")
Back to Journals » International Journal of General Medicine » Volume 16
Incidence and Predictors of Aspiration Pneumonia Among Stroke Patients in Western Amhara Region, North-West Ethiopia: A Retrospective Follow Up Study
Authors Lidetu T , Muluneh EK , Wassie GT
Received 22 February 2023
Accepted for publication 12 April 2023
Published 15 April 2023 Volume 2023:16 Pages 1303—1315
DOI https://doi.org/10.2147/IJGM.S400420
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Luca Testarelli
Tadios Lidetu, Essey Kebede Muluneh, Gizachew Tadesse Wassie
School of Public Health, Bahir Dar University, Bahir Dar, Ethiopia
Correspondence: Essey Kebede Muluneh, Bahir Dar University, P.O. Box 79, Office No. 114, First Floor, Wisdom Tower, Bahir Dar, Ethiopia, Tel +251932808002, Email [email protected]; [email protected]
Background: Aspiration pneumonia is one of the major complications among hospitalized stroke patients, with global incidence ranging from 5– 83% and hospital mortality rate of up to 70%. This study aimed to assess the incidence and identify predictors of aspiration pneumonia among stroke patients in Western Amhara region, North-West Ethiopia.
Methods: An institution-based retrospective follow-up study was conducted on a simple random sample of 568 stroke patients in Western Amhara region admitted at Felege Hiwot Referral Hospital. Log binomial regression model, a generalized linear model with log link, was applied to identify significant predictors of aspiration pneumonia.
Results: Cumulative incidence of aspiration pneumonia among the 568 sampled patients was 23.06%. Males were 1.71 times more at risk to acquire aspiration pneumonia than females (ARR = 1.71, 95% CI 1.07– 2.74). Patients with vomiting and dysphagia were at more risk of acquiring aspiration pneumonia as compared with patients without vomiting and dysphagia (ARR = 1.81, 95% CI 1.04– 3.14 and ARR = 1.95, 95% CI 1.10– 3.48, respectively). Patients who received antibiotic prophylaxis and patients with Glasgow Coma Scale greater than 12 had less risk of acquiring aspiration pneumonia as compared with those who did not receive antibiotic prophylaxis and patients with Glasgow Coma Scale less than 8 (ARR = 0.10, 95% CI 0.04– 0.28 and ARR = 0.45, 95% CI 0.22– 0.94, respectively).
Conclusion: The cumulative incidence of aspiration pneumonia among sampled patients was 23.06%. Vomiting, dysphagia, antibiotic treatment and Glasgow Coma Scale showed significant correlation with the acquiring of aspiration pneumonia. Therefore, we recommend health-care providers should give special attention for patients with these risk factors to prevent aspiration pneumonia.
Keywords: incidence, aspiration, pneumonia, stroke patients, log binomial regression model
Introduction
Aspiration is often the result of impaired swallowing, which allows oral or gastric contents, or both, to enter the lung, especially in patients who also have an ineffective cough reflex. The material that can be aspirated varies and includes saliva, nasopharyngeal secretions, bacteria, liquids, toxic substances, food, or gastric contents.1–3 The entrance of gastrointestinal (GI) content into the lungs suppresses the natural defenses of the respiratory system resulting in a broad spectrum of pulmonary diseases such as airway obstruction, aspiration pneumonia and acute respiratory distress syndrome which significantly increase the patient’s morbidity and mortality.3–5 Aspiration pneumonia is an acute infection of the lung induced by the inhalation or entrance of endogenous flora and different body chemicals from the gastrointestinal (GI) tract into the respiratory system.6,7 It is one of the major complications among hospitalized stroke patients.8 Among different aspirations, food aspiration is common in debilitated patients such as patients with stroke and leads them to a high risk of aspiration pneumonia.9
Despite the different preventive and therapeutic approaches being practiced for patients with post stroke aspiration pneumonia at health facilities level, patient morbidity and mortality is still increasing (incidence up to 83% and mortality rate up to 70%).7,10–12 The global incidence of aspiration pneumonia among post-stroke patients is 14%. However, the incidence has significant variations among the different regions of the world ranging from 5% in the USA up to 83% in Iraq.13–15 The incidence in Nigeria, Sierra Leone and Egypt in post-stroke patients is 12.4%, 18% and 44%, respectively.16–18
Different risk factors influence the entrance of gastrointestinal contents into the respiratory system contributing to the occurrence of aspiration pneumonia.19 Reduced level of consciousness and improper positioning (e.g. simple supine position) exposes the patient for aspiration that leads to aspiration pneumonia.20,21 Patients with advanced age have reduced muscle mass and strength which results in impaired chewing and swallowing function and cough reflex and hence experience reduced immunity and increased comorbidities that increase the risk of aspiration and lastly aspiration pneumonia.14,18,22,23 It is also associated with more severe neurological outcome.24
Hemorrhagic stroke and comorbidities such as congestive heart failure, ischemic heart disease, neurological diseases, diabetes mellitus, hypertension, oxygen saturation below the normal range (less than 95%) and pulmonary diseases suppress immunity and increase the risk of aspiration, which further results in the occurrence of aspiration pneumonia.13,25–27 Aspiration pneumonia is more common among patients residing in rural areas than those residing in urban settings, which may be due to the differences in economic status, health service availability, education and living habits.28–31
Clinical factors are very important for the occurrences of aspiration pneumonia in post-stroke patients. Any condition or health problem that impairs the level of consciousness can cause a person to aspirate oropharyngeal or gastric contents that mimic the occurrence of aspiration pneumonia.32 Dysphagia is a complication associated with neurological diseases such as dementia, Parkinson’s disease, multiple sclerosis, and stroke. It is another main clinical factor for aspiration pneumonia. Patients with dysphagia take more time and effort to move food from the mouth to their stomach which increases the aspiration risk of oropharyngeal contents.33,34 Increased severity of dysphagia increases the risk of aspiration pneumonia.35
Neurological problems such as seizure can predispose a patient to acquire post-stroke aspiration pneumonia.36 Patients with ischemic stroke are less likely to develop aspiration pneumonia compared with patients with a hemorrhagic type of stroke.29 Hyperglycemia is also a common risk factor for aspiration pneumonia.37
Patients with multiple risks have increased rates of aspiration pneumonia, death, and other adverse outcomes. Frail elderly patients having both dysphagia and cerebrovascular diseases are more at risk of aspiration pneumonia than patients with only one of these diseases.38
Care processes that include positioning of the patient, mobilization, health-care provider competences and adherence to safe swallowing techniques are clinical and pharmacological management approaches that decrease incidence of aspiration pneumonia.39 Giving antibiotic prophylaxis for post-stroke patients greatly reduces the risk of aspiration pneumonia.40,41
A randomized control trial study showed that giving anti-vomiting medications and putting the patient on nasogastric tube feeding decreases the risk of aspiration pneumonia.40 Patients who are on tube feeding are less exposed to aspiration pneumonia than those on non-tube feeding. That is because the nasogastric tube protects against the entrance of gastrointestinal contents into the respiratory system.34 Oxygen saturation below the normal range (less than 95%) accounts for 20.6% of the risk of developing aspiration pneumonia.42
Identifying the risk factors for aspiration pneumonia is critical for prevention, early treatment, and reduced mortality of patients after stroke attacks.19 Different studies in different countries showed that the incidence of aspiration pneumonia varied across the world. In Ethiopia, the incidence and predictors of aspiration pneumonia among post-stroke patients are not well studied. Therefore, this study aimed to determine the incidence and identify predictors of aspiration pneumonia among post-stroke patients of Western Amhara region admitted at Felege Hiwot Referral Hospital, North-West Ethiopia.
Materials and Methods
Study Design
An institution-based retrospective follow-up study design was conducted to determine the incidence and identify the predictors of aspiration pneumonia among stroke patients of Western Amhara region admitted at Felege Hiwot Referral Hospital, Bahir Dar, Ethiopia. Felege Hiwot Referral Hospital provides services for over 12 million people in the Amhara and neighboring regions. It is a referral hospital having more than 400 hospital beds with 95.5% bed occupancy rate (BOR) and 4.7 days average length of patient stay in the hospital. The hospital has 15 adult outpatient departments (OPD) and it serves an average of 935 patients per month within each OPD. The services it provides include antiretroviral therapy (ART), psychiatry, internal medicine, surgery, gynecologic and obstetric, pediatric, orthopedic, oncologic, laboratory, and pharmacy.
The study period was from July 2017 to June 2021 and the data were extracted from September 20, 2021 to October 10, 2021. The study population comprises all stroke patients of Western Amhara region admitted at Felege Hiwot specialized hospital from July 2017 to June 2021. Stroke patients who had aspiration pneumonia at admission or were diagnosed within 48 hours of hospital stay and patients who had less than two days (48 hours) length of stay in the hospital were excluded.
The sample size is calculated using Epi-Info version-7.2. Double population-proportion formula using 95% confidence level, 80% power of the test and 1:1 ratio of unexposed to exposed group was applied. Final sample size determined by using these assumptions and results from related studies37 was found to be 568.
The required data were collected by trained data collectors (trained nurses in the hospital) using a well-structured checklist prepared by the investigators from patients’ chart review. To ensure data quality, the consistency between the data extraction checklist and completeness of the recording system was first checked piloting 5% (28 charts) of the selected sample. The investigators checked the completeness and consistency of the collected data.
Variables
The response variable of this study is a binary variable aspiration pneumonia (No = 0, Yes = 1). Independent variables include:
Socio-demographic variables such as sex, age, residence, marital status, and occupational status, clinical variables such as Glasgow Coma scale, stroke side of the body, types of stroke, hypertension, diabetes mellitus, heart diseases, vomiting, dysphagia, seizure and hyperglycemia, and treatment-related variables such as surgical treatment, heparin, warfarin, aspirin, anticholestrol, mannitol, antibiotic prophylaxis, antipain, antivomiting, nasogastric tube feeding, oxygen therapy, intravenous fluid therapy and patient length of hospital stay.
Data Management and Analysis Procedure
The data were entered using EpiData version 3.1 and then exported to STATA version-14 for analysis. Before conducting the analysis, missing values were checked and handled using multiple imputation technique. Multicollinearity between independent variables was checked using variance inflation factor for continuous independent variables and Spearman’s rank correlation for categorical independent variables.
For binary outcome data odds ratio is the most prevalent measure of association. However, odds ratios are difficult to interpret and have sometimes been erroneously described as though they were relative risks. When the outcome of interest is rare (less than 10%), the odds ratio, which is the output of logistic regression, indirectly estimates the risk ratio. However, when the outcome is not rare, the odds ratio becomes inflated and it could not estimate the risk ratio. Recently, much attention has been given to the estimation of relative risk instead of the odds ratio.43–45 There are different alternatives to estimate risk ratio when the odds ratio is not a good estimator. Generalized linear model (log binomial regression model with log-link function) is one of the alternative methods.
The method of analysis used for this data was a log binomial regression model. One of the reasons is that the objective of this study was determining incidence and estimating the risk ratio of each predictor. The other reason is that the outcome of interest in this study was not rare (23.06%). Log binomial models use a log link function, rather than a logit link, to connect the dichotomous outcome to the linear predictor.46 The log binomial model is given by

where β0, β1, …, βk are the coefficients of the predictor variables X1, X2, …, Xk and k is the number of the predictor variables and p is the proportion of cases who experience aspiration pneumonia. Whereas logistic regression gives odds ratio, the log binomial gives risk ratio which is the appropriate measure of association in a cohort study.43,44,47,48
Estimation of risk ratios using a generalized linear model with a log link and binomial distribution was proposed in 1986 by Wacholder.49 In general, log binomial model is the form given by equation

where π = P (Y = 1) for some binary outcome Y.45 From this model, relative risks are naturally computed as eβjXj and the log binomial regression coefficient β associated with a predictor X is the expected change in log risk or incidence of the outcome per unit change in X. Therefore, increasing the predictor by 1 unit (or going from 1 level to the next) multiplies the risk (incidence) of having the outcome by eβ, which is the antilog of β.
The standard estimation procedure for all generalized linear models is based on maximum likelihood estimation. The maximization technique depends on the way it has been implemented in the software. For example, in STATA there is a convergence tolerance for the coefficient vector and the log-likelihood.
The risk ratio (especially, the crude risk ratio) obtained from log binomial regression through STATA software was crosschecked with risk ratio obtained through another method of analysis. The Hosmer–Lemeshow test was used to test the model goodness of fit and its value was 0.14 for this study. Statistical significance of the association between outcome variable and independent variables was declared when the P-value is less than 5% (0.05).
Ethical Clearance
The ethical review board of the College of Medicine and Health Sciences, Bahir Dar University approved this research protocol. We confirm that all methods were performed in accordance with the relevant guidelines and regulations. The authors confirm that the study complies with the Declaration of Helsinki.
This research was conducted as a requirement for the fulfillment of the Master of Public Health in Epidemiology by Tadios Lidetu. Essey Kebede Muluneh and Gizachew Tadesse Wassie were his thesis advisers. According to Bahir Dar University bylaws theses rated “Very Good” or “Excellent” by internal and external examiners will be uploaded on the university’s repository. This paper was uploaded by Atkilet Beyene ([email protected]) to the Bahir Dar University’s repository as a thesis on 2022-06-15 T07:40:55Z.
https://ir.bdu.edu.et/bitstream/handle/123456789/13756/Tadios%20Lidetu.pdf?sequence=1andisAllowed=y.
Informed Consent
Informed consent was obtained from all subjects.
Results
Socio-Demographic Characteristics of Patients
In this study, 568 charts of adult stroke patients were reviewed. Of those, 342 (60.21%) were males and 226 (39.79%) were females. The median age of the patients was 65 years and the range was 23–115 years. Majority of patients, 438 (77.10%), were from rural areas and more than half of the patients, 335 (58.99%), were farmers. Regarding marital status, two-thirds of the patients were married, 430 (77.70%), and 28 (4.93%) were divorced (Table 1).
 |
Table 1 Socio-Demographic Characteristics of Patients with Stroke at Felege Hiwot Referral Hospital, North-West Ethiopia, July 01, 2009 to June 30, 2021 (N = 568) |
Clinical Characteristics of Patients
Among the 568 patients, 253 (44.54%) had Glasgow Coma scale of greater than 12 and 438 (85.05%) patients had unilateral stroke attack. The predominant stroke type was ischemic, 392 (69.01%), followed by hemorrhagic, 176 (30.99%). Half of the patients had at least one chronic disease such as hypertension, 314 (44.72%), heart disease, 94 (16.15%), and diabetes mellitus, 61 (10.74%). Clinical manifestations that were seen in the stroke patients were vomiting, 206 (36.27%), dysphagia, 244 (39.79%), seizure, 125 (22.01%), and hyperglycemia, 79 (13.91%) (Table 2).
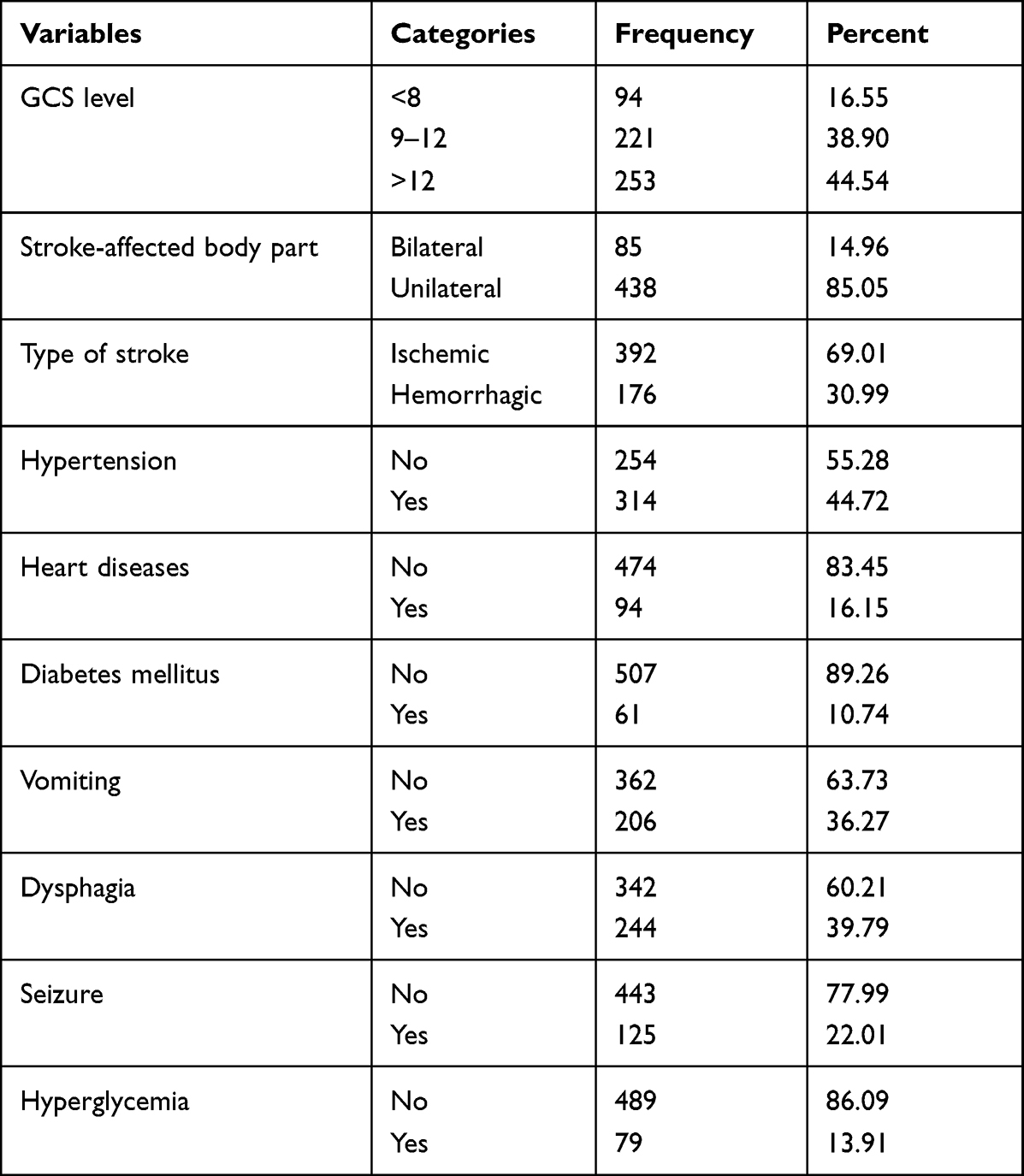 |
Table 2 Clinical Characteristics of Patients with Stroke at Felege Hiwot Referral Hospital, North-West Ethiopia, July 01, 2009 to June 30, 2021 (N = 568) |
Treatment-Related Characteristics of Patients
Among the 568 patients the majority, 543 (95.59%), were treated by non-surgical treatments (medication therapy) and only 25 (4.41%) were treated with surgery. Among medication therapies, aspirin was the most administered, accounting for 413 (72.71%), while warfarin was administered only for 76 (13.38%) patients during the study period. Most patients did not receive antibiotic prophylaxis, 411 (72.36%). Among the 568 patients 180 (31.7%) received oxygen therapy during the study period. Regarding hospital stay, length of hospital stay for 397 (69.89%) patients was 3–7 days and 171 (30.11%) patients stayed for 8–29 days (Table 3).
 |
Table 3 Treatment Related Characteristics of Patients with Stroke at Felege-Hiwot Referral Hospital, North-West Ethiopia, July 01, 2009 to June 30, 2021 (N = 568) |
Incidence of Aspiration Pneumonia
The cumulative incidence (CI) and incidence density rate (IDR) of aspiration pneumonia were 23.06% (95% CI 20–27%) and 38/1000 persons per day observation (95% CI 32/1000 – 45/1000) respectively (Figure 1). Regarding stroke type the incidence of aspiration pneumonia is higher (26.10%) among patients with hemorrhagic type of stroke than patient with ischemic stroke, which accounted for 21.70% (Figure 2).
 |
Figure 1 Incidence of aspiration pneumonia among hospital admitted adult stroke patients at Felege Hiwot Referral Hospital, North-West Ethiopia, from July 2017 to June 2021. |
 |
Figure 2 The incidence of aspiration pneumonia is higher (26.10%) among patients with hemorrhagic type of stroke than patient with ischemic type of stroke (21.70%). |
Predictors of Aspiration Pneumonia
Twenty-eight possible variables believed to be predictors of aspiration pneumonia were entered into the bivariable log binomial regression model. Twenty-two predictors that were significant at the level of significance 0.25 were considered in the multi-variable log binomial regression model and only eight variables (sex, age, GCS level, vomiting, dysphagia, antibiotic prophylaxis, oxygen therapy, and length of hospital stay) were significant at the 0.05 level of significance on the final log binomial regression model.
In this study, 39 (17.3%) female and 92 (26.9%) male patients acquired aspiration pneumonia during the study period. Males were 1.71 times more at risk to develop aspiration pneumonia (ARR = 1.71, 95% CI 1.07–2.74) than females. As age increased by one year the risk of acquiring aspiration pneumonia increased by 4% (ARR = 1.04, 95% 1.01–1.06). Among patients whose GCS level is greater than 12, 34 (13.4%) patients have acquired aspiration pneumonia while 39 (41.5%) of the patients having GCS level less than 8 have acquired aspiration pneumonia during the study period. Patients with GCS level of less than 8 were 2.22 times more at risk to acquire aspiration pneumonia than patients with a GCS level of greater than 12 (ARR = 2.22, 95% CI 1.06–4.55). In this study, 62 (30.1%) of patients with vomiting have developed aspiration pneumonia while 69 (19.1%) patients without vomiting have developed aspiration pneumonia. Patients with vomiting were 1.81 times more at risk to acquire aspiration pneumonia as compared with patients without vomiting (ARR = 1.81, 95% CI 1.04–3.14). During the study period patients with dysphagia were 1.95 times more at risk to acquire aspiration pneumonia as compared with patients without dysphagia (ARR = 1.95, 95% CI 1.10–3.48) (Table 4).
 |
Table 4 Multi-Variable Log Binomial Regression Analysis to the Predictors of Aspiration Pneumonia Among Hospital Admitted Adult Stroke Patients at Felege Hiwot Referral Hospital, North-West Ethiopia, from July 2017 to June 2021 |
Of the patients who received antibiotic prophylaxis only 8 (5.1%) have developed aspiration pneumonia while 123 (29.9%) of the patients who did not receive antibiotic prophylaxis, have developed aspiration pneumonia. Patients who had antibiotic prophylaxis were 90% less at risk to acquire aspiration pneumonia as compared with patients who had not received antibiotic prophylaxis (ARR = 0.10, 95% CI 0.04–0.28). Patients who received oxygen therapy were 3.66 times higher risk to acquire aspiration pneumonia as compared with those patients did not receive oxygen therapy (ARR = 3.66, 95% CI 1.93–6.94). As the length of hospital stay of the patient increased by one day duration in the hospital, the risk of acquired aspiration pneumonia increased by 14% (ARR = 1.14, 95% CI 1.06–1.21). Those significant predictors contributed a favorable impact on post-stroke patients to acquire aspiration pneumonia in the hospital setting (Table 4).
Discussion
This study showed that the cumulative incidence and the incidence density rate of aspiration pneumonia were 131/568 (23.06%) and 38/1000 persons day-observation, respectively. This cumulative incidence was higher than reports from studies conducted in Nigeria (12.40%), China (13.20%), the United Kingdom (7.12%), and USA (5%)12,14,34,50 and less than studies conducted in Egypt (40%) and India (32%).13,18 The discrepancy may be due to the differences in post-stroke patient care and different diagnosis approaches of post-stroke aspiration pneumonia or the study design used.
In this study, the risk of acquiring aspiration pneumonia was significantly higher among males as compared with females. This may be because in the area where this study was conducted, smoking and drinking alcohol to excess is more prevalent among males than females and heavy alcohol consumption may impact on an individual’s ability to fight infection which further increases the risk of aspiration pneumonia.51 This finding was similar with other studies conducted in the United Kingdom and China.37,50
Age is also one of the important factors referred to by most studies. Old age is associated with more severe neurological outcomes, impaired swallowing function, reduced immunity and increased comorbidities. These conditions increase the susceptibilities of the patient for post-stroke aspiration pneumonia. Similar to other studies conducted in other countries,18,52 this study also revealed that the risk of acquired aspiration pneumonia increases when the age of the patient increases.
High Glasgow Coma scale score was negatively associated with aspiration pneumonia, which means that it is protective for aspiration pneumonia in post-stroke adult patients. In this study we found that patients with Glasgow Coma scale greater than 12 had lower risk of acquiring aspiration pneumonia as compared with Glasgow Coma scale less than 8. This finding was similar with a study conducted in Nigeria.14 Low Glasgow Coma scale level was significantly associated with higher risk of aspiration pneumonia, which was due to lack of patient oral care and positioning, because patients with low Glasgow Coma scale level were more susceptible to aspiration that increased the risk of aspiration pneumonia after a stroke episode. Low Glasgow Coma scale level or unconsciousness brings loss of airway reflexes, which are a protective mechanism against aspiration. As a result, patients facing loss of airway reflexes are easily exposed to aspiration and then they develop aspiration pneumonia.
In this and other research in other countries,29,53 patients with vomiting had higher risk to acquire aspiration pneumonia as compared with patients without vomiting. Aspiration pneumonia occurs when food, saliva, liquid, or vomit are breathed into the lungs, instead of being swallowed into the esophagus and stomach. Therefore, when any gastrointestinal system contents enter into the lung, the patients are at higher risk of developing aspiration pneumonia.
Dysphagia is one of the most common clinical factors for aspiration pneumonia because individuals with defective corticodiaphragmatic pathways experience abnormal diaphragmatic motion, which leads to dysphagia. This study revealed that patients with dysphagia had higher risk to acquire aspiration pneumonia compared with patients without dysphagia. As the severity of dysphagia increases, the risk of aspiration pneumonia increases, that is because dysphagia causes allows aspiration of gastrointestinal contents that cause infection of lung/aspiration pneumonia. This finding was in line with other studies conducted in China and Iraq.34,54
In this study, antibiotic prophylaxis showed a negative relationship with aspiration pneumonia. Patients who received antibiotic prophylaxis had lower risk to acquire aspiration pneumonia as compared with patients who had not received antibiotic prophylaxis, implying that antibiotic prophylaxis was protective for aspiration pneumonia. This finding was similar with studies conducted in other countries.40,55
The present study found that oxygen therapy was linked to a high risk of aspiration pneumonia. The risk of acquired aspiration pneumonia was higher in patients who had received oxygen therapy as compared with patients who had not received oxygen therapy. Patients with oxygen therapy are more prone to aspiration/swallowing of either gastrointestinal contents or fluids in the oxygen therapy system to respiratory system, which results in infection that is aspiration pneumonia. This finding is in contradiction with studies conducted in other countries.40,41 The reason of the difference was due to patient clinical status difference, the type of stroke, the ways of oxygen administration to the patients and the clinical setting of health facilities such as treatment modalities.
According to this study, as the length of a patient’s stay in the hospital increases the risk of acquired aspiration pneumonia also increases. If patients stay at hospital for a prolonged time, they might be exposed to sustained prone position that causes aspiration/entrance of gastrointestinal contents to respiratory system, which is capable of inducing aspiration pneumonia. This finding was similar with studies undertaken in Egypt and Indonesia.18,54 From the total of 131 patients who acquired aspiration pneumonia, 54.19% had a hospital stay of more than 7 days, while 45.81% had a hospital stay of less than or equal to 7 days.
In clinical settings, antibiotic prophylaxis, gastro-esophageal reflux therapy, nasogastric tube feeding, and oral care are all significant medical treatments and therapeutic methods for aspiration pneumonia.56 In addition to these in clinical setting, patient care strategies such as positioning, mobilization, close monitoring of stroke patients and adherence to safe swallowing are clinical techniques that should be practiced in health facilities to prevent and decrease the risk of aspiration pneumonia.39
Conclusion
The aim of this study was to determine the incidence and identify predictors of post-stroke aspiration pneumonia. This study showed that the cumulative incidence was 23.06%, with an incidence density rate of 38/1000 persons day-observation. Being male, advanced age, vomiting, a lower Glasgow Coma scale score, dysphagia, long period of hospital stay, and oxygen therapy were risk factors that increase the risk of post-stroke aspiration pneumonia. On the other hand, antibiotic prophylaxis was discovered as a preventive factor that reduces the risk of post-stroke aspiration pneumonia. Patients with vomiting, low Glasgow Coma scale score, and dysphagia problems need to be closely monitored and administered early with anti-emetic medication, with positioning, ABC stabilization, dietary changes, swallowing technique training, and other clinical interventions. Patients with advanced age, particularly males and those spending a longer time in hospital need close monitoring and to receive antibiotic prophylaxis, because their risk of aspiration pneumonia is increased. Preventive measures should be used for patients at risk for aspiration.
Acknowledgments
The authors would like acknowledge the Felege Hiwot Referral Hospital management and staff for providing the data.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
The authors received no external funding for this research.
Disclosure
The authors declare no potential conflicts of interest.
References
1. Mandell LA, Niederman MS, Longo DL. Aspiration pneumonia. N Engl J Med. 2019;380(7):651–663. doi:10.1056/NEJMra1714562
2. Huxley EJ, Viroslav J, Gray WR, et al. Pharyngeal aspiration in normal adults and patients with depressed consciousness. Am J Med. 1978;64(4):564–568. doi:10.1016/0002-9343(78)90574-0
3. Son YG, Shin J, Ryu HG. Pneumonitis and pneumonia after aspiration. J Dental Anesth Pain Med. 2017;17(1):1–12. doi:10.17245/jdapm.2017.17.1.1
4. Hu X, Yi ES, Ryu JH, Seijo L. Aspiration-related deaths in 57 consecutive patients: autopsy study. PLoS One. 2014;9(7):e103795. doi:10.1371/journal.pone.0103795
5. Alexander Makhnevich M, Feldhamer KH, Kast CL, Sinvani L. Aspiration pneumonia. J Hosp Med. 2019;14(7):429–435. doi:10.12788/jhm.3154
6. Mackenzie G. The definition and classification of pneumonia. Pneumonia. 2016;8(1):1–5. doi:10.1186/s41479-016-0012-z
7. Ali A, Howe J, Majid A, et al. The economic cost of stroke-associated pneumonia in a UK setting. Top Stroke Rehabil. 2018;25(3):214–223. doi:10.1080/10749357.2017.1398482
8. Kishore AK, Vail A, Chamorro A, et al. How is pneumonia diagnosed in clinical stroke research? A systematic review and meta-analysis. Stroke. 2015;46(5):1202–1209. doi:10.1161/STROKEAHA.114.007843
9. Chen S, Kent B, Cui Y. Interventions to prevent aspiration in older adults with dysphagia living in nursing homes: a scoping review. BMC Geriatr. 2021;21(1):1–14. doi:10.1186/s12877-021-02366-9
10. Neill S, Dean N. Aspiration pneumonia and pneumonitis: a spectrum of infectious/noninfectious diseases affecting the lung. Curr Opin Infect Dis. 2019;32(2):152–157. doi:10.1097/QCO.0000000000000524
11. Gadisa DA, Busawa G, Gebremariam E, et al. Clinical characteristics, treatment outcomes, and its predictors among hospitalized stroke patients in Ambo University Referral Hospital, West Ethiopia: a retrospective hospital-based study. Vasc Health Risk Manag. 2020;16:591. doi:10.2147/VHRM.S287465
12. Watila MM, Nyandaiti YW, Balarabe SA, Bakki B, Alkali NH, Ibrahim A, Tonde EG, Chiroma I. Aspiration pneumonia in patients with stroke in Northeast Nigeria. Int J Stroke. 2013;8(4):E16.
13. Pacheco-Castilho AC, Vanin GDM, Dantas RO, et al. Dysphagia and associated pneumonia in stroke patients from Brazil: a systematic review. Dysphagia. 2019;34(4):499–520. doi:10.1007/s00455-019-10021-0
14. Chang C-Y, Cheng T-J, Lin C-Y, et al. Reporting of aspiration pneumonia or choking as a cause of death in patients who died with stroke. Stroke. 2013;44(4):1182–1185. doi:10.1161/STROKEAHA.111.000663
15. Cacha Villanueva DV. Riesgo de Neumonía que requiere hospitalización en pacientes post accidente Cerebrovascular en el Hospital de Chancay 2017–2019. Int J Med Res Prof. 2016. Available from: http://repositorio.unjfsc.edu.pe/handle/UNJFSC/3970
16. Ibrahim A, Tonde EG, Chiroma I. Aspiration pneumonia in patients with stroke. In: International Journal of Stroke © 2013. World Stroke Organization; 2013:8.
17. Russell JBW, Charles E, Conteh V, et al. Risk factors, clinical outcomes and predictors of stroke mortality in Sierra Leoneans: a retrospective hospital cohort study. Ann Med Surg. 2020;60:293–300. doi:10.1016/j.amsu.2020.10.060
18. Belal ES, Selim S, Mohammad A, Mohammad A. Detection of airway protective level of the cough reflex in acute stroke patients. Egyptian J Neurol Psychiatry Neurosur. 2020;56(1):1–6. doi:10.1186/s41983-020-0157-9
19. Yu KJ, Moon H, Park D. Different clinical predictors of aspiration pneumonia in dysphagic stroke patients related to stroke lesion: a STROBE-complaint retrospective study. Medicine. 2018;97(52):e13968. doi:10.1097/MD.0000000000013968
20. Schallom M, Dykeman B, Metheny N, et al. Head-of-bed elevation and early outcomes of gastric reflux, aspiration and pressure ulcers: a feasibility study. Am J Crit Care. 2015;24(1):57–66. doi:10.4037/ajcc2015781
21. Metheny NA. Risk factors for aspiration. J Parent Enter Nutr. 2002;26:S26–S33. doi:10.1177/014860710202600605
22. Watila MM, Nyandaiti YW, Balarabe SA, et al. Aspiration pneumonia in patients with stroke, northeast Nigeria. Natl J Neurol. 2013;3:48–55.
23. Cichero JA. Age-related changes to eating and swallowing impact frailty: aspiration, choking risk, modified food texture and autonomy of choice. Geriatrics. 2018;3(4):69. doi:10.3390/geriatrics3040069
24. Li Y, Song B, Fang H, et al. Risk factors for stroke-associated pneumonia in a Chinese population: a prospective cohort study. Life Sci J. 2014;11(6):378–382.
25. Benfield J, Michou E. Dysphagia screening and assessment in the stroke unit. Br J Neurosci Nurs. 2016;12(Sup2):S24–S28. doi:10.12968/bjnn.2016.12.Sup2.S24
26. Won JH, Byun SJ, Oh B-M, et al. Risk and mortality of aspiration pneumonia in Parkinson’s disease: a nationwide database study. Sci Rep. 2021;11(1):6597. doi:10.1038/s41598-021-86011-w
27. Manabe T, Teramoto S, Tamiya N, et al. Risk factors for aspiration pneumonia in older adults. PLoS One. 2015;10(10):e0140060. doi:10.1371/journal.pone.0140060
28. Li Y, Zhang X, Sang H, et al. Urban-rural differences in risk factors for ischemic stroke in northern China. Medicine. 2019;98(21):e15782.
29. de Souza Oliveira AR, Costa AGDS, Morais HCC, et al. Clinical factors predicting risk for aspiration and respiratory aspiration among patients with Stroke. Rev Lat Am Enfermagem. 2015;23(2):216–224. doi:10.1590/0104-1169.0197.2545
30. Kiconco G, Turyasiima M, Ndamira A, et al. Prevalence and associated factors of pneumonia among under-fives with acute respiratory symptoms: a cross sectional study at a Teaching Hospital in Bushenyi District, Western Uganda. Afr Health Sci. 2021;21(4):1701–1710. doi:10.4314/ahs.v21i4.25
31. Mi T, Sun S, Du Y, et al. Differences in the distribution of risk factors for stroke among the high‐risk population in urban and rural areas of Eastern China. Brain Behav. 2016;6(5):e00461. doi:10.1002/brb3.461
32. Orso D, Vetrugno L, Federici N, et al. Endotracheal intubation to reduce aspiration events in acutely comatose patients: a systematic review. Scand J Trauma Resusc Emerg Med. 2020;28(1):1–10. doi:10.1186/s13049-020-00814-w
33. Ali KM, Muhammad AS, Nafee R, Amin IH. Aspiration pneumonia in acute stroke patients in Sulaimani City-Iraq. Int J Med Res Prof. 2016;2(2):113–118.
34. Matsumura T, Mitani Y, Oki Y, et al. Risk factors for the onset of aspiration pneumonia among stroke patients in the recovery stage. Nihon Ronen Igakkai zasshi. 2014;51(4):364–368. doi:10.3143/geriatrics.51.364
35. Lee KB, Lim SH, Park G-Y, et al. Effect of brain lesions on voluntary cough in patients with supratentorial stroke: an observational study. Brain Sci. 2020;10(9):627. doi:10.3390/brainsci10090627
36. Li -C-C, Oreská S, Špiritović M, et al. Risk and outcomes of diabetes in patients with epilepsy. Sci Rep. 2021;11(1):1–7. doi:10.1038/s41598-020-79139-8
37. Li Y, Zhang Y, Ma L, et al. Risk of stroke-associated pneumonia during hospitalization: predictive ability of combined A 2 DS 2 score and hyperglycemia. BMC Neurol. 2019;19(1):1–7. doi:10.1186/s12883-019-1497-x
38. van der Maarel-Wierink CD, Vanobbergen JNO, Bronkhorst EM, et al. Meta-analysis of dysphagia and aspiration pneumonia in frail elders. J Dent Res. 2011;90(12):1398–1404. doi:10.1177/0022034511422909
39. Eltringham SA, Kilner K, Gee M, et al. Factors associated with risk of stroke-associated pneumonia in patients with dysphagia: a systematic review. Dysphagia. 2020;35(5):735–744. doi:10.1007/s00455-019-10061-6
40. Warusevitane A, Karunatilake D, Sim J, et al. Safety and effect of metoclopramide to prevent pneumonia in patients with stroke fed via nasogastric tubes trial. Stroke. 2015;46(2):454–460. doi:10.1161/STROKEAHA.114.006639
41. Collins J, Rybinnik I, Fischberg B, et al. Stroke, oxygen and prehospital care: a commentary on current treatments and opportunities for improvement. J Exp Neurol. 2021;2(1):39.
42. Wang Q, Liu Y, Han L, et al. Risk factors for acute stroke-associated pneumonia and prediction of neutrophil-to-lymphocyte ratios. Am J Emerg Med. 2021;41:55–59. doi:10.1016/j.ajem.2020.12.036
43. Fekedulegn D, Andrew M, Violanti J, et al. Comparison of statistical approaches to evaluate factors associated with metabolic syndrome. J Clin Hyperten. 2010;12(5):365–373. doi:10.1111/j.1751-7176.2010.00264.x
44. Chen W, Qian L, Shi J, et al. Comparing performance between log-binomial and robust Poisson regression models for estimating risk ratios under model misspecification. BMC Med Res Methodol. 2018;18(1):1–12. doi:10.1186/s12874-018-0519-5
45. Williamson TS, Sy S, Ugarte-Torres A. Log-binomial models: maximum Likelihood and failed convergence. Leukemia. 2011;26(2):359–362. doi:10.1038/leu.2011.195
46. Williamson T, Eliasziw M, Fick GH. Log-binomial models: exploring failed convergence. Emerg Themes Epidemiol. 2013;10(1):1–10. doi:10.1186/1742-7622-10-14
47. McNutt L-A, Wu C, Xue X, Hafner JP. Estimating the relative risk in cohort studies and clinical trials of common outcomes. Am J Epidemiol. 2003;157(10):940–943. doi:10.1093/aje/kwg074
48. Blizzard L, Hosmer W. Parameter estimation and goodness‐of‐fit in log binomial regression. Biometr J. 2006;48(1):5–22. doi:10.1002/bimj.200410165
49. Wacholder S. Binomial regression in GLIM: estimating risk ratios and risk differences. Am J Epidemiol. 1986;123(1):174–184. doi:10.1093/oxfordjournals.aje.a114212
50. Teh W-H, Smith CJ, Barlas RS, et al. Impact of stroke‐associated pneumonia on mortality, length of hospitalization, and functional outcome. Acta Neurol Scand. 2018;138(4):293–300. doi:10.1111/ane.12956
51. Gluckman SJ, Dvorak VC, MacGregor RR. Host defenses during prolonged alcohol consumption in a controlled environment. Arch Intern Med. 1977;137(11):1539–1543. doi:10.1001/archinte.1977.03630230033011
52. Prust ML, Saylor D, Zimba S, et al. Inpatient management of acute stroke of unknown type in resource-limited settings. Stroke. 2022;53(3). doi:10.1161/STROKEAHA.121.037297
53. Quyet D, Hien NM, Khan MX, et al. Risk factors for stroke associated pneumonia. Open Access Macedon J Med Sci. 2019;7(24):4416. doi:10.3889/oamjms.2019.873
54. Widyantara IW, Purwata TE, Putra IB, et al. Factors that affecting the event of pneumonia in stroke patients treated in the intensive space of Sanglah Denpasar hospital. Int J Med Rev Case Rep. 2020;4(4):6–10.
55. El Solh AA, Saliba R. Pharmacologic prevention of aspiration pneumonia: a systematic review. Am J Geriatr Pharmacother. 2007;5(4):352–362. doi:10.1016/j.amjopharm.2007.12.005
56. Beavan J. Update on management options for dysphagia after acute stroke. Br J Neurosci Nurs. 2015;11(Sup2):10–19. doi:10.12968/bjnn.2015.11.Sup2.10
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.