Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Increased Serum S100β Concentration is Associated with Depression in Parkinson’s Disease
Authors Jiang G, Sheng C ![]() , Yan L
, Yan L ![]() , Wang Z, Wang Q, Chen R, Zhao Y
, Wang Z, Wang Q, Chen R, Zhao Y ![]()
Received 29 May 2023
Accepted for publication 14 August 2023
Published 28 August 2023 Volume 2023:19 Pages 1865—1873
DOI https://doi.org/10.2147/NDT.S423312
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Guanghui Jiang,* Cuicui Sheng,* Luxia Yan,* Zipeng Wang, Qing Wang, Rui Chen, Ying Zhao
Department of Neurology, The Affiliated Huai’an Hospital of Xuzhou Medical University, Huai’an, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Zhao; Rui Chen, Email [email protected]; [email protected]
Purpose: To explore the relationship between the serum level of S100 calcium-binding protein, beta chain (S100β) and Parkinson’s disease (PD) with depression.
Patients and Methods: A total of 145 patients with PD and 60 healthy controls matched for sex, age, and years of education in our hospital were selected. Fluorescence quantitative immunochromatography was used to quantify the level of S100β in serum. Clinical manifestations were assessed by Unified Parkinson’s Disease Rating Scale part-III (UPDRS-III), Hoehn & Yahr (H-Y) stage and 17-item Hamilton Rating Scale for Depression (HAMD-17). According to the results of HAMD-17, PD patients were divided into PD with depression group and PD without depression group. The relationship between serum S100β and HAMD-17 scores in PD patients with depression was investigated through correlation analysis and multivariate regression analysis, and receiver operating characteristic (ROC) curve was used to evaluate the diagnostic value of serum S100β.
Results: The level of serum S100β in PD with depression group was significantly higher than that in PD without depression group and control group. In PD patients with depression, serum S100β level was positively correlated with UPDRS-III score, H-Y Scale and HAMD-17 score. The HAMD-17 score was positively correlated with the UPDRS-III and H-Y scales, and the increase in the HAMD-17 score was associated with women. Elevated serum S100β level and UPDRS-III score are independent risk factors for PD with depression. Analysis of receiver operating characteristic (ROC) curves showed that the serum S100β level with a cutoff of 0.28 ng/mL distinguished patients with PD with or without depression with an area under the ROC curve (AUC) of 0.742, sensitivity of 0.696, and specificity of 0.779.
Conclusion: The serum S100β level could be a biomarker of PD with depression.
Keywords: Parkinson’s disease, depression, S100β, risk factors
Introduction
Parkinson’s disease (PD) is a common neurodegenerative disease in middle-aged and elderly people.1 The typical clinical manifestations of PD include bradykinesia, rigidity, tremors, and postural balance disorders.2 Non-motor symptoms of PD have attracted much attention in recent years. Depression is one of the common non-motor symptoms of PD and seriously affects the quality of life of patients.3–5 The incidence of PD with depression is 2.7 ~ 90.0%,6 which affects the quality of life of patients. In severe cases, this can lead to the aggravation of patients’ movement disorders and cognitive disorders, and cause great burden to families and society.7,8 Therefore, early screening and effective interventions for PD patients with depression are important to improve the quality of life and prognosis of patients.
S100 calcium-binding protein, beta chain (S100β), also known as central nervous system-specific protein, is mainly expressed by astrocytes in the brain. It is considered to be a potential biomarker for blood-brain barrier (BBB) dysfunction, decreased neuronal activity and reduced neuroplasticity.9–11 Damage to glial cell activity, BBB function and neuroplasticity is associated with various neurological and psychological disorders. Therefore, we believe that S100β protein may be involved in the pathophysiology of emotional disorders, and thus has some potential links with PD depression.
Previous studies have shown that there is a correlation between cerebrospinal fluid S100β concentration and depressive episodes.12 The serum S100β level in patients with depression is significantly higher than that in patients without depression.13 In PD patients, studies have shown that elevated serum S100β protein levels are associated with the severity of PD and motor symptoms.14 However, the relationship between serum S100β levels and depressive symptoms in PD has not been studied. At present, the pathogenesis of depression in PD is not clear, which may be related to the loss of neurotransmitters such as 5-hydroxytryptamine (5-HT) and norepinephrine in the brain.15 In patients with depression treated with 5-HT reuptake inhibitors, we found a decrease in S100β levels.16 It is also believed that the occurrence of depression in PD may be related to the severity and motor symptoms of PD itself. Herein, the purpose of this study was to investigate whether serum S100β levels are associated with PD with depression.
Materials and Methods
Participants
All participants were recruited from the Affiliated Huai’an Hospital of Xuzhou Medical University. This study included 145 participants: 69 PD patients with depression, 76 PD patients without depression, and 60 healthy controls. All patients with PD met the following inclusion criteria: (a) Meeting the diagnostic criteria set by the UK Brain Bank for PD;17 (b) Aged 40–80 years, Han Chinese. Exclusion criteria: (a) History of craniocerebral trauma, surgery, or cancer; (b) drug-induced secondary Parkinsonian syndrome, severe craniocerebral trauma, vascular and other secondary syndromes of PD; (c) Progressive supranuclear palsy, multiple-system atrophy or other syndromes of PD; (d) Patients using dopamine agonists, monoamine oxidase-B inhibitors and other anti-Parkinson’s disease drugs, antidepressants and anti-anxiety drugs; (e) Severe cognitive impairment, Mini-Mental State Examination (MMSE) score18 less than 24 points; (f) Serious systemic diseases of the heart, liver, or kidney; (g) Recent infection. The healthy control group was healthy volunteers in the physical examination center of the Affiliated Huai’an Hospital of Xuzhou Medical University. Their age, gender, and years of education were matched with PD patients, and there were no severe physical or mental illnesses.
The study protocol was approved by the Ethics Committee of the Second People’s Hospital of Huai’an City (Huai’an, China).
Clinical Assessment
All patients in the PD group were evaluated for severity of PD using H–Y Scale.19 UPDRS-III20 was used to assess the motor function of PD patients, and MMSE18 was used to evaluate the cognitive function of patients. All clinical evaluations were performed during “on” condition.
Depression Measure and Criteria
The screening or measuring the severity of such depressive symptoms in PD was measured by the HAMD-17,21 it has been validated and traditionally recommended tool in individuals with PD. The scale includes 17 aspects: depression, guilt, suicidal ideation, sleep disorders (difficulty falling asleep, lack of sleep, early awakening), work and interest, block, agitation, mental anxiety, somatic anxiety, gastrointestinal symptoms, systemic symptoms, sexual symptoms, hypochondria, weight loss and insight. Among them, sleep disorders, gastrointestinal symptoms, systemic symptoms, sexual symptoms and weight loss were scored as follows: no abnormal 0 points, mild 1 points, severe 2 points; the remaining aspects were recorded as no abnormal 0 points, mild 1 point, moderate 2 points, severe 3 points, and extremely severe 4 points according to the severity; the full score of the scale was 54 points, and the higher the score, the more severe the depression.
According to the literature report,22 the optimal threshold to utilize for maximum discrimination between depressed and non-depressed PD patients was reached at a cut-off score of 13/14 for the HAMD-17. Therefore, we divided PD patients into two groups according to the HAMD-17 score: PD without depression group (HAMD-17 ≤ 13 points) and PD with depression group (HAMD-17 ≥ 14 points). HAMD-17 assessment was also performed during “on” condition.
Measurement of S100β
Venous blood (5 mL) was collected on an empty stomach in people from both groups in the morning. The sample was allowed to stand at room temperature for 25 min. Then, the sample was centrifuged (4000 rpm, 15 min, room temperature) to separate and extract serum. Fluorescence quantitative immunochromatography was used to quantify the level of S100β in serum. This serum marker was detected by a fluorescence immunoassay analyzer (1600; Getein Biotech; Nanjing, China).
Acquisition of Remaining Risk Factors
Basic information such as gender, age, years of education and body mass index (BMI) were collected. The course of disease, hypertension history, diabetes history, smoking history and drinking history were recorded. Neutrophil ratio and high-sensitivity C-reactive protein (hs-CRP) were measured with an automatic biochemical analyzer (TBA 40FR, Toshiba, Tokyo, Japan).
Statistical Analyses
Data were analyzed using SPSS 25.0 (IBM, Armonk, NY, USA). Graphs were created using Prism 9.0 (GraphPad. La Jolla, CA, USA). The normality test was carried out on measurement data. Data with a normal distribution are expressed as the mean ± SD. Data with a non-normal distribution are expressed as median (interquartile range). The Student’s t-test was employed to compare data between the two groups. Multiple groups of data were compared by ANOVA for those satisfying the conditions of a parametric test, and further two-by-two comparisons were made by the Bonferroni method. The Kruskal–Wallis test was used for data not satisfying the conditions of a parametric test, and further two-by-two comparisons were made by the Nemenyi method. Count data describe the number ofcases, and the χ2 test was used for comparison between groups. Correlations between variables were analyzed by applying Pearson or Spearman correlation coefficients. Multiple linear regression analysis was employed to explore independent risk factors for PD with depression. ROCs were used to the efficacy of serum S100β level in distinguishing PD with and without depression. P < 0.05 (two-tailed) was deemed significant.
Results
Comparison of Baseline Characteristics of Participants
The demographic characteristics of PD patients and normal controls are shown in Table 1. There was no significant difference in gender, age, years of education, BMI, disease duration, smoking history, drinking history, hypertension, diabetes, neutrophil ratio and hs-CRP between PD with depression group, PD without depression group and normal control group (all p > 0.05). However, compared with PD without depression group, the UPDRS-III score (p < 0.05), H-Y Scale score (p < 0.05) and HAMD-17 score (p < 0.05) of PD with depression group were significantly higher (Table 1). There was no significant correlation between serum S100β level and age, sex, education years, BMI, course of disease, drinking and smoking history, hypertension and diabetes history, neutrophil ratio and hs-CRP level in each group.
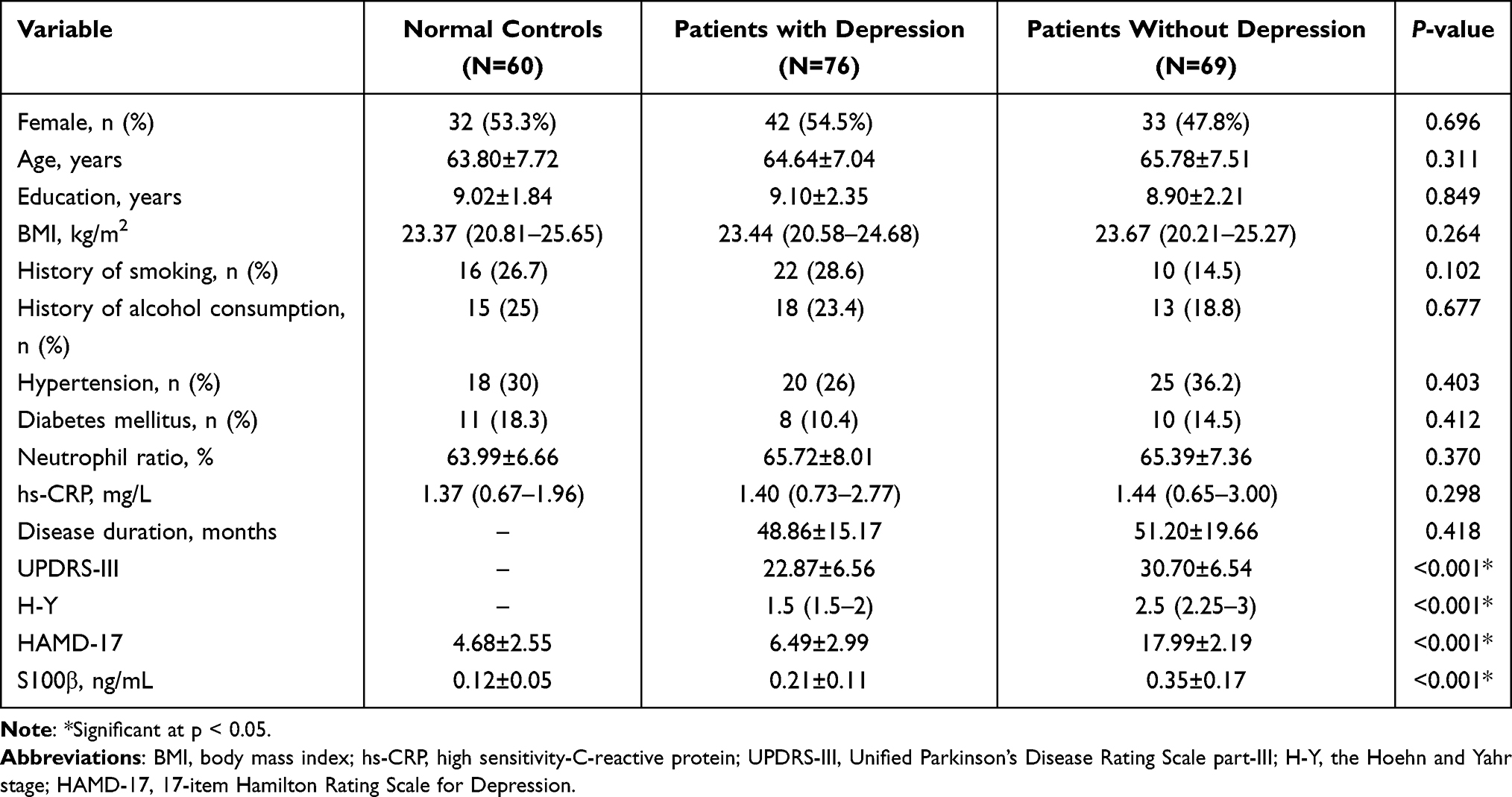 |
Table 1 Comparison of Baseline Characteristics Between PD Patients with and without Depression and Healthy Controls |
Serum S100β Level and Its Relationship with Clinical Features in PD Patients with and without Depression
The levels of serum S100β in PD with depression group (0.35 ± 0.17 ng/mL) and PD without depression group (0.21 ± 0.11 ng/mL) were higher than those in control group (0.12 ±0.05 ng/mL) (Figure 1).
 |
Figure 1 Comparison of serum S100β among PD with depression group, PD without depression group and normal control group. Note: ****p < 0.001. |
Correlation analysis showed that serum S100β level was positively correlated with UPDRS-III, H-Y grade and HAMD-17 score in PD patients with depression. HAMD-17 score was positively correlated with UPDRS-III and H-Y, and the increase of HAMD-17 score was related to women (Figure 2). In PD patients without depression, serum S100β level was positively correlated with UPDRS-III (r = 0.493, p < 0.001) and H-Y (r = 0.352, p = 0.002). The control group showed no significant correlation.
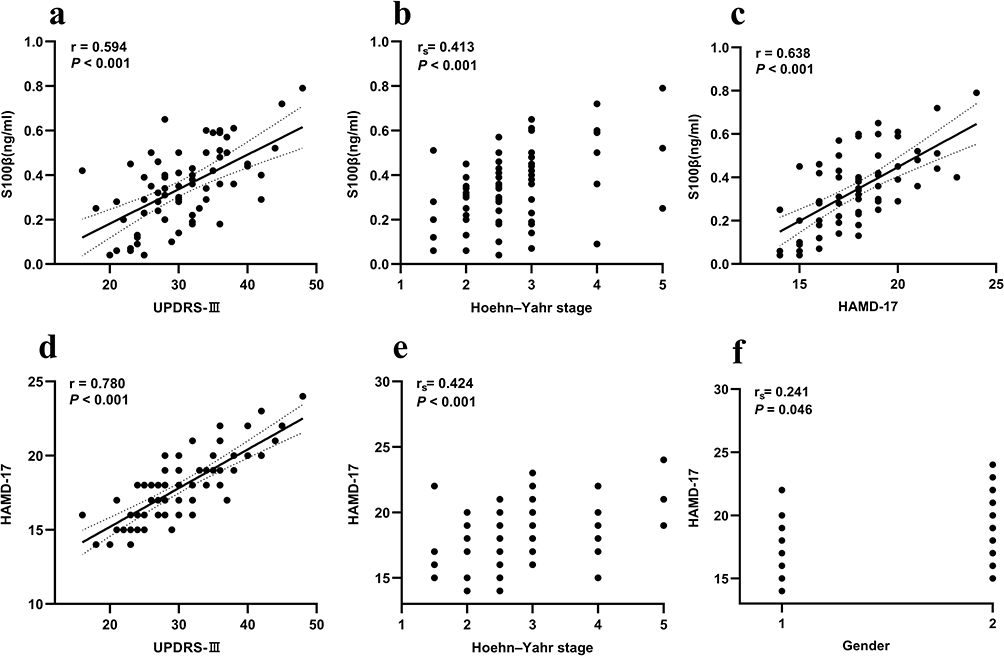 |
Figure 2 Correlation analysis of serum S100β levels according to UPDRS-III score (a), Hoehn and Yahr stage (b) and HAMD-17 score (c), and HAMD-17 score according to UPDRS-III score (d), Hoehn and Yahr stage (e) and Gender (f) in PD patients with depression. Gender 1 for male, 2 for female. Abbreviations: UPDRS-III, Unified Parkinson’s Disease Rating Scale Part-III; HAMD-17, 17-item Hamilton Rating Scale for Depression; r, Pearson’s correlation coefficient, rs, Spearman’s rank correlation coefficient; P, level of significance of r or rs. |
Predictive Value of Serum S100β Level in PD with Depression
After collinearity diagnosis, we used UPDRS-III, H-Y Scale score, serum S100β level and gender as independent variables, and HAMD-17 score as dependent variable to perform multiple linear regression analysis. The results showed that serum S100β level (p = 0.002), and UPDRS-III score (p < 0.001) were independent risk factors for PD with depression (Table 2).
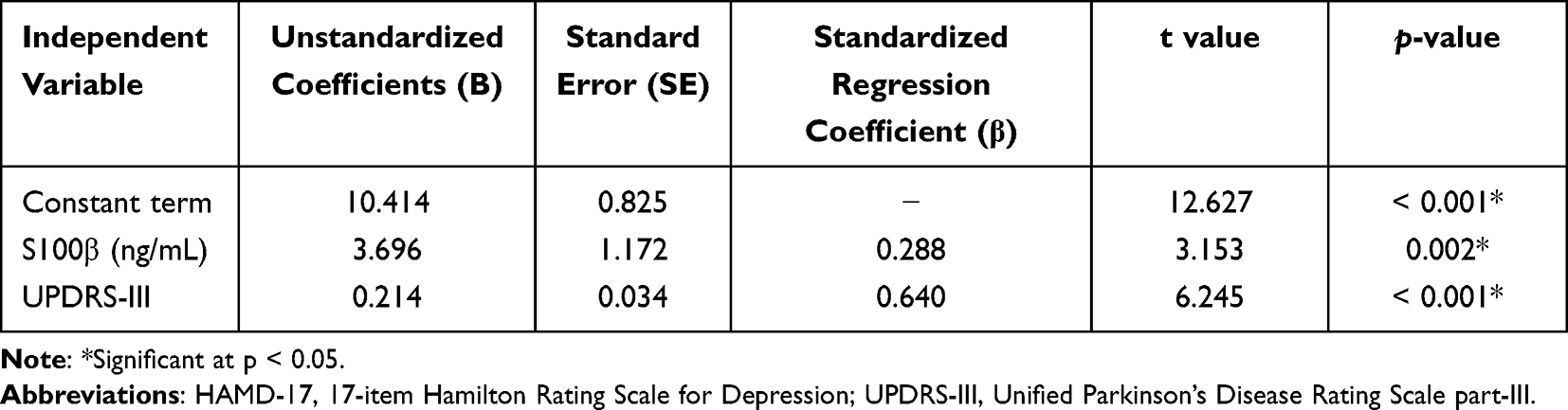 |
Table 2 Multiple Linear Regression Analysis Result of HAMD-17 as the Dependent Variable |
ROC curve analysis showed that serum S100β could distinguish PD patients with depression from those without depression with a cut-off value of 0.28 ng/mL. The area under the ROC curve (AUC) was 0.742, the sensitivity was 0.696, and the specificity was 0.779 (Figure 3).
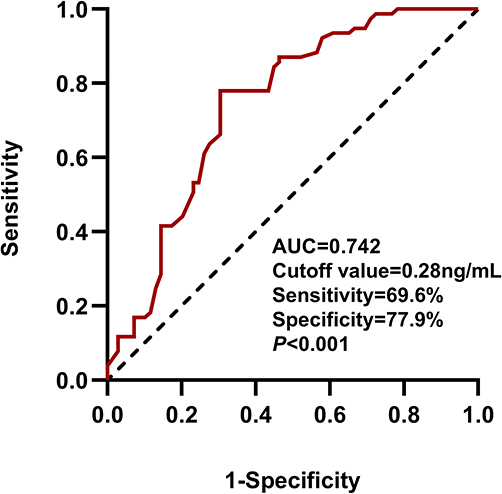 |
Figure 3 ROC to evaluate the ability of serum S100β levels to differentiate PD patients with depression from PD without depression. Abbreviations: ROC, Receiver operating characteristic curve; AUC, area under curve. |
Discussion
In this study, we collected clinical data from 145 PD patients and 60 healthy controls, and analyzed the relationship between serum S100β levels and the results of clinical evaluation. The results showed that: (1) Serum S100β levels in PD with depression were significantly higher than that in PD without depression group and the control group. (2) Serum S100β levels in PD with depression group were positively correlated with UPDRS-III, H-Y scale and HAMD-17 scores. (3) Elevated serum S100β levels and UPDRS-III scores were independent risk factors for PD with depression. Serum S100β level has a high efficacy in distinguishing PD with depression and PD without depression.
Consistent with previous studies,23 we found that serum S100β levels in PD patients were higher than those in healthy controls, suggesting that S100β may play a role in the pathogenesis of PD. Human autopsy studies24 also showed that compared with the control controls, the levels of S100β in substantia nigra and cerebrospinal fluid of PD patients increased, and S100β may be a new mediator of PD neurodegeneration. The activation of astrocytes in PD patients will promote the release of S100β. S100β binds to advanced glycation end products (RAGE) and triggers the activation of downstream factors, leading to neuroinflammation amplification, oxidative damage and neurotransmitter metabolism disorder. The interaction with dopamine D2 receptor affects dopamine metabolism, which is a potential mechanism of PD pathogenesis.25–27
At the same time, we also found that serum S100β levels in PD patients with depression were significantly higher than that in PD patients without depression. The serum S100β level in PD patients with depression was significantly positively correlated with HAMD-17 score, indicating that S100β may play an essential role in the occurrence and development of PD depression. Studies28 have shown that depression is related to the density of glial cells in the prefrontal cortex. The increase of S100β observed in this study may be closely related to the activation of astrocytes. The binding of extracellular 5-HT to 5-HT1A receptor on astrocytes in patients with depression can also cause S100β release.15 In addition, this study showed that compared with PD patients without depression, PD patients with depression have higher motor symptoms and disease severity scores. UPDRS-III score was an independent risk factor for PD with depression. It is considered that there may be a common pathological basis with PD motor symptoms and depression. With the decline of motor dysfunction and the progressive decline of patients’ daily living ability, they lose confidence in disease control and further aggravate depression. It may also be that depression has a greater impact on the motor symptoms of PD patients. In addition to the strong correlation in the correlation analysis of PD with depression, serum S100β also showed high sensitivity and specificity in distinguishing PD with depression from PD without depression. Therefore, serum S100β may be an effective biomarker for PD with depression.
In a previous study, Benitez et al29 who found that S100β levels of participants with reported history of depression were higher than for those without such a history. In our study, the control group did not include patients with a history of reported depression. Therefore, it was not possible to verify the results of the previous study. In future studies, we will consider including such a population to further explore the relationship between S100β and depression. Riedel et al30 found that women are more prone to depression than men, and the probability of depression in female PD patients is 1.3 times that of men. In our study, we did not find significant gender differences in the incidence of PD depression. However, the HAMD-17 score of PD patients with depression was correlated with women, but the correlation was not strong. And women were not independent risk factors for PD depression. Further research is needed to explore the relationship between PD depression and gender.
However, the exact mechanism underlying the relationship between S100β and depression in PD is unclear. It may be related to the influence of the 5-HT function.31 The disorder of 5-HT and norepinephrine signaling pathways in the brain is considered to be related to the pathophysiology of various psychiatric disorders.32 5-HT plays an essential role in the regulation of depression. However, S100β is the main neurotrophic factor of 5-HT neurons at physiological concentration, while elevated concentration will produce cytotoxic.33 The binding of extracellular 5-HT to 5-HT1A receptor on astrocytes can trigger the release of S100β. Another possible explanation is based on the pathological mechanism of PD. It is currently believed that in addition to the metabolic imbalance of dopamine and acetylcholine in the brain of patients with Parkinson’s disease, there is still a decrease in 5-HT.34 The pathological changes of PD, that is, the aggregation of α-synuclein, can activate astrocytes, increase the synthesis and secretion of S100β, and enter the blood through the damaged blood-brain barrier, eventually increasing the level of S100β protein in the blood. As an inflammatory factor, S100β can increase the release of pro-inflammatory cytokines by activating NF-kβ and p38 MAPK, leading to neuroinflammation amplification, oxidative damage and neurotransmitter metabolism disorder, thus affecting the level of 5-HT and leading to depression.35 In addition, the loss of dopaminergic neurons in the ventral tegmental area was found to be associated with depression in PD patients. We believe that the relationship between S100β and depression in PD patients deserves further study.
Chronic neuroinflammation is one of the characteristics of PD and may be involved in the beginning and progression of the disease. Considering that S100β is also elevated in other acute inflammatory diseases, this study also analyzed the levels of infection-related indicators such as neutrophil ratio and hs-CRP in each group of patients, and the results did not show significant differences (Table 1). At the same time, combined with the patient’s clinical manifestations and other auxiliary examinations, the impact of other acute infectious diseases on the results of this study was excluded.
This study explored the clinical characteristics of PD patients with depression and its relationship with serum S100β levels, but there are still some limitations: First, our clinical data lack some information, such as employment information, family history and other data, which may also affect the depression of PD patients. Second, the sample size is relatively modest, and larger sample size studies are still needed in the future to further verify our results. Third, our study was entirely Han Chinese and lacked ethnic diversity. Fourth, this study is a cross-sectional study. In the future, longitudinal studies are still needed to determine whether serum S100β can be used as an effective biomarker for PD with depression.
Conclusion
Elevated serum S100β level is an independent risk factors for PD with depression. Serum S100β is expected to be a biomarker for PD with depression. The detection of serum S100β level may be helpful for the early identification of PD with depression.
Abbreviations
PD, Parkinson’s disease; S100β, S100 calcium-binding protein, beta chain; UPDRS-III, part III of the Unified Parkinson Disease Rating Scale-III; H–Y, Hoehn–Yahr; HAMD-17, 17-item Hamilton Rating Scale for Depression; ROC, receiver operating characteristic; AUC, area under the ROC curve; MMSE, Mini-Mental State Examination; BMI, Body Mass Index; hs-CRP, high-sensitivity C-reactive protein; 5-HT, 5-hydroxytryptamine.
Ethics Approval and Consent to Participate
The studies involving human participants were reviewed and approved by the Human Ethics Committees of The Affiliated Huai’an Hospital of Xuzhou Medical University. Informed consent was obtained for experimentation with human subjects. Every individual was informed about the aims of the study and provided written consent before participation. Written Informed consent was obtained from healthy controls and from the legal guardian/next of kin for Parkinson’s Disease patients. All methods were carried out in accordance with relevant guidelines and regulations/Declaration of Helsinki.
Author Contributions
Rui Chen and Ying Zhao are co-corresponding authors. All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest.
References
1. Homayoun H. Parkinson disease. Ann Intern Med. 2018;169(5):ITC33–ITC48. doi:10.7326/AITC201809040
2. Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: a review. JAMA. 2020;323(6):548–560. doi:10.1001/jama.2019.22360
3. Ray S, Agarwal P. Depression and anxiety in Parkinson disease. Clin Geriatr Med. 2020;36(1):93–104. doi:10.1016/j.cger.2019.09.012
4. Heimrich KG, Schönenberg A, Santos-García D, Mir P, Group CS, Prell T. The impact of non motor symptoms on health-related quality of life in Parkinson’s Disease: a network analysis approach. J Clin Med. 2023;12(7):2573.
5. Modugno N, Antonini A, Tessitore A, et al. Impact of supporting people with advanced Parkinson’s Disease on carer’s quality of life and burden. Neuropsychiatr Dis Treat. 2020;16:2899–2912. doi:10.2147/NDT.S256217
6. Cong S, Xiang C, Zhang S, Zhang T, Wang H, Cong S. Prevalence and clinical aspects of depression in Parkinson’s disease: a systematic review and meta-analysis of 129 studies. Neurosci Biobehav Rev. 2022;141:104749. doi:10.1016/j.neubiorev.2022.104749
7. Heyn PC, Wong DC, Hirsch MA, van Wegen E, Hein A, Sood P. Falls prevention, home safety, and rehabilitation services for people with Parkinson disease: a client and caregiver guide. Arch Phys Med Rehabil. 2023;104(7):1161–1164. doi:10.1016/j.apmr.2022.11.020
8. Frisina PG, Borod JC, Foldi NS, et al. Depression in Parkinson’s disease: health risks, etiology, and treatment options. Neuropsychiatr Dis Treat. 2008;4(1):81–91. doi:10.2147/ndt.s1453
9. Jang BS, Kim H, Lim SW, Jang KW, Kim DK. Serum S100B levels and major depressive disorder: its characteristics and role in antidepressant response. Psychiatry Investig. 2008;5(3):193–198. doi:10.4306/pi.2008.5.3.193
10. Kim JK, Kim SG, Kim HJ, Song YR. Serum S100B protein is associated with depressive symptoms in patients with end-stage renal disease. Clin Biochem. 2012;45(18):1573–1577. doi:10.1016/j.clinbiochem.2012.08.014
11. Güleş E, Iosifescu DV, Tural Ü. Plasma neuronal and glial markers and anterior cingulate metabolite levels in major depressive disorder: a Pilot Study. Neuropsychobiology. 2020;79(3):214–221. doi:10.1159/000505782
12. Grabe HJ, Ahrens N, Rose HJ, Kessler C, Freyberger HJ. Neurotrophic factor S100 beta in major depression. Neuropsychobiology. 2001;44(2):88–90. doi:10.1159/000054922
13. Fang Y, Xiao SF, Zhang SY, Qiu Q, Wang T, Li X. Increased plasma S100β level in patients with major depressive disorder. CNS Neurosci Ther. 2016;22(3):248–250. doi:10.1111/cns.12517
14. Schaf DV, Tort AB, Fricke D, et al. S100B and NSE serum levels in patients with Parkinson’s disease. Parkinsonism Relat Disord. 2005;11(1):39–43. doi:10.1016/j.parkreldis.2004.07.002
15. Stroth N, Svenningsson P. S100B interacts with the serotonin 5-HT7 receptor to regulate a depressive-like behavior. Eur Neuropsychopharmacol. 2015;25(12):2372–2380. doi:10.1016/j.euroneuro.2015.10.003
16. Pawluski JL, Brain U, Hammond GL, Oberlander TF. Selective serotonin reuptake inhibitor effects on neural biomarkers of perinatal depression. Arch Womens Ment Health. 2019;22(3):431–435. doi:10.1007/s00737-018-0931-1
17. Hughes AJ, Daniel SE, Kilford L, Lees AJ. Accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992;55(3):181–184. doi:10.1136/jnnp.55.3.181
18. Li H, Jia J, Yang Z, Moreau N. Mini-mental state examination in elderly Chinese: a Population-Based Normative Study. J Alzheimers Dis. 2016;53(2):487–496. doi:10.3233/JAD-160119
19. Goetz CG, Poewe W, Rascol O, et al. Movement disorder society task force report on the Hoehn and Yahr staging scale: status and recommendations. Mov Disord. 2004;19(9):1020–1028. doi:10.1002/mds.20213
20. Goetz CG, Fahn S, Martinez-Martin P, et al. Movement disorder society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): process, format, and clinimetric testing plan. Mov Disord. 2007;22(1):41–47. doi:10.1002/mds.21198
21. Leentjens AF, Verhey FR, Lousberg R, Spitsbergen H, Wilmink FW. The validity of the hamilton and montgomery-asberg depression rating scales as screening and diagnostic tools for depression in Parkinson’s disease. Int J Geriatr Psychiatry. 2000;15(7):644–649. doi:10.1002/1099-1166(200007)15:7<644::AID-GPS167>3.0.CO;2-L
22. Lj Z, Stefanova E, Petrovic M, Stojkovic T, Kostic VS. Apathy and depression in Parkinson’s disease: the Belgrade PD study report. Parkinsonism Relat Disord. 2012;18(4):339–342. doi:10.1016/j.parkreldis.2011.11.020
23. Michetti F, D’Ambrosi N, Toesca A, et al. The S100B story: from biomarker to active factor in neural injury. J Neurochem. 2019;148(2):168–187. doi:10.1111/jnc.14574
24. Sathe K, Maetzler W, Lang JD, et al. S100B is increased in Parkinson’s disease and ablation protects against MPTP-induced toxicity through the RAGE and TNF-α pathway. Brain. 2012;135(Pt 11):3336–3347. doi:10.1093/brain/aws250
25. Bidasee KR, Dinçer UD, Besch HR
26. MacMahon Copas AN, McComish SF, Fletcher JM, Caldwell MA. The pathogenesis of Parkinson’s disease: a complex interplay between astrocytes, microglia, and T lymphocytes. Front Neurol. 2021;12:666737. doi:10.3389/fneur.2021.666737
27. Koerich S, Parreira GM, de Almeida DL, Vieira RP, de Oliveira A, de Almeida DL. Receptors for Advanced Glycation End Products (RAGE): promising targets aiming at the treatment of neurodegenerative conditions. Curr Neuropharmacol. 2023;21(2):219–234. doi:10.2174/1570159X20666220922153903
28. Sarrouilhe D, Mesnil M, Dejean C. Targeting gap junctions: new insights into the treatment of major depressive disorder. Curr Med Chem. 2019;26(20):3775–3791. doi:10.2174/0929867325666180327103530
29. Benitez A, Gunstad J, Hughes J, et al. Troponin and S100 beta are associated with depression in healthy older adults. Aging Ment Health. 2009;13(6):894–898. doi:10.1080/13607860903046438
30. Riedel O, Heuser I, Klotsche J, Dodel R, Wittchen HU. Occurrence risk and structure of depression in Parkinson disease with and without dementia: results from the GEPAD Study. J Geriatr Psychiatry Neurol. 2010;23(1):27–34. doi:10.1177/0891988709351833
31. Fakhoury M. Revisiting the serotonin hypothesis: implications for major depressive disorders. Mol Neurobiol. 2016;53(5):2778–2786. doi:10.1007/s12035-015-9152-z
32. Bhatt S, Devadoss T, Manjula SN, Rajangam J. 5-HT(3) receptor antagonism a potential therapeutic approach for the treatment of depression and other disorders. Curr Neuropharmacol. 2021;19(9):1545–1559. doi:10.2174/1570159X18666201015155816
33. Schulte-Herbrüggen O, Hörtnagl H, Ponath G, Rothermundt M, Hellweg R. Distinct regulation of brain-derived neurotrophic factor and noradrenaline in S100B knockout mice. Neurosci Lett. 2008;442(2):100–103. doi:10.1016/j.neulet.2008.07.013
34. Samudra N, Patel N, Womack KB, Khemani P, Chitnis S. Psychosis in Parkinson disease: a review of etiology, phenomenology, and management. Drugs Aging. 2016;33(12):855–863. doi:10.1007/s40266-016-0416-8
35. Angelopoulou E, Paudel YN, Piperi C. Emerging role of S100B protein implication in Parkinson’s disease pathogenesis. Cell Mol Life Sci. 2021;78(4):1445–1453. doi:10.1007/s00018-020-03673-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Psychological Impact of Quarantine During the COVID-19 Pandemic on Quarantined Non-Healthcare Workers, Quarantined Healthcare Workers, and Medical Staff at the Quarantine Facility in Saudi Arabia
Alfaifi A, Darraj A, El-Setouhy M
Psychology Research and Behavior Management 2022, 15:1259-1270
Published Date: 17 May 2022
Depression and Associated Risk Factors Among Type 2 Diabetic Patients: A Cross Sectional Study on a Convenience Sample from the Diabetic Center, Khamis Mushait; Saudi Arabia
Abuhegazy H, Mujairi A, Banah F, Agdi Y, Elkeshishi H, Kamel A, Abdullah A, Elsheikh M
Neuropsychiatric Disease and Treatment 2022, 18:1975-1984
Published Date: 31 August 2022
Association Between Breakfast Consumption and Suicidal Attempts in Adolescents
Park H, Lee K
Psychology Research and Behavior Management 2022, 15:2529-2541
Published Date: 13 September 2022
Risk Factors for Negative Emotions in Patients Undergoing Radical Resection of Hilar Cholangiocarcinoma and Their Influence on Prognosis
Yin R, Xu S, Zhu J, Zhu H, He C
International Journal of General Medicine 2023, 16:5841-5853
Published Date: 11 December 2023
Development and Validation of a Nomogram Model for Accurately Predicting Depression in Maintenance Hemodialysis Patients: A Multicenter Cross-Sectional Study in China
Zhou X, Zhu F
Risk Management and Healthcare Policy 2024, 17:2111-2123
Published Date: 3 September 2024