Back to Journals » Cancer Management and Research » Volume 17

Induction Chemoimmunotherapy Followed by Radiotherapy in Locally Advanced Head and Neck Squamous Cell Carcinoma
Authors Tian Y ![]() , Fan Z
, Fan Z ![]() , Qin Y, Zhang M, Xiong Y
, Qin Y, Zhang M, Xiong Y ![]() , Ren XY, Wang X, Wu S
, Ren XY, Wang X, Wu S
Received 14 May 2025
Accepted for publication 26 September 2025
Published 13 October 2025 Volume 2025:17 Pages 2365—2375
DOI https://doi.org/10.2147/CMAR.S540239
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Kattesh Katti
Yan Tian,1,* Zenan Fan,1,* Yong Qin,2 Min Zhang,3 Yan Xiong,4 Xue-Ying Ren,5 Xiaoyun Wang,1 Shikai Wu1
1Department of Oncology, Peking University First Hospital, Beijing, 100034, People’s Republic of China; 2Department of Otolaryngology Head and Neck Surgery, Peking University First Hospital, Beijing, 100034, People’s Republic of China; 3Department of Radiation Oncology, Peking University People’s Hospital, Beijing, 100044, People’s Republic of China; 4Department of Pathology, Peking University First Hospital, Beijing, 100034, People’s Republic of China; 5Department of Radiation Oncology, Peking University First Hospital, Beijing, 100034, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shikai Wu, Department of Oncology, Peking University First Hospital, Beijing, 100034, People’s Republic of China, Tel +86-010-64007836, Email [email protected]
Introduction: The majority of head and neck squamous cell carcinomas (HNSCC) are diagnosed at an advanced stage, often necessitating standard treatments such as surgery or concurrent chemoradiotherapy.
Methods: This was a real-world study conducted between January 2021 and October 2024. The study enrolled 42 previously untreated patients diagnosed with locally advanced head and neck squamous cell carcinoma (LA-HNSCC). Patients received induction chemotherapy (IC) with or without immunotherapy followed by radiotherapy at our hospital.
Results: The group receiving immunotherapy with IC (I+IC, N=26) demonstrated an 82.6% objective response rate (ORR) and a 92.3% disease control rate (DCR). In contrast, patients treated with IC (N=16) alone exhibited an ORR of 37.5% and a DCR of 93.8%. With a median follow-up of 28.9 months, the I+IC group showed a 100% 6-month progression-free survival (PFS) and an 88.5% 12-month PFS, with a 92.3% overall survival (OS) rate at 12 months.
Discussion: This real-world study suggests that the addition of immunotherapy to IC holds promise for improving treatment outcomes in locally advanced HNSCC. The findings underscore the need for further research involving a larger patient population to validate these preliminary results.
Keywords: locally advanced head and neck squamous cell carcinoma, chemoimmunotherapy, induction chemotherapy, checkpoint inhibitor, immunotherapy
Introduction
The majority of head and neck squamous cell carcinomas (HNSCC) are diagnosed at an advanced stage, often necessitating standard treatments such as surgery or concurrent chemoradiotherapy.1 An alternative approach for patients with extensive tumor involvement or those seeking organ preservation is induction chemotherapy followed by concurrent chemoradiotherapy. Induction therapy is vital in locally advanced HNSCC (LA-HNSCC) for organ preservation, particularly in locally advanced laryngeal and hypopharyngeal cancers. It is also indicated for very advanced diseases (N2c, N2b, N3), high-risk distant metastasis, tumors adjacent to or invading surrounding organs (eg, tracheal compression), symptomatic locally advanced diseases impeding radical chemoradiotherapy, and as a bridge when radiotherapy is delayed.2 However, the effectiveness of this combined approach in terms of extending patient survival has been a subject of debate in various trials.3,4
Recent years have witnessed the remarkable impact of immunotherapy on the outcomes of several cancers. Immune checkpoint inhibitors have secured approval as first-line treatments for recurrent and/or metastatic HNSCC as well.5 Early clinical studies have shown promise in enhancing clinical outcomes for operable LA-HNSCC with neoadjuvant immunotherapy.6,7 This year, the Phase III Keynote 689 trial demonstrated that neoadjuvant and adjuvant pembrolizumab significantly improved event-free survival in LA-HNSCC.8 The theoretical potential for immunotherapy to be clinically effective in patients with locally inoperable advanced head and neck squamous cell carcinoma is significant. Among these patients, those with human papillomavirus (HPV) - positive tumors may derive particular benefit from immunotherapy, as emerging evidence suggests that HPV positivity is associated with enhanced response to immune checkpoint inhibitors.9
However, two pivotal randomized phase III trials exploring the combination of chemoradiotherapy with checkpoint inhibitors for LA-HNSCC, namely the Keynote-412 trial and Javelin Head and Neck 100 trial, yielded disappointing results.10–12 These disappointments may, in part, be attributed to T-cell dysfunction induced by excessive radiation to the lymph node drainage areas. The utilization of induction chemotherapy in conjunction with immunotherapy could mitigate the impact of over-irradiation of lymphatic drainage regions and, as a result, potentially improve clinical efficacy.
This study, therefore, sets out to investigate the safety and efficacy of combining induction chemotherapy with a PD-1 inhibitor in the treatment of LA-HNSCC.
Methods
Study Design and Treatment
This was a real-world study conducted between January 2021 and October 2024. The study enrolled 42 previously untreated patients diagnosed with LA-HNSCC. Patients received induction chemotherapy (IC) with or without immunotherapy followed by radiotherapy at our hospital. After three cycles of IC, patients proceeded with immunotherapy combined with chemoradiotherapy and received immunomaintenance therapy for one year unless intolerable adverse effects occurred. In cases where IC failed, patients were transitioned to concurrent chemoradiotherapy immediately.
The IC regimen consisted of 3 cycles, with paclitaxel for injection (albumin-bound) (CSPC OUYI Pharmaceutical Co., Ltd.) at a dosage of 175–200 mg/m^2 administered on day 1 and cisplatin (QILU Pharmaceutical Co, Ltd). at a dosage of 70–75 mg/m2 given between days 1 and 2, with a three-week interval between cycles. Pembrolizumab (Merck Sharp & Dohme, MSD), a PD-1 inhibitor, was administered at a fixed dose of 200 mg once every three weeks. Definitive chemoradiotherapy involved a combination of radiotherapy with an approximate dose of 70 Gy and cisplatin (40 mg/m2) administered weekly.
Patients
Eligible patients had histologically confirmed HNSCC at stage III–IVB, defined as cT0N3/cT1-2-N1-3/CT3-4 N0-3 based on the 8th AJCC classification, originating from the oral cavity, oropharynx, hypopharynx, or larynx. All patients had not undergone prior anti-cancer therapy and exhibited normal hematological, hepatic, and renal function. Patients were classified based on the Eastern Cooperative Oncology Group (ECOG) performance status, which was 0 or 1. HPV status for oropharyngeal cancer was determined through p16 IHC, and PD-L1 status was assessed using the 22C3 antibody.
Endpoints
The primary endpoint was the objective response rate (ORR) of IC. Secondary endpoints included progression-free survival (PFS), overall survival (OS), and safety. ORR was defined as the proportion of patients achieving a complete or partial response according to RECIST 1.1 criteria, as assessed by the treating physicians before radiotherapy. PFS measured the time from the initiation of IC to disease recurrence or death from any cause, while OS calculated the period from the start of IC to all-cause mortality. Toxicity was assessed based on the National Cancer Institute Common Terminology Criteria for Adverse Events (version 5.0) during IC. Patient dropouts were primarily due to the COVID-19 pandemic, which led to disruptions in treatment schedules and follow-up visits.
Statistical Analysis
Statistical analyses were conducted using SPSS version 27.0, and graphical representations were generated using GraphPad Prism version 9.00. Numerical variables are presented as medians with 95% confidence intervals [CI]. ORR, disease control rate (DCR), and their 95% CIs were computed using the Clopper and Pearson method. Survival analysis was performed using the Kaplan–Meier method, assessing PFS and OS. Univariate Cox regression analysis incorporated various factors to identify prognostic factors for survival and disease relapse, yielding hazard ratios (HRs) and 95% CIs. Statistical significance was defined as p < 0.05.
Results
Characteristics of the Patients
Demographics
The median age at diagnosis for the entire cohort was 57 years, with an age range of 45 to 81. Males constituted the majority, comprising 88% of the patient population.
Treatment Regimens
Out of the 42 patients included in the study, 26 individuals underwent a combined treatment approach with programmed death 1 (PD-1) inhibitors alongside IC, while the remaining patients received IC as a standalone therapy. Among those who received PD-1 inhibitors, Pembrolizumab was administered to 15 patients, sintilimab to 4 patients, Tririplizumab to 2 patients, Carrezizumab to 4 patients, and Tislelizumab to 1 patient. Detailed baseline characteristics of the patient cohort are summarized in Table 1.
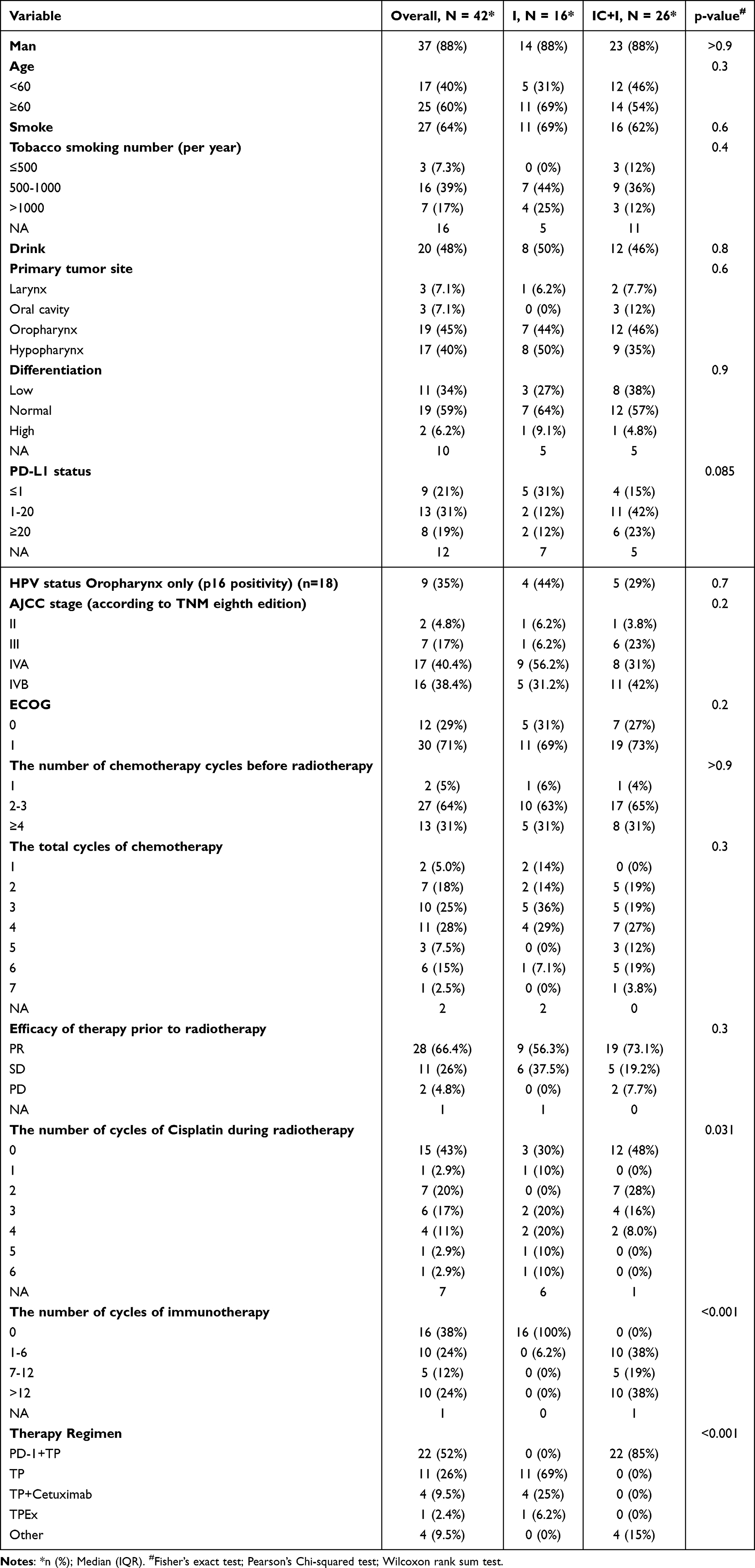 |
Table 1 Patient Characteristics of Treated Patients |
Safety and Feasibility
Within the I+IC group, treatment specifics varied. Two patients received only one cycle of IC due to cervical lymph node enlargement, while three patients underwent four cycles of IC while waiting for radiotherapy. One patient completed six IC cycles but did not proceed to radiotherapy due to the impact of the COVID-19 pandemic. The majority in this group successfully completed the intended three cycles of IC. Importantly, all patients in this group received a minimum of five cycles of immunotherapy. As of the most recent update, fourteen patients have ceased immunotherapy: six due to adverse reactions (specifically, recurrence of psoriasis and immune pneumonia), three owing to disease progression, and five who discontinued treatment voluntarily. Ten patients successfully completed a full year of immunotherapy, and the remaining two patients continue on immunomaintenance therapy. In contrast, all patients in the IC-only group completed two or three cycles of IC.
Notably, the incidence of adverse events of any grade in the IC+I group did not exceed that of the IC group. The detailed composition of adverse events in both groups can be found in Table 2.
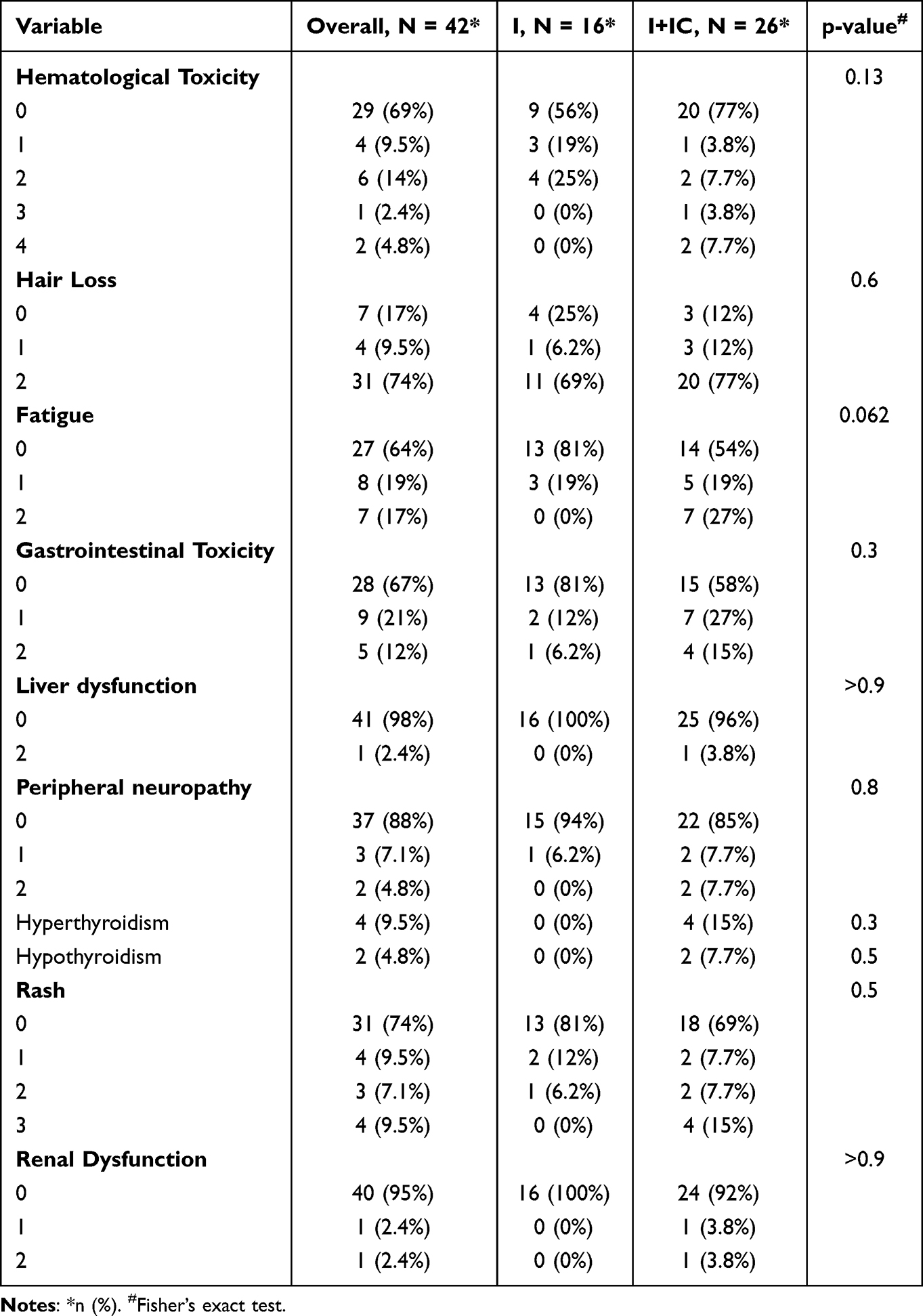 |
Table 2 Adverse Events in the Two Groups |
Efficacy Outcomes
Regarding the therapeutic effects before radiotherapy, the 26 patients who received immunotherapy demonstrated a significant tumor response: 19 patients exhibited PR, five maintained SD, and two experienced PD. This resulted in an impressive ORR of 82.6% and a DCR of 92.3%, as visually depicted in Table 1 and Figure 1. In contrast, among the 16 patients who received IC alone, a lower proportion achieved PR, with no CR observed. Consequently, the ORR in this group was 37.5%, while the DCR was 93.8%. Statistical analysis using Fisher’s Exact Test for Count Data revealed a significant difference in ORR between the two groups (P = 0.0002).
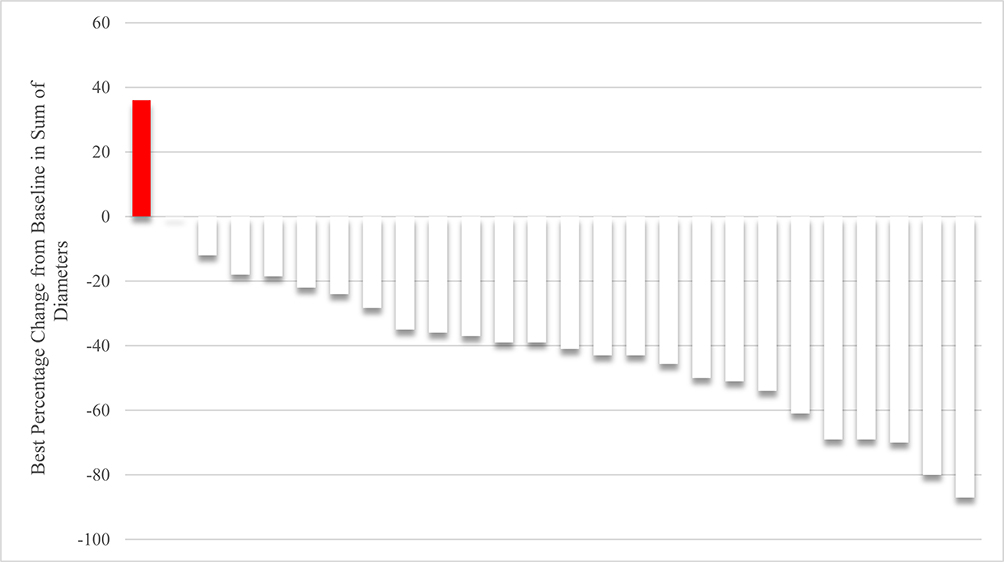 |
Figure 1 Waterfall plot of tumor shrinkage in patients treated with induction chemotherapy and immunotherapy. This figure illustrates the individual tumor shrinkage in 26 patients with locally advanced head and neck squamous cell carcinoma (LA-HNSCC) treated with induction chemotherapy in combination with immunotherapy (I+IC). The waterfall plot shows the percentage change in tumor size for each patient, highlighting the response to treatment. Among these patients, 19 exhibited partial response (PR), 5 had stable disease (SD), and 2 experienced progressive disease (PD), resulting in an objective response rate (ORR) of 82.6% and a disease control rate (DCR) of 92.3%. |
In our study, PD-L1 expression was assessed in 31 patients, revealing varied ORR across different PD-L1 expression levels. Specifically, in the PD-L1 < 1 group, the ORR was 50% (n=2) in the TP + PD-1 group, 0% (n=2) in the TP group, and 25% (n=4) in the TP + Cetuximab group. In the PD-L1 ≥ 1 and < 10 group, the ORR was 83.3% (n=6) in the TP + PD-1 group and 33.3% (n=3) in the other + PD-1 group. In the PD-L1 ≥ 10 and < 20 group, the ORR was 66.7% (n=3) in the TP + PD-1 group. Lastly, in the PD-L1 ≥ 20 group, the ORR was 100% (n=1) in the TPEx group, 0% (n=1) in the TP group, and 83.3% (n=6) in the PD-1 + TP group. Fisher’s exact test showed no statistically significant differences in ORR between groups within each PD-L1 expression level.
In our study, we evaluated the efficacy of different treatment regimens in 26 patients with documented HPV status, of whom 9 were HPV-positive and 17 were HPV-negative. Among the HPV-positive patients, 7 had oropharyngeal cancer and 2 had hypopharyngeal cancer. The ORR for the different treatment groups within the HPV-positive cohort were 50% in the TP group (n=2), 100% in the TPEx group (n=1), and 75% in the TP + PD-1 group (n=4). In the HPV-negative cohort, the ORR was 50% in the TP group (n=2), 80% in the TP + PD-1 group (n=10), 66.7% in the TP + Cetuximab group (n=3), and 100% in the other + PD-1 group (n=2). Fisher’s exact test revealed no statistically significant differences in ORR between HPV-positive and HPV-negative groups (p=0.34).
Follow-Up and Survival Outcomes
As of October 27, 2024, with a median follow-up duration of 28.9 months, ranging from 22.9 to 34.9 months, the group receiving induction chemotherapy combined with immunotherapy (I+IC) exhibited a noteworthy 6-month PFS rate of 100%, indicating a favorable early outcome. At the 12-month mark, the PFS rate remained encouraging at 88.5% (23 out of 26), suggesting sustained disease control. Furthermore, the OS rate at 12 months was robust, with 92.3% of patients (24 out of 26) achieving this milestone. Comparatively, the 12-month PFS and OS rates in the IC group showed significant differences compared to the I+IC group (PFS p = 0.02, OS p = 0.006).
These findings suggest that the addition of immunotherapy to induction chemotherapy may offer potential benefits in terms of PFS and OS. Although these differences did not reach statistical significance in our current analysis, there was a trend towards improvement within the IC+I group suggesting potential improvement in PFS and OS (PFS p-value = 0.53, OS p-value = 0.19). With a median follow-up of 28.9 months, the median PFS and OS endpoints were not achieved for either Group I or Group I+IC within the study period (Figures 2 and 3).
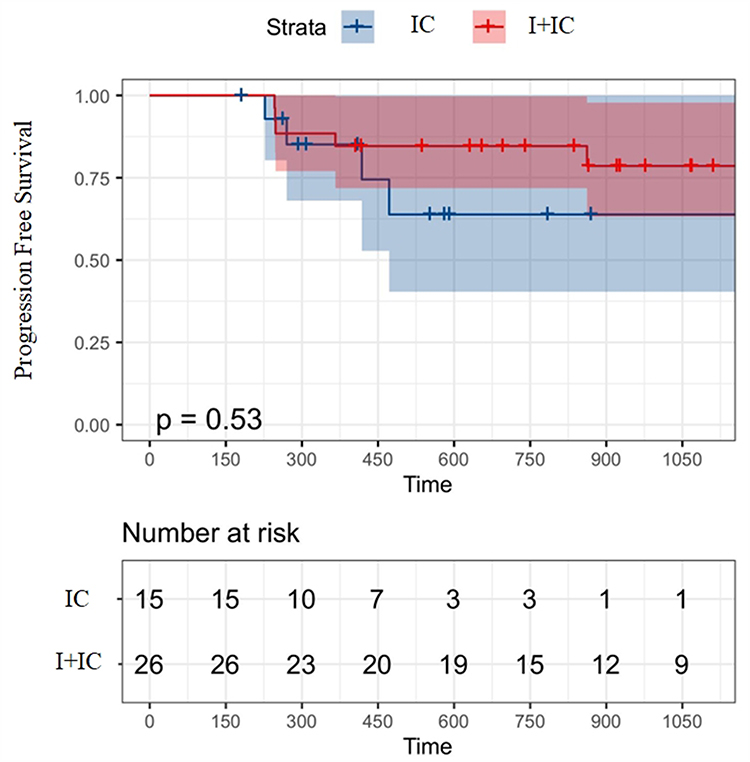 |
Figure 2 Kaplan-Meier curves for progression-free survival (PFS) in patients with LA-HNSCC. This figure presents the Kaplan-Meier curves for progression-free survival (PFS) in patients with locally advanced head and neck squamous cell carcinoma (LA-HNSCC) treated with induction chemotherapy (IC) alone or in combination with immunotherapy (I+IC). The curves depict the time to disease progression or death from any cause. The addition of immunotherapy to IC showed a trend towards improved PFS, although the difference did not reach statistical significance (PFS p-value = 0.53). The median PFS was not reached for either group within the study period. |
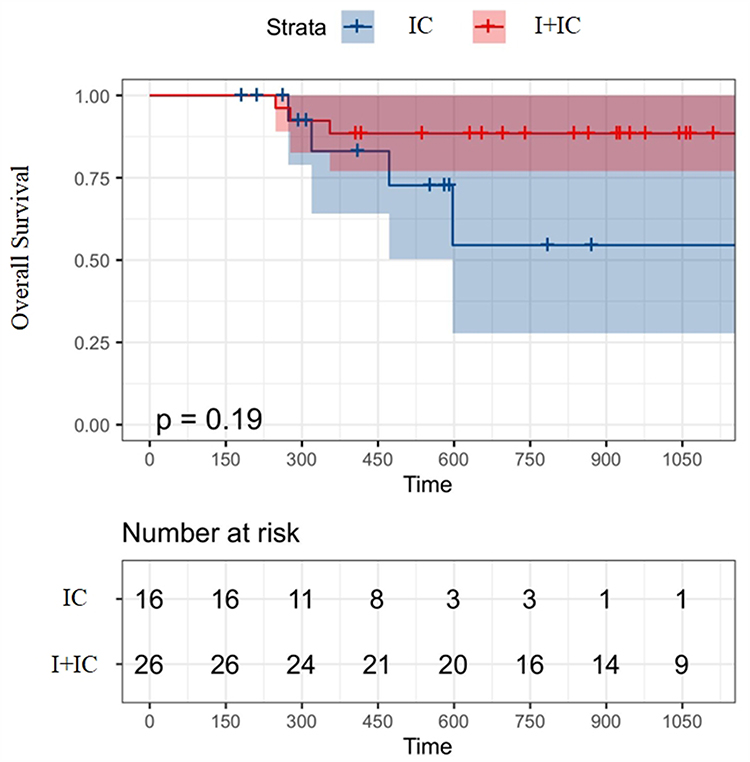 |
Figure 3 Kaplan-Meier curves for overall survival (OS) in patients with LA-HNSCC. This figure displays the Kaplan-Meier curves for overall survival (OS) in patients with locally advanced head and neck squamous cell carcinoma (LA-HNSCC) treated with induction chemotherapy (IC) alone or in combination with immunotherapy (I+IC). The curves illustrate the survival rates over time for the two treatment groups. The addition of immunotherapy to IC showed a trend towards improved OS, although the difference did not reach statistical significance (OS p-value = 0.19). The median OS was not reached for either group within the study period. |
Discussion
This is a real-world study, and preliminary results suggest that immunotherapy combined induction chemotherapy can lead to higher ORR, PFS, and OS benefits compared to induction chemotherapy alone.
The majority of LA-HNSCC is deemed unresectable due to the intricate anatomical structure of the head and neck region. Consequently, treatment strategies must not only prioritize therapeutic efficacy and toxicity but also strive to preserve organ function to the utmost extent.
Induction chemotherapy not only reduces tumor micrometastasis but also decreases the tumor stage, thereby enhancing organ function preservation. However, the standard TPF (docetaxel, cisplatin, 5-fluorouracil) regimen is highly toxic and poorly tolerated by a majority of patients. Furthermore, there is insufficient evidence to confirm the ability of the TPF regimen to prolong patient survival and improve prognosis; thus, its clinical application remains limited.13
In recent years, immunotherapy has demonstrated remarkable success in treating various tumors and has emerged as a groundbreaking therapy for malignancies. For relapsed and/or metastatic HNSCC, immunotherapy has been recommended as the preferred first-line treatment option. This recommendation primarily stems from the findings of KEYNOTE-048 study results. The latest follow-up data revealed that among individuals with PD-L1 CPS ≥ 20, monotherapy with pembrolizumab achieved a 5-year survival rate of 19.9%, significantly surpassing the control group’s rate of 7.4%. Additionally, combination therapy involving immunotherapy and chemotherapy yielded a 5-year survival rate of 23.9%, compared to just 6.4% in the control group.14 Consequently, immunotherapy intervention has altered the prognosis for HNSCC patients.
Many attempts have been made to explore immunotherapy in the context of locally advanced malignancies. In non-small cell lung cancer, combining immunotherapy with chemoradiotherapy has shown success for patients with unresectable locally advanced tumors. The PACIFIC study confirmed that sequential administration of duvalizumab (a PD-L1 inhibitor) after concurrent chemoradiotherapy can significantly prolong median survival time from 29.1 months to 47.5 months and increase the 5-year survival rate by 9.5%.15 However, in the case of locally advanced head and neck squamous cell carcinoma (LA-HNSCC), two important phase III clinical trials, JAVELIN Head & Neck 10012 and KEYNOTE 41216 failed to demonstrate survival benefits when combining chemoradiotherapy with immunotherapy. Subsequent analyses revealed that pembrolizumab plus CRT was effective specifically for patients with CPS≥20, resulting in a higher 3-year overall survival rate of 79.1% compared to CRT alone; this benefit continued to increase over time during follow-up periods. Additionally, recent four-year follow-up results from another study presented at ESMO suggest that concurrent chemoradiotherapy followed by pembrolizumab may be more effective than concurrent chemoradiation combined with pembrolizumab, providing clinical benefits independent of PD-L1 expression status.17 Therefore, further exploration is needed regarding the model of combining immunotherapy with radiotherapy for LA-HNSC. Thus, for LA-HNSCC, the model of immunotherapy combined with radiotherapy still needs to be explored.
In recent years, preliminary findings have shown that neoadjuvant immunotherapy combined with chemotherapy LA-HNSCC can provide clinical benefits. In 2023, ASCO reported two clinical trials investigating the combination of neoadjuvant chemotherapy and immunotherapy: the DEPEND trial18 and the NeoCPC trial.19 The DEPEND trial is a Phase II study evaluating nivolumab, paclitaxel, and carboplatin followed by response-stratified chemoradiotherapy in previously untreated stage IVA-B HPV (-) HNSCC patients. The results demonstrated an ORR of 89%, with tumor regression of ≥50% observed in 54% of patients. The 2-year PFS was 64%, while overall survival (OS) reached 76%. In the NeoCPC trial, locoregionally advanced resectable HNSCC patients received neoadjuvant immunochemotherapy with camrelizumab, nab-paclitaxel, and cisplatin for three cycles followed by radiotherapy or surgery. The ORR achieved was 89.6% (43/45), with a major pathological response (MPR) observed in 63% of surgically treated patients including a pathologic complete response (pCR) rate of 55.6%. A retrospective study investigated the clinical outcomes of DCF induction chemotherapy combined with or without sintilimab followed by surgery for LA-HNSCC.19 After three cycles of treatment, compared to chemotherapy alone group, immunochemotherapy showed an ORR of 84.6% and a higher two-year PFS rate at 44%, whereas control group had rates at only 68.4% and 17%. Although statistical significance was not reached between groups, this study also explored immunotherapy combined with nab-paclitaxel and cisplatin regimen which exhibited better tolerability among patients achieving an ORR reaching 74%, as well as showing trends towards improved PFS and OS outcomes over time during follow-up period. Currently, the standard regimen for induction chemotherapy remains the TPF regimen, followed by sequential radiotherapy alone due to its poor tolerability. In this study, most patients exhibited good tolerance and subsequently received CCRT. However, we also observed that when the number of cycles of induction chemotherapy reached or exceeded 4 cycles, there was a significant decline in patient physical fitness and a notable increase in the number of patients receiving radiotherapy alone. Therefore, our study suggests that the optimal number of cycles for induction chemotherapy is still 2–3 cycles.
In China, various PD-1 monoclonal antibodies are currently being used clinically across different cancer types. Among them, non-small cell lung cancer has witnessed extensive clinical applications with different PD-1 monoclonal antibodies such as pembrolizumab, tislelizumab, nivolumab, sintilimab and tislelizumab. These antibodies have demonstrated similar efficacy results in clinical studies while maintaining acceptable side effects profiles. Due to various reasons specific to our patients’ conditions, treatment regimens involving different PD-1 monoclonal antibodies were employed. However, the findings from our research indicate that regardless of which PD-1 monoclonal antibody patients choose, effective outcomes and tolerability are consistently achieved.
In conclusion, this real-world study suggests that the addition of immunotherapy to IC holds promise for improving treatment outcomes in locally advanced HNSCC. The findings underscore the need for further research involving a larger patient population to validate these preliminary results. Such validation could pave the way for a more effective and personalized therapeutic approach in the management of locally advanced HNSCC. Thus, suggesting that combining immunotherapy with induction chemotherapy followed by CCRT, and subsequent immune sequential therapy, may emerge as an effective treatment option for LA-HNSCC.
Despite the encouraging preliminary findings, our study is subject to several limitations that must be acknowledged. Firstly, the observational nature of our study design inherently introduces potential biases and challenges in controlling for unmeasured confounders and selection bias, which are common limitations of non-randomized studies. This may affect the robustness of our conclusions.
Secondly, the relatively small sample size limits the statistical power of our analyses, making it difficult to detect significant differences in PFS and OS between treatment groups. This also restricts our ability to perform more granular subgroup analyses, such as stratifying by PD-L1 expression levels or HPV status, which could provide deeper insights into treatment efficacy. The lack of statistical significance in PFS and OS, as well as the inability to conduct comprehensive stratified analyses, underscores the need for larger, more diverse patient cohorts in future studies.
Thirdly, the heterogeneity in treatment regimens, including the use of different PD-1 inhibitors and chemotherapy combinations, adds complexity to the interpretation of our results. While this reflects real-world clinical practice, it also introduces variability that can obscure the true effects of individual treatments.
Lastly, the short follow-up period precludes definitive conclusions about long-term outcomes, including the durability of response and the incidence of late toxicities. Longer-term follow-up is essential to fully assess the impact of these treatment regimens on patient survival and quality of life.
Conclusion
In summary, our study indicates that incorporating immunotherapy into IC may enhance PFS and OS in patients with LA-HNSCC. Although statistical significance was not achieved, the observed trends suggest potential benefits of this combination therapy. Further investigation in larger clinical trials is warranted to validate these findings and optimize treatment protocols for LA-HNSCC.
Data Sharing Statement
The datasets generated and analyzed during the current study are available from the corresponding author on reasonable request.
Ethical Approval
This retrospective study was approved by the Institutional Review Board of Peking University First Hospital (2020 scientific research 179, 2020-09-17). Given the retrospective nature of the study and the use of de-identified patient data, the requirement for informed consent was waived by the IRB. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by Wu Jieping Medical Foundation (320.6750.2020-10-112) and Peking University First Hospital cross-over clinical research (2022CR31).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Cohen EE, Karrison TG, Kocherginsky M, et al. Phase III randomized trial of induction chemotherapy in patients with N2 or N3 locally advanced head and neck cancer. J Clin Oncol. 2014;32(25):2735–2743.
2. Gong H, Tian S, Ding H, et al. Camrelizumab-based induction chemoimmunotherapy in locally advanced stage hypopharyngeal carcinoma: phase II clinical trial. Nat Commun. 2024;15(1):5251. doi:10.1038/s41467-024-49121-3
3. Haddad R, O’Neill A, Rabinowits G, et al. Induction chemotherapy followed by concurrent chemoradiotherapy (sequential chemoradiotherapy) versus concurrent chemoradiotherapy alone in locally advanced head and neck cancer (PARADIGM): a randomised Phase 3 trial. Lancet Oncol. 2013;14(3):257–264. doi:10.1016/S1470-2045(13)70011-1
4. Lorch JH, Goloubeva O, Haddad RI, et al. Induction chemotherapy with cisplatin and fluorouracil alone or in combination with docetaxel in locally advanced squamous-cell cancer of the head and neck: long-term results of the TAX 324 randomised phase 3 trial. Lancet Oncol. 2011;12(2):153–159. doi:10.1016/S1470-2045(10)70279-5
5. Burtness B, Harrington KJ, Greil R, et al. Pembrolizumab alone or with chemotherapy versus cetuximab with chemotherapy for recurrent or metastatic squamous cell carcinoma of the head and neck (KEYNOTE-048): a randomised, open-label, phase 3 study. Lancet. 2019;394(10212):1915–1928. doi:10.1016/S0140-6736(19)32591-7
6. Hong MH, Kim CG, Kim DH, et al. Preoperative durvalumab (D) with or without tremelimumab (T) for resectable head and neck squamous cell carcinoma (HNSCC). ESMO. 2021;32(S5):S787.
7. Huang X, Liu Q, Zhong G, et al. Neoadjuvant toripalimab combined with gemcitabine and cisplatin in resectable locally advanced head and neck squamous cell carcinoma (NeoTGP01): an open label, single-arm, phase Ib clinical trial. J Exp Clin Cancer Res. 2022;41(1):300. doi:10.1186/s13046-022-02510-2
8. Uppaluri R, Haddad RI, Tao Y, et al. Neoadjuvant and adjuvant pembrolizumab in locally advanced head and neck cancer. N Engl J Med. 2025;393(1):37–50. doi:10.1056/NEJMoa2415434
9. Huang H, Zhao Q, Zhang Y, et al. Immunotherapy advances in locally advanced and recurrent/metastatic head and neck squamous cell carcinoma and its relationship with human papillomavirus. Front Immunol. 2021;12:652054. doi:10.3389/fimmu.2021.652054
10. Uppaluri R, Chernock R, Mansour M, et al. Enhanced pathologic tumor response with two cycles of neoadjuvant pembrolizumab in surgically resectable, locally advanced HPV-negative head and neck squamous cell carcinoma (HNSCC). J Clin Oncol. 2021;6008:342S.
11. Machiels J, Tao Y, Burtness B, et al. Primary results of the phase III KEYNOTE-412 study: pembrolizumab (pembro) with chemoradiation therapy (CRT) vs placebo plus CRT for locally advanced (LA) head and neck squamous cell carcinoma (HNSCC). Ann Oncol. 2022;S808–S869.
12. Lee NY, Ferris RL, Psyrri A, et al. Avelumab plus standard-of-care chemoradiotherapy versus chemoradiotherapy alone in patients with locally advanced squamous cell carcinoma of the head and neck: a randomised, double-blind, placebo-controlled, multicentre, phase 3 trial. Lancet Oncol. 2021;22(4):450–462. doi:10.1016/S1470-2045(20)30737-3
13. Zheng S, Feng Y, Li C, et al. Induction therapy for locally advanced head and neck squamous cell carcinoma. Oncol Ther. 2023;11(2):185–198. doi:10.1007/s40487-023-00226-7
14. Harrington KJ, Burtness B, Greil R, et al. Pembrolizumab with or without chemotherapy in recurrent or metastatic head and neck squamous cell carcinoma: updated results of the phase III KEYNOTE-048 study. J Clin Oncol. 2023;41(4):790–802. doi:10.1200/JCO.21.02508
15. Spigel DR, Faivre-Finn C, Gray JE, et al. Five-year survival outcomes from the PACIFIC trial: durvalumab after chemoradiotherapy in stage III non-small-cell lung cancer. J Clin Oncol. 2022;40(12):1301–1311. doi:10.1200/JCO.21.01308
16. Zandberg DP, Clump DA, Isett BR, et al. A randomized phase II study of concurrent vs. sequential pembrolizumab with chemoradiation (CRT) in locally advanced head and neck cancer (LA HNSCC): 4-year results and tumor-immune microenvironment analysis. J Clin Oncol. 2023;34(suppl_2):S554–S593.
17. Rosenberg A, Juloori A, Agrawal N, et al. Neoadjuvant nivolumab, paclitaxel, and carboplatin followed by response-stratified chemoradiation in locoregionally advanced HPV negative head and neck squamous cell carcinoma (HNSCC): the DEPEND trial. J Clin Oncol. 2023;41(16_suppl):6007. doi:10.1200/JCO.2023.41.16_suppl.6007
18. Wu D, Li Y, Xu P, et al. A pilot phase II trial of neoadjuvant camrelizumab plus nab-paclitaxel and cisplatin (NeoCPC) for locoregionally advanced, resectable squamous cell carcinoma of the head and neck. J Clin Oncol. 2023;41(16_suppl):6069. doi:10.1200/JCO.2023.41.16_suppl.6069
19. Li X, Fang Q, Du W, et al. Induction chemotherapy combined with immunotherapy in locally advanced head and neck squamous cell carcinoma. BMC Cancer. 2021;21(1):622. doi:10.1186/s12885-021-08373-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of Sintilimab in Combination with Concurrent Chemoradiotherapy for Locally Advanced Gastric or Gastroesophageal Junction (GEJ) Adenocarcinoma (SHARED): Study Protocol of a Prospective, Multi-Center, Single-Arm Phase 2 Trial
Wei J, Lu X, Liu Q, Fu Y, Liu S, Li L, Liu F, Fan X, Yang J, Yang Y, Zhao Y, Guan W, Liu B
Cancer Management and Research 2022, 14:2007-2015
Published Date: 17 June 2022
Myasthenia Gravis-Like Symptoms Following Immune Checkpoint Inhibitor Therapy for Hepatocellular Carcinoma: A Case Report
Ha F, Wang H, Cai J, Liang J, Liu H
Cancer Management and Research 2025, 17:1819-1823
Published Date: 27 August 2025
Divergent Outcomes in Lung Adenocarcinoma with Paraneoplastic Hypereosinophilia in Patients Treated with Pembrolizumab: A Two-Case Report
Oza A, Stickler MB, Little FF
International Medical Case Reports Journal 2026, 19:550027
Published Date: 10 July 2026