Back to Journals » Orthopedic Research and Reviews » Volume 15
Incidence and Distribution of Deep Vein Thrombosis Following Total Hip Arthroplasty Using an Anterolateral Supine Approach
Authors Itou J ![]() , Munakata Y, Kuramitsu Y, Madarame H, Okazaki K
, Munakata Y, Kuramitsu Y, Madarame H, Okazaki K ![]()
Received 11 July 2023
Accepted for publication 21 September 2023
Published 3 November 2023 Volume 2023:15 Pages 199—205
DOI https://doi.org/10.2147/ORR.S430145
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Clark Hung
Junya Itou, Yutaro Munakata, Yujiro Kuramitsu, Hiromi Madarame, Ken Okazaki
Department of Orthopaedic Surgery, Tokyo Women’s Medical University, Tokyo, Japan
Correspondence: Ken Okazaki, Department of Orthopaedic Surgery, Tokyo Women’s Medical University, 8-1 Kawada-cho, Shinjuku-ku, Tokyo, 162-8666, Japan, Tel +81-3-3353-8111, Fax +81-3-5269-7618, Email [email protected]
Purpose: Venous thromboembolism (VTE) is a potential major complication in patients undergoing total hip arthroplasty (THA). However, the incidence of VTE following THA using anterolateral supine approach (ALS) has not been reported. The purpose of this study was to investigate the incidence of perioperative VTE and the distribution and characteristics of deep vein thrombosis (DVT) following ALS THA.
Patients and Methods: This retrospective single-arm study analyzed the 182 consecutive hips of 164 patients who underwent primary ALS THA. Pharmacological prophylaxis consisted of enoxaparin 20 mg twice daily for approximately 6 days starting 24 h postoperatively until duplex ultrasonography was performed to determine whether postoperative DVT was present. DVT was assessed by whole-leg Doppler ultrasound, and the location and characteristics of any thrombus were recorded. If pulmonary thromboembolism was suspected, contrast-enhanced computed tomography was performed.
Results: The overall incidence of VTE was 9.9% for DVT (18/182 hips) and 0.5% for pulmonary thromboembolism (1/182 hips). Most DVTs were in the soleal vein on the affected side and showed isoechoic or hypoechoic echogenicity. All thrombi were non-floating.
Conclusion: Following ALS THA with standard pharmacological prophylaxis and an early weight-bearing protocol, the incidence of perioperative DVT was approximately 10%, mostly occurring in the lower leg.
Keywords: anterolateral supine approach, deep vein thrombosis, pulmonary thromboembolism, total hip arthroplasty, venous thromboembolism
Introduction
Venous thromboembolism (VTE) is a potential major complication in patients undergoing total hip arthroplasty (THA). VTE consists of deep vein thrombosis (DVT) and pulmonary embolism (PE).1 It is well known that postoperative immobility is a risk factor for DVT following THA.2 Therefore, early ambulation is recommended.
Although a posterior surgical approach has often been used, an anterior approach is now preferred because it is associated with less soft tissue damage.3 Both the direct anterior approach (DAA) and the anterolateral supine approach (ALS) are intermuscular anterior approaches4–7 that are expected to allow early recovery, which may be beneficial for preventing postoperative DVT. The ALS technique is an intermuscular approach that enters between the gluteus medius and the tensor facia latae.4–6 Indeed, Zeng et al8 reported that the incidence of DVT in patients who have undergone DAA THA was 0%. However, one of the limitations of their study was that the imaging tests are often focused on symptomatic patients, and asymptomatic patients are missed. In addition, to our knowledge, the incidence of DVT following ALS THA has not been reported.
Furthermore, there was a problem with the previous reports regarding the diagnosis of DVT. The DVT detection rate is lower when contrast-enhanced computed tomography (CT) or contrast venography is used as the detection method.9 On the other hand, it is well known that Doppler ultrasound is a useful initial investigation for the diagnosis of DVT following THA.
The purpose of this study was to investigate the incidence of perioperative VTE following ALS THA and the distribution and characteristics of DVT using Doppler ultrasound.
Materials and Method
Patient Eligibility and Selection
This was a retrospective single-arm study that involved 270 consecutive hips of 224 patients who underwent primary ALS THA at our institution between January 2019 and June 2022. D-dimer plasma levels were assessed preoperatively to rule out DVT. All patients received a combination of physical and pharmacological prophylaxis. Standard physical prophylaxis consisted of use of elastic stockings and an intermittent pneumatic compression device in the early postoperative period. Pharmacological prophylaxis consisted of administration of enoxaparin 20 mg twice daily for approximately 6 days starting 24 h postoperatively and continued until duplex ultrasonography was performed to determine whether postoperative DVT was present. Of the 270 consecutive hips, 88 were excluded for the following reasons: THA was performed for a femoral neck or acetabular fracture (n = 12); history of antiplatelet agent or anticoagulant use (n = 60), and bleeding risk (n = 16). Bleeding risk was defined as a history of peptic ulcer, hemostatic disorder, or current severe renal dysfunction. Finally, 182 hips were included in the study (Figure 1). The patients comprised 134 women and 30 men with a median age of 60.5 [50.7–73.0] years. The median body mass index was 23.5 [20.4–26.1]. Preoperative diagnoses were hip dysplasia, avascular necrosis of the femoral head, rheumatoid arthritis, primary/secondary osteoarthritis of the hip, rapidly destructive coxopathy, and subchondral insufficiency fracture of the femoral head. There were 18 patients (36 hips) who underwent 1-stage bilateral THA. The median operation time was 77.7 [65.0–102.2] min with a median intraoperative blood loss of 235 [124.7–375.0] mL (Table 1).
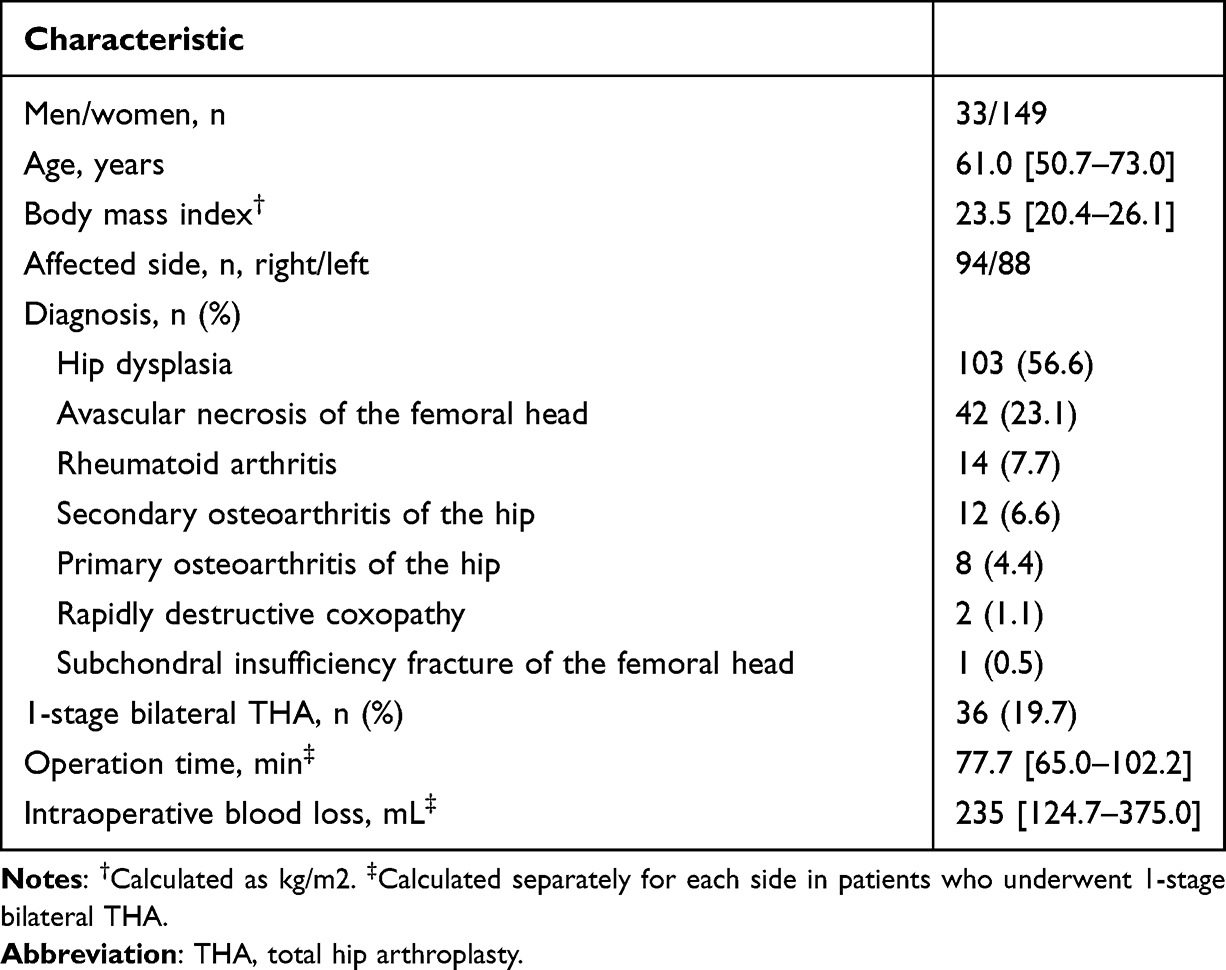 |
Table 1 Patient Demographic Characteristics |
 |
Figure 1 Flowchart for the current retrospective study showing the cohort of patients following ALS THA at our institution. |
Surgical Technique and Rehabilitation
The surgical procedures were performed by either of 2 specialist hip surgeons (Y.M., Y.K.) with attention paid to consistency of surgical technique and intraoperative management across cases. All surgeries were performed via ALS. The decision to perform 1-stage bilateral THA was based on the patient’s demographic and clinical characteristics.10 The iliofemoral ligament, conjoint tendon, and anterior capsule were preserved. Cementless acetabular and femoral components were used. No postoperative drainage tube was placed. Tranexamic acid 1000 mg was administered intravenously before the surgical time-out. All surgeries were performed under general anesthesia, with regional anesthesia added under ultrasound guidance11 at the discretion of the anesthesiologist. Patients were allowed to ambulate with full weight bearing as pain permitted from the day following surgery and underwent rehabilitation without restriction of range of motion.
Assessment for VTE
Doppler ultrasound was performed in all patients on postoperative day 7 to determine whether postoperative DVT was present. DVT was assessed by whole-leg Doppler ultrasound,12–14 and the location and characteristics of any thrombus were recorded. Proximal DVT was defined as DVT occurring in the popliteal vein or above. If multiple thrombi were found in the same case, each location was counted. Echogenicity (hyperechoic, isoechoic, hypoechoic) and whether the thrombus was attached to the vein wall or free-floating were also investigated. All Doppler ultrasound procedures were performed by the same team of ultrasonographers, all of whom were non-physicians. Whereas the gold standard for diagnosing DVT has historically been conventional contrast venography, venography is an invasive procedure and is not advised for those who have kidney disease or an allergy to the contrast agent.9 Therefore, Duplex ultrasound was chosen for this study.
Pharmacological prophylaxis was discontinued if Doppler ultrasound revealed no DVT. Apixaban was administered to patients in whom Doppler ultrasound revealed signs of DVT unless contraindicated. Contrast-enhanced CT was performed if PE was suspected based on clinical findings, such as chest pain, shortness of breath, and desaturation.
Assessment for Complications
Complications were assessed retrospectively by review of the medical records. Complications related to pharmacological prophylaxis were defined as major bleeding (death or a life-threatening clinical event), minor bleeding (an overt bleeding episode that did not meet the criteria for major bleeding),15 and additional wound procedures. Surgical complications, such as superficial and deep wound infections, periprosthetic fractures, nerve lesions, dislocation, and revision THA, were also assessed.6
Ethical Approval
This study was approved by the institutional review board of Tokyo Women’s Medical University (approval number 5280). Informed consent was obtained via the opt-out method. All procedures involving human participants were in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments.
Statistical Analysis
Descriptive statistics are reported as the median (range) or count (percentage) or as the mean and standard deviation. Categorical variables were examined using Fisher’s exact test. All statistical analyses were performed using JMP software version 16 (SAS Institute Inc., Cary, NC). A p-value < 0.05 was considered statistically significant.
Results
Incidence of VTE
The overall incidence of VTE was 9.9% for DVT (18/182 hips) and 0.5% for PE (1/182 hips, Table 1). There was no significant difference in the incidence of DVT between 1-stage bilateral THA and unilateral THA (p = 0.73, Table 2).
 |
Table 2 Incidence of Deep Vein Thrombosis in the 2 Groups |
One patient with PE was a 71-year-old woman with a diagnosis of avascular necrosis of the femoral head and a body mass index of 30.6 who underwent ALS THA. The operation time was 78 min and blood loss during surgery was 230 mL. She had symptoms of respiratory distress from the day after surgery and received oxygen therapy, but with limited improvement. A contrast-enhanced CT scan performed on postoperative day 3 revealed a proximal (common femoral vein) to distal (soleal vein) continuous isoechoic non-floating thrombus that was treated with apixaban by cardiologists. The patient was finally discharged home.
Distribution and Characteristics of DVTs
Table 3 show the details of the postoperative DVTs, all of which were asymptomatic, except for patient 2. Most DVTs were in the soleal vein on the affected side and had isoechoic or hypoechoic echogenicity. All thrombi were non-floating.
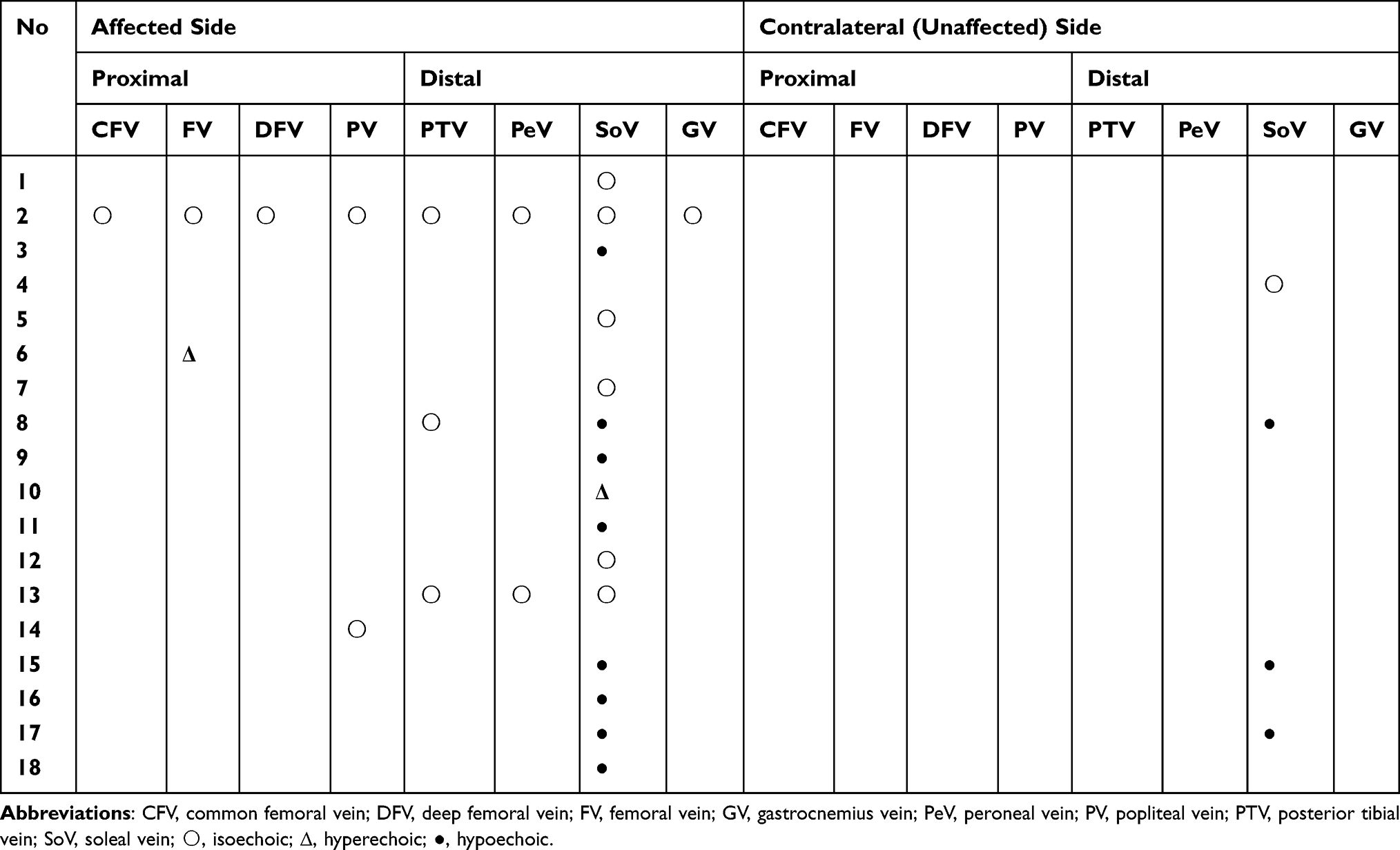 |
Table 3 Comparison of the Distribution of DVT and Echogenicity in the Veins of the Lower Extremities in the 2 Groups |
Complications
There were no major/minor bleeding episodes, and no additional wound procedures were required.
Intraoperative periprosthetic femoral fractures occurred in 17 hips and intraoperative periprosthetic acetabular fractures in 2 (Table 4). Although 5 intraoperative calcar fractures were managed with a cable at the level of the lesser trochanter,16 the remaining 12 non-displaced greater trochanter fractures were left without fixation. The 2 hips with intraoperative periprosthetic acetabular fractures did not undergo additional fixation. Partial weight bearing was performed in 7 cases evaluated as unstable with or without use of a cable. Of these 7 hips, 2 had postoperative DVT. Otherwise, there were no changes in postoperative rehabilitation, and no cases required additional surgery.
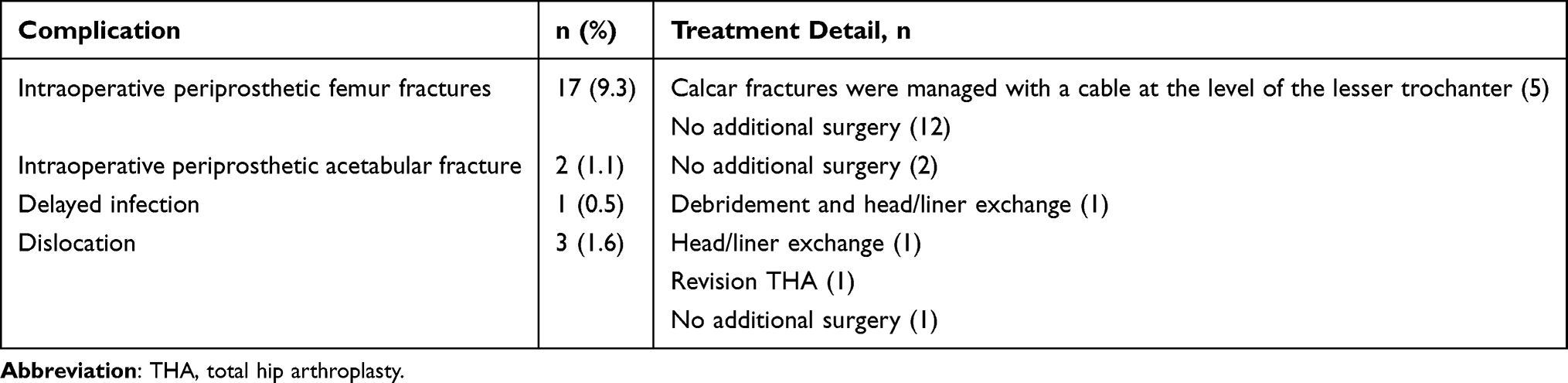 |
Table 4 Details of Complications |
There was 1 case of delayed infection via hematogenous spread in a patient with appendicitis and 3 cases of dislocation of the THA. The treatment details for each case are shown in Table 4.
Discussion
To our knowledge, this is the first study to evaluate the incidence of VTE following ALS THA. On pharmacological prophylaxis with enoxaparin, the incidence of DVT was 9.9% and that of PE was 0.5%. The strength of this study is that all cases were investigated using Doppler ultrasound and a detailed thrombus evaluation was performed. Previous studies have reported that the incidence of asymptomatic DVT following THA using the posterior approach ranged from 11.1 to 28.2%.17–20 The incidence of postoperative VTE was lower in ALS THA than in the conventional posterior approach, suggesting that ALS approach is effective with respect to the risk of asymptomatic DVT.
Unlike the posterior approach, ALS has the advantage of being an intermuscular approach, which allows early recovery.4,21 It has been reported that patients who undergo ALS THA have a shorter hospital stay3 and start using a cane earlier than their counterparts in whom a posterior approach is used.4 Other advantages in terms of decreasing the incidence of VTE include the fact that ALS THA is performed in the supine position, unlike the posterior approach, and does not require flexion and adduction during hip dislocation, which would prevent venous flow.8,22 A previous study found lower VTE incidence rates after DAA THA (DVT, 0%; PE, 0.5%).8 However, that study had a weakness in that they diagnosed DVT based only on clinical suspicion. Therefore, the actual incidence of DVT after DAA THA was likely to be slightly higher in their patients. In another study, asymptomatic DVT occurred in 2.8% of patients after DAA THA.23 Although no direct comparison has been performed, the incidence of DVT/PE in ALS and DAA approaches may be less than that in the posterior approach.
It is well known that VTE following THA is associated with multiple factors. In their systematic review, Zhang et al stated that potential risk factors for VTE following THA could be divided into several types, including demographic factors, clinical factors, health care provider-related factors, and thromboprophylaxis.24 Demographic factors include age, sex, obesity,25 and ethnicity,9,26 while clinical factors include underlying diagnosis, comorbidity, and medication. Comorbidity may include factors such as diabetes mellitus, history of VTE, and malignancy. However, considering all these factors and making comparisons would require a large number of eligible patients and be difficult to perform. Moreover, the clinical significance of the results obtained is small, given that the incidence of VTE following THA can be predicted to some extent.9,26 Therefore, it may be better to perform more cohort studies like the present study so that a meta-analysis may be performed in the future.
Given its invasiveness, 1-stage bilateral THA is thought to be associated with a higher incidence of VTE. However, this was not the case in our present study. Shao et al also found that the risk of VTE was lower after 1-stage bilateral THA than after 2-stage bilateral THA.27 Total operation time and blood loss may be associated with the occurrence of VTE,7,10 but no such associations were found in our study.
To our knowledge, there have been no previous published comparisons of the location or quality of thrombus in patients undergoing ALS THA. Most of the DVTs in our study were located in the soleal vein on the affected side. It is widely known that DVT develops in the soleal vein because of stasis of blood flow.18 However, we identified several cases of distal DVT in the contralateral lower extremity. Thus, it would be better to include both lower extremities when screening for DVT by Doppler ultrasound. Considering that Doppler ultrasound is non-invasive and has high sensitivity and specificity for the diagnosis of DVT,9 it could be used to clarify the actual incidence of DVT, including asymptomatic cases, when THA is performed using an ALS approach. As reported by Zeng et al.8 Doppler ultrasound performed based on clinical suspicion is certainly reasonable in practice, but it cannot assess the actual incidence of DVT. Of course, there is still controversy as to whether acute isolated distal DVT found incidentally warrants treatment.28,29 However, accurate assessment and diagnosis of DVT is essential as a basis for this discussion.
This study had several limitations. First, it had a retrospective single-arm design, which means that there was a possibility of patient selection bias. Furthermore, ethnic and cultural differences may have affected the results. In general, the incidence of VTE has been shown to be lower in Asian countries than in Western countries.26 Therefore, care is needed when extrapolating the results of this study to other populations and institutions. Second, the sample size was small. Third, only enoxaparin was used for pharmacological prophylaxis. However, enoxaparin has been widely used for pharmacological prophylaxis following total joint arthroplasty.13,14,29 Fourth, DVTs that developed after postoperative day 7 may have been undetected. It has been reported that most asymptomatic DVTs following THA occur in the first 4 postoperative days.17 Therefore, the assessment of DVT by Doppler ultrasound was appropriately timed.
Conclusion
This study retrospectively investigated the incidence of perioperative VTE and the distribution and characteristics of DVT in patients who underwent ALS THA with pharmacological prophylaxis. The overall incidence of DVT was 9.9% and that of PE was 0.5%. Although no direct comparison has been performed, the incidence of DVT/PE in ALS approach may be less than that in the posterior approach.
Acknowledgments
We thank ThinkSCIENCE, Tokyo, Japan, for English language editing.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zeng Y, Si H, Wu Y, et al. The incidence of symptomatic in-hospital VTEs in Asian patients undergoing joint arthroplasty was low: a prospective, multicenter, 17,660-patient-enrolled cohort study. Knee Surg Sports Traumatol Arthrosc. 2019;27(4):1075–1082. doi:10.1007/s00167-018-5253-3
2. White RH, Henderson MC. Risk factors for venous thromboembolism after total Hip and knee replacement surgery. Curr Opin Pulm Med. 2002;8:365–371. doi:10.1097/00063198-200209000-00004
3. Higgins BT, Barlow DR, Heagerty NE, Lin TJ. Anterior vs. posterior approach for total Hip arthroplasty, a systematic review and meta-analysis. J Arthroplasty. 2015;30:419–434. doi:10.1016/j.arth.2014.10.020
4. Ukai T, Ebihara G, Watanabe M. Comparison of short-term outcomes of anterolateral supine approach and posterolateral approach for primary total Hip arthroplasty: a retrospective study. J Orthop Traumatol. 2021;22:6. doi:10.1186/s10195-021-00570-2
5. Munakata Y, Kuramitsu Y, Usui Y, Okazaki K. Comparison of radiographic changes in rectangular curved short stem with thin versus thick porous coating for cementless total Hip arthroplasty: a retrospective study with a propensity score matching. J Orthop Surg Res. 2021;16:247. doi:10.1186/s13018-021-02397-3
6. Luger M, Hochgatterer R, Schopper C, et al. Obesity in short stem total Hip arthroplasty using a minimally invasive supine anterolateral approach-a risk factor for short-term complications? Int Orthop. 2021;45:2833–2841. doi:10.1007/s00264-021-05079-1
7. Lanting BA, Odum SM, Cope RP, Patterson AH, Masonis JL. Incidence of perioperative events in single setting bilateral direct anterior approach total Hip arthroplasty. J Arthroplasty. 2015;30:465–467. doi:10.1016/j.arth.2014.09.021
8. Zeng GJ, Xu S, Pang HN. Incidence of deep vein thrombosis and pulmonary embolism in Asian patients after direct anterior total Hip arthroplasty. J Orthop. 2020;21:528–531. doi:10.1016/j.jor.2020.08.027
9. Ngarmukos S, Kim KI, Wongsak S, et al. Asia-Pacific venous thromboembolism consensus in knee and Hip arthroplasty and Hip fracture surgery: part 1. Diagnosis and risk factors. Knee Surg Relat Res. 2021;33:18. doi:10.1186/s43019-021-00099-y
10. Macaulay W, Salvati EA, Sculco TP, Pellicci PM. Single-stage bilateral total Hip arthroplasty. J Am Acad Orthop Surg. 2002;10(3):217–221. doi:10.5435/00124635-200205000-00008
11. Wang X, Sun Y, Wang L, Hao X. Femoral nerve block versus fascia iliaca block for pain control in total knee and Hip arthroplasty: a meta-analysis from randomized controlled trials. Medicine. 2017;96(27):e7382. doi:10.1097/MD.0000000000007382
12. Guyatt GH, Norris SL, Schulman S, et al. Methodology for the development of antithrombotic therapy and prevention of thrombosis guidelines: antithrombotic therapy and prevention of thrombosis, 9th ed: American College Of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:53S–70S. doi:10.1378/chest.11-2288
13. Itou J, Kuwashima U, Itoh M, Okazaki K. No difference in the incidence or location of deep venous thrombosis according to use of pharmacological prophylaxis following total knee arthroplasty. BMC Musculoskelet Disord. 2021;22:819. doi:10.1186/s12891-021-04707-6
14. Itou J, Kuwashima U, Itoh M, Okazaki K. Robotic-assisted total knee arthroplasty is not associated with increased risk of postoperative deep vein thrombosis. J Exp Orthop. 2023;10(1):65. doi:10.1186/s40634-023-00628-6
15. Colwell CW, Collis DK, Paulson R, et al. Comparison of enoxaparin and warfarin for the prevention of venous thromboembolic disease after total Hip arthroplasty. Evaluation during hospitalization and three months after discharge. J Bone Joint Surg Am. 1999;81:932–940. doi:10.2106/00004623-199907000-00005
16. Siddiqi A, Springer BD, Chen AF, Piuzzi NS. Diagnosis and management of intraoperative fractures in primary total Hip arthroplasty. J Am Acad Orthop Surg. 2021;29:e497–e512. doi:10.5435/JAAOS-D-20-00818
17. Yamaguchi T, Hasegawa M, Niimi R, Sudo A. Incidence and time course of asymptomatic deep vein thrombosis with fondaparinux in patients undergoing total joint arthroplasty. Thromb Res. 2010;126:e323–326. doi:10.1016/j.thromres.2010.03.018
18. Abe K, Yuda S, Yasui K, et al. Soleal vein dilatation assessed by ultrasonography is an independent predictor for deep vein thrombosis after major orthopedic surgery. J Cardiol. 2017;69:756–762. doi:10.1016/j.jjcc.2016.07.004
19. Kim YH, Park JW, Kim JS. Chemical thromboprophylaxis is not necessary to reduce risk of thromboembolism with tranexamic acid after total Hip arthroplasty. J Arthroplasty. 2017;32:641–644. doi:10.1016/j.arth.2016.07.048
20. Imai N, Dohmae Y, Suda K, Miyasaka D, Ito T, Endo N. Tranexamic acid for reduction of blood loss during total Hip arthroplasty. J Arthroplasty. 2012;27:1838–1843. doi:10.1016/j.arth.2012.04.024
21. Wang Z, Hou JZ, Wu CH, et al. A systematic review and meta-analysis of direct anterior approach versus posterior approach in total Hip arthroplasty. J Orthop Surg Res. 2018;13:229. doi:10.1186/s13018-018-0929-4
22. Binns M, Pho R. Femoral vein occlusion during Hip arthroplasty. Clin Orthop Relat Res. 1990;255:168–172.
23. Zha GC, Zhu XR, Wang L, Li HW. Tranexamic acid reduces blood loss in primary total Hip arthroplasty performed using the direct anterior approach: a one-center retrospective observational study. J Orthop Traumatol. 2022;23:12. doi:10.1186/s10195-022-00638-7
24. Zhang ZH, Shen B, Yang J, Zhou ZK, Kang PD, Pei FX. Risk factors for venous thromboembolism of total Hip arthroplasty and total knee arthroplasty: a systematic review of evidences in ten years. BMC Musculoskelet Disord. 2015;16:24. doi:10.1186/s12891-015-0470-0
25. Sloan M, Sheth N, Lee GC. Is obesity associated with increased risk of deep vein thrombosis or pulmonary embolism after Hip and knee arthroplasty? A large database study. Clin Orthop Relat Res. 2019;477:523–532. doi:10.1097/CORR.0000000000000615
26. Kanchanabat B, Stapanavatr W, Meknavin S, Soorapanth C, Sumanasrethakul C, Kanchanasuttirak P. Systematic review and meta-analysis on the rate of postoperative venous thromboembolism in orthopaedic surgery in Asian patients without thromboprophylaxis. Br J Surg. 2011;98:1356–1364. doi:10.1002/bjs.7589
27. Shao H, Chen CL, Maltenfort MG, Restrepo C, Rothman RH, Chen AF. Bilateral total Hip arthroplasty: 1-stage or 2-stage? A meta-analysis. J Arthroplasty. 2017;32:689–695. doi:10.1016/j.arth.2016.09.022
28. Kearon C, Akl EA, Comerota AJ, et al. Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141:e419S–e496S. doi:10.1378/chest.11-2301
29. Sidhu VS, Kelly T-L, Pratt N, et al. Effect of aspirin vs enoxaparin on symptomatic venous thromboembolism in patients undergoing Hip or knee arthroplasty. JAMA. 2022;328:719–727. doi:10.1001/jama.2022.13416
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Venous Thromboembolism Among Hospitalized Patients: Incidence and Adequacy of Thromboprophylaxis – A Retrospective Study
Ambra N, Mohammad OH, Naushad VA, Purayil NK, Mohamedali MG, Elzouki AN, Khalid MK, Illahi MN, Palol A, Barman M, Sharif M, Chalihadan S, Punnorath A, Mostafa A, Al Hariri B, Khidir TGM, Varikkodan I
Vascular Health and Risk Management 2022, 18:575-587
Published Date: 24 July 2022
Thromboprophylaxis in Patients Admitted to the Surgical Ward: Clinical Audit
Abdalla YA, Kamil AM, Mohamed SAA, Mohamed AHA, Khalifa E, Mohamed MHA, Abdelgadir EEA, Dabora M, Awoda MSEME
Vascular Health and Risk Management 2023, 19:651-656
Published Date: 22 September 2023