Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 11
Increased incidences of noninfectious comorbidities among aging populations living with human immunodeficiency virus in Ecuador: a multicenter retrospective analysis
Authors Hernández I ![]() , Barzallo J, Beltrán S, Castillo A
, Barzallo J, Beltrán S, Castillo A ![]() , Cevallos N
, Cevallos N ![]() , Hernández P, López C, Vera R
, Hernández P, López C, Vera R ![]() , Yerovi G, Mendoza A, Terán S, Izurieta A, Teran E
, Yerovi G, Mendoza A, Terán S, Izurieta A, Teran E ![]()
Received 4 November 2018
Accepted for publication 18 February 2019
Published 1 April 2019 Volume 2019:11 Pages 55—59
DOI https://doi.org/10.2147/HIV.S193412
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Isabel Hernández,1,2 Julio Barzallo,3 Simón Beltrán,4 Alberto Castillo,5 Nelson Cevallos,6 Patricio Hernández,7 Camilo López,8 Rita Vera,9 Gabriela Yerovi,10 Alejandra Mendoza,1 Santiago Terán,1 Andres Izurieta,11 Enrique Teran1
1Colegio de Ciencias de la Salud, Universidad San Francisco de Quito, Quito, Ecuador; 2Facultad de Enfermería, Pontificia Universidad Católica del Ecuador, Quito, Ecuador; 3Hospital Teofilo Dávila, Ministerio de Salud Pública, Machala, Ecuador; 4Hospital Carlos Andrade Marín, Instituto Ecuatoriano de Seguridad Social, Quito, Ecuador; 5Hospital Eugenio Espejo, Ministerio de Salud Pública, Quito, Ecuador; 6Hospital Enrique Garcés, Ministerio de Salud Pública, Quito, Ecuador; 7Hospital de Infectología Dr. José Daniel Rodríguez Maridueña, Ministerio de Salud Pública, Guayaquil, Ecuador; 8Hospital Teodoro Maldonado Carbo, Instituto Ecuatoriano de Seguridad Social, Guayaquil, Ecuador; 9Hospital Abel Gilbert Pontón, Ministerio de Salud Pública, Guayaquil, Ecuador; 10Programa Nacional para Control del VIH, Ministerio de Salud Pública, Quito, Ecuador; 11Department of Computer Engineering, College of Engineering, University of South Florida, Tampa, FL, USA
Introduction: Besides the well-known increased risk of developing HIV-related infectious comorbidities; compared with the general population, people living with HIV (PLHIV) may also have an increased risk of developing noninfectious comorbidities (NICMs). This is the first study intended to determine the NICMs rates affecting PLHIV who were under cART regimen in Ecuador.
Methods: A total of 503 HIV-positive patients were evaluated during the period June 2015-November 2016 and included in a multicenter retrospective, cross-sectional study conducted in seven main government and nongovernment community-based hospitals in Ecuador.
Results: The average age of the participants was 39.2±11.9 years old and the majority of them were male (67.2%). The average age at HIV diagnosis was 34.1 years old and cART in average was started 15.9 months after HIV-diagnosis. Recruited patients were receiving cART for an average of 59.2±40.2 months. Only 9.9% (n=50) of the patients did not show any NICMs. Diabetes and pre-diabetes was found in 6% (n=30) and 16.3% (n=82) patients, respectively; however, dyslipidemia and overweight/obesity was frequent, as they affected 41.4% (n=208) and 36.4% (n=183) patients, respectively. Sixty patients (11.9%) were diagnosed with depression and 28.2% (n=142) of the studied subjects were found to have other NICMs.
Conclusion: Prevalence of NICMs among subjects under cART was greater than that reported among the Ecuadorian general population, therefore specific public health actions are required to make patients aware of and prevent NICMs among PLHIV in Ecuador.
Keywords: HIV noninfectious comorbidities, people living with HIV, HIV combined antiretroviral therapy, HIV diagnosis, HIV treatment, HIV in developing countries, HIV in Ecuador
Introduction
In developing countries, the epidemic of human immunodeficiency virus (HIV) and the growing prevalence of noninfectious comorbidities (NICMs) are interconnected health crises.1 Cardiovascular disease, hypertension, and diabetes mellitus all have direct and indirect relationships with HIV and combined antiretroviral therapy (cART). There is also a growing prevalence of NICMs in the populations of many developing countries due to dietary and lifestyle changes and the increase of life expectancies.1 The implementation of combined antiretroviral therapy (cART) therapy among HIV patients from developing countries has substantially increased the survival of these populations, as evidence, Ugandan patients receiving cART can expect an almost normal life expectancy.2 As people living with HIV (PLHIV) in developing countries are experiencing life expectancies similar to those of the general population, they may have an increased risk of developing noninfectious comorbidities (NICMs) due to aging of the HIV population, acquiring HIV at older ages, the disease itself, and the use of long-term ART.3–6
NICMs among PLHIV include: HIV-associated neurocognitive disorders,7 AIDS-defining illness,8 and mortality,9 diabetes, dyslipidemias, chronic kidney disease, etc.,10 which may be driven by a variety of factors not limited to aging of the populations living with HIV, acquiring of HIV at older ages, delayed diagnosis, immune senescence,11 and differential response to antiretroviral therapy (ART).12
Although prevalence rates of human immunodeficiency virus (HIV) in Latin America remain stable (between 0.2% and 0.7%),13 in other populations living with the virus the epidemic is globally expanding among men who have sex with men (MSM) independently of country or gross domestic product.14 In 2013, the United Nations estimated between 0.3% and 0.7% of adults aged 15–49 years old were living with HIV in Ecuador.15 In addition, according to the Ecuadorian Ministry of Public Health and its National Epidemiological Program of HIV/AIDS, in 2014 there were 6,765 subjects under combination antiretroviral therapy (cART)-treated HIV, and 72.5% of cases of those people were between 20 and 44 years old.16
The HIV epidemic in Ecuador has been reported to be concentrated among high risk populations. Previous research conducted in two major cities of Ecuador estimated the prevalence of HIV among MSM to be 14.5% in Quito and 27.8% in Guayaquil,17 meanwhile in Esmeraldas MSM estimated a prevalence of 10%18 and among Female Commercial Sex Workers (FCSW) 0.7%.19
In Ecuador, cART was introduced more than 10 years ago and provided free of charge by the government. For that reason, there are national treatment guidelines for PLHIV requiring patients to visit the clinics frequently to monitor viral load, response to treatment and overall health. However, there is no data on the noninfectious diseases affecting people under the antiretroviral regimen. Thus, the aim of this study was to determine the NICMs affecting people living with HIV infection while receiving cART in Ecuador and the association between cART and NICMs prevalence.
Methods
This was a multicenter retrospective cross-sectional study conducted between June 2015 and November 2016 at seven public community-based hospitals that provide services to most of the PLHIV in Ecuador including the capital Quito, the main port Guayaquil, and the border port Machala. Based on the total number of diagnosed patients registered by the Ecuadorian Ministry of Public Health in 2014 and using 80% power with an estimated error of 5%, a proper sample size was determined. Those cases were later distributed according to the demographic density of each hospital they attended. A simple randomized sample was implemented to select the participants at each research center.
Access to medical records and data analysis was approved by the Human Research Ethics Committee from Universidad San Francisco de Quito (2014-168IN). It was a retrospective study using data already collected, patient data was anonymized in accordance with the Declaration of Helsinki and patients’ written consent was not obtained. Moreover, a waiver from the Human Research Ethics Committees was obtained.
The investigator or qualified designee reviewed all inclusion and exclusion criteria to ensure that the subject qualified for the study. Criteria for inclusion in the study was: 1) HIV positive; 2) adults 21 years or older at the beginning of the data collection period; and 3) patients with active charts who had been receiving health care at that clinic for 6 months or longer. Records were excluded if: 1) AIDS stages 3 and 4 had already been diagnosed as defined by World Health Organization (this group was excluded due to the possibility of specific comorbidities not necessarily associated with those not having AIDS); 2) Pregnant women (this group was excluded because during pregnancy women can present comorbid conditions not necessarily related to HIV status); and 3) patients that participated in a clinical trial during the period of the sample selection or that are currently enrolled in a clinical trial.
The following demographic information was collected from each patient: date of birth (to calculate age in years), gender (male, female, or transgender), weight (in kilograms), height (in centimeters). The weight and height were used to calculate the Body Mass Index (BMI). Age at HIV diagnosis was also registered and then grouped into four pre-defined groups: younger than 26, 26–30, 31–40, and older than 40 years old.
The following comorbidities, post-HIV infection, were assessed: 1) history of acute coronary syndrome, angina pectoris, congestive heart failure, or revascularization procedure; 2) pre-diabetes or diabetes mellitus; 3) hypertension, dyslipidemia, previous stroke/transient ischemic attack (TIA), peripheral vascular disease, or chronic kidney disease; 4) smoker/history of smoking, history of drug/alcohol abuse, overweight/obesity, chronic Hepatitis C, chronic Hepatitis B, tuberculosis, depression, lipodystrophy, fat accumulation, and osteoporosis; and 5) Any other comorbid condition described in the patient’s record was also documented. In all cases, the treating physician defined clinical events.
Descriptive statistics were used to summarize patient demographics, morbidity, and clinical characteristics. For the inferential statistical analysis, Pearson Chi-Square tests and ANOVA were calculated to assess the possible association of cART beginning and duration with NICMs prevalence and a p-value <0.05 was consider as significant.
Results
A total of 503 patients were analyzed. Average age was 39.2 (SD 11.9) years old and there was a predominance of males (67.2%). Interestingly, average age at HIV diagnosis was 34.1 years old and it was equally distributed among the pre-defined groups.
Thirty percent of patients began treatment early, during the first month after diagnosis. Another 18% subjects began their treatment up to 6 months after confirmation that they had HIV and in 13% of the cases therapy initiated before the first year. Treatment was initiated until 2 years after diagnosis in 17% of the subjects, and unfortunately in 24% of the patients, therapy did not start until more than 2 years.
Patients recruited in the study had been receiving HIV-treatment for 59.2 (SD 40.2) months. From those, 19% have been treated for less than 24 months, 20% between 24 and 48 months, and the remaining 51% had been treated longer than 48 months and up to 244 months.
It is important to note that only 9.9% (n=50) of the HIV-positive patients under cART regimen, did not show any NICMs during the medical assessments. Table 1 shows the frequency of the different NICMs reported in those patients.
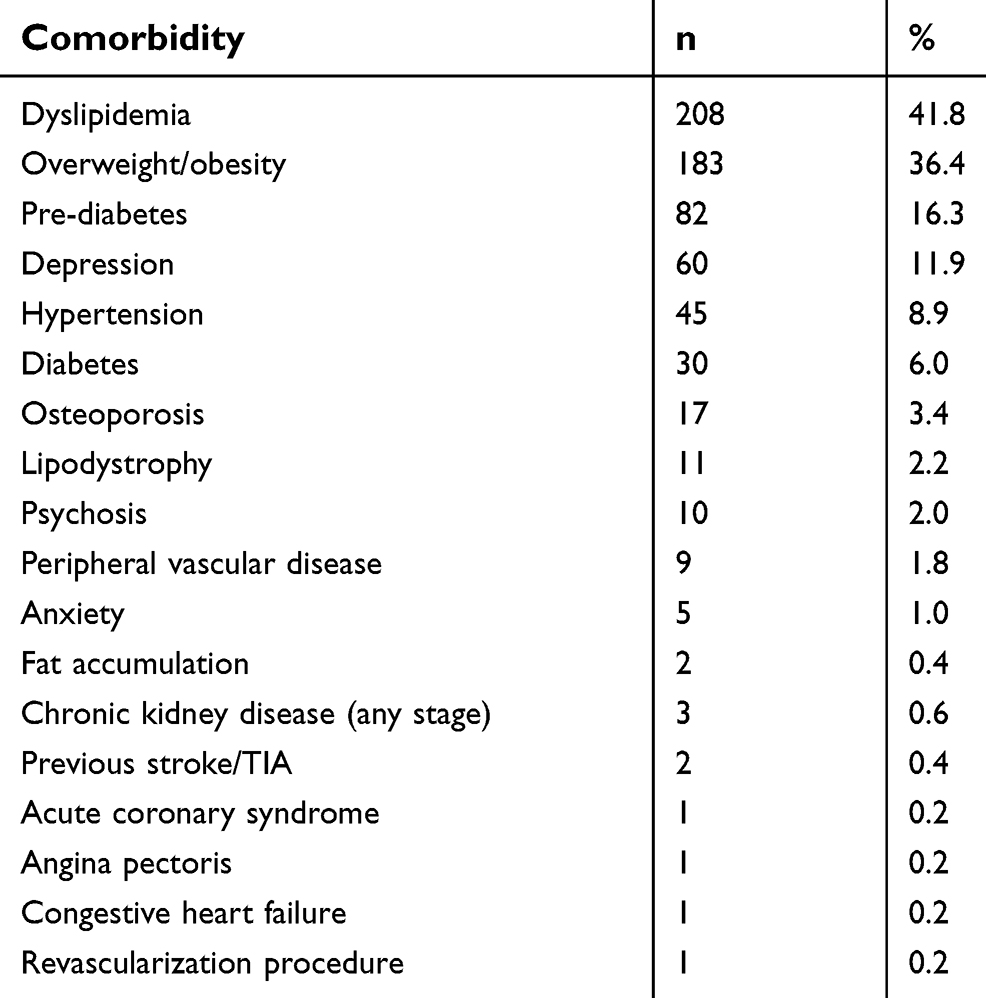 | Table 1 Noninfectious comorbidities (NICMs) among people living with HIV and under combined antiretroviral therapy in Ecuador |
About 8.5% (n=43) of the HIV patients under cART regimen were active smokers or reported a history of smoking, but nearly double (16.7%; n=84) had a history of drug/alcohol abuse. Although the main objective of this study was NICMs, it is important to report the medical diagnosis of tuberculosis (8.5%), chronic hepatitis C (4%), syphilis (4%), genital herpes (1%), herpes zoster (<1%), HPV (1%), and chronic hepatitis B (0.6%) in these patients.
Overall, 28.2% (n=142) of this population were found to have other comorbidities like gastritis (5%), hypothyroidism (3%), and low-weight/undernutrition (3%). Other diseases reported a prevalence of 2% each, like anemia, seizures, and gout. Additionally, there were a few cases of cancer, rheumatoid arthritis, asthma, hemorrhoids (1% each). Finally, with a prevalence of less than 1% each: cellulitis, dermatitis, prostate hyperplasia, and hyperuricemia were found.
Age at HIV diagnosis was significantly related with later development of prediabetes (p=0.006), hypertension (p=0.0001), dyslipidemia (p=0.0001) and overweight/obesity (p=0.03). Similarly, treatment duration was related with development of prediabetes (p=0.008) and dyslipidemia (p=0.0001). Also, there was a significant (p=0.0095) correlation between earliest age at diagnosis and later treatment initiation, while it was not related with gender (p=0.87).
Discussion
This study represents the whole population of HIV-positive patients under cART from eight main hospitals and clinics from the government and nongovernment HIV treatment centers in Ecuador. Thirty percent of the studied subjects received early treatment (ie, within a month after a confirmatory diagnosis), which increases their chances of longer survival.20
Unfortunately, although in Ecuador the government provides HIV treatment free of charge, almost 25% of the diagnosed subjects did not receive it for more than 2 years after diagnosis. This delay, usually by patient decision, does not exclude them to maintain their right for later free treatment, but together with the low rates of voluntary testing in the general population suggest that further transmission might be dramatically increased and somehow explain the growing problem in Ecuadorian population.16
Regarding noninfectious comorbid conditions in HIV subjects with cART in this cohort, as was expected, almost 90% of subjects reported one or more NICMs, therefore yielding a higher prevalence than the general Ecuadorian population. Of course, high prevalence of NICMs in PLHIV might also relate to national guidelines, as they state that patients follow-up is trimestral16 However, when comparing the same age group in the Ecuadorian general population,21 diabetes mellitus was more than double (5.7% HIV subjects vs 2.4% general population), dyslipidemia almost doubled (40.1% vs 27.6%), yet overweight/obesity was not higher in HIV subjects when compared to the general population. The explanation for the overweight/obese subjects may be because, obesity has been recently reported as a public health concern in Ecuador, affecting approximately 60% of the population.21 Another finding was the hypertension rate in the studied group was comparable to the general population (9% each), which might be related with the high prevalence of cardiovascular diseases reported in Ecuador (24%).22 All those diseases are, in fact, typically found among people living with HIV.23–25
Renal disease although reported in a few cases (0.6%), seems to be higher than in the general population where official data is not available, but may be related to antiretroviral therapy associated renal dysfunction.26 In the same sense, it is well known that due to the renal compromise, parathyroid hormone is higher and osteoporosis develops,27 then national treatment guidelines require PLVH get a DXA yearly.16 Unfortunately, there is no national data regarding osteoporosis in the general population.
Although the focus of our study was NICMs, it is important to mention the presence of coinfections commonly affecting PLHIV at higher rates, as has been reported in other regions of the world.3–6 Mental health is a usually neglected area among health care services in Ecuador which leads to failure to diagnose physiological and psychiatric problems among the general population not to mention among PLHIV. In our study, psychiatric disorders and depression (28.1%) were higher than in the general population (0.05%, 0% and 4.6%; respectively).28
Illicit drug abuse or alcohol abuse prevalence (16.7% vs 7.1%)29 and rates of smoking (8.5% vs 3.7%), although seemingly low compared to other populations,3–6 were also found to be higher in PLHIV than in the general Ecuadorian population.30
It is important to note that PLHIV might have an optimal prognosis of not developing AIDS if treatment is provided early and in a sustained manner. Although the whole population in government and nongovernment HIV treatment services were under cART regimen, only one third of the patients started treatment less than 1 month after diagnosis. Lastly, from our knowledge this constitutes the first report of NICMs in a representative population of Ecuadorian PLHIV and under cART regimen.
Conclusion
Prevalence of NICMs among subjects under cART was greater than that reported among the Ecuadorian general population, therefore urging specific public health actions to raise awareness and prevent NICMs among PLHIV in Ecuador.
Acknowledgments
This research was partially founded by an unrestricted grant from Merck Sharp & Dohme, Ecuador and a School of Medicine Research Grant from Universidad San Francisco de Quito.
Author Contributions
All authors contributed toward data analysis, drafting and revising the paper, gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0
2. Mills EJ, Bakanda C, Birungi J, et al. Life expectancy of persons receiving combination antiretroviral therapy in low-income countries: a cohort analysis from Uganda. Ann Intern Med. 2011;155:209–216. doi:10.7326/0003-4819-155-4-201108160-00358
3. Peters B, Post F, Wierzbicki AS, et al. Screening for chronic comorbid diseases in people with HIV: the need for a strategic approach. HIV Med. 2013;14(Suppl 1):1–11. doi:10.1111/j.1468-1293.2012.01055.x
4. Balderson B, Grothaus L, Harrison R, McCoy K, Mahoney C, Catz S. Chronic illness burden and quality of life in an aging HIV population. AIDS Care. 2013;25(4):451–458. doi:10.1080/09540121.2012.712669
5. Foster R, Morris S, Ryder N, Wray L, McNulty A. Screening for HIV-infected patients for non-AIDS-related morbidity: an evidence-based model of practice. Sex Health. 2011;8:30–42. doi:10.1071/SH10021
6. Vance D, Mugavero M, Willing J, Raper J, Saag M. Aging with HIV: a cross-sectional study of comorbidity prevalence and clinical characteristics across decades of life. J Assoc Nurses AIDS Care. 2011;22(1):17–25. doi:10.1016/j.jana.2010.04.002
7. Valcour V, Shikuma C, Shiramizu B, et al. Higher frequency of dementia in older HIV-1 individuals: the Hawaii aging with HIV-1 cohort. Neurology. 2004;63:822–827.
8. Phillips AN, Lee CA, Elford J, et al. More rapid progression to AIDS in older HIV-infected people: the role of CD4+ T-cell counts. J Acquir Immune Defic Syndr. 1991;4:970–975.
9. Egger M, Chene G, Phillips AN, et al. Prognosis of HIV-1 infected patient starting highly active antiretroviral therapy: a collaborative analysis of prospective studies. Lancet. 2002;360:119–129.
10. Deeks S, Phillips A. HIV infection, antiretroviral treatment, ageing, and non-AIDS related morbidity. BMJ. 2009;338:a3172. doi:10.1136/bmj.b902
11. Blanco JR, Caro AM, Perez-Cachafeiro S, et al. HIV infection and aging. AIDS Rev. 2010;12:218–230.
12. Rodriguez-Penney A, Ludicello J, Riggs P, et al. Co-morbidities in persons infected with HIV: increased burden with older age and negative effects on health-related quality of life. AIDS Patient Care STDS. 2013;27(1):5–16. doi:10.1089/apc.2012.0329
13. De Boni R, Veloso VG, Grinsztejn B. Epidemiology of HIV in Latin America and the Caribbean. Curr Opin HIV AIDS. 2014;9:192–198. doi:10.1097/COH.0000000000000031
14. Beyrer C, Baral SD, van Griensven F, et al. Global epidemiology of HIV infection in men who have sex with men. Lancet. 2012;380:367–377. doi:10.1016/S0140-6736(12)60821-6
15. The Joint United Nations Programme on HIV/AIDS. Available from:
16.
17. Montano SM, Sanchez JL, Laguna-Torres A, et al. Prevalences, genotypes, and risk factors for HIV transmission in South America. J Acquir Immune Defic Syndr. 2005;40:57–64.
18. Hernandez I, Reina-Ortiz M, Johnson A, et al. Risk factors associated with HIV among men who have sex with men (MSM) in Ecuador. Am J Mens Health. 2017;11(5):1331–1341. doi:10.1177/1557988316646757
19. Hernandez I, Reina-Ortiz M, Adegoke K, et al. Risk factors for HIV and STI among female 1 sex workers in a high HIV prevalent region of Ecuador. Cogent Med. 2019. doi:10.1080/2331205X.2019.1565292
20.
21. Freire WB, Ramírez-Luzuriaga MJ, Belmont P, et al. Tomo I: Encuesta Nacional de Salud y Nutrición de la población ecuatoriana de cero a 59 años. ENSANUT-ECU 2012. Quito: Ministerio de Salud Pública/Instituto Nacional de Estadísticas y Censos; 2014.
22.
23. Adelzon P, Falcão M, Pacheco A. Metabolic syndrome in HIV-infected individuals: underlying mechanisms and epidemiological aspects. AIDS Res Ther. 2013;10:21.
24. Triant V. Cardiovascular disease and HIV infection. Curr HIV/AIDS Rep. 2013;10:199–206. doi:10.1007/s11904-013-0168-6
25. Currier SJ. Update on cardiovascular complications in HIV infection. Top HIV Med. 2009;17(3):98–103.
26. Crabtree-Ramírez B, Del Río C, Grinsztejn B, Sierra-Madero J. HIV and Noncommunicable Diseases (NCDs) in Latin America: a call for an integrated and comprehensive response. J Acquir Immune Defic Syndr. 2014;67:S96–S98. doi:10.1097/QAI.0000000000000261
27. Mallon PW. Aging with HIV: osteoporosis and fractures. Curr Opin HIV AIDS. 2014;9:428–435. doi:10.1097/COH.0000000000000080
28.
29.
30.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.