")
Back to Journals » Infection and Drug Resistance » Volume 16
Incidence Rate and Associated Factors of Early Onset Sepsis Among Neonate Born at ≥35 Weeks’ Gestation in Thai Tertiary Hospital
Authors Aeimcharnbanchong K
Received 3 April 2023
Accepted for publication 21 June 2023
Published 26 June 2023 Volume 2023:16 Pages 4093—4100
DOI https://doi.org/10.2147/IDR.S415590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Kanokwan Aeimcharnbanchong
Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, Nonthaburi, Thailand
Correspondence: Kanokwan Aeimcharnbanchong, Department of Pediatrics, Panyananthaphikkhu Chonprathan Medical Center, Srinakarinwirot University, P.O. Box 222 Moo 1, Tiwanon Road, Pak Kret, Nonthaburi, 11120, Thailand, Tel +66 2 502 2345, Fax +66 2 502-2305, Email [email protected]
Purpose: This study aimed to find the incidence rate and associated factors of EOS in neonates with 35 weeks of gestational age or more at Panyananthaphikkhu Chonprathan Medical Center (PCMC) in order to develop effective prevention and treatment strategies to reduce neonatal mortality.
Methods: A cross-sectional study was done in a single-center neonatal intensive care unit at PCMC. Data were collected from October 2016 to September 2021 from all neonates with 35 weeks of gestational age or more with EOS and randomly collected from neonates with 35 weeks of gestational age or more without EOS. The associated factors of EOS were shown as an odds ratio by multivariate analysis of binary logistic regression.
Results: In this study, 595 neonates were enrolled and divided into 2 groups – EOS group (193 neonates) and non-EOS group (402 neonates). The incidence rate of EOS was 21.23/1000 live births, comprising 2 culture-positive EOS neonates (0.22/1000 live births) and 191 culture-negative EOS neonates (21/1000 live births). The common clinical manifestations in the EOS group were respiratory distress (157 neonates, 81%), temperature instability (43 neonates, 22.3%) and poor feeding (39 neonates, 20.2%). Statistically significant relationship (p-value < 0.05) was found in prolonged rupture of membrane (OR 11.7, 95% CI: 2.54– 53.88), low birth weight (OR 2.3, 95% CI: 1.25– 4.4) and normal Apgar score at 5 minutes after birth (OR 0.5, 95% CI: 0.31– 0.71).
Conclusion: Our study shows that the incidence rate of culture positive EOS in late preterm and term is very low. EOS was significantly associated with prolonged rupture of membrane and low birth weight whereas lower rate of EOS was significantly associated with normal Apgar score at 5 minutes after birth. Efforts to recognize these factors early and effectively resuscitate neonates may reduce and prevent neonatal morbidity and mortality.
Keywords: prolonged rupture of membrane, low birth weight, term infant, preterm infant
Introduction
Neonatal early onset sepsis (EOS) is an important cause of neonatal morbidity and mortality. EOS is defined as blood or cerebrospinal fluid (CSF) bacterial infection of the newborn within 72 hours after birth.1 Incident rates of EOS in many developed countries have declined after implementing maternal antenatal screening and GBS intrapartum antibiotic prophylaxis.2 However, in most developing countries, these screening and antibiotic prophylaxis are not widely implemented. Therefore, the incidence rates of EOS are varied across developing countries. The incidence rate of EOS in late preterm and term neonates in developing countries is about 0.2–0.3/1000 live births which is lower than that of very preterm and moderate preterm neonates, but there are potential risks of subsequent serious sequelae and mortality.3,4
The diagnosis of EOS remains a challenge due to unspecific clinical signs and low specificity of laboratory tests.5 Until 2019, AAP launched the clinical report of management of infants at risk for Group B Streptococcal Disease with three approaches for EOS risk assessment among infants born ≥35 weeks’ gestation: (1) Categorical risk assessment recommends full septic work up for all infants with maternal fever which could lead to unnecessary investigations and antibiotics exposure in well-appearing infants, (2) Enhance observation recommends treatment only infants who have clinical illness and performing serial physical examinations for well-appearing infants with maternal risk factors for EOS which reduces antibiotic use but some infants with proven sepsis could be missed, and (3) Neonatal Early Onset Sepsis Calculator (EOSC) recommends management following three levels of risk based on the incidence of EOS, gestational age, highest maternal antepartum temperature, duration of ROM, maternal GBS status, type of intrapartum antibiotic prophylaxis plus neonatal clinical status at birth. In particular, EOSC recommends (a) routine neonatal care, (b) obtaining a blood culture and monitoring vital signs for at least 24 hours, and (c) start treatment with empirical antibiotic therapy after obtaining a blood culture.5,6
In our view, EOSC provides a clear definition of clinical illnesses, a decrease in NICU admissions, less unnecessary investigation and antibiotic use, as well as improved mother-child bonding.7–10 In addition, Thailand still does not have any standard EOS guidelines until now. We are interested in applying EOSC to Panyananthaphikkhu Chonprathan Medical Center (PCMC)’s EOS management. However, there are no data regarding the incidence rate of EOS in late preterm and term neonates in Thailand. Therefore, the objective of this study is to find the incidence rate of EOS in late preterm and term neonates at PCMC. In addition, this study also investigates the associated factors of EOS in late preterm and term neonates at PCMC in order to develop effective treatment strategies to reduce neonatal mortality.
Materials and Methods
Study Design and Data Collection
This is a cross-sectional study with retrospective data collection. The Committee on Human Rights related to research involving subjects at PCMC, Srinakharinwirot University approved this study. We conducted the study following the Declaration of Helsinki. We did not require the patient’s informed consent as the data were anonymized. To ensure the confidentiality of the data from the participants’ records, we did not record any personal identifiers on the data collection sheet, and the data from participant records were not available to anyone except the researchers.
We included all neonates with 35 weeks of gestational age or more diagnosed with EOS in a five-year period from October 2016 to September 2021 at PCMC, which is a tertiary care hospital and excellent center for neonates in urban area. We searched ICD-10 diagnosis P36.0-P36.9 (sepsis of newborn due to bacterial infection), reviewed all medical charts and collected data of culture-positive/culture-negative EOS neonates (case group). We also searched ICD-10 diagnosis z38.0, z38.1, z38.3, z38.4, z38.6, z38.7, z38.8 (singleton or twin or multiple, born in hospital or out hospital or unspecified as to place of birth), randomly reviewed some medical charts and collected data of non-sepsis neonates (control group). Then, we obtained data from medical charts such as gestational age, birth weight, small for gestational age (SGA), sex, Apgar score, maternal age, delivery type, maternal risk factors of EOS (maternal prolonged rupture of membrane, maternal chorioamnionitis, previous infant with invasive GBS disease, late preterm between 350/7 to 366/7 weeks’ gestation with true labor pain and/or ROM regardless of rupture duration, and term with ROM ≥ 18 hours), presence of antepartum antibiotic administration, neonatal signs and symptoms of clinical illness. We also obtained neonatal laboratory results and laboratory data for all participants throughout pregnancy such as GBS bacteriuria during any trimester of the current pregnancy and maternal positive for GBS culture during current pregnancy.
Definition
EOS group includes culture-positive and culture-negative EOS neonates. Culture-positive EOS neonate is a neonate who has clinical signs and symptoms consistent with sepsis and positive blood culture in the first 72 hours of life.11,12 Culture-negative EOS neonate is a neonate who has clinical sepsis and receives antibiotics at least 5 days with negative blood culture.11,12
Non-EOS group includes neonates who do not have clinical sepsis and do not receive antibiotics or neonates who receives antibiotics less than 5 days with negative blood culture.
Small for gestational age (SGA) is defined as a birth weight of less than 10th percentile for gestational age.
Prolonged rupture of membrane is a rupture or leak of fetal membranes (amniotic sac) lasting longer than 18 hours prior to delivery.
Chorioamnionitis is an acute inflammation of the membranes and chorion of the placenta. The key clinical findings associated with clinical chorioamnionitis include fever, uterine fundal tenderness, maternal tachycardia (>100/min), fetal tachycardia (>160/min) and purulent or foul amniotic fluid.
Normal Apgar score is a score of 7 to 10 which indicates that the neonate does not need resuscitation or intervention.
Sample Size
A two population proportion formula was used to estimate the adequate sample size for the study by considering the proportion of low birth weight among the controls of 11.8% which was estimated from a previous study,13 95% confidence interval and 80% power of the study case-to-control ratio of 1:2 to detect an estimated odds ratio of 2.2. The required sample size was 570 neonates after considering a 10% non-response rate (190 cases and 380 controls).
Statistical Analysis
Statistical analyses were conducted using IBM SPSS Statistics for Windows ver. 18 (IBM Corp., Armonk, NY, USA). The Mann–Whitney U-test was used to compare differences between two independent groups when the dependent variables were either ordinal or continuous, but not normally distributed. The Chi-square test and Fisher exact were used to compare a group with a value or to compare two or more groups, using categorical data. Binary logistic regression was performed to test the association between independent variables and EOS. Both the Crude Odds Ratio (COR) and the Adjusted Odds Ratio (AOR) with a 95% confidence interval (CI) were computed to test the strength of association. Variables with p-value <0.2 during bivariate analysis were selected for multivariate analysis of binary logistic regression. Variables with p-value <0.05 in the multivariate analysis were declared significantly associated with EOS.
Results
In this study, 595 neonates were enrolled and divided into 2 groups – EOS group (193 neonates) and non-EOS group (402 neonates). The incidence rate of EOS was 21.23/1000 live births, comprising 2 culture-positive EOS neonates (0.22/1000 live births) and 191 culture-negative EOS neonates (21/1000 live births). The ratio of culture-positive EOS to culture-negative EOS is 1 to 95.5.
One culture-positive EOS neonate who was a 38 week-gestation male infant had E. coli ESBL septicemia. His mother’s risk factor was unknown GBS status. At birth, he was presented with tachypnea (respiratory rate 80/min). At 50 hours after birth, he developed feeding intolerance, temperature instability and poor perfusion. He also received meropenem for 14 days and was discharged. Another culture-positive EOS neonate who was a 39 week-gestation female had Staphylococcal hemolyticus septicemia. Her mother’s risk factor was unknown GBS status. At 36 hours after birth, she had pus and redness at umbilicus. She received vancomycin for 14 days and could be discharged.
Table 1 displays the demographic data of enrolled mothers and neonates. The gestational age less than 37 weeks was 43 (22.3%) and 39 (9.7%) among neonates with and without EOS, respectively. The low birth weight of the EOS group was 35 neonates (18.1%) compared to 25 neonates (6.2%) in the non-EOS group. Small for gestational age were 12 (6.2%) and 16 (4%) among neonates with and without EOS, respectively. There were 7 neonates (3.6%) in the EOS group and none in the non-EOS group with Apgar score at 5 minutes after birth <7.
 |
Table 1 Demographic Data of Enrolled Mothers and Neonates (n=595) |
Table 2 shows the associated factors of EOS. Chorioamnionitis, preterm premature rupture of membrane or preterm labor pain and prolonged rupture of membrane were significantly higher in the EOS group than those in the non-EOS group. The most common associated factor of EOS was preterm premature rupture of membrane or preterm labor pain observing at 31 mothers (16.1%). Almost all mothers had unknown maternal GBS status of current pregnancy. In addition, GBS bacteriuria during any trimester of the current pregnancy and previous infant with invasive GBS disease were not detected in our study.
 |
Table 2 Associated Factors of EOS (n=595) |
Table 3 displays clinical manifestations. The common clinical manifestations of the EOS group were respiratory distress (157 neonates, 81.3%), temperature instability (43 neonates, 22.3%) and poor feeding (39 neonates, 20.2%). For the EOS group, 108 neonates had symptoms at birth and 85 neonates developed symptoms later. The average duration to develop symptoms was 4.7 hours. In addition, approximately 99.5% of neonates in the EOS group were diagnosed less than 48 hours after birth.
 |
Table 3 Clinical Manifestations (n=595) |
Table 4 shows the bivariate and multivariate analysis of binary logistic regression of factors associated with EOS. The normal Apgar score at 5 minutes after birth, vaginal delivery, chorioamnionitis, PPROM/preterm labor pain, prolonged ROM, gestational age 350/7–366/7 weeks and low birth weight passed the variable screening criteria (p-value < 0.2) and were entered into the multivariate analysis of binary logistic regression. We found that neonates of mothers with prolonged rupture of membrane (OR 11.7, 95% CI: 2.54–53.88) and neonates with low birth weight (OR 2.3, 95% CI: 1.25–4.4) were significantly associated with EOS whereas neonates with normal Apgar score at 5 minutes after birth (OR 0.5, 95% CI: 0.31–0.71) were significantly associated with a lower rate of EOS under multivariate analysis of binary logistic regression (p-value < 0.05).
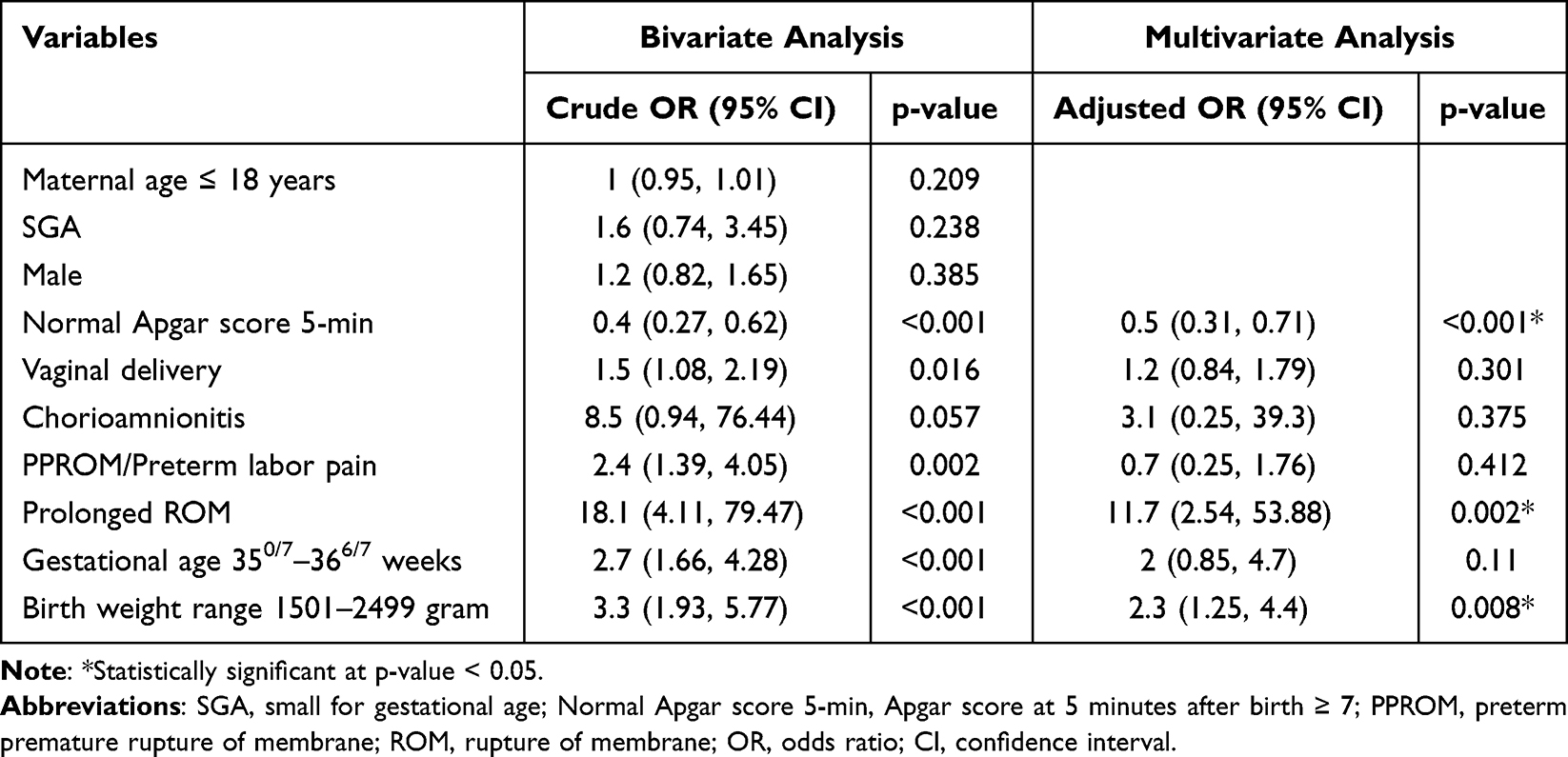 |
Table 4 Bivariate and Multivariate Analysis of Binary Logistic Regression of Factors Associated with EOS |
Discussion
Our study shows that the incidence rate of EOS in neonates with 35 weeks of gestational age or more is 21.23/1000 live births, comprising 2 culture-positive EOS neonates (0.22/1000 live births) and 191 culture-negative EOS neonates (21/1000 live births). This finding of EOS incidence proven by positive blood cultures is similar to the studies from Brazil and Italy which showed the EOS incidence of 0.2–0.3/1000 live births.3,4 However, our EOS incidence is less than the study in Sweden (0.9/1000 live births), United Kingdom (0.7/1000 live births) and USA (0.77–1.08/1000 live births).14–18 These differences can be explained by the inclusion of infants born at term or late preterm in our study, whereas other analyses described the global incidence rate of EOS without distinction between gestational ages. In particular, preterm neonates have deficient and immature immunological systems. Therefore, they are more susceptible to infection.
We find a ratio of culture-positive EOS to culture-negative EOS at about 1:95.5, which is less than many studies from Norway, Canada and Switzerland (1:6–1:16).19–21 The lower rate of culture-positive EOS to culture-negative EOS in our study might be attributed to low level of bacteremia or small volumes of blood obtained from sick neonates, intrapartum antibiotic prophylaxis and over-diagnosis of sepsis among non-infected neonates.
The common clinical manifestations of EOS in our study are respiratory distress, temperature instability and poor feeding. These features are similar to the findings in the previous studies.22–24 We also find that 99.5% of neonates in the EOS group are diagnosed within 48 hours after birth. This finding is similar to the study of Nanduri.2 Some clinical manifestations are unspecific and found in both EOS group and non-EOS group because there is a dynamic adaptation of many organ systems to extra-uterine life. Therefore, the decision to start treatment should rely on the evaluation of neonatal risk factors and development of symptoms.
Many studies found the risk factors associated with EOS in preterm and term infants were (1) intrauterine inflammation or infection of both or Triple I, (2) current GBS bacteriuria, (3) previous infant with invasive GBS disease, (4) positive maternal GBS status of current pregnancy, (5) preterm labor pain, (6) premature rupture of membranes and (7) prolonged rupture of membranes (≥18 hours).25–27 Our study finds that neonates of mothers with prolonged rupture of membrane and neonates with low birth weight were significantly associated with EOS whereas neonates with normal Apgar score at 5 minutes after birth were significantly associated with lower rate of EOS.
In our study, the significant associated factor is prolonged rupture of membrane (OR 11.7, 95% CI: 2.54–53.88). The studies conducted in Mwananyamala-Tanzania, Mashhad-Iran and Bangladesh had similar findings.28–31 Prolonged rupture of membrane increases the risk of ascending bacterial infection from genital tract, resulting in infectious morbidities, fetal inflammation and neonatal sepsis.32
Our study also finds the significant relationship between low birth weight and EOS. The odds of developing EOS among neonates who have low birth weight are 2.3 times higher as compared to neonates with normal birth weight. This finding is consistent with Shitaye’s study and Khatua’s study.33,34 This may be because neonates who have low birth weight are mostly premature. The prematurity has immature immune system which is one of the leading causes of increased susceptibility to infections.35
This study reports that the normal Apgar score at 5 minutes after birth is associated with a lower rate of EOS. Similar observation was also shown in the studies investigated in Ghana and Nigeria.36,37 The normal Apgar score at 5 minutes after birth indicates that the neonates do not need resuscitation or invasive procedure such as suctioning, endotracheal intubations and umbilical venous catheter insertion. Therefore, they have low probability of developing neonatal bacterial sepsis. In addition, poor adherence to neonatal resuscitation guidelines by medical personnel as well as non-sterile procedure and equipment can increase the risk of developing neonatal bacterial sepsis. Moreover, neonates with low Apgar score impair the immune response and are more vulnerable to infection.
The strength of our study is the 5-year study period and its ability to identify the incidence rate and associated factor of EOS in a tertiary hospital in Thailand. The result might be a useful information for applying our local incidence rate in EOSC and developing effective prevention strategies to reduce EOS. However, our study has some limitations. In particular, the definition of culture-negative EOS is no uniform consensus. Therefore, the diagnosis of culture-negative EOS is varied, depending on the judgment of the attending staffs. This may lead to overdiagnosis. Next, most maternal GBS statuses of current pregnancy in our study are unknown because GBS screening is not yet widely implemented in Thailand. The other limitation is that our study investigates only one hospital, and the results may not be generalizable to other institutions. We think it would be important for future studies to investigate more hospitals so that the results would be more generalizable and reliable. Another important area would be using culture-positive EOS, which is a gold standard of diagnosis of EOS, to diagnose EOS in order to accurately determine the incidence rate and associated factors of EOS.
Conclusion
Our study shows that the incidence rate of culture positive EOS in late preterm and term is very low and similar to the data from developed countries. EOS was significantly associated with prolonged rupture of membrane and low birth weight whereas lower rate of EOS was significantly associated with normal Apgar score at 5 minutes after birth. Efforts to recognize these factors early and effectively resuscitate neonates may reduce and prevent neonatal morbidity and mortality.
Acknowledgments
The author thanks all patients, health practitioners and director of PCMC authorized to collect research data.
Disclosure
The author reports no conflicts of interest in relation to this work and has no known competing financial interest or personal relationship that could have appeared to influence the work reported in the research.
References
1. Puopolo KM, Benitz WE, Zaoutis TE; Committee in Fetus and Newborn and Committee in Infectious Disease. Management of neonates born at ≥ 350/7 weeks’ gestation with suspected or proven early-onset bacterial sepsis. Pediatrics. 2018;142:6.
2. Nanduri SA, Petit S, Smelser C, et al. Epidemiology of invasive early-onset and late-onset group B streptococcal disease in the United States, 2006 to 2015: multistate laboratory and population-based surveillance. JAMA Pediatr. 2019;173(3):224–233. doi:10.1001/jamapediatrics.2018.4826
3. Camargo JF, Caldas JP, Marba ST. Early neonatal sepsis: prevalence, complications and outcomes in newborn with 35 weeks of gestrational age or more. Rev Paul Pediatr. 2022;40:e202383.
4. Berardi A, Fornaciari S, Rossi C, et al. Safety of physical examination alone for managing well-appearing neonates ≥ 35 weeks’ gestation at risk for early-onset sepsis. J Matern Fetal Neonatal Med. 2015;28(10):1123–1127. doi:10.3109/14767058.2014.946499
5. Deleon C, Shattuck K, Jain SK. Biomarkers of neonatal sepsis. Neoreviews. 2015;16(5):e297–e308. doi:10.1542/neo.16-5-e297
6. Mukhopadhyay S, Eichenwald EC, Puopolo KM. Neonatal early-onset sepsis evaluations among well appearing infants: projected impact of changes in CDC GBS guidelines. J Perinatol. 2013;33(3):198–205. doi:10.1038/jp.2012.96
7. Bailey LC, Forrest CB, Zhang P, Richards TM, Livshits A, DeRusso PA. Association of antibiotics in infancy with early childhood obesity. JAMA Pediatr. 2014;168(11):1063–1069. doi:10.1001/jamapediatrics.2014.1539
8. Greenwood C, Morrow AL, Lagomarcino AJ, et al. Early empiric antibiotic use in preterm infants is associated with lower bacterial diversity and higher relative abundance of Enterobacter. J Pediatr. 2014;165(1):23–29. doi:10.1016/j.jpeds.2014.01.010
9. Madan JC, Farzan SF, Hibberd PL, Karagas MR. Normal neonatal microbiome variation in relation to environmental factors, infection and allergy. Curr Opin Pediatr. 2012;24(6):753–759. doi:10.1097/MOP.0b013e32835a1ac8
10. Madan JC, Salari RC, Saxena D, et al. Gut microbial colonisation in premature neonates predicts neonatal sepsis. Arch Dis Child Fetal Neonatal Ed. 2012;97(6):F456–62. doi:10.1136/fetalneonatal-2011-301373
11. Fjalstad JW, Stensvold HJ, Bergseng H, et al. Early-onset sepsis and antibiotic exposure in term infants: a nationwide population-based study in Norway. Pediatr Infect Dis J. 2016;35:1–6. doi:10.1097/INF.0000000000000906
12. Stocker M, van Herk W, El Helou S, et al. Procalcitonin-guided decision making for duration of antibiotic therapy in neonates with suspected early-onset sepsis: a multicentre, randomized controlled trial (NeoPIns). Lancet. 2017;390:871–881. doi:10.1016/S0140-6736(17)31444-7
13. Srijunthongsiri S, Srising K, Werakul J. Associated risk factors of neonatal Sepsis in naresuan hospital. J Public Health (Bangkok). 2015;45(3):256–271.
14. Johansson Gudjónsdóttir M, Elfvin A, Hentz E, Adlerberth I, Tessin I, Trollfors B. Changes in incidence and etiology of early-onset neonatal infections 1997–2017 - a retrospective cohort study in western Sweden. BMC Pediatr. 2019;19:490. doi:10.1186/s12887-019-1866-z
15. Cailes B, Kortsalioudaki C, Buttery J, et al. Epidemiology of UK neonatal infections: the neonIN infection surveillance network. Arch Dis Child Fetal Neonatal Ed. 2018;103:F547–53. doi:10.1136/archdischild-2017-313203
16. Cohen-Wolkowiez M, Moran C, Benjamin DK, et al. Early and late onset sepsis in late preterm infants. Pediatr Infect Dis J. 2009;28:1052–1056. doi:10.1097/INF.0b013e3181acf6bd
17. Stoll BJ, Hansen NI, Sanchez PJ, et al. Early onset neonatal sepsis: the burden of group B streptococcal and E. coli disease continues. Pediatrics. 2011;127:817–826. doi:10.1542/peds.2010-2217
18. Weston EJ, Pondo T, Lewis MM, et al. The burden of invasive early-onset neonatal sepsis in the United States, 2005–2008. Pediatr Infect Dis J. 2011;30:937–941. doi:10.1097/INF.0b013e318223bad2
19. Drageset M, Fjalstad JW, Mortensen S, Klingenberg C. Management of early onset neonatal sepsis differs in the north and south of Scandinavia. Acta Paediatr. 2017;106:375–381. doi:10.1111/apa.13698
20. Hofer N, Muller W, Resch B. Neonates presenting with temperature symptoms: role in the diagnosis of early onset sepsis. Pediatr Int. 2012;54:486–490. doi:10.1111/j.1442-200X.2012.03570.x
21. Lacaze-Masmonteil T, Rosychuk RJ, Robinson JL. Value of a single C-reactive protein measurement at 18 h of age. Arch Dis Child Fetal Neonatal Ed. 2014;99:F76–9. doi:10.1136/archdischild-2013-303984
22. Saxena S, Anand NK, Saini L, Mittal SK. Bacterial infections among home delivered neonates. Clinical picture and bacteriological profile. Indian Pediatr. 1980;17:17–24.
23. Arowosegbe AO, Ojo DA, Dedeke IO, Shittu OB, Akingbade OA. Neonatal sepsis in a Nigerian tertiary hospital: clinical features, clinical outcome, aetiology and antibiotic susceptibility pattern. South Afri J Infect Dis. 2017;4:127–131. doi:10.4102/sajid.v32i4.37
24. Awaisu A, Sulaiman SAS, Ibrahim MIM, Saad A. Antimicrobials utilization and outcomes of neonatal sepsis among patients admitted to a University Teaching Hospital in Malaysia. East J Med. 2007;12(1):6–14.
25. Escobar GJ, Li DK, Armstrong MA, et al. Neonatal sepsis workups in infants >/=2000 grams at birth: a population-based study. Pediatrics. 2000;106:256–263. doi:10.1542/peds.106.2.256
26. Benitz WE, Gould JB, Druzin ML. Risk factors for early-onset group B streptococcal sepsis: estimation of odds ratios by critical literature review. Pediatrics. 1999;103(6). Available from: www.pediatrics.org/cgi/content/full/103/6/e77.
27. Mukhopadhyay S, Puopolo KM. Risk assessment in neonatal early onset sepsis. Semin Perinatol. 2012;36(6):408–415. doi:10.1053/j.semperi.2012.06.002
28. Jabiri A, Herman LW, Avelina S, et al. Prevalence and factors associated with neonatal sepsis among neonates in Temeke and Mwananyamala Hospitals in Dar es Salaam. Tanzania. J Health Res. 2016;18:1–7.
29. Chan GJ, Stuart EA, Zaman D, et al. The effect of intrapartum antibiotics on early-onset neonatal sepsis in Dhaka, Bangladesh: a propensity score matched analysis. BMC Pediatr. 2014;14:18. doi:10.1186/1471-2431-14-104
30. Boskabadi H, Maamouri G, Mafinejad S. Neonatal complications related with prolonged rupture of membranes. Maced J Med Sci. 2011;4:93–98.
31. Masanja PP, Kibusi SM, Mkhoi ML. Predictors of early onset neonatal sepsis among neonates in Dodoma, Tanzania: a case control study. J Trop Pediatr. 2020;66(3):257–266. doi:10.1093/tropej/fmz062
32. Rathore H, Rahman AJ, Salman M, Nasir M, Sherali S. Frequency of early-onset neonatal sepsis following prolonged rupture of membranes. Cureus. 2020;12(2). doi:10.7759/cureus.6864
33. Shitaye D, Asrat D, Woldeamanuel Y, Worku B. Risk factors and etiology of neonatal sepsis in Tikur Anbessa University Hospital, Ethiopia. Ethiop Med J. 2010;48(1):11–21.
34. Khatua SP, Das AK, Chatterjee BD, Khatua S, Ghose B, Saha A. Neonatal septicemia. Indian J Pediatr. 1986;53:509–514. doi:10.1007/BF02749537
35. Stoll BJ. Infections of the neonatal infant. In: Berhman RE, Kliegman RM, Jenson HB, editors. Nelson Textbook of Pediatrics.
36. Adatara P, Afaya A, Salia SM, et al. Risk Factors for Neonatal Sepsis: a Retrospective Case-Control Study among Neonates Who Were Delivered by Caesarean Section at the Trauma and Specialist Hospital, Winneba, Ghana. BioMed Res Int. 2018;2018:7. doi:10.1155/2018/6153501
37. Ogundare E, Akintayo A, Aladekomo T, Adeyemi L, Ogunlesi T, Oyelami O. Presentation and outcomes of early and late onset neonatal sepsis in a Nigerian Hospital. Afr Health Sci. 2019;19(3):2390–2399. doi:10.4314/ahs.v19i3.12
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.