")
Back to Journals » International Journal of Women's Health » Volume 12
Inadequate and Late Antenatal Contacts Among Saudi Mothers: A Hospital-Based Cross-Sectional Study
Authors Al-Wutayd O
Received 21 June 2020
Accepted for publication 2 September 2020
Published 14 September 2020 Volume 2020:12 Pages 731—738
DOI https://doi.org/10.2147/IJWH.S265941
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Elie Al-Chaer
Osama Al-Wutayd
Department of Family and Community Medicine, Unaizah College of Medicine and Medical Sciences, Qassim University, Unaizah, Saudi Arabia
Correspondence: Osama Al-Wutayd Email [email protected]
Background: Antenatal care is a major contributor to the reduction of perinatal and maternal mortality and morbidity, through the identification of high risk pregnancies and early intervention for pregnant women with complications. Inadequate (less than eight contacts) and late antenatal care (starting after 12 weeks) have implications for the health of mothers, fetuses, and newborns. The aim of this study was to assess proportion and determinants of inadequate and late antenatal care among Saudi mothers in Unaizah, Qassim, Saudi Arabia.
Methods: This was a cross-sectional study among 537 mothers who gave birth at King Saud Hospital, Unaizah City. Face-to-face interviews were conducted using a structured questionnaire covering sociodemographic information, antenatal care, and determinants that might affect the use of antenatal care. The data were entered into Excel and exported in STATA version 16. Simple and multiple logistic regressions were used to identify the determinants of inadequate and late antenatal care.
Results: The mean (standard deviation) age of the participants was 30.71 (5.73) years. The proportion of inadequate and late antenatal care was 34% (95% CI 30– 38) and 25% (95% CI 21– 29). Inadequate antenatal care was independently associated with employed mothers (OR 1.91, 95% CI 1.13– 3.22) and high parity (three or more) (OR 2.21, 95% CI 1.17– 4.16). Late antenatal care was independently associated with employed mothers (OR 1.87, 95% CI 1.07– 3.27) and high parity (OR 2.04, 95% CI 1.01– 4.16).
Conclusion: This study found that the proportion of inadequate and late ANC was less than in other regions of Saudi Arabia, but it is still important to decrease this rate. The findings of this study will be useful for policy makers in Qassim region to help them design interventions to target mothers at high risk of inadequate and late ANC.
Keywords: antenatal care, determinants, Qassim, Saudi Arabia, parity, employment
Background
Antenatal care (ANC) is important for a variety of reasons. It is a major contributor to the reduction of perinatal and maternal mortality and morbidity, through the identification of high risk pregnancies and early intervention for pregnant women with complications such as preeclampsia.1 The 2016 guidelines from the World Health Organization (WHO) expanded the model of ANC to improve maternal and newborn outcomes. Instead of suggesting at least four ANC visits, the expanded model renamed antenatal visits “antenatal contacts”, and increased the required number to at least eight.2 Inadequate (less than the recommended number) and late antenatal care (starting after 12 weeks) have implications for the health of mothers, fetuses, and newborns. Adequate and early antenatal care have an important role because early antenatal contact increases the probability of mothers attending screening tests, having non-communicable diseases detected, and modifying lifestyle risk factors such as malnutrition and smoking. These interventions are most effective in early pregnancy. Furthermore, early contact also increases the chances that women will receive the recommended number of antenatal contacts and services, and is therefore an important indicator of ANC quality.3–5 Adequate ANC increases the follow-up and monitoring of maternal health and fetal growth, provides a positive pregnancy experience, and promotes healthy behaviors into the postnatal period, including healthy lifestyle and diet, breastfeeding, and family planning.6,7 Despite the evidence of the importance of antenatal care, however, there are still pregnant women who do not receive the recommended number of contacts and start antenatal care late. Every day in 2017, around 800 women around the world died from pregnancy-related complications, childbirth, or during the postnatal period, many of which could have been preventable.8 The prevalence and determinants of inadequate and late ANC vary across and within countries. Factors such as maternal age, income, employment, education, parity, and desirability of pregnancy are strong determinants of inadequate and late ANC.9–13 In 10 low to middle-income countries, over two-fifths of women had at least four antenatal contacts ranging from 44% in Rwanda to 94% in Jordan.14 Other studies found 81.1% in Canada,15 and 93% in Italy.16 Early ANC contact also varied between low- and high-income countries (24% vs 82%).17 A recent study in the Riyadh region reported that 48% of women did not attend one or more antenatal contacts and 34% initiated contact late.18 A study in Medinah region reported that 80% of women stated that they followed up their pregnancy regularly, 16% did not, and 4% did not attend at all.19 Another study reported that most women attended their first antenatal appointment after the first trimester.20 To the authors’ knowledge, few studies on antenatal care have been conducted in Saudi Arabia, and none in the Qassim region. Information about ANC and potential determinants is important to prevent maternal and newborn mortality and is useful for policy makers particularly, the Qassim region has one of the highest delivery rates in Saudi Arabia.21 This study therefore aimed to assess the proportion and potential determinants of inadequate and late antenatal care in Unaizah city, Qassim region, Saudi Arabia.
Materials and Methods
Study Design and Setting
This was a cross-sectional study among mothers who gave birth at King Saud Hospital, in Unaizah City, Qassim region, Saudi Arabia. It is the only governmental hospital run by the Ministry of Health, and has a capacity of around 294 beds.22 Unaizah is the second largest city in the Qassim region, in the middle of Saudi Arabia. It has a population of approximately 165,000, and 17 primary healthcare centers (PHC).23 At least eight antenatal contacts offered for uncomplicated pregnancy,18 starting their antenatal contacts in PHCs or private clinics, and at week 36, are referred to King Saud Hospital for their seventh and eighth antenatal contacts. Some women may require additional contacts, depending on their condition. In total, 75% of the deliveries in the Qassim region occur in governmental hospitals rather than private hospitals.21 In Saudi Arabia, the maternal mortality rate is 11.9 per 100,000 live births, the stillbirth and neonatal mortality rates are 13 and 5 per 1000 live births, and the rate of preterm delivery is 3.3%.24
Definitions
Participants: includes mothers who delivered in the obstetric ward at King Saud Hospital, Unaizah City, Qassim region. A systematic sampling technique was used to get 550 participants out of around 4000 mothers who delivered during 2019. Every 3rd mothers admitted to obstetric ward after delivery for periods 5 months was recruited.
Inadequate ANC: means less than eight antenatal contacts as defined by WHO.3
Late use of ANC: means that the first antenatal contact was after 12 weeks (first trimester).3
Interpregnancy interval: means the period between the end of one pregnancy and the beginning of the subsequent pregnancy. The WHO recommends that this should be at least 24 months.25
Questionnaire
Face-to-face interviews were conducted with the mothers using a predesigned validated questionnaire based on previous studies.9–13 The questionnaire was pretested in a pilot study among a sample of 40 women, whose results were not included in the study. Some modifications were made after their feedback as shortening the questionnaire and interview time to increase the ability to recall. The face and content validity of the questionnaire were reviewed by two experts. The questionnaire included two parts. The first covered sociodemographic data (age, education, working status, family income “1$=3.75 Saudi Riyals”), and the second obstetric data (number and timing of initiation of antenatal contacts of the index pregnancy, parity, planning for pregnancy, interpregnancy interval, any placental problem during the index pregnancy, preexisting chronic conditions such as hypertension and diabetes, and any history of miscarriage, delivery before 37 weeks, or cesarean section).
Data Collection
Data were collected by a trained female intern and nurse who interviewed the mothers after explaining the details of the study.
Sample Size Estimation
Sample size was estimated considering a type I error possibility of 5%, a statistical power of 80% and an assumption that the prevalence of inadequate and late ANC is 50%, to provide the maximum sample size. The anticipated nonresponse rate was 20%. The minimum required sample was 462 participants.
Statistical Analysis
Data were analyzed using Stata v16. Frequencies and percentages of each variable, number of ANC contacts, and timing of first contact were calculated. Simple and multiple logistic regression analysis was used to show the association of potential determinants as independent variables with inadequate and late ANC as dependent variables. Potential risk or protective factors included in the model were based on previous background information despite non significance, and the rule of events per predictor variable in logistic regression.26 The unadjusted model included only one potential determinant and the dependent variable, and the adjusted model included all potential determinants to calculate the adjusted odds ratios and 95% confidence intervals. The appropriateness of the model was assessed by area under ROC curve. A two-tailed p-value of 0.05 or less was considered to be strong evidence against the null hypothesis.
Ethical Considerations
Approval for the study was obtained from Qassim Region Research Ethics Committee (Registration No. 20180217). A copy of the questionnaire was given to each participant to read before the interview after explaining the purpose of the study, and those who agreed to participate and signed the consent form were included in the study. This study was conducted in accordance with the Declaration of Helsinki.
Results
The response rate in our study was 96% (537/550). The mean (standard deviation) age of the participants was 30.71 (5.73) with a range from 18 to 49 years. Table 1 shows the descriptive characteristics of participants by the two outcome variables. In total, 183 (34%) mothers had inadequate antenatal contacts and 133 (25%) started contact late. Table 2 shows the unadjusted and adjusted associations between potential determinants and each of the two outcome variables. The unadjusted analysis shows that the odds ratio of having inadequate antenatal contacts was significantly higher among mothers who were employed (p = 0.019), whose family income was >8000SR (p = 0.042), and who had a parity of three or more (p = 0.042). The odds ratio of late first antenatal contact was significantly higher among mothers who were employed (p = 0.017), and had a parity of three or more (p = 0.009). The adjusted odds ratio of having inadequate antenatal contacts was 1.9 times higher among mothers who were employed than unemployed (p = 0.016), also, women with a parity of three or more have 2.2 times more likely to have inadequate antenatal contacts than nulliparous (p = 0.014). The adjusted odds ratio of late first antenatal contact was 1.8 times higher among mothers who were employed than unemployed (p = 0.028). Women who were a parity of three or more have 2 times more likely to have inadequate antenatal contacts than nulliparous (p = 0.049).
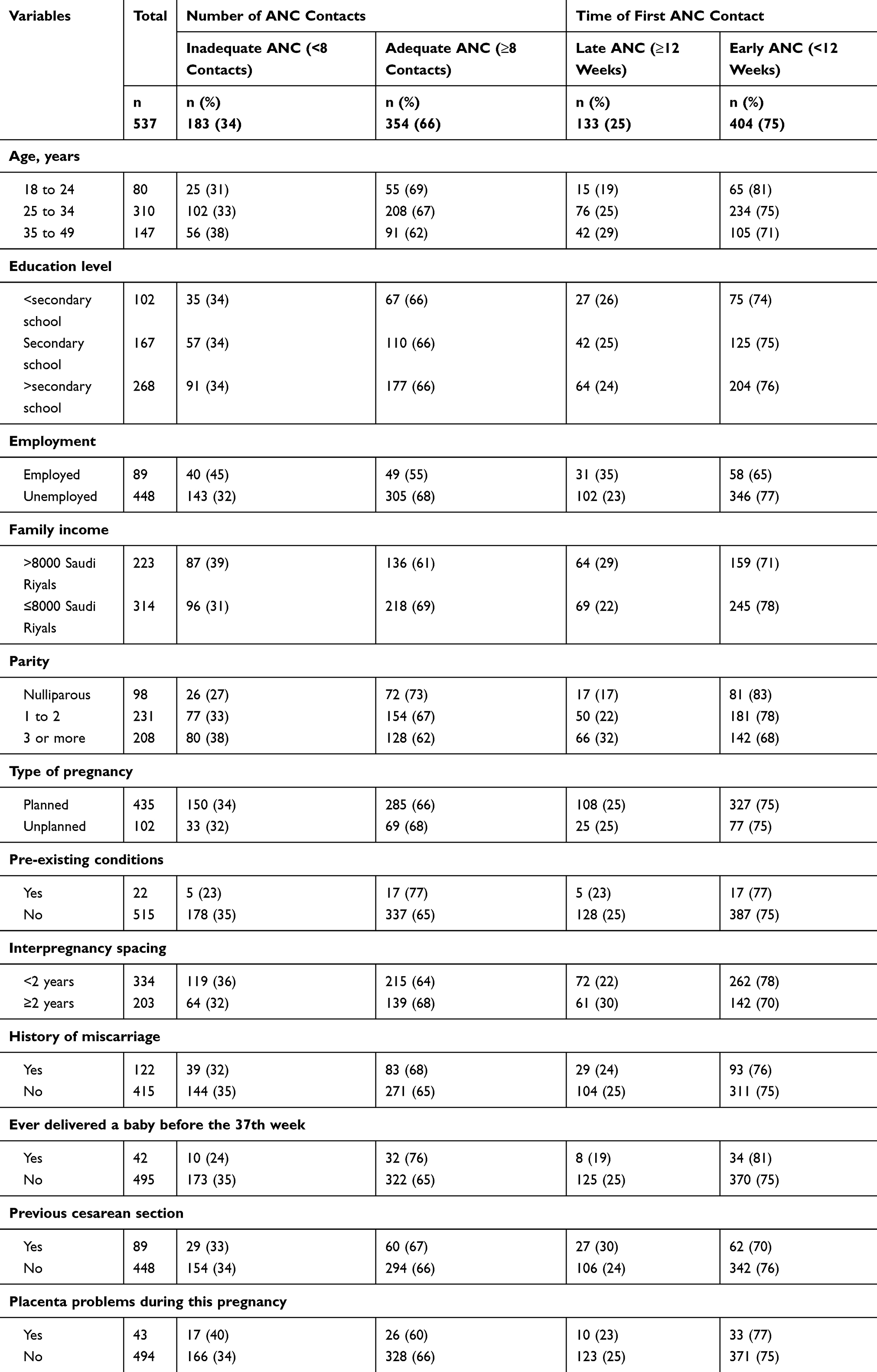 |
Table 1 Descriptive Statistics of the Participants |
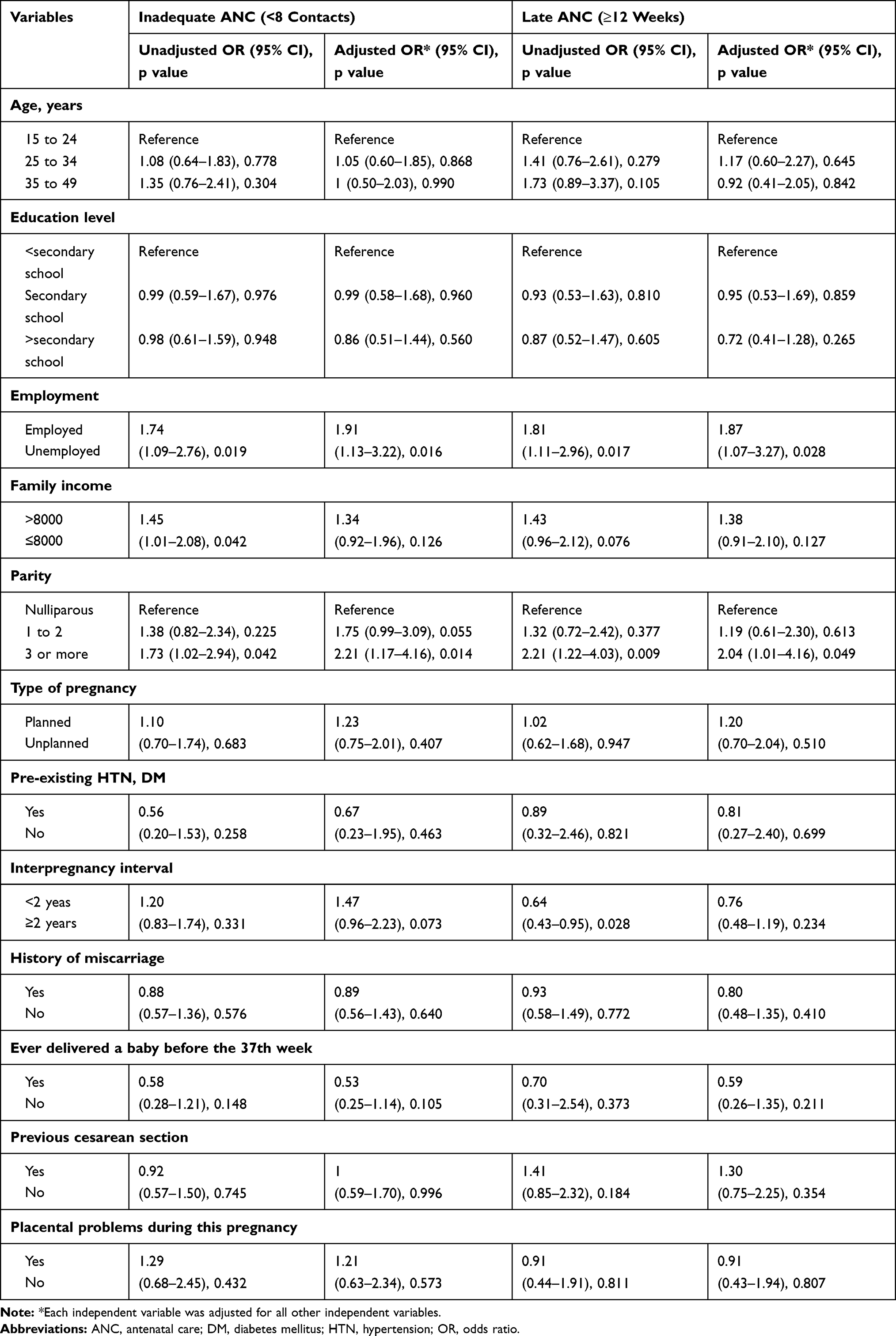 |
Table 2 Unadjusted and Adjusted Associations Between Potential Determinants and Inadequate and Late Antenatal Care Among Saudi Mothers |
Discussion
The proportion of inadequate antenatal contacts was 34%. A study in the Riyadh region of Saudi Arabia found that around 48% of women missed one or more appointments.18 We found that employment and high parity were independently associated with inadequate antenatal contacts. The association between employment and inadequate antenatal contacts is consistent with a previous study in Saudi Arabia,10 and Kenya,27 while inconsistent with study in Nigeria.28 This may be because work commitments mean there is insufficient time to go to a PHC. High parity was also associated with inadequate antenatal care, which is consistent with a systematic review in high-income countries.11 This is probably because women with previous experience of pregnancy feel less need of ANC than women with low parity. The WHO recommends that pregnant women should initiate ANC within the first trimester, but there is still a percentage of women who do not follow this recommendation. This study found the proportion of late first antenatal contact was 25%. A study in another region of Saudi Arabia reported that 33.9% of pregnant women have a late first contact. However, that study defined “late” as after 8 weeks of pregnancy, which is less than the WHO definition.18 This could be explained by a regional variation within Saudi Arabia. A study in Oman reported that 23% have a late first antenatal contact, with regional variation ranging from 12% to 47%.29 Early initiation of ANC is essential to monitor the health of women and their fetus, and also for early diagnosis and treatment of pregnancy-related conditions. The development of the fetus in the first trimester is especially important.30 We found that mothers being employed, and having a parity of three or more, were independently associated with late first antenatal contacts. Employed mothers had odds of 1.9 of late initiation of ANC. This is in line with a study in Saudi Arabia that reported that employed women were more likely to delay initiation of ANC10 whereas, inconsistent with a study in England,31 and Ethiopia.13 Women with three or more previous births had double the odds of late initiation of ANC. This was the strongest determinant for late initiation of ANC, which is consistent with a previous study in the UK,32 Ghana,33 and Indonesia,34 whereas inconsistent with a study in Canada.15 It is possible that women with higher parity feel more confident after their previous experience, and feel that starting ANC early is not necessary. However, differences in the prevalence of inadequate and late ANC between and within countries may also be because of variations in the definitions of inadequate and late ANC. Overall, our findings show that inadequate and late ANC is common in the Qassim region, although both governmental and private health sectors are accessible to the whole Saudi population. The governmental health facility provides high-quality healthcare free for all Saudis. There was also some evidence of an association between inadequate ANC and both a short inter-pregnancy interval (p = 0.073) and parity of one or two (p = 0.055). However, there was no association between inadequate and late ANC and age or education level. A similar finding in other regions of Saudi Arabia has been reported,18,19 but this is inconsistent with other countries.11,12 This may be because most of the mothers in this study have secondary school education and above.
In conclusion, the proportion of inadequate and late ANC was less than in other regions of Saudi Arabia, but it is still important to decrease this rate. The findings of this study will be useful for policy makers in Qassim region to help them design interventions to target mothers at high risk of inadequate and late ANC.
Strengths and Limitations of the Study
The study sample may not be representative of the whole community in the Qassim region. However, the selection of participants was conducted in the hospital rather than PHCs, to try to capture more women, because some women may not attend some or any of their antenatal contacts. In total, 75% of the deliveries in the Qassim region occur in governmental hospitals rather than private hospitals.21 Misclassification bias should also be considered because data were collected by interviewers and relied on participant recall. Other studies have found that enabling factors such as distance to primary healthcare centers or hospitals were important, but these were not included in this study because there are PHCs in each neighborhood. Some explanatory variables were also not included, such as smoking, because it is not culturally acceptable in Saudi Arabia to ask women about this, and alcohol, which is illegal in Saudi Arabia. During the pilot study, some women suggested shortening the questionnaire and interview time to increase the ability to recall, so it was not considered helpful to include any more questions.
Acknowledgment
I thank Melissa Leffler, MBA, from Edanz Group for editing a draft of this manuscript.
Funding
This research received no external funding.
Disclosure
The author declares no conflicts of interest for this work.
References
1. Carroli G, Rooney C, Villar J. How effective is antenatal care in preventing maternal mortality and serious morbidity? An overview of the evidence. Paediatr Perinat Epidemiol. 2001;15(Suppl 1):1–42. doi:10.1046/j.1365-3016.2001.00001.x
2. World Health Organization. Sexual and reproductive health: new guidelines on antenatal care for a positive pregnancy experience; 2020. Available from: https://www.who.int/reproductivehealth/news/antenatal-care/en/.
3. World Health Organization. WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. Geneva: World Health Organization; 2016.
4. Zolotor A, Carlough MC. Update on prenatal care. Am Fam Physician. 2014;89:199–208.
5. Committee ES. The public health importance of antenatal care. Facts Views Vis Obgyn. 2015;7:5–6.
6. Lincetto O, Mothebesoane-Anoh S, Gomez P, et al. Antenatal care. Oppor Africa’s newborns pract data, policy program support newborn care Africa; 2006:55–62.
7. WHO recommendation on antenatal care contact schedules. Available from: https://extranet.who.int/rhl/topics/improving-health-system-performance/who-recommendation-antenatal-care-contact-schedules.
8. World Health Organization. Maternal mortality, Key facts, 19 September, 2019. Available from: https://www.who.int/news-room/fact-sheets/detail/maternal-mortality.
9. Guliani H, Sepehri A, Serieux J. Determinants of prenatal care use: evidence from 32 low-income countries across Asia, Sub-Saharan Africa and Latin America. Health Policy Plan. 2014;29:589–602. doi:10.1093/heapol/czt045
10. El-Gilany AH, El-Wehady A, El-Hawary A. Maternal employment and maternity care in Al-Hassa, Saudi Arabia. Eur J Contracept Reprod Heal Care. 2008;13:304–312. doi:10.1080/13625180802185080
11. Feijen-de Jong EI, Jansen DEMC, Baarveld F, et al. Determinants of late and/or inadequate use of prenatal healthcare in high-income countries: a systematic review. Eur J Public Health. 2012;22:904–913. doi:10.1093/eurpub/ckr164
12. Wolde F, Mulaw Z, Zena T, et al. Determinants of late initiation for antenatal care follow up: the case of northern Ethiopian pregnant women. BMC Res Notes. 2018;11:837. doi:10.1186/s13104-018-3938-9
13. Wolde HF, Tsegaye AT, Sisay MM. Late initiation of antenatal care and associated factors among pregnant women in Addis Zemen primary hospital, South Gondar, Ethiopia. Reprod Health. 2019;16:73. doi:10.1186/s12978-019-0745-2
14. Benova L, Tunçalp Ö, Moran AC, et al. Not just a number: examining coverage and content of antenatal care in low-income and middle-income countries. BMJ Glob Health. 2018;3:e000779. doi:10.1136/bmjgh-2018-000779
15. Debessai Y, Costanian C, Roy M, et al. Inadequate prenatal care use among Canadian mothers: findings from the maternity experiences survey. J Perinatol. 2016;36:420–426. doi:10.1038/jp.2015.218
16. Chiavarini M, Lanari D, Minelli L, et al. Socio-demographic determinants and access to prenatal care in Italy. BMC Health Serv Res. 2014;14:174. doi:10.1186/1472-6963-14-174
17. Moller A-B, Petzold M, Chou D, et al. Early antenatal care visit: a systematic analysis of regional and global levels and trends of coverage from 1990 to 2013. Lancet Glob Health. 2017;5:e977–e983. doi:10.1016/S2214-109X(17)30325-X
18. Brown W. A Individual and healthcare system factors influencing antenatal care attendance in Saudi Arabia. BMC Health Serv Res. 2020;20:49. doi:10.1186/s12913-020-4903-6
19. Al Hamazi JM, Habib HM, Sebeih SH, et al. Awareness of antenatal care importance among Saudi women in Madina. J Gynecol Women’s Health. 2017;4:555649.
20. Al-Ateeq MA, Al-Rusaiess AA, Al-Dughaither AA. Perceptions and effects of antenatal education. Saudi Med J. 2013;34:1287–1293.
21. Saudi Ministry of Health. Statistical yearbook. Available from: https://www.moh.gov.sa/Ministry/Statistics/book/Pages/default.aspx.
22. Saudi Ministry of Health. Statistical yearbook 2017. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/Statistical-Yearbook-1438-Appendix.pdf.
23. General Authority for Statistics. Qassim region; 2017. Available from: https://www.stats.gov.sa/sites/default/files/al-qaseem_region_ar.pdf.
24. Saudi Ministry of Health. Statistical yearbook, 2018. Available from: https://www.moh.gov.sa/en/Ministry/Statistics/book/Documents/book-Statistics.pdf.
25. Marston C Report of a technical consultation on birth spacing, Geneva, 13–15 June, 2005. 2006
26. Vittinghoff E, McCulloch CE. Relaxing the rule of ten events per variable in logistic and Cox regression. Am J Epidemiol. 2007;165(6):710–718. doi:10.1093/aje/kwk052
27. Magadi MA, Madise NJ, Rodrigues RN. Frequency and timing of antenatal care in Kenya: explaining the variations between women of different communities. Soc Sci Med. 2000;51(4):551–561. doi:10.1016/s0277-9536(99)00495-5
28. Agho KE, Ezeh OK, Ogbo FA, Enoma AI, Raynes-Greenow C. Factors associated with inadequate receipt of components and use of antenatal care services in Nigeria: a population-based study. Int Health. 2018;10(3):172–181. doi:10.1093/inthealth/ihy011
29. Ministry of Health Sultanate of Oman. Annual Health Report, Chapter 8 (Health Domain); 2018. Available from: https://www.moh.gov.om/documents/274609/3563447/%D8%A7%D9%84%D9%81%D8%B5%D9%84+%D8%A7%D9%84%D8%AB%D8%A7%D9%85%D9%86/383080f3-a72e-5c05-fd09-c7b5fb2c985b.
30. Haddrill R, Jones GL, Mitchell CA, et al. Understanding delayed access to antenatal care: a qualitative interview study. BMC Pregnancy Childbirth. 2014;14:207. doi:10.1186/1471-2393-14-207
31. Barber C, Rankin J, Heslehurst N. Maternal body mass index and access to antenatal care: a retrospective analysis of 619,502 births in England. BMC Pregnancy Childbirth. 2017;17(1):290. doi:10.1186/s12884-017-1475-5
32. Cresswell JA, Yu G, Hatherall B, et al. Predictors of the timing of initiation of antenatal care in an ethnically diverse urban cohort in the UK. BMC Pregnancy Childbirth. 2013;13:103. doi:10.1186/1471-2393-13-103
33. Asundep NN, Carson AP, Turpin CA, et al. Determinants of access to antenatal care and birth outcomes in Kumasi, Ghana. J Epidemiol Glob Health. 2013;3(4):279–288. doi:10.1016/j.jegh.2013.09.004
34. Titaley CR, Dibley MJ, Roberts CL. Factors associated with underutilization of antenatal care services in Indonesia: results of Indonesia Demographic and Health Survey 2002/2003 and 2007. BMC Public Health. 2010;10:485. doi:10.1186/1471-2458-10-485
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.