")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Increasing Use of Telemedicine for Neurological Disorders During the COVID-19 Pandemic: A Mini-Review
Authors Tu CC, Weng SY, Hsieh NC, Cheng WC, Alizargar J, Chang KS
Received 20 September 2022
Accepted for publication 2 December 2022
Published 14 February 2023 Volume 2023:16 Pages 411—418
DOI https://doi.org/10.2147/JMDH.S390013
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chuan-Chou Tu,1,* Shih-Yen Weng,2– 4,* Nan-Chen Hsieh,2,3 Wen-Chang Cheng,5 Javad Alizargar,3,6 Ko-Shih Chang7
1Department of Internal Medicine, Yuan Rung Hospital, Changhua, 510, Taiwan, Republic of China; 2College of Health Technology, National Taipei University of Nursing and Health Sciences, Taipei City, 112, Taiwan, Republic of China; 3Research Center for Healthcare Industry Innovation, National Taipei University of Nursing and Health Sciences, Taipei City, 112, Taiwan, Republic of China; 4Smart Healthcare Interdisciplinary College, National Taipei University of Nursing and Health Sciences, Taipei City, 112, Taiwan, Republic of China; 5Hyperbaric Oxygen Therapy and Wound Treatment Centre, Yuan Rung Hospital, Changhua, 510, Taiwan, Republic of China; 6College of Nursing, School of Nursing, National Taipei University of Nursing and Health Sciences, Taipei, 112, Taiwan, Republic of China; 7Department of Cardiology, Yuan Rung Hospital, Changhua, 510, Taiwan, Republic of China
*These authors contributed equally to this work
Correspondence: Ko-Shih Chang, Department of Cardiology, Yuan Rung Hospital, No. 201, Zhongzheng Road, Yuanlin, Changhua, 510, Taiwan, Republic of China, Tel +886 4 8326161 ext 2702, Fax +886 4 8317776, Email [email protected]
Abstract: Coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a highly contagious viral infection. In addition to its association with common pulmonary and gastrointestinal complications, COVID-19 is also associated with numerous neurological and neuropsychiatric conditions. This minireview aims to cover current literature addressing the application of telemedicine in neurological disorders and neuropsychiatric conditions, especially in response to the COVID-19 pandemic. This article revealed that quarantine, masking, and social distancing policies practiced during the COVID-19 pandemic involved restrictions and challenges to providing medical services, especially for patients with neurological disorders with or without COVID-19 infection. During the pandemic, both healthcare administrators and clinicians, including neurologists, have rapidly adapted or introduced telemedicine technologies for delivering specialty care. In some areas in the world, telemedicine has been successfully applied to reduce the impact imposed by COVID-19. Conclusively, this article supports the idea that telemedicine is an effective tool for providing specialized healthcare for patients with neurological conditions while adhering to social distancing or lockdown policies instituted during the COVID-19 pandemic. Government and medical/healthcare authorities, physicians and healthcare providers need to work together to expand the adoption of telemedicine applications, even after the COVID-19 crisis.
Keywords: COVID-19 infection, neurological disorders, social distancing, telemedicine
Introduction
Coronavirus disease 2019 (COVID-19), which is caused by the virus severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a highly contagious infection transmitted easily human-to-human through respiratory droplets and saliva, as evidenced in the recent global outbreak from 2019 to the present.1,2 In addition to pulmonary, gastrointestinal, renal and hematologic complications, COVID-19 is causally associated with numerous neurological and neuropsychiatric effects.3 In addition, patients with pre-existing neurological diseases are at higher risk for complications if they contract the coronavirus.4 Neurological manifestations of COVID-19 involve both the central nervous system (CNS) and peripheral nervous system, and vary in severity from mild (eg, anosmia and ageusia, headache) to severe (eg, ischemic stroke, encephalitis).3,5 Underlying mechanisms involve both indirect (inflammatory consequences, thrombotic complication, hypoxia, blood pressure dysregulation), and direct (neurotropic properties of the virus) pathways.5 Currently, although several vaccines have been developed, there are no highly safe and effective therapeutic drugs or vaccines, and social distancing policies remain the most important measures to reduce the spread of COVID-19. However, strict social distancing policies have brought restrictions and challenges to provision of medical services, especially for those with neurological or neuromuscular diseases who require routine face-to-face health care. Moreover, quarantine and isolation requirements for people with COVID-19 infection or suspected COVID-19 infection may initiate new psychiatric symptoms in people without mental illness or may aggravate existing conditions.6
Telemedicine, noted for delivering direct healthcare services from nurses and clinicians to distant recipients, has been implemented more often and more widely in the COVID era to help address the challenges in medical care delivery during periods of physical distancing and lockdown.7 Telemedicine has been particularly useful for patients with long-term chronic conditions and could be considered essential to help reduce physical contact during outbreaks such as COVID-19.8,9 This article presents our narrative mini-review of the current literature, focusing on the development and application of telemedicine in treating neurological disorders and neuropsychiatric conditions, particularly over the last two years in response to COVID-19. Finally, as a broader concept that encompasses telemedicine, digital health for this issue is also briefly described.
Mini-Review of the Literature
In this narrative mini-review, we identified and selectively reviewed the current literature, published within the last ten years (2012 to 2022), before and during the recent years of the COVID-19 era (2019–2022). We focused on the application of telemedicine in the care of different neurological disorders during the global pandemic. Studies from 2012 to 2018 were included as applicable to the background of telemedicine development and patterns of use in treating certain neurological disorders prior to the pandemic. Study selection involved electronic and manual search of the literature using the databases PubMed and Cochrane Database of Systematic Reviews. All types of articles except basic studies were considered eligible if the main topic was telemedicine in neurological disorders, including original articles, clinical research, essays and review articles. Information from the reviewed studies was summarized narratively to present the most relevant findings. Below we report our integrated findings from the selected studies, which are grouped by telemedicine development and use in specific neurological disorders.
Development of Telemedicine and Benefits to Patients
Telemedicine describes direct provider-to-patient services delivered from a distance, including nursing services, monitoring and physician consultation.7 Modern telemedicine was developed during the 1970s and 1980s to meet the needs for medical care during space travel.10 At present, telemedicine has become even more accessible given the advances in mobile and electronic technologies. Today’s telemedicine formats include the telephone, video, digital photography and remote monitoring using electronic devices that capture patient health data for review by healthcare providers, enabling early intervention as needed, synchronously or asynchronously.7 However, despite rapid evolution over earlier decades, telemedicine still has unresolved issues surrounding regulatory laws across state lines and lacks supportive payment structures, which keeps the technology from being more widely implemented.10,11
In response to the COVID-19 pandemic, administrators and clinicians have been forced to quickly adapt or introduce telehealth technology to provide specialty care. Some procedures, such as teleconsultations, were not adopted until the advent of the COVID-19 pandemic. The main benefits derived by patients from telemedicine include saving time and reducing costs of consultation and specialists’ visits while gaining remote access to professional medical care (including specialist consultation when needed), which is especially valuable when contagion and rapid spreading of disease are a concern, as in the COVID era.10,13 However, telemedicine also has certain disadvantages or deficiencies compared to in-person physical consultation, including that performing physical examinations remotely or online is nearly impossible and some patients, such as older adults living alone or those with comorbid chronic disease or dementia may lack the knowledge or resources needed to use mobile devices or computers that would allow them to participate in telemedicine visits.13,14 The security of patient data is another issue that remains to be addressed.10
Telemedicine in Neurological Practice
As neurological patients are more susceptible to SARS-CoV-2 infection and associated complications,3,4 the use of telemedicine may benefit these patients by reducing physical contact while maintaining medical care. Indeed, during the COVID-19 pandemic, the use of telemedicine in neurology has increased worldwide, as well as in Taiwan.3,15 Application of telemedicine in some neurological practice is summarized in Table 1.
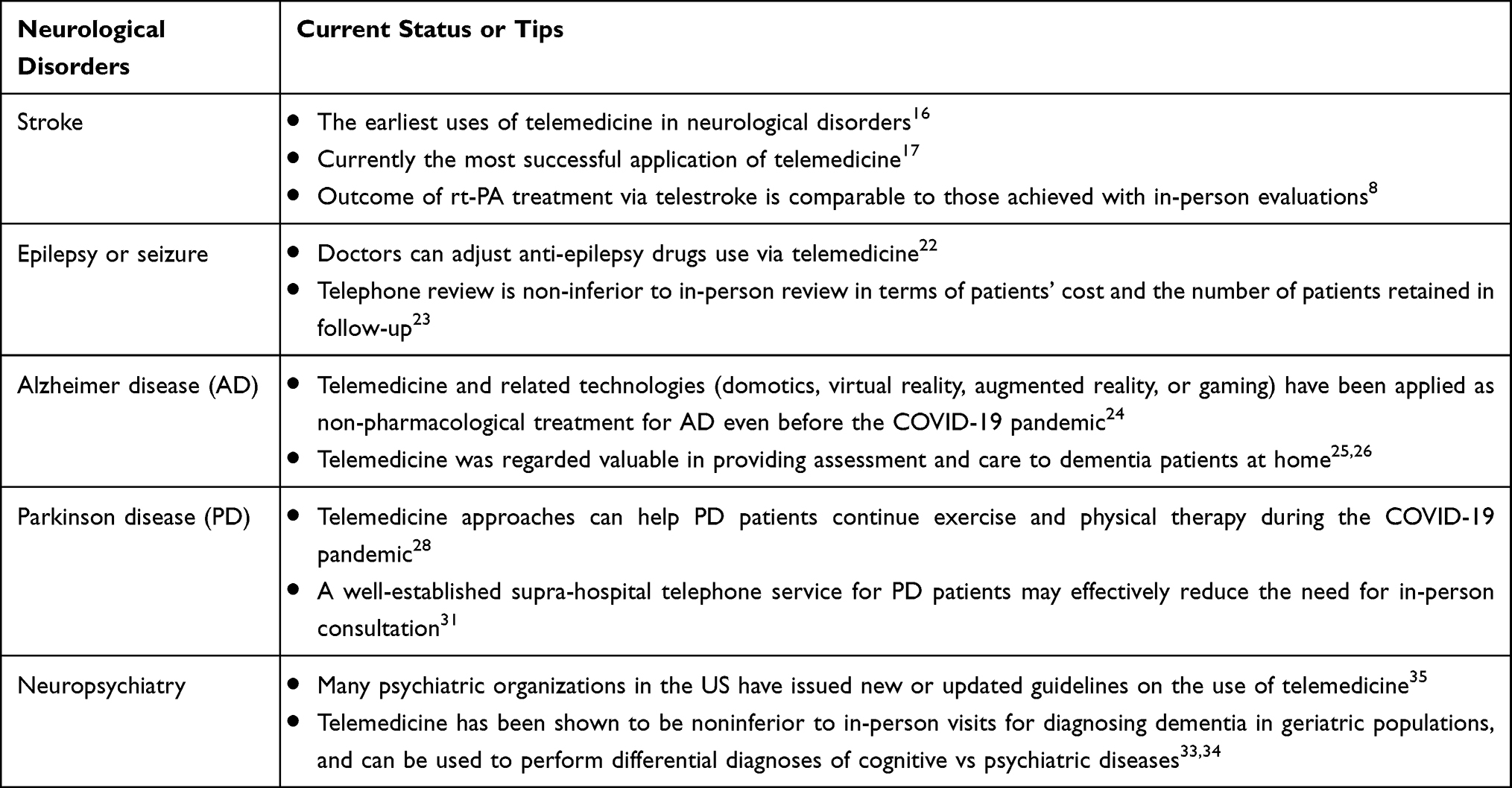 |
Table 1 Application of Telemedicine in Major Neurological Disorders |
Telemedicine in Stroke
Telestroke, or using telemedicine for stroke care, is among the earliest uses of telemedicine in neurological practice.16 It is also one of the most successful applications of telemedicine, accessing the experience of stroke specialists by hospitals that lack sufficient stroke expertise, and the number and extent of telestroke networks continues to grow worldwide.17 In fact, telestroke services are expanding to help reduce or avoid physical contact during the COVID-19 pandemic.8 In some countries during the initial onset of COVID-19, the reported number of acute stroke admissions was reduced by 50%–80%,18 suggesting that many patients with moderate and even severe stroke were avoiding seeking medical care, probably due to fear of contracting infection if referred to a hospital. Inpatient telemedicine has become an important tool for treating stroke patients with suspected or confirmed COVID-19, enabling stroke specialists to perform essential monitoring and assessment of patients’ neurological status in dedicated COVID-19 areas, especially during shortages of trained personnel.12 Emergency department evaluation of stroke patients can also be entirely conducted virtually using telestroke equipment.7 Telestroke is shown to be safe, and standardization of stroke treatment throughout a telestroke network ensures the quality of treatment. Outcomes after intravenous recombinant tissue plasminogen activator (rt-PA) treatment via telestroke compare favorably to outcomes of face-to-face evaluations.8
Recently, Singh and co-researchers conducted a global-scaled individual patient data meta-analysis and reported that encephalopathy and cerebrovascular events (mainly ischemic and hemorrhagic stroke) were the most frequent identified neurological manifestations of COVID-19, whereas a poor outcome (moderate to severe disability or death) was more common in cerebrovascular cases than in encephalopathy, suggesting that stroke is a major factor associated with poor prognosis in neurological COVID-19 disease.19 Cardiovascular diseases are also highly associated with COVID-19, serve both as a risk factor and prognostic indicator, and can be a complication of the disease itself.20 In sight of these findings, it is important to identify patients potentially developing cardio/cerebrovascular complications, especially during the COVID-19 era. Telemedicine may be helpful for this issue. For example, blood pressure monitoring is well suited to telemedicine approaches.21 We think telemedicine may lead to better monitoring that can facilitate patient self-management, improve medication adherence, or encourage healthier lifestyles that reduce the risk of cardiovascular and cerebrovascular diseases, although more evidence is needed.
Telemedicine in Epilepsy or Seizure
Several aspects of telemedicine are of particular note for patients with epilepsy or seizure. First, telemedicine consultation may help physicians determine whether patients will require clinic visits or if the telemedicine approach will suffice.11,14 Secondly, the side-effects of anti-epilepsy drugs (AEDs) can be reviewed and adjusted via telemedicine and in situations where side-effects are critical, clinic appointments may still be required.22 Lastly, some patients with epilepsy may practice dietary therapy, and clinicians can confirm their dietary compliance via telemedicine; or dieticians can provide online dietary counseling.14 Results of a randomized controlled trial conducted by Bahrani et al23 showed that telephone review was non-inferior to in-person review for outpatients with epilepsy in terms of patients’ costs and the number of patients retained in follow-up. As with other clinical conditions, the feasibility and accessibility of telemedicine for patients with epilepsy influence whether or not they continue to rely on telemedicine. Despite the risk of contracting infection during the COVID-19 pandemic, patients with epilepsy are still encouraged to physically visit hospitals and laboratories or imaging centers when in-person clinical testing is required (eg, blood tests, cerebrospinal fluid tests, electroencephalogram, or neuroimaging).14
Telemedicine in Alzheimer Disease
Alzheimer disease (AD), the most widespread form of two types of dementia, is a chronic disease with progressive deterioration of cognition, function, and behavior leading to disability and death.24 Most patients with AD are aged 65 years and older and are included in the older adult population more susceptible to SARS-CoV-2 infection. These patients are often unaware of the hygienic measures and social distancing requirements mandated by government and healthcare authorities during the pandemic, and these practices must be reinforced continuously by caregivers.3 In the absence of highly effective pharmacologic treatments for AD, virtual reality, augmented reality, and gaming were applied as non-pharmacological treatment, even before the COVID-19 pandemic, contributing to at-home patient assessments and providing consultation for caretakers.24 Studies have also found that telemedicine can help patients with dementia maintain their independence in their own homes, improving their safety and clinical outcome.25,26 The use of telemedicine has increased during the COVID era due to its ability to help provide cognitive neurorehabilitation for AD patients outside of conventional care settings.27
Telemedicine in Parkinson Disease
Parkinson disease (PD) is the second most common neurodegenerative disorder following Alzheimer disease, affecting nearly 1% of people over age 60 years.28 Studies have found that COVID-19 increases the risk of mortality in PD patients by 20%–40% compared to the 7%–19% mortality risk of the general population.29,30 Quarantine measures also pose long-term negative effects on PD patients because healthcare services such as physical therapy, which can be critical for chronically ill patients, are significantly reduced. Physical therapy and exercise, which are known to improve motor and non-motor symptoms of PD patients, and PD patients may be severely affected if these practices are interrupted. Many telemedicine approaches can be applied to help PD patients continue to exercise and receive physical therapy, including telerehabilitation, apps, motivational tools, virtual reality exercise and exergaming.28 In fact, these approaches have shown great potential for the support and wellbeing of PD patients even though long-term efficacy remains to be validated. During COVID-19 quarantine, PD patients and patients with other neurological diseases are also prevented from travelling to hospitals for appropriate care. Two different types of synchronous telemedicine, telephone and video links, have been used to address this issue. Cilia and colleagues31 established a supra-hospital telephone service delivered by Parkinson disease nurse specialists (PDNS) with access to a multidisciplinary team. Telephone service can be combined with video consultation with a neurologist when required, and results showed that only about 1 in 45 PD patients originally contacted by a PDNS actually received consultation.
Telemedicine in Neuropsychiatry
Among the above-mentioned neurological disorders, stroke, PD, AD, and epilepsy may involve neuropsychiatric manifestations during disease development.32–35 The prevalence of PD-related psychosis is estimated to be 50% or more throughout the disease course.35 Depending on patients’ dementia subtype, psychosis is reported to occur broadly in 10% to 75% of people with dementia. If left untreated, psychosis symptoms tend to reduce the quality of life, leading to poor outcomes, increased mortality, and high healthcare costs.32 Notably, neuropsychiatric symptoms could be independently caused by SARS-CoV-2 infection. In 2020, Lu et al36 firstly reported a case of a COVID-19 patient who had no history of psychiatric disorder but developed manic-like symptoms when the vital signs recovered on illness day 17. The manic episode, according to the author, might be a delayed response to CNS infection by SARS-CoV-2. Recently, it has been increasingly obvious that patients with COVID-19 have higher incidence of neuropsychiatric manifestations including depression, anxiety, and post-traumatic stress symptoms when compared with non-COVID controls.37 The possible underlying mechanisms, as summarized in a review article by E. Jansen van Vuren et al,38 may involve unmitigated neuro-inflammatory responses.
Telemedicine has been used successfully in long-term care residents with dementia and those with neuropsychiatric symptoms. These patients have been treated successfully using telemedicine, and many medical and psychiatric organizations in the US have updated their guidelines on the use of telemedicine during the COVID-19 era.35 Telemedicine has been shown to be noninferior to in-person visits for diagnosing dementia in geriatric populations, and can be used to perform differential diagnoses of cognitive vs psychiatric diseases.33,34 Successful telemedicine in long-term care facilities or nursing homes requires collaboration between specialists, facility administrators and staff. Some long-term care facilities or nursing homes that are facing closure because of the COVID-19 pandemic may seek to stay open by offering behavioral or psychiatric specialty care, which can be facilitated readily through adopting telemedicine.35
Digital Health for This Issue
In several studies, terms like “telehealth” or “digital health” were used instead of “telemedicine”. According to FDA, digital health represents a broad-scope concept that encompasses mobile health, health information technology, wearable devices, telehealth and telemedicine, and personalized medicine.39 Regarding the use of digital health in the COVID-19 era, a systematic review exploring the deployment of digital health technologies in South Africa showed that various specific digital health technologies have been successfully applied, including short messaging service-based solutions, mobile health applications, telemedicine and telehealth, WhatsApp-based systems, artificial intelligence, and chatbots and robotics.40 These innovative technologies, as indicated by the authors, have been employed for purposes such as screening infectious and non-infectious diseases, disease monitoring, medication and treatment compliance, creating awareness and communication.40 For neurological disorders, digital health technologies may accelerate objective evaluation of changes in cognitive functioning,41 which is of particular benefit.
Discussion
This article presents the findings of our mini-review of recent literature, which focused on the use of telemedicine in neurological disorders during the COVID-19 pandemic. The unique ability of telemedicine to deliver healthcare remotely makes it an effective tool for providing specialized healthcare for patients with chronic neurological conditions while meeting social distancing or lockdown policies instituted to reduce physical contact. Recent studies have stated that telemedicine replicates almost everything that can be done through in-person consultation. It is also generally popular with patients, reduces patients’ healthcare costs and has a low carbon footprint. This article supports the idea that telemedicine is useful for the neurological disease care in the COVID-19 era, thereby encouraging the adoption of telemedicine in neurological practices, especially for those requiring persistent medical care but with reduced patients seeking care, such as stroke.
Relatively few neurologists used telemedicine in everyday practice before the pandemic. Although the concept is understood and appreciated, issues remain surrounding reimbursement and regulation, which has slowed the implementation of telemedicine more broadly into the healthcare system.11 The underutilization of telemedicine can also be attributed in part to a lack of incentives for physicians to change their practice methods, and a general concern that using telemedicine may not be entirely legal.12 Other barriers may include poorly established patient-physician relationships and patients’ lack of knowledge about telemedicine visits.42,43 However, utilization increased as a result of the need for remote care and consultation during the current COVID era. Awareness and use of telemedicine may also be improved by providing appropriate incentives for physicians to use telemedicine technologies and developing educational tools and programs to teach patients about accessing telemedicine services. Telemedicine legislation was introduced in the US Congress in February 2022 in the form of the bipartisan Telehealth Extension and Evaluation Act, which establishes a two-year extension for COVID-19 emergency health waivers.44 It is aimed at ending geographic and site restrictions and is intended to support Medicare beneficiaries access telemedicine services at home and allow controlled substances to be prescribed remotely. However, it will not be implemented until 2024.
Increased use of telemedicine appears to be unbalanced between countries, according to a global survey on telemedicine utilization for movement disorders.45 According to the survey study, major limitations to the adoption of telemedicine for movement disorders include restricted internet connection (eg, in remote areas, or prohibitive costs of data or devices), lack of physician reimbursement, and patients’ lack of familiarity with telemedicine. This seems to suggest that the existing disparities may even increase if these obstacles to use are not addressed and resolved.
In Taiwan, the laws governing medical practices originally restricted the use of telemedicine to provide medical care to patients in mountainous regions, outlying islands and remote areas. Nevertheless, because of the highly contagious nature of COVID-19, the government has eased restrictions in order to make telemedicine accessible to individuals under home quarantine, wherever they are located. Moreover, the new laws stipulate that the Taiwan National Health Insurance, which covers 99% of the population, can be used to support telemedicine services.46 Telemedicine services are continuously evolving, and to help prepare for this, the Taiwan Ministry of Health and Welfare is developing an official mobile app platform to make it easier for patients to pay for services and to obtain prescribed medications. This applies to different medical specialties, including neurology.
COVID-19 has made a notable impact on the healthcare system. Authors of a review article that evaluated the acceleration of telemedicine for treating children with cerebral palsy indicated that the pandemic has increased the use of home-based telemonitoring, and that these services are expected to expand to even broader use beyond the pandemic.47 In particular, tele-monitoring is exceptionally useful for functional assessments such as gait monitoring and remote rehabilitation monitoring in the patients’ natural environment. In the post-pandemic era, telemedicine is expected to become more coordinated and patient-centric, providing more tools for assessment and improved payment options such as reimbursement of multidisciplinary tele-care.48 Such patient-centric care tends to improve outcomes, increase the efficiency of care and reduce patients’ costs.
Limitations
The present review has several limitations. First, it was a narrative review rather than a systematic review of the literature, and certain studies that could have been identified through the more detailed and rigorous systematic review may have been missed. Additionally, we focused on common neurological disorders even though telemedicine has been applied to many other neurological disorders, including head trauma, amyotrophic lateral sclerosis (ALS), and polyneuropathy;8 cerebellar ataxia48 and cerebral palsy,47 none of which were discussed in depth.
Conclusions
In conclusion, recent studies have demonstrated the safety and effectiveness of telemedicine as a tool for providing specialized healthcare for patients with chronic neurological conditions while adhering to social distancing or lockdown policies instituted during the COVID-19 pandemic. The use of telemedicine extends well beyond neurological disorders, and the advantages of this modern contact-free consultation and delivery of medicine are essentially valid across medical specialties. Telemedicine can help achieve the goals of long-term treatment and rehabilitation that have been challenged during the pandemic by providing specialized consultation and medical care as needed without physical contact. Government and medical/healthcare authorities, physicians and healthcare providers need to work together to expand the adoption of telemedicine applications, even after the COVID-19 crisis.
Abbreviations
AD, Alzheimer disease; COVID-19, Coronavirus disease 2019; PD, Parkinson disease; SARS-CoV-2, Severe acute respiratory syndrome coronavirus-2.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Informed Consent
This is a mini-review article, which do not need the IRB approval and informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors have no conflicts of interest to declare for this work.
References
1. Jayaweera M, Perera H, Gunawardana B, Manatunge J. Transmission of COVID-19 virus by droplets and aerosols: a critical review on the unresolved dichotomy. Environ Res. 2020;188:109819. doi:10.1016/j.envres.2020.109819
2. WHO. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19); 2020. Available from: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf.
3. Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-Leon J, Kanti Ray B. Neurological and Neuropsychiatric Impacts of COVID-19 Pandemic. Can J Neurol Sci. 2021;48(1):9–24. doi:10.1017/cjn.2020.173
4. Marsh EB, Kornberg M, Kessler K, et al. COVID-19 and vaccination in the setting of neurologic disease: an emerging issue in neurology. Neurology. 2021;97(15):720–728. doi:10.1212/WNL.0000000000012578
5. Wenting A, Gruters A, van Os Y, et al. COVID-19 neurological manifestations and underlying mechanisms: a scoping review. Front Psychiatry. 2020;11:860. doi:10.3389/fpsyt.2020.00860
6. Venketasubramanian N, Anderson C, Ay H, et al. Stroke Care during the COVID-19 Pandemic: international Expert Panel Review. Cerebrovasc Dis. 2021;50(3):245–261. doi:10.1159/000514155
7. Mahoney MF. Telehealth, Telemedicine, and Related Technologic Platforms: current Practice and Response to the COVID-19 Pandemic. Journal of Wound, Ostomy & Continence Nursing. 2020;47(5):439–444. doi:10.1097/WON.0000000000000694
8. Ganapathy K. Telemedicine and Neurological Practice in the COVID-19 Era. Neurol India. 2020;68(3):555–559. doi:10.4103/0028-3886.288994
9. Ignatowicz A, Atherton H, Bernstein CJ, et al. Internet videoconferencing for patient-clinician consultations in long-term conditions: a review of reviews and applications in line with guidelines and recommendations. Digit Health. 2019;5:2055207619845831. doi:10.1177/2055207619845831
10. Kichloo A, Albosta M, Dettloff K, et al. Telemedicine, the current COVID-19 pandemic and the future: a narrative review and perspectives moving forward in the USA. Fam Med Community Health. 2020;8(3). doi:10.1136/fmch-2020-000530
11. Patterson V. Neurological telemedicine in the COVID-19 era. Nat Rev Neurol. 2021;17(2):73–74. doi:10.1038/s41582-020-00438-9
12. Nursing AAoAC. Scope and Standards of Practice for Professional Telehealth Nursing.
13. Vimalananda VG, Gupte G, Seraj SM, et al. Electronic consultations (e-consults) to improve access to specialty care: a systematic review and narrative synthesis. J Telemed Telecare. 2015;21(6):323–330. doi:10.1177/1357633X15582108
14. Kuroda N. Decision Making on Telemedicine for Patients With Epilepsy During the Coronavirus Disease 2019 (COVID-19) Crisis. Front Neurol. 2020;11:722. doi:10.3389/fneur.2020.00722
15. Chen YH, Wu HW, Huang CC, et al. The Logistics of Medication and Patient Flow in Video-Based Virtual Clinics During a Sudden COVID-19 Outbreak in Taiwan: observational Study. Interact J Med Res. 2022;11(1):e37880. doi:10.2196/37880
16. Wechsler LR, Tsao JW, Levine SR, et al. Teleneurology applications: report of the telemedicine work group of the American Academy of neurology. Neurology. 2013;80(7):670–676. doi:10.1212/WNL.0b013e3182823361
17. Wechsler LR, Demaerschalk BM, Schwamm LH, et al. Telemedicine Quality and Outcomes in Stroke: a Scientific Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2017;48(1):e3–e25. doi:10.1161/STR.0000000000000114
18. Brainin M. Stroke Care and the COVID19 Pandemic. World Stroke Organization; 2020.
19. Singh B, Lant S, Cividini S, et al. Prognostic indicators and outcomes of hospitalised COVID-19 patients with neurological disease: an individual patient data meta-analysis. PLoS One. 2022;17(6):e0263595. doi:10.1371/journal.pone.0263595
20. Greenberg A, Pemmasani G, Yandrapalli S, Frishman WH. Cardiovascular and Cerebrovascular Complications With COVID-19. Cardiol Rev. 2021;29(3):143–149. doi:10.1097/CRD.0000000000000385
21. Omboni S, McManus RJ, Bosworth HB, et al. Evidence and recommendations on the use of telemedicine for the management of arterial hypertension: an international expert position paper. Hypertension. 2020;76(5):1368–1383. doi:10.1161/HYPERTENSIONAHA.120.15873
22. Liptrott S, Bee P, Lovell K. Acceptability of telephone support as perceived by patients with cancer: a systematic review. Eur J Cancer Care (Engl). 2018;27(1):e12643. doi:10.1111/ecc.12643
23. Bahrani K, Singh MB, Bhatia R, et al. Telephonic review for outpatients with epilepsy-A prospective randomized, parallel group study. Seizure. 2017;53:55–61. doi:10.1016/j.seizure.2017.11.003
24. Zucchella C, Sinforiani E, Tamburin S, et al. The multidisciplinary approach to alzheimer’s disease and dementia. a narrative review of non-pharmacological treatment. Front Neurol. 2018;9:1058. doi:10.3389/fneur.2018.01058
25. Barton C, Morris R, Rothlind J, Yaffe K. Video-telemedicine in a memory disorders clinic: evaluation and management of rural elders with cognitive impairment. Telemed J E Health. 2011;17(10):789–793. doi:10.1089/tmj.2011.0083
26. Brims L, Oliver K. Effectiveness of assistive technology in improving the safety of people with dementia: a systematic review and meta-analysis. Aging Ment Health. 2019;23(8):942–951. doi:10.1080/13607863.2018.1455805
27. Mantovani E, Zucchella C, Bottiroli S, et al. Telemedicine and virtual reality for cognitive rehabilitation: a roadmap for the COVID-19 Pandemic. Front Neurol. 2020;11:926. doi:10.3389/fneur.2020.00926
28. Pedersen SW, Suedmeyer M, Liu LW, et al. The role and structure of the multidisciplinary team in the management of advanced Parkinson’s disease with a focus on the use of levodopa-carbidopa intestinal gel. J Multidiscip Healthc. 2017;10:13–27. doi:10.2147/JMDH.S111369
29. Antonini A, Leta V, Teo J, Chaudhuri KR. Outcome of Parkinson’s Disease Patients Affected by COVID-19. Mov Disord. 2020;35(6):905–908. doi:10.1002/mds.28104
30. Langer A, Gassner L, Flotz A, et al. How COVID-19 will boost remote exercise-based treatment in Parkinson’s disease: a narrative review. NPJ Parkinsons Dis. 2021;7(1):25. doi:10.1038/s41531-021-00160-3
31. Cilia R, Mancini F, Bloem BR, Eleopra R. Telemedicine for parkinsonism: a two-step model based on the COVID-19 experience in Milan, Italy. Parkinsonism Relat Disord. 2020;75:130–132. doi:10.1016/j.parkreldis.2020.05.038
32. Aarsland D. Epidemiology and pathophysiology of dementia-related psychosis. J Clin Psychiatry. 2020;81(5). doi:10.4088/JCP.AD19038BR1C
33. Harrell KM, Wilkins SS, Connor MK, Chodosh J. Telemedicine and the evaluation of cognitive impairment: the additive value of neuropsychological assessment. J Am Med Dir Assoc. 2014;15(8):600–606. doi:10.1016/j.jamda.2014.04.015
34. Martin-Khan M, Flicker L, Wootton R, et al. The diagnostic accuracy of telegeriatrics for the diagnosis of dementia via video conferencing. J Am Med Dir Assoc. 2012;13(5):487 e419–424. doi:10.1016/j.jamda.2012.03.004
35. Shaughnessy L, Brunton S, Chepke C, Farmer JG, Rosenzweig AS, Grossberg G. Using telemedicine to assess and manage psychosis in neurodegenerative diseases in long-term care. J Am Med Dir Assoc. 2022;23(7):1145–1152. doi:10.1016/j.jamda.2021.12.033
36. Lu S, Wei N, Jiang J, et al. First report of manic-like symptoms in a COVID-19 patient with no previous history of a psychiatric disorder. J Affect Disord. 2020;277:337–340. doi:10.1016/j.jad.2020.08.031
37. Guo Q, Zheng Y, Shi J, et al. Immediate psychological distress in quarantined patients with COVID-19 and its association with peripheral inflammation: a mixed-method study. Brain Behav Immun. 2020;88:17–27. doi:10.1016/j.bbi.2020.05.038
38. Jansen E, Steyn SF, Brink CB, Moller M, Viljoen FP, Harvey BH. The neuropsychiatric manifestations of COVID-19: interactions with psychiatric illness and pharmacological treatment. Biomed Pharmacother. 2021;135:111200. doi:10.1016/j.biopha.2020.111200
39. U.S. Food & Drug Administration. What is Digital Health? Available from: https://www.fda.gov/medical-devices/digital-health-center-excellence/what-digital-health.
40. Mbunge E, Batani J, Gaobotse G, Muchemwa B. Virtual healthcare services and digital health technologies deployed during coronavirus disease 2019 (COVID-19) pandemic in South Africa: a systematic review. Glob Health J. 2022;6(2):102–113. doi:10.1016/j.glohj.2022.03.001
41. D’Arcy RCN, Sandhu JK, Marshall S, Besemann M. Mitigating Long-Term COVID-19 Consequences on Brain Health. Front Neurol. 2021;12:630986. doi:10.3389/fneur.2021.630986
42. Ahmed MH, Awol SM, Kanfe SG, et al. Willingness to use telemedicine during COVID-19 among health professionals in a low income country. Inform Med Unlocked. 2021;27:100783. doi:10.1016/j.imu.2021.100783
43. Portnoy J, Waller M, Elliott T. Telemedicine in the Era of COVID-19. J Allergy Clin Immunol Pract. 2020;8(5):1489–1491. doi:10.1016/j.jaip.2020.03.008
44. Ferrante TB, Lacktman NM The federal telehealth extension and evaluation act: what you need to know. Available from: https://www.foley.com/en/insights/publications/2022/02/federal-telehealth-extension-evaluation-act.
45. Hassan A, Mari Z, Gatto EM, et al. Global Survey on Telemedicine Utilization for Movement Disorders During the COVID-19 Pandemic. Mov Disord. 2020;35(10):1701–1711. doi:10.1002/mds.28284
46. Chu CM, Wang TH, Lee HC, Lin CS, Feng CC. Emergency physicians’ role in telemedicine care during the coronavirus disease pandemic: experiences from Taiwan. Emerg Med Australas. 2021;33(3):569–571. doi:10.1111/1742-6723.13731
47. Ben-Pazi H, Beni-Adani L, Lamdan R. Accelerating Telemedicine for Cerebral Palsy During the COVID-19 Pandemic and Beyond. Front Neurol. 2020;11:746. doi:10.3389/fneur.2020.00746
48. Manto M, Dupre N, Hadjivassiliou M, et al. Management of Patients with Cerebellar Ataxia During the COVID-19 Pandemic: current Concerns and Future Implications. Cerebellum. 2020;19(4):562–568. doi:10.1007/s12311-020-01139-1
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.