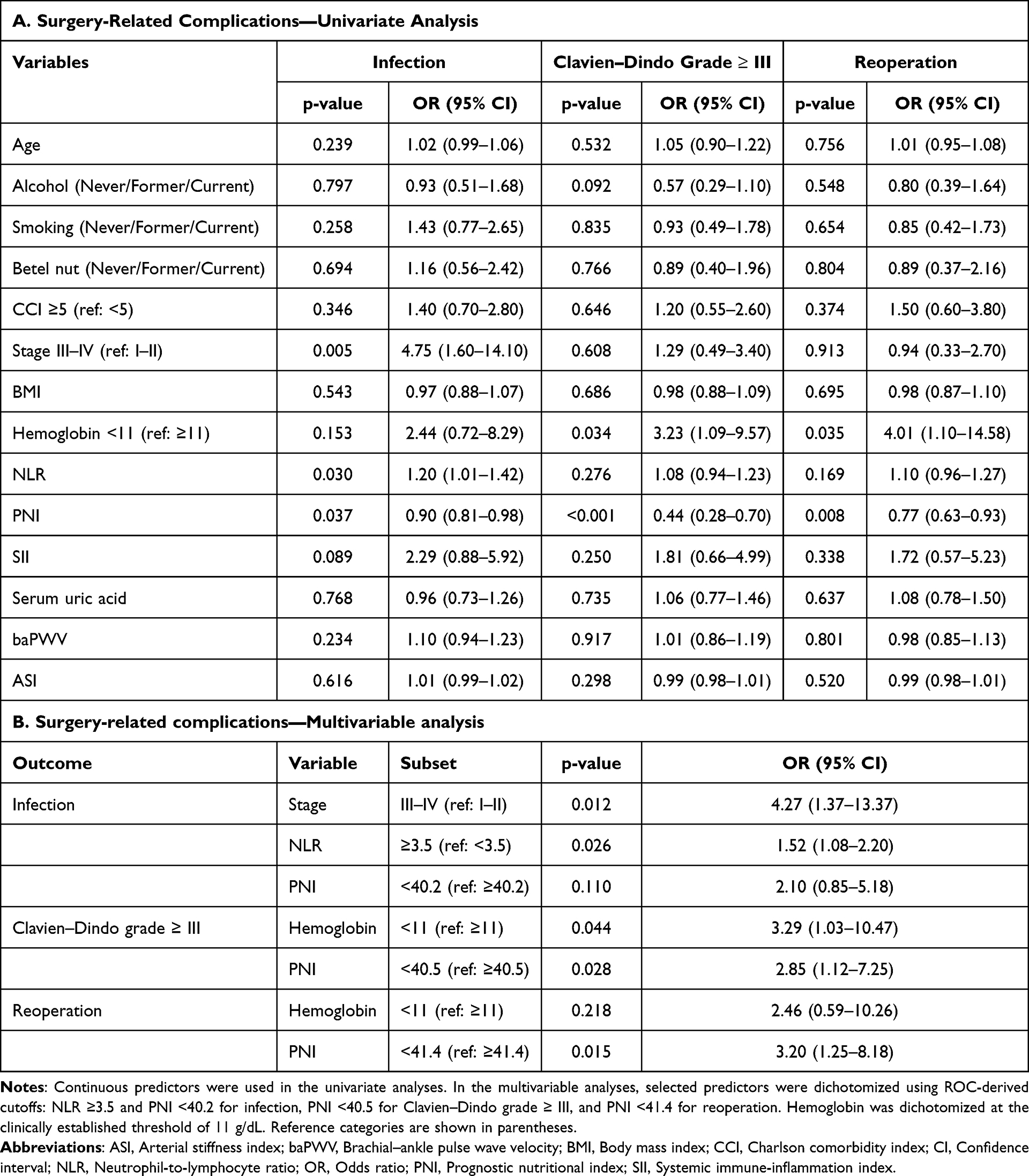 |
Table 3 Logistic Regression Analysis of Clinical Variables Associated with Surgery-Related Complications |
Among patients receiving CCRT (Table 4), multivariable analysis identified that febrile neutropenia was independently associated with hemoglobin < 11 g/dL (OR = 7.10, 95% CI = 1.90 to 26.50, p = 0.003), NLR ≥ 3.1 (OR = 1.56, 95% CI = 1.04 to 2.26, p = 0.024), and elevated UA ≥ 5.5 mg/dL (OR = 1.67, 95% CI = 1.06 to 2.65, p = 0.028). Severe mucositis was associated with advanced stage (OR = 8.50, 95% CI = 2.45 to 29.50, p = 0.001), high SII ≥ 1100 (OR = 3.45, 95% CI = 1.17 to 10.21, p = 0.025), and elevated UA ≥ 5.3 mg/dL (OR = 1.90, 95% CI = 1.14 to 3.15, p = 0.014). Severe dysphagia was associated with advanced stage (OR = 7.20, 95% CI = 2.50 to 20.80, p < 0.001) and hemoglobin < 11 g/dL (OR = 5.85, 95% CI = 1.90 to 18.00, p = 0.002).
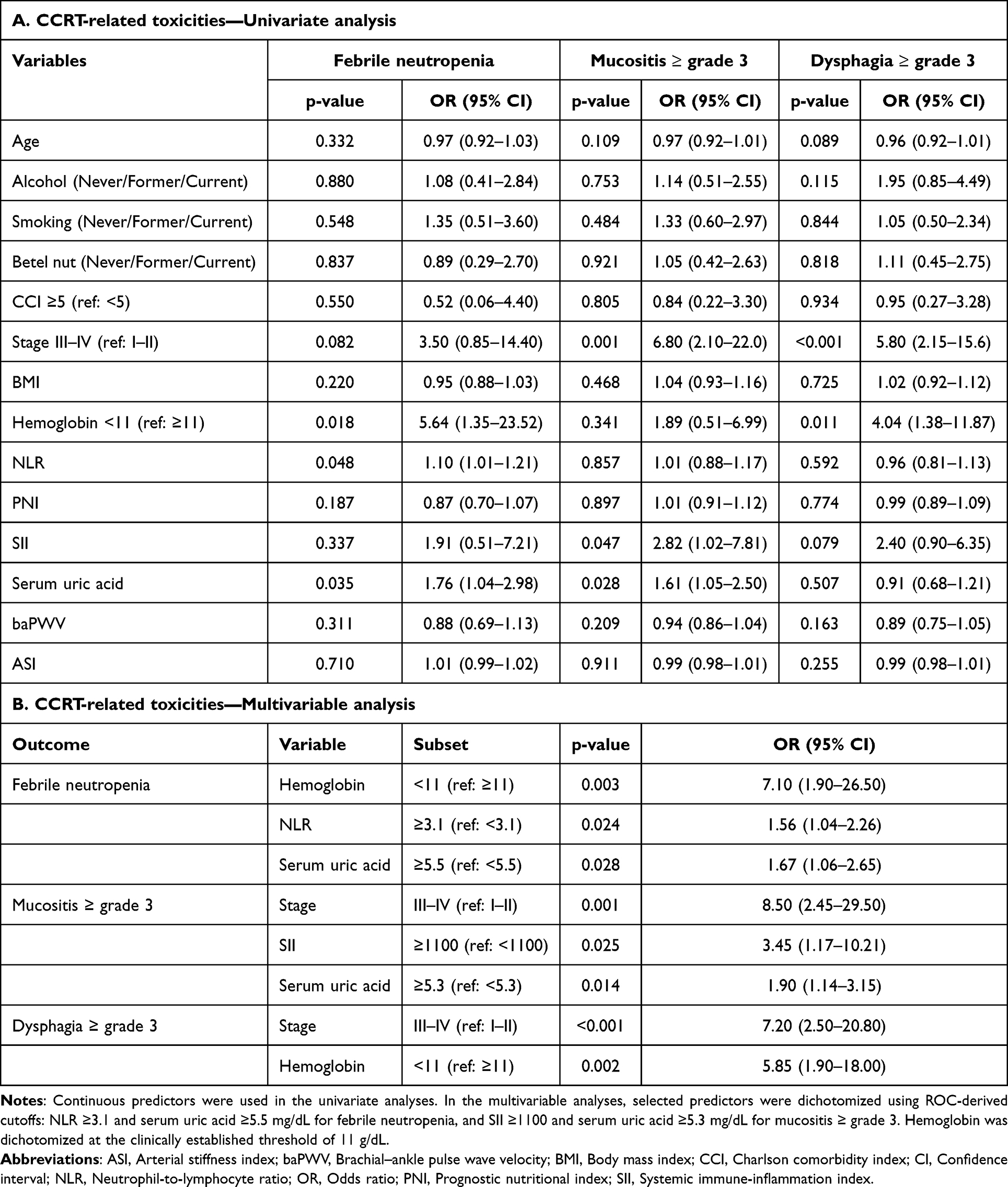 |
Table 4 Logistic Regression Analysis of Clinical Variables Associated with Chemoradiotherapy-Related Toxicities |
Discussion
This prospective longitudinal study evaluated temporal changes in inflammatory, immune-metabolic, and vascular biomarkers across escalating treatment intensities in OSCC: surgery alone, surgery with CCRT, or surgery with CCRT and UFUR maintenance. Serial assessments at baseline and weeks 2, 12, and 24 revealed intensity-dependent response patterns. Because the two CCRT groups received identical treatment during weeks 0–12, early trajectory differences should be interpreted as reflecting baseline risk stratification and planned treatment intensity rather than a direct UFUR effect. CCRT induced sustained elevations in NLR and SII, transient declines in PNI and hemoglobin at weeks 2–12, and temporary increases in ASI and baPWV at week 12 that returned toward baseline by week 24, whereas surgery alone caused only transient perturbations. Advanced stage, elevated NLR, and low PNI were independent predictors of postoperative complications, whereas elevated NLR, low hemoglobin, elevated SII and UA were associated with an increased risk of CCRT-related toxicities. Collectively, these findings provide an integrated framework for risk stratification across treatment intensities in OSCC.
In the present study, patients receiving postoperative CCRT exhibited sustained elevations of NLR and SII during the 24-week period that peaked at week 12, whereas the surgery-only group showed minimal fluctuations resolving by week 12. These inflammatory dynamics are consistent with cross-malignancy findings, including reports of NLR elevations during chemoradiotherapy in nasopharyngeal cancer by Muangwong et al24 and in cervical cancer by Hyder et al.25 Notably, chronic betel quid exposure, prevalent in eastern Taiwan, may contribute to baseline inflammatory burden in OSCC patients. Arecoline, the principal alkaloid, activates NF-κB and NLRP3 inflammasome pathways while promoting oxidative stress,26 potentially amplifying treatment-induced systemic inflammation.27
While NLR reflects neutrophil-driven inflammation and lymphocyte-mediated immunity, SII additionally incorporates platelets and captures the thromboinflammatory component of treatment response. In our cohort, SII demonstrated parallel elevation patterns, consistent with findings in esophageal28 and lung cancers,29 including the PROCLAIM trial,30 which indicates that SII elevation represents a general systemic reaction to multimodality treatment. These differing trajectories between surgery-alone and CCRT cohorts reflect distinct immune activation kinetics. Surgical inflammation is transient and resolves within 2–4 weeks as wound healing progresses.31 By contrast, platinum-based chemotherapy induces sustained oxidative stress and DNA damage and drives persistent IL-6 and TNF-α release.32 Concurrent radiotherapy amplifies these effects through immunogenic cell death and cytokine release (IL-6, IL-8, and TNF-α) leading to neutrophilia, lymphopenia, and platelet activation33,34 and is collectively reflected in the concurrent NLR and SII elevations observed during CCRT.
Systemic inflammatory and metabolic biomarkers provide prognostic insights, yet longitudinal characterization remains limited, which hinders cross-study comparability.35 Most studies rely on pretreatment values to predict treatment-related toxicities.36–39 Therefore, the present study used pretreatment values to explore ROC-derived cutoffs that may help characterize patients at higher risk of treatment-related complications. These thresholds should be interpreted as hypothesis-generating rather than definitive prediction tools. The NLR and PNI thresholds align with previous reports,36,38 while the higher SII cutoff likely reflects OSCC-specific heterogeneity, which emphasizes the importance of population-tailored thresholds.40
Elevated pretreatment NLR was associated with postoperative infections and febrile neutropenia during chemoradiotherapy, suggesting that an impaired neutrophil-lymphocyte balance may reflect compromised immune defense across treatment modalities. Beyond OSCC, NLR has emerged as a practical tool for infection risk assessment in immunocompromised settings, including transplantation and major surgery, where dynamic monitoring alongside other inflammatory indices may refine risk stratification. This prognostic role is further supported by the McGill cohort of 456 patients with HNC, in which low NLR was associated with better treatment tolerance.8 By contrast, elevated SII predicted severe oral mucositis and likely reflected synergistic neutrophil–platelet activation that amplified mucosal inflammation. This outcome is supported by evidence linking elevated IL-1β, IL-6, TNF-α, and IFN-γ to mucositis severity.40,41
PNI declined across groups without significant treatment-by-time interactions, whereas hemoglobin showed additional week-12 declines in both CCRT cohorts. The clinical relevance of PNI has been reported in head and neck and lung cancers,39,42 and the present trajectory suggests that postoperative immune-metabolic deterioration may partly reflect surgical stress, cancer-related catabolism, and nutritional vulnerability rather than CCRT-specific toxicity alone.43,44 Low pretreatment hemoglobin independently predicted febrile neutropenia, major complications, and dysphagia, consistent with prior evidence linking anemia to poor outcomes in OSCC.15 Anemia may aggravate tissue hypoxia and impair healing, while its coexistence with malnutrition further increases feeding-tube dependence and delays recovery.45,46 These findings underscore the importance of perioperative nutritional and hematologic optimization to enhance treatment tolerance in OSCC.
Pretreatment UA was associated with CCRT-related toxicities, including febrile neutropenia and severe mucositis, but not with surgical complications. This treatment-specific pattern is broadly consistent with the dual biological role of UA described in the literature. At physiological concentrations, UA acts as an antioxidant, whereas elevated levels have been shown to activate NADPH oxidase and the NLRP3 inflammasome, promoting reactive oxygen species generation and IL-1β release.47,48 Elevated UA has also been linked to poorer cancer survival in a meta-analysis of 43 cohorts,49 to chemotherapy-induced febrile neutropenia,17 and to adverse oncologic outcomes in head and neck cancers.16 Although the underlying mechanisms were not directly examined in this study, it is plausible that chemoradiotherapy amplifies pre-existing oxidative and inflammatory stress, whereas surgery elicits a more localized and transient response.50,51 Elevated baseline UA may therefore represent a metabolic risk signal more relevant to CCRT-related toxicity than to surgical complications. These findings should be regarded as hypothesis-generating and warrant further mechanistic and interventional investigation.
ASI reflects oscillometric waveform-derived peripheral stiffness, whereas baPWV captures central-to-peripheral pulse propagation; their parallel elevation supports generalized endothelial stress during CCRT. ASI and baPWV increased significantly at week 12, and baPWV rose by 2.0–2.2 m/s, consistent with a meta-analysis reporting an average increase of 2.05 m/s within 2–4 months of antitumor therapy.18 Both indices returned to baseline by week 24, indicating transient vascular alterations likely reflecting radiation- and platinum-related endothelial stress. Although UFUR maintenance therapy has been associated with improved survival after chemoradiotherapy in locally advanced head and neck squamous cell carcinoma,52 the limited 3-month UFUR exposure in the present cohort was likely insufficient to determine maintenance-specific vascular or inflammatory effects. Endothelial dysfunction is a key pathway linking vascular injury with atherosclerotic risk,53 and therapeutic radiation has been associated with cardiovascular manifestations, including vascular injury.54
Baseline arterial stiffness markers showed no association with postoperative or CCRT-related complications, consistent with their role as indicators of long-term cardiovascular risk. Head and neck radiotherapy has been associated with an increased risk of cardiovascular disease,55 while arterial stiffness has been recognized as a subclinical marker of cardiovascular risk in cancer populations.18,19 Vallée et al further demonstrated the added predictive value of ASI for cardiovascular risk stratification.56 Fluoropyrimidine-related cardiovascular toxicity is commonly discussed in relation to coronary vasospasm and endothelial injury rather than as a well-established cause of persistent arterial stiffening,57,58 and the observation window likely captured neither sustained vascular remodeling nor maintenance-specific immune shifts. These findings support ongoing vascular monitoring in patients receiving high-intensity CCRT and highlight the need for studies evaluating prolonged UFUR exposure and cardioprotective strategies.
This study has several limitations. First, the single-center design may limit generalizability, and betel quid exposure was not quantified, precluding dose-response analyses. Second, although the sample size was adequate for longitudinal biomarker assessment, statistical power for multivariable complication modeling was limited. In addition, all patients received standard-dose radiotherapy according to institutional protocols, but detailed patient-level dose-volume parameters were not analyzed; therefore, the potential contribution of radiation dose distribution to systemic inflammation, mucosal toxicity, or arterial stiffening could not be evaluated. Third, the CCRT and CCRT with UFUR groups received identical treatment during weeks 0–12, and the limited UFUR exposure may have been insufficient to detect maintenance-specific biomarker changes; however, the three-group framework was retained to reflect real-world treatment stratification and explore whether patients selected for maintenance therapy exhibited distinct trajectory characteristics. Fourth, pretreatment DPYD genotyping was not performed because the DPYD variants routinely screened in European populations occur at very low frequencies in East Asian populations, and no validated genotyping strategy has yet been established for this population.59 Accordingly, clinical toxicity monitoring and timely dose adjustment served as the principal safeguards against severe fluoropyrimidine toxicity. Finally, ROC-derived cutoffs showed relatively low specificity and require validation in independent cohorts. Despite these limitations, this prospective study with high retention (87.5%) provides novel longitudinal data on inflammatory, immune-metabolic, and vascular dynamics across treatment intensities in OSCC, offering a framework for biomarker-based risk stratification and supportive care optimization. These findings highlight the feasibility of integrating longitudinal biomarker monitoring into postoperative follow-up to anticipate complications and guide supportive interventions.
Conclusion
This prospective study demonstrated that patients with OSCC exhibited distinct inflammatory, immune-metabolic, and vascular responses across treatment intensities. CCRT induced sustained systemic alterations, whereas surgery alone caused transient changes. Pretreatment UA was associated with chemoradiotherapy-related toxicities, and transient arterial stiffening during CCRT at week 12, captured non-invasively by ASI and baPWV, supports incorporating vascular assessment into on-treatment surveillance.
Readily available blood-based biomarkers may help identify patients at higher risk of postoperative infection, major complications, febrile neutropenia, and severe mucositis, supporting more tailored surveillance and proactive toxicity management.
Ethics Approval
The study protocol was reviewed and approved by the Research Ethics Committee of Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation (IRB Number 112-261-B). Written informed consent was obtained from all participants prior to enrollment.
Funding
This work was financially supported by Hualien Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, under Grant Number TCRD113-053.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–15. doi:10.3322/caac.21660
2. Filho AM, Warnakulasuriya S. Epidemiology of oral cancer in South and South-East Asia: incidence and mortality. Oral Dis. 2024;30(8):4847–4854. doi:10.1111/odi.14906
3. Pfister DG, Ang KK, Brizel DM, et al. Head and neck cancers. J Natl Compr Canc Netw. 2011;9(6):596–650. doi:10.6004/jnccn.2011.0053
4. Lin CY, Fan KH, Lee LY, et al. Precision adjuvant therapy based on detailed pathologic risk factors for resected oral cavity squamous cell carcinoma: long-term outcome comparison of CGMH and NCCN guidelines. Int J Radiat Oncol Biol Phys. 2020;106(5):916–925. doi:10.1016/j.ijrobp.2019.08.058
5. Tsai WC, Kung PT, Wang ST, Huang KH, Liu SA. Beneficial impact of multidisciplinary team management on the survival in different stages of oral cavity cancer patients: results of a nationwide cohort study in Taiwan. Oral Oncol. 2015;51(2):105–111. doi:10.1016/j.oraloncology.2014.11.006
6. Lee HL, Chen PH, Huang TC, et al. Tegafur-uracil maintenance therapy in non-metastatic head and neck cancer: an exploratory systematic review. Curr Oncol. 2025;32(5):286. doi:10.3390/curroncol32050286
7. Wang Y, Wang M, Tang Y, Sun B, Wang K, Zhu F. Perioperative mortality of head and neck cancers. BMC Cancer. 2021;21(1):256. doi:10.1186/s12885-021-07998-z
8. Chowdhury R, Botros K, Richardson K, et al. Pretreatment Neutrophil-to-Lymphocyte Ratio (NLR) predicts treatment toxicity and intolerance in operable head and neck cancer: an ambispective cohort study. Head Neck. 2025;47(11):2950–2955. doi:10.1002/hed.28212
9. Cooper JS, Pajak TF, Forastiere AA, et al. Postoperative concurrent radiotherapy and chemotherapy for high-risk squamous-cell carcinoma of the head and neck. N Engl J Med. 2004;350(19):1937–1944. doi:10.1056/NEJMoa032646
10. Itaki R, Taufa S. Association between habitual betel quid chewing and risk of adverse cardiovascular outcomes: a systematic review. Trop Med Int Health. 2024;29(6):447–453. doi:10.1111/tmi.13988
11. Rangani SC, Marapana RAUJ, Senanayake GSA, Perera PRD, Pathmalal MM, Amarasinghe HK. Alkaloids and nitrosamines in betel quid: a biochemical exploration of carcinogenicity. Chem Biol Interact. 2025;407:111383. doi:10.1016/j.cbi.2025.111383
12. Zarifa A, Albittar A, Kim PY, et al. Cardiac toxicities of anticancer treatments: chemotherapy, targeted therapy and immunotherapy. Curr Opin Cardiol. 2019;34(4):441–450. doi:10.1097/HCO.0000000000000641
13. Kubota K, Ito R, Narita N, et al. Utility of prognostic nutritional index and systemic immune-inflammation index in oral cancer treatment. BMC Cancer. 2022;22(1):368. doi:10.1186/s12885-022-09439-x
14. Valero C, Zanoni DK, Pillai A, et al. Host factors independently associated with prognosis in patients with oral cavity cancer. JAMA Otolaryngol Head Neck Surg. 2020;146(8):699–707. doi:10.1001/jamaoto.2020.1019
15. Ito Y, Abe A, Hayashi H. Impact of preoperative haemoglobin, albumin, lymphocyte, and platelet score on oral cancer prognosis. Oral Dis. 2024;30(8):4855–4866. doi:10.1111/odi.14950
16. Lee S, Li X, Kim JH, Wu HG, Eom KY, Lee JH . Prognostic value of uric acid in predicting metastasis following definitive radiotherapy in patients with head and neck cancer. In Vivo. 2025;39(4):2464–2473. doi:10.21873/invivo.14047
17. Sütcüoğlu O, Akdoğan O, İnci BK, Gürler F, Özdemir N, Yazıcı O. Effect of serum uric acid level and Multinational Association for Supportive Care in Cancer risk score on febrile neutropenia mortality. Support Care Cancer. 2021;29(2):1047–1053. doi:10.1007/s00520-020-05587-7
18. Parr SK, Liang J, Schadler KL, Gilchrist SC, Steele CC, Ade CJ. Anticancer therapy-related increases in arterial stiffness: a systematic review and meta-analysis. J Am Heart Assoc. 2020;9(14):e015598. doi:10.1161/JAHA.119.015598
19. Diao Y, Liu Z, Chen L, Zhang W, Sun D. The relationship between cancer and functional and structural markers of subclinical atherosclerosis: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:849538. doi:10.3389/fcvm.2022.849538
20. Deyo RA, Cherkin DC, Ciol MA. Adapting a clinical comorbidity index for use with ICD-9-CM administrative databases. J Clin Epidemiol. 1992;45(6):613–619. doi:10.1016/0895-4356(92)90133-8
21. Del Giorno R, Troiani C, Gabutti S, Stefanelli K, Gabutti L. Comparing oscillometric and tonometric methods to assess pulse wave velocity: a population-based study. Ann Med. 2021;53(1):1–16. doi:10.1080/07853890.2020.1794538
22. Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004;240(2):205–213. doi:10.1097/01.sla.0000133083.54934.ae
23. National Cancer Institute. Common Terminology Criteria for Adverse Events (CTCAE) version 5.0. Available from: https://ctep.cancer.gov/protocoldevelopment/electronic_applications/ctc.htm.
24. Muangwong P, Homkham N, Narueban W, et al. Longitudinal measurements of neutrophil-to-lymphocyte ratio in nasopharyngeal cancer treated with concurrent chemoradiotherapy. PLoS One. 2023;18(10):e0292591. doi:10.1371/journal.pone.0292591
25. Hyder J, Jang H, Kim S, et al. Prognostic value of changes in neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and lymphocyte-to-monocyte ratio (LMR) for patients with cervical cancer undergoing definitive chemoradiotherapy (dCRT). Int J Radiat Oncol Biol Phys. 2019;105(1):E663–E664. doi:10.1016/j.ijrobp.2019.06.1061
26. Faouzi M, Neupane RP, Yang J, Williams P, Penner R. Areca nut extracts mobilize calcium and release pro-inflammatory cytokines from various immune cells. Sci Rep. 2018;8(1):1075. doi:10.1038/s41598-017-18996-2
27. Lee CH, Chang JS, Syu SH, et al. IL-1β promotes malignant transformation and tumor aggressiveness in oral cancer. J Cell Physiol. 2015;230(4):875–884. doi:10.1002/jcp.24816
28. Geng Y, Shao Y, Zhu D, et al. Systemic immune-inflammation index predicts prognosis of patients with esophageal squamous cell carcinoma: a propensity score-matched analysis. Sci Rep. 2016;6:39482. doi:10.1038/srep39482
29. Wang Q, Tan X, Deng G, Fu S, Li J, Li Z. Dynamic changes in the systemic immune-inflammation index predict the prognosis of EGFR-mutant lung adenocarcinoma patients receiving brain metastasis radiotherapy. BMC Pulm Med. 2022;22(1):75. doi:10.1186/s12890-022-01866-7
30. Biswas T, Kang K, Bajor D, et al. Using the systemic inflammation index (SII) as a mid-treatment marker for overall survival among patients undergoing chemo-radiation therapy for stage-III locally advanced non-small cell lung cancer (NSCLC): secondary analysis of PROCLAIM trial. Int J Radiat Oncol Biol Phys. 2020;108(3):S103–S104. doi:10.1016/j.ijrobp.2020.07.2283
31. Alazawi W, Pirmadjid N, Lahiri R, Bhattacharya S. Inflammatory and immune responses to surgery and their clinical impact. Ann Surg. 2016;264(1):73–80. doi:10.1097/SLA.0000000000001691
32. Zhang Y, Ding C, Zhu W, et al. Chemotherapeutic drugs induce oxidative stress associated with DNA repair and metabolism modulation. Life Sci. 2022;289:120242. doi:10.1016/j.lfs.2021.120242
33. McLaughlin M, Patin EC, Pedersen M, et al. Inflammatory microenvironment remodelling by tumor cells after radiotherapy. Nat Rev Cancer. 2020;20(4):203–217. doi:10.1038/s41568-020-0246-1
34. Yamaga S, Aziz M, Murao A, Brenner M, Wang P. DAMPs and radiation injury. Front Immunol. 2024;15:1353990. doi:10.3389/fimmu.2024.1353990
35. Xiang X, Li N, Ding Z, Jin J. Peripheral lymphocyte counts and lymphocyte-related inflammation indicators during radiotherapy for pelvic malignancies: temporal characterization and dosimetric predictors. Technol Cancer Res Treat. 2022;21:15330338221116494. doi:10.1177/15330338221116494
36. Islam MM, Satici MO, Eroglu SE. Unraveling the clinical significance and prognostic value of the neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, systemic immune-inflammation index, systemic inflammation response index, and delta neutrophil index: an extensive literature review. Turk J Emerg Med. 2024;24(1):8–19. doi:10.4103/tjem.tjem_198_23
37. Reyes-Chicuellar N, Kagan R, Friedland P. Prognostic impact of neutrophil-lymphocyte ratio in head and neck cancer: a decade of evidence. Aust J Otolaryngol. 2025;8:13. doi:10.21037/ajo-24-52
38. Zhang J, Dai S. Prognostic and clinicopathological role of pretreatment systemic immune-inflammation index in patients with oral squamous cell carcinoma: a meta-analysis. Front Oncol. 2024;13:1303132. doi:10.3389/fonc.2023.1303132
39. Uri I, Horváth A, Tamás L, Polony G, Dános K. Prognostic nutritional index (PNI) correlates with survival in head and neck cancer patients more precisely than other nutritional markers - real world data. Eur Arch Otorhinolaryngol. 2024;281(12):6599–6611. doi:10.1007/s00405-024-08865-w
40. Takenaka Y, Oya R, Takemoto N, Inohara H. Neutrophil-to-lymphocyte ratio as a prognostic marker for head and neck squamous cell carcinoma treated with immune checkpoint inhibitors: meta-analysis. Head Neck. 2022;44(5):1237–1245. doi:10.1002/hed.26997
41. Song J, Wen Y, Liang L, et al. Prediction of severe radiation-induced oral mucositis in locally advanced nasopharyngeal carcinoma using the combined systemic immune-inflammatory index and prognostic nutritional index. Eur Arch Otorhinolaryngol. 2024;281(5):2627–2635. doi:10.1007/s00405-024-08536-w
42. Okada S, Shimada J, Kato D, Tsunezuka H, Teramukai S, Inoue M. Clinical significance of prognostic nutritional index after surgical treatment in lung cancer. Ann Thorac Surg. 2017;104(1):296–302. doi:10.1016/j.athoracsur.2017.01.085
43. Martinovic D, Tokic D, Puizina Mladinic E, et al. Nutritional management of patients with head and neck cancer-a comprehensive review. Nutrients. 2023;15(8):1864. doi:10.3390/nu15081864
44. Matsuda Y, Okui T, Tatsumi H, et al. Oral dysfunction in patients with oral cancer could occur before treatment and require early nutritional improvement: a cross-sectional study. Dysphagia. 2023;38(4):1096–1105. doi:10.1007/s00455-022-10531-4
45. Chiu YH, Tseng WH, Ko JY, Wang TG. Radiation-induced swallowing dysfunction in patients with head and neck cancer: a literature review. J Formos Med Assoc. 2022;121(1 Pt 1):3–13. doi:10.1016/j.jfma.2021.06.020
46. List MA, Knackstedt M, Liu L, et al. Enhanced recovery after surgery, current, and future considerations in head and neck cancer. Laryngoscope Investig Otolaryngol. 2023;8(5):1240–1256. doi:10.1002/lio2.1126
47. Joosten LAB, Crişan TO, Bjornstad P, Johnson RJ. Asymptomatic hyperuricaemia: a silent activator of the innate immune system. Nat Rev Rheumatol. 2020;16(2):75–86. doi:10.1038/s41584-019-0334-3
48. Braga TT, Forni MF, Correa-Costa M, et al. Soluble uric acid activates the NLRP3 inflammasome. Sci Rep. 2017;7:39884. doi:10.1038/srep39884
49. Liu X, Chen H, Wang S, Lei Y. Correlation of serum uric acid with cancer: a systematic evaluation and dose-response meta-analysis of 43 cohort studies. Int J Surg. 2025;111(12):9656–9668. doi:10.1097/JS9.0000000000003150
50. Kampman SL, Smalbroek BP, Dijksman LM, Smits AB. Postoperative inflammatory response in colorectal cancer surgery: a meta-analysis. Int J Colorectal Dis. 2023;38(1):233. doi:10.1007/s00384-023-04525-3
51. Sonis ST. A hypothesis for the pathogenesis of radiation-induced oral mucositis: when biological challenges exceed physiologic protective mechanisms. Implications for pharmacological prevention and treatment. Support Care Cancer. 2021;29(9):4939–4947. doi:10.1007/s00520-021-06108-w
52. Hsieh JC, Lien MY, Chang PH, et al. UFUR maintenance therapy significantly improves survival in locally advanced head and neck squamous cell carcinoma following definitive chemoradiotherapy. Cancer Cell Int. 2025;25(1):187. doi:10.1186/s12935-025-03807-w
53. Siasos G, Sara JD, Zaromytidou M, et al. Local low shear stress and endothelial dysfunction in patients with nonobstructive coronary atherosclerosis. J Am Coll Cardiol. 2018;71(19):2092–2102. doi:10.1016/j.jacc.2018.02.073
54. Mitchell JD, Cehic DA, Morgia M, et al. Cardiovascular manifestations from therapeutic radiation: a multidisciplinary expert consensus statement from the international cardio-oncology society. JACC CardioOncol. 2021;3(3):360–380. doi:10.1016/j.jaccao.2021.06.003
55. Lin PY, Cheng PC, Hsu WL, et al. Risk of CVD following radiotherapy for head and neck cancer: an updated systematic review and meta-analysis. Front Oncol. 2022;12:820808. doi:10.3389/fonc.2022.820808
56. Vallée A. Added value of arterial stiffness index for the 10-year atherosclerotic cardiovascular disease risk determination in a middle-aged population-based study. Clin Res Cardiol. 2023;112(11):1679–1689. doi:10.1007/s00392-023-02267-4
57. Lyon AR, López-Fernández T, Couch LS, et al. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022;43(41):4229–4361. doi:10.1093/eurheartj/ehac244
58. Jensen SA, Sørensen JB. 5-fluorouracil-based therapy induces endovascular injury having potential significance to development of clinically overt cardiotoxicity. Cancer Chemother Pharmacol. 2012;69(1):57–64. doi:10.1007/s00280-011-1669-x
59. Kanai M, Kawaguchi T, Kotaka M, et al. Poor association between dihydropyrimidine dehydrogenase (DPYD) genotype and fluoropyrimidine-induced toxicity in an Asian population. Cancer Med. 2023;12(7):7808–7814. doi:10.1002/cam4.5541
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Influence of Characteristics and Indexes (NLR, PNI, and SII) Evaluated at Admission on the Mortality Prediction of Infectious Endocarditis Patients
Sezen AI, Ozdemir YE, Borcak D, Goklu BN, Bilgin Z, Turkyilmaz G, Caglar FNT, Gedik H, Kart Yasar K
International Journal of General Medicine 2025, 18:5617-5627
Published Date: 18 September 2025