Back to Journals » Nutrition and Dietary Supplements » Volume 13
Infant and Young Child Feeding Practice Status and Its Determinants in Kalu District, Northeast Ethiopia: Community-Based Cross-Sectional Study
Authors Hassen SL ![]() , Temesgen MM
, Temesgen MM ![]() , Marefiaw TA
, Marefiaw TA ![]() , Ayalew BS
, Ayalew BS ![]() , Abebe DD
, Abebe DD ![]() , Desalegn SA
, Desalegn SA
Received 7 December 2020
Accepted for publication 26 February 2021
Published 29 March 2021 Volume 2021:13 Pages 67—81
DOI https://doi.org/10.2147/NDS.S294230
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gary Johanning
Seid Legesse Hassen,1 Minwuyelet Maru Temesgen,1,* Tefera Alemu Marefiaw,2,* Birtukan Shiferaw Ayalew,1,* Daniel Dagne Abebe,3,* Seid Ali Desalegn3,*
1Amhara Public Health Institute, Research and Technology Transfer Directorate, Dessie Branch, Dessie, Ethiopia; 2Amhara Public Health Institute, Bahir Dar Headquarters, Bahir Dar, Ethiopia; 3Amhara Public Health Institute, Laboratory Directorate, Dessie Branch, Dessie, Ethiopia
*These authors contributed equally to this work
Correspondence: Seid Legesse Hassen
Amhara Public Health Institute, Research and Technology Transfer Directorate, Dessie Branch, P.O. Box 686, Dessie, Ethiopia
Tel +251 913645489
Email [email protected]
Background: Appropriate nutrition during infancy and early childhood is a cornerstone of care for ensuring optimal child growth and development during the first 2 years of life. Globally, about 40% of under two years of age deaths are attributed to inappropriate infant and young child feeding practices. In Ethiopia, a large range of inappropriate feeding practices of mothers during infancy and early childhood were documented. This study aims to assess infant and young child feeding practice status and its determinants among mothers of children aged 6– 23 months in Kalu district, Northeast Ethiopia.
Methods: Community-based cross-sectional study design was applied from May 1– 30/2019. A total of 605 mothers–children pair’s 6– 23 months were included in the study using multi-stage sampling followed by a simple random sampling technique. Data were collected using a pretested semi-structured interviewer-administered questionnaire. Bi-variate and multivariable logistic regression were used to assess determinants associated with child feeding practices. Statistical significance was decided at p-value less than 0.05.
Results: Of six hundred five (605) sampled mothers having an infant and young child age 6– 23 months, 589 were successfully included in the study making a response rate of 97.35%. In our study, the overall proportion of appropriate infant and young child feeding practices was 57.7%. Place of delivery (AOR=1.977; 95% Cl (1.101, 3.552)), mothers’ age being 25– 35 years (AOR =2.091; 95% Cl: (1.452, 3.011)) and family size > 4 members (AOR=1.873; 95% CI: (1.311, 2.675)) were determinants positively associated with appropriate infant and young child feeding practices in Kalu district at 95% CI.
Conclusion: The overall appropriate infant and young child feeding practices were better in general in Kalu district. However, this prevalence is not acceptable to ensure good health and better nutritional status of children. As a result, intervention initiatives should focus on institution delivery services that are crucial to implementing appropriate infant and young child feeding practice. Health facilities need to be strengthened and fully utilized to provide high-quality feeding counseling. Special attention needs to be given to younger mothers, in addition to increasing institution delivery service.
Keywords: infant and young child feeding, practice, Kalu district, Ethiopia
Introduction
Appropriate feeding practice during infancy and early childhood is a cornerstone of care for ensuring optimal child growth and development during the first 2 years of life, as this period is the “critical window” for the promotion of health, good growth, behavioral, cognitive development and overall well-being in early vulnerable years of life.1 Inappropriate feeding practices in these window periods are a major cause of childhood under nutrition.2–4 The potential negative impact of under nutrition during this critical period also has long-lasting and irreversible consequences, including growth failure, poor resistance to infections, impaired learning capabilities and diminishes the individual level of productivity during adulthood.5 Furthermore, negatively affecting the future social and economic development of countries6 and leading the vicious cycle of intergenerational malnutrition.7
Globally, about 40% of under two years of deaths are associated with poor feeding practices.8 In developing countries, approximately 25–50% of infant mortality is attributed to inappropriate infant and young child feeding (IYCF) practices.9,10 About two-third of malnutrition associated mortality with inappropriate feeding practices during the first year of life.11 Every day, 3 to 4 thousand infants die in the low-income countries from diarrhea and acute respiratory infections because they are given inadequate amounts of breast milk. A major contributor to their deaths is poor breastfeeding practices.12 Optimal breastfeeding and appropriate complementary feeding could prevent 13% and 6% under-five mortality, respectively.13 Other contemporary studies in Ethiopia, Ghana, Bolivia, and Madagascar have shown that optimal breastfeeding prevents 20–22% of neonatal deaths.10,14,15 Child malnutrition causes approximately 2.7 million deaths per year, 156 million stunting, and 50 million wastings.16
In Ethiopia, a large range of inappropriate IYCF practices was documented. The Central Statistical Agency (CSA) 2016 report indicated that the neonatal mortality rate in Ethiopia accounts for 43% of under 5 mortality.17 Poor feeding practices and their consequences, therefore, are a major threat to sustainable socio-economic development and poverty reduction as they are among the most serious obstacles to attaining and maintaining the health of this important age group. Governments would be unsuccessful in their efforts to hasten economic development in any significant long-term sense until optimal child growth and development, particularly through appropriate feeding practices, are ensured.18
Achieving optimum IYCF practices is a major challenge in developing and developed countries. To optimize global IYCF practices, World health organization (WHO) and United Nations Children’s Fund (UNICEF) put a universal strategy for appropriate IYCF practices.19 This strategy recommends early initiation of breastfeeding within an hour of birth, exclusive breastfeeding under 6 months (EBF), subsequent to timely introduction of solid, semi-solid and soft foods, minimum dietary diversity (MDD), meal frequency (MF), and minimum acceptable diet, consumption of iron-rich food or iron-fortified foods alongside with continued breastfeeding at 2 years and beyond. Therefore, Improving IYCF practice particularly for children younger than 2 years of age should be a high worldwide priority.20,21
The government of Ethiopia has also developed and implemented the IYCF guideline in 2004 to enhance child feeding practice, training health extension workers, developing and revising procedural manuals for implementing the community integrated management of childhood illnesses (IMNCI), and adopted a Baby-friendly Hospital Initiative program.22–24 However, these efforts have unsuccessful to bring about substantive and sustainable changes leading to the improvement of IYCF practices.3 According to 2016 Ethiopian Demographic and Health Survey (EDHS), IYCF practice is not as suggested by WHO. Only 45% of infants 6–24 months of age received minimum meal frequency, 58% infants of <6 months of age are exclusive breastfeeding (EBF) and Contrary to the WHO recommendation. Nine percent of infants <6 months of age use a bottle with a teat, a practice that is discouraged because of the risk of illness to the child.25 There are fewer studies from the Ethiopian scenario related to IYCF practices that have revealed the appropriateness of breast and complementary feeding practices.26–28 but it was also advisable that time-to-time assessment to find out the improvement in the feeding practices of IYC and keeping in view this concept for study has been planned.
Methods
The study was done in Kalu district. Which is located in the south wollo zone of the Amhara national regional state, Ethiopia. It is situated at 375 kilometers (km) far from capital city of Ethiopia (Adis Ababa). The administrative center for this district is Kombolcha; other towns in Kalu include Harbu, Ancharo, Gerba, and Degan. There are three agro-ecological zones (high, middle and low land) in the district in a range between 800 meters above sea level in the lowlands bordering the Oromia Zone and 1750 m at the foot of the mountains north of Kombolcha. The district is the first ranked populated among the twenty-three districts in the south wollo zone. It is administratively subdivided into five urban and thirty-five rural kebeles (the smallest administration unit) with an estimated total population size of about 231,087 according to the 2018 district-based census. Of which 117,162 were females and 113,925 were male. Kaludistrict has a population density of 218.64, which is greater than the Zone average of 147.58 persons per square kilometer. Estimated 41,627 households were counted in the district, resulting an average of 4.47 persons to a household, and the number of children aged 6 to 23 months is 11,670 (5.05%) (District health office report 2019). Currently, nine health centers and thirty-three health posts are provided that health services access to the community. The major livelihood of the district population is based on diverse farming, crop and livestock production. The major crops cultivated in the district include both rain-fed and irrigated crops, namely, maize, millet, teff, fruits, and vegetables.29
A community-based cross-sectional study design was applied from May 1–30/2019. Source populations for this study were all mothers or caregivers having an IYC aged 6 to 23 months living in the district and randomly selected mothers who had children age 6–23 months old living in the study area for more than six months were included in the study.
The sample size was determined using Epi-info version 7.2, by considering the following assumption; the proportion of appropriate IYCF practices 50% in the study area since there is no study showing the prevalence of appropriate IYCF practices, 95% level of confidence (CI), marginal error of 5% and 5% non-responsive rate. Using 1.5 design effect the final sample size was 605.
A stratified sampling technique was carried out to select kebeles in the district, firstly; the district was stratified to urban and rural kebeles. Ten rural and two urban kebeles were selected using simple random sampling among a total of forty.
To select each household from the selected kebeles, the first sampling frame was done, that the household had children aged 6–24 months old were identified with help of community-based demographic and health information registration prepared by health extension workers. Finally, the number of households was proportionally allocated to each selected kebeles according to their population proportion to size allocation technique that was used in the determination of the number of study units included in each selected kebeles.
IYCF practices were assessed by using eight-core WHO feeding practice indicators to estimate the appropriateness of IYCF practices.30 However, the WHO guidelines on IYCF practices do not provide the baseline or minimum standard that needs to be reached nor what percentage should be considered alarming for public health importance.18 Logically, all children 0–23 months should meet the recommended feeding practices. To appreciate the similarities and differences of the prevalence and determinants of IYCF practice in logistic regression with other studies are difficult due to the lack of study on IYCF practices in the composite of similar indicators. This study’s findings were discussed based on the individual components of IYCF.
Despite this limitation used to construct scores, we tried to discuss the prevalence and its determinants with IYCF practice by considering eight core indicators for appropriate IYCF practice (if the study subject use 50% or above (≥4) of the 8 core WHO IYCF indicators). Which includes EBF, early initiation of breastfeeding, continued breastfeeding at one year, introduction of soft or semi-solid and solid foods at 6 to 8 months, Minimum meal frequency (MMF), Minimum dietary diversity (MDD), minimum acceptable diet and consumption of iron-rich or iron-fortified foods.
A semi-structured interviewer-administered questionnaire was carried out to collect data. The questioners composed of socio-demographic and household composed of socio-demographic and household character, maternal health care service utilization character and behavioral-related variables (knowledge and attitude of the mothers) on IYCF practice. It was adapted from different literatures and guidelines. The questionnaire was first translated from English to native language of the study area (Amharic), and it was retranslated back to English by an expert who is fluent in both languages to maintain its consistency. Twelve professional nurses as data collectors and two public health officers as field supervisors were recruited for the study. Data enumerators and supervisors were trained for two days. The pretest was done in similar settings but not included in the main study of 5% of the sample size. In order to assure the quality of data principal investigators and supervisors were closely checked data collection techniques on daily bases reviewed for its completeness. They also checked the activities of each data collector by random spot-checking of the households to ensure the reliability of the data. Any error, ambiguity, incompleteness, or any other problems were addressed on the following day before starting the next day's activities.
All mothers/caregivers who have children aged 6 to 23 months who lived in the study area for more than 6 months were included in the study. Those mothers who are unable to communicate due to serious illness at the time of data collection and those children having any illness 15 days before the survey were excluded from the study because they affect feeding practices during data collection. In the case of, mothers with multiple children, one child was selected randomly using the lottery method.
Data were entered into Epi data version 3.1 and exported to SPSS version21 statistical software for analysis. Further, data cleaning (editing, recording, checking for missing values, and outliers) was made after exported to SPSS. Descriptive analysis was used to see frequency, proportion, mean and standard deviation. The proportion of recommended IYCF practices was reported as a percentage. Binary logistic regression was used to assess significant factors of the outcome variable. Variables with p-value <20 were taken as a cut-off point to select eligible variables for the multiple logistic regression analysis and p-value less than 0.05 was considered as statically significant in the final model.
Operational and Standard Definition
- Appropriate IYCF practice: Defined as eight-core WHO recommended practices were considered as appropriate if the summed score of all the eight indicators is 4 or above. Otherwise, an inappropriate practice, if the summed score of the indicators is <4.22,31,32
- Infant and young child: age of children 0–23 months.
- Exclusive breastfeeding under 6 months: proportion of infant under 6 months of age who receives only breast milk and no other liquids or solids, not even water apart from drops or syrups consisting of vitamins, mineral supplements, or medicines.
- Pre-lacteal feeding: Proportion of infants given something other than breast milk during the few days of delivery.
- Timely introduction of solid, semi-solid and soft foods: Proportion of infants who received solid, semi-solid and soft foods at 6–8 months of age in addition to breast milk or a breast milk substitute.
- Early initiation of breastfeeding within an hour of birth: proportion of infant is put to breastfeeding within one hour of delivery.
- Ever breast feeding: proportion of child who had received breastfeed at least once any before the survey.
- Consumption of iron-rich foods: proportion of children 6–23 months of age who received iron-rich or iron-fortified foods which are specially designed for infants.
- Minimum dietary diversity: Proportion of children 6–23 months of age who received four or more food groups from seven food groups with 24 hours of dietary recall.
- Minimum meal frequency: Proportion of children age 6 to 23 months who received minimum of three meals with 24 hours dietary recall.
- Minimum acceptable diet: composite indicators of minimum dietary diversity and meal frequency meet both minimum dietary diversity and meal frequency.
- Maternal knowledge on IYCF practice was measured by using twelve questions those respondents who score≥9 were taken to “high knowledge” 6–8 “medium knowledge” and <6 taken as “low knowledge”.
- Attitude towards IYCF practices was measured using 5 points Likert scale. There were a total of 8 questions assessing the attitude of mothers. The order of scoring statements was (strongly agree = 2, agree = 1, undecided = 0, disagree = −1, strongly disagree = −2) The total score was obtained and computed for means to categorize it into positive and negative attitudes. Score ≥mean was taken as “positive attitude”, while score < mean was taken as “negative attitude”.
Results
Socio-Demographic and Household Characteristics-Related Variables of the Child and Their Mothers
Of six hundred five (605) sampled mothers having an infant and young children age 0 to 23 months, 589 were successfully included in the study with the response rate of 97.35%. Almost 570 (96.8%) Biological mothers were involved as caregivers, while 19 (3.2%) were other caregivers such as grandmothers or sisters. The mean age of the infant and young child 14.1 months ± 5.140 (SD). A total of 220 (37.4%) were in the age range from 6 to 11 months and 369 (62.6%) were between 12 and 23 months. Of these 280 (47.5%) were male and 309 (52.5%) were female with male to a female sex ratio of 0.906. The mean age of mothers or caregivers was 27.1 (±5.89) years and nearly half of the 244 (41.4%) were in the age range of 25–35 years. Concerning the mother’s religion, almost all 575 (97.6%) mothers were Muslim. Of the total 414 (70.3%) were from rural residences, and 513 (87.1%) of the mothers were currently married (Table 1).
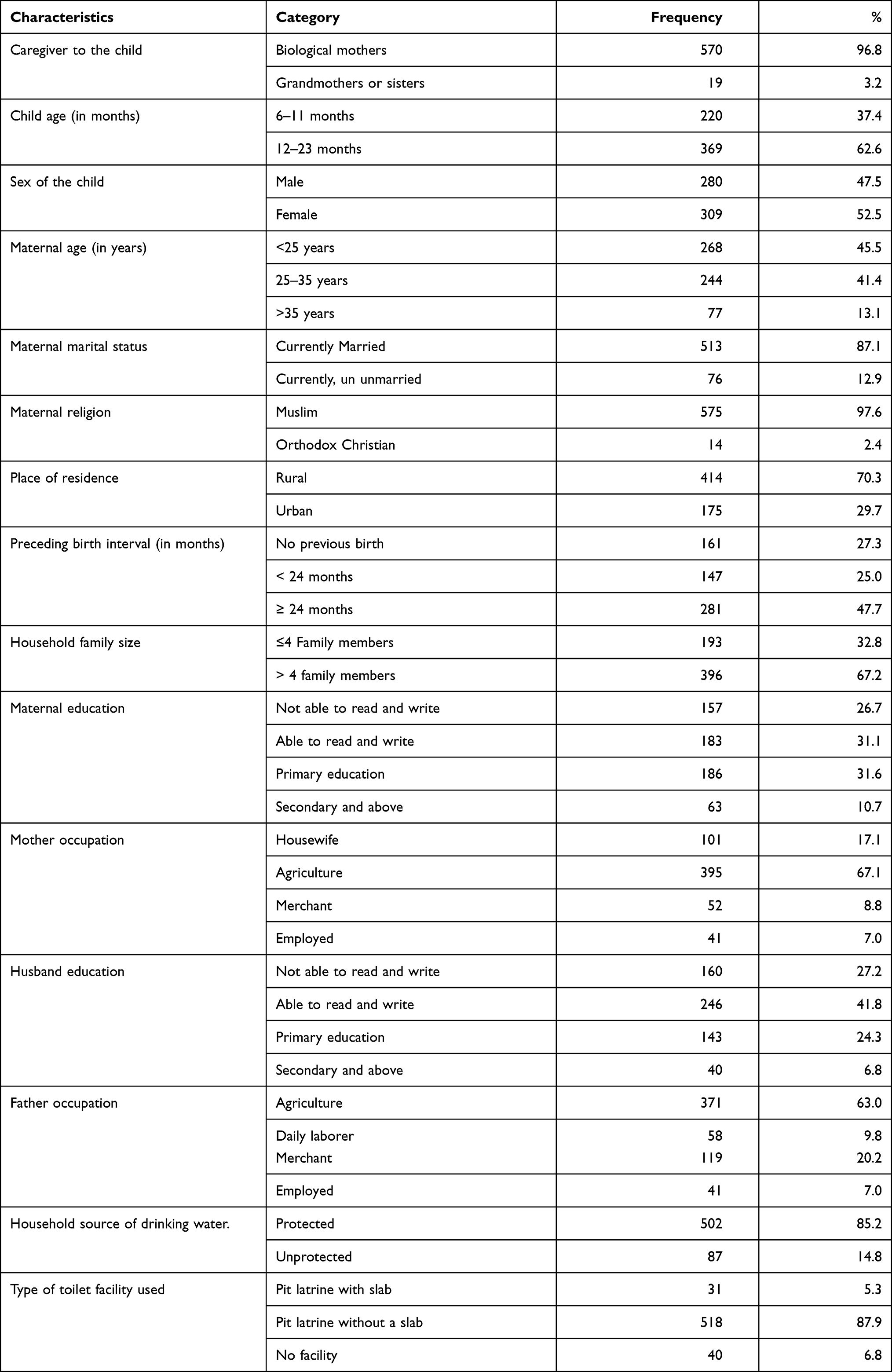 |
Table 1 Socio-Demographic and Household Characteristics of IYCF Practice in Kalu District, Northeast Ethiopia, 2019 (n=589) |
The mean (±SD) of family size was 4.5 (±1.53), and about 396 (67.2%) households had >4 family size. About 340 (57.72%) and 426 (72.3%), of the mothers and fathers, had no formal education, respectively. The majority of 395 (67.1%) of mothers were involved in agriculture while nearly 41 (7%) of mothers were employed. About 371 (63%) of fathers worked in the agricultural and only 41 (7%) of them in paid work. Regarding the household facilities, protected drinking water was available in 85.2% of the households while almost all of the households 549 (93.2%) used toilet facilities (Table 1).
Maternal Health Care Utilization and Maternal Practical Support-Related Determinants for IYCF Practices
Almost all, 93% of mothers attended antenatal care services (ANC) at least once during the last pregnancy. About (20%) had ANC follow-up greater than or equal to four times as recommended and only 41 (7%) had not ANC follow-up at all for their last pregnancy. About, 80.1% of mothers gave birth to their last child at a health facility and 19.9% of mothers delivered at home. Approximately 65% of mothers had received postnatal care (PNC) at least once and 35% had no PNC services. The majority of mothers 353 (59.9%) received counseling on IYCF practice during ANC and/or postnatal visits (Table 2).
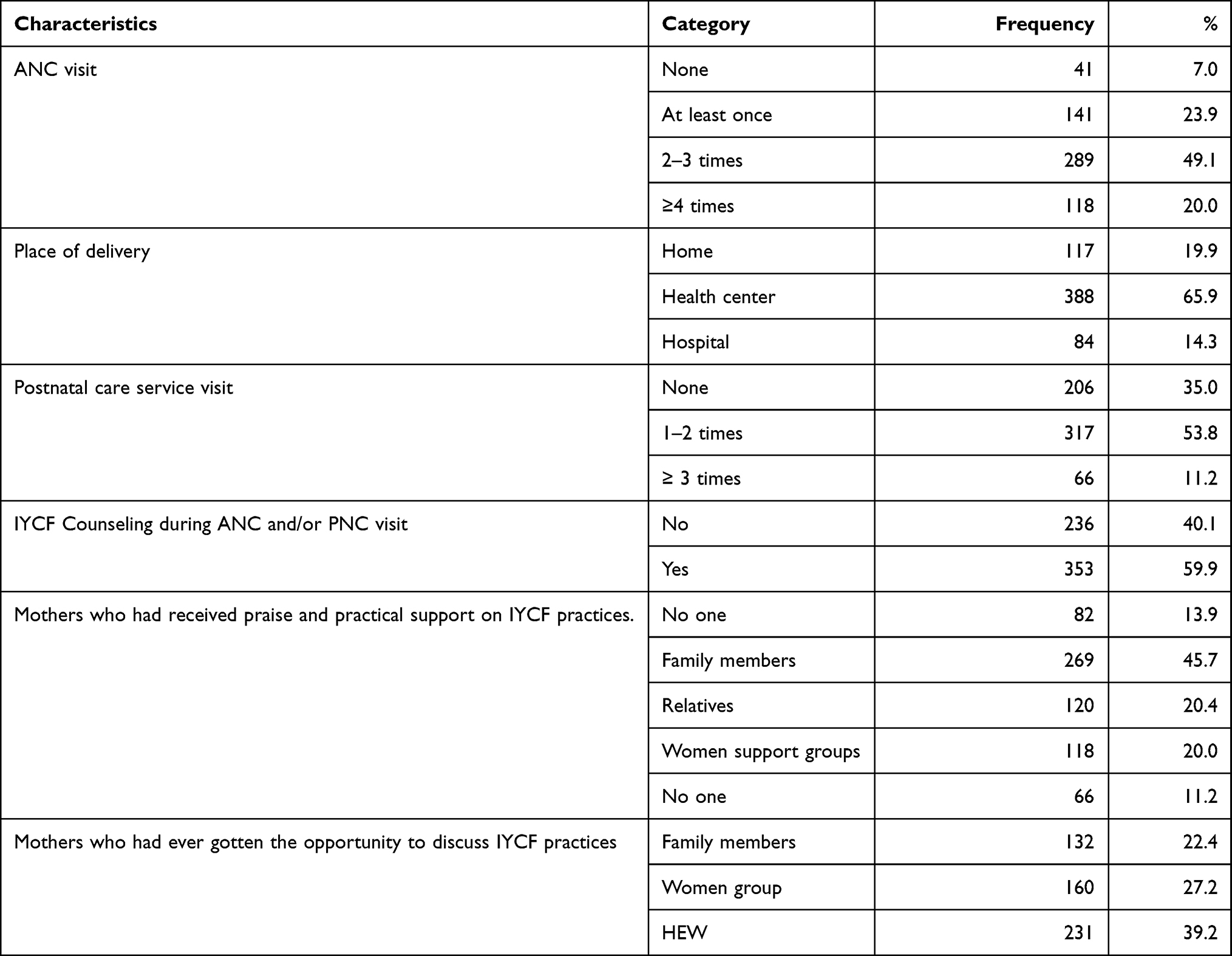 |
Table 2 Maternal Health Care Utilization and Maternal Practical Support-Related Determinants for IYCF in Kalu District, Northeast Ethiopia, 2019 (n=589) |
Nearly, 86.07% of mothers had received practical support for their IYCF practices and about 88.79% of mothers had gotten an opportunity to discuss with family members, health extension workers, and women supporting group (WSG) (Table 2).
Behavioral Determinants (Maternal Knowledge and Attitudes)
Among the study, 366 (62.1%) had medium knowledge of IYCF practice, only 187 (31.7%) of mothers were found to have high knowledge. The rest 36 (6.1%) mothers or caregivers had low knowledge. Among the study mothers, only 119 (20.2%) of the mothers found to have a positive attitude towards IYCF practice.
Prevalence of IYCF Practices by Using WHO Recommendations in Kalu District, Northeast Ethiopia, 2019
The result of this study showed that breastfeeding was practiced by almost all mothers. About 576 (97.8%) of the mothers reported that they had ever breastfed their children at least once before the survey and 453 (76.9%), had initiation of breastfeeding within one hour of delivery, but the rest one-third (23.1%) of mothers had started breastfeeding after one hour of birth. Around 88 (14.9%) had practiced pre-lacteal feeding during two to three days after delivery and out of this, they were swallowed sugar water 44 (50%), butter 23 (26.1%), and animal milk 20 (22.73%) respectively. As regards colostrums feeding, we found that 528 (89.6%) of all mothers had fed colostrums to their new-born babies, whereas 61 (10.4%) discarded colostrums. Reasons not fed colostrums, mothers who perceived cause of baby’s sickness (24.6%) and culturally dirty 75.4% (Table 3, Figure 1).
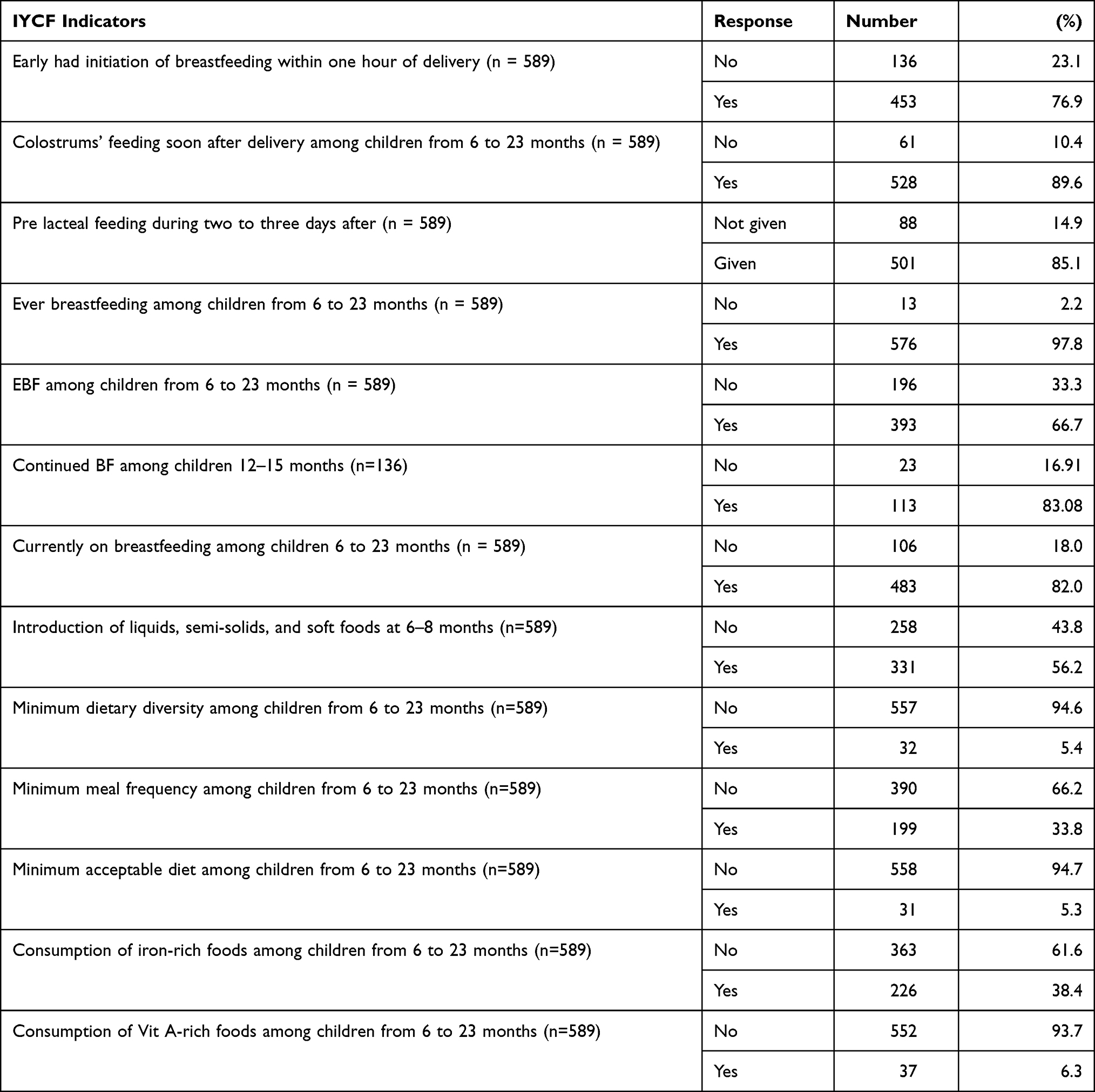 |
Table 3 Prevalence of IYCF Practice by Using WHO Recommendation in Kalu District, Northeast Ethiopia, 2019 (n=589) |
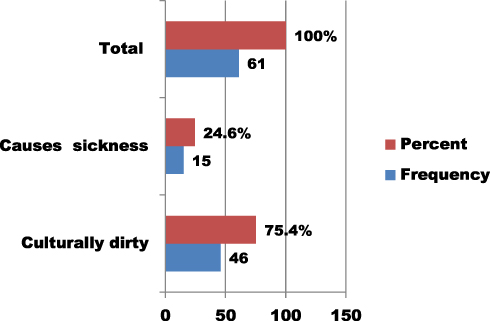 |
Figure 1 Reasons for mothers did not feed colostrums soon after delivery of IYCF practices in Kalu district, Northeast Ethiopia, 2019. |
Regarding EBF, 393 (66.7%) mothers, were exclusively breastfed to their child. Besides, 483 (82%) of the children of age less than 24 months were continued to breastfeed during the time of the survey, out of which 113 (83.08%) were 12–15 months old (Table 3).
The proportion of 331 (56.2%) of the mothers initiated liquids, semi-solids, and soft foods at 6–8 months of life, 199 (33.8%) received the recommended minimum meal frequency, and only 32 (5.4%) of children 6–23 months of age who received four or more food groups from seven food groups within 24 hours preceding the survey as per the recommendations. Cereal foods (porridge, rice, bread, kita firfir, potatoes, pasta, Seraphim, macaroni) were the most commonly consumed food items by children within the 24 hours preceding the survey, which accounts about 546 (92.7%). The second most frequently consumed food groups were pulses, legumes and nuts foods (Injera firfir/Shiro firfir) 330 (56%) followed by eggs 124 (21.1%). Fleshed foods 34 (5.8%) such as meat, poultry, fish, sea foods were not consumed/the least consumed food group by the children in the past 24 hours. The proportion of children 6–23 months of age who met a minimum acceptable diet was 31 (5.3%) and 558 (94.7%) did not meet the requirement. Nearly half 226 (38.4%) of the child consumed iron-rich foods in the last 24 hrs before the survey, whereas very smallest number 37 (6.3%) of children were consumed Vit A-rich foods (Table 3).
Determinants Associated with Appropriate IYCF Practices in Kalu District, Northeast Ethiopia, 2019
In the first Bivariate regression model, the age of the mother or caregivers, family size, maternal education, father education, father occupation, and place of delivery were identified as determinants associated with appropriate IYCF practices with p-value less than 20. However, in a multivariable logistic regression analysis, the age of the mother/caregivers, family size, and place of delivery were the only independent variables associated with IYCF practice. There was no significant association between other socio-demographic and household character, maternal health care service utilization and behavioral-related variables (knowledge and attitude of the mothers) with IYCF practice (Table 4).
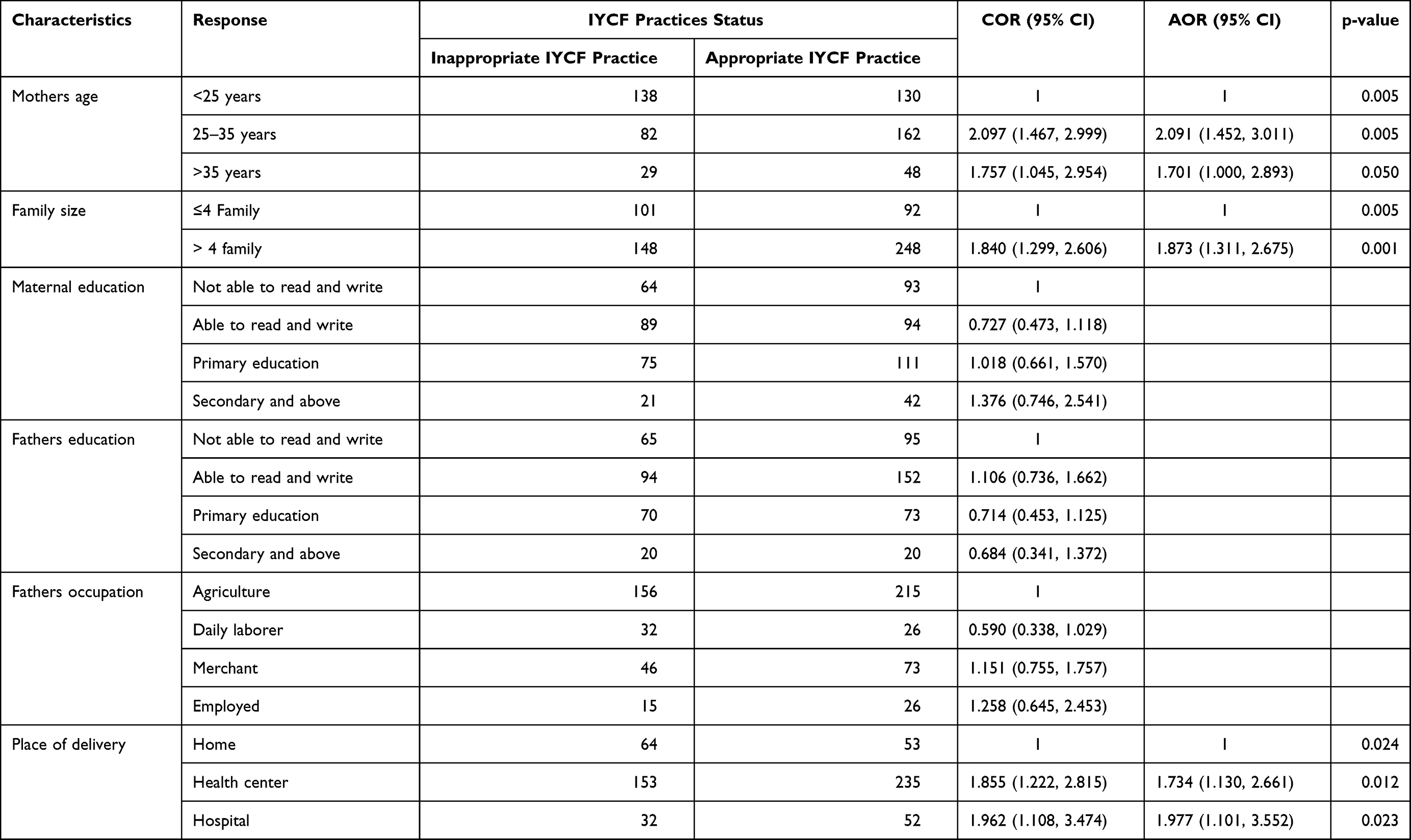 |
Table 4 Logistic Regression Analysis Output of Determinants Affecting Appropriate IYCF Practice Status in Kalu District, Northeast Ethiopia, 2019 (n=589) |
The results revealed that increased age of the mothers was significantly associated with better IYCF practice for their infant. As a result, mothers’ age being between 25 and 35 years was 2.091 times more likely to have IYCF practice than those mothers’ age less than 25 years (AOR = 2.091; 95% CI: (1.452, 3.011)). The odds of IYC feeding practice were 1.757 times more likely among mothers aged >35 years than those aged <25 years (AOR=1.757; 95% CI: (1.045, 2.954)) (Table 4).
Household family size was another factor significantly associated with appropriate IYCF practices. Mothers with >4 family size at household 1.873 times more likely to have appropriate IYCF practice compared with women with 1–4 family size (AOR =1.873; 95% Cl: (1.311, 2.675)) (Table 4).
Mothers who gave birth at health center were 1.734 times more likely to have appropriate IYCF practice than mothers who gave birth at home (AOR =1.734; 95% CI: (1.130, 2.661)). This also extends to mothers who delivered at the hospital level were significantly associated with IYCF feeding performance (AOR=1.977; 95% CI: (1.101, 3.552)) (Table 4).
Discussion
This study was designed to assess IYCF practice status and its determinants among children aged 6 to 23 months in Kalu district, northeast Ethiopia. In our study, the prevalence of appropriate IYCF practice was found to be 57.7%.
In our study finding showed that the prevalence of appropriate IYCF practice was much better than the study conducted in Bahir Dar city (7%),26 Assayita (9.2%),28 and Shashemene which was 32.1%.27 As indicated in the results of our study, around 80.1% % of mothers received delivery services at health facility. This implies a potential to deliver child feeding recommendations through counseling of mothers.
This better rate of IYCF practice within the study could be due to increasing community awareness, increasing potential, and accessibility of health information at the result of community-based women development army promoting the importance of the appropriate IYCF practices in the community level and one to five network meeting and mother support group forum.17,33 Moreover, the role of provincial difference between study highlights, the content of services received and the kind of information puts to mothers during their delivery health facility are relevant to the subsequent child feeding pattern in the local contexts.34 Other possible reasons can be the time gap between studies, ie, the past local study was carried out over five years ago. Furthermore, it could also be due to socioeconomic, variations in study settings, sample size consideration, and time gap among studies. This study showed the proportion of ever breastfed was 97.8%. This was nearly almost like to the study conducted in Mekelle city 98.9%35 and Shshemene which was 99.3%.27 This high rate of breastfeeding within the study area may could also be due to the truth that breastfeeding practice is common and normal in society.
Even though WHO Global and National IYCF Guidelines recommend that the mothers should start breastfeeding the newborn immediately within the few hours after delivery, our study revealed that 76.9% of the study mothers initiated breastfeeding within an hour of birth, which was almost like the study conducted in Mekelle 78%34 and Asela 86.3%.36 But it is higher than another recent study conducted in Jimma Arjo district, 62.6%,37 Debre Berhan town, 62.6%,38 and Ethiopia national figure 73% 17. Could be attributed to the very fact that the bulk 472 (80.13%) of the mothers had born at a health institution, which creates an honest.
The difference could be attributed to the very fact that the majority 472 (80.13%) of the mothers had born at a health institution, which creates the chance for health professionals to promote the initiation of breastfeeding within an hour of birth and better performance within the study area. Furthermore, may be due to the tine between studies in Ethiopia.
Our study finding revealed that 528 (89.6%) mothers gave colostrums to their infants; This finding was found to be high as compared to other findings from Raya Kobo district (86.5%),39 Debre Markos, 62.7%40 and far higher than Karachi Pakistan 48.8%.41 This result could also be justified that within the study area mothers fed colostrums as they considered that it encourages disease protection 210 (39.8%), nutritive value 125 (23.7%), and culturally beneficial 193 (36.6%). Furthermore, could be due to increasing community awareness, increasing potential, and accessibility of health coverage.
In this study, the pre-lacteal feed was observed to 14.8% of the studied children, which was less than a previous study conducted in Raya kobo, Ethiopia (38.8% %),42 and from Delhi state (45.7%),43 but, higher than national EDHS report in 2016 (8%).17 This might be due to the accessibility of information in recent times. Although this practice is prevalent across the cultures, there is an international consensus that providing other liquids in addition to breast milk in the first 6 months of life is unnecessary and harmful.
As WHO recommended that EBF for 6 months of age as the major component of feeding practices, in our study, the EBF under six months was 66.7%, which is lower than the WHO recommendation of 90%.44 This finding also almost meets with the national Health Sector Development plan that had shown 70% by the end of 2020,22 however, it was lower than the previous studies conducted in Bahir Dar City (83%),26 Shashemene (87.8%).27 On the other hand, the rate of EBF practice was somewhat better compared to the previously documented result in the national prevalence reported in the EDHS 2016 (58%),17 Mekelle city (60.8%)35 and other Asian countries like north India (51.3%)43 and Pakistan (37%).41 The most common reasons for not giving EBF were not having enough breast milk 114 (58.16%), mother sickness 32 (16.33%), and time to stop/pregnancy 50 (25.5%). Another possible explanation for this difference could be due to sample size, and method of data collection, Socio-demographic determinants, environmental condition, human Cultural Behaviors, awareness of mother, commitments of health extension worker.
As per the finding of this study about 113 (83.08%) mothers have continued breastfeeding their children at age one year. This result is nearly similar to a study conducted in Ethiopia27 and in EDHS report 2016 92%.17 But, it is higher than the study finding in Tanzania.45 This difference might be due to the socio-cultural difference between the study participants as breastfeeding for a long duration is a traditional practice of Ethiopian mothers and currently, there is increased promotion of breastfeeding.
Our study finding revealed that the introduction of solid, semisolid, and soft foods at 6–8 months of age was 56.2%. This finding is consistent with the study done in Harare 54%,46 but slightly lower than the national EDHS report in 2016 (60%),17 previous studies were done from Mekele 62.8%,47 Southern Ethiopia (74.2%)49 and Abiy Adi town (80%)49 The possible explanation of this discrepancy could be attributed to variation in the measurement of initiation of complementary feeding, in which the latter studies assessed initiation of complementary food at 6–8 months of age of the child while it was at a 6 months for the former study. Thus, the use of a reference period of 6–8 months might overestimate the prevalence. Furthermore, the difference might be due to socio-cultural differences or lack of knowledge about the initiation of complementary feeding.
The proportion of children who received minimum meal frequency found to be adequate 33.8% of children, which was much lower than a study done in Derashe, Southern Ethiopia (95%),50 national level 45%17 and other countries like in rural Bangladesh (81%)51 and coastal, South India (77.5%).52 The lower figure observed in this study as compared to the National level (45%) might be because EDHS, 2016 was a nationally representative survey with a wide range of child feeding styles in different regions of Ethiopia. Other differences also might be as a result of social, cultural, and educational differences existed between the current study and others.
The present study found that only 5.4% of children received the recommended dietary diversity, that fed at least four and more foods from seven food groups which are lower than the findings from Ethiopia (16.5%)48 and national EDHS report in 201617 (14%). It is also lower than the findings of another country Delhi, India which was 32.6%.53 Minimum acceptable diet, a combination of minimum dietary diversity and minimum meal frequency was 5.3%, which is also lower than Ethiopia national survey (14%)17 and the study conducted from Abiy Adi, Ethiopia 11.9%.49 The finding is also much lower than other countries like Tanzania (16.3%) Bangladesh 40%, Delhi, India 19.7%.53–55 This difference could be due to the population has also different feeding habits with a tradition of cooking a few verities of food for the family. Moreover, there appears to be a tendency to share food with siblings at home. This population has also different feeding habits with a tradition of cooking a few verities of food for the family.
These findings revealed that the consumption of iron-rich and animal-source foods was 38.4%. This finding is higher than the study finding in Shashemene, Ethiopia.27 This difference might be due to a lack of awareness about nutritional requirements for IYC, affordability to a food product, and low purchasing power for food.
Concerning determinants associated with IYCF practice, it was found that mothers who gave birth at the health center were 1.734 more likely to carry out appropriate IYCF practice than mothers who gave birth at home (AOR =1.734; 95% C: (1.130, 2.661)). This also extends to mothers who delivered at hospital level were significantly associated with appropriate IYCF feeding practice than their counterparts (AOR=1.977; 95% CI: (1.101, 3.552)) which is similar to the findings from Assayita (AOR=2.55 (1.32, 4.93))28 and from Asella Town (AOR=1.77 (1.02, 3.06)).36 This could be due to the fact that mothers who gave birth at health facility would have proper child feeding advice and that encourages and fosters child feeding practice during health care service, which are the main fertile grounds to step up mothers’ confidence in challenging the community attitude towards appropriate feeding practices.
Evidence from Ethiopia and other Asian countries reveals that maternal education and father’s education were significantly associated with mother towards IYCF feeding practice.26,28,56 Mother’s ANC and PNC service visit were also positively associated with infant feeding practices in other studies28,49,51 but in our study, only delivery service at health facility showed association with IYCF practices related to maternal health care utilization determinants.
Our study also showed that study subjects whose mothers’ age is between 25 and 35 years were 2.091 times more likely to have appropriate IYCF practice than those mothers’ age less than 25 years (AOR = 2.091; 95% CI: (1.452, 3.011)). The odds of IYC feeding practice were 1.757 times more likely among mothers aged >35 years than those aged <25 years (AOR=1.757; 95% CI: (1.045, 2.954)). This study consistent with a study done in Bennatsemay district, children whose mothers’ age had ≥30 years were 86% less likely to behave poor practice on child feeding than children whose mothers’ age had in between 15 and 19 years (AOR= 0.14, 95% CI, 0.03–0.63)) 57. This could be due to the fact that older mothers may be better experienced/confident in feeding children, health care services, and encouraging different types of foods than younger mothers.
Household family size was another factor significantly associated with appropriate IYCF practices. Mothers with >4 family size at household 1.873 times more likely practice appropriate IYCF compared with women with 1–4 family size (AOR =1.873; 95% Cl: (1.311, 2.675)). Mother those who had more families may decrease the level of workload and it may have time for better commitment and good motivation to feed and care her child appropriately. Another possible explanation could be that mothers with more childbirths may have a better level of experience than with a few childbirth mothers.
The limitation of this study is the possible recall bias involved in collecting information regarding feeding practices in retrospect and it was not feasible to assess information on exact quantities of food consumed by the child.
Conclusion
The overall appropriate IYCF practices were better in general in Kalu district. But this prevalence is not acceptable to ensure good health and better nutritional status of children. In particular, dietary diversity and consumption of iron-rich and animal-source foods should receive greater focus in the study area. As a result, interventional initiatives should focus on institution delivery service are crucial to implementing appropriate IYCF practice. Health facilities need to be strengthened and fully utilized to provide high-quality feeding counseling. Special attention needs to be given to younger mothers, in addition to increasing institution delivery service.
Recommendations
Based on the current finding the following recommendations are suggested to the zonal health department, district health office, and respective health institutions:
- Awareness should be raised among reproductive age group women on appropriate IYCF practice and maternal healthcare services utilization. Health information dissemination should be strengthened to all expectant mothers.
- Efforts should be made to enhance maternal healthcare services utilization.
- Maternal health service outlets should be used to transmit child feeding information and hence, training should be given for all health workers to focus on IYCF practice as well.
Abbreviation
ANC, antenatal care; CF, complementary feeding; EBF, exclusive breast feeding; EDHS, Ethiopian demography health survey; IYCF, infant and young child feeding; MDD, minimum dietary diversity; MMF, minimum meal frequency; OR, odds ratio; PI, principal investigator; PNC, postnatal care: UNICEF, United Nation Children’s Fund; WHO, World Health Organization; TICF, time of initiating complementary feeding.
Data Sharing Statement
All the datasets during and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval and Consent to Participate
We got Ethical approval from Amhara Public Health Institute Ethical review committee (Protocol No: H/R/T/T/D/03/363) and a support letter from the research and technology transfer directorate of the institute to get the permission and cooperation of concerned bodies in South Wollo Zone Health Department. We got an informed oral consent from each participant, which was approved by the ethical review committee. The interviewers took precautionary measures a brief discussion and explanation with the mothers or caregivers having children aged 6–23 months before the interview. The study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We acknowledge Amhara Public Health Institute Dessie Branch for giving us the chance to do this study and covering data enumeration expenses. We also appreciate the administrative of selected districts for their cooperation and commitment to this work.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the beginning, carried out the overall design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have decided on the journal to which the article has been submitted; and agree to be responsible for all aspects of the work.
Funding
APHI has covered data enumeration cost.
Disclosure
The authors report no conflicts of interest for this work.
References
1. UNICEF. Programming Guide: Infant and Young Child Feeding. New York: Nutrition section. Programmes; 2011. Available from: unicef-iycf-programming-guide-may-26-2011.pdf. Accessed March 24, 2021.
2. Galler JR. Behavioral consequences of malnutrition in early life. In: Nutrition and Behavior. Springer; 1984:63–117.
3. Disha A, Rawat R, Subandoro A, Menon P. Infant and young child feeding (IYCF) practices in Ethiopia and Zambia and their association with child nutrition: analysis of demographic and health survey data. Afr J Food Agric Nutr Dev. 2012;12(2):5895–5914.
4. De Onis M, Branca F. Childhood stunting: a global perspective. Matern Child Nutr. 2016;12:12–26. doi:10.1111/mcn.12231
5. Victora CG, Adair L, Fall C, et al. Maternal and child undernutrition: consequences for adult health and human capital. Lancet. 2008;371(9609):340–357. doi:10.1016/S0140-6736(07)61692-4
6. Lomborg B. Global Crises, Global Solutions. Cambridge, UK: Cambridge University Press; 2004.
7. Troesch B, Biesalski HK, Bos R, et al. Increased intake of foods with high nutrient density can help to break the intergenerational cycle of malnutrition and obesity. Nutrients. 2015;7(7):6016–6037. doi:10.3390/nu7075266
8. Pan American Health Organization, World Health Organization. Guiding Principles for complementary feeding of the breastfeeding child .In division of Health promotion, Protection and Food and nutrition program. December-10-2001, Pan American Organization, World Health Organization; USA, America. p.40.
9. World Health Organization. Exclusive breastfeeding for six months best for babies everywhere. Newsline of Nutrition [serial online]; 2011. [cited April 15, 2012]. Available from: https://www.who.int/news/item/15-01-2011-exclusive-breastfeeding-for-six-months-best-for-babies-everywhere. Accessed March 23, 2021.
10. Edmond KM, Zandoh C, Quigley MA, Amenga-Etego S, Owusu-Agyei S, Kirkwood BR. Delayed breastfeeding initiation increases risk of neonatal mortality. Pediatrics. 2006;117(3):e380–e386. doi:10.1542/peds.2005-1496
11. Kimani-Murage EW, Madise NJ, Fotso J-C, et al. Patterns and determinants of breastfeeding and complementary feeding practices in urban informal settlements, Nairobi Kenya. BMC Public Health. 2011;11(1):396. doi:10.1186/1471-2458-11-396
12. Popkin BM, Adair L, Akin JS, Black R, Briscoe J, Flieger W. Breast-feeding and diarrheal morbidity. Pediatrics. 1990;86(6):874–882.
13. Holla-Bhar R, Iellamo A, Gupta A, Smith JP, Dadhich JP. Investing in breastfeeding–the world breastfeeding costing initiative. Int Breastfeed J. 2015;10(1):8. doi:10.1186/s13006-015-0032-y
14. Setegn T, Gerbaba M, Belachew T. Determinants of timely initiation of breastfeeding among mothers in Goba Woreda, South East Ethiopia: a cross sectional study. BMC Public Health. 2011;11(1):217. doi:10.1186/1471-2458-11-217
15. Baker EJ, Sanei LC, Franklin N. Early initiation of and exclusive breastfeeding in large-scale community-based programmes in Bolivia and Madagascar. J Health Popul Nutr. 2006;24(4):530.
16. Ke E. Feeding of young infants and children in exceptionally difficult circumstances (like, HIV and humanitarian emergencies). In: Solution Exchange MCH Community Newsletter Breastfeeding Month Special; 2008. Available from: https://apps.who.int/iris/bitstream/handle/10665/204824/B3195.pdf?sequence=1&isAllowed=y. Accessed March 3, 2021.
17. Central Statistical Agency, The DHS Program. Ethiopia. Ethiopia Demographic and Health Survey2016. Addis Ababa, Ethiopia: Central Statistical Agency (CSA); 2016. Available from: https://dhsprogram.com/pubs/pdf/FR328/FR328.pdf. Accessed March 23, 2021.
18. World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices: Part 1: Definitions: Conclusions of a Consensus Meeting Held 6–8 November 2007 in Washington DC, USA; 2008.
19. Daelmans B, Dewey K, Arimond M. New and updated indicators for assessing infant and young child feeding. Food Nutr Bull. 2009;30(2_suppl2):S256–S262. doi:10.1177/15648265090302S210
20. World Health Organization. Comprehensive Implementation Plan on Maternal, Infant and Young Child Nutrition; 2014.
21. Arimond M, Daelmans B, Dewey K. Indicators for feeding practices in children. Lancet (London, England). 2008;371(9612):541. doi:10.1016/S0140-6736(08)60250-0
22. Federal Ministry of Health Family Health Department. National Strategy for Infant and Young Child Feeding. Addis Ababa, Ethiopia: Federal Ministry of Health Family Health Department Ethiopia; 2004.
23. Miller NP, Amouzou A, Tafesse M, et al. Integrated community case management of childhood illness in Ethiopia: implementation strength and quality of care. Am J Trop Med Hyg. 2014;91(2):424–434. doi:10.4269/ajtmh.13-0751
24. Labbok MH. Global baby-friendly hospital initiative monitoring data: update and discussion. Breastfeed Med. 2012;7(4):210–222. doi:10.1089/bfm.2012.0066
25. Demographic E. Health Survey 2016. 2016 Key Indicators Report. Addis Ababa, Ethiopia and Rockville, MD: Ethiopian Central Statistical Agency & ICF International.
26. Demilew YM, Tafere TE, Abitew DB. Infant and young child feeding practice among mothers with 0–24 months old children in slum areas of Bahir Dar City, Ethiopia. Int Breastfeed J. 2017;12(1):26. doi:10.1186/s13006-017-0117-x
27. Yonas F. Infant and young child feeding practice status and associated factors among mothers of under 24-month-old children in Shashemene Woreda, Oromia region, Ethiopia. OAlib. 2015;2(07):1. doi:10.4236/oalib.1101583
28. Kahssay M, Ebrahim E, Seid O, Woldu E, Reddy S. Infant and young child feeding practices and associated factors among children aged 0–23 months in Assayita District Afar Region Ethiopia. J Food Nutr Sci. 2019;7(6):96–104. doi:10.11648/j.jfns.20190706.13
29. Ethiopia Ministry of Agriculture. Coping with Drought and Climate Change Project Kalu Woreda of South Wollo Zone, Ethiopia. UNDP/GEF. Addis Ababa, Ethiopia Ministry of Agriculture MOA/DRMFSS; 2012. Available from: http://www.undp.org/content/dam/undp/documents/projects/ETH/Expert%20use%20report%20Final.pdf. Accessed March 23, 2021.
30. World Health Organization. Indicators for Assessing Infant and Young Child Feeding Practices. Part 1 Definitions. Washington, DC, USA; 2007. Available from: https://apps.who.int/iris/bitstream/handle/10665/43895/9789241596664_eng.pdf. Accessed March 23, 2021.
31. World Health Organization. Complementary Feeding: Report of the Global Consultation, and Summary of Guiding Principles for Complementary Feeding of the Breastfed Child. Geneva, Switzerland; 2003. Available from: https://apps.who.int/iris/handle/10665/42739. Accessed March 23, 2021.
32. World Health Organization. Infant and young child feeding. In: Model Chapter for Textbooks for Medical Students and Allied Health Professionals. Geneva 27, Switzerland: World Health Organization; 2009. Available from: https://apps.who.int/iris/bitstream/handle/10665/44117/9789241597494_eng.pdf. Accessed March 23, 2021.
33. Central Statistical Agency. Ethiopia Mini Demographic and Health Survey. Ethiopia: Addis Ababa; 2014.
34. McGuire S. International Food Policy Research Institute. 2014. Washington, DC: global Nutrition Report 2014: actions and accountability to accelerate the world’s progress on nutrition. Adv Nutr. 2015;6(3):278–279. doi:10.3945/an.115.008599
35. Berhe H, Mekonnen B, Bayray A, Berhe H. Determinants of breast feeding practices among mothers attending public health facilities, Mekelle, northern Ethiopia; a cross sectional study. Int J Pharm Sci Res. 2013;4(2):650.
36. Sasie SD, Oljira L, Demena M, Teshome M. Breastfeeding practice and associated factors among mothers/caretakers of children aged 0‐23 months in Asella Town, South East Ethiopia, 2015. Global J Med Public Health. 2017;6(4):1–11.
37. Tamiru D, Belachew T, Loha E, Mohammed S. Sub-optimal breastfeeding of infants during the first six months and associated factors in rural communities of JimmaArjo Woreda, Southwest Ethiopia. BMC Public Health. 2012;12(1):363. doi:10.1186/1471-2458-12-363
38. Tilahun G, Degu G, Azale T, Tigabu A. Prevalence and associated factors of timely initiation of breastfeeding among mothers at Debre Berhan town, Ethiopia: a cross-sectional study. Int Breastfeed J. 2016;11(1):27. doi:10.1186/s13006-016-0086-5
39. Egata G, Berhane Y, Worku A. Predictors of non-exclusive breastfeeding at 6 months among rural mothers in east Ethiopia: a community-based analytical cross-sectional study. Int Breastfeed J. 2013;8(1):8. doi:10.1186/1746-4358-8-8
40. Mekuria G, Edris. M. Exclusive breast feeding and associated factors among mother’s in Debre Markos, North west Ethiopia: a cross_sectional study. Int Breastfeed J. 2015;10(1):1. doi:10.1186/s13006-014-0027-0
41. Khan GN, Ariff S, Khan U, et al. Determinants of infant and young child feeding practices by mothers in two rural districts of Sindh, Pakistan: a cross-sectional survey. Int Breastfeed J. 2017;12(1):40.
42. Legesse M, Demena M, Mesfin F, Haile D. Prelacteal feeding practices and associated factors among mothers of children aged less than 24 months in Raya Kobo district, North Eastern Ethiopia: a cross-sectional study. Int Breastfeed J. 2014;9(1):189. doi:10.1186/s13006-014-0025-2
43. Dabar D, Verma A, Mangal A, Singh S, Yadav V. Feeding practices of children under 24 months of age attending a tertiary care hospital in Delhi. Children. 2014;75(10/75):
44. Doherty T, Sanders D, Goga A, Jackson D. Implications of the new WHO guidelines on HIV and infant feeding for child survival in South Africa. Bull World Health Organ. 2011;89(1):62–67. doi:10.2471/BLT.10.079798
45. Ogbo FA, Ogeleka P, Awosemo AO. Trends and determinants of complementary feeding practices in Tanzania, 2004–2016. Trop Med Health. 2018;46(1):40. doi:10.1186/s41182-018-0121-x
46. Semahegn A, Tesfaye G, Bogale A. Complementary feeding practice of mothers and associated factors in HiwotFana Specialized Hospital, Eastern Ethiopia. Pan Afr Med J. 2014;18.
47. Shumey A, Demissie M, Berhane Y. Timely initiation of complementary feeding and associated factors among children aged 6 to 12 months in Northern Ethiopia: an institution-based cross-sectional study. BMC Public Health. 2013;13(1):1050. doi:10.1186/1471-2458-13-1050
48. Areja A, Yohannes D, Yohannis M. Determinants of appropriate complementary feeding practice among mothers having children 6–23 months of age in rural Damot sore district, Southern Ethiopia; a community based cross sectional study. BMC Nutr. 2017;3(1):82. doi:10.1186/s40795-017-0202-y
49. Mekbib E, Shumey A, Ferede S, Haile F. Magnitude and factors associated with appropriate complementary feeding among mothers having children 6–23 months-of-age in northern Ethiopia; a community-based cross-sectional study. J Food Nutr Sci. 2014;2(2):36.
50. Wondafrash M, Amsalu T, Woldie M. Feeding styles of caregivers of children 6–23 months of age in Derashe special district, Southern Ethiopia. BMC Public Health. 2012;12(1):235. doi:10.1186/1471-2458-12-235
51. Saha KK, Frongillo EA, Alam DS, Arifeen SE, Persson LÅ, Rasmussen KM. Appropriate infant feeding practices result in better growth of infants and young children in rural Bangladesh. Am J Clin Nutr. 2008;87(6):1852–1859. doi:10.1093/ajcn/87.6.1852
52. Rao S, Swathi P, Unnikrishnan B, Hegde A. Study of complementary feeding practices among mothers of children aged six months to two years-A study from coastal south India. Australas Med J. 2011;4(5):252. doi:10.4066/AMJ.2011.607
53. Khan AM, Kayina P, Agrawal P, Gupta A, Kannan AT. A study on infant and young child feeding practices among mothers attending an urban health center in East Delhi. Indian J Public Health. 2012;56(4):301. doi:10.4103/0019-557X.106420
54. Victor R, Baines SK, Agho KE, Dibley MJ. Factors associated with inappropriate complementary feeding practices among children aged 6–23 months in Tanzania. Matern Child Nutr. 2014;10(4):545–561. doi:10.1111/j.1740-8709.2012.00435.x
55. Senarath U, Agho KE, AkramDe S, et al. Comparisons of complementary feeding indicators and associated factors in children aged 6–23 months across five South Asian countries. Matern Child Nutr. 2012;8:89–106. doi:10.1111/j.1740-8709.2011.00370.x
56. Khan GN, Ariff S, Khan U, Habib A. Determinants of infant and young child feeding practices by mothers in two rural districts of Sindh, Pakistan: a cross-sectional survey. Int Breastfeed J. 2017;12(1):40. doi:10.1186/s13006-017-0131-z
57. Tadesse A. Predictors of infant and young feeding practices among children 6–23 months old in Bennatsemayworeda, Ethiopia. J Nutr Health Food Eng. 2018;8(6):410–420. doi:10.15406/jnhfe.2018.08.00304
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.