Back to Journals » Clinical Epidemiology » Volume 14
Indirect Comparisons via Sorafenib for the Comparative Effectiveness of Two PD-1/PD-L1 Inhibitors to Treat Advanced Hepatocellular Carcinoma Patients without Prior Systemic Therapies
Authors Jiang Y ![]() , Cai D, Shi S
, Cai D, Shi S
Received 9 December 2021
Accepted for publication 8 March 2022
Published 29 April 2022 Volume 2022:14 Pages 581—590
DOI https://doi.org/10.2147/CLEP.S352045
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Irene Petersen
Yawen Jiang, Dan Cai, Si Shi
School of Public Health (Shenzhen), Sun Yat-sen University, Shenzhen, Guangdong, People’s Republic of China
Correspondence: Yawen Jiang, School of Public Health (Shenzhen), Shenzhen Campus of Sun Yat-sen University, NO. 66 Gongchang Road, Guangming District, Shenzhen, Guangdong, People’s Republic of China, Tel +86 13266737281, Email [email protected]
Introduction: Advanced hepatocellular carcinoma (HCC) represents a major public health threat. Several emerging combination therapies have shown promising results for the first-line treatment of advanced HCC. The present study compared the efficacy of atezolizumab plus bevacizumab (AB) with lenvatinib plus pembrolizumab (LP), which were two of the leading combination therapies.
Methods: The outcomes of the present analysis were overall survival (OS) time and progression-free survival (PFS) time. Two matching-adjusted indirect comparisons (MAICs) were first conducted using the individual-level patient data (IPD) of the sorafenib arm from a previous clinical trial and the aggregate data (AgD) of the AB and LP arms from the corresponding published trials. From the MAICs, the hazard ratios (HRs) of AB and LP vs sorafenib were estimated by conducting weighted Cox regressions. The HRs from the two MAICs were then pooled to conduct a second-order indirect comparison of AB vs LP.
Results: In the MAIC analyses, AB had better efficacy on both OS (HR: 0.58, 95% CI: 0.42– 0.79) and PFS (HR: 0.59, 95% CI: 0.47– 0.76) than sorafenib, whereas LP had significantly better efficacy on PFS (HR: 0.62, 95% CI: 0.41– 0.94) but not OS (HR: 0.83, 95% CI: 0.52– 1.32). In the second-order comparison, AB was insignificantly more efficacious on OS (HR: 0.71, 95% CI: 0.42– 1.23) than and similarly efficacious on PFS (HR: 0.95, 95% CI: 0.60– 1.51) as the LP regimen.
Conclusion: LP regimen may be a potential first-line immunotherapy option for advanced HCC given its comparative effectiveness in relation to AB.
Keywords: matching, adjusted, overall, progression-free, survival, PD-1, PD-L1, balancing, first-line, unresectable
Introduction
Causing more cancer-related mortality than any other tumor types except lung cancer,1,2 hepatocellular carcinoma (HCC) poses as a major threat to population health worldwide. Accounting for approximately 80% of all cases, Asian countries are heavily disproportionately afflicted by HCC.3 For example, China alone was home to about half of the world HCC population.4 The substantial disease burden of HCC is only matched by the currently unmet need in the management of HCC patients, the filling of which requires continuous scientific research and evidence generation.
Characterized by macrovascular invasion and extrahepatic metastases, advanced HCC represents a prominent clinical challenge.2 At the advanced stage, patients are usually recommended to receive systemic therapies.1,2,5 However, the efforts in the past decades to identify effective therapies have been unproductive until very recently.5 Until 2017, sorafenib was the only first-line drug treatment with proven survival benefit among advanced HCC patients.4 However, recent evidence suggests that the efficacy of sorafenib may be hampered by acquired tyrosine kinase inhibitor resistance.6 Featured by non-inferiority to sorafenib, lenvatinib became another drug approved by the US Food and Drug Administration (FDA) and European Medicines Agency (EMA) for the first-line treatment of advanced HCC in 2018. More recently, combination therapies are gaining prominence,5 among which programmed cell death receptor 1 (PD-1)/programmed cell death ligand 1 (PD-L1) inhibitors are the leading new constitutions.7–9 Blocking the PD-1/PD-L1 signaling pathways can effectively relieve immune escape, thereby fortifying T cell-mediated anti-tumor immunity.10 To date, the forerunner of the PD-1/PD-L1-enabled combination regimens is atezolizumab plus bevacizumab (hereinafter referred to as AB).8,9,11,12 The IMbrave150 Phase III trial, which randomized 501 advanced HCC patients to atezolizumab plus bevacizumab or sorafenib, showed that AB significantly improved both overall survival (OS) and progression-free survival (PFS) over sorafenib.11 In the subgroup analysis of IMbrave150 using the Chinese samples, a significant improvement in OS and PFS associated with AB was also observed.12 Due to its favorable efficacy profile, AB has been approved by FDA for the first-line treatment and granted an upfront position by several guidelines in the therapies of advanced HCC.8,9 Another PD-1/PD-L1-based combination regimen with the potential to become a first-line therapy is lenvatinib plus pembrolizumab (hereinafter referred to as LP).8 In the single-arm phase Ib KEYNOTE 524 trial that enrolled 100 patients, LP-treated patients showed promising results of having a median OS of 22 months and a median PFS of 9.3 months. Despite such clinically meaningful data readings, FDA held off on the approval of LP for the first-line treatment of advanced HCC based on KEYNOTE 524 trial.13 Therefore, further evidence is necessary to understand the value of LP in the hierarchy of HCC therapies, some efforts towards which are ongoing. In light of the remarkable progresses in the therapies of advanced HCC, it is important to gain insight into the comparative effectiveness profiles of these novel therapies. To facilitate informed clinical decision-making, the present study aimed to fill the evidentiary gap in the comparative efficacy of AB in relation to LP for the first-line treatment of advanced HCC.
Since KEYNOTE 524 trial only had one arm, meta-analyses to compare AB and LP were not possible,14 which was likely an important reason why existing meta-analyses of first-line PD-1/PD-L1 therapies of advanced HCC did not account for LP.10,15 To compare therapies based on single-arm trials, matching-adjusted indirect comparisons (MAIC) that exploit the individual-level patient data (IPD) of one treatment and the published aggregate data (AgD) of another treatment are frequently used.16–18 However, MAIC only evaluates the regimen in the IPD against that in the AgD. In the setting of the current study, only AgD were available to both IMbrave150 and KEYNOTE 524 trials. As such, we exploited the IPD of the sorafenib arm in a previous trial to conduct and link the MAICs of sorafenib versus AB and LP.
Methods
Overall Analytic Strategy
To compare AB and LP in the absence of common comparators and the availability of the IPD of either trial, at least one set of IPD of a third drug in the same treatment class was necessary. Specifically, the IPD of the sorafenib arm in a trial that compared sunitinib and sorafenib for the first-line treatment of advanced HCC was used.19 The sorafenib arm IPD from this trial has several desirable features. First, the sunitinib vs sorafenib trial was also conducted in an advanced HCC population to evaluate front-line treatments. Second, the comparator drug for AB in the IMbrave150 trial was sorafenib, the comparative results of which can be used to validate MAIC results. Third, the sorafenib arm IPD had already been made publicly available online, which circumvented the challenges in securing access to proprietary information.
In the present analysis, sorafenib IPD was first compared to the AB arm in the IMbrave150 trial using MAIC. The same approach was used to compare sorafenib IPD to the LP arm in the KEYNOTE 524 trial. The comparative efficacy results from the two MAICs were further synthesized to obtain the effects of AB in relation to LP since both MAICs shared the comparator of sorafenib. The overall comparison strategy is illustrated in Figure 1.
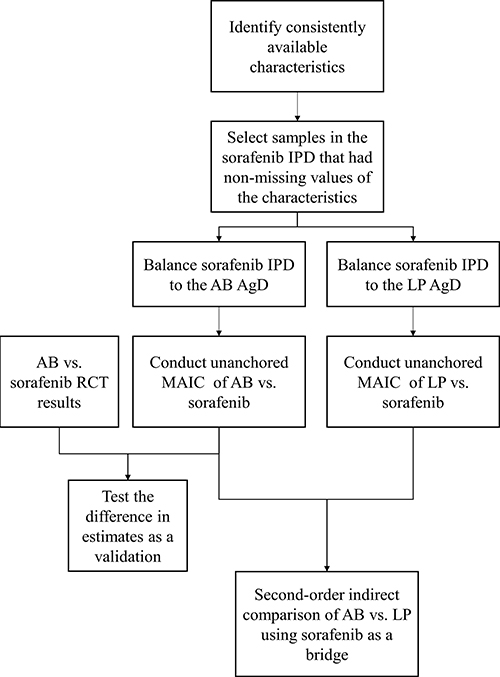 |
Figure 1 Flowchart of matching-adjusted indirect comparisons (MAIC), the validation of the MAIC method, and the second-order indirect comparison. |
The present study used de-identified secondary data that were publicly available and data from the literature. Hence, it was exempted from ethical reviews per local policies, which was confirmed in paper by the Human Studies Ethical Review Committee of Sun Yat-sen University School of Public Health (Shenzhen) (NO. 2021[053]).
Outcomes
Although not all the abovementioned trials shared the same primary and secondary endpoints, they did include the common outcomes of overall survival (OS) time and progression-free survival (PFS) time.11,19,20 OS and PFS are also critical efficacy endpoints commonly used to sketch the clinical profiles of anti-cancer medications therapeutics.4,8,9,21 Therefore, the outcomes in the present study were also chosen to be OS and PFS. The comparative efficacy estimates were represented by hazard ratios (HRs).
MAIC
To evaluate an existing treatment against a new treatment for which only AgD from a single-arm trial is available, the MAIC method utilizes the IPD from the trial of the existing treatment and re-weights the IPD such that their characteristics are balanced with those of the patients from the trial of the new treatment.16 The outcomes of the re-weighted IPD are then compared with the AgD of the new treatment.16 For linear outcomes such as mean values and percentages, the outcomes from re-weighted IPD and AgD can be directly compared. However, additional steps are necessary when the outcomes are time to event in nature such as those in the present study. To evaluate the HRs of OS and PFS, regression techniques such as Cox regressions should be conducted, which requires the reconstructed IPD of the new treatment’s AgD. The reconstruction was fulfilled by digitizing the published Kaplan–Meier (K-M) curves of OS and PFS using established techniques.22,23
In the current analysis, characteristics that were available in all trials were chosen to balance patients, the implementation of which was based on entropy balancing (EB). The EB process created weights that could be used to align the characteristics of the IPD with those of the AgD in subsequent analyses.17,18 Using this process, sorafenib IPD were first balanced to the AB AgD, following which the effective sample size (ESS) with the EB weights was also calculated. After the EB process, the OS and PFS K-M curves of the AB arm in the IMbrave150 trial were then digitized using Engauge Digitizer 10.11 to reconstruct the corresponding individual-level survival data with an established method.22,24 The reconstructed survival data of the AB arm were then pooled with the re-weighted sorafenib IPD to estimate the HRs of AB vs sorafenib with regard to OS and PFS using weighted Cox regressions. The HRs in this set of MAIC were denoted by  and
and  . These metrics represented the OS and PFS benefits of AB in relation to sorafenib had the sorafenib arm IPD patients looked the same as the AB arm patients in the IMbrave150 trial.
. These metrics represented the OS and PFS benefits of AB in relation to sorafenib had the sorafenib arm IPD patients looked the same as the AB arm patients in the IMbrave150 trial.
The process of the LP vs sorafenib MAIC followed that of the AB vs sorafenib MAIC. Accordingly, the HRs were denoted as  and
and  .
.
Validation of the MAIC Approach
The specification of the covariates for EB relied on the availability of information. However, whether the covariates included in the analysis were adequate to mitigate bias due to patient population heterogeneity could not be tested. As such, alternative approaches should be taken to examine the validity of the MAIC analyses. Since the IMbrave150 trial randomized patients to AB and sorafenib regimens, the results from the trial could be compared against the MAIC results of  and
and  . If the MAIC results and the IMbrave150 trial results had good similarity, then the MAIC specification in the current study for advanced HCC patients requiring first-line therapies might be relatively reliable. To that end, we tested
. If the MAIC results and the IMbrave150 trial results had good similarity, then the MAIC specification in the current study for advanced HCC patients requiring first-line therapies might be relatively reliable. To that end, we tested  and
and  against the counterpart estimates from the IMbrave150 trial. The absence of statistical significance was considered favorable evidence of the validity of the MAIC approach.
against the counterpart estimates from the IMbrave150 trial. The absence of statistical significance was considered favorable evidence of the validity of the MAIC approach.
The validity of the MAIC model specification was also necessary to prescribe the use of the second-order indirect comparison, which required the lack of residual effect modifiers. In other words, the comparative effectiveness of each of the regimens over sorafenib and in relation to each other were independent of factors that were not already considered. Although residual effect modifiers were likely to exist, they had minor chances of biasing the effect estimates if they had strong correlation with the ones already adjusted for. The validity of the MAIC approach wrapped up these conditions required to rule out residual effect modifiers.
Second-Order Indirect Comparison
Following the MAIC estimation, the ratio of the AB-sorafenib HR to the LP-sorafenib HR for each of the outcome was taken. The second-order indirect comparison resembled the Bucher’s method.25 Specifically, the final estimate of the HR of OS comparing AB with LP,  , was calculated as
, was calculated as 
Similarly, the final estimate of the HR of PFS comparing AB with LP,  , was calculated as
, was calculated as

In the estimation of the standard errors of  , the standard errors of both preceding HRs used in the calculation were taken into account to comprehensively capture the uncertainty of the estimates. The same approach was also used in the estimation of
, the standard errors of both preceding HRs used in the calculation were taken into account to comprehensively capture the uncertainty of the estimates. The same approach was also used in the estimation of  .
.
Robustness Check
Although the validation of the MAIC approach represents a useful technique to provide evidence on potential bias due to omitted prognostic factors and effect modifiers or lack thereof, it does not quantify the robustness of estimates to such bias. To that end, we engaged E-values to examine the robustness of our estimates to unobserved prognostic factors and effect modifiers. The E-value quantifies the minimal amount of correlation an unmeasured confounder would need to have with both the treatment exposure and a certain outcome to nullify the observed treatment effect in the scale of hazard ratio conditional on the measured covariates.26 Accordingly, the greater the E-value, the more robust the HR estimates.
Results
After comparing the available and reported information across trials, 12 common variables were identified and used to balance baseline characteristics across studies. Of note, all of the variables were reported as percentages in the AgD of the IMbrave150 and KEYNOTE 524 trials. Namely, the variables were whether aged 65 years and older, male, Asian, Black, White (other races used as the reference category), Eastern Cooperative Oncology Group performance status (ECOG PS), extrahepatic spread, macrovascular invasion, α-fetoprotein level (AFP) ≥400 ng/mL, and three classifications of etiology (hepatitis B, hepatitis C, and alcohol abuse). The characteristics are listed in Table 1, which also describes the differences of the patients before and after EB with weights. In the sorafenib IPD, 533 patients with non-missing information on all covariates were selected for subsequent analyses. Before EB, the 533 patients from the sorafenib IPD were significantly different from the AB arm in the percentages of 65 years and older patients (36% vs 48%, p < 0.001), Asian patients (78% vs 56%, p < 0.001), White patients (20% vs 37%, p < 0.001), patients with a ECOG PS score of 1 (46% vs 38%, p < 0.001), patients with macrovascular invasion (28% vs 38%, p < 0.001), patients who had baseline AFP ≥ 400 ng/mL (48% vs 38%, p < 0.001), patients with an etiology of hepatitis B (54% vs 49%, p < 0.001), and patients with an etiology of alcohol abuse (14% vs 10%, p < 0.001). To visualize the overall imbalance across the IPD and AgD, the kernel density of the entropy balancing weights of sorafenib arm IPD when balanced to the AB and LP AgD is presented in Figure 2. The deviation and dispersion of each kernel density line from the black vertical line demonstrate the imbalance of sorafenib IPD and the aggregate data of the corresponding comparator regimen before entropy balancing. The dissimilarity of the two kernel density lines of entropy balancing weights represents the imbalance between the aggregate data of the AB and LP arms. The differences across the sorafenib IPD and the AgD of the AB arm were substantially reduced through the EB process. Specifically, the re-weighted sorafenib IPD did not have significant differences in any of the characteristics compared with the AgD of the AB arm after EB. When the sorafenib IPD were compared with the LP arm, the differences in the characteristics before EB were even more pronounced than those with the AB arm. Specifically, the 533 sorafenib arm patients had significant differences in the percentages of 65 years and older patients (36% vs 62%, p < 0.001), male patients (84% vs 81%, p = 0.041), Asian patients (78% vs 28%, p < 0.001), White patients (20% vs 51%, p < 0.001), patients with a ECOG PS score of 1 (46% vs 38%, p < 0.001), patients with extrahepatic spread of disease (65% vs 52%, p < 0.001), patients with macrovascular invasion (28% vs 20%, p < 0.001), patients who had baseline AFP ≥ 400 ng/mL (48% vs 30%, p < 0.001), patients with an etiology of hepatitis B (54% vs 19%, p < 0.001), patients with an etiology of hepatitis C (22% vs 36%, p < 0.001), and patients with an etiology of alcohol abuse (14% vs 28%, p < 0.001). Similar to the AB arm, the EB process for the sorafenib IPD data and the AgD of the LP arm resulted in balanced characteristics without significant differences. Moreover, the ESS of the AB-weighted sorafenib IPD was 277, whereas that of the LP-weighted sorafenib IPD was 65.
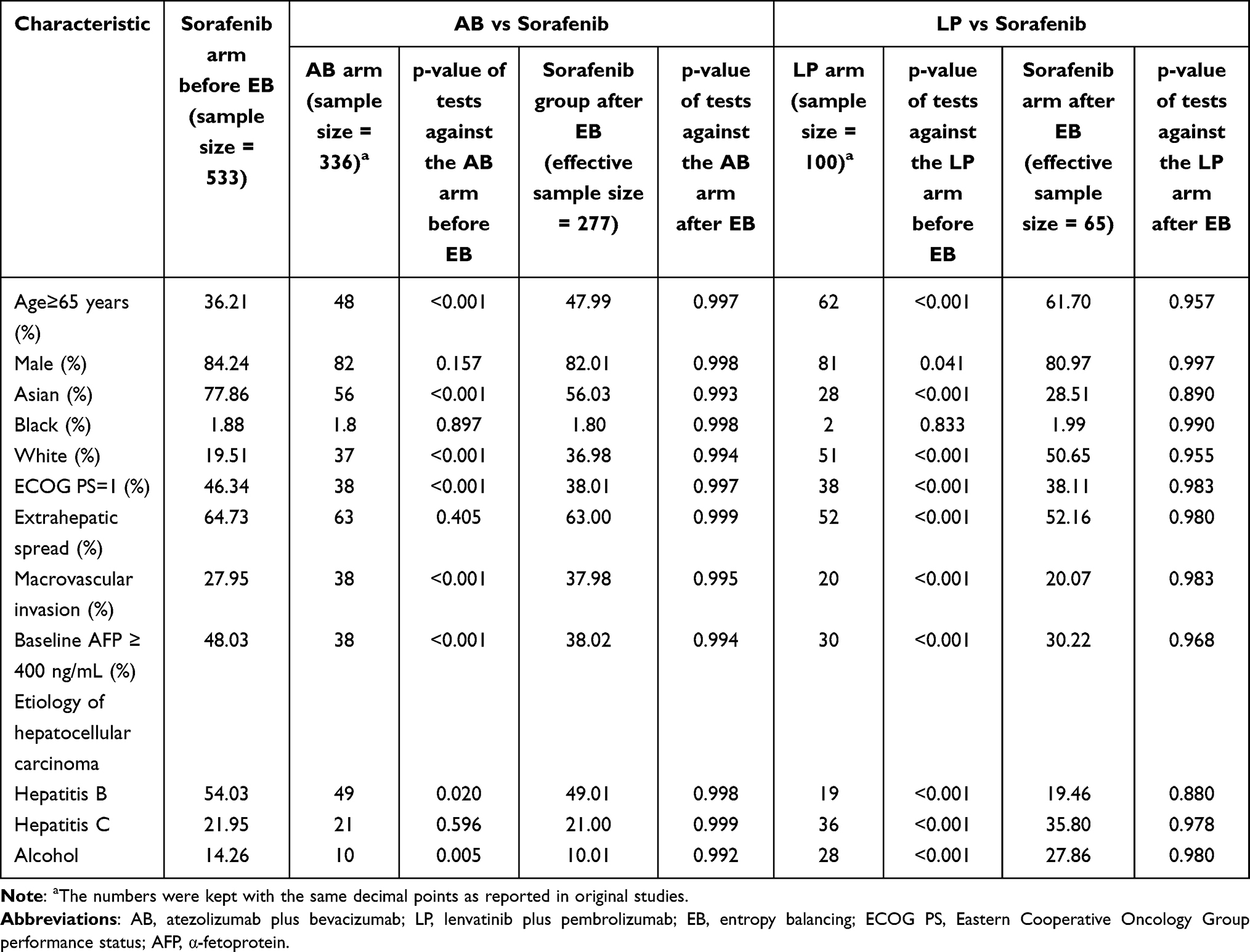 |
Table 1 Comparison of Characteristics Before and After Entropy Balancing |
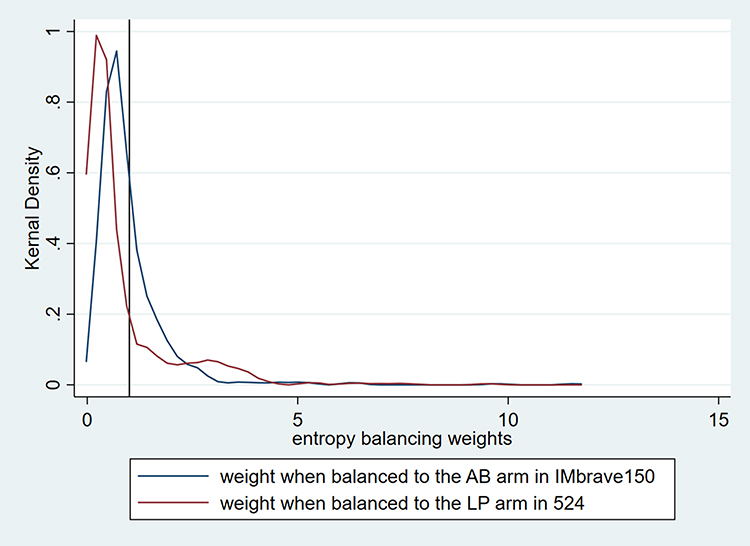 |
Figure 2 The kernel density of the entropy balancing weights of individual-level patients (IPD) in the sorafenib arm when balanced to the atezolizumab plus bevacizumab (AB) arm and the lenvatinib plus pembrolizumab (LP) arm. The deviation and dispersion of each line from the black vertical line demonstrate the unbalance of sorafenib IPD and the aggregate data of the corresponding comparator regimen before entropy balancing. The dissimilarity of the two lines of entropy balancing weights represents the unbalance between the aggregate data of the AB and LP arms. |
Table 2 displays the results of the MAIC analyses. In the MAIC analyses of AB vs sorafenib, AB was associated with significantly better efficacy on both OS (HR: 0.58, 95% CI: 0.42–0.79) and PFS (HR: 0.59, 95% CI: 0.47–0.76) compared with sorafenib. Both estimates had good proximity to the RCT results from the IMbrave150 trial (OS HR: 0.59, 95% CI: 0.46–0.76; PFS HR: 0.59, 95% CI: 0.48–0.73) such that the tests of the MAIC estimates against the RCT results were not statistically different (OS: p = 0.450; PFS: p = 0.497). In the MAIC analyses of LP vs sorafenib, LP had significantly better efficacy on PFS (HR: 0.62, 95% CI: 0.41–0.94) but not OS (HR: 0.83, 95% CI: 0.52–1.32).
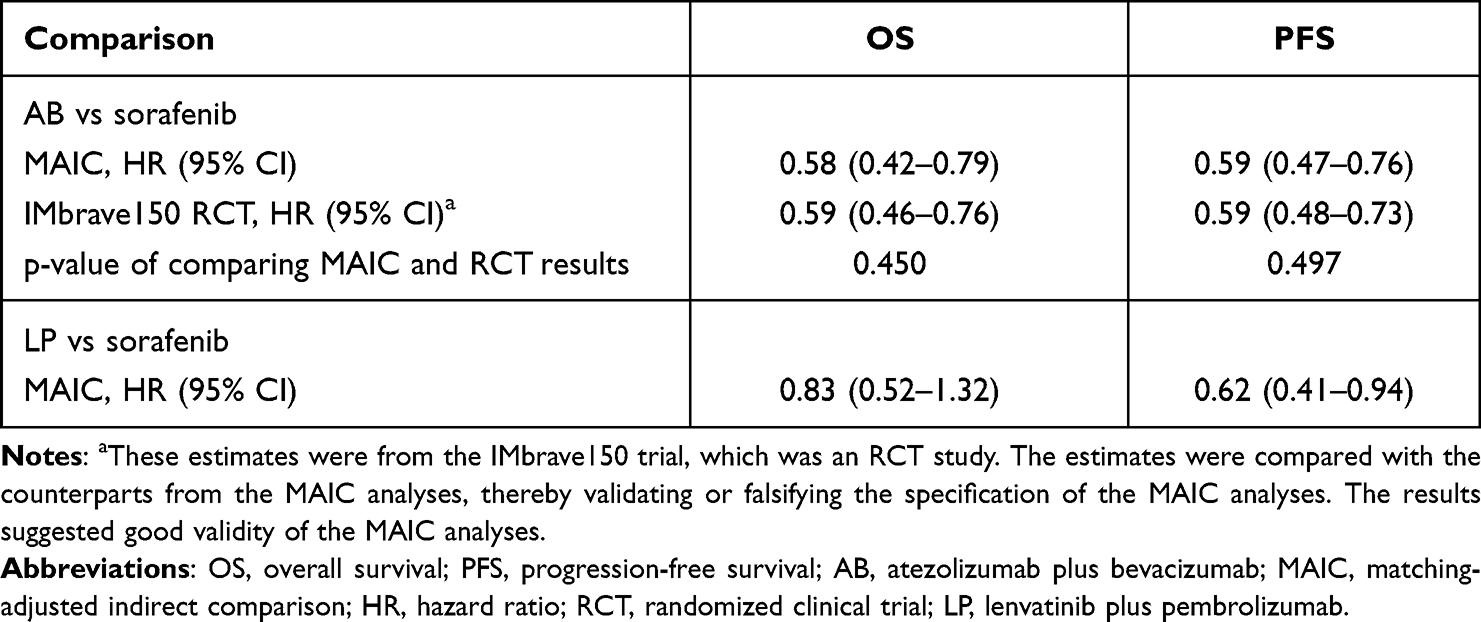 |
Table 2 The Matching-Adjusted Indirect Comparison Estimates of Hazard Ratios of Overall Survival and Progression-Free Survival |
The results of the final comparison of AB and LP are shown in Table 3. The AB regimen was insignificantly more efficacious on OS (HR: 0.71, 95% CI: 0.42–1.23) than and similarly efficacious on PFS (HR: 0.95, 95% CI: 0.60–1.51) as the LP regimen.
 |
Table 3 Second-Order Indirect Comparisons of Atezolizumab Plus Bevacizumab vs Lenvatinib Plus Pembrolizumab |
The E-values of the HR estimates from the present study are listed in Table 4. According to the results, the effects of AB in relation to sorafenib on both OS and PFS are relatively robust since strong associations of omitted factors with both the treatment assignment and the outcomes are needed to counteract the observed effects. Likewise, the effect of LP on PFS compared with sorafenib is relatively robust. However, the point estimates of the effects of LP on OS in relation to sorafenib and the effects of AB on both outcomes in relation to LP are vulnerable to potential bias. In these comparisons, weak associations of omitted factors with both the treatment assignment and the outcomes suffice to negate the observed effects.
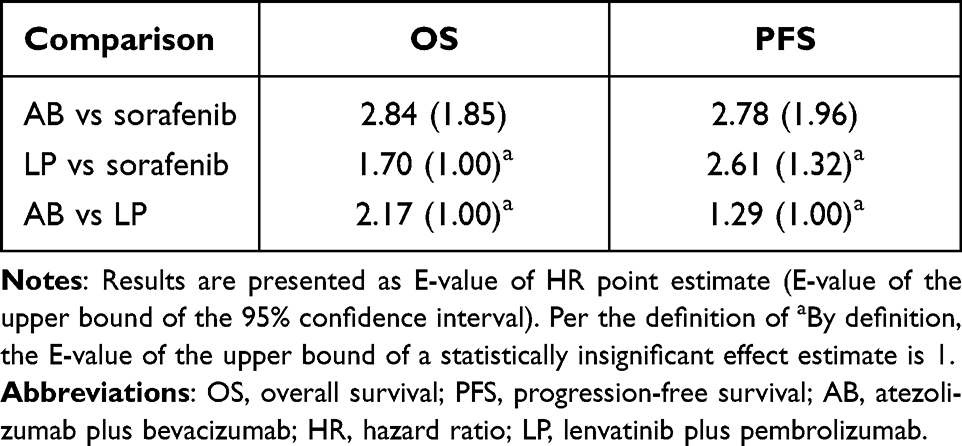 |
Table 4 The E-Values of Estimated Hazard Ratios in the Present Study |
Discussion
In the present study, MAIC analyses were conducted to compare the efficacy of AB and LP with sorafenib for the first-line treatment of advanced HCC, which were sequenced by second-order comparisons via re-weighted sorafenib IPD. Neither superior nor inferior efficacy of AB compared with LP on reducing mortality and delaying progression was identified per the current results.
The findings from the present analysis have important implications for the clinical management of advanced HCC patients. Like several other tumor types, HCC community has seen a storm of explorations to expand the first-line treatment indications for PD-1/PD-L1. AB was the only PD-1/PD-L1 regimen approved for the first-line treatment of advanced HCC by FDA and EMA by far and is becoming equally popular as sorafenib and lenvatinib. With the seemingly promising results of the KEYNOTE 524 trial, it is also natural to consider LP as a competing option for advanced HCC.8,20 The current results indicate that LP is indeed more efficacious than sorafenib on increasing PFS. In the meantime, LP was not found to be significantly less efficacious than AB on both OS and PFS. As such, LP may have the potential to possess sufficient clinical value as an option for first-line therapy for HCC in spite of prior setbacks in the regulatory process. In the meantime, it is not necessarily helpful to rush to the decision of engaging LP as an alternative to AB for patients without prior systemic therapies since the current evidence does not support the superiority of LP over AB on any measurable scale. To the extent that an ongoing investigation will likely generate relatively high-quality data on the efficacy of LP, it is advisable to consider this regimen in future based on solid evidence.27
In the absence of common comparators, MAIC could be used to synthesize results from single-arm trials if the IPD of one of the comparators was available. In the present analysis, MAICs of AB vs sorafenib and LP vs sorafenib were conducted, the former of which generated outputs that resonated well with the RCT results of the IMbrave150 trial. Such resemblance supported the validity of the model specification used for MAICs. However, the first-order MAICs can only provide insight into the comparative effectiveness of the relatively new therapies over sorafenib. To conduct further comparisons between the new therapies without access to the IPD for either treatment, a second-order indirect comparison was conducted following the first-order MAIC results. Such an approach enables researchers to expand indirect comparisons to a greater network of treatment options for the same population when only one set of IPD was available. Given its potential to be used in similar comparative effectiveness studies, this approach may represent a marginal novelty in the area of indirect treatment comparison based on MAIC.
The results of the present study should be interpreted with several caveats. First, the present analysis relied on data from existing trials, yet it was not meant to replace the results of clinical trials. Instead, it was conducted to provide preliminary evidence regarding two competing regimens. To profoundly understand the clinical profiles of the therapies, it is necessary to carry out RCTs. Second, although the RCT-MAIC cross validation suggested good validity of the MAIC analyses, residual effect modifiers that might confound the results could not be fully ruled out.17 The E-values suggest that, whereas the effects of AB and LP compared with sorafenib were relatively robust to residual confounders, the effects of AB in relation to LP might entail some sensitivity to bias. Third, the sample size of the KEYNOTE 524 trial and the ESS of the corresponding MAIC were moderate, which might undermine the power of the analyses to detect true effectiveness. In particular, the point estimate of the OS HR of AB vs LP was non-trivial. Future evidence with a more powerful sample size is necessary to shed light on the effect, if any. Despite these limitations, the present findings provided previously unavailable evidence that can be considered in clinical practice.
Conclusions
Both AB and LP are more efficacious than sorafenib in extending PFS for the first-line treatment of advanced HCC patients. There is also no evidence that AB is associated with superior or inferior efficacy than LP, suggesting the potential of the latter as an option for first-line treatment of advanced HCC.
Data Sharing Statement
The data used in this study are presented in the manuscript or publicly available at Project Data Sphere (https://projectdatasphere.org). The program code used for analysis has been submitted for peer review and is available from the corresponding author upon reasonable requests.
Acknowledgments
The authors would like to thank Project Data Sphere (https://projectdatasphere.org) for providing access to the clinical trial data of the sorafenib arm.
Author Contributions
Y.J.: study design, data curation, statistical analysis, and drafting of the manuscript. D.C.: literature review, data extraction, and substantial revision of the manuscript. S.S.: data analysis, preparation of the manuscript, substantial revision of the manuscript. All authors agreed to submit the manuscript to Clinical Epidemiology, have reviewed and agreed on all submitted versions of the manuscript, and agreed to take responsibility and be accountable for the contents of the article.
Funding
The authors did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors for the submitted work.
Disclosure
The authors claim no conflicts of interest related to the subject of the submitted work.
References
1. Heimbach JK, Kulik LM, Finn RS, et al. AASLD guidelines for the treatment of hepatocellular carcinoma. Hepatol. 2018;67(1):358–380. doi:10.1002/hep.29086
2. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatol. 2018;68(2):723–750.
3. Tang H, Huang Y, Duan W, Li C, Meng X, Dong J. A concise review of current guidelines for the clinical management of hepatocellular carcinoma in Asia. Transl Cancer Res. 2017;6(6):1214–1225.
4. Xie D-Y, Ren ZG, Zhou J, Fan J, Gao Q. 2019 Chinese clinical guidelines for the management of hepatocellular carcinoma: updates and insights. Hepatobiliary Surg Nutr. 2020;9(4):452–463.
5. Zhang T, Merle P, Wang H, et al. Combination therapy for advanced hepatocellular carcinoma: do we see the light at the end of the tunnel? Hepatobiliary Surg Nutr. 2021;10(2):180–192. doi:10.21037/hbsn-2021-7
6. Gnoni A, Licchetta A, Memeo R, et al. Role of BRAF in hepatocellular carcinoma: a rationale for future targeted cancer therapies. Medicina. 2019;55(12) 754.
7. Vogel A, Cervantes A, Chau I, et al. Hepatocellular carcinoma: ESMO clinical practice guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2018;29(Suppl 4):iv238–iv255. doi:10.1093/annonc/mdy308
8. Benson AB, et al. NCCN clinical practice guidelines in oncology (NCCN guidelines®) hepatobiliary cancers version 2.2021; 2021 [cited May 1, 2021]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/hepatobiliary.pdf.
9. Vogel A, Martinelli E, Vogel A. Updated treatment recommendations for hepatocellular carcinoma (HCC) from the ESMO clinical practice guidelines. Ann Oncol. 2021;32:801–805. doi:10.1016/j.annonc.2021.02.014
10. Feng Z, Rong P, Wang W. Meta-analysis of the efficacy and safety of PD-1/PD-L1 inhibitors administered alone or in combination with anti-VEGF agents in advanced hepatocellular carcinoma. Gut. 2020;69(10):1904–1906. doi:10.1136/gutjnl-2019-320116
11. Finn RS, Qin S, Ikeda M, et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N Engl J Med. 2020;382(20):1894–1905. doi:10.1056/NEJMoa1915745
12. Qin S, Ren Z, Feng Y-H, et al. Atezolizumab plus bevacizumab versus sorafenib in the Chinese subpopulation with unresectable hepatocellular carcinoma: Phase 3 randomized, open-label IMbrave150 study. Liver Cancer. 2021;10:296–308. doi:10.1159/000513486
13. Astor L. FDA holds off on approval of pembrolizumab/lenvatinib for frontline unresectable HCC; 2020 [cited November 8, 2020]. Available from: https://www.targetedonc.com/view/fda-denies-approval-of-pembrolizumab-lenvatinib-for-frontline-unresectable-hcc.
14. Phillippo DM, Ades AE, Dias S, et al. Methods for population-adjusted indirect comparisons in health technology appraisal. Med Decis Making. 2018;38(2):200–211. doi:10.1177/0272989X17725740
15. Vogel A, Rimassa L, Sun H-C, et al. Comparative efficacy of atezolizumab plus bevacizumab and other treatment options for patients with unresectable hepatocellular carcinoma: a network meta-analysis. Liver Cancer. 2021;10:240–248. doi:10.1159/000515302
16. Signorovitch JE, Sikirica V, Erder MH, et al. Matching-adjusted indirect comparisons: a new tool for timely comparative effectiveness research. Value Health. 2012;15(6):940–947. doi:10.1016/j.jval.2012.05.004
17. Jiang Y, Ni W. Performance of unanchored matching-adjusted indirect comparison (MAIC) for the evidence synthesis of single-arm trials with time-to-event outcomes. BMC Med Res Methodol. 2020;20(1):241. doi:10.1186/s12874-020-01124-6
18. Petto H, Kadziola Z, Brnabic A, et al. Alternative weighting approaches for anchored matching-adjusted indirect comparisons via a common comparator. Value Health. 2019;22(1):85–91. doi:10.1016/j.jval.2018.06.018
19. Cheng AL, Kang Y-K, Lin D-Y, et al. Sunitinib versus sorafenib in advanced hepatocellular cancer: results of a randomized phase III trial. J Clin Oncol. 2013;31(32):4067–4075. doi:10.1200/JCO.2012.45.8372
20. Finn RS, Ikeda M, Zhu AX, et al. Phase ib study of lenvatinib plus pembrolizumab in patients with unresectable hepatocellular carcinoma. J Clin Oncol. 2020;38(26):2960–2970. doi:10.1200/JCO.20.00808
21. Chen LT, Martinelli E, Cheng A-L, et al. Pan-Asian adapted ESMO clinical practice guidelines for the management of patients with intermediate and advanced/relapsed hepatocellular carcinoma: a TOS–ESMO initiative endorsed by CSCO, ISMPO, JSMO, KSMO, MOS and SSO. Ann Oncol. 2020;31(3):334–351. doi:10.1016/j.annonc.2019.12.001
22. Guyot P, Ades AE, Ouwens MJ, et al. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. doi:10.1186/1471-2288-12-9
23. Wei Y, Royston P. Reconstructing time-to-event data from published Kaplan-Meier curves. Stata J. 2017;17(4):786–802. doi:10.1177/1536867X1801700402
24. Mitchell M, Muftakhidinov B, Winchen T, van Schaik B, Wilms AK. Engauge digitizer software; 2019 [cited April 27, 2019]. Available from: http://markummitchell.github.io/engauge-digitizer.
25. Bucher HC, Guyatt GH, Griffith LE, et al. The results of direct and indirect treatment comparisons in meta-analysis of randomized controlled trials. J Clin Epidemiol. 1997;50(6):683–691. doi:10.1016/S0895-4356(97)00049-8
26. Haneuse S, VanderWeele TJ, Arterburn D. Using the E-value to assess the potential effect of unmeasured confounding in observational studies. JAMA. 2019;321(6):602–603. doi:10.1001/jama.2018.21554
27. Merck Sharp & Dohme Corp. Safety and efficacy of coformulated pembrolizumab/quavonlimab (MK-1308A) in combination with lenvatinib (E7080/MK-7902) in advanced hepatocellular carcinoma (MK-1308A-004). Available from: https://ClinicalTrials.gov/show/NCT04740307. NLM identifier: NCT04740307. Accessed April 27, 2022.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.