Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 15
Incidence and Prevalence of Septic Arthritis in Thailand: A Database from the Ministry of Public Health
Authors Foocharoen T, Onchan T, Pongkulkiat P, Mahakkanukrauh A, Suwannaroj S, Foocharoen C ![]()
Received 11 August 2023
Accepted for publication 28 October 2023
Published 7 November 2023 Volume 2023:15 Pages 213—222
DOI https://doi.org/10.2147/OARRR.S434983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chuan-Ju Liu
Thanit Foocharoen,1 Tippawan Onchan,2 Patnarin Pongkulkiat,2 Ajanee Mahakkanukrauh,2 Siraphop Suwannaroj,2 Chingching Foocharoen2
1Department of Orthopedics, Khon Kaen Hospital, Khon Kaen, 40000, Thailand; 2Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand
Correspondence: Chingching Foocharoen, Department of Medicine, Faculty of Medicine, Khon Kaen University, Khon Kaen, 40002, Thailand, Tel +66-43-363-746, Email [email protected]
Background: A better understanding of the epidemiological profile of septic arthritis or pyogenic arthritis in Thais could improve care and provide information for better infectious control. We aimed to determine the incidence and prevalence of septic arthritis in Thailand between 2017 and 2020.
Methods: A descriptive epidemiological study was performed using demographic data from patients over 18 years of age having a primary diagnosis of M00 pyogenic arthritis between 2017 and 2020. Data were sourced from the Information and Communication Technology Center, Ministry of Public Health database. The incidence and prevalence of septic arthritis were calculated, and their respective 95% confidence interval (CI).
Results: The number of patients with septic arthritis in 2017 was 26,878 from a total Thai population of 65,204,797. The prevalence of septic arthritis in 2017 was 41.2 per 100,000 (95% CI 40.7– 41.7). The prevalence of septic arthritis among women was slightly higher than among men (42.2 vs 40.2 per 100,000). The incidence of septic arthritis slightly increased from 2018 to 2019 but was stable in 2020 (22.6, 23.3, and 23.1 per 100,000 person-years, respectively). The incidence was highest in the southern region between 2018 and 2019 but highest in the northeast in 2020. The peak was in the elderly population 60 and older (56.4, 59.5, and 57.3 per 100,000 person-years in 2018, 2019, and 2020, respectively). The incidence increased with age and the maximum rate was in those ≥ 70 years (70.2 per 100,000 person-years in 2019).
Conclusion: Septic arthritis commonly presents in the elderly and is comparable between men and women. The disease was found mainly in the northeastern and southern regions. The incidence remained stable during the study period.
Keywords: septic arthritis, pyogenic arthritis, infectious arthritis, epidemiology, observational study
Introduction
Septic arthritis or pyogenic arthritis is a medical emergency requiring prompt diagnosis and treatment. If left untreated, the bacteria responsible for septic arthritis can rapidly destroy joints and cause joint disability. Acute bacterial arthritis is usually caused by gonococcal or nongonococcal septic arthritis. The most common cause of non-gonococcal septic arthritis in all age groups is Staphylococcus aureus.1 Key symptoms of septic arthritis include high fever, pain, swelling, and warmth around the infected joint. Detecting pathogens from synovial fluid through staining and/or culture is crucial to diagnosing the condition. Infected synovial fluid is typically cloudy or purulent, and the white blood cell count is usually elevated to more than 50,000 cells/mm3.2 Both nongonococcal and gonococcal septic arthritis have their clinical features and prognosis differ. Non-gonococcal septic arthritis tends to be more severe and has a worse prognosis than gonococcal septic arthritis.
It is recommended that all patients with suspected bacterial arthritis, whether it is caused by gonorrhea or non-gonorrhea, be admitted for observation and treatment with intravenous antibiotics.3 A clinical study conducted in Thailand in 2010 found that septic arthritis was the third most common rheumatic disease leading to hospitalization, following osteoarthritis and gout. The prevalence rate was 13.5 per 100,000 population, with higher rates in the northern and northeastern regions, particularly among individuals over 60.4 Since there have been no recent reports of the incidence of septic arthritis in Thailand, we felt it prudent to update the incidence and prevalence of bacterial arthritis for a more comprehensive epidemiological picture in Thailand. We reasoned an epidemiological study comparing past and current data should yield valuable insights into the epidemiology of septic arthritis in the Thai population and contribute to better care planning for patients with bacterial arthritis, as well as help in manpower planning and the allocation of public health policy budgets for the care of septic arthritis.
Methods
A descriptive epidemiological study was conducted among patients over 18 with a primary diagnosis of M00 pyogenic arthritis using the International Classification of Diseases, Tenth Revision (ICD-10). Data were recorded in the Information and Communication Technology Center, Ministry of Public Health database between 2017 and 2020.
Information Resources and Statistical Analysis
The study was carried out using the Information and Communication Technology Center, Ministry of Public Health database, which comprises healthcare paid for by (i) the National Health Security Office (NHSO), (ii) the Civil Servant Medical Benefit Scheme of the Comptroller General’s Department; (iii) the Social Security Office; and (iv) self-payment. Databases were constituted from a collection of data submitted by hospitals. The diagnosis was coded using ICD-10. Epidemiological data from patients with a primary diagnosis of M00 pyogenic arthritis between 2017 and 2020 were extracted and reviewed. Data included age on the date of diagnosis of septic arthritis, sex, year of visit, hospital name, municipal district (Amphoe), and province. Duplicate entries were removed. The incidence and cumulative incidence of septic arthritis were analyzed, including the respective 95% confidence interval (CI). The data included an overall national and regional perspective (viz., the northern, eastern, northeastern, southern, and central regions). Population data for disease prevalence came from the National Statistical Office of Thailand.5 Categorical data were presented as numbers and percentages of observed events (septic arthritis). The continuous data that exhibited a symmetrical distribution without skew by the Shapiro–Wilk test were presented as means and standard deviations (SD). The results were presented as median with interquartile range (IQR) for data with an abnormal distribution. All data analyses were performed with STATA version 16.0 (StataCorp., College Station, TX, USA).6
Results
Between 2017 and 2020, 72,005 cases from the database had a primary diagnosis of M00 pyogenic arthritis. In 2017, the number of patients with septic arthritis was 26,878 cases, from a total Thai population of 65,204,797, including 31,966,108 men and 33,238,689 women. Thus, the prevalence of septic arthritis in 2017 was 41.2 per 100,000 (95% CI 40.7–41.7). The proportion of females was slightly higher than that of males. The respective number of septic arthritis in 2017 in Thai women and men was 14,034 and 12,844 cases, with a prevalence of 42.2 per 100,000 (95% CI 41.5–42.9) and 40.2 per 100,000 (95% CI 39.5–40.9). The overall mean age of the prevalence cases in 2017 was 54.9±19.2 years.
The incidence of septic arthritis in Thailand increased slightly from 2018 to 2019 but trended to be stable between 2019 and 2020 and was slightly higher in women than men. The respective incidence of septic arthritis in 2018, 2019, and 2020 was 22.6 per 100,000 person-years (95% CI 22.2–23.0), 23.3 per 100,000 person-years (95% CI 22.9–23.6), and 23.1 per 100,000 person-years (95% CI 22.7–23.4). The number of new cases of septic arthritis and the total Thai population stratified by year are presented in Table 1, and the incidence of septic arthritis stratified by year is presented in Table 2.
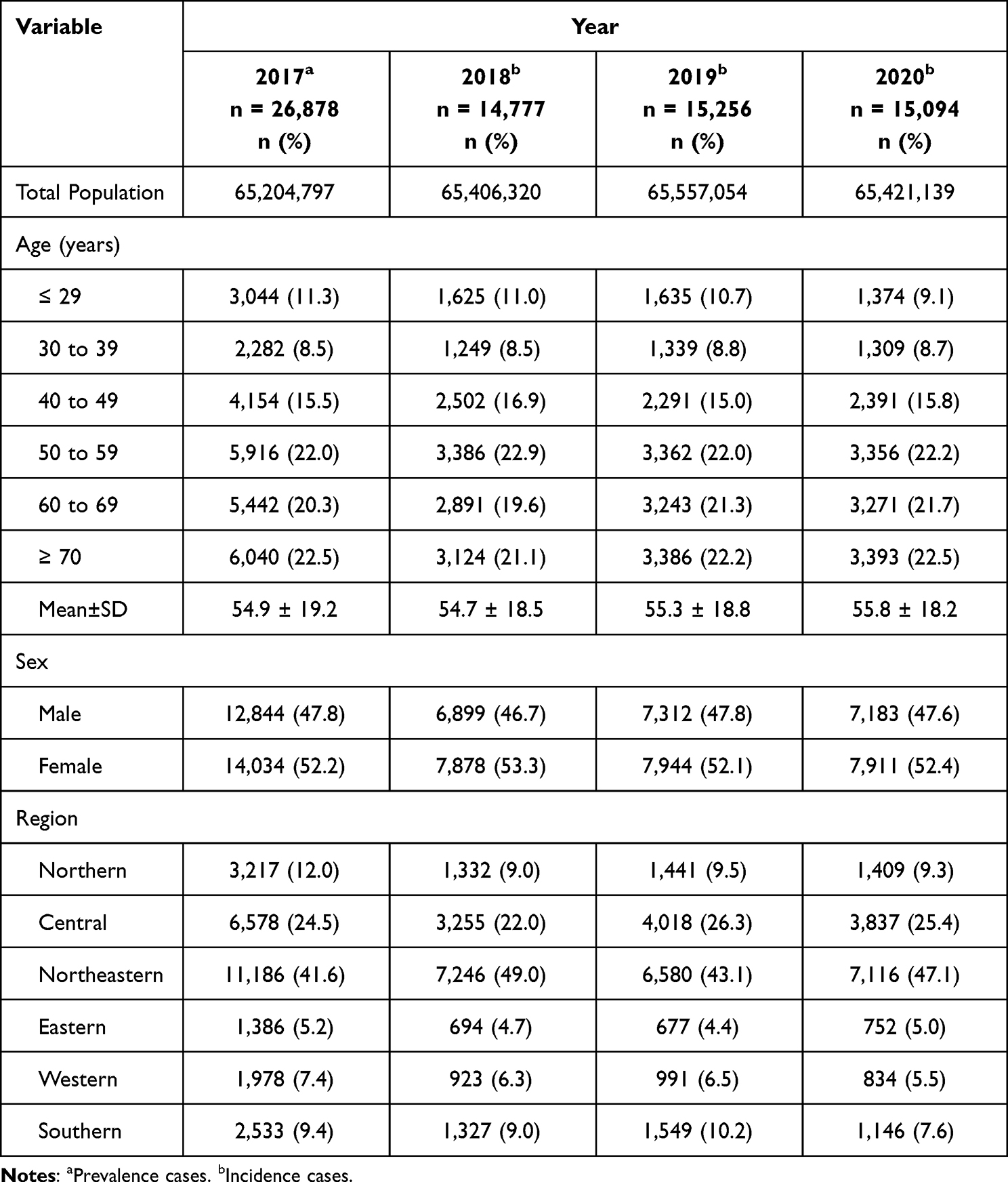 |
Table 1 Data from Septic Arthritis Cases Between 2017 and 2020 (n=72,005) |
 |
Table 2 Prevalence and Incidence of Septic Arthritis per 100,000 Person-Years with 95% CI in Thailand from 2017 to 2020 |
The mean age of incidence cases from 2018 to 2020 was comparable to that of the prevalence cases in 2017. The incidence was highest in those 60 and older, and the findings were similar over a 3-year period. The southern region had the highest incidence of septic arthritis between 2018 and 2019, but it was highest in the northeastern region in 2020 (Table 2.).
The highest number of patients in 2017 was in the northeastern region (11,186 cases; 41.6%) according to the number of patients with septic arthritis per 100,000 based on hospital visits, followed by the central region (6,578 cases; 24.5%), and the northern region (3,217; 12.0%) (Figure 1A). New cases of septic arthritis were found mainly in the northeast region, mainly in Khon Kaen province in 2018–2019, with a respective incidence of 149.4 and 87.7 per 100,000 person-years, while Phichit province, in the north-central region, had the highest incidence of septic arthritis in 2020 (88.3 per 100,000 person-years). Few cases were reported in the western, southern, and eastern regions (Figures 1B-D).
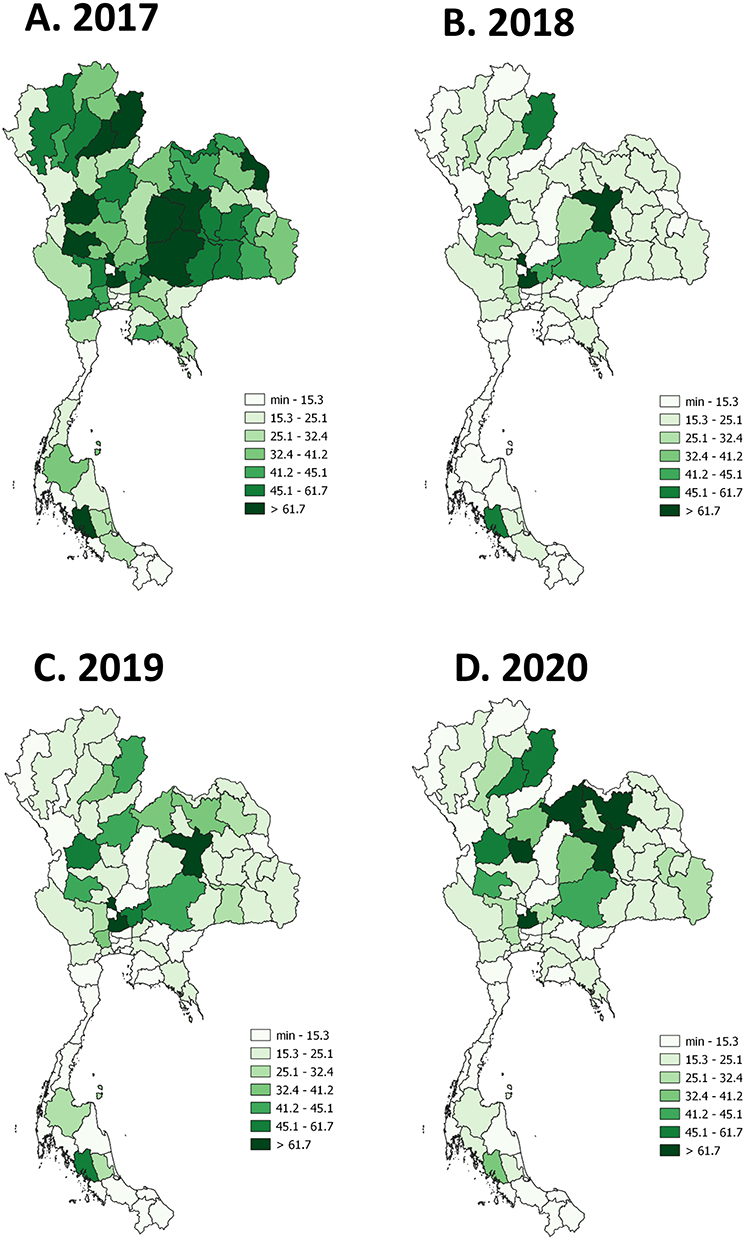 |
Figure 1 Number of patients with septic arthritis per 100,000 by hospital-based visit. (QGIS software version 3.8.2: an open source and free software of geographic data system information was used for generating the maps; https://www.qgis.org/en/site/). (A) Number of septic arthritis in 2017 (prevalence cases). (B) Number of new cases of septic arthritis in 2018 (incidence cases). (C) Number of new cases of septic arthritis in 2019 (incidence cases). (D) Number of new cases of septic arthritis in 2020 (incidence cases). Abbreviation: Min; minimum. |
The most prevalent causative organisms among Thais were species of Staphylococcus, with the knee joint being the most frequently affected. Details regarding the common causative organisms and joint involvements in the prevalence cases of 2017 are presented in Table 3.
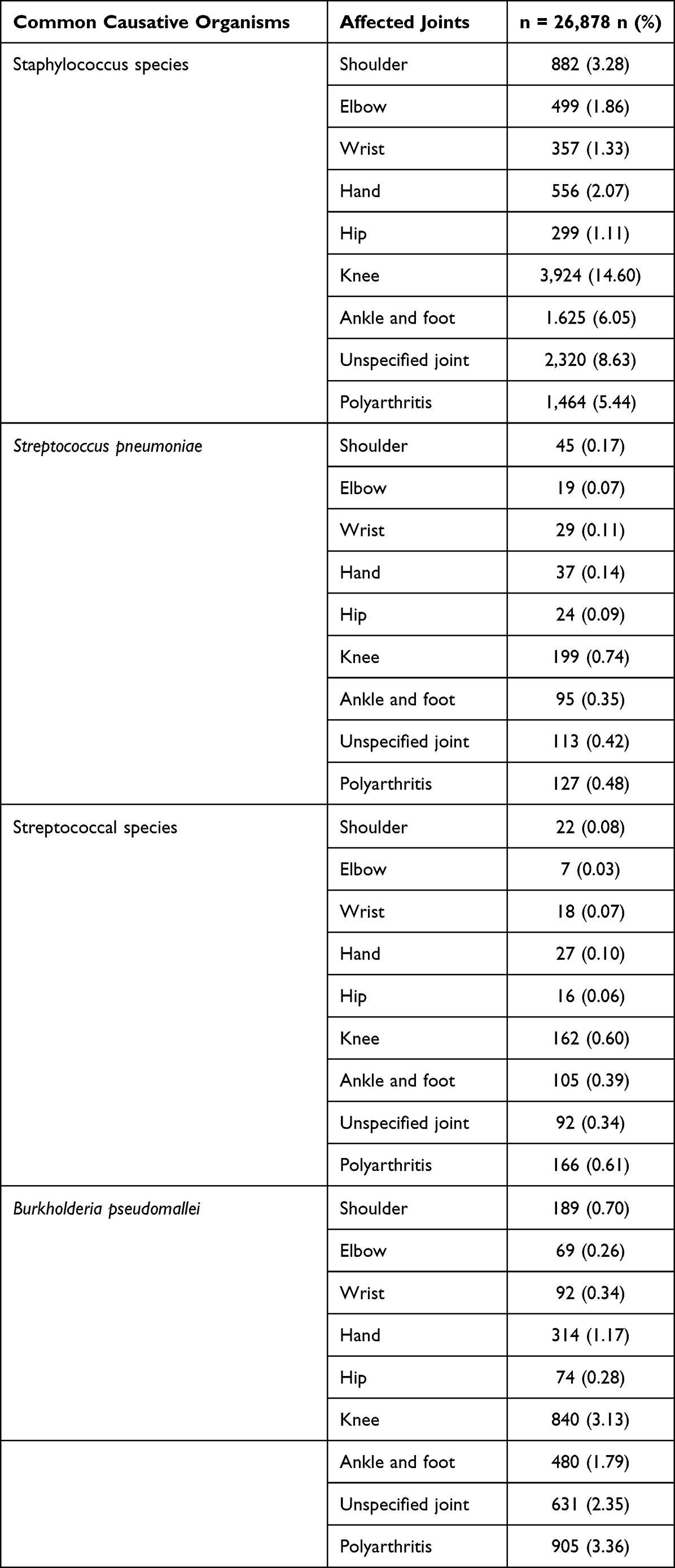 |
Table 3 Common Causative Organisms and Affected Joints in the 2017 |
Two thousand eight hundred twenty-seven patients with septic arthritis died in 2017–2020, with a median age of 70.0 years (IQR 59.6–81.0). The most common cause of non-survived septic arthritis was sepsis and septic shock (285 cases), followed by pneumonia (114 cases), hypertension (99 cases), type 2 diabetes mellitus (97 cases), and chronic kidney disease (CKD) (73 cases). The majority of the non-survived cases were elderly patients 60 and over. Age group classified by common causes of death is presented in Figure 2.
 |
Figure 2 Age group in the top 5 common causes of death in patients with septic arthritis in 2017–2020. |
Discussion
Herein, we report the epidemiology of septic arthritis in Thailand, including data from the National Information and Communication Technology Center the Ministry of Public Health that covers all healthcare providers. Most Thais receive health services in hospitals under the Ministry of Public Health, and their information is recorded during visits to out- and/or in-patient departments. The diagnoses per the ICD were extracted from the database (M00). Our epidemiological study explored the prevalence and incidence of septic arthritis among Thais between 2017 and 2020, which overlapped with the emergence of the COVID-19 pandemic (early January 2020).7
From 2018 to 2020, the prevalence and incidence of septic arthritis was approximately 41 per 100,000 population and 22–23 per 100,000 person-years. The incidence seemed higher than a previous report in the Australian population (9.2 per 100,000 person-years)8 but comparable to a New Zealand study.9 McBride et al reported the prevalence of septic arthritis among New Zealand adults from 2006 to 2013 at 21 per 100,000 person-years using ICD-10 from the electronic review.9 Our incidence was slightly less than among Aboriginal Australians, with 29.1 per 100,000 person-years.8 Modifications to the study method, such as the definition of septic arthritis and the time duration of the study, might explain the discrepancies in the findings. Unfortunately, there are no data on the epidemiology of septic arthritis in adults from Southeast Asia, where the population is comparable to Thailand’s, so we do not have information on those countries to compare with ours.
The prevalence and incidence increased with age, mainly among those ≥ 60 years of age. The age group of septic arthritis in Thais was similar to the age group of septic arthritis in the Portuguese population (median age 67 years),10 the New Zealand population (mean age 60 years),11 and the Maltese population (median age 66 years).12 However, the age group was slightly higher than in a previous study of the Thai population. Teparrukkul et al13 reported that the median age of patients with septic arthritis between 2012 and 2014 in northeast Thailand was 55 years. The difference in the findings could be related to the causative organism and the specific area of the study. Burkholderia pseudomallei is a common infectious disease in northeastern Thailand13,14 and is found more frequently in patients with diabetes mellitus.15 Additionally, type 2 diabetes mellitus in Thais mainly presents in a late-middle-aged group, particularly 50 and older.16 We included not only patients with septic arthritis from the northeastern but also the other regions of Thailand and not limited to the causative organism. Therefore, the demographics of the disease can explain why the age group of the patients with septic arthritis in the previous study was lower than ours. Our age group was also higher than in the Brazilian population (mean age 41.6)17 and the New Zealand population (mean age 49).9 The difference in the study method could also explain the difference in the findings, the definition of septic arthritis, and the study period.
Elderly patients with septic arthritis had poor outcomes. Our results showed that the median age for non-survived septic arthritis cases was 70. An aging population generally has more underlying diseases and health problems that might be at risk of infection (including joint infection), resulting in higher morbidity and mortality. Septic arthritis should be examined in the elderly with fever and joint pain because of the prevalence of septic arthritis among elderly patients, the poor prognosis among those older patients, and the aging society. Once septic arthritis is diagnosed, early treatment with close monitoring is warranted to prevent disease complications and decrease morbidity and mortality among elderly patients.
The new cases of septic arthritis were revealed mainly in the Northeast region and the majority in Khon Kaen province, with a prevalence in 2018–2020 of approximately 30–35.5 per 100,000 person-years. The incidence of septic arthritis in this region was comparable to a previous report by Teparrukkul et al13 in which the cumulative incidence of bacteremia in patients with septic arthritis was around 31–39 per 100,000 person-years in the northeast in 2012–2014 for gram-positive bacterial septic arthritis. However, the cumulative incidence was much higher in those diagnosed with Burkholderia pseudomallei septic arthritis (45 per 100,000 person-years). The finding is supported by the high prevalence of Burkholderia pseudomallei in Northeastern Thailand (1,160 cases; 32.3%) (data not shown). Our findings might help assess the geographic distribution of septic arthritis in Thailand.
Staphylococcal septic arthritis is the most common type among Thais, with the knee joint being the most commonly affected. These findings are consistent with those of previous studies in the last decade,11,18 suggesting that globally there has been no change in the distribution of causative organisms and joint involvement. For patients with clinicals suspicious of septic arthritis and no definite organism identified at presentation, initial treatment should include antibiotics with Staphylococcal aureus coverage.
Septic arthritis in Thais was comparable between males and females, while previous studies reported a male predominance with a male-to-female ratio around 2:1 to 1.5:1.10,12,13,17,19 The more significant number of females in the Thai population could explain the finding5 as well as the longer life expectancy of Thai females over Thai males.20 According to our results, wherein incidence increased with age, it is possible that elderly females might have an increased risk of septic arthritis with age.
Further study should be conducted to define the predisposing factors that can increase the risk of developing septic arthritis, such as joint trauma, invasive joint procedures, intravenous drug use, concomitant comorbid diseases, immunocompromised conditions, preexisting joint conditions, and prosthetic joints.
Our study had some limitations, including that (a) the clinical information from the database was incomplete; (b) the data were collected from almost all hospitals in Thailand, but not private clinics and some university hospitals in the central region, which usually absorb many complicated patients, so the prevalence and incidence of septic arthritis might have been underestimated; (c) the principal diagnosis in the database was coded according to the ICD-10, which does not provide a specific code for clinical features, disease complications, and treatment. So we are not able to provide detailed epidemiology of septic arthritis; and, (d) ICD-10 coding errors can occur in daily practice, so we cannot be certain that all patients in the database had a correct diagnosis. The study strengths were: (a) all necessary demographic data were analyzed; (b) the data were sufficient to complete an overall assessment of the epidemiology of septic arthritis in Thailand; (c) the study was based on a most extensive database from the Ministry of Public Health, thereby ensuring a complete set of epidemiological characteristics for septic arthritis in Thailand; and, (d) the results can be generalized to other Southeast Asian and/or Asian-Pacific countries with similar ethnicity and geography.
Conclusion
The prevalence of septic arthritis in Thais in 2017 was 41.2 per 100,000, while the incidence remained stable during the study period, with the respective incidence in 2018, 2019, and 2020 being 22.6, 23.3, and 23.1 per 100,000 person-years. Septic arthritis commonly presents in the elderly, and the incidence is comparable between men and women. The disease is found mainly in the Northeast and South regions. Elderly patients have poor outcomes. The epidemiologic study of septic arthritis might help assess the geographic distribution, human resource planning, and allocation of public health policy budgets for treating septic arthritis in Thailand.
Data Sharing Statement
Data and material are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The Human Research Ethics Committee of Khon Kaen University reviewed and approved the study per the Helsinki Declaration and the Good Clinical Practice Guidelines (HE641592). The Human Research Ethics Committee of Khon Kaen University waived the requirement for informed consent because of the retrospective nature of the study. Participant privacy was protected by anonymized data and kept confidentiality.
Acknowledgments
The authors thank (a) the Information and Communication Technology Center, Ministry of Public Health database for providing access to the database, (b) Mrs. Udomluck Piansukvej for research assistance, and (c) Mr. Bryan Roderick Hamman—under the aegis of the Publication Clinic Khon Kaen University, Thailand—for assistance with the English-language presentation.
Disclosure
All authors declare that they do not have a conflict of interest.
References
1. Shirtliff ME, Mader JT. Acute septic arthritis. Clin Microbiol Rev. 2002;15(4):527–544. doi:10.1128/CMR.15.4.527-544.2002
2. Turner EHG, Lang MDH, Spiker AM. A narrative review of the last decade’s literature on the diagnostic accuracy of septic arthritis of the native joint. J Exp Orthopaedics. 2021;8(1):3. doi:10.1186/s40634-020-00315-w
3. Hassan AS, Rao A, Manadan AM, Block JA. Peripheral Bacterial Septic Arthritis: review of Diagnosis and Management. J Clin Rheumatol. 2017;23(8):435–442. doi:10.1097/RHU.0000000000000588
4. Mahakkanukrauh A, Thavornpitak Y, Foocharoen C, Suwannaroj S, Nanagara R. Features and outcomes of hospitalized Thai patients with pyogenic arthritis: analysis from the nationwide hospital database. Int J Rheum Dis. 2013;16(4):387–391. doi:10.1111/1756-185X.12071
5. National Statistical Office. Available from: http://statbbi.nso.go.th/staticreport/page/sector/en/01.aspx.
6. College Station, TX, StataCorp LLC. Stata Statistical Software: Release 16. College Station, TX, StataCorp LLC; 2019.
7. Coronavirus disease 2019 (COVID-19) WHO Thailand Situation Report - 2 September 2020 [EN/TH] - Thailand | reliefWeb. Available from: https://reliefweb.int/report/thailand/coronavirus-disease-2019-covid-19-who-thailand-situation-report-2-september-2020.
8. Morgan DS, Fisher D, Merianos A, Currie BJ. An 18 year clinical review of septic arthritis from tropical Australia. Epidemiol Infect. 1996;117(3):423–428. doi:10.1017/S0950268800059070
9. McBride S, Mowbray J, Caughey W, et al. Epidemiology, Management, and Outcomes of Large and Small Native Joint Septic Arthritis in Adults. Clin Infect Dis. 2020;70(2):271–279. doi:10.1093/cid/ciz265
10. Rego de Figueiredo I, Vieira Alves R, Guerreiro Castro S, Antunes AM, Gruner H, Panarra A. Septic arthritis incidence and risk factors: a 5-year cross-sectional study. Infect Dis. 2019;51(8):635–637. doi:10.1080/23744235.2019.1633471
11. Kennedy N, Chambers ST, Nolan I, et al. Native Joint Septic Arthritis: epidemiology, Clinical Features, and Microbiological Causes in a New Zealand Population. J Rheumatol. 2015;42(12):2392–2397. doi:10.3899/jrheum.150434
12. Vassallo C, Borg AA, Farrugia D, Mercieca C. The Epidemiology and Outcomes of Septic Arthritis in the Maltese Islands: a Hospital-Based Retrospective Cohort Study. Mediterr J Rheumatol. 2020;31(2):195. doi:10.31138/mjr.31.2.195
13. Teparrukkul P, Nilsakul J, Dunachie S, Limmathurotsakul D. Clinical Epidemiology of Septic Arthritis Caused by Burkholderia pseudomallei and Other Bacterial Pathogens in Northeast Thailand. Am J Trop Med Hyg. 2017;97(6):1695–1701. doi:10.4269/ajtmh.17-0288
14. Limmathurotsakul D, Wongratanacheewin S, Teerawattanasook N, et al. Increasing incidence of human melioidosis in Northeast Thailand. Am J Trop Med Hyg. 2010;82(6):1113–1117. doi:10.4269/ajtmh.2010.10-0038
15. Chowdhury S, Barai L, Afroze SR, et al. The Epidemiology of Melioidosis and Its Association with Diabetes Mellitus: a Systematic Review and Meta-Analysis. Pathogens. 2022;11(2):149. doi:10.3390/pathogens11020149
16. Papier K, Jordan S, D’Este C, et al. Incidence and risk factors for type 2 diabetes mellitus in transitional Thailand: results from the Thai cohort study. BMJ Open. 2016;6(12):e014102. doi:10.1136/bmjopen-2016-014102
17. Helito CP, Noffs GG, Pecora JR, et al. Epidemiology of septic arthritis of the knee at Hospital das Clínicas, Universidade de São Paulo. Braz J Infect Dis. 2014;18(1):28–33. doi:10.1016/j.bjid.2013.04.010
18. Dubost JJ, Couderc M, Tatar Z, et al. Three-decade trends in the distribution of organisms causing septic arthritis in native joints: single-center study of 374 cases. Joint Bone Spine. 2014;81(5):438–440. doi:10.1016/j.jbspin.2014.05.001
19. Mue D, Salihu M, Awonusi F, Yongu W, Kortor J, Elachi I. The epidemiology and outcome of acute septic arthritis: a hospital based study. J West Afr Coll Surg. 2013;3(1):567.
20. Thailand - life expectancy at birth by gender 2011-2021. Statista. Available from: https://www.statista.com/statistics/974709/life-expectancy-at-birth-in-thailand-by-gender/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.