Back to Journals » Clinical Interventions in Aging » Volume 18
Individualized Hospital to Home, Exercise-Nutrition Self-Managed Intervention for Pre-Frail and Frail Hospitalized Older Adults: The INDEPENDENCE Randomized Controlled Pilot Trial
Authors Han CY ![]() , Sharma Y
, Sharma Y ![]() , Yaxley A, Baldwin C
, Yaxley A, Baldwin C ![]() , Woodman R, Miller M
, Woodman R, Miller M
Received 17 January 2023
Accepted for publication 22 April 2023
Published 17 May 2023 Volume 2023:18 Pages 809—825
DOI https://doi.org/10.2147/CIA.S405144
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Chad Yixian Han,1 Yogesh Sharma,2,3 Alison Yaxley,1 Claire Baldwin,1 Richard Woodman,2 Michelle Miller1
1Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, Adelaide, SA, Australia; 2College of Medicine and Public Health, Flinders University, Adelaide, SA, Australia; 3Department of General Medicine, Flinders Medical Centre, Adelaide, SA, Australia
Correspondence: Chad Yixian Han, Caring Futures Institute, College of Nursing and Health Sciences, Flinders University, Sturt Road, Bedford Park, SA5042; GPO Box 2100, Adelaide, SA, 5001, Australia, Tel +61 8201 3911, Email [email protected]
Purpose: Pre-frailty and frailty in older adults are associated with poor health outcomes and increase health-care costs, and further worsening during hospitalization. This study aimed to examine the effect of an individualized hospital to home, exercise-nutrition self-managed intervention for pre-frail and frail hospitalized older adults.
Patients and Methods: Older adults admitted to an acute medical unit of a tertiary hospital in South Australia who were pre-frail or frail were recruited from September 2020 to June 2021, randomized to either control or intervention group and followed up at 3 and 6 months. The outcome variables were program adherence, frailty status by the Edmonton Frail Scale (EFS) score, lower extremity physical function, handgrip strength, nutritional status, cognition, mood, health-related quality of life, risk of functional decline, unplanned readmissions.
Results: Participants were 79.2 ± 6.6 years old, 63% female, mostly frail (67%), with EFS of 8.6± 1.9. Adherence to the inpatient and home visits/telehealth intervention were high (91± 13% and 92± 21%, respectively). Intention-to-treat analysis using linear regression models showed that participants in the intervention group had significantly greater reduction in EFS at 3 (− 3.0; 95% CI: − 4.8 to − 3.0) and 6 months (− 2.5; 95% CI: − 3.8 to − 1.0, P< 0.001 for both) compared to the control group; particularly the functional performance component. There were also improvements in overall Short Physical Performance Battery score at 3 (4.0; 95% CI: 1.3 to 6.6) and 6 months (3.9; 95% CI: 1.0 to 6.9, P< 0.05 for both), mini-mental state examination (2.6; 95% 0.3– 4.8, P=0.029) at 3 months and handgrip strength (3.7; 95% CI: 0.2– 7.1, P=0.039) and Geriatric Depression Scale, at 6 months (− 2.2; 95% CI: − 4.1 to − 0.30, P=0.026) in the intervention group as compared to control.
Conclusion: This study provided evidence of acceptability to a patient self-managed exercise-nutrition program that may benefit and alleviate pre-frailty and frailty in hospitalised older adults.
Keywords: frailty, self-management, exercise, nutrition therapy
Introduction
Frailty, as described by Fried et al, is a clinical syndrome in which three or more of the following conditions are present: unintentional weight loss, self-reported exhaustion, weak grip strength, slow walking speed, and low physical activity.1 Pre-frailty or intermediate frailty is defined as a state before frailty, in which an individual has one or two of the aforementioned criteria.1 It identifies those patients who are at a high risk of progression to frailty. Frailty and pre-frailty increase an individual’s vulnerability to higher dependency during/after periods of acute stress,2 and are associated with increased mortality.3 A previous study suggests that up to a quarter of individuals above the age of 85 may be frail.4 With a global ageing population, the prevalence of these geriatric syndromes is expected to increase in almost every country.5
The Australian and New Zealand Society for Sarcopenia and Frailty Research (ANZSSFR) Expert Working Group now recommends multifaceted interventions combining exercise and nutrition as part of management strategies for pre-frail and frail hospitalised older adults.6 Exercise and nutrition interventions have been suggested to be amongst the most effective to treat and prevent aspects of frailty.7 Exercise, in particular strength training, can improve muscle strength and reverse frailty.8 Similarly, individualized medical nutrition therapy (MNT) and counselling by a dietitian has been found to be associated with an improvement in nutritional status and clinical outcomes after 3 months of intervention.9 However, the authors from the ANZSSFR Working Group also reported that there were some inconsistencies from the results of the studies cited for their recommendations, especially since majority of randomized controlled trials (RCTs) that have investigated the effectiveness of combined exercise and nutrition interventions to reverse frailty, have been limited to otherwise well older adults from the community.6 More research is to be done on hospitalized older adults as hospitalization is a vulnerable period for older adults, especially if they are pre-frail or frail, because acute catabolic stress and physical deconditioning due to immobility and malnutrition can further aggravate this syndrome.10,11
Furthermore, potential limitations to the future scalability and sustainability of exercise-nutrition interventions for pre-frailty and frailty may also relate to the coordination and availability of care by different allied health-care professionals (eg, exercise and nutrition professionals). The sustainability of treatment effects should be considered in intervention design, such that a self-management model to target pre-frailty and frailty would appear to align well to the values and preferences of older adults about hospital to home care but has not been studied in this population previously.12 It is possible that a pre-frailty and frailty intervention which involves a more collaborative partnership approach with patients may be at least as beneficial as existing models but better reduce burden on healthcare resources.13 There is an evidence gap in the acceptability and benefits of self-managed exercise and nutrition interventions in hospitalised pre-frail and frail older adult patients.14
The INDividualized therapy for Elderly Patients using Exercise and Nutrition to reduce depenDENCE post discharge (INDEPENDENCE) pilot RCT aimed to examine the acceptability and benefits of an individualized community-extended, combined exercise and nutrition intervention on outcome variables that include pre-frailty, frailty (as assessed by Edmonton Frail Scale (EFS)) and frailty-related health outcomes. We hypothesize that such a self-managed program will have a good adherence rate and can alleviate pre-frailty and frailty, and improve frailty-related outcomes such as physical, nutritional status and mood. The results may provide guidance to clinicians and researchers looking to develop or implement self-managed exercise-nutrition program for pre-frail and frail hospitalized older adults.
Materials and Methods
Study Design
This study (INDEPENDENCE) was a pilot RCT conducted among older adults who were pre-frail or frail and hospitalised for an acute medical illness. The study was reported with the Consolidated Standards of Reporting Trials (CONSORT) statement – randomized pilot and feasibility trials,15 and the intervention was described with reference to the TIDieR checklist.16 This study was registered with the Australia New Zealand Clinical trials Register ACTRN 12619001367134.
Assessment of Pre-Frailty and Frailty
The EFS is commonly used to assess pre-frailty and frailty in hospitalised older adults.17 The EFS assesses nine domains contributing to pre-frailty and frailty – cognition, general health status, functional independence, social support, medication use, nutrition, mood, continence, and functional performance. The EFS score ranges from 0 to 17 points with higher scores indicative of a greater severity of frailty,18 and the total score categorises a patient into either non-frail; pre-frail; frail – a score of 6–7 indicates pre-frail and ≥8 indicates frail with the higher the number, the more severe the frailty (ie, mild (8–9), moderate (10–11), severe (≥12)).The EFS evaluates the highest number of clinical domains which makes it the most comprehensive assessment tool covering all physical, psychological, and social aspects of pre-frailty and frailty.
Participant Recruitment
Potential participants were patients admitted through the Acute Medical Unit (AMU) at the Flinders Medical Centre (FMC), Adelaide, South Australia. Participants who met the inclusion and exclusion criteria below were invited by the study’s research team to participate.
Inclusion and Exclusion Criteria
Older adults aged ≥65 years; residing within Southern Adelaide Local Health Network (SALHN); an EFS score ≥6; able to understand English instructions; without cognitive impairment (standardised mini-mental state examination (MMSE) ≥25); had access to a mobile or home phone were eligible. Those receiving palliative care, on home oxygen or assessed by treating physician as unsafe to participate were not eligible.
Sample Size Calculation
During the conception of this study, there was no RCT that had investigated the effect of an individualised hospital to home, self-managed combined exercise and nutrition intervention in pre-frail and frail hospitalised older adults. Hence, the study aimed to recruit 16 participants in each study arm, considering a minimal of 12 per group,19 and accounting for a 25% attrition rate.20 The proposed sample size also falls within the range reported in an audit of pilot trials.21 Moreover, to determine the statistical power of this study, post-hoc power estimates were calculated for the mean and SD EFS scores at 3 and 6 months, alpha level of 0.05.22
Randomization and Blinding
After screening, consent, enrolment, and baseline assessments, the recruiting research staff sent an identification number to a central research office, and the participant was randomized into either intervention or control group. The randomization schedule was created by an external research officer through computerised randomization using randomly permuted blocks, size of eight. Treatment codes were concealed in numbered opaque envelopes and opened by another research staff member not involved with participants directly, at the time of randomization. Therapists (for intervention delivery) and participants were aware of the allocated group, as it was not possible to blind them due to the nature of the intervention. However, the research staff that performed outcome assessments and data analyses were blinded to group allocation.
Control
Participants in the control group received usual care available to older adults in the local health network from their acute care and community services, from attending medical consultants, general practitioners, allied health, and nursing staff both during and post hospitalisation. The usual inpatient standard of care involved referral to allied health professionals (eg, dietitian, physiotherapist, occupational therapist) and/or other allied health care personnel such as allied health assistants, at the discretion of the participants’ treating medical team, with no dedicated outpatient follow-up plan.
Intervention
The design of the intervention was informed by a systematic review of exercise and nutrition interventions for pre-frail/frail hospitalised older adults.14 Participants assigned to the intervention group received an individualized exercise and nutrition care plan, by the research dietitian and physiotherapist, while admitted and that continued for 3-month post discharge, through an ambulatory service in the form of four home visits and four telephone calls (Table 1).
 |
Table 1 Outline of Default Participant Activities (for the Intervention Group) |
Exercise
In addition to any usual physiotherapy care, inpatient participants in the intervention group were offered a daily (on weekdays only) supervised physical activity program of up to 30 minutes duration that was individualized to their physical capabilities. Participants who were able to safely walk either independently or with minimal assistance (may include a gait aid) were firstly offered the opportunity to walk for as long as they could. Then with any remaining session time, they completed exercises adapted from the STAND-Cph trial.23 Participants who were physically dependent or unable to move away from the bedside completed the STAND-Cph program only. All participants were encouraged to work at their highest level of function for as long as they could. For the STAND-Cph component, following a range of motion “warm-up”, participants completed chair stand and heel raise exercises at their maximum tolerated intensity, with options for progression and regression as per the STAND-Cph program. Each of the two exercises followed a predefined progression model that allowed participants to complete three sets of 8–12 repetitions to fatigue. There are eight levels of difficulty to allow exercise from seated to unilateral positions with extra loads up to 8kg.
For the home-based exercise program, the focus was resistance training for completion 3 days a week along with muscle strengthening exercises which were derived from the Otago community exercise program.24 The original Otago exercise program consist of 17 strength (eg, knee extensor, hip adductor) and balance (eg, heel walking, one leg stand) exercises and a walking routine, performed three times per week. For this study, participants performed an adapted version. After a warm-up session of head, neck, trunk and ankle movement, and back extension, participants performed three sets of 8–10 repetitions to fatigue of the following six strengthening exercises: (1) front knee, (2) back knee, (3) side hip, (4) toe raises, (5) calf raises, and (6) sit-to-stand. This was individualized to personal capacity and the starting level is determined by the amount of ankle cuff weight (up to 8kg) the person can use to perform 8–10 repetitions before fatigue. The intervention did not include balance exercises because the home exercises were mostly performed unsupervised by the patients, and also to minimise participant burden and maximise adherence. Consistent with the Otago program, participants were also provided with advice about walking three times a week, in between strength training exercises.
Nutrition Therapy
For all participants, including those identified as malnourished (as ascertained by the Patient-generated Subjective Global Assessment (PG-SGA)), the research dietitian formulated an individualized nutrition care plan to maintain/improve diet quality with a focus on (1) ensuring 100% of their energy requirements to achieve ideal body weight, estimated from the Harris Benedict equation25 and (2) meeting the recommended protein intake (1–1.2g/kg body weight/d) to maintain and regain lean body mass.26 The Australian Guide to Healthy Eating was also referred to when optimising diet quality and ensuring sufficient hydration.27 For all intervention participants, depending on the participants’ nutrition status, comorbidities and dietary preferences and tolerances, the nutrition therapy provided included one or more of the following strategies – use of commercial oral nutrition supplements (selected within hospital’s inpatient formulary), mid-meal snacks (limited to hospital’s food service menu) and food fortification. Optimal care in terms of frequency of reviews and input was left to the discretion of the dietitian as individualized therapy varied between participants. Nutrition counselling delivered by the research dietitian, with a focus to augment energy and protein intake, was provided to participants prior to discharge to ensure continuity of the nutritional care plan at home. For participants who were well-nourished as per the PG-SGA, nutrition counselling prior to discharge was focused on optimisation of diet quality, protein intake, and hydration status. This was consistently followed through by the research dietitian from the time the participants were in hospital, and throughout the 3-month period of community care.
Self-Management
Uniquely, the program (all sessions within the intervention (ie, inpatient period, four telephone calls and four home visits)) was informed by a patient self-management model, providing a mechanism for participants to take the lead in reversing pre-frailty or frailty through independent exercises and nutritional self-care. This patient self-management model is adapted from the Flinders Chronic condition management model – a one-on-one patient-health provider approach, based on cognitive behavioural therapy, coupled with problem solving and motivational interviewing techniques.28 This involved the use of a 12-question partners in health module derived from four factors of chronic condition self-management – knowledge, coping, recognition and management of symptoms, adherence to treatment. These questions bring up discussion around knowledge about own health problems, medication, and treatments; health services and assessing them; symptom management; physical, social, and emotional impact of illness. Thereafter, there would be goal settings and formulation of a personalised care plan with the participant. As the information and instructions were rather extensive, each intervention participant was provided with a printed program guidebook (Supplementary Table 1 and Supplementary Figure 1), with all the above-mentioned information (ie, exercise, nutrition, chronic condition self-management).
Delivery of Intervention
In hospitals, each intervention session was supervised by an allied health professional, being a research dietitian who was trained by the project team to additionally deliver the exercise program in the scope of an allied health assistant. Program oversights were provided by each participant’s treating physiotherapist during inpatient stay. Participants were assisted to self-regulate their effort by monitoring perceived exertion, ensuring safe program delivery (ie, verbally report their perceived exertion and negotiate maximum exercise intensity using the BORG category ratio-10 scale), which was consistent with other similar studies in older adult populations with resistance training.29 Patients were asked to aim and maintain a perceived exertion rate of 3–4. For the post-discharge follow-ups, participants were guided by the same research dietitian with responsibilities for exercise program supervision akin to an allied health assistant, and who was also trained in the Flinders chronic condition self-management program; distance supervision by the research physiotherapist (available as needed by phone) was available to the research dietitian to facilitate the home exercise program. This intervention was designed to ensure continuity of care from hospital to home and build confidence in participants for self-management.
Patient and Public Involvement
To maintain a participatory/co-design approach while designing the protocol,30 the researchers took into consideration their findings from an earlier qualitative study (unpublished results) of hospitalised pre-frail/frail older adults ≥65 years, using the above protocol as reference. There was a consensus that the type of intervention delivered was familiar, manageable, and perceived as beneficial. The intervention period was also viewed as acceptable and not too lengthy. There was acceptance towards the intervention for (1) its emphasis on a patient-led self-managed approach that would be able to accommodate participants’ current situation (existing schedules and lifestyle; changing physical capabilities that required adaptive interventions), (2) its delivery by a trusted health provider whom participants would get acquainted with from the daily inpatient therapy and (3) its timeliness to attempt to treat the problem early. However, there appeared to be a unanimous agreement that the program was only for motivated older adults receptive to the idea of home visits. In addition, the use of an educational resource such as a printed booklet was also suggested to accompany the intervention.
Program Adherence
The degree of adherence to the intervention was recorded for completed intervention participants (1) attendance to the inpatient and home visits (recorded by the research staff who delivered), (2) mean adherence as a reasonable attempt at each 3×/week strength-focused training session as self-reported by participants in the exercise monitoring diaries in the education booklet and (3) percentage of energy and protein intake over estimated requirements as prescribed by the dietitian, as self-reported from the diet monitoring diaries in the education booklet.
Outcome Variables
The outcomes variables used to assess the benefits of the INDEPENDENCE program in pre-frail and frail hospitalised older adults improved the following outcomes at 3 and 6 months, compared to baseline (Table 2).
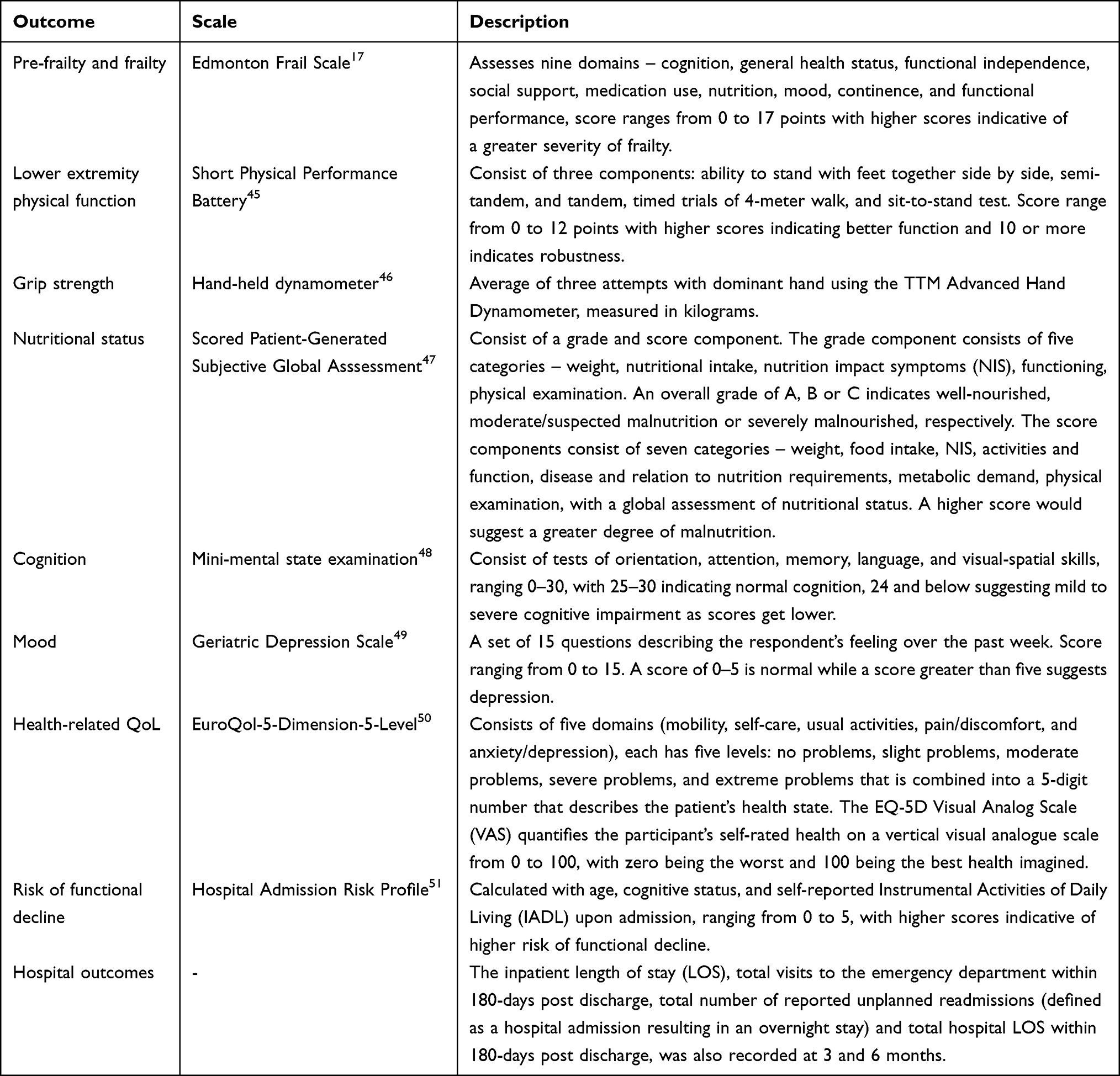 |
Table 2 Outcome Variables Measured for All Study Participants |
Adverse Events
Adverse events were monitored from baseline to 6-month follow-up, being defined as injuries or medical events due to participation in the trial/intervention that resulted in medical attention or restriction of daily living activities for more than 2 days.
Statistical Analyses
Participants were assessed at baseline (before randomization), 3 and 6 months. Treatment groups were coded to blind research staff involved in statistical tests prior to analyses. Normality tests (Kolmogorov–Smirnov and Shapiro–Wilk) showed normal distribution for all baseline measures, except PG-SGA and scored PG-SGA. Baseline data were described and compared with the use of independent sample t-tests or Mann–Whitney U-test for continuous data and chi square or Fisher’s exact test, for categorical data. The primary analyses were conducted with an intention-to-treat (ITT) principles with all participants randomized included in the analysis and assigned to the group they were randomized to regardless of their received treatment.31 Multiple imputation methods (Markov chain, Monte Carlo) were used to derive any missing data points, with 20 imputations carried out for each missing value for the ITT analyses.32 To determine differences between the groups at 3 and 6 months, we used linear regression models for continuous outcomes, with follow-up changes from baseline as dependent variables, and adjusted for baseline covariates.33 The effect sizes as measured by Cohen’s D for responsiveness of tools were calculated for EFS, GDS and MMSE.
Statistical analysis was performed using SPSS version 28 (SPSS Inc, Chicago, IL, USA). Statistical significance was set using a 2-sided Type 1 error rate of alpha=0.05 and differences between groups at 3- and 6-month follow-up were described as mean and standard deviation (SD) for continuous variables, as number (percent) for categorical variables, and differences between groups as mean difference with 95% confidence intervals (CI).
Results
Recruitment
A total of 1371 participants, who presented to the AMU at FMC from September 2020 to June 2021, were screened consecutively for participation in this study. A total of 723 (54%) patients screened were not eligible due to age <65 years. As per the CONSORT flow diagram in Figure 1, 32 participants were randomized into intervention and control groups each. Follow-up data from 75% (12/16) of the intervention and 100% (16/16) of the control group were available for analysis at 3 months. At 6 months, the availability of follow-up data was 75% (12/16) and 94% (15/16) of the intervention and control group, respectively. The follow-up attrition rate at 6-month period within the entire cohort was 16%, with 4/5 losses due to death.
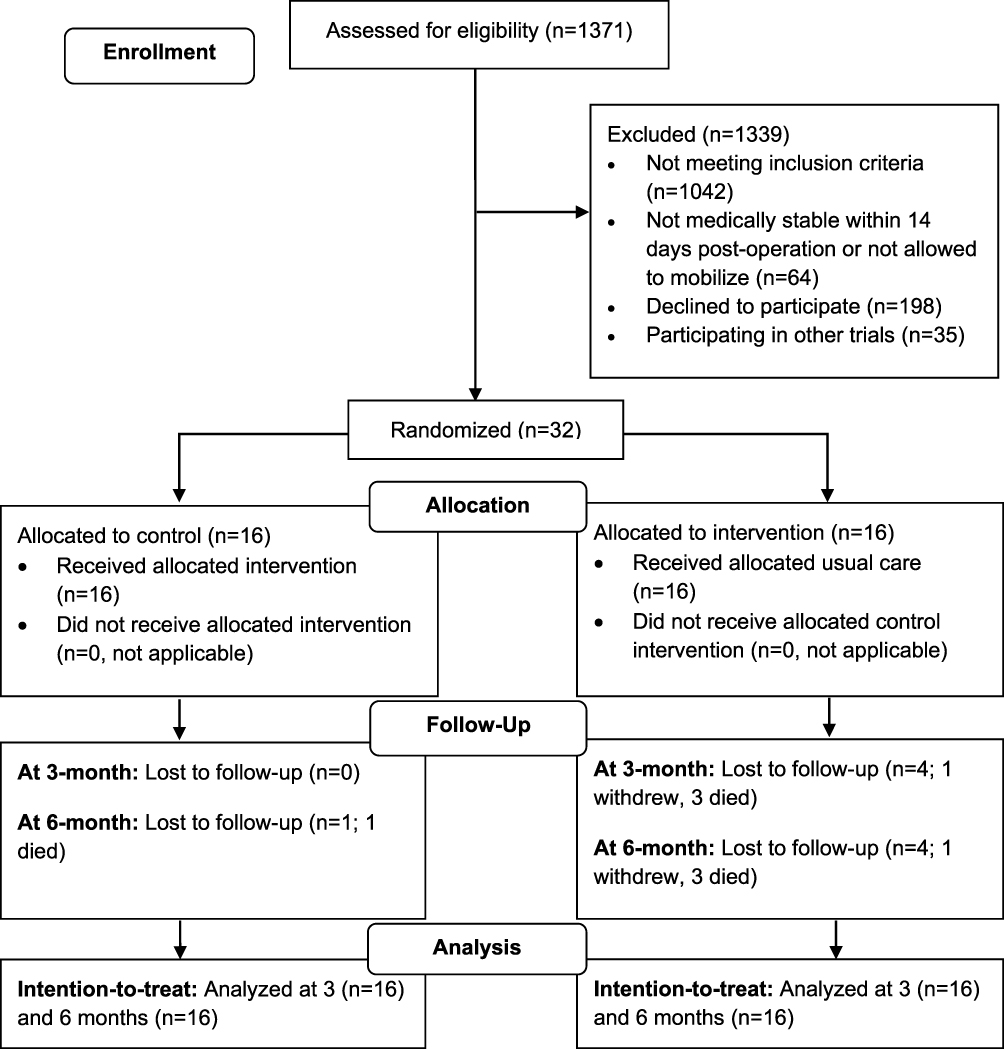 |
Figure 1 Overview of the Independence study with CONSORT Flow Diagram. Notes: Adapted from Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;355. Copyright: © 2016 Eldridge et al. Creative Commons Attribution License.15. |
Characteristics of the Study Population
Participant characteristics are shown in Table 3. Baseline characteristics between groups were well matched with the exceptions of overall SPPB, specifically the balance component (Table 4).
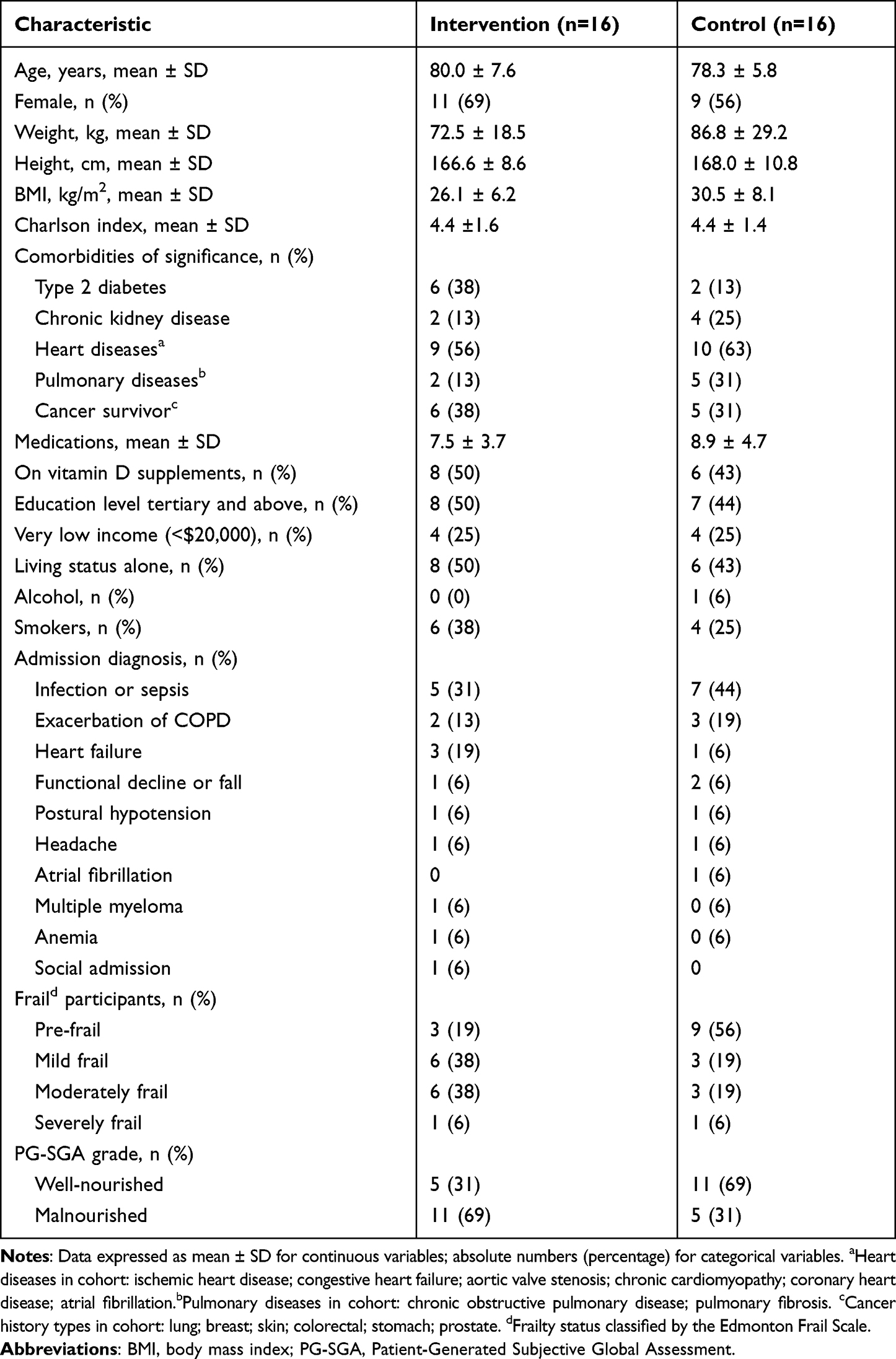 |
Table 3 Baseline Characteristics of Study Participants (n=32) |
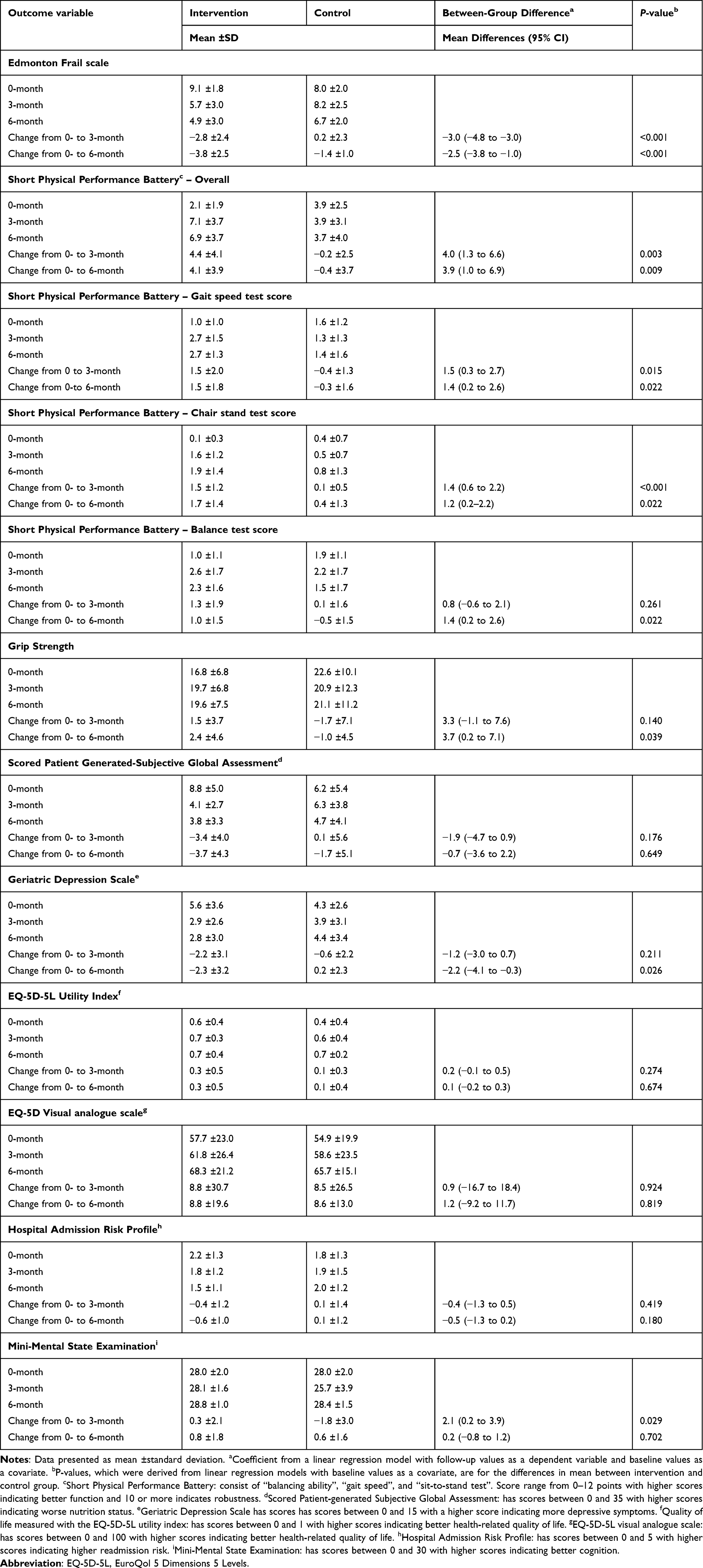 |
Table 4 Baseline and Effects of Intervention on Outcome Variables, Intention-to-Treat Analyses |
Adherence to Program in the Intervention Group
The mean ±SD percentage attendance (completion) of the inpatient and home visits/telehealth follow-ups were 91±13% and 92 ±21%, respectively. For the home-based component, the mean adherence to the exercise program was 66% ±33%. At home, the percentages of energy and protein requirement being met were 89% ±17% and 82% ±20%, respectively. The daily mean ±SD energy and protein intake were 1604 ±471kcal and 71.1 ±24.0g, respectively.
Responsiveness of Assessment Tools (EFS, GDS, MMSE)
The effect sizes using ITT analyses at 3 and 6 months were 0.91 and 0.71 for EFS; 0.35 and 0.50 for GDS, and 0.81 and 0.31 for MMSE, respectively.
Edmonton Frail Scale
As shown in Table 4, participants in the intervention group had a significantly greater reduction in EFS scores (indicative of an improvement in degree of pre-frailty and frailty) compared to those in the control group at both 3 and 6 months post randomization (P<0.001). At 3 months, the prevalence of frailty as identified by the EFS, was significantly higher in the control group when compared to those patients who were in the intervention group (14 out of 16, 88% vs 5 out of 12, 42%, P=0.028, respectively). At 6 months, there was a trend towards increasing prevalence of frailty in the control group when compared to the intervention group; however, this difference was not statistically significant (11 out of 15, 73% vs 4 out of 12, 33%, P=0.051, respectively).
Analyses of individual components of the EFS showed that changes in “Functional performance” was significantly different between groups at 3 (0.9, 95% CI: 0.3 to 1.5, P=0.003) and 6 months (1.0, 95% CI: 0.4 to 1.6, P=0.002), both with large effect size Cohen-D >1. Changes in “General health status” was significantly different between groups at 3 months (1.1, 95% CI: 0.2 to 2.0, P=0.017, Cohen D=0.6) but not 6 months. Changes in Functional independence was significant at 6 months (0.7, 95% CI: 0.1 to 1.3, P=0.018, Cohen D=0.4) but not at 3 months.
Other Outcomes
There were significantly greater improvements in total SPPB score in the intervention group compared to the control group, specifically in the sub-category of gait speed and chair-stand components, at both 3- and 6-month period. The significant difference in mean change from baseline between groups in SPPB-balance can be observed during 6-month follow-up but not immediately after the intervention at 3 months. Participants in the intervention group also had significantly greater improvements in cognition at 3 months, and handgrip strength and mood at 6 months. There was a trend towards an improved nutritional status, as determined by the PG-SGA score, in the intervention group at 3 months; however, this difference was not significant. It is noteworthy to mention that the proportion of well-nourished participants was trended to be higher for intervention than control at 3 (75% vs 56%), and 6 months (83% vs 67%), albeit not statistically significantly different. There were no significant differences between groups with respect to EQ-5D-5L UI and VAS, and HARP at 3 or 6 months in both PP and ITT analyses.
Length of Hospital Stay, Readmissions, and Visits to Emergency Department
There were no significant differences in inpatient LOS and total LOS of unplanned readmissions within 180-days post discharge between the two groups (Table 5). Although the total number of readmissions within 180 days post discharge were not significantly different between the two groups, there was a trend towards reduced hospital readmission rate in the intervention group when compared to the control group at both 3 months (33% versus 63%, P=0.132) and 6 months (25% versus 53%, P=0.431). Participants in the intervention group had significantly lesser visits to the emergency department compared to those in the control group.
 |
Table 5 Effects of Intervention on Clinical Outcomes, Intention-to-Treat Analyses |
Adverse Events
No adverse events or deaths due to the intervention, as defined as injuries or medical events due to the trial that result in medical attention or restriction of daily living activities for more than 2 days, were documented or reported to ethics.
Discussion
This study suggests preliminary evidence on acceptability and benefits of a new approach in pre-frailty and frailty care in hospitalised older adults. This intervention re-directed autonomy of care back to a selected group of patients, with an individualised hospital to home, self-managed, exercise-nutrition intervention and delivered in mixed modes (telehealth/in-person care) facilitated by an allied health assistant with support from a team of physiotherapist and dietitian. To the best of our knowledge, this study is one of the first pilot RCTs to evaluate the effects of such an intervention compared to usual care, to alleviate or reverse the progression of pre-frailty and frailty in hospitalised older adults.
In the acute setting, such self-managed, exercise-nutrition model of intervention seems practicable in older adults when delivered after an early detection of pre-frailty and frailty. The intervention was also well accepted, as reflected by good patient adherence to both supervised and non-supervised components in hospital and at home, and a low voluntary drop-out rate. The results also suggested that effects were durable as there were good retention of positive effects on pre-frailty and frailty at 6-month period. The medium-to-large effect size seen in the EFS and the 3-point mean difference (18% on the 17-point scale) can have a clinically meaningful impact on the degree of frailty and hence frailty status in this group of patients (eg, a mild-frail patient with the EFS=8), would be classified as non-frail after a 3-point improvement. However, the ability to draw any firm conclusions from the results is limited as this was a pilot study and the post-hoc power estimates of the EFS scores were <0.8 at both 3 and 6 months of follow-up.
The improvement in SPPB may be explained by the high adherence to both supervised and unsupervised exercise components of the program in this study. Cameron et al demonstrated that higher levels of adherence to intervention produce a greater effect on physical performance in the previous Frailty Intervention Trial.34 Another explanation may be that the exercises in the referenced study and within the INDEPENDENCE program were focused on strength training, and in particular functional sit-to-stand. The significant difference observed between total and individual SPPB component scores could have been affected by the baseline differences in the SPPB. It could also reflect different patient trajectories based on acquired ADL impairment as a result of hospitalisation.35 The improvement in balance scores at 6 months could be part of a general recovery trajectory of the participants post hospitalisation; however, this recovery could have been further accelerated by participation in the INDEPENDENCE trial, even though the exercises included in this trial did not specifically target balance. Conversely, the control group did not have such a trajectory and either plateaued (health took a hit) or continued to decline post hospitalisation. Future studies could also measure community participation or other changes in lifestyle/activity post-hospitalisation to elucidate this. Another possibility could be a far-reaching effect of the strength training exercises on balance and stability. Balance training has been shown to improve only the performance of trained tasks.36 However, strength training exercises can also benefit balance, as it is dependent on lower limb muscle strength.37 This suggests that strength training exercises might be prioritised when time for physical activities is limited in pre-frail/frail older adults.
In the intervention group, grip strength increased by 3.3 and 3.7kg at 3 and 6 months compared to the control group, although this difference was found to be significantly different only at 6-month follow-up. This finding is comparable to a study by Haider et al, who found that an intervention, involving physical activity-nutritional supplementation delivered by trained non-professionals for older adults with pre-frailty and frailty, improved grip strength by 2.4 kg in the intervention group when compared to their attention-controlled group.38 This study also found that participants who were frail were 2.8 times (95% CI: 1.0 to 7.7) more likely to benefit from the intervention than those who were assessed to be pre-frail. The proportion of participants who were pre-frail in both the referenced and present study was similar (34% vs 33%). Also, the INDEPENDENCE program did not include any upper limb or upper body-specific training, so with a program lacking that specificity, grip strength may not be expected to change. The significant change between groups at 6 months could also be contributed by a weaker baseline grip strength in the intervention compared to control (albeit not statistically significant). While the exercise program did not include upper body-specific training, the overall participant gains in change in frailty status and physical performance could also have encouraged a better engagement in a range of activities of daily living, and whole-body activities that could have influenced grip strength.
Nutritional status trended to improve more in the intervention group. However, the effect was not large enough to detect a difference with more rigorous ITT analyses nor at 6 months. A possible explanation of this could be that participants in the usual care group might have received nutritional therapy, improving their nutritional status, albeit at a slower rate than those in the intervention group. A recent qualitative study on older patient’s perception of nutritional care in the transition between hospital and home care highlighted the need for a comprehensive and individualized approach.39
Cognitive status as determined by the MMSE scores was significantly better in the intervention group when compared to the control group only at 3 months. This concurs with a trial examining physiotherapist-delivered exercise intervention with protein supplementation on frail older adults in the community (EFS: >8; MMSE ≥25), where MMSE was improved in intervention group but declined in control group (28.9 ±3.9 vs 25.9 ±7.3) post intervention.40 However, there was no follow-up data in that study. The short-term beneficial effects of intervention on cognition with later weaning of effect is unexplained, but it is possible that some control patients also received nutritional/physiotherapy intervention post discharge, which led to dilution of the beneficial effects of intervention.
The present study observed a trend of improvement in GDS in the intervention group at 3 months, and a significant difference between groups at 6 months. Exercise can improve mood in older adults, especially in those suffering from depression.41 Hence, the improvement in GDS could be attributed to good adherence to the exercise components of the INDEPENDENCE program. Furthermore, the nutrition intervention within the INDEPENDENCE program focuses on sufficient protein and encourages intake of foods such as olive oil, fish, fruits, vegetables, legumes, poultry, dairy, and meat (unprocessed). This could have contributed to the improvement in GDS as a dietary pattern high in consumption of these aforementioned foods have been associated with depression risk and suggested to improve depressive symptoms.42
The intervention had no remarkable effects on the quality of life as assessed by the EuroQoL questionnaire and on the risk of predicting functional decline as assessed by hospital admission risk profile (HARP) tool. Like grip strength, the effects of interventions on quality of life may also require a longer period to show effect.43 Therefore, additional studies should explore the effects of self-managed combined exercise and nutrition interventions on QoL using multiple or an assessment tool that is sensitive enough to measure as an older adult transit through different settings and have a longer follow-up period.
The HARP tool assesses risk of hospital admission by three factors related to hospital admissions – age, an abbreviated MMSE and reported independent instrumental activities of daily living (IADL). The lack of significance found between groups could be to the following three reasons. Firstly, age was a non-modifiable risk factor, and no intervention will be able to reverse that. Secondly, participants were all cognitively well and thus the abbreviated MMSE would not have been useful in this cohort to differentiate cognitive functions. Considering that both factors were less likely to be impacted by intervention, the HARP tool probably only measured one risk factor for hospital admission, which was independent IADL in this study.
In this study population, the incidence of unplanned hospital readmissions within 180-days post discharge was double for participants in the control group as compared to intervention, albeit not statistically significant. A large-scale study of over a million hospitalised frail older adults 65 years and above, admitted with coronary heart diseases, reported ascending trends of readmission rates as frailty risk increased.44 Hence, the INDEPENDENCE intervention should be further studied to assess its impact on clinical outcomes (ie, hospital readmission, LOS post discharge).
Strengths and Limitations
The novelty of this intervention was the application of a chronic disease care model to an otherwise recommended therapy (exercise-nutrition), to alleviate pre-frailty and frailty with a legacy effect. It offers new perspectives in the interim and as a step towards definitive studies, for anyone seeking to design, refine and test clinical pathways with a desire for sustainability in addressing such geriatric syndromes.
The study is not without limitations. Although it meets the sampling standards for a pilot study, it is not powered sufficiently and should only be used as a proof of concept. The results cannot be extrapolated to assume an improvement on hospital and economical outcomes at this stage. Hence, a larger, statistically powered clinical trial would be needed to confirm the evidence presented here and to further examine its impact on mortality rates, length of stay, and readmission rates. The inclusion of a cost-effectiveness analysis could further support its implementation and uptake by existing geriatric clinical services, if also found to be effective. Moreover, as discussed above, the findings are largely plausible and consistent with other emerging research. As the program was built around patient self-management, it may not be as useful for older adults with cognitive deficits affecting functional independence. The combined exercise-nutrition intervention also made it difficult to narrow down the individual components that contributed most to its effectiveness. However, it might not be necessary to differentiate between them because combined interventions have been suggested to tackle pre-frailty and frailty.6
Conclusion
In conclusion, this study provided proof of acceptability and adherence to a patient self-managed exercise-nutrition program that may reverse or slow down the progression of pre-frailty and frailty in hospitalised older adults. In a selected group of older adults, such a program might support patient autonomy, enabling them to maintain independence, through implementation of exercise and nutritional self-care. It is also important to note that results could change with longer follow-up beyond 6 months, and further research is required to assess the sustainability of such an intervention.
Abbreviations
BMI, body mass index; CCM, chronic condition management; CONSORT, Consolidated Standards of Reporting Trials; COREQ, Consolidated criteria for Reporting Qualitative; EFS, Edmonton Frail Scale; INDEPENDENCE, INDividualized therapy for Elderly Patients using Exercise and Nutrition to reduce depenDENCE post discharge; MMSE, mini-mental state examination; PG-SGA, Patient-Generated Subjective Global Assessment; SALHN, Southern Adelaide Local Health Network; SHARE-FI, Survey of Health Ageing and Retirement Frailty Instrument; SPPB, Short Physical Performance Battery; TFI, Tilburg frailty indicator.
Data Sharing Statement
The dataset generated and analyzed for the purpose of the present study is not publicly available due to data confidentiality requirements of the ethics committee but will be available from the corresponding author on reasonable request and approval from the ethics committee.
Ethics Approval and Informed Consent
The study was approved by the Southern Adelaide Clinical Human Research Ethics Committee (HREC reference number: REDACTED) − within which the work was undertaken and conforms to the provisions of the Declaration of Helsinki in 1995 (as revised in Edinburgh 2000). A written informed consent was obtained from each participant.
Acknowledgments
The authors would like to thank Dr Jenni Suen in helping with operations, and Ms Mitali Mukherjee for setting up the randomization for this study. All authors would also like to thank respective Heads of Departments and nurse managers at the Flinders Medical Centre for facilitating the study. Lastly, the authors would like to thank all older adults who helped advocate for the better care for pre-frailty and frailty through participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is partially supported by Flinders University’s College of Nursing and Health Sciences Research Student Maintenance and the Australian Government Research Training Program Scholarship. In addition, in kind support for the staff working on this project has been provided by the Flinders Medical Centre, Southern Adelaide Local Health Network. The funder had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M157. doi:10.1093/gerona/56.3.M146
2. Morley JE, Vellas B, Van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392–397. doi:10.1016/j.jamda.2013.03.022
3. Crow RS, Lohman MC, Titus AJ, et al. Mortality risk along the frailty spectrum: data from the National Health and Nutrition Examination Survey 1999 to 2004. J Am Geriatr Soc. 2018;66(3):496–502. doi:10.1111/jgs.15220
4. Song X, Mitnitski A, Rockwood K. Prevalence and 10‐year outcomes of frailty in older adults in relation to deficit accumulation. J Am Geriatr Soc. 2010;58(4):681–687. doi:10.1111/j.1532-5415.2010.02764.x
5. Cesari M, Prince M, Thiyagarajan JA, et al. Frailty: an emerging public health priority. J Am Med Dir Assoc. 2016;17(3):188–192. doi:10.1016/j.jamda.2015.12.016
6. Daly RM, Iuliano S, Fyfe J, et al. Screening, diagnosis and management of sarcopenia and frailty in hospitalized older adults: recommendations from the Australian and New Zealand Society for Sarcopenia and Frailty Research (ANZSSFR) expert working group. J Nutr Health Aging. 2022;26:1–15. doi:10.1007/s12603-022-1725-8
7. Negm AM, Kennedy CC, Thabane L, et al. Management of frailty: a systematic review and network meta-analysis of randomized controlled trials. J Am Med Dir Assoc. 2019;20(10):1190–1198. doi:10.1016/j.jamda.2019.08.009
8. de Labra C, Guimaraes-Pinheiro C, Maseda A, Lorenzo T, Millán-Calenti JC. Effects of physical exercise interventions in frail older adults: a systematic review of randomized controlled trials. BMC Geriatr. 2015;15(1):154. doi:10.1186/s12877-015-0155-4
9. Beck AM, Kjær S, Hansen BS, Storm RL, Thal-Jantzen K, Bitz C. Follow-up home visits with registered dietitians have a positive effect on the functional and nutritional status of geriatric medical patients after discharge: a randomized controlled trial. Clin Rehabil. 2013;27(6):483–493. doi:10.1177/0269215512469384
10. Brown CJ, Redden DT, Flood KL, Allman RM. The underrecognized epidemic of low mobility during hospitalization of older adults. J Am Geriatr Soc. 2009;57(9):1660–1665. doi:10.1111/j.1532-5415.2009.02393.x
11. Fisher SR, Goodwin JS, Protas EJ, et al. Ambulatory activity of older adults hospitalized with acute medical illness. J Am Geriatr Soc. 2011;59(1):91–95. doi:10.1111/j.1532-5415.2010.03202.x
12. Koenders N, Marcellis L, Nijhuis-van der Sanden MW, Satink T, Hoogeboom TJ. Multifaceted interventions are required to improve physical activity behaviour in hospital care: a meta-ethnographic synthesis of qualitative research. J Physiother. 2021;67(2):115–123. doi:10.1016/j.jphys.2021.02.012
13. Dineen-Griffin S, Garcia-Cardenas V, Williams K, Benrimoj SI. Helping patients help themselves: a systematic review of self-management support strategies in primary health care practice. PLoS One. 2019;14(8):e0220116. doi:10.1371/journal.pone.0220116
14. Han CY, Miller M, Yaxley A, Baldwin C, Woodman R, Sharma Y. Effectiveness of combined exercise and nutrition interventions in prefrail or frail older hospitalised patients: a systematic review and meta-analysis. BMJ open. 2020;10(12):e040146. doi:10.1136/bmjopen-2020-040146
15. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. BMJ. 2016;24:355.
16. Hoffmann TC, Glasziou PP, Boutron I, et al. Better reporting of interventions: template for intervention description and replication (TIDieR) checklist and guide. BMJ. 2014;348:g1687. doi:10.1136/bmj.g1687
17. Rolfson DB, Majumdar SR, Tsuyuki RT, Tahir A, Rockwood K. Validity and reliability of the Edmonton Frail Scale. Age Ageing. 2006;35(5):526–529. doi:10.1093/ageing/afl041
18. Perna S, Francis MDA, Bologna C, et al. Performance of Edmonton Frail Scale on frailty assessment: its association with multi-dimensional geriatric conditions assessed with specific screening tools. BMC Geriatr. 2017;17(1):1–8. doi:10.1186/s12877-016-0382-3
19. Julious SA. Sample size of 12 per group rule of thumb for a pilot study. Pharm Stat. 2005;4(4):287–291. doi:10.1002/pst.185
20. Serra-Prat M, Sist X, Domenich R, et al. Effectiveness of an intervention to prevent frailty in pre-frail community-dwelling older people consulting in primary care: a randomised controlled trial. Age Ageing. 2017;46(3):401–407. doi:10.1093/ageing/afw242
21. Billingham SA, Whitehead AL, Julious SA. An audit of sample sizes for pilot and feasibility trials being undertaken in the United Kingdom registered in the United Kingdom Clinical Research Network database. BMC Med Res Methodol. 2013;13(1):1–6. doi:10.1186/1471-2288-13-104
22. Rosner B. Fundamentals of Biostatistics.
23. Pedersen MM, Petersen J, Beyer N, Damkjaer L, Bandholm T. Supervised progressive cross-continuum strength training compared with usual care in older medical patients: study protocol for a randomized controlled trial (the STAND-Cph trial). Randomized Controlled Trial Research Support, Non-U.S. Gov’t. Trials. 2016;17:176.
24. Robertson MC, Campbell AJ, Gardner MM, Devlin N. Preventing injuries in older people by preventing falls: a meta‐analysis of individual‐level data. J Am Geriatr Soc. 2002;50(5):905–911. doi:10.1046/j.1532-5415.2002.50218.x
25. Alix E, Berrut G, Boré M, et al. Energy requirements in hospitalized elderly people. J Am Geriatr Soc. 2007;55(7):1085–1089. doi:10.1111/j.1532-5415.2007.01236.x
26. Bauer J, Biolo G, Cederholm T, et al. Evidence-based recommendations for optimal dietary protein intake in older people: a position paper from the PROT-AGE Study Group. J Am Med Dir Assoc. 2013;14(8):542–559. doi:10.1016/j.jamda.2013.05.021
27. Gopinath B, Russell J, Flood VM, Burlutsky G, Mitchell P. Adherence to dietary guidelines positively affects quality of life and functional status of older adults. J Acad Nutr Diet. 2014;114(2):220–229. doi:10.1016/j.jand.2013.09.001
28. Battersby M, Harris M, Smith D, Reed R, Woodman R. A pragmatic randomized controlled trial of the Flinders Program of chronic condition management in community health care services. Patient Educ Couns. 2015;98(11):1367–1375. doi:10.1016/j.pec.2015.06.003
29. Morishita S, Tsubaki A, Nakamura M, Nashimoto S, Fu JB, Onishi H. Rating of perceived exertion on resistance training in elderly subjects. Expert Rev Cardiovasc Ther. 2019;17(2):135–142. doi:10.1080/14779072.2019.1561278
30. Langley J, Wolstenholme D, Cooke J. ‘Collective making’as knowledge mobilisation: the contribution of participatory design in the co-creation of knowledge in healthcare. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-3397-y
31. Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res. 2011;2(3):109. doi:10.4103/2229-3485.83221
32. Lane P. Handling drop‐out in longitudinal clinical trials: a comparison of the LOCF and MMRM approaches. Pharm Stat. 2008;7(2):93–106. doi:10.1002/pst.267
33. Vickers AJ, Altman DG. Analysing controlled trials with baseline and follow up measurements. BMJ. 2001;323(7321):1123–1124. doi:10.1136/bmj.323.7321.1123
34. Cameron ID, Fairhall N, Langron C, et al. A multifactorial interdisciplinary intervention reduces frailty in older people: randomized trial. BMC Med. 2013;11(1):1–10. doi:10.1186/1741-7015-11-65
35. Boyd CM, Landefeld CS, Counsell SR, et al. Recovery of activities of daily living in older adults after hospitalization for acute medical illness. J Am Geriatr Soc. 2008;56(12):2171–2179. doi:10.1111/j.1532-5415.2008.02023.x
36. Kümmel J, Kramer A, Giboin LS, Gruber M. Specificity of balance training in healthy individuals: a systematic review and meta-analysis. Sports Med. 2016;46(9):1261–1271. doi:10.1007/s40279-016-0515-z
37. Lopez P, Pinto RS, Radaelli R, et al. Benefits of resistance training in physically frail elderly: a systematic review. Aging Clin Exp Res. 2018;30(8):889–899. doi:10.1007/s40520-017-0863-z
38. Haider S, Dorner TE, Luger E, et al. Impact of a home-based physical and nutritional intervention program conducted by lay-volunteers on handgrip strength in prefrail and frail older adults: a randomized control trial. PLoS One. 2017;12(1):e0169613. doi:10.1371/journal.pone.0169613
39. Hestevik CH, Molin M, Debesay J, Bergland A, Bye A. Older patients’ and their family caregivers’ perceptions of food, meals and nutritional care in the transition between hospital and home care: a qualitative study. BMC Nutr. 2020;6(1):1–13. doi:10.1186/s40795-020-00335-w
40. Tarazona-Santabalbina FJ, Gómez-Cabrera MC, Pérez-Ros P, et al. A multicomponent exercise intervention that reverses frailty and improves cognition, emotion, and social networking in the community-dwelling frail elderly: a randomized clinical trial. J Am Med Dir Assoc. 2016;17(5):426–433.
41. Catalan-Matamoros D, Gomez-Conesa A, Stubbs B, Vancampfort D. Exercise improves depressive symptoms in older adults: an umbrella review of systematic reviews and meta-analyses. Psychiatry Res. 2016;244:202–209. doi:10.1016/j.psychres.2016.07.028
42. Lang UE, Beglinger C, Schweinfurth N, Walter M, Borgwardt S. Nutritional aspects of depression. Cell Physiol Biochem. 2015;37(3):1029–1043. doi:10.1159/000430229
43. Haraldstad K, Wahl A, Andenæs R, et al. A systematic review of quality of life research in medicine and health sciences. Qual Life Res. 2019;28(10):2641–2650. doi:10.1007/s11136-019-02214-9
44. Davis-Ajami ML, Chang P-S WJ. Hospital readmission and mortality associations to frailty in hospitalized patients with coronary heart disease. Aging Health Res. 2021;1(4):100042. doi:10.1016/j.ahr.2021.100042
45. Guralnik JM, Simonsick EM, Ferrucci L, et al. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85–M94. doi:10.1093/geronj/49.2.M85
46. Schaubert KL, Bohannon RW. Reliability and validity of three strength measures obtained from community-dwelling elderly persons. J Strength Cond Res. 2005;19(3):717. doi:10.1519/R-15954.1
47. Thomas J, Isenring E, Kellett E. Nutritional status and length of stay in patients admitted to an Acute Assessment Unit. J Hum Nutr Diet. 2007;20(4):320–328. doi:10.1111/j.1365-277X.2007.00765.x
48. Pangman VC, Sloan J, Guse L. An examination of psychometric properties of the mini-mental state examination and the standardized mini-mental state examination: implications for clinical practice. Appl Nurs Res. 2000;13(4):209–213. doi:10.1053/apnr.2000.9231
49. Incalzi RA, Cesari M, Pedone C, Carbonin P. Construct validity of the 15-item geriatric depression scale in older medical inpatients. J Geriatr Psychiatry Neurol. 2003;16(1):23–28. doi:10.1177/0891988702250532
50. Oppe M, Devlin NJ, Szende A. EQ-5D Value Sets: Inventory, Comparative Review and User Guide. Springer; 2007.
51. Sager MA, Rudberg MA, Jalaluddin M, et al. Hospital admission risk profile (HARP): identifying older patients at risk for functional decline following acute medical illness and hospitalization. J Am Geriatr Soc. 1996;44(3):251–257. doi:10.1111/j.1532-5415.1996.tb00910.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.