Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Increased Frequency of Severe Hypoglycemia with the Modified-Release Gliclazide Compared to Glimepiride in Diabetic Older Adults; Propensity Score-Adjusted Analysis
Authors Fouad Algendy A ![]() , Illigens B, Alyazeedi A
, Illigens B, Alyazeedi A
Received 26 September 2021
Accepted for publication 12 November 2021
Published 19 May 2022 Volume 2022:15 Pages 1563—1575
DOI https://doi.org/10.2147/DMSO.S339331
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ming-Hui Zou
Ahmed Fouad Algendy,1 Ben Illigens,2 Ameena Alyazeedi3
1Clinical Pharmacy, Geriatric Department, Rumailah Hospital, Hamad Medical Corporation, Doha, Qatar; 2Dresden International University, Division of Health Care Sciences, Center for Clinical Research and Management Education, Dresden, Germany; 3Pharmacy Department, Rumailah Hospital, Hamad Medical Corporation, Doha, Qatar
Correspondence: Ahmed Fouad Algendy, Pharmacy Department, Rumailah Hospital, Hamad Medical Corporation, PO 3050, Doha, Qatar, Tel +0097470094424, Fax +0097444397600, Email [email protected]
Objective: The main aim is to compare the risk of severe hypoglycemia associated with the modified-release (MR) gliclazide against glimepiride in diabetic older adults.
Methods: All older adult diabetic patients who attended the emergency department (ED) between the 1st of Aug. 2017 and the end of Mar 2020 on gliclazide MR or glimepiride are included in two cohorts. We compared baseline differences between cohorts in demographics, lab results, diabetes complications, comorbidities, and drugs using the chi-squared test for categorical variables and unpaired t-test for continuous variables. All the baseline variables are used in a logistic regression to produce the propensity scores for receiving gliclazide MR. The primary outcome was Severe Hypoglycemia requiring Emergency Admission (SHEA). We used documented hypoglycemia, falls, fractures, Cardiovascular ED Admission (CVEA), and recurrent ED admissions as secondary outcomes. We used a univariate logistic regression followed by a propensity score-adjusted logistic regression to identify the adjusted odds ratio. We did a subgroup analysis for low and moderate-high doses users.
Results: We included 2320 patients, 1786 were on gliclazide MR while 534 were on glimepiride. The risk of SHEA (Adjusted Odds Ratio AOR 6.74, p=0.002), falls (AOR 1.43, p=0.003), fractures (AOR 1.43, p=0.01), CVEA (AOR 1.66, p< 0.001), recurrent ED admission (AOR 1.39, p=0.002) were significantly higher. At the same time, documented hypoglycemia was insignificantly higher (AOR 1.17, p= 0.444) with gliclazide MR compared to glimepiride. The low doses of both treatments did not show any SHEA cases, while the results with higher doses showed the same pattern of increased risk with gliclazide MR as the principle analysis.
Conclusion: Using gliclazide MR for older patients may not be a relatively safer alternative to avoid severe hypoglycemia and its possible consequences compared to glimepiride. It may be added to glimepiride in the Beers list of medications to be avoided in older adults.
Keywords: sulfonylurea, diabetes, cardiovascular, falls, fractures
Introduction
Background
Impact of Hypoglycemia in Older Adults
According to the International Diabetes Federation, 14.1% of the adult population in Qatar had diabetes, representing more than 250 thousand cases in 2017.1 The prevalence of diabetes increases with age, reaching 26.8% among those who are aged 65 years or older compared with 17.5% for those who are 45–64 years old, in the United States.2 Hypoglycemia is one of the biggest challenges in older adults’ diabetes management. There was a 60% increase in hypoglycemia-related deaths between 2000 and 2010 and stable rate trends till 2014 in 109 countries.3 A study found that about 10 thousand hospitalizations and ED visits for hypoglycemia attributed to intensive diabetes control in clinically complicated patients in 2 years in the U.S.4
In older adults, the early symptoms of hypoglycemia can be undetectable due to the impaired sympathetic response and unrecognized cognitive deficits. As a result, they may develop sudden severe hypoglycemia without alarming signs. Hypoglycemia causes QTc prolongation, increases proinflammatory markers, platelet activation, oxidative stress, and decreases endothelial function and myocardial blood flow.5 It can create excitotoxic insults and neuron cell death in the brain in severe and prolonged cases, leading to significant cognitive and physical disabilities and even cerebrovascular events and death.6
Causes of Hypoglycemia in Older Adults
As patients with diabetes get old, their diabetes management is significantly affected by age-related pathophysiological and socio-economic changes. β-cell sensitivity to incretin hormones may decrease, insulin resistance gets higher, its secretion and clearance may decline while glucose tolerance progressively declines.7 Also, decreased physical activity, increased comorbidities, polypharmacy, the longer course of diabetes, and changing pharmacokinetics and pharmacodynamics of diabetes medications increase the possibility of improper diabetes management with advancing age. In addition, older diabetic patients may have a higher risk of hypoglycemia due to weight loss, changing eating habits, decreased independence with difficulty following healthcare plans, and deteriorated renal functions. In addition to age-related changes, factors highly associated with hypoglycemia included gender, overtreated diabetes, using insulin, insulin secretagogues as sulphonylureas, and the interacting medications.8–12
Current Recommendations to Avoid Sulfonylurea Induced Hypoglycemia in Older Adults
Avoiding hypoglycemia is one of the four diabetes management goals mentioned by the American Geriatric Society (AGS). The American Diabetes Association (ADA) standards for older adults stated that hypoglycemia should be assessed and managed by adjusting glycemic targets and pharmacologic interventions.13 The 1st generation sulfonylureas (ex. glyburide and chlorpropamide) are well-known to cause severe and prolonged hypoglycemia in diabetic older adults more than other SUs, and almost their use is deprecated in many countries. Furthermore, the European list of potentially inappropriate medications in older adults (EU7-PIM 2015) recommended avoiding glimepiride while suggesting gliclazide as a safer alternative when sulfonylureas are needed for those patients.14 In 2019, the AGS updated its Beers criteria and added glimepiride to the list of medications to be avoided in older adults due to prolonged hypoglycemia,15 while gliclazide MR is not added. These recommendations may direct some prescribers to switch patients from glimepiride to gliclazide MR or prefer the latter seeking a lower risk of hypoglycemia.
The Modified-Release Gliclazide Is It a Safer Alternative?
All sulfonylureas have a considerable risk of causing hypoglycemia. However, many physicians have to use them for older adults whose blood glucose targets are not achieved or those who do not tolerate other antidiabetic agents. Although the immediate-release form of gliclazide has some pharmacokinetic (PK) benefits that may be associated with lower hypoglycemic risk compared to other long-acting SU, the commonly used MR form may not. For gliclazide MR, the half-life range in adults is higher than glimepiride (12–20 vs 5–9 hours), while the duration of action for both is almost 24 hours.16,17 Although few articles have compared the hypoglycemic risk of gliclazide MR against rarely used SUs as glyburide,18 little information is available about the comparison to the common SUs as glimepiride, particularly in older adults. So, we decided to evaluate this risk to help physicians and diabetes guidelines writers choose safe, effective, and patient-tailored antidiabetic plans for older adults.
Objectives
This study aims primarily to compare the risk of severe hypoglycemia associated with the modified-release (MR) gliclazide against glimepiride in diabetic older adults who are admitted to emergency departments. The secondary objectives include comparing the risk of documented hypoglycemia, falls, fractures, cardiovascular admissions, and recurrent ED admissions of both treatments.
Methods
Study Design
This is a retrospective propensity score-adjusted cohort study of diabetic patients who attended our Emergency Department (ED) between the 1st of Aug. 2017 and the end of Mar 2020, who were 65 years or older and were on gliclazide MR or glimepiride at the time of admission. We used this time as an indexing point for data extraction to collect the patient information at the time of admission. The detailed baseline characteristics were collected and compared between the two cohorts and then used to produce a propensity score (PS) for each admission representing the probability of receiving gliclazide MR. We used Severe hypoglycemia requiring ED admission as a primary outcome. Documented hypoglycemia at any healthcare setting, falls, fractures, Cardiovascular ED admission (CVEA), and recurrent ED admissions were used as secondary outcomes. We excluded patients who did not receive gliclazide MR or glimepiride or those who had incomplete identifiers, as shown in Figure 1.
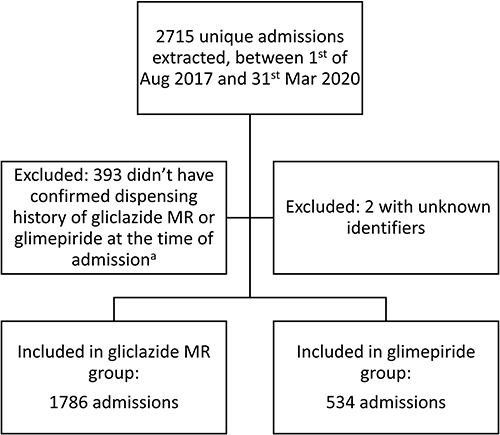 |
Figure 1 Study flow diagram. Notes: aThose patients had a gliclazide MR or glimepiride prescription but had no dispensing history. This may be because they were visitors to the country or followed up in private hospitals or other reasons. We excluded them because we doubt they received any of the study medications and had incomplete files. |
Setting
We did this study in the ED department at Hamad Medical Corporation (HMC) in Qatar. HMC is the governmental tertiary hospital providing specialized healthcare services and has many international quality accreditations.19 The targeted population was older adults with diabetes who attended ED departments and were on gliclazide MR or glimepiride.
Statistical Methods
We divided the included patients into two arms according to receiving gliclazide MR or glimepiride. We compared the baseline characteristics of both study arms using the chi-square test for categorical variables and an unpaired t-test for continuous variables.
Principle Analysis
Due to the expected large number of confounding variables and the small number of observations in some essential variables, we preferred using propensity scores for confounders’ adjustment as a continuous probability scale from 0 to 1 to manage the confounding effect and keep the study power at the same time. Using a multivariate probit regression model, we included all the confounders listed in Table 1 in calculating the PSs. Continuous variables as age, Body Mass Index (BMI), glycated hemoglobin (HbA1c), and kidney function were included in the PS model without categorization. The PSs are described in Appendix 1.
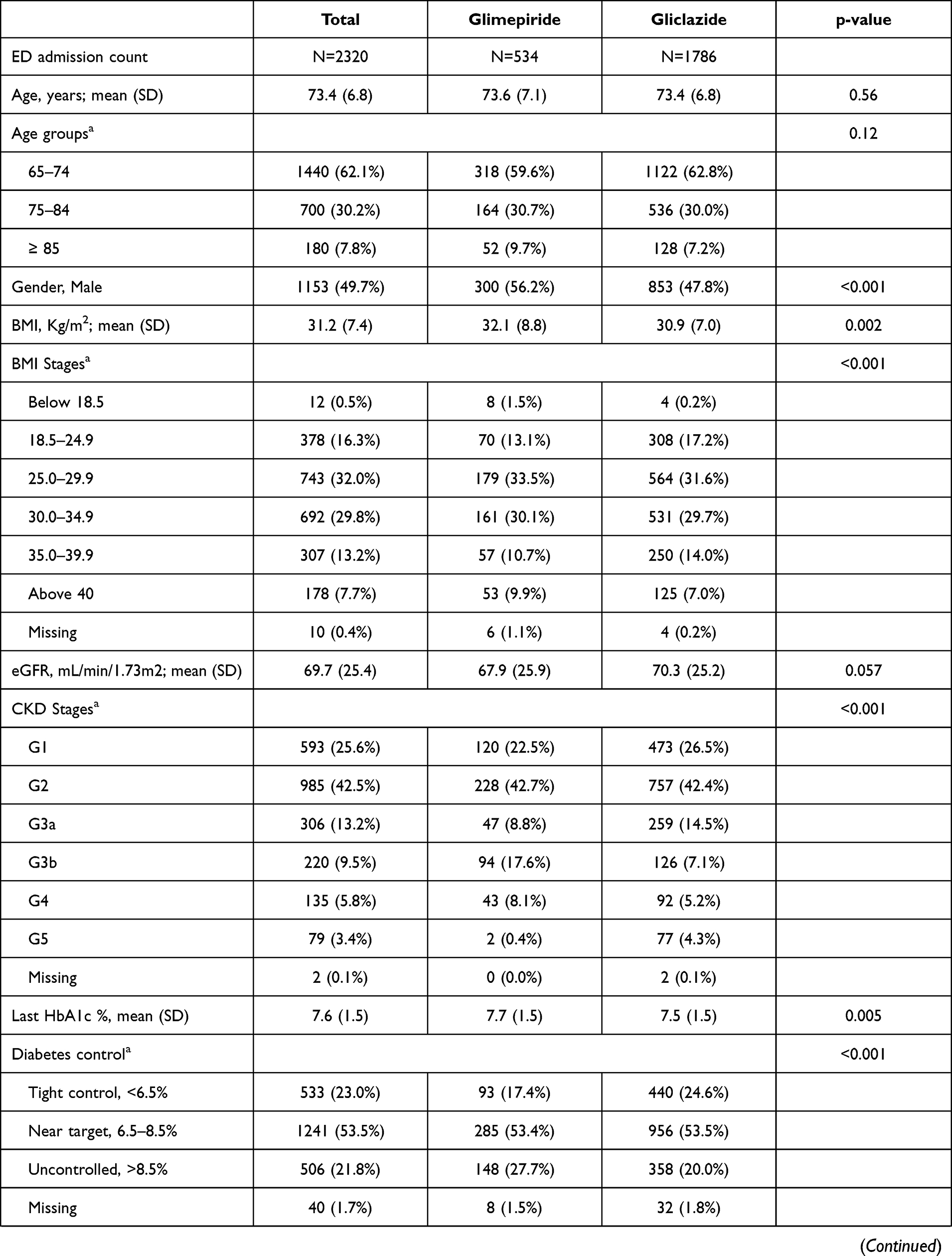 | 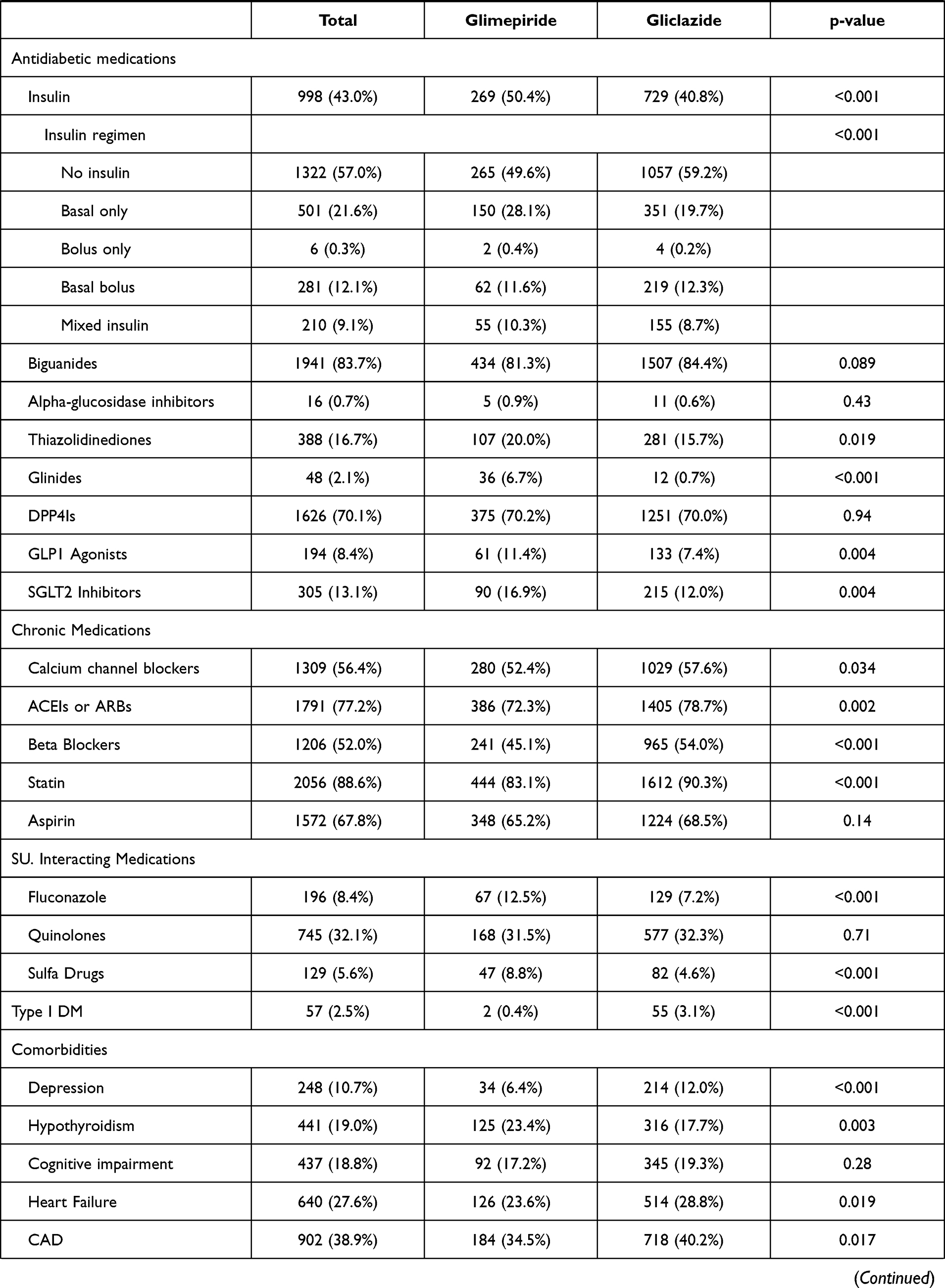 |  |
Table 1 Baseline Characteristics of the Study Groups |
All primary and secondary outcomes are binary. We included each of them in a univariate logistic regression to evaluate the crude OR, followed by propensity score-adjusted logistic regression using PSs as a single confounder to obtain the adjusted odds ratios of receiving gliclazide MR considering glimepiride users as a baseline. We did a subgroup analysis to investigate the primary and secondary measures between the two drugs at low and moderate-high dosing.
Sensitivity Analysis
We did a Multiple Imputation (MI) for missing data that utilized all the available patient information to predict the missing values using the Gaussian normal regression imputation method. We reproduced the PSs and repeated the PS-adjusted regressions for the principle and the subgroup analyses using the complete dataset after MI.
We used an alpha level of 0.05 with a two-tailed test as a cut-off value for significance in all the statistical tests. We used STATA® 16 for all statistical work.
Variables
The primary outcome is SHEA, defined as hypoglycemia diagnosed by the ED healthcare professionals or blood glucose of 3.9 or less at the ED admission time, consistent with the ADA and The Endocrine Society definition of SH.20 Falls and fractures are defined as any documented diagnosis of each before or at the admission time. The combined CVEA is any ED admission due to heart failure, acute coronary syndrome, or arrhythmia, while the recurrent ED admission is being admitted two or more times while using any of the study treatments through the study duration.
The main exposure is gliclazide MR vs glimepiride as a binary treatment variable. Other antidiabetic drugs were included in the PS model as confounders. This included insulin, biguanide (metformin), glinide (repaglinide), Glucagon-Like Peptide 1 (GLP1) agonists (exenatide, liraglutide, dulaglutide), DiPeptidyl Peptidase 4 Inhibitors (DPP4Is) (sitagliptin, vildagliptin), alpha-glucosidase inhibitor (acarbose), Sodium-GLucose coTransporter 2 Inhibitors (SGLT2Is) (dapagliflozin, empagliflozin, canagliflozin), and thiazolidinedione (TZD) (pioglitazone). In addition, we used a wide range of baseline patient characteristics to control for the confounding effect of demographics, last lab measurements before admission, comorbidities, diabetes complications, chronic medications, and commonly interacting medications (quinolones, sulfa drugs, and fluconazole), all listed in Table 1. For the subgroup analysis, gliclazide MR and glimepiride doses are considered low only if below 60 mg or 2 mg, respectively. Otherwise, they were considered mod-high.
Data Source and Management
The hospital professionals are trained and monitored for the quality of their clinical documentation. The Electronic Health Record (EHR) is Cerner® software that allows healthcare professionals to document the patient’s diagnosis or problem in SNOMED CT® terminology or as a free text. Both options were captured through the PowerInsight®, an enterprise-level data warehouse that updates on a nightly basis from the live EHR. The extracted data was validated by two researchers who reviewed a random sample of 20% of the collected data against patients’ profiles. Data were de-identified and then encrypted to ensure patient confidentiality. The encrypted data were handled, analyzed, and stored in special secured devices and servers.
Sample Size and Power Analysis
We used convenience sampling and included all the eligible patients who attended the ED departments in our hospitals through the 32 months before starting the COVID19 pandemic in our country at the end of Mar 2020. We had a sample of 2320 patients. Considering the prevalence of 1.2% SH in patients with SU and a 1:3 allocation ratio,21 the study is 80% powered to detect a 0.48 difference in odds ratios. We did the power analysis using the Chi-squared test comparing two independent proportions.
Results
Participants
The number of included older adults ED admissions was 2320, from which 1768 were on gliclazide MR and 534 were on glimepiride, while 393 were excluded due to the absence of any confirmed dispensing history of the two study interventions and two patients due to unknown identifiers, Figure 1.
Sample Characteristics
In the total sample, the means and the standard deviations (SD) for age in years, BMI in kg/m2, last HbA1c%, and last eGFR in mL/min/1.73m2 were 73.4 (6.8), 31.2 (7.4), 7.6 (1.5), and 69.7 (25.4), respectively. Males consisted 49.7% of the sample.
There were no significant differences in age, renal function, cognitive impairment, retinopathy, and diabetic foot, as well as the use of biguanide, alpha-glucosidase inhibitors, DPP4Is, aspirin, or quinolones. However, the gliclazide MR group had less male gender (47.8 vs 56.2%, p<0.001), 0.2% (p=0.005) lower HbA1c, 1.2 kg/m2 lower BMI, and less users of insulin (40.8 vs 50.4%, p<0.001), TZD (15.7 vs 20.0%, p=0.019), glinides (0.7 vs 6.7%, p<0.001), GLP1 agonists (7.4 vs 11.4%, p=0.004), SGLT2Is (12.0 vs 16.9%, p=0.004), fluconazole (7.2 vs 12.5%, p<0.001), and sulfa drugs (4.6 vs 8.8%, p<0.001).
The gliclazide MR group had more users of calcium channel blockers (57.6 vs 52.4%, p=0.034), Angiotensin-Converting Enzyme Inhibitors or Angiotensin II Receptor Blockers (78.7 vs 72.3%, p=0.002), Beta Blockers (54.0 vs 45.1%, p<0.001), and statin (90.3 vs 83.1%, p<0.001) compared to the glimepiride group. Besides, gliclazide MR group had more type I DM (3.1 vs 0.4%, p<0.001), depression (12.0 vs 6.4%, p<0.001), heart failure (28.8 vs 23.6%, p=0.019), CAD (40.2 vs 34.5%, p=0.017), neuropathy (40.0 vs 28.3%, p<0.001), and PAD (23.0 vs 20.2%, p=0.016), while it had less hypothyroidism (17.7% vs 23.4%, p=0.003) compared to the glimepiride group. The differences between the two study interventions are listed in Table 1.
Principle Analysis
In the univariate logistic regression model (N=2320), gliclazide MR was associated with a significant increase in SHEA (OR 5.62, p=0.004), falls (OR 1.45, p=0.001), fractures (OR 1.55, p=0.001), CVEA (OR 1.65, p<0.001), and recurrent ED admissions (OR 1.53, p<0.001). In contrast, the increase in any documented hypoglycemia was insignificant (OR 1.25, p=0.054) compared to glimepiride.
In the PS adjusted analysis, the involved sample was 2270 patients. Gliclazide MR continued to be associated with a significant increase in SHEA (Adjusted Odds Ratio AOR 6.74, p=0.002), falls (AOR 1.43, p=0.003), fractures (AOR 1.43, p=0.01), CVEA (AOR 1.66, p<0.001), and recurrent ED admissions (AOR 1.39, p=0.002). In contrast, the increase in any documented hypoglycemia was insignificant (AOR 1.17, p=0.209) compared to glimepiride, Table 2.
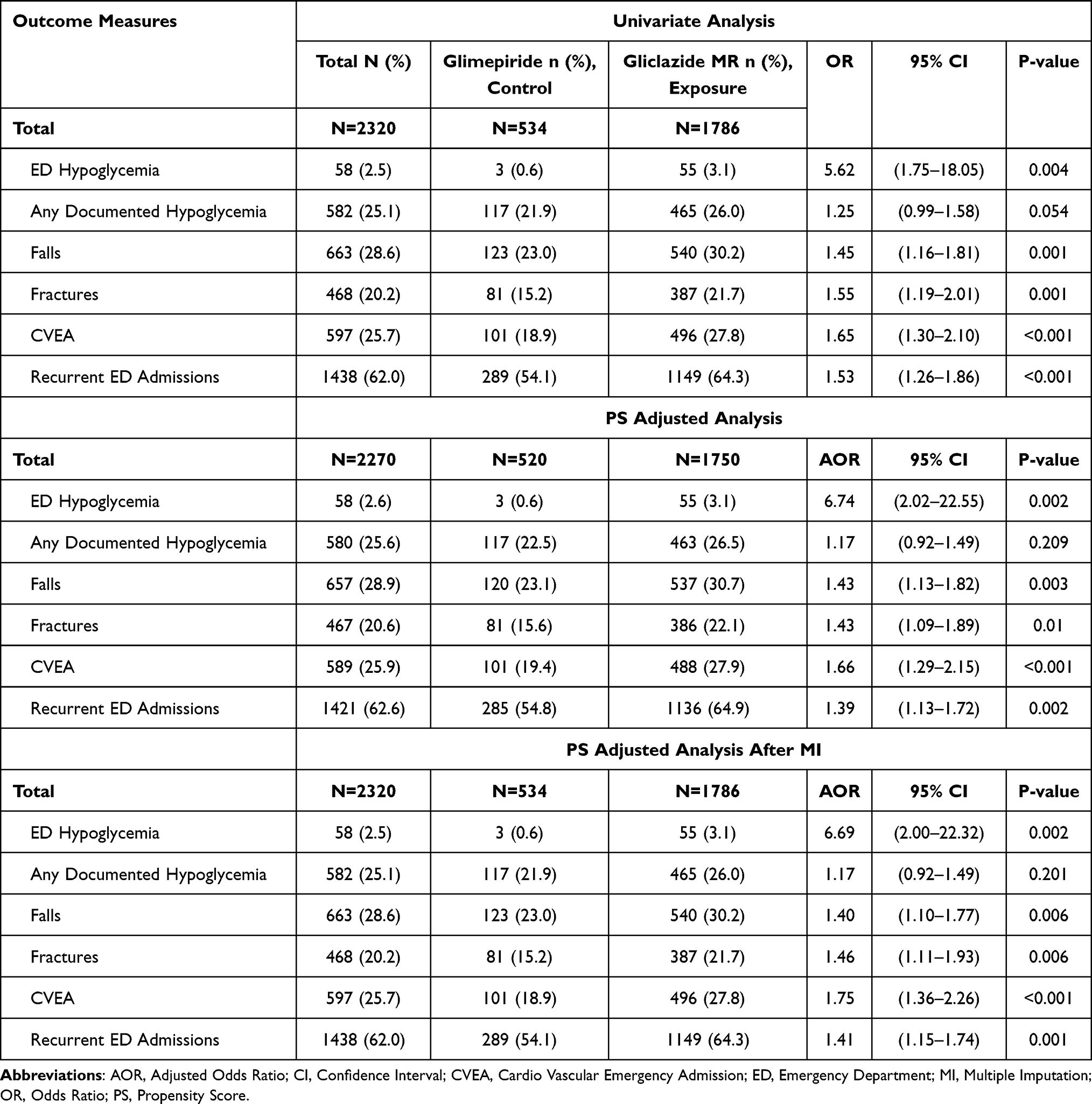 |
Table 2 Univariate and Propensity Score-Adjusted Analysis Results |
Subgroup Analysis
The subgroup analysis of patients on low doses (n=189) reveals no cases of SHEA with both treatments. There were no documented hypoglycemia and falls with glimepiride, while we found 30.7% and 32.3% with gliclazide MR, respectively. So we could not do the regression model for those outcomes. In contrast to the principle analysis, there were no significant differences between both treatments in fractures, CVEA, and recurrent ED admissions, in the univariate and the PS-adjusted model, Table 3.
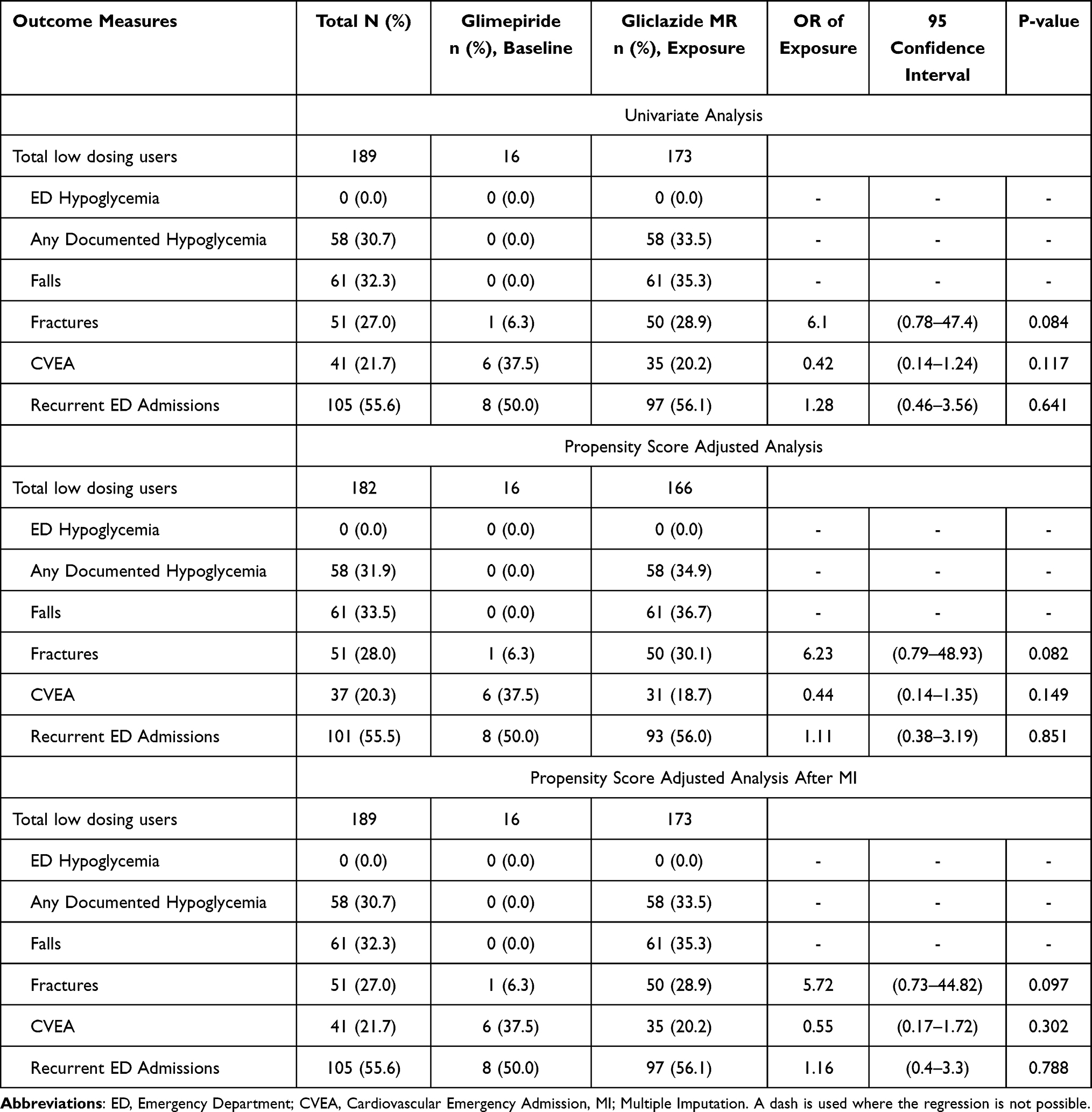 |
Table 3 Odds Ratio of Gliclazide MR Using Glimepiride as a Baseline in the Study Measures in Patients Using Low Doses |
While similar to the principle analysis, the subgroup analysis of patients on mod-high doses (n=2131) reveals the same pattern of significantly increased risk with gliclazide MR in all the study outcomes and insignificant difference in documented hypoglycemia in the univariate and the PS-adjusted model, Table 4.
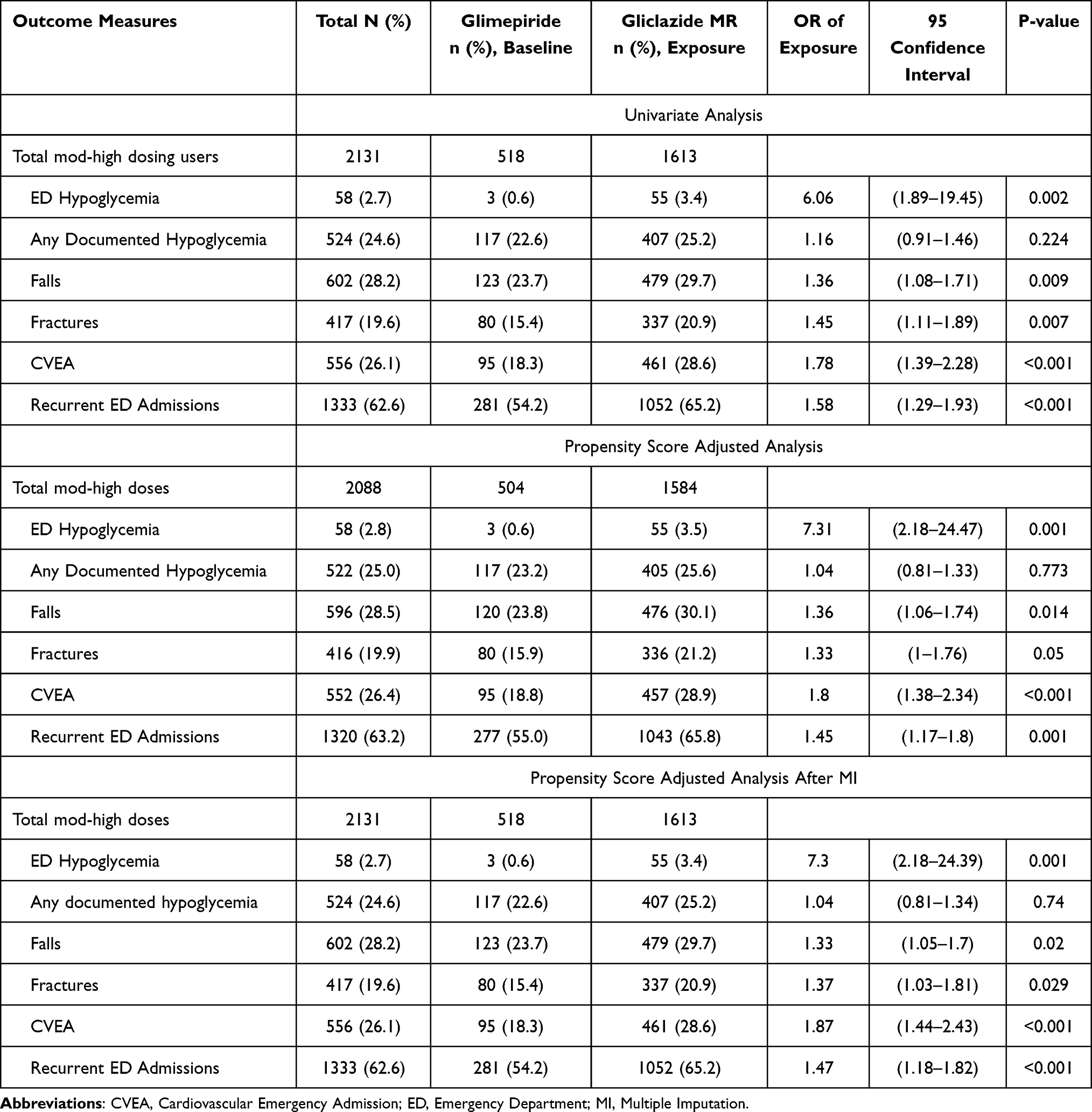 |
Table 4 Odds Ratio of Gliclazide MR Using Glimepiride as a Baseline in the Study Measures in Patients Using Mod-High Doses |
Sensitivity Analysis
The missing data was only 2.2% in BMI, serum creatinine, and HBA1c variables. However, we repeated the principle and the subgroup analysis after MI. None of the significant outcome results became insignificant or vice versa, and there were no considerable differences in the AORs, as shown in the last sections of Tables 2–4.
Discussion
This study showed an increased frequency of severe hypoglycemia associated with the use of gliclazide MR compared to glimepiride in older adults admitted to ED departments nationwide. Regardless of the overall differences between groups, gliclazide MR was associated with an increased risk of SHEA, in addition to falls, fractures, CVEA, and recurrent ED admissions compared to glimepiride. Moreover, there was no significant difference between both treatments in the risk of documented hypoglycemia. The results of the univariate analysis remained consistent in the PS adjusted analysis and the sensitivity analysis. The increased risk associated with gliclazide MR in older adults comes mainly from moderate-high doses, and it could be due to the modified PK properties that prolong its half-life and duration of action. Another reason could be the inflexibility of the dosing regimen, where prescribers have to increase the dose by at least 30 mg with each titration step, particularly in older people who are more sensitive to higher doses of hyperglycemic medications. Although the low doses of both medications showed no cases of SHEA, around one-third of patients on low-dose gliclazide MR had documented hypoglycemia and falls. In contrast, those on low-dose glimepiride showed zero cases, either due to the relative safety of the low-dose glimepiride or less likely due to the underpowered subgroup analysis.
Little studies have compared the safety of the modified-release form of gliclazide to glimepiride in older adults.22 In a meta-analysis published 2015, hypoglycemia was lower with gliclazide compared to other sulfonylureas (RR 0.47, 95% CI 0.27 to 0.79, P = 0.004, I2 = 0%).23 However, there was no specification of the gliclazide dosage form, and the comparator group was a mixture of glyburide and glimepiride users. Besides, there was no subgroup analysis of older adult results. In the GUIDE double-blind study published in 2004, comparing gliclazide MR to glimepiride, the investigators included 842 patients in the safety analysis, 294 out of them were more than 65 years, 139 on gliclazide MR and 155 on glimepiride.24 In the total population, hypoglycemia (blood glucose level < 3 mmol/L) was significantly lower with gliclazide MR (3.7% vs 8.9%, p≤ 0.02), however in the older adults subgroups, the difference was insignificant. In a population-based matched retrospective cohort study of 8748 patients on monotherapy, glyburide was associated with a higher risk for hypoglycemia than gliclazide MR (OR 8.63, 95% CI 4.15 to 17.93, p<0.0001).18 The mean age was 75.7 years. However, they did not include glimepiride in the comparison.
The evidence of any preferential impact of a particular new SU drug against the others is still conflicting. In a Cochrane systematic review of 72 RCTs, the investigators stated insufficient evidence to support the mortality or the cardiovascular benefits of using second-generation SU. (including gliclazide IR) against first-generation or using third-generation SU (including gliclazide MR and glimepiride) against other antidiabetics.25 While in concordance with our results, an RCT of 180 patients stated that glimepiride with metformin was superior to gliclazide plus metformin in alleviating the cardiovascular risk factors.26 However, this study used gliclazide in its immediate-release form. In a retrospective cohort study of 195,235 patients with mean age (SD) 58.9 (11.2), monotherapy with gliclazide was associated with increased risk of all-cause mortality and similar risk of acute myocardial infarction and stroke compared to glimepiride monotherapy. While in patients who were 70 years or older, the increase in the adjusted hazard ratio of gliclazide compared to glimepiride for acute myocardial infarction was not significant (HR 1.24, 95% CI 0.63 to 2.42).27
Choosing an antidiabetic agent is a multifactor process that should consider patient preferences, comorbidities, and other medical and socio-economic characteristics. Gliclazide MR was the most prescribed SU for older adults after claims of hypoglycemic and CV safety, particularly after adding glimepiride to the 2019 list of Beers criteria for medications to be avoided in older adults. However, gliclazide MR did not show any of these benefits for older adults compared to glimepiride. Although the MR form of gliclazide provides a more convenient once-daily dosage than the IR form, our study introduces more information about this modification’s impact on the prolonged hypoglycemic effect in older adults, particularly those with multiple comorbidities.
Strengths and Limitations
Up to our knowledge, this is one of the first studies that is enough powered to compare the hypoglycemic and cardiovascular risks of the modified release form of gliclazide to glimepiride in the older adult diabetic population using a propensity score-adjusted model. Our study results are adjusted to most of the significant confounders for both risk types. While, the limitations include unmeasured confounders as alcohol use, diet style, and the regular source of bias in similar retrospective studies, which is the documentation accuracy. However, we do not expect these limitations to significantly change our result as they are expected to be independent of the exposure variable and almost randomly distributed in both groups. Also, HMC professionals are trained and watched regularly for the quality of documentation. Besides, the documentation of hypoglycemia may be neglected in general practice, but it is expected to have the highest priority in ED departments. Furthermore, the clinical notes of a 20% random sample of patients without any hypoglycemia were screened thoroughly for documented or SH, and it was 100% free of data collection errors.
This study included only diabetic patients over 65 years who were admitted to ED departments with higher rates of comorbidities than the general population of older adults. The results can be generalized to older diabetic adults with multiple comorbidities and with caution to healthier populations. We know that PS adjusted regression balanced only the overall effect of a set of confounders rather than balancing each variable separately, so we cannot conclude an independent cause-effect relationship of the measured outcomes with the exposure. The increased risk of CVEA, recurrent ED admissions, falls, and fractures with gliclazide MR could be explained by the increased hypoglycemic risk or the frequent prescribing to patients with cardiovascular history due to the previous claims of more cardiac safety compared to other SUs.
Conclusion
In older adults, gliclazide MR was associated with a higher risk of severe hypoglycemia requiring ED admission, falls, fractures, cardiovascular ED admissions, recurrent ED admissions, and a similar risk of documented hypoglycemia compared to glimepiride. Initiation of or switching to gliclazide MR instead of glimepiride for the sake of a lower risk of hypoglycemia or cardiovascular events may not be a good choice. When physicians must initiate SU, limiting doses to 30 mg gliclazide MR or 1 mg glimepiride may alleviate the risk of severe hypoglycemia for older adults, particularly those with multiple comorbidities. Gliclazide MR, particularly moderate-high doses, may be added to glimepiride in the Beers list of medications to be avoided in older adults. Furthermore, we recommend undertaking a well-designed clinical trial to evaluate the study findings.
Ethics
We conducted this study in full conformance with the Declaration of Helsinki principles, Good Clinical Practice (GCP), within the Qatari Ministry of Public Health (MoPH) laws and regulations, and in compliance with the Hamad Medical Corporation regulatory standards as the study site. The Medical Research Center (MRC) of Hamad Medical Corporation in Qatar approved this study. We kept all data anonymous, stored encrypted data in secured computers, and transferred only within the HMC secured servers to protect patients’ confidentiality during and after the study.
Acknowledgment
We gratefully thank Dr. Hanadi Al-hamad, the head of the geriatric department, for her support. Also, we thank our colleagues Mr. Ahmed Karawia who took part in data extraction and preparation, and Ms. Mona Khalid and Mr. Justin Kurian, who took part in the manual data collection and validation. This study is the master thesis of the primary investigator and was done through the Master Program of Clinical Research (MPCR) at Dresden International University, Dresden, Germany. The Qatar National Library provided the Open Access funding.
Disclosure
The authors report no conflict of interest in this work.
References
1. International Diabetes Federation. IDF diabetes atlas. Brussels, Belgium; 2019. Available from: https://www.diabetesatlas.org.
2. Centers for Disease Control and Prevention. National diabetes statistics report. Atlanta, GA: Centers for Disease Control and Prevention, US Dept of Health and Human Services; 2020. Available from. https://www.cdc.gov/diabetes/data/statistics-report/index.html.
3. Zaccardi F, Dhalwani NN, Webb DR, Davies MJ, Khunti K. Global burden of hypoglycaemia-related mortality in 109 countries, from 2000 to 2014: an analysis of death certificates. Diabetologia. 2018;61(7):1592–1602. doi:10.1007/s00125-018-4626-y
4. Mahoney GK, Henk HJ, McCoy RG. Severe hypoglycemia attributable to intensive glucose-lowering therapy among US adults with diabetes: population-based modeling study, 2011–2014. Mayo Clin Proc. 2019;94(9):1731–1742. doi:10.1016/j.mayocp.2019.02.028
5. Halter JB, Musi N, McFarland Horne F, et al. diabetes and cardiovascular disease in older adults: current status and future directions. Diabetes. 2014;63(8):2578–2589. doi:10.2337/db14-0020
6. Zoungas S, Patel A, Chalmers J, et al. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410–1418. doi:10.1056/NEJMoa1003795
7. Chang AM, Halter JB. Aging and insulin secretion. Am J Physiol Endocrinol Metab. 2003;284(1):E7–E12. doi:10.1152/ajpendo.00366.2002
8. Thorpe CT, Gellad WF, Good CB, et al. Tight glycemic control and use of hypoglycemic medications in older veterans with type 2 diabetes and comorbid dementia. Diabetes Care. 2015;38(4):588–595. doi:10.2337/dc14-0599
9. Kumar JG, Abhilash KP, Saya RP, Tadipaneni N, Bose JM. A retrospective study on epidemiology of hypoglycemia in Emergency Department. Indian J Endocrinol Metab. 2017;21(1):119–124. doi:10.4103/2230-8210.195993
10. Hodge M, McArthur E, Garg AX, Tangri N, Clemens KK. Hypoglycemia incidence in older adults by estimated GFR. Am J Kidney Dis. 2017;70(1):59–68. doi:10.1053/j.ajkd.2016.11.019
11. Kim HM, Seong JM, Kim J. Risk of hospitalization for hypoglycemia among older Korean people with diabetes mellitus: interactions between treatment modalities and comorbidities. Medicine. 2016;95(42):e5016. doi:10.1097/MD.0000000000005016
12. Abad S, Moachon L, Blanche P, Bavoux F, Sicard D, Salmon-Céron D. Possible interaction between gliclazide, fluconazole, and sulfamethoxazole resulting in severe hypoglycaemia. Br J Clin Pharmacol. 2001;52(4):456–457. doi:10.1046/j.0306-5251.2001.01456.x-i2
13. American Diabetes Association. 11. older adults: standards of medical care in diabetes-2018. Diabetes Care. 2018;41(Suppl1):S119–S125. doi10.2337/dc18-S011
14. Renom-Guiteras A, Meyer G, Thurmann PA, The EU. (7)-PIM list: a list of potentially inappropriate medications for older people consented by experts from seven European countries. Eur J Clin Pharmacol. 2015;71(7):861–875. doi:10.1007/s00228-015-1860-9
15. By the 2019 American Geriatrics Society Beers Criteria® Update Expert Panel. American geriatrics society 2019 updated AGS beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi10.1111/jgs.15767
16. [product monograph]. Diamicron® MR (gliclazide modified release). Laval, Quebec, Canada: Servier Canada Inc; last revised Sep 2019. Available from https://pdf.hres.ca/dpd_pm/00053765.PDF.
17. Amaryl® (glimepiride) prescribing information. Bridgewater, NJ: Sanofi-Aventis; 2018. Available from https://products.sanofi.us/Amaryl/Amaryl.pdf.
18. Clemens KK, McArthur E, Dixon SN, Fleet JL, Hramiak I, Garg AX. The hypoglycemic risk of glyburide (glibenclamide) compared with modified-release gliclazide. Can J Diabetes. 2015;39(4):308–316. doi:10.1016/j.jcjd.2015.01.001
19. Hamad medical corporation, international accreditations. Available from https://www.hamad.qa/EN/About-Us/Our-Accreditations/Pages/default.aspx.
20. Seaquist ER, Anderson J, Childs B, et al. hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care. 2013;36(5):1384–1395. doi:10.2337/dc12-2480
21. Shorr RI, Ray WA, Daugherty JR, Griffin MR. Incidence and risk factors for serious hypoglycemia in older persons using insulin or sulfonylureas. Arch Intern Med. 1997;157(15):1681–1686. doi:10.1001/archinte.1997.00440360095010
22. Glyburide, gliclazide or glimepiride for elderly patients with type 2 diabetes: a review of the clinical effectiveness and safety – an update [internet]. Ottawa (ON): Canadian Agency for Drugs and Technologies in Health; 2015. Available from: https://www.ncbi.nlm.nih.gov/books/NBK315873.
23. Chan SP, Colagiuri S. Systematic review and meta-analysis of the efficacy and hypoglycemic safety of gliclazide versus other insulinotropic agents. Diabetes Res Clin Pract. 2015;110(1):75–81. doi:10.1016/j.diabres.2015.07.002
24. Schernthaner G, Grimaldi A, Di Mario U, et al. GUIDE study: double-blind comparison of once-daily gliclazide MR and glimepiride in type 2 diabetic patients. Eur J Clin Invest. 2004;34(8):535–542. doi:10.1111/j.1365-2362.2004.01381.x
25. Hemmingsen B, Schroll JB, Lund SS, et al. Sulphonylurea monotherapy for patients with type 2 diabetes mellitus. Cochrane Database Syst Rev. 2013;(4):CD009008. doi:10.1002/14651858.CD009008.pub2
26. Hassan MH, Abd-Allah GM. Effects of metformin plus gliclazide versus metformin plus glimepiride on cardiovascular risk factors in patients with type 2 diabetes mellitus. Pak J Pharm Sci. 2015;28(5):1723–1730.
27. Cho EH, Han K, Kim B, Lee DH. Gliclazide monotherapy increases risks of all-cause mortality and has similar risk of acute myocardial infarction and stroke with glimepiride monotherapy in Korean type 2 diabetes mellitus. Medicine. 2020;99(29):e21236. doi:10.1097/MD.0000000000021236
 © 2022 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2022 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.