")
Back to Journals » Infection and Drug Resistance » Volume 16
Infection Prevalence at a Tertiary Hospital in Hail, Saudi Arabia: A Single-Center Study to Identify Strategies to Improve Antibiotic Usage
Authors Alanazi M, Alqahtani HM, Alshammari MK, Alshammari RM, Malik JA, Ahmed S, Aroosa M, Shinde M, Alharby TN, Ansari M , Hussain A , Alkhrshawy FF, Anwar S
Received 11 April 2023
Accepted for publication 2 June 2023
Published 13 June 2023 Volume 2023:16 Pages 3719—3728
DOI https://doi.org/10.2147/IDR.S413295
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Muteb Alanazi,1 Hassan Mohammed Alqahtani,1 Mohammad Khalid Alshammari,1 Raad Mohammed Alshammari,1 Jonaid Ahmad Malik,2,3 Sakeel Ahmed,4 Mir Aroosa,5 Mrunal Shinde,6 Tareq Nafea Alharby,1 Mukhtar Ansari,1 Arshad Hussain,1 Fahad F Alkhrshawy,7 Sirajudheen Anwar8
1Department of Clinical Pharmacy, College of Pharmacy, University of Hail, Hail, Saudi Arabia; 2Department of Pharmacology and Toxicology, National Institute of Pharmaceutical Education and Research, Guwahati, India; 3Department of Biomedical Engineering, Indian Institute of Technology Ropar, Rupnagar, India; 4Department of Pharmacology and Toxicology, National Institute of Pharmaceutical Education and Research, Ahmedabad, India; 5Department of Pharmacology and Toxicology, Jamia Hamdard, New Delhi, India; 6Department of Pharmaceutical Analysis, National Institute of Pharmaceutical Education and Research, Guwahati, India; 7Pharmaceutical Care Department, Hail General Hospital - Hail Health Cluster, Hail, Saudi Arabia; 8Department of Pharmacology and Toxicology, College of Pharmacy, University of Hail, Hail, Saudi Arabia
Correspondence: Sirajudheen Anwar, Email [email protected]
Objective: Identifying the burden of disease and the condition of the Saudi population is in high demand from both a surveillance and analytical standpoint. The objective of this study was to determine the most prevalent infections among hospitalized patients (both community-acquired and hospital-acquired), the antibiotics prescribing pattern, and their relationship with patient characteristics like age and gender.
Methods: A retrospective study was conducted comprising 2646 patients with infectious diseases or complications admitted to a tertiary hospital in the Hail region of Saudi Arabia. A standardized form was used to collect information from patient’s medical records. Demographic data such as age, gender, prescribed antibiotics, and culture-sensitivity tests were included in the study.
Results: Males represented about two-thirds (66.5%, n = 1760) of the patients. Most patients (45.9%) who suffered from infectious diseases were between the ages of 20 and 39. The most prevalent infectious ailment was respiratory tract infection (17.65%, n = 467). Furthermore, the most common multiple infectious diseases were gallbladder calculi with cholecystitis (40.3%, n = 69). Similarly, COVID-19 had the greatest impact on people over 60. Beta-lactam antibiotics were the most commonly prescribed (37.6%), followed by fluoroquinolones (26.26%) and macrolides (13.45%). But performing culture sensitivity tests were rather uncommon (3.8%, n = 101). For multiple infections, beta-lactam antibiotics (such as amoxicillin and cefuroxime) were the most commonly prescribed antibiotics (2.26%, n = 60), followed by macrolides (such as azithromycin and Clindamycin) and fluoroquinolones (eg, ciprofloxacin and levofloxacin).
Conclusion: Respiratory tract infections are the most prevalent infectious disease among hospital patients, who are primarily in their 20s. The frequency of performing culture tests is low. Therefore, it is important to promote culture sensitivity testing in order to support the prudent use of antibiotics. Guidelines for anti-microbial stewardship programs are also highly recommended.
Keywords: antibiotics, infections, prescribing pattern, Hail region, Saudi Arabia
Introduction
Infectious diseases remain a prominent source of mortality and morbidity worldwide, amounting to nearly 8 million fatalities in 2016.1 Infectious diseases are the second highest cause of fatality and disability-adjusted life years globally.2 According to WHO estimates, there are 300–500 million instances of malaria, 333 million cases of sexually transmitted diseases (syphilis, gonorrhea, and chlamydia), 33 million infections of HIV/AIDS, 14 million people suffering from tuberculosis, and 3–5 million people infected with cholera.3 Even though infectious diseases are more prevalent in the non-industrialized sector, infection in industrialized nations is still relatively high for specific infectious diseases. In the United States, roughly 48 million episodes of diarrhea result in 128,000 hospitalizations and 3000 fatalities related to diarrheal infections each year.4 Not unexpectedly, there is a significant disparity in infectious illness death rates between non-industrialized and industrialized countries. Infectious diseases are responsible for one out of every three deaths worldwide. In 1990, approximately 17 million people died from infectious diseases, malnutrition, and maternal and perinatal ailments, with the poor accounting for nearly all of these deaths.3
A study was conducted in a tertiary hospital based in Germany (2015–2020) on infections regarding the genomic analysis of carbapenem-resistant P. aeruginosa specimens. The study concluded that ST111 VIM-2 P. aeruginosa was the main carbapenemase-producing strain that spread in the hospitals.5 In Thailand, a study revealed that two N. gonorrhoeae isolates in heterosexual subjects had reduced susceptibility to ceftriaxone. The study isolated around 134 isolates of N. gonorrhoeae, and they found that two isolates NG-083 and NG-091 were not susceptible to ceftriaxone. Molecular docking revealed that they had occupied the penicillin-binding sites.6 Similar studies have been conducted in the United Kingdom, Netherlands, and the United States of America, revealed by molecular epidemiology data.6 Infections by Klebsiella pneumoniae that causes catheter-related biofilm infections in hospitals have been critical. A study suggested that colistin and EDTA had reduced the biofilm formation of Klebsiella pneumoniae (colistin-resistant) by the combination of colistin and EDTA. This combination can reduce the eradication of infections in hospitals7 In Iran, the prevalence of infections by C. hominis transmission occurs in hospital subjects via anthroponotic transmission.8 Due to a lack of effective antibiotics against resistant Acinetobacter baumannii, a new combination of colistin plus sulbactam has demonstrated a synergistic effect against Acinetobacter baumannii-resistant strains than sulbactam which is an excellent strategy to curb the deadly infections9 A study conducted in Germany on the Blood-stream Infection Due to Multi-Drug Resistant Organisms on Risk Factors and Clinical Outcomes (BLOOMY) concluded that BLOOMY scores demonstrated and good discrimination and the predictive values and could support the progress of procedures to manage infections in blood-stream and help to estimate the short- and long-term infection burdens in blood-stream.10 A study was conducted in Brazil on the clonal spread of infections by ArmA and OXA-23-co-producing Acinetobacter baumannii. The study found that the rapid spread of the carbapenem-resistant Acinetobacter baumannii clone was majorly responsible for the large outbreak in a hospital in Brazil. It is suggested that prospective and continuous vigilance is warranted to estimate the influence of this clone on hospitals.11
The intensity and duration of infections are determined by several parameters, such as the pathogenicity of the invading organism’s strain and the individual’s resilience, which may be weakened by starvation or concurrent sickness.12 A few major contributors to this issue are environmental modifications caused by human activities, greater worldwide movement, inadequate community healthcare systems, and microbial adaptability.13 The background of infectious disease medicine is littered with remarkable achievements. The successful identification, diagnosis, and therapeutic approaches of infectious diseases have altered society’s fabric, resulting in significant social, economic, and political benefits.
There is immense demand from both surveillance and analytical method point of view for documenting the influence of disease and conditions on the Saudi population.14–16 So a comprehensive effort needs to quantify the global population’s health so that it can tell us suitable methods to compare different places, regions, and periods.17 It is reported that the global burden of diseases (GBD) in Saudi Arabia from 1990 to 2017 decreased the age-associated death rate because of improved health facilities.17 However, infections, substance use disorders, neoplasms, and neurological disorders continue to rise from 1990 to 2017. Respiratory infections and tuberculosis have hiked annually because of poor management in the clinical settings in Saudi Arabia.17
The objective of this study was to determine the most prevalent infections among hospitalized patients (both community-acquired and hospital-acquired), the antibiotics prescribing pattern, and their relationship with patient characteristics like age and gender. The outcomes of the present research can help to better understand the single-center epidemiology of illnesses, guide infection control strategies, and enhance surveillance and public health practices.
Methods
Study Design
This study is cross-sectional and retrospective in nature. The study was accomplished from March 2021 to November 2021 in a tertiary care hospital in Hail, Saudi Arabia. Two thousand six hundred and forty-six medical records of hospitalized patients were examined for infectious diseases, and administered medications, and microbial culture sensitivity test reports.
Data Collection
Data collectors approached the General Directorate of Health Affairs, Hail region, and the hospital administrator to seek permission before collecting the data. A standardized form was used to gather data from patient medical records for those who were admitted to the hospital between March 2021 and November 2021 due to infectious diseases or complications. The information included demographic data such as age, gender, medication prescribed, and culture-sensitivity test reports. The information and details acquired were treated with confidentiality. There was no personal information utilized in this study. This was a secondary examination of anonymized data from routine monitoring.
Sample Analysis
Biological sample analysis (Blood, Urine, Throat swabs, Stool sample, Spinal tap) was formerly performed in accordance with internal policy and procedure (IPP) at the Department of Microbiology laboratory, Hail General Hospital, Hail, Saudi Arabia. Final recorded results from the medical file were taken for our study’s purpose.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and the Institutional Review Board (IRB), approved the study, General Directorate of Health Affairs, Hail region (Protocol number H-08-L-074). The details and information gathered are kept confidential. The ethics committee approved our study stating no need for consent from participants since it is a retrospective data analysis.
Statistical Analysis
The data were analyzed using GraphPad Prism 9.0. Descriptive statistics were used where needed, such as variable frequencies, mean, standard deviation, and cross-tabulations. The data were analyzed statistically using the chi-square test measuring the association between the most frequent infection with gender and the trend of performing culture sensitivity tests. A P <0.05 was considered significant throughout the analyses.
Results
About two-thirds (66.5%, n = 1760) of the patients were represented by males and the remaining (33.5%, n = 886) were females. The majority (45.9%) of the patients were 20 to 39 years old, followed by 40 years and above (33.8%). The patients’ median age (interquartile range) was 32 (21.5 to 46.5) years. The analysis by age group reveals that patients from the age of 20 years to 39 years suffered the most from infectious diseases. Furthermore, the patients aged 20 years to 29 years had a higher fraction of infection (eg, respiratory tract infections and gastroenteritis along with colitis); whereas UTI, calculus of gall bladder, renal colic, and cholecystitis were more prevalent in patients with the age group of 30 years to 39 years. Similarly, COVID-19 affected patients above 60 years the most (Table 1).
 |
Table 1 Distribution of the Ten Most Frequent Infectious Diseases Among Hospitalized Patients by Age Group |
Respiratory tract infection (17.65%; n = 467) was found to be the most common infectious ailment for which patients visited the hospital followed by renal colic (10.24%; n = 271), gastroenteritis and colitis (7.02%; n = 186), and UTI (6.72%; n = 178) Table 2. A chi-square test revealed a significant association between gender and infectious diseases diagnosed in hospitals (p < 0.001). Calculus of gallbladder with cholecystitis was found to be the most frequent multiple infectious diseases diagnosed among hospitalized patients in the top ten list with a percentage of 40.3% (n = 69) followed by gastroenteritis and colitis of infectious origin with 25.7% (n = 44). The remaining represented 29.01% (n = 50) Table 3.
 |
Table 2 The Ten Most Frequent Infectious Diseases Diagnosed Among Hospitalized Patients and Their Association with Gender |
 |
Table 3 The Ten Most Frequent Multiple Infectious Diseases Diagnosed Among the Hospitalized Patients |
The trend of performing culture sensitivity tests was found quite uncommon (3.8%, n = 101). However, acute cholecystitis due to gallbladder calculus and COVID-19 got a bit more attention compared to other diseases in executing the culture sensitivity tests (Table 4). There was a significant relationship between the infectious diseases diagnosed and the trend of performing culture sensitivity tests (p < 0.001).
 |
Table 4 Relationships Between Infectious Diseases and the Trend of Performing Culture Sensitivity Tests |
Beta-lactam antibiotics were highly prescribed (37.6%), followed by fluoroquinolones (26.26%), macrolides (13.45%), and miscellaneous antibiotics (22.69%) (Table 5). The prescription pattern of most often used antibiotics for more than one infection among hospitalized patients is given below (Table 6). It was found that amoxicillin was the most commonly administered antibiotic across all diagnosed categories, followed by cefuroxime and azithromycin, and all were consistent with the primary diagnosis.
 |
Table 5 The Most Prescribed Antibiotics for Infectious Diseases Among Hospitalized Patients |
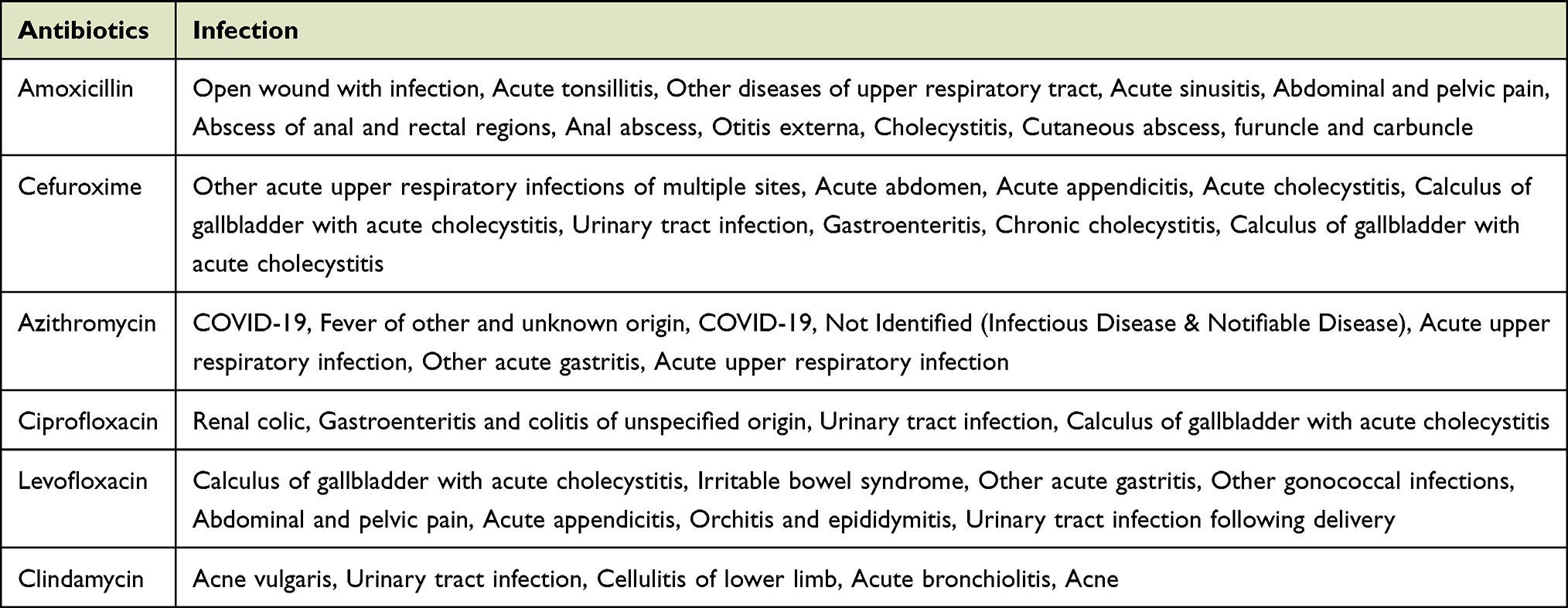 |
Table 6 Antibiotics Prescribed for More Than One Infection Among Hospitalized Patients |
Although the use of an antibiotic in more than one infection among the hospitalized patients was very rare (3.84%, n = 102), beta-lactam antibiotics (eg, amoxicillin and cefuroxime) represented the topmost prescribed antibiotics (2.26%, n = 60) followed by macrolides (eg, azithromycin and clindamycin) and fluoroquinolones (eg, ciprofloxacin and levofloxacin) Figure 1.
 |
Figure 1 Antibiotics prescribed for more than one infection among hospitalized patients. |
Discussion
Infectious diseases continuously emerging, leading to resistance to the available antibiotic therapy.18 As antibiotic resistance increases, understanding the pattern of infection and antibiotic prescription in Hospitals is of utmost importance. Thus, we conducted a retrospective analysis at a tertiary care hospital in Saudi Arabia’s Hail region to investigate infection prevalence and the antibiotics prescribed. Infectious diseases are a growing public health concern worldwide, and managing them rationally is another challenge.19 The COVID-19 era is a witness to how an infectious disease affects the whole world.14,20,21 Even though the conditions are still worse despite the availability of different vaccines.22–24 Antibiotics play a vital role in preventing infectious diseases and thus improving human health.25 However, improper selection of antibiotics or their overuse may play a significant role in the development of antibiotic resistance, which poses a significant threat to infectious disease management. According to national monitoring of Saudia Arabia for Gram positive (+ve) cocci; 32% of S. aureus is MRSA, 33% of S. pneumoniae are penicillin G resistant, and 26% is erythromycin-resistant.26 Additionally, the prevalence of ESBL (extended-spectrum beta-lactamase) in E. coli is growing, with 29% ESBL rates and 65% ESBL rates in K. pneumoniae.27 This necessitates preventing the unnecessary use of antibiotics in the community and hospital settings and encouraging the sensible use of antibiotics10,12. The resistance towards carbapenems by gram-negative bacteria is increasing dramatically. A study on 360 antibacterial prescriptions was estimated, where it was concluded that the appropriateness of prescribing was high after anti-microbial restriction than before using anti-microbial restriction. These findings reveal that an anti-microbial restriction system can increase the appropriateness of prescribing antibiotics.28
The prevalence of infection was the highest in the age group 20–29 and 30–39. The finding is supported by the study conducted by Balkhy et al in Riyadh.29 However, the latter study particularly highlighted the highest vulnerability of hospital-acquired infection (HAI) among patients above 50 years of age. This is due to weaker immunity among old-aged patients29 due to opportunistic infections. Among different infections, respiratory tract infection (17.65%) was found to be the most common infectious ailment for which patients visited the hospital, followed by renal colic (10.24%), gastroenteritis, and colitis (7.02%), and UTI (6.72%). Our data on Renal colic are consistent with the study published by Safdar O.Y et al, 2021 among residents of Saudi Arabia.30 Also, our previous study demonstrated that the major UTIs causing organism is E. coli in Tertiary Hospital in Al-Baha Region, Saudi Arabia.31
In multiple infectious diseases, calculus of the gallbladder with cholecystitis was the most frequent among hospitalized patients with 40.3%, followed by gastroenteritis and colitis of infectious origin with 25.7%. The trend of performing culture sensitivity tests was quite uncommon (3.8%). In executing the culture sensitivity tests, acute cholecystitis related to gallbladder calculus and COVID-19 received more attention than other diseases. In the case of antibiotic prescription, Beta-lactam antibiotics were the most highly prescribed (37.6%), followed by fluoroquinolones (26.26%), macrolides (13.45%), and miscellaneous antibiotics (22.69%). Amoxicillin was the most preferred antibiotic across all diagnosed categories, followed by cefuroxime and azithromycin, and all were consistent with the primary diagnosis. For multiple infections, beta-lactam antibiotics (eg, amoxicillin and cefuroxime) are top on the list (2.26%), followed by macrolides (eg, azithromycin and clindamycin) and fluoroquinolones (eg, ciprofloxacin and levofloxacin).
The infection prevalence was reported in a study conducted in Hail Hospital of Saudi Arabia, where it was observed that pneumonia (27.2%), Urinary tract infections (20.2%), and blood-stream infections (10.5%) were the most common infections. It was also observed that around 19.2% of infections were healthcare-associated infections or hospital-acquired infections (HAI).32 The Gram-negative bacteria collected from UTI patients in Ha’il exhibited strong amikacin sensitivity, which is consistent with findings from a similar study in Al-Jouf,33, and Al Baha region, Saudi Arabia.34 As a result, amikacin is one of the potential choices for usage as a first-line medicine to treat patients with UTIs in the Saudi Arabian provinces of Hail and Al-Jouf, as well as other places with comparable characteristics. Amikacin is also considered as a first line of drug for UTIs.35,36 However, there is a significant danger that amikacin will cause kidney and hearing problems. Our earlier study observed that E. coli is the main etiological agent for UTIs in Al Baha region of Saudi Arabia. The most prescribed antibiotic was ciprofloxacin (20.29%) and cefuroxime (16.14%), followed by ceftriaxone (12.96%) and then tazocin (8.80%). But the most sensitive antibiotics were imipenem, meropenem, amikacin, vancomycin, tigecycline, linezolid, and colistin.34
Our study has observed antibiotic susceptibility patterns and the most common antibiotics prescribed against diverse infections. The study also noticed that amoxicillin was one of the highly prescribed drugs for most infections. It is also the preferred antibiotic for many bacterial infections.37 The other antibiotics preferred as per the guidelines are cefdinir, cefpodoxime, moxifloxacin, levofloxacin, and these antibiotics were also prescribed for many infections, as described above in Table 5.37 Antibiotics like clindamycin, levofloxacin, azithromycin, cefuroxime, and ciprofloxacin were the most common antibiotics prescribed to in-hospital patients. Amoxicillin was one of the most highly prescribed antibiotics for hospital inpatients.
However, respiratory tract infections were common among the 20–29 age group, with the highest prevalence of azithromycin/amoxicillin as prescribed antibiotics. Our results are consistent with the study by Iven et al, 2018. It is observed that one in five adults suffered from respiratory tract infection in primary care in 11 European countries.38 Further, there is a need to conduct multicentric studies at different locations in Saudi Arabia to get more information on the prevalence of infectious diseases and antibiotic prescribing behavior in other geographical regions in Saudi Arabia.
The main issue with anti-microbial resistance is increased death rate, morbidity, and cost.39 Antibiotic resistance can be decreased by following the guidelines of ASPs (anti-microbial stewardship programs) and several other things like pharmacodynamic and pharmacokinetic parameters of the antibiotics, AST (anti-microbial susceptibility testing), clinical response, alteration of microbiota, new antibiotics, and diagnostic testing. The regulated usage of antibiotics in foods might also reduce resistance. There should be awareness programs for children and healthcare professionals regarding antibiotic resistance and bacterial infections. Everyone needs to come forward and ensure all members of society are concerned and responsible for taking measures against antibiotic resistance.40 The most important thing is to control and prevent the dissemination of resistant strains.39
Conclusion
Respiratory tract infection was the most common infectious condition for which patients went to the hospital, especially among those in their 20s. The use of beta-lactam antibiotics is still the top choice of prescribers. The trend of performing culture sensitivity tests is uncommon in the hospital except for acute cholecystitis owing to gallbladder calculus and COVID-19. However, in order to promote sensible antibiotic use, culture sensitivity testing should be encouraged in hospitals. Among the recommendations are instructing residents how to properly classify antibiotic prescriptions, reducing the use of prescriptions with a double anaerobic cover, and reviving the custom of sending culture reports. Guidelines for surgery prophylactic treatment can be improved by limiting the use of some broad-spectrum antibiotics for the same conditions and limiting the duration of surgical prophylaxis to one day.
Recommendations
- ASPs should be followed to enhance clinical outcomes, optimize anti-microbial therapy, and decrease cost and toxicity.
- The prescribers should have thorough knowledge regarding the antibiotics while prescribing.
- To control and prevent the dissemination of resistant strains.
- To conduct awareness programs for children and healthcare professionals regarding antibiotic resistance and bacterial infections.
- To maintain hygiene to reduce the occurrence of infections.
- To develop novel antibiotics.
- To reduce the use of antibiotics in agriculture.
Data Sharing Statement
Available on request from the corresponding author. The data are not publicly available to maintain privacy and adhere to the guidelines of the ethics protocol.
Ethical Approval
The study was conducted in accordance with the Declaration of Helsinki and the Institutional Review Board (IRB), approved the study, General Directorate of Health Affairs, Hail region (Protocol number H-08-L-074). The details and information gathered are kept confidential. The ethics committee approved our study stating no need for consent from participants since it is a retrospective data analysis.
Acknowledgments
Authors extend their appreciation to the project fund from the Research Deanship in the University of Ha’il – Saudi Arabia through project number BA-23 004.
Funding
This research has been funded by Scientific Research Deanship at the University of Ha’il, Saudi Arabia, through project number BA-23 004.
Disclosure
The authors declare no conflict of interest.
References
1. Alghamdi A, Alamoudi O, Ghabrah T, Al-Kassimi M. Pattern of infectious diseases in the western region of Saudi Arabia; a study of 495 hospitalized patients. J King Abdulaziz Univ Med Sci. 2009;16(2):3–15. doi:10.4197/Med.16-2.1
2. Blas E, Sommerfeld J. Editorial. Int J Health Plann Manage. 2004;19(S1):S1–S2. doi:10.1002/HPM.780
3. Straif-Bourgeois S, Ratard R, Kretzschmar M. Infectious Disease Epidemiology. Handbook Epidemiol. 2014;2041. doi:10.1007/978-0-387-09834-0_34
4. Mounts AW, Holman RC, Clarke MJ, Bresee JS, Glass RI. Trends in hospitalizations associated with gastroenteritis among adults in the United States, 1979-1995. Epidemiol Infect. 1999;123(1):1–8. doi:10.1017/s0950268899002587
5. Wendel AF, Malecki M, Mattner F, et al. Genomic-based transmission analysis of carbapenem-resistant pseudomonas aeruginosa at a tertiary care centre in cologne (Germany) from 2015 to 2020. JAC Antimicrob Resist. 2022;4(3). doi:10.1093/JACAMR/DLAC057
6. Kueakulpattana N, Wannigama DL, Luk-in S, et al. Multidrug-Resistant Neisseria gonorrhoeae infection in heterosexual men with reduced susceptibility to ceftriaxone, first report in Thailand. Sci Rep. 2021;11(1). doi:10.1038/S41598-021-00675-Y
7. Shein AMS, Wannigama DL, Higgins PG, et al. Novel Colistin-EDTA Combination for Successful Eradication of Colistin-Resistant Klebsiella Pneumoniae Catheter-Related Biofilm Infections. Sci Rep. 2021;11(1). doi:10.1038/S41598-021-01052-5
8. Izadi S, Mohaghegh MA, Ghayour-Najafabadi Z, et al. Frequency and molecular identification of cryptosporidium species among immunocompromised patients referred to hospitals, central Iran, 2015-2016. Int J Med. 2015;15(1):31–39.
9. Srisakul S, Wannigama DL, Higgins PG, et al. Overcoming addition of phosphoethanolamine to lipid a mediated colistin resistance in Acinetobacter baumannii clinical isolates with colistin-sulbactam combination therapy. Sci Rep. 2022;12(1). doi:10.1038/S41598-022-15386-1
10. Tacconelli E, Göpel S, Gladstone BP, et al. Development and Validation of BLOOMY Prediction Scores for 14-Day and 6-Month Mortality in Hospitalised Adults with Bloodstream Infections: a Multicentre, Prospective, Cohort Study. Lancet Infect Dis. 2022;22(5):731–741. doi:10.1016/S1473-3099(21)00587-9
11. Camargo CH, Yamada AY, Nagamori FO, et al. Clonal Spread of ArmA- and OXA-23-Coproducing Acinetobacter Baumannii International Clone 2 in Brazil during the First Wave of the COVID-19 Pandemic. J Med Microbiol. 2022;71(4). doi:10.1099/JMM.0.001509
12. Nicoloff H. Standing up to Infectious Disease. Nat Microbiol. 2019;4(1):41564. doi:10.1038/s41564-018-0331-3
13. Ellwanger JH, Kaminski V, Chies JAB. Emerging infectious disease prevention: where should we invest our resources and efforts? J Infect Public Health. 2019;12(3):313–316. doi:10.1016/j.jiph.2019.03.010
14. Albanghali M, Alghamdi S, Alzahrani M, et al. Clinical Characteristics and Treatment Outcomes of Mild to Moderate COVID-19 Patients at Tertiary Care Hospital, Al Baha, Saudi Arabia: a Single Centre Study. J Infect Public Health. 2022;15(3):331–337. doi:10.1016/J.JIPH.2022.02.001
15. Alzahrani M, Ali M, Anwar S. Bacteria Causing Urinary Tract Infections and Its Antibiotic Susceptibility Pattern at Tertiary Hospital in Al-Baha Region, Saudi Arabia: a Retrospective Study. J Pharm Bioallied Sci. 2020;12(4):449. doi:10.4103/JPBS.JPBS_294_19
16. Alzahrani MA, Sadoma HHM, Mathew S, Alghamdi S, Malik JA, Anwar S. Retrospective analysis of antimicrobial susceptibility of uropathogens isolated from pediatric patients in tertiary hospital at Al-Baha Region, Saudi Arabia. Healthcare. 2021;9(11):1564. doi:10.3390/HEALTHCARE9111564
17. Tyrovolas S, El Bcheraoui C, Alghnam SA, et al. The Burden of Disease in Saudi Arabia 1990–2017: results from the Global Burden of Disease Study 2017. Lancet Planet Health. 2020;4(5):e195–e208. doi:10.1016/S2542-5196(20)30075-9
18. Murray CJ, Ikuta KS, Sharara F, et al. Global Burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655. doi:10.1016/S0140-6736(21)02724-0/ATTACHMENT/B227DEB3-FF04-497F-82AC-637D8AB7F679/MMC1.PDF
19. Tabish SA. Recent Trends in Emerging Infectious Diseases. Int J Health Sci. 2009;3(2):V–VIII.
20. Malik JA, Ahmed S, Mir A, et al. The SARS-CoV-2 mutations versus vaccine effectiveness: new opportunities to new challenges. J Infect Public Health. 2022;15(2):228–240. doi:10.1016/J.JIPH.2021.12.014
21. Ahmad Malik J, Ahmed S, Shinde M, et al. The impact of COVID-19 on comorbidities: a review of recent updates for combating it. Saudi J Biol Sci. 2022;29(5):3586–3599. doi:10.1016/J.SJBS.2022.02.006
22. Farooqi T, Malik JA, Mulla AH, et al. An overview of SARS-COV-2 epidemiology, mutant variants, vaccines, and management strategies. J Infect Public Health. 2021;14(10):1299–1312. doi:10.1016/J.JIPH.2021.08.014
23. Malik JA, Mulla AH, Farooqi T, Pottoo FH, Anwar S, Rengasamy KRR. Targets and strategies for vaccine development against SARS-CoV-2. Biomed Pharmacother. 2021;137:111254. doi:10.1016/J.BIOPHA.2021.111254
24. Malik JA, Aroosa M, Ahmed S, et al. SARS-CoV-2 vaccines: clinical endpoints and psychological perspectives: a literature review. J Infect Public Health. 2022;15(5):515–525. doi:10.1016/J.JIPH.2022.03.017
25. McGowan JE. Economic impact of antimicrobial resistance. Emerg Infect Dis. 2001;7(2):286–292. doi:10.3201/EID0702.010228
26. Shibl AM, Memish ZA, Kambal AM, et al. National surveillance of antimicrobial resistance among gram-positive bacteria in Saudi Arabia. J Chemother. 2014;26(1):13–18. doi:10.1179/1973947813Y.0000000084
27. Zowawi HM. Antimicrobial Resistance in Saudi Arabia. An Urgent Call for an Immediate Action. Saudi Med J. 2016;37(9):935–940. doi:10.15537/SMJ.2016.9.16139
28. Wanla W, Katip W, Supakul S, Apiwatnakorn P, Khamsarn S. Effects of an antimicrobial restriction system on appropriate carbapenem use in a hospital without infectious diseases consultation. Taylor & Francis. 2017;10:443–449. doi:10.2147/IJGM.S145133
29. Balkhy HH, Cunningham G, Chew FK, et al. Hospital- and community-acquired infections: a point prevalence and risk factors survey in a tertiary care center in Saudi Arabia. Int J Infect Dis. 2006;10(4):326–333. doi:10.1016/J.IJID.2005.06.013
30. Safdar OY, Alzahrani WA, Kurdi MA, et al. The Prevalence of Renal Stones among Local Residents in Saudi Arabia. J Family Med Prim Care. 2021;10(2):974. doi:10.4103/JFMPC.JFMPC_262_20
31. Alzahrani MA, Sadoma HHM, Mathew S, Alghamdi S, Malik JA, Anwar S. Retrospective analysis of antimicrobial susceptibility of uropathogens isolated from pediatric patients in tertiary hospital at al-baha region, Saudi Arabia. Healthcare. 2021;9(11):1–11. doi:10.3390/healthcare9111564
32. Alshamrani MM, El-Saed A, Alsaedi A, et al. Burden of healthcare-associated infections at six tertiary-care hospitals in Saudi Arabia: a point prevalence survey. Infect Control Hosp Epidemiol. 2019;40(3):355–357. doi:10.1017/ice.2018.338
33. Merga Duffa Y, Terfa Kitila K, Mamuye Gebretsadik D, Bitew A. Prevalence and Antimicrobial Susceptibility of Bacterial Uropathogens Isolated from Pediatric Patients at Yekatit 12 Hospital Medical College, Addis Ababa, Ethiopia. Int J Microbiol. 2018;2018. doi:10.1155/2018/8492309
34. Alzahrani MA, Ali MS, Anwar S. Bacteria causing urinary tract infections and its antibiotic susceptibility pattern at tertiary hospital in al-baha region, Saudi Arabia: a retrospective study. J Pharm Bioallied Sci. 2020;12(4):449. doi:10.4103/JPBS.JPBS_294_19
35. Ferrara P, Cutrona C, Sbordone A. Which treatment for upper respiratory tract infections? Ital J Pediatr. 2015;41(Suppl 2):A31. doi:10.1186/1824-7288-41-S2-A31
36. Woodhead M, Blasi F, Ewig S, et al. Guidelines for the management of adult lower respiratory tract infections. Eur Respir J. 2005;26(6):1138–1180. doi:10.1183/09031936.05.00055705
37. Yoon YK, Park C-S, Kim JW, et al. Guidelines for the antibiotic use in adults with acute upper respiratory tract infections. Infect Chemother. 2017;49(4):326. doi:10.3947/IC.2017.49.4.326
38. Ieven M, Coenen S, Loens K, et al. Aetiology of lower respiratory tract infection in adults in primary care: a prospective study in 11 European countries. Clin Microbiol Infect. 2018;24(11):1158–1163. doi:10.1016/J.CMI.2018.02.004
39. Shlaes DM, Gerding DN, John JF, et al. Society for Healthcare Epidemiology of America and Infectious Diseases Society of America joint committee on the prevention of antimicrobial resistance: guidelines for the prevention of antimicrobial resistance in hospitals. Clin Infect Dis. 1997;25(3):584–599. doi:10.1086/513766
40. Lee CR, Cho IH, Jeong BC, Lee SH. Strategies to minimize antibiotic resistance. Int J Environ Res Public Health. 2013;10(9):4274. doi:10.3390/IJERPH10094274
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.