Back to Journals » Nature and Science of Sleep » Volume 9
Infant sleep and its relation with cognition and growth: a narrative review
Authors Tham EK ![]() , Schneider N, Broekman BF
, Schneider N, Broekman BF
Received 28 October 2016
Accepted for publication 9 March 2017
Published 15 May 2017 Volume 2017:9 Pages 135—149
DOI https://doi.org/10.2147/NSS.S125992
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Steven Shea
Elaine KH Tham,1 Nora Schneider,2 Birit FP Broekman1
1Singapore Institute for Clinical Sciences, Agency for Science, Technology and Research (A*STAR), Singapore, Singapore; 2Nestec Ltd., Nestlé Research Center, Lausanne, Switzerland
Objective: Infant sleep development is a highly dynamic process occurring in parallel to and in interaction with cognitive and physical growth. This narrative review aims to summarize and discuss recent literature and provide an overview of the relation between infant sleep and cognitive development as well as physical growth.
Methods: We conducted online literature search using MEDLINE, Embase, and Cochrane Library databases. We considered original research on humans published in the English language from January 2005 to December 2015. Search terms included “sleep” AND “infant” AND “cognition” OR “memory” OR “executive functioning”, OR “growth” OR “obesity” OR “growth hormone” OR “stunting”, and combinations thereof.
Results: Ten studies on infant sleep and cognition were included in this review. Overall, findings indicated a positive association between sleep, memory, language, executive function, and overall cognitive development in typically developing infants and young children. An additional 20 studies support the positive role of infant sleep in physical growth, with the current literature focusing largely on weight gain and obesity rather than healthy growth. Existing evidence in both the domains is mainly based on cross-sectional designs, on association studies, and on parental reports. In contrast, there were limited studies on longitudinal sleep trajectories and intervention effects, or studies have not used more objective sleep measures such as actigraphy and polysomnography.
Conclusion: The reviewed studies support a critical and positive role of infant sleep in cognition and physical growth. Future studies should consider key environmental and parental confounders, include a combination of more objective (actigraphy) and subjective measures (sleep diaries and questionnaires), and move towards longitudinal trajectory designs of infant sleep and development.
Keywords: infant sleep, cognition, growth
Introduction
Sleep develops rapidly during the first few years of life and is a highly dynamic process. At birth, infants lack an established circadian rhythm and hence sleep across multiple intervals throughout the day and night in short bouts, which may also be due to infants’ feeding needs.1 At about 10–12 weeks of age, the first signs of a circadian rhythm begin to develop, marked by an increased ease of sleeping through the night.2 The change in total sleep duration over 24 hours continues and decreases from 16 to 17 hours in newborns, to 14–15 hours at 16 weeks of age, and 13–14 hours by 6 months of age.3,4 While the need for day sleep decreases,5 night sleep duration increases through the first year of life,5–7 resulting in a shift towards more nocturnal patterns of sleep.
Infant sleep studies show that about 20%–30% of all infants experience night awakenings throughout their first 2 years of life.8,9 Yet, with children’s development, the number of awakenings per night reduces, and the ability to sleep through the night increases with ~50%–75% of infants sleeping through the night at 12 weeks of age10 and at least 90% at 6 months of age.11 Despite the general trend of decrease, night awakenings show the highest levels of variability across all sleep measures,4 which makes it an interesting research target for sleep quality in young infants.
Concerns that children are not getting enough sleep have been around for over 100 years, with recommendations of ideal sleep duration for children being provided as early as 1897.12 The National Sleep Foundation (NSF) recommends a daily sleep duration of 14–17 hours/day from birth to 3 months, 12–15 hours/day from 4 to 11 months, 11–14 hours/day for infants aged 1–2 years, and 10–13 hours/day for preschoolers aged 3–5 years. In all cases except for newborns to 3 months, the latest NSF recommendations increased by at least 1 hour from the preceding (NSF) recommendations due to reported changes in sleep durations over the last years (from a systematic literature search) as reviewed by an expert panel.13 However, many infants and young children sleep less than the above-recommended amount.12 Short sleep duration is particularly prevalent in predominantly Asian countries. A study conducted on caregivers of 29287 children between the ages of 0 and 36 months from 17 countries reports that total sleep duration in children from predominantly Asian counties is significantly lower than children from predominantly Caucasian countries.14 Moreover, regardless of age group, children from predominantly Asian countries consistently sleep less or at the lower extreme of the NSF recommendation.
Sleep is a highly dynamic developmental process, particularly in the first 2 years of life, with a high inter- and intraindividual variability. While many studies have focused on children, the link between variations in sleep and developmental outcomes in healthy infants remains less explored. The objective of this narrative review is therefore to summarize and evaluate available literature on the relation between infant sleep during the first 2 years of life and cognitive and physical growth in healthy typically developing infants and young children.
Methods
We searched MEDLINE, Embase, and Cochrane Library databases for articles in English and published between 2005 and December 2015. Search terms included “sleep” AND “infant”, in combination with “cognition” OR “memory” OR “executive functioning” OR “growth” OR “obesity” OR “growth hormone” OR “stunting”. Search terms had to be present in either the title or the abstract of the article. In addition, we limited results to original research articles investigating infant sleep during the first 2 years of life in relation to cognitive development and physical growth outcomes both during the first 2 years of life or later, human studies, and studies on term-born, cognitively healthy infants. Studies on sleep disorders, including sleep-disordered breathing symptoms, were excluded from this review, as well as studies in psychiatric populations or preterm infants.
Our literature search resulted in the following hits:
Sleep and infant and cognition, and/or memory, and/or executive functioning: 85 MEDLINE hits, 89 Embase hits, and eight Cochrane Library hits. After examining all the extracted titles and abstracts, 31 overlapping articles were removed, four articles were excluded as they were review papers that did not have a focus on sleep and cognition in healthy typically developing infants, and 98 were excluded as sleep was not the main variable of interest or that sleep was not measured during infancy amongst healthy term-born infants. After the exclusion, ten publications were considered relevant for the scope of the review.
Sleep and infant and growth and/or obesity and/or growth hormone and/or stunting: 29 MEDLINE hits, four Cochrane Library hits, and 47 Embase hits. Of the 80 screened publications, 29 were considered for inclusion having removed overlapping publications. After screening titles and abstracts and reading the full-length papers, 20 publications were considered relevant for infant sleep and growth, and hence included in this review.
Results
Infant sleep and cognition
Sleep is a period that is characterized by marked change in brain activity,15 in addition to being a resting period of reduced sensory activity and responsiveness to external stimuli.16 As such, sleep has been related to subsequent cognitive and developmental benefits.17 Multiple studies have found relationships between sleep duration and cognitive benefits in school-aged children.18–21 Unlike studies on older children, there have been fewer studies regarding the effects of infant sleep on cognitive outcomes. Out of the ten studies reviewed in this paper, seven were cross-sectional studies, and three were longitudinal studies. Table 1 presents a summary of the reviewed articles.
 | Table 1 Summary of reviewed studies for sleep and cognitive development Abbreviations: WPPSI, Wechsler Preschool and Primary Scale of Intelligence; BMI, body mass index. |
Cross-sectional studies
The majority of the reviewed articles for sleep and cognition consist of cross-sectional studies. Within the cross-sectional studies, four studies focused on the effect of post-learning sleep on memory consolidation, one study examined relations between sleep (1 week) prior to learning and subsequent memory, and two studies investigated overall associations between sleep and general cognitive development.
Similar to findings in adults,22,23 researchers have found evidence that infant sleep also plays an important role in memory consolidation, a process whereby a initially weak memory representation becomes stable and more resistant to forgetting.22,24 Seehagen et al found that 6- and 12-month-old infants who napped for at least 30 minutes after learning a set of object–action pairings from a puppet toy recalled significantly more target actions while tested after 4-hour delay and 24-hour delay compared to infants in the baseline condition who were not trained on the object–action pairings and to infants in the no-nap group who spent an equivalent time awake after learning (at the 24-hour delay test).25 Even though the researchers found an overall benefit of sleep towards object–action memory especially compared to infants in the baseline condition and at the 24-hour delay test, it should be noted that there were no differences in memory performance between the nap group and no-nap group at the 4-hour delay test.
Apart from object–action memory, studies have also shown that infant sleep, in particular daytime naps, is beneficial towards language learning. Gómez et al found that after learning an artificial language, 15-month-old infants who napped for at least 30 minutes were able to abstract grammatical relations amongst the learnt words at a subsequent test session that occurred 4 hours after learning, where they looked longer at trials where stimuli were consistent with the learnt artificial language as compared to inconsistent trials.26 In contrast, infants who did not nap (but spent an equivalent time awake) did not look significantly longer at consistent compared to inconsistent trials during testing, and hence were not able to learn the abstracted relations between the artificial language.26 In addition, a further experiment by the above researchers on a similar group of 15-month-old infants showed that the nap-dependent benefits towards language learning (where infants learnt abstract grammatical relations) persisted even after 24 hours.27 A recent study by a separate group of researchers also highlighted nap-dependent benefits towards language in terms of vocabulary learning.28 In the study, Horváth et al found that 16-month-old infants who napped after learning sets of new object–word associations spent more time looking at the correct associative pairing at the 2-hour delayed test session, whereas infants who remained awake did not display any differences in looking between the learning and delayed test sessions.
Overall, the above studies on object–action memory and language learning all support the claim that sleep benefits memory consolidation. However, it is interesting that there were no differences between the nap and no-nap group at the 4-hour delay test in Seehagen et al’s object–action memory study, whereas differences between infants who napped and those who spent an equivalent time awake emerged after a similar 4-hour delay in Gómez et al’s study on language learning. In Horváth et al’s vocabulary-learning study, the nap-dependent effects were present just after at a 2-hour delayed test session. One possible reason for the different findings could be that the infants in Seehagen et al’s study were younger (6- and 12-month olds) than the 15- and 16-month olds in Gómez et al’s and Horváth et al’s studies; sleep changes and matures rapidly during infancy,29 and hence the 3- to 10-month age difference between the infants may have contributed to the different sleep-associated effects between the studies. Another reason for the difference in findings may be due to the nature of the experimental task and test stimuli. Studies in adults demonstrate that sleep shows a preferential benefit towards memories that are deemed to be more relevant for the future.30,31 It is plausible that the object–action associations in Seehagen et al’s study are “less relevant” to 6- and 12-month-old infants, whereas the language stimuli in Gómez et al’s and Horváth et al’s studies may be more relevant and salient to the 15- and 16-month-old infants who are also undergoing a period of rapid vocabulary development (“vocabulary spurt”).32
In addition to post-learning sleep, a study by Lukowski and Milojevich indicates that normative variation in everyday habitual infant sleep prior to learning may also affect memory of the newly learnt information.33 First, the researchers collected parental reports of twenty-five 10-month-old infants’ sleep habits for the week prior to the encoding session. Next, during the encoding session, the infants were visually presented with six two-step object–action event sequences with narration during an encoding session. Recall memory and memory generalization (ability to generalize responses to new stimuli that were similar to those presented at encoding) were tested after a 2-hour delay. Infants with a greater number of night awakenings performed poorer (displayed fewer target actions) in the memory generalization task, and infants with longer daytime nap durations performed better in the same task. There was a positive relation between duration of daytime naps and memory recall immediately after encoding, and a negative correlation between higher percentages of night sleep duration (out of total sleep duration) and immediate recall. In contrast, there was no relation between habitual sleep duration and delayed memory recall of the event sequences. The lack of significant associations between sleep duration and memory recall of the object–action event sequences at the delayed testing session is particularly interesting in comparison to the positive nap-dependent effects in the reviewed memory consolidation studies where infants who napped displayed better memory and learning when they were tested after a delay.
Although the cross-sectional studies amongst typically developing infants mainly focused on memory consolidation and learning, two of the reviewed studies examined the relation between infant sleep and general cognitive development. In the first study, researchers found that greater movements or activity during sleep and greater number of awakenings after sleep onset measured via sleep actigraphy recordings were negatively correlated with scores on the Bayley Scales of Infant and Toddler Development second edition (BSID-II) Mental Development Index (MDI) amongst 10-month-old infants.34 In contrast, greater sleep efficiency (i.e. spending a larger percentage of time asleep between sleep onset and wakefulness) was positively correlated with BSID-II MDI scores in the same group of infants.34 In the second study, researchers found that 11- to 13-month-old infants who had greater sleep efficiency measured via sleep actigraphy data also displayed better overall cognitive problem-solving skills as measured by the Ages and Stages Questionnaire.35 Besides sleep efficiency, longer proportions of sleep at night were also associated with better cognitive problem-solving skills.35 It should be noted that both of these studies also explored parental sleep reports in addition to sleep actigraphy data; however, unlike the sleep actigraphy data, there were no significant associations between parental sleep reports and any of the cognitive measures.
Despite the fact that all the reviewed cross-sectional studies showed sleep-associated benefits, there were no consistent findings amongst the studies regarding the component of sleep (i.e. sleep duration, sleep efficiency, night awakenings, etc.) that benefitted cognition. However, it may also not be feasible to directly compare the studies due to differences in study design as the effects of sleep in the memory consolidation studies were explored in a between-participant design involving sleep within a nap period, whereas Lukowski and Milojevich’s study and the two studies on general cognitive development explored within-infant normative variations in sleep habits.
Longitudinal studies
In addition to the above-mentioned cross-sectional studies, three studies investigated longitudinal relations between sleep and cognition. Two out of the three studies highlighted that infant sleep was related to subsequent executive functioning during toddlerhood and early childhood.36–38 One of the studies showed that higher percentages of parent-reported night sleep (out of total sleep duration) at 12 and 18 months of age were significantly associated with better executive functioning performance at 26 months of age, especially performance related to impulse-control tasks.38 The benefits of higher percentages of sleep duration at night seemed to extend beyond toddlerhood. Findings from a second study report that 12-month-old infants with higher proportions of night sleep displayed better executive functioning performance at 4 years, measured by the Matrix Reasoning subscale of Wechsler Preschool and Primary Scale of Intelligence (WPPSI) third edition.37 In contrast, the study found that there was no relation between 12-month-old sleep duration and concurrent general cognitive functioning (Bayley Scales of Infant Development).37 In all the above studies, the longitudinal relations between infant sleep and executive functioning were independent of confounders such as family socioeconomic status.
One of the reviewed longitudinal studies explored the relation between infant sleep, psychosocial adversity, and IQ scores (assessed using the WPPSI – Revised).39 Unlike the studies on infant sleep and executive functioning, the longitudinal relation between infant sleep and IQ scores of WPPSI – Revised seems less direct. This current study reports high amounts of maternal-reported infant sleep difficulties and sleep disturbances at 12 and 18 months to be correlated with lower IQ scores at 5 years of age.39 However, the above finding was no longer statistically significant after adjusting for psychosocial adversity. In addition, the study did not find any significant relations between IQ scores and sleep actigraphy data that were collected at 5 years of age.
In summary, ten studies have been identified that describe the relation between sleep and cognition in typically developing infants. Cross-sectional studies revealed that, similar to adults, sleep benefits memory and (language) learning in infants, both before and after learning. Although all reviewed memory and language-learning studies showed sleep-associated benefits towards cognition, the sleep parameter (i.e. night sleep duration, daytime napping, night awakenings, etc.) that benefitted cognition remained inconsistent. Longitudinal studies on infant sleep and executive functioning consistently showed that higher percentages of parent-reported infant night sleep were related to better subsequent executive functioning performance.36–38 However, it should be noted that the studies were conducted by a single research group using the same participant pool. Although this may not affect the validity of the findings, replication studies in other samples would be useful in interpreting the generalizability of the findings beyond the existing participant pool.25–28,33 Although majority of the cross-sectional studies recorded sleep via actigraphy data, the sleep data used in the longitudinal studies were primarily obtained from parental reports. Future longitudinal studies may also consider collecting sleep data via actigraphy; especially, some cross-sectional studies have reported sleep-associated findings with actigraphy data but not parental reports.34,35
Infant sleep and growth
Sleep is controlled by chronobiological mechanisms, and the most rapid development in sleep organization occurs during the first 6 months of life, a period that is also marked by rapid physical growth. Yet, the relation between sleep and growth with a focus on infancy, early childhood, and healthy development has not been systematically addressed in the literature. However, some plausible relationships between sleep and growth have been explored, mainly in epidemiological studies: i) sleep and weight gain/obesity, ii) growth retardation/stunting and sleep, and iii) sleep and growth hormone. Table 2 provides a summary of the reviewed studies.
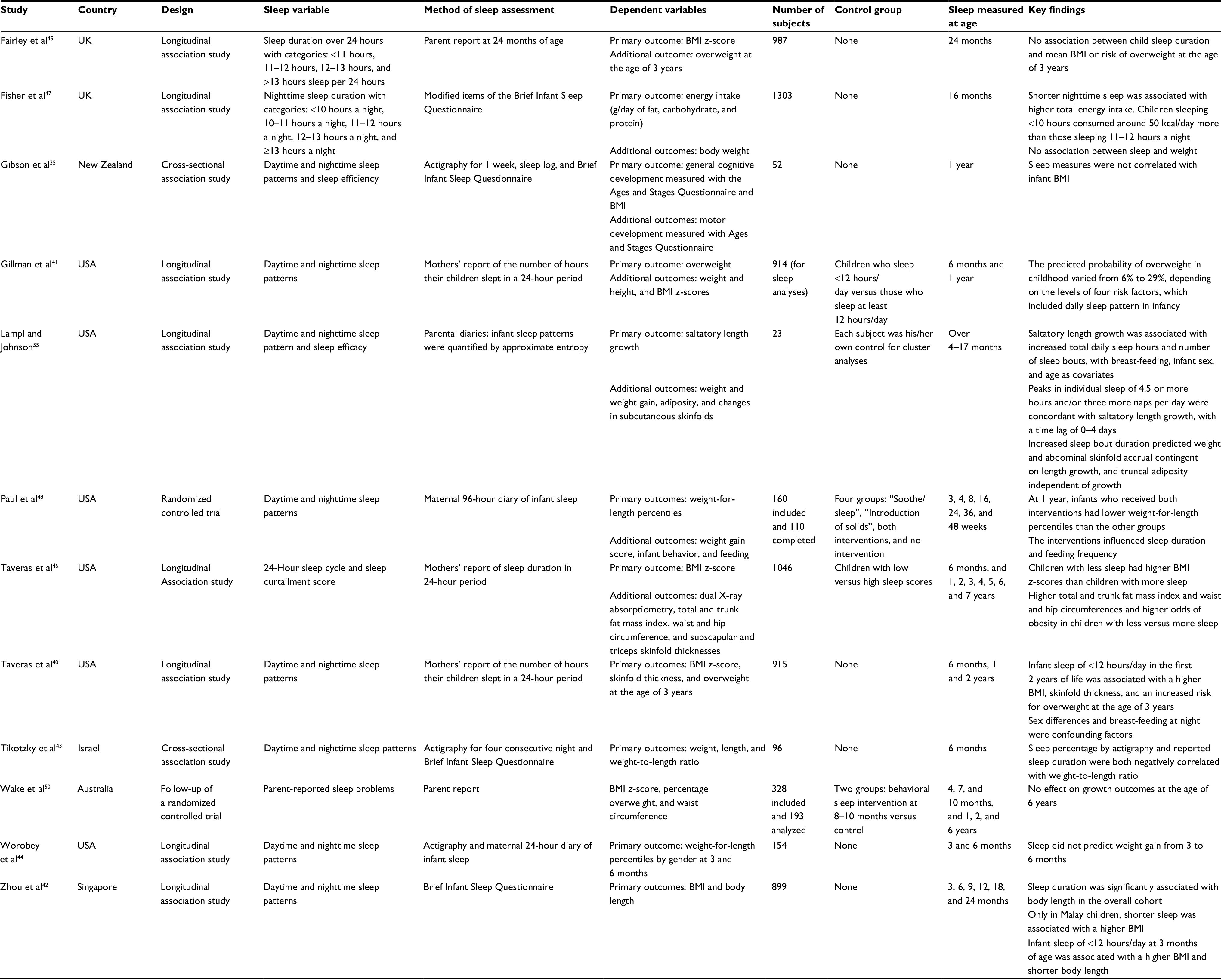 | Table 2 Summary of reviewed studies for sleep and growth Abbreviation: BMI, body mass index. |
Weight gain and obesity measures
Compared to adolescent and adult studies, only a few studies have examined the impact of sleep on physical growth parameters in infants specifically. However, the relation to obesity appears one of the most investigated concepts with regard to sleep. A study for example found that infant sleep of <12 hours/day in the first 2 years of life was associated with a higher body mass index (BMI), skinfold thickness, and an increased risk of being overweight at 3 years.40 Secondary analyses of longitudinal changes in sleep duration over the first 3 years of life revealed an increase in mean weight-for-length z-score by 0.02 for each hour/day decrease. Analyses based on the same cohort confirmed the inverse relation of sleep duration of <12 hours/day and the probability of overweight at 3 years of age.41 The cut-off at 12 hours/day seems supported by the GUSTO study in Singapore which reported sleep of <12 hours/day at 3 months of age to be associated with a higher BMI and shorter body length.42 However, in both studies, sleep data were based on parental report of infant sleep, while no objective sleep measures were applied. A cross-sectional study points in the same direction: a shorter sleep duration as assessed by parent report was linked to an increase in weight-to-length ratio as early as 6 months of life. In girls only, those findings could be substantiated by actigraphy data with a shorter sleep duration being associated with larger body size measures.43 In contrast, a study of actigraphic sleep in 1-year-old infants35 and an observation study using a sleep-monitoring device over the first 6 months of life44 did not find significant correlations with BMI or weight gain. Similarly, researchers did not find any significant association between sleep duration at 24 months as assessed by sleep questionnaire and BMI or risk of overweight at the age of 3 years in the Born in Bradford birth cohort study.45 Looking at longer term consequences of infant sleep, a follow-up of the above-mentioned prospective cohort highlights as one of the first studies of the impact of chronic sleep curtailment from infancy to mid-childhood on BMI and adiposity measures.40 Children with less sleep compared to children with more sleep had a higher BMI z-score, skinfold thickness, total and trunk fat mass index, waist circumference, hip circumference, and higher odds of obesity. Curtailed sleep was defined as <12 hours/day from age 6 months to 2 years, <10 hours/day from age 3–4 years, and <9 hours/day from age 5–7 years.46
One of the mediating factors in the relation of sleep and weight gain or risk of obesity may be energy intake, as suggested by a study of 16-month-old children of the Gemini twin birth cohort. While the association between sleep and weight was not significant at this age, shorter nighttime sleep as measured by a sleep questionnaire was associated with a higher total energy intake, with children sleeping <10 hours consuming around 50 kcal/day more than children sleeping 11–12 hours a night.47
In addition, most evidence from our review stems from observation and cohort studies, whereas evidence from intervention studies is still scarce. Only two intervention studies were identified in the context of this review and yielded mixed findings. A pilot randomized controlled trial investigating the effect of modification of parental behaviors with regard to feeding, sleeping, and crying on infant weight gain and early obesity risk found that behavioral modification resulted in lower weight-for-length percentiles at 1 year of age for infants who received a combined soothe/sleep and introduction of solid foods intervention (33rd percentile; P = 0.009) compared to those who received the soothe/sleep intervention only (50th percentile), to those who received the introduction of solid foods intervention only (56th percentile), and to the control group (50th percentile). In addition, the soothe/sleep intervention yielded prolonged nocturnal sleep during the first year of life compared to the control group, especially in predominantly breast-fed infants.48 As the observed effect on weight gain was strongest in the combined intervention, it cannot be attributed to longer sleep duration as such, but those findings suggest that prolonged nocturnal sleep plays a relevant role as part of a multicomponent intervention early in life. This study served as a pilot to the larger, currently ongoing Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study.49 In contrast, a short intervention delivering behavioral sleep strategies from 8 to 10 months postpartum did not show beneficial effects on BMI z-score, percentage of overweight/obesity, and waist circumference at 6 years of life.50 The two intervention studies differ in several aspects, most notably in intervention duration and intensity (1 year vs 2 months), start of intervention (shortly after birth vs at 8 months), follow-up duration (1 year versus 6 years), and most importantly in modulating sleep as a single factor versus modulating multiple factors to impact weight gain and risk of obesity.
Overall, those results indicate the potential risk of shorter sleep duration early in life for overweight and adiposity later in life. Suggested mechanisms that link shorter sleep or sleep restriction to weight gain, obesity, and insulin resistance include counter-regulatory hormones such as cortisol and growth hormone,51 altered activity of the autonomous nervous system,52 and the alteration of appetite-regulating hormones like leptin and ghrelin which increases appetite and hunger.53 Behaviorally, longitudinal data analyses, for example, from the National Longitudinal Study of Adolescent Health, suggest an association between later bedtime and an increase in BMI.54
Length and height
A recent study suggests sleep and episodic length growth in 4- to 17-month-old infants to be a temporally coupled process with prolonged sleep preceding length growth by 0–4 days.55 The authors found an increase of up to 4.5 hours and/or three more naps per day to be predictive of length growth suggesting an underlying biological system. In turn, growth restriction or growth-rate reduction as early as in utero (intrauterine growth restriction, IUGR) alters sleep patterns.56,57 IUGR fetuses have decreased amounts of active sleep and increased amounts of quiet sleep and indeterminate sleep compared to appropriately grown fetuses. The time spent in active sleep could have an especially significant effect on brain maturation.58 Those alterations in sleep organization early in life may persist into childhood: a study showed, for example, lower sleep efficiency and more awakenings during the sleep period in IUGR children aged 4–7 years.59 In addition, researchers investigated the relation between stunting, iron deficiency anemia, and maternal reports of sleep in 6- to 18-month-old infants in two studies from Zanzibar and one from Nepal.60 Stunting was associated with a shorter night sleep duration, higher frequency of night waking, and shorter nap duration.
While related mechanisms are not yet well understood, sleep plays an important role in energy balance. Altered sleep-state organization may be an adaptive response to preserve energy in states of IUGR or stunting.58
Growth hormone
A bidirectional interaction between hormones and sleep can be assumed. Several hormones are both involved in circadian rhythm and sleep and affected by the quantity and quality of sleep. Those hormones include, for example, melatonin, cortisol, leptin, ghrelin, insulin-like growth factor-1, prolactin, and growth hormone.61 The latter hormone plays a major role in stimulating body growth, and its high levels in plasma of infants suggest an important role in the first months of life.62 The secretion of growth hormone is influenced by factors such as nutrition, physical activity, and sleep patterns. Increased levels of hormones are secreted during sleep, peaking shortly after sleep onset.63 In the context of this review, no study has been identified to specifically investigate the link or the impact of growth hormone on sleep in healthy infants and young children. While well-characterized data on growth hormone release in association with healthy sleep pattern maturation during the first months of life are lacking,64 pediatric patients with growth hormone deficiency have been shown to display a reduced total sleep time with increased wakefulness and subsequently a decrease in sleep efficiency compared to control subjects as assessed by polysomnography.65 The relation between growth hormone and sleep in infants may not be fully understood, but a close interaction of the neuroendocrine and the chronobiological system has been shown in different populations. The (dys-)regulation of one system can affect the other.
In summary, while physical growth and weight gain in the first 2 years of life are largely predicted by birth weight, prenatal factors, and nutrition,66 a growing body of evidence supports the critical role of infant sleep in growth. Several aspects of growth can be considered in relation to sleep, such as weight gain, stunting, and hormone release. However, the current literature focuses largely on weight gain and obesity rather than healthy growth. In particular, the detrimental impact of sleep deprivation on glucose tolerance, insulin sensitivity, and appetite-regulating hormones has been widely reviewed. In that context, infant and child sleep seems to provide a modifiable and thus promising target for obesity prevention, especially when regarded within multicomponent approaches. It is to be noted that most studies rely on parental report measures, and the quantification of sleep is usually converted to express hours of sleep; objective methods like actigraphy however gain more and more in relevance. Influencers for the sleep–growth relation, especially in infants and young children, include gender, prematurity, health conditions like allergies, nutritional factors like iron deficiencies, energy intake or feeding paradigm, and nighttime versus daytime sleep.43,47,67
General discussion
Overall, the review of recent literature highlights that normative variations in infant sleep play an important role in cognitive development and physical growth. Studies on cognition show that individual differences in sleep quantity and quality are particularly important for the development of memory, language, and executive functions. Studies on physical growth indicate the potential risk of sleep problems, in particular shorter sleep duration early in life, for overweight, obesity, or measures of adiposity in infants, toddlers, and preschool-age children.
The findings from this review in infants are in line with epidemiological evidence from studies in older children and adolescents,29,68–73 and some associations suggest persisting impact beyond infancy and young childhood. Although normative variations in habitual sleep in infants may be important for development, the review showed little consistency across the studies with regard to the component of sleep investigated (i.e. night sleep duration, daytime napping, night awakenings, etc.). This makes comparisons of studies and the generalization of the findings difficult and may likely be due to different methodologies used across studies. Many tools are available for assessing infant’s and young children’s sleep with different strengths and limitations. Questionnaires and sleep diaries are cost-efficient and can be administered to a large participant pool; however, these measures are also more subjective and less accurate in estimating sleep parameters when used as stand-alone measures. In contrast, sleep polysomnography and actigraphy provide more accurate and objective assessments of sleep, but are often very costly. While polysomnography requires the placement of electrodes by specialist staff and the children to stay overnight at a sleep lab, actigraphy watch may be worn by the children at home for longer periods of time,74,75 and is therefore particularly useful for an objective assessment of sleep in infants and young children or when conducting sleep assessments in large samples as it enables nonintrusive measurement of sleep in one’s natural environment.76 Hence, it would also be useful for future longitudinal studies to incorporate more objective sleep measures like actigraphy for at least a subsample of participants. Still, particular challenges occur even with more objective measures; for example, individual differences in sleep arrangements77 such as falling asleep alone versus being rocked to sleep may interfere with the accuracy of the collected data. Therefore, it is also important to consider these methodological differences and individual differences when measuring infant sleep. Overall, a combination of approaches such as using questionnaires and diaries for a large sample and validating data with actigraphy in a smaller subsample may be most promising and yet feasible. Amongst the reviewed studies where both actigraphy and questionnaire data were collected at the same time point, researchers found positive associations between infants’ sleep actigraphy data and general cognitive development,34,35 but no equivalent findings with questionnaire data. With regard to weight gain, most findings are based on parent report and questionnaire measures and largely point towards shorter sleep duration being linked to higher body size measures. Only three studies used actigraphy35,43 and one study a sleep-monitoring device44 and resulted in conflicting findings.
With regard to study designs, most reviewed studies used cross-sectional and observational designs with infants sampled at different ages. This may be a limitation as both sleep and neurodevelopment are very age-dependent and vary across different developmental stages due to their highly dynamic nature. Alternatively, longitudinal sleep and development assessments with repeated measurements for the same individuals at various time points may allow for a better understanding of developmental trajectories in those domains. Future work would benefit from trajectory studies with objective data (such as actigraphy and polysomnography) from infancy onwards, to detect the role of early infant sleep on later outcomes. Only two of the reviewed studies investigated the effect of sleep-related interventions and only with regard to weight gain.48,50 While the longer (1 year) intervention trial that targeted multiple parental behaviors in the intervention resulted in a positive effect on lower weight-for-length percentiles at 1 year of life, the shorter (2 months) trial targeting behavioral sleep strategies did not show any effects on growth parameters at 6 years of life. In the absence of a bigger body of evidence, no recommendations can be made; however, sleep-related multicomponent interventions may be promising for supporting or improving healthy infant and child development.
Notably, some studies25,33 did not control for known confounding variables such as socioeconomic status,73 maternal mental health,78 and parenting effects or effects of bedtime routines,79 which may explain some of the variations in the cognition-related findings. It would moreover be interesting to explore the role of gender in sleep and cognitive and physical growth outcomes. Gender differences have been reported for sleep and growth; for example, shorter sleep duration was associated with larger body size measures in 6-month-old infant girls but not boys.43 Although the scope of this review excluded studies on sleep disorders, conditions such as sleep-disordered breathing symptoms have been reported to lead to differences in cognitive outcomes. Recent studies found that infants with sleep-disordered breathing or primary snoring problems performed poorer on BSID scales as compared to age-matched controls.80–83 Therefore, in addition to understanding the role of “normal” infant sleep in cognitive development and physical growth, more research on the impact of infant sleep disorders on cognitive, behavioral, and growth outcomes may be desirable.
Conclusion
Infant sleep is a particularly interesting field of research due to its dynamic trajectories, the developmental changes that occur during this period, and the interaction with other developmental domains. More specifically, we reviewed the association between infant sleep and cognition as well as physical growth. From the reviewed literature, we conclude that sleep plays a key role in those domains with its maturation paralleling, preceding, as well as resulting from interactions with cognitive and physical maturation. Exact mechanisms have not been the focus of this review and still remain to be understood; however, the maturation of central nervous system structures like the hypothalamus or the neurotransmitter system underlies both cognitive development and the regulation of sleep/wake cycles.84
For future research, a combination of objective and subjective methods of sleep assessment is desirable, especially in the longitudinal exploration of both quantitative and qualitative aspects of sleep and infant development. From the cross-sectional studies, it is not possible to draw strong causal links between the two based on existing literature. For future studies, we propose to adopt a trajectory design which may reflect better the maturation and dynamic development, especially at young ages. It may furthermore improve the predictability of long-term effects on health and development compared to the predictability of cross-sectional time-point estimates as well as enabling us to examine the effects of cumulative sleep as compared to critical periods in the above relation. This is important to understand as sleep is one early life factor that can be targeted for interventions to optimize early development.
Disclosure
Nora Schneider is an employee of Nestec Ltd. The authors report no other conflicts of interest in this work.
References
Davis KF, Parker KP, Montgomery GL. Sleep in infants and young children: Part one: normal sleep. J Pediatr Heal Care. 2004;18(2):65–71. | ||
Mirmiran M, Baldwin RB, Ariagno RL. Circadian and sleep development in preterm infants occurs independently from the influences of environmental lighting. Pediatr Res. 2003;53(6):933–938. | ||
Adams SM, Jones DR, Esmail A, Mitchell EA. What affects the age of first sleeping through the night? J Paediatr Child Health. 2004;40(3):96–101. | ||
Galland BC, Taylor BJ, Elder DE, Herbison P. Normal sleep patterns in infants and children: a systematic review of observational studies. Sleep Med Rev. 2012;16(3):213–222. | ||
Sadeh A, Mindell JA, Luedtke K, Wiegand B. Sleep and sleep ecology in the first 3 years: a web-based study. J Sleep Res. 2009;18(1):60–73. | ||
Bruni O, Baumgartner E, Sette S, et al. Longitudinal study of sleep behavior in normal infants during the first year of life. J Clin Sleep Med. 2014;10(10):1119–1127. | ||
Iglowstein I, Jenni OG, Molinari L, Largo RH. Sleep duration from infancy to adolescence: reference values and generational trends. Pediatrics. 2003;111(2):302–307. | ||
Mindell JA, Kuhn B, Lewin DS, Meltzer LJ, Sadeh A; American Academy of Sleep Medicine. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep. 2006;29(10):1263–1276. | ||
Elias MF, Nicolson NA, Bora C, Johnston J. Sleep/wake patterns of breast-fed infants in the first 2 years of life. Pediatrics. 1986;77(3):322–329. | ||
Adam EK, Gunnar MR, Tanaka A. Adult attachment, parent emotion, and observed parenting behavior: mediator and moderator models. Child Dev. 2004;75(1):110–122. | ||
Jaffa T, Scott S, Hendriks JH, Shapiro CM. ABC of sleep disorders. Sleep disorders in children. BMJ. 1993;306(6878):640–643. | ||
Matricciani LA, Olds TS, Blunden S, Rigney G, Williams MT. Never enough sleep: a brief history of sleep recommendations for children. Pediatrics. 2012;129(3):548–556. | ||
Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s sleep time duration recommendations: methodology and results summary. Sleep Heal. 2015;1(1):40–43. | ||
Mindell JA, Sadeh A, Wiegand B, How TH, Goh DY. Cross-cultural differences in infant and toddler sleep. Sleep Med. 2010;11(3):274–280. | ||
Rechtschaffen A, Kales A. A Manual of Standardized Terminology, Techniques and Scoring System for Sleep Stages of Human Subjects. Washington, DC: Public Health Service, US Government Printing Office; 1968. | ||
Cirelli C, Tononi G. Is sleep essential? PLoS Biol. 2008;6(8):e216. | ||
Tarullo AR, Balsam PD, Fifer WP. Sleep and infant learning. Infant Child Dev. 2011;20(1):35–46. | ||
Gruber R, Laviolette R, Deluca P, Monson E, Cornish K, Carrier J. Short sleep duration is associated with poor performance on IQ measures in healthy school-age children. Sleep Med. 2010;11(3):289–294. | ||
Paavonen EJ, Räikkönen K, Pesonen AK, et al. Sleep quality and cognitive performance in 8-year-old children. Sleep Med. 2010;11(4):386–392. | ||
Touchette É, Petit D, Séguin J, Boivin M, Tremblay RE, Montplaisir JY. Associations between sleep duration patterns and behavioral/cognitive functioning at school entry. Sleep. 2007;30(9):1213–1219. | ||
Sadeh A, Gruber R, Raviv A. The effects of sleep restriction and extension on school-age children: what a difference an hour makes. Child Dev. 2003;74(2):444–455. | ||
Stickgold R, Walker MP. Sleep-dependent memory consolidation and reconsolidation. Sleep Med. 2007;8(4):331–343. | ||
Stickgold R, Walker MP. Memory consolidation and reconsolidation: what is the role of sleep? Trends Neurosci. 2005;28(8):408–415. | ||
Rasch B, Born J. About sleep’s role in memory. Physiol Rev. 2013;93(2):681–766. | ||
Seehagen S, Konrad C, Herbert JS, Schneider S. Timely sleep facilitates declarative memory consolidation in infants. Proc Natl Acad Sci U S A. 2015;112(5):1625–1629. | ||
Gómez RL, Bootzin RR, Nadel L. Naps promote abstraction in language-learning infants. Psychol Sci. 2006;17(8):670–674. | ||
Hupbach A, Gomez RL, Bootzin RR, Nadel L. Nap-dependent learning in infants. Dev Sci. 2009;12(6):1007–1012. | ||
Horváth K, Myers K, Foster R, Plunkett K. Napping facilitates word learning in early lexical development. J Sleep Res. 2015;24(5):503–509. | ||
Gomez RL, Newman-Smith KC, Breslin JH, Bootzin RR. Learning, memory, and sleep in children. Sleep Med Clin. 2011;6(1):45–57. | ||
van Dongen EV, Thielen JW, Takashima A, Barth M, Fernández G. Sleep supports selective retention of associative memories based on relevance for future utilization. PLoS One. 2012;7(8):e43426. | ||
Wilhelm I, Diekelmann S, Molzow I, Ayoub A, Mölle M, Born J. Sleep selectively enhances memory expected to be of future relevance. J Neurosci. 2011;31(5):1563–1569. | ||
Goldfield BA, Reznick JS. Early lexical acquisition: rate, content, and the vocabulary spurt. J Child Lang. 1990;17(1):171–183. | ||
Lukowski AF, Milojevich HM. Sleeping like a baby: examining relations between habitual infant sleep, recall memory, and generalization across cues at 10 months. Infant Behav Dev. 2013;36(3):369–376. | ||
Scher A. Infant sleep at 10 months of age as a window to cognitive development. Early Hum Dev. 2005;81(3):289–292. | ||
Gibson R, Elder D, Gander P. Actigraphic sleep and developmental progress of one-year-old infants. Sleep Biol Rhythms. 2012;10(2):77–83. | ||
Bernier A, Bélanger MÈ, Tarabulsy GM, Simard V, Carrier J. My mother is sensitive, but I am too tired to know: infant sleep as a moderator of prospective relations between maternal sensitivity and infant outcomes. Infant Behav Dev. 2014;37(4):682–694. | ||
Bernier A, Beauchamp MH, Bouvette-Turcot AA, Carlson SM, Carrier J. Sleep and cognition in preschool years: specific links to executive functioning. Child Dev. 2013;84(5):1542–1553. | ||
Bernier A, Carlson SM, Bordeleau S, Carrier J. Relations between physiological and cognitive regulatory systems: infant sleep regulation and subsequent executive functioning. Child Dev. 2010;81(6):1739–1752. | ||
Sheridan A, Murray L, Cooper PJ, Evangeli M, Byram V, Halligan SL. A longitudinal study of child sleep in high and low risk families: relationship to early maternal settling strategies and child psychological functioning. Sleep Med. 2013;14(3):266–273. | ||
Taveras EM, Rifas-Shiman SL, Oken E, Gunderson EP, Gillman MW. Short sleep duration in infancy and risk of childhood overweight. Arch Pediatr Adolesc Med. 2008;162(4):305–311. | ||
Gillman MW, Rifas-Shiman SL, Kleinman K, Oken E, Rich-Edwards JW, Taveras EM. Developmental origins of childhood overweight: potential public health impact. Obesity (Silver Spring). 2008;16(7):1651–1656. | ||
Zhou Y, Aris IM, Tan SS, et al. Sleep duration and growth outcomes across the first two years of life in the GUSTO study. Sleep Med. 2015;16(10):1281–1286. | ||
Tikotzky L, DE Marcas G, Har-Toov J, Dollberg S, Bar-Haim Y, Sadeh A. Sleep and physical growth in infants during the first 6 months. J Sleep Res. 2010;19(1 Pt 1):103–110. | ||
Worobey J, Peña J, Ramos I, Espinosa C. Infant difficulty and early weight gain: does fussing promote overfeeding? Matern Child Nutr. 2014;10(2):295–303. | ||
Fairley L, Santorelli G, Lawlor DA, et al. The relationship between early life modifiable risk factors for childhood obesity, ethnicity and body mass index at age 3 years: findings from the Born in Bradford birth cohort study. BMC Obes. 2015;2:9. | ||
Taveras EM, Gillman MW, Peña MM, Redline S, Rifas-Shiman SL. Chronic sleep curtailment and adiposity. Pediatrics. 2014;133(6):1013–1022. | ||
Fisher A, McDonald L, van Jaarsveld CH, et al. Sleep and energy intake in early childhood. Int J Obes (Lond). 2014;38(7):926–929. | ||
Paul IM, Savage JS, Anzman SL, et al. Preventing obesity during infancy: a pilot study. Obesity (Silver Spring). 2011;19(2):353–361. | ||
Paul IM, Williams JS, Anzman-Frasca S, et al. The Intervention Nurses Start Infants Growing on Healthy Trajectories (INSIGHT) study. BMC Pediatr. 2014;14(1):184. | ||
Wake M, Price A, Clifford S, Ukoumunne OC, Hiscock H. Does an intervention that improves infant sleep also improve overweight at age 6? Follow-up of a randomised trial. Arch Dis Child. 2011;96(6):526–532. | ||
Nedeltcheva AV, Kessler L, Imperial J, Penev PD. Exposure to recurrent sleep restriction in the setting of high caloric intake and physical inactivity results in increased insulin resistance and reduced glucose tolerance. J Clin Endocrinol Metab. 2009;94(9):3242–3250. | ||
Spiegel K, Leproult R, Van Cauter E. Impact of sleep debt on metabolic and endocrine function. Lancet. 1999;354(9188):1435–1439. | ||
Spiegel K, Tasali E, Penev P, Van Cauter E. Brief comunication: sleep curtailment in healthy young men is associated with decreased leptin levels, elevated ghrelin levels, and increased hunger and appetite. Ann Intern Med. 2004;141(11):846–850. | ||
Asarnow LD, McGlinchey E, Harvey AG. Evidence for a possible link between bedtime and change in body mass index. Sleep. 2015;38(10):1523–1527. | ||
Lampl M, Johnson ML. Infant growth in length follows prolonged sleep and increased naps. Sleep. 2011;34(5):641–650. | ||
Evsyukova II, Koval’chuk-Kovalevskaya OV, Maslyanyuk NA, Dodkhoev DS. Features of cyclic sleep organization and melatonin production in full-term newborns with intrauterine growth retardation. Hum Physiol. 2013;39(6):617–624. | ||
Sriram B, Mencer MA, McKelvey S, et al. Differences in the sleep states of IUGR and low-risk fetuses: an MCG study. Early Hum Dev. 2013;89(10):815–819. | ||
Yiallourou SR, Wallace EM, Miller SL, Horne RS. Effects of intrauterine growth restriction on sleep and the cardiovascular system: the use of melatonin as a potential therapy? Sleep Med Rev. 2015;26:64–73. | ||
Leitner Y, Bloch AM, Sadeh A, et al. Sleep-wake patterns in children with intrauterine growth retardation. J Child Neurol. 2002;17(12):872–876. | ||
Kordas K, Siegel EH, Olney DK, et al. Maternal reports of sleep in 6–18 month-old infants from Nepal and Zanzibar: association with iron deficiency anemia and stunting. Early Hum Dev. 2008;84(6):389–398. | ||
González-Ortiz M, Martínez-Abundis E. Impact of sleep deprivation on insulin secretion, insulin sensitivity, and other hormonal regulations. Metab Syndr Relat Disord. 2005;3(1):3–7. | ||
Cornblath M, Parker ML, Reisner SH, Forbes AE, Daughaday WH. Secretion and metabolism of growth hormone in premature and full-term infants1. J Clin Endocrinol Metab. 1965;25(2):209–218. | ||
Kim TW, Jeong JH, Hong SC. The impact of sleep and circadian disturbance on hormones and metabolism. Int J Endocrinol. 2015;2015:1–9. | ||
Salzarulo P, Fagioli I. Sleep for development or development for waking? – some speculations from a human perspective. Behav Brain Res. 1995;69(1–2):23–27. | ||
Verrillo E, Bizzarri C, Bruni O, et al. Effects of replacement therapy on sleep architecture in children with growth hormone deficiency. Sleep Med. 2012;13(5):496–502. | ||
Küpers LK, L’Abée C, Bocca G, Stolk RP, Sauer PJJ, Corpeleijn E. Determinants of weight gain during the first two years of life—the GECKO Drenthe birth cohort. PLoS One. 2015;10(7):e0133326. | ||
Hibbs AM, Storfer-Isser A, Rosen C, Ievers-Landis CE, Taveras EM, Redline S. Advanced sleep phase in adolescents born preterm. Behav Sleep Med. 2014;12(5):412–424. | ||
Hart CN, Cairns A, Jelalian E. Sleep and obesity in children and adolescents. Pediatr Clin North Am. 2011;58(3):715–733. | ||
Taumann R. Sleep and obesity in children. In: Preedy VR, Patel VB, Le LA, editors. Handbook of Nutrition, Diet and Sleep. Wageningen: Wageningen Academic Publishers; 2013. | ||
Kopasz M, Loessl B, Hornyak M, et al. Sleep and memory in healthy children and adolescents – a critical review. Sleep Med Rev. 2010;14(3):167–177. | ||
Sivertsen B, Harvey AG, Reichborn-Kjennerud T, Torgersen L, Ystrom E, Hysing M. Later emotional and behavioral problems associated with sleep problems in toddlers: a longitudinal study. JAMA Pediatr. 2015;169(6):575–582. | ||
Paavonen EJ, Porkka-Heiskanen T, Lahikainen AR. Sleep quality, duration and behavioral symptoms among 5–6-year-old children. Eur Child Adolesc Psychiatry. 2009;18(12):747–754. | ||
Stein MA, Mendelsohn J, Obermeyer WH, Amromin J, Benca R. Sleep and behavior problems in school-aged children. Pediatrics. 2001;107(4):E60. | ||
Hyde M, O’Driscoll DM, Binette S, et al. Validation of actigraphy for determining sleep and wake in children with sleep disordered breathing. J Sleep Res. 2007;16(2):213–216. | ||
Markovich AN, Gendron MA, Corkum PV. Validating the Children’s Sleep Habits Questionnaire against polysomnography and actigraphy in school-aged children. Front Psychiatry. 2015;5:188. | ||
Gertner S, Greenbaum CW, Sadeh A, Dolfin Z, Sirota L, Ben-Nun Y. Sleep–wake patterns in preterm infants and 6 month’s home environment: implications for early cognitive development. Early Hum Dev. 2002;68(2):93–102. | ||
Sadeh A. A brief screening questionnaire for infant sleep problems: validation and findings for an internet sample. Pediatrics. 2004;113(6):e570–e577. | ||
Field T. Prenatal depression effects on early development: a review. Infant Behav Dev. 2011;34(1):1–14. | ||
Pesonen AK, Räikkönen K, Paavonen EJ, et al. Sleep duration and regularity are associated with behavioral problems in 8-year-old children. Int J Behav Med. 2010;17(4):298–305. | ||
Piteo AM, Kennedy JD, Roberts RM, et al. Snoring and cognitive development in infancy. Sleep Med. 2011;12(10):981–987. | ||
Piteo AM, Lushington K, Roberts RM, et al. Parental-reported snoring from the first month of life and cognitive development at 12 months of age. Sleep Med. 2011;12(10):975–980. | ||
Montgomery-Downs HE, Gozal D. Snore-associated sleep fragmentation in infancy: mental development effects and contribution of secondhand cigarette smoke exposure. Pediatrics. 2006;117(3):e496–e502. | ||
Smith CB, Walker K, Badawi N, Waters KA, MacLean JE. Impact of sleep and breathing in infancy on outcomes at three years of age for children with cleft lip and/or palate. Sleep. 2014;37(5):919–925. | ||
España RA, Scammell TE. Sleep neurobiology from a clinical perspective. Sleep. 2011;34(7):845–858. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.