Back to Journals » Breast Cancer: Targets and Therapy » Volume 17
Inavolisib-Based Therapy for PIK3CA-Mutated Advanced Male Breast Cancer: A Cost-Effectiveness Analysis
Authors Huang X, Lin S, Lin R, Luo S, Huang P, Zeng D
Received 25 September 2025
Accepted for publication 17 December 2025
Published 26 December 2025 Volume 2025:17 Pages 1385—1396
DOI https://doi.org/10.2147/BCTT.S566088
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Pranela Rameshwar
Xiaoting Huang,1,2,* Shen Lin,1,2,* Rongfang Lin,1,2 Shaohong Luo,1,2 Pinfang Huang,1,2 Dayong Zeng1,2
1Department of Pharmacy, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China; 2Department of Pharmacy, National Regional Medical Center, Binhai Campus of the First Affiliated Hospital, Fujian Medical University, Fuzhou, 350212, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Pinfang Huang, Department of Pharmacy, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China, Tel +8613600898956, Email [email protected] Dayong Zeng, Department of Pharmacy, The First Affiliated Hospital of Fujian Medical University, Fuzhou, 350005, People’s Republic of China, Tel +8613860613541, Email [email protected]
Background: The Phase III INAVO120 trial established inavolisib-based therapy as a superior first-line treatment for PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer, a finding of particular importance for the historically underrepresented male population with high unmet need.
Methods: A lifetime Markov model was developed from a US payer perspective to evaluate the cost-effectiveness of inavolisib plus palbociclib and fulvestrant versus placebo plus palbociclib and fulvestrant in men with PIK3CA-mutated advanced breast cancer. Primary outcomes were life-years (LYs), quality-adjusted life-years (QALYs), and the incremental cost-effectiveness ratio (ICER).
Results: The inavolisib group provided an additional 1.23 LYs and 0.69 QALYs compared to the placebo group, resulting in an ICER of $886,440 per QALY. One-way sensitivity analysis identified the price of inavolisib as the primary driver of the ICER. Probabilistic sensitivity analysis showed a 0% probability of inavolisib being cost-effective at a willingness-to-pay threshold of $150,000 per QALY.
Conclusion: Inavolisib-based therapy is not cost-effective for treating PIK3CA-mutated advanced male breast cancer at its current price. Significant price reductions or adjustments to value assessment frameworks are required to ensure equitable access for this underserved population.
Plain Language Summary: 1. First Economic Model for Ultra-Rare Subgroup
This study presents the first economic evaluation of inavolisib for the treatment of PIK3CA-mutated male breast cancer—an ultra-orphan population with an incidence rate of 0.5– 1.3 per 100,000 individuals, and significant unmet medical needs.
2. Clinically Effective but Cost-Prohibitive
Although inavolisib extends median progression-free survival by 10 months, its incremental cost-effectiveness ratio (ICER) is $886,440 per quality-adjusted life year (QALY), which exceeds conventional US cost-effectiveness thresholds ($150,000/QALY) by nearly six-fold, resulting in a 0% probability of affordability under current benchmarks.
3. Orphan-Specific Value Distortions
Standard cost-effectiveness models fail to account for male-specific health utilities and societal productivity costs, thereby underestimating the true therapeutic value.
4. Policy Solutions for Rare Cancers
To improve access and equity, policy interventions should include prevalence-adjusted ICER thresholds, cross-indication drug subsidy mechanisms, and universal PIK3CA mutation screening.
Keywords: inavolisib, PIK3CA-mutated, male breast cancer, cost-effectiveness
Introduction
Male breast cancer (MBC), accounting for less than 1% of male malignancies and less than 0.9% of all breast cancers, presents distinct epidemiological, clinicopathological, and socioeconomic challenges relative to female breast cancer (FBC). Epidemiologically, its incidence is approximately 130-fold lower than that of FBC, yet diagnoses occur at a later median age with significantly higher rates of advanced-stage presentation.1–3 Clinicopathologically, MBC exhibits more aggressive features, including larger tumors, frequent nodal involvement, and near-universal estrogen receptor positivity.4,5 These disparities are biologically rooted in dysregulated androgen-estrogen crosstalk that amplifies PI3K/AKT signaling. PIK3CA mutations are recurrent in MBC and represent a clinically actionable target in a substantial subset of patients, particularly in the hormonal receptor (HR) positive/human epidermal growth factor receptor 2 (HER2) negative subtype common among males.6,7
Despite this high mutation prevalence, therapeutic approaches for MBC largely remain extrapolated from FBC guidelines due to systemic limitations: 97% of clinical trials exclude male patients,8 and only 29% undergo guideline-recommended PIK3CA testing.9 Consequently, patients often experience delayed diagnoses,4 limited availability of targeted therapies, and significantly worse survival outcomes.10 This therapeutic marginalization compounds socioeconomic burdens, including 50% higher diagnostic costs and 136% greater productivity losses. These disparities are amplified by the demographic predominance of male patients as primary household earners, intensifying the societal economic toll.11 The distinct clinical trajectory and economic profile of MBC necessitate a dedicated cost-effectiveness evaluation, rather than extrapolation from female data, to accurately assess the value of new interventions in this underserved population.
Inavolisib, an orally administered, phosphatidylinositol-3-kinase alpha (PI3Kα) inhibitor, represents a breakthrough for PIK3CA-mutated advanced breast cancer, receiving FDA approval in October 2024 for the treatment of adults with endocrine-resistant, PIK3CA-mutated, HR-positive, HER2-negative, locally advanced or metastatic breast cancer.12 This development holds particular significance for the historically underrepresented male patient population. The mature overall survival (OS) data from the INAVO120 trial, published subsequently, confirmed a significant clinical benefit, with the inavolisib-based regimen demonstrating a median OS of 34.0 months versus 27.0 months with placebo, and a median progression-free survival (PFS) of 17.3 months versus 7.3 months.13 This clinical breakthrough holds particular significance for MBC, who have historically been excluded from pivotal trials. However, the substantial incremental clinical benefit provided by inavolisib raises a critical economic question: does this survival gain justify the associated costs within this high-need, ultra-rare population marked by accelerated productivity loss and distinct care pathways? A formal cost-effectiveness analysis of inavolisib-based therapy in PIK3CA-mutated MBC is therefore imperative to inform equitable reimbursement policies and gender-specific clinical guideline development. The objective of this study was to evaluate the cost-effectiveness of inavolisib-based therapy versus placebo in the first-line setting for men with PIK3CA-mutated, HR-positive, HER2-negative advanced breast cancer in the US.
Methods
Patients and Treatment
The target population was aligned with that of the INAVO120 trial,14 comprising men diagnosed with PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer. Patients received a luteinizing hormone-releasing hormone agonist for hormone suppression throughout the trial intervention period. Participants were randomly assigned to receive either inavolisib or placebo, both administered in combination with palbociclib and fulvestrant. For the present cost-effectiveness analysis, model survival inputs for both the inavolisib and placebo groups were derived from the updated, mature survival data of the INAVO120 trial (median OS: 34.0 vs 27.0 months; median PFS: 17.3 vs 7.3 months).13
The drugs were administered as follows:
- Inavolisib: 9 mg orally once daily on days 1 to 28 of each 28-day cycle.
- Palbociclib: 125 mg orally once daily on days 1 to 21 of each 28-day cycle.
- Fulvestrant: 500 mg administered intramuscularly on days 1 and 15 of cycle 1, and then every 28 days thereafter.
Model Structure
We developed a Markov model to evaluate the cost-effectiveness of the inavolisib plus palbociclib and fulvestrant (inavolisib group) compared to placebo plus palbociclib and fulvestrant (placebo group) in men with PIK3CA-mutated, HR-positive, HER2-negative locally advanced or metastatic breast cancer, from the US payer perspectives over a lifetime horizon. The Markov model consisted of three mutually exclusive health states: progression-free survival (PFS), progression of disease (PD), and death (Figure 1). Only direct medical costs were considered. Each model cycle represented 28 days to align precisely with the administration schedule of the evaluated treatment regimens. A half-cycle correction was applied to account for the assumption that state transitions occur continuously throughout a cycle, thereby improving the accuracy of cost and outcome estimates. Only direct medical costs were considered. Both costs and effectiveness outcomes were discounted at an annual rate of 3%.
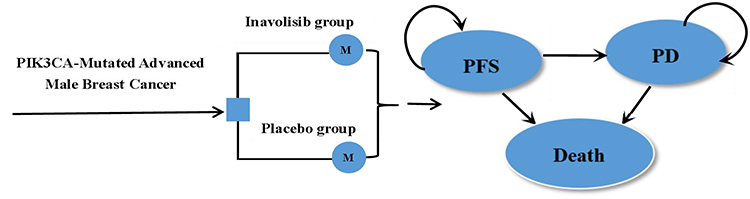 |
Figure 1 Markov state transition model. A three-health-state Markov model comprising progression-free survival (PFS), progressive disease (PD), and death was developed. At each cycle initiation, all patients entered the model in the PFS with stable disease state and immediately initiated treatment; from this state, patients could: (1) achieve complete/partial response and transition to PFS with response, (2) experience disease progression and transition to PD, or (3) die and transition to death. Patients in the PD state could either remain in progression or transition to death. |
The Markov model embraced the following key assumptions:
- All patients entered the model in the PFS state and initiated first-line therapy.
- Patients received the assigned first-line regimen while in the PFS state and discontinued it upon transition to the PD state or due to unacceptable toxicity.
- Patients who transitioned to the PD state received subsequent standard-of-care systemic therapies in accordance with the National Comprehensive Cancer Network guidelines.15 All patients have good compliance in any state.
- In the model, probabilities from PFS to death were assumed to be the same as the natural mortality rate,16 derived from US life tables accounting for age- and sex-specific death rates.17
- Health-state utilities were sourced from published studies with patient demographics matching the INAVO120 trial population, assuming equivalence to FBC utility values.18–21
Survival Analysis and Parameter Estimation
Data Extraction and Curve Fitting
Individual patient time-to-event data for PFS and OS were digitally reconstructed from the published Kaplan-Meier curves of the INAVO120 trial (based on the updated 2025 data) using GetData Graph Digitizer software (version 2.26). The reconstructed data for both the inavolisib and placebo groups were then used to fit parametric survival distributions. The Weibull distribution was selected for extrapolation based on visual inspection of the curve fit and comparison of statistical goodness-of-fit criteria, specifically the Akaike Information Criterion (AIC). The scale (λ) and shape (γ) parameters for the Weibull models were estimated via maximum likelihood estimation using R software (version 4.3.1). The goodness-of-fit for each fitted curve is reported as the R2 value (Table 1).
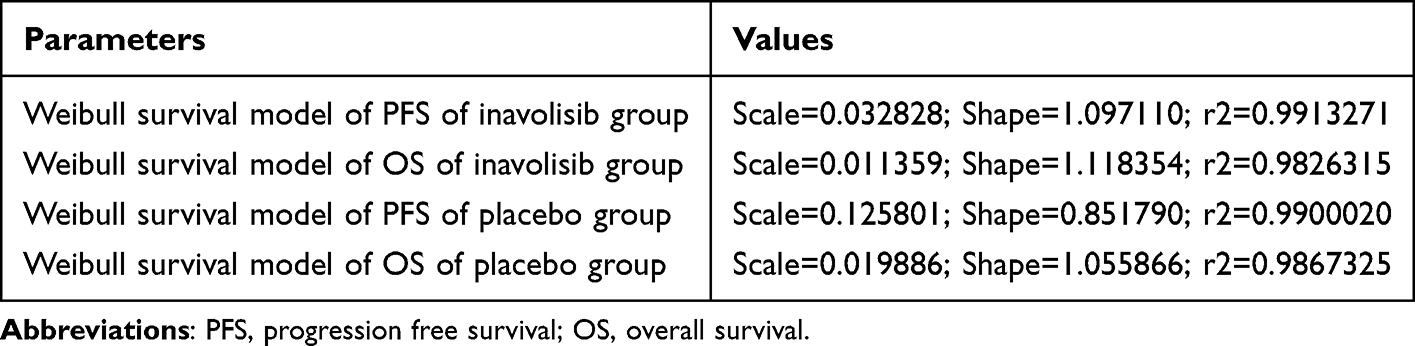 |
Table 1 Key Clinical and Health Parameters |
Calculation of Transition Probabilities
Cycle-specific transition probabilities for the Markov model were derived from the fitted Weibull survival functions. The probability of transitioning from a given health state (PFS) to an event state (PD or Death) within a specific model cycle (t) was calculated using the standard hazard conversion formula for the Weibull distribution:22 P(t) = 1 – exp [λ (t − 1) γ – λ t γ], where P(t) represents the probability of the event occurring within cycle t, and λ and γ are the estimated scale and shape parameters, respectively. This method was applied identically to derive progression risks from the PFS curves and mortality risks from the OS curves for both treatment groups (Supplemental Table 1).
Cost and Utility Inputs
Cost Estimation
Direct medical costs, including the drug acquisition and administration, management of treatment-related serious adverse events (SAEs), routine follow-ups, monitoring, and best supportive care (BSC), are detailed in Table 2. Drug acquisition costs per 28-day cycle were based on the average wholesale price (AWP) from Micromedex RED BOOK Online, applied according to the dosing regimen specified in Patients and Treatment. The cost of managing grade ≥ 3 SAEs was modeled as a one-time expense. It was calculated by multiplying the unit treatment cost for each specific SAE by its corresponding incidence rate reported in the INAVO120 trial. Monthly medical resource utilization costs were applied separately for patients in the PFS and PD states. These costs, which include hospitalizations, outpatient visits, laboratory tests, imaging, and surveillance, were derived from published literature.23–25 Costs were applied according to health state: the PFS state accrued costs for the first-line regimen, monitoring, and AE management; the PD state accrued costs for subsequent therapies and progressed disease care, with first-line treatment discontinued. The total cost for each treatment strategy was calculated as the sum of the cumulative discounted drug costs, the cumulative discounted state-based costs over the time spent in each health state, and the one-time SAE cost. The incremental cost was derived from the difference in total discounted costs between the inavolisib and placebo groups over the model time horizon.
 |
Table 2 Sensitivity Analysis Parameter Ranges and Distribution |
Health State Utilities and Disutilities
Health state utility values for PFS and PD were sourced from previously published studies conducted in advanced breast cancer populations, which employed standard preference-based measures such as the visual analog scale and standard gamble.19,20 Disutility values, representing temporary quality-of-life decrements associated with the occurrence of specific adverse events, were also obtained from the literature.25 All utility and disutility values applied in the model are detailed in Table 2.
Model Outputs
The primary outcomes of the model comprised the total cost, life-years (LYs), quality-adjusted life-years (QALYs), and incremental cost-effectiveness ratios (ICERs). QALYs were calculated as the duration time weighted by the utility of each state. A willingness-to-pay (WTP) threshold was set based on published US benchmarks, which was $150,000 per QALY,26 with ICERs below the WTP threshold considered cost-effective. This Markov model was implemented using TreeAge Pro 2020.
Sensitivity Analyses
Model uncertainty was assessed through one-way sensitivity analysis and probabilistic sensitivity analysis (PSA). One-way sensitivity analysis evaluated the impact of individual parameters by varying each within 95% credible intervals or ±20% ranges from base-case values, with results visualized via tornado diagrams. PSA using a Monte Carlo simulation of 10,000 random individuals with variables varying concurrently in specific distribution patterns was carried out to further test the robustness of the result (Table 2).
Results
Base-Case Analysis
Table 3 displays detailed results of the base case analysis for the US. The model predicted that patients in the inavolisib group had a life expectancy of 4.46 LYs, representing a gain of 1.23 LYs compared to the placebo group. After accounting for quality of life, patients receiving inavolisib-based therapy gained 2.49 QALYs, which was 0.69 QALYs more than those receiving placebo plus palbociclib and fulvestrant. Treatment with inavolisib group incurred an additional cost of $611,420.16, resulting in an ICER of $499,007.92 per LY and $886,439.73 per QALY compared with placebo group.
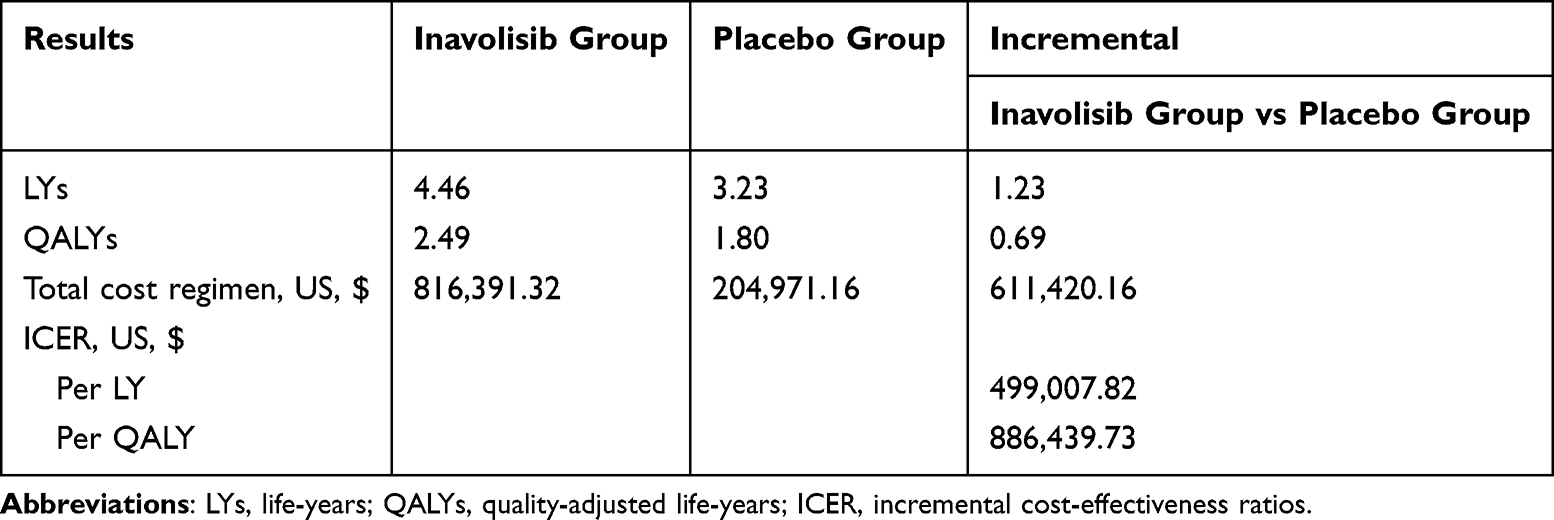 |
Table 3 Base Case Results |
Sensitivity Analyses
One-Way Sensitivity Analysis
The results of the one-way sensitivity analysis are summarized in the Tornado diagrams (Figure 2). The price of inavolisib exerted the greatest impact on the ICERs. Utility of PFS, the discount rate, and utility of PD had moderate influences on the cost-effectiveness results. None of the parameters evaluated was able to render the ICERs greater than the WTP thresholds. These one-way sensitivity analysis results confirm the robustness of the model.
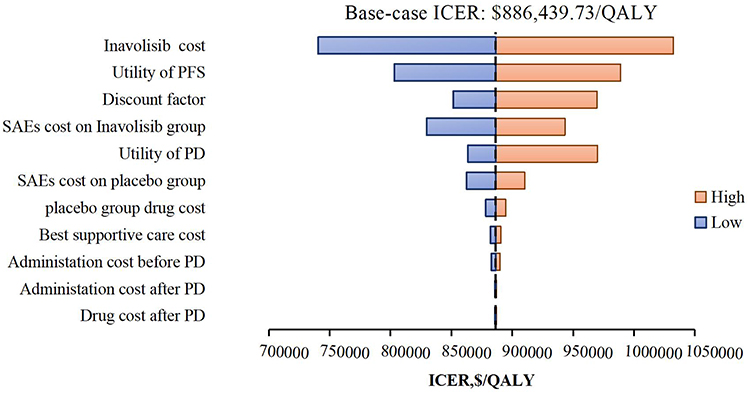 |
Figure 2 Results of One-Way Sensitivity Analysis. This diagram shows ICERs for inavolisib group versus placebo group for different model input parameters. The dotted line intersecting the sky blue and Orange bars represents an ICER of $886,439.73 per QALY in the US. |
Probabilistic Sensitivity Analysis
The results of PSA suggested that the probabilities of inavolisib group being cost-effective over placebo group was 0% at a WTP threshold of $150,000 per QALY in the US (Figure 3). The probability reached 50% only when the WTP threshold increased to approximately $880,000 per QALY. Notably, even with a 50% reduction in inavolisib cost, the ICER for inavolisib group compared with placebo group still higher than the WTP threshold.
 |
Figure 3 Cost-Effectiveness Acceptability Curve. The probabilistic sensitivity analyses based on the 10,000 Monte Carlo simulations, which through sampling model variable values from distributions imposed on variables to indicate uncertainty about whether inavolisib group and placebo group is cost-effective at different WTP thresholds. The probabilities that inavolisib group was cost-effective at thresholds of $150,000 per QALY in the US was 0%. |
Scenario Analyses
Scenario A (Price Reduction)
To explore potential pathways toward cost-effectiveness, we conducted a scenario analysis modeling progressive price reduction for inavolisib. As presented in Table 4, the ICER demonstrated a direct and substantial response to drug price adjustments. A 25% price reduction lowered the ICER to $627,447 per QALY, while a 50% reduction resulted in an ICER of $451,333 per QALY. Notably, even a 75% price reduction yielded an ICER of $275,219 per QALY, which still exceeds the conventional US WTP threshold of $150,000 per QALY, with only a 3.12% probability of being cost-effective. The analysis indicates that an approximately 90% price reduction would be required to approach the $150,000/QALY benchmark, producing an ICER of $156,800 per QALY and a 46.24% probability of cost-effectiveness (Figure 4). This scenario quantitatively underscores that achieving cost-effectiveness within standard US benchmarks would necessitate a profound downward adjustment in the drug’s acquisition cost.
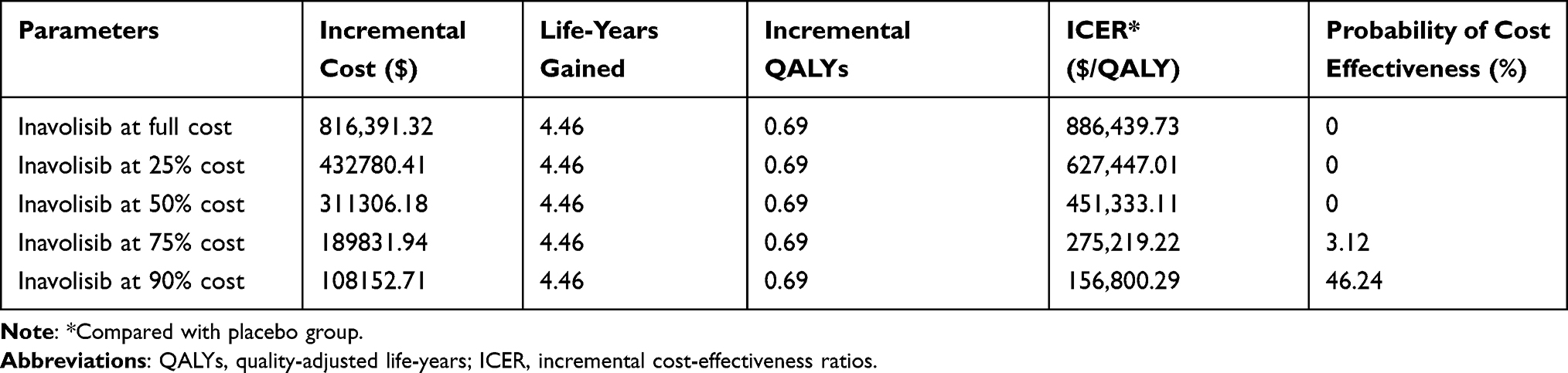 |
Table 4 Adjust the Price of Inavolisib in Accordance with the Corresponding Results |
 |
Figure 4 Cost-Effectiveness Acceptability Curve for Inavolisib Price Reduction. The analysis indicates that an approximately 90% price reduction would be required to approach the $150,000/QALY benchmark, producing an ICER of $156,800 per QALY and a 46.24% probability of cost-effectiveness. |
Scenario B (Adjusted Health Utilities)
This scenario was conducted to assess the sensitivity of the base-case cost-effectiveness results to a key parameter: the health state utility value assigned to PFS. As noted in the study limitations, the base-case utility for PFS (0.78) may not fully reflect gender-specific quality-of-life impacts. Therefore, Scenario B incorporates a lower, referenced gender-specific utility value of 0.62 for the PFS state. As shown in Table 5, this adjustment increased the incremental QALYs gained with inavolisib from 0.69 to 0.76, reflecting a more accurate, albeit lower, quality-of-life weighting specific to the male patient experience. Consequently, the ICER improved from $886,440 to $808,208.08 per QALY (Table 5). The application of a lower utility for the PFS state paradoxically results in a more favorable (lower) ICER per QALY for inavolisib. This occurs because the utility adjustment, while lowering the absolute quality-weight for both treatment arms, disproportionately benefits the inavolisib group. Since inavolisib provides a longer duration in the PFS state compared to placebo, the difference in accumulated QALYs between the two groups becomes larger. A greater incremental QALY gain for the same incremental cost directly leads to a lower cost per QALY.
 |
Table 5 The Results After Adjusting for Health Utilities |
This reduction in the ICER demonstrates that the use of generic, female-derived utility values in the base-case analysis likely inflates the calculated ICER, thereby underestimating the true quality-adjusted value of the therapy for men. Despite this adjustment, the ICER of $808,208.08 per QALY remains substantially above the $150,000 per QALY WTP threshold, reinforcing the conclusion that inavolisib is not cost-effective under current valuation frameworks, even when accounting for a more pessimistic, gender-specific utility assessment. This finding underscores the importance of developing and applying validated, population-specific utility instruments in future economic evaluations of MBC treatments.
Discussion
The Value Paradox: Clinical Superiority vs Economic Unsustainability
The phase III INAVO120 trial established inavolisib-based therapy as a superior first-line treatment, with updated mature data confirming a median OS of 34.0 months versus 27.0 months with placebo, and a median PFS of 17.3 months versus 7.3 months. This clinical breakthrough is particularly significant for the historically underrepresented MBC population. However, our cost-effectiveness analysis reveals a stark economic paradox. Despite this unequivocal clinical benefit, the addition of inavolisib resulted in an ICER of $886,440 per QALY, which substantially exceeds conventional US WTP thresholds ($150,000 per QALY). Thus, while the therapy is clinically transformative, its current cost renders it economically unsustainable under standard valuation frameworks, highlighting a critical challenge in reconciling innovation with affordability in oncology.
Structural Determinants of Cost-Ineffectiveness
Our sensitivity analyses pinpoint the structural drivers of this result. The one-way sensitivity analysis (Figure 2) conclusively identified the price of inavolisib as the dominant driver of the high ICER. This finding directly links the cost-ineffectiveness outcome to a specific, modifiable variable: drug pricing. It exemplifies the broader orphan drug pricing paradox, where incentives for innovation in small populations collide with affordability and value-based reimbursement principles.27,28 The analysis suggests that achieving an ICER aligned with a $150,000 per QALY threshold would require a substantial price reduction, highlighting the magnitude of misalignment between the drug’s price and the value it delivers in this specific indication under standard evaluation methods.
Integrated Policy Interventions to Mitigate the Value Gap
The relevance of our findings extends to informing potential solutions for ultra-rare cancers. To mitigate the identified value gap, policy interventions must be tailored. First, value assessment frameworks could be adapted, for example, by considering prevalence-adjusted ICER thresholds that acknowledge the high unmet need and limited population size in diseases like MBC29,30 Second, innovative contracting mechanisms, such as indication-specific pricing for inavolisib in this niche population or outcomes-based agreements, could better align price with delivered value while maintaining sustainability. Third, optimizing clinical pathways—ensuring timely PIK3CA mutation testing to guide appropriate therapy initiation—can improve system efficiency. These proposals are direct logical extensions of our results, which quantified the problem and its primary driver.
Limitations and Future Research Imperatives
Although this analysis presents the first MBC-specific cost-effectiveness model, several limitations still remain. First, while we used the most mature survival data available, long-term efficacy data specific to men remain limited. Second, there is a systematic undervaluation of health-related quality-of-life utilities, as generic instruments such as the EQ-5D fail to capture the profound gender-specific psychosocial burdens associated with MBC. These burdens are particularly pronounced among male patients, who report significantly lower utility scores compared to female counterparts (0.62 vs 0.81; P<0.01), driven by high prevalence rates of body image distress (72%), sexual dysfunction (51%)31 and isolation during rehabilitation (30%).10,32 This measurement gap results in underestimated QALYs and inflated ICERs. Although we partially addressed this limitation through sensitivity analyses using adjusted utility values, such interim approaches cannot fully resolve the fundamental inadequacy in current utility assessment tools. Future research should prioritize the development of validated, MBC-specific utility instruments that incorporate gender-specific burdens using qualitative methodologies and discrete choice experiments to generate more accurate quality-of-life valuations. Finally, the omission of critical societal costs including productivity losses, caregiver burden, cascade genetic testing, and the economic impact of disease-related stigmatization, despite many patients are primary earners.33 While our sensitivity analyses attempted to mitigate this deficiency by adjusting treatment and adverse event management costs, such adjustments remain an incomplete proxy for a formal societal perspective. Consequently, future research must prioritize adopting a comprehensive societal perspective in reference case analyses, formally quantifying productivity losses and stigmatization costs using linked employment and patient-reported outcome data, alongside implementing advanced modeling techniques (such as Bayesian evidence synthesis) to manage the inherent uncertainty associated with sparse societal cost data.
Conclusion
While inavolisib represents a significant clinical advancement for patients with PIK3CA-mutated advanced MBC, our analysis reveals a pronounced value paradox: despite clear survival gains, its current pricing renders the therapy cost-ineffective within conventional US payer frameworks. This economic unsustainability is primarily driven by the high drug acquisition cost, as confirmed in our sensitivity analysis. Bridging this value gap demands urgent, coordinated multi-stakeholder action. Required interventions include: 1) substantial price adjustments for inavolisib within this niche indication; 2) optimization of clinical pathways through universal PIK3CA testing; 3) adaptation of reimbursement policies to incorporate prevalence-adjusted value thresholds for ultra-rare cancers; and 4) dedicated research to integrate gender-specific utility measures and societal cost perspectives into economic evaluations. Without such comprehensive efforts, equitable access to this targeted therapy for this marginalized patient population will remain critically constrained.
Abbreviations
MBC, Male breast cancer; FBC, Female breast cancer; HR, Hormone receptor; HER2, Human epidermal growth factor 2; PI3Kα, Phosphatidylinositol-3-kinase alpha; PFS, Progression-free survival; PD, Progression of disease; OS, Overall survival; SAEs, Serious adverse events; BSC, Best supportive care; LYs, Life-years; QALYs, Quality-adjusted life-years; ICERs, Incremental cost-effectiveness ratios; WTP, Willingness-to-pay; PSA, Probabilistic sensitivity analysis.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethical Approval
This analysis is based solely on digitized data from published survival curves of the INAVO120 trial. Since no new patient data were collected or used, and all information is publicly available and anonymized, this study did not require separate ethical approval. This article does not contain any studies with human participants or animals performed by any of the authors.
Informed Consent
Informed consent was obtained from all individual participants included in the study.
Acknowledgments
The authors extend their sincere gratitude to Professor Xiuhua Weng for their expertise in developing the Markov model and probabilistic sensitivity analyses.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Startup Fund for scientific research, Fujian Medical University (No. 2021QH1059). This study was not supported by any pharmaceutical company.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Anonymous. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries - sung - 2021 - CA: a cancer journal for clinicians - Wiley Online Library. n.d. Available from: https://acsjournals.onlinelibrary.wiley.com/doi/10.3322/caac.21660.
2. Cardoso F, Bartlett JMS, Slaets L, et al. Characterization of male breast cancer: results of the EORTC 10085/TBCRC/BIG/NABCG international male breast cancer program. Ann Oncol. 2018;29(2):405–417. doi:10.1093/annonc/mdx651
3. Yadav S, Karam D, Riaz IB, et al. Male breast cancer in the United States: treatment patterns and prognostic factors in the twenty-first century. Cancer. 2020;126(1):26–36. doi:10.1002/cncr.32472
4. Wang F, Shu X, Meszoely I, et al. Overall mortality after diagnosis of breast cancer in men vs women. JAMA Oncol. 2019;5(11):1589–1596. doi:10.1001/jamaoncol.2019.2803
5. Leone JP, Freedman RA, Leone J, et al. Survival in male breast cancer over the past 3 decades. J Natl Cancer Inst. 2022;115(4):421–428. doi:10.1093/jnci/djac241
6. Piscuoglio S, Ng CKY, Murray MP, et al. The genomic landscape of male breast cancers. Clin Cancer Res. 2016;22(16):4045–4056. doi:10.1158/1078-0432.CCR-15-2840
7. Gucalp A, Traina TA, Eisner JR, et al. Male breast cancer: a disease distinct from female breast cancer. Breast Cancer Res Treat. 2019;173(1):37–48. doi:10.1007/s10549-018-4921-9
8. Ruddy KJ, Winer EP. Male breast cancer: risk factors, biology, diagnosis, treatment, and survivorship. Ann Oncol. 2013;24(6):1434–1443. doi:10.1093/annonc/mdt025
9. Yadav S, Hu C, Hart SN, et al. Evaluation of germline genetic testing criteria in a hospital-based series of women with breast cancer. J Clin Oncol. 2020;38(13):1409–1418. doi:10.1200/JCO.19.02190
10. Abboah-Offei M, Bayuo J, Salifu Y, et al. Experiences and perceptions of men following breast cancer diagnosis: a mixed method systematic review. BMC Cancer. 2024;24(1):179. doi:10.1186/s12885-024-11911-9
11. Anonymous. Male breast cancer: a review on diagnosis, treatment, and survivorship - PubMed. n.d. Available from: https://pubmed.ncbi.nlm.nih.gov/38224426/.
12. Blair HA. Inavolisib: first Approval. Drugs. 2025;85(2):271–278. doi:10.1007/s40265-024-02136-y
13. Jhaveri KL, Im S-A, Saura C, et al. Overall survival with inavolisib in PIK3CA-mutated advanced breast cancer. N Engl J Med. 2025;393(2):151–161. doi:10.1056/NEJMoa2501796
14. Turner NC, Im S-A, Saura C, et al. Inavolisib-based therapy in PIK3CA-mutated advanced breast cancer. N Engl J Med. 2024;391(17):1584–1596. doi:10.1056/NEJMoa2404625
15. Gradishar WJ, Moran MS, Abraham J, et al. Breast cancer, version 3.2024, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2024;22(5):331–357. doi:10.6004/jnccn.2024.0035
16. Wu B, Gu X, Zhang Q, et al. Cost-effectiveness of osimertinib in treating newly diagnosed, advanced EGFR-mutation-positive non-small cell lung cancer. Oncologist. 2019;24(3):349–357. doi:10.1634/theoncologist.2018-0150
17. Wan X, Zhang Y, Tan C, et al. First-line nivolumab plus ipilimumab vs sunitinib for metastatic renal cell carcinoma: a cost-effectiveness analysis. JAMA Oncol. 2019;5(4):491. doi:10.1001/jamaoncol.2018.7086
18. Lloyd A, van Hanswijck de Jonge P, Doyle S, et al. Health state utility scores for cancer-related anemia through societal and patient valuations. Value Health. 2008;11(7):1178–1185. doi:10.1111/j.1524-4733.2008.00394.x
19. Shiroiwa T, Fukuda T, Shimozuma K, et al. Long-term health status as measured by EQ-5D among patients with metastatic breast cancer: comparison of first-line oral S-1 and taxane therapies in the randomized phase III SELECT BC trial. Qual Life Res. 2017;26(2):445–453. doi:10.1007/s11136-016-1388-1
20. Lloyd A, Nafees B, Narewska J, et al. Health state utilities for metastatic breast cancer. Br J Cancer. 2006;95(6):683–690. doi:10.1038/sj.bjc.6603326
21. Guyot P, Ades A, Ouwens MJ, et al. Enhanced secondary analysis of survival data: reconstructing the data from published Kaplan-Meier survival curves. BMC Med Res Methodol. 2012;12(1):9. doi:10.1186/1471-2288-12-9
22. Weibull CE, Eloranta S, Johansson ALV, et al. Reply to Silvia Selinski, Daniel Ovsiannikov, Jan G. Hengstler and Klaus Golka’s Letter to the Editor re: caroline E. Weibull, Sandra Eloranta, Daniel Altman, Anna L.V. Johansson, Mats Lambe. Childbearing and the risk of bladder cancer: a nationwide population-based cohort study. Eur urol 2013;63:733–8. Europ Urol. 2013;64(4):e81. doi:10.1016/j.eururo.2013.05.040
23. Wu B, Zhang Q, Sun J. Cost-effectiveness of nivolumab plus ipilimumab as first-line therapy in advanced renal-cell carcinoma. J ImmunoTher Cancer. 2018;6(1):124. doi:10.1186/s40425-018-0440-9
24. Xie J, Hao Y, Zhou Z-Y, et al. Economic evaluations of everolimus versus other hormonal therapies in the treatment of HR+/HER2- advanced breast cancer from a US payer perspective. Clin Breast Cancer. 2015;15(5):e263–276. doi:10.1016/j.clbc.2015.04.001
25. Huang X, Lin S, Rao X, et al. First-line treatment with ribociclib plus endocrine therapy for premenopausal women with hormone-receptor-positive advanced breast cancer: a cost-effectiveness analysis. Clinical Breast Cancer. 2021;21(4):e479–e488. doi:10.1016/j.clbc.2021.01.019
26. Anonymous. Institute for clinical and economic review, overview of the ICER value framework and proposals for an update for 2017. n.d. Available from: http://icer-review.org/wp-content/uploads/2016/02/ICER-VAF-Update-Proposals-020117.pdf.
27. Simoens S. Pricing and reimbursement of orphan drugs: the need for more transparency. Orphanet J Rare Dis. 2011;6(42):42. doi:10.1186/1750-1172-6-42
28. Pauwels K, Huys I, Vogler S, et al. Managed entry agreements for oncology drugs: lessons from the european experience to inform the future. Front Pharmacol. 2017;8(171). doi:10.3389/fphar.2017.00171
29. Conti RM, Demartino P, Gruber J, et al. Innovative insurance to improve US patient access to cell and gene therapy. Milbank Q. 2025;103(1):32–51. doi:10.1111/1468-0009.12728
30. Michaeli DT, Michaeli T. Value-based indication-specific pricing and weighted-average pricing: estimated price and cost savings for cancer drugs. Pharmacoeconomics. 2025;43(4):415–427. doi:10.1007/s40273-024-01448-x
31. Goldfarb S, Mulhall J, Nelson C, et al. Sexual and reproductive health in cancer survivors. Semin Oncol. 2013;40(6):726–744. doi:10.1053/j.seminoncol.2013.09.002
32. Aryannejad A, Saeedi Moghaddam S, Mashinchi B, et al. National and subnational burden of female and male breast cancer and risk factors in Iran from 1990 to 2019: results from the global burden of disease study 2019. Breast Cancer Res. 2023;25(1):47. doi:10.1186/s13058-023-01633-4
33. Bradley CJ, Yabroff KR, Dahman B, et al. Productivity costs of cancer mortality in the United States: 2000-2020. J Natl Cancer Inst. 2008;100(24):1763–1770. doi:10.1093/jnci/djn384
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.