Back to Journals » Infection and Drug Resistance » Volume 16
In vitro Synergistic Activity of Ceftazidime-Avibactam in Combination with Aztreonam or Meropenem Against Clinical Enterobacterales Producing blaKPC or blaNDM
Authors Kuai J, Zhang Y, Lu B ![]() , Chen H
, Chen H ![]() , Zhang Y, Li H
, Zhang Y, Li H ![]() , Wang Y, Wang Q, Wang H, Wang X
, Wang Y, Wang Q, Wang H, Wang X
Received 11 February 2023
Accepted for publication 3 May 2023
Published 23 May 2023 Volume 2023:16 Pages 3171—3182
DOI https://doi.org/10.2147/IDR.S408228
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Suresh Antony
Junyang Kuai,1 Yawei Zhang,1 Binghuai Lu,2 Hongbin Chen,1 Yulin Zhang,2 Henan Li,1 Yuanyuan Wang,3 Qi Wang,1 Hui Wang,1 Xiaojuan Wang1
1Department of Clinical Laboratory, Peking University People’s Hospital, Beijing, People’s Republic of China; 2Department of Pulmonary and Critical Care Medicine, Laboratory of Clinical Microbiology and Infectious Diseases, Center for Respiratory Diseases, National Clinical Research Center of Respiratory Diseases, China-Japan Friendship Hospital, Beijing, People’s Republic of China; 3Department of Clinical Medical Laboratory, the First Affiliated Hospital of Henan University of Science and Technology, Luoyang, People’s Republic of China
Correspondence: Xiaojuan Wang, Department of Clinical Laboratory, Peking University People’s Hospital, Beijing, People’s Republic of China, Tel/Fax +86 010 8832 6310, Email [email protected]; [email protected]
Background: It is often challenging to select appropriate combination therapies to treat infections caused by carbapenem-resistant Enterobacterales (CRE) with high-level resistance to carbapenem.
Methods: We investigated the in vitro synergistic activity of ceftazidime-avibactam-, polymyxin- or tigecycline-, and meropenem-based combinations using checkerboard assays against 16 CRE including Klebsiella pneumoniae carrying blaKPC-2 (CR1-blaKPC-2) and Enterobacter cloacae carrying blaNDM-1 (CR2-blaNDM-1) with meropenem MICs ≥ 128 mg/L. Time-kill assays were used to observe synergistic bactericidal activity.
Results: Meropenem in combination with ertapenem, amikacin, tigecycline or polymyxin B, and tigecycline plus ceftazidime-avibactam showed weak synergistic activities against CR1-blaKPC-2 and CR2-blaNDM-1. Polymyxin B combined with tigecycline or ceftazidime-avibactam, and ceftazidime-avibactam plus amikacin showed synergistic effects against two tigecycline-non-susceptible KPC-producers or three ceftazidime-avibactam-resistant NDM-producer, and 50% (5/10) of strains with amikacin MICs ≥ 4096 mg/L, respectively. Synergistic interactions of ceftazidime-avibactam plus aztreonam or meropenem in checkerboard assays were measured for 100% (16/16) and 93.8% (15/16) of strains, respectively. The time-kill assay further verified that the ceftazidime-avibactam combination had the potential to restore aztreonam susceptibility and reduced meropenem MICs to 8 mg/L.
Conclusion: Ceftazidime-avibactam plus aztreonam or meropenem could be an effective strategy for treating CRE infections, particularly those with high-level resistance to carbapenems and/or ceftazidime-avibactam.
Keywords: ceftazidime-avibactam, checkerboard assays, time-kill assays, synergistic effect, meropenem, aztreonam
Introduction
Carbapenem-resistant Enterobacterales (CRE), owing to its multi-drug resistance and worldwide dissemination characteristics associated with high morbidity and mortality, is an urgent public health concern.1,2 A longitudinal large-scale CRE network in China showed that meropenem minimal inhibitory concentration (MIC) for 89.0% of KPC-producing CREs and 62.3% NDM-producing CREs were ≥8 mg/L.2 The antibiotics used for CRE treatment are limited, and only left salvage antibiotics such as tigecycline, polymyxin, and ceftazidime-avibactam (approved in China in 2019). Polymyxin shows nephrotoxicity and neurotoxicity, and tigecycline has low free serum concentrations. Ceftazidime-avibactam shows activity against ESBL-, AmpC-, and serine-carbapenemase-producing Enterobacterales strains, including KPC and OXA-48 carbapenemases but not metallo-β-lactamases (MBLs).1 Moreover, tigecycline-, polymyxin-, and ceftazidime-avibactam-resistant strains have been isolated during clinical treatment. Previously reported polymyxin or ceftazidime-avibactam heteroresistance might be an important reason for treatment failure and repeated infections.3
Appropriate combination therapy is an important strategy for delaying the development of antibiotic-resistant bacteria. However, it is challenging to select appropriate combination drugs against CRE, particularly for those with high-level resistance to carbapenems. Regimens based on double carbapenems are recommended for CRE infections when the MICs of meropenem are ≤8 mg/L.4 Another report showed that double carbapenems work in vitro only if the meropenem MICs of the isolates are ≤128 mg/L.5 Whether in vitro tigecycline combinations are effective remains controversial. Previous reports have indicated that tigecycline enhances the synergistic bactericidal activity of polymyxin and meropenem.6 However, several other reports have indicated that tigecycline, in combination with polymyxin or meropenem, shows antagonistic effects.7,8 Polymyxin-based combinations have fallen out of favor due to the refutation of clinical trial data and concerns about pharmacokinetic/pharmacodynamics (PK/PD) and its toxicity.9 Tigecycline combined with polymyxin B shows low synergistic activity against 20% of CREs (5/25), 92% (23/25) of which the meropenem MICs were ≥16 mg/L, 24% (6/25) of which tigecycline MICs were ≥4 mg/L, and 36% (9/25) of which polymyxin MICs were >4 mg/L.10 The in vitro and in vivo assays of ceftazidime-avibactam-based combinations against CRE have been reported, whereas only few data show that the combination of each drug can restore drug susceptibility, particularly for high-level resistant strains. For MBL producers, ceftazidime-avibactam combined with aztreonam has been shown to exhibit a good synergistic effect in in vitro or in vivo animal infection models.11 Gaibani et al reported that ceftazidime-avibactam combined with meropenem/imipenem displayed synergistic effects against both ceftazidime-avibactam-susceptible (n = 11) and ceftazidime-avibactam-high-level resistant (n = 2, MICs ≥256 mg/L) KPC-producing CREs through gradient diffusion method, whereas this combination could restore meropenem susceptibility in 50% of KPC-3 producers but not in two ceftazidime-avibactam-susceptible KPC-2 producers.12
To obtain effective drug combinations targeting high-level-carbapenem resistant CREs, we investigated the synergistic activity of meropenem-, tigecycline-, polymyxin B-, and ceftazidime-avibactam-based combinations against Klebsiella pneumoniae carrying blaKPC-2 (CR1-blaKPC-2), Enterobacter cloacae carrying blaNDM-1 (CR2-blaNDM-1), and 14 other CREs using checkerboard assays that were then validated using time-kill assays. We then investigated whether the synergistic combinations could restore the susceptibility of the combined drugs using time-kill assays.
Materials and Methods
Ethics
The study was approved by the research ethics board at Peking University People’s Hospital, a tertiary care teaching hospital (Approval No. 2019PHB233-01) and was approved by each participating hospital according to local requirements. Informed consent was not required because only strains isolated from patients were involved. The data were anonymous.
Bacterial Strains
A total of 16 non-duplicate clinical CREs were collected. Fifteen CREs were isolated from viral pneumonia patients secondary to or co-infection with CRE from two tertiary hospitals in Beijing and one teaching hospital in Henan Province between 1 Jan 2018 and 31 Mar 2021. Three out of 15, five out of 15, and seven out of 15 strains were isolated from blood, sputum, and bronchoalveolar lavage fluid, respectively. Another strain isolated from urine in 2017 was collected from the CRE network in China. These strains included 12 K. pneumoniae, two E. cloacae, and two E. coli. The strains were identified by MALDI-TOF-MS (Bruker Daltonik, Bremen, Germany).
Antimicrobial Susceptibility Testing
The MICs of meropenem, ceftazidime-avibactam (avibactam was fixed at the concentration of 4 mg/L), aztreonam, tigecycline, amikacin, and polymyxin B were initially determined by the broth microdilution method.13 Each experiment was performed in triplicate. E. coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853 were used as quality control strains.
Whole Genome Sequencing, Antimicrobial Resistance Genes and MLST Analysis
Genomic DNA was extracted using TIANamp Bacteria DNA Kit (Tiangen, Beijing, China) according to the manufacturer’s protocol. Library preparation and sequencing were performed by Illumina HiSeq 2000 platform (2×100 bp) second-generation sequencing platform. Reads were assembled and annotated using SPAdes (version 3.13.0).14 MLST and plasmid-mediated antimicrobial resistance genes were analyzed based on the MLST database (https://cge.cbs.dtu.dk/services/MLST/) and ResFinder database (https://cge.cbs.dtu.dk/services/ResFinder) from the CGE online website, respectively.
Checkerboard Assays
Checkerboard assays were carried out as previously described10 with some modifications. Briefly, 100 µL of a 1:100 dilution of 0.5 McFarland bacterial suspension liquid (5×108 CFU/mL) was added to a mixture of serial gradient diluted concentrations of 50 µL of drug A and 50 µL of drug B. Checkerboard assays were performed for three biological replicates. The plates were incubated at 37 °C for 16–18 h. The FICI was calculated and interpreted as described previously:15 For the two antibiotics A and B acting alone and in combination, the FICI was calculated as the MIC of drug A in combination / the MIC of drug A alone + the MIC of drug B in combination / the MIC drug B alone. FICI≤ 0.5, synergy; 0.5 < FICI ≤ 1, additive; FICI 1 < FICI < 2, indifference, and FICI ≥ 2, antagonism.15
Time-Kill Assays
Time-kill assays for ceftazidime-avibactam plus meropenem or aztreonam were carried out according to the reference.16 Considering the high MIC values of these three antibiotics against CR1-blaKPC-2 and CR2-blaNDM-1, the ceftazidime-avibactam plus meropenem or aztreonam combination assays were performed with each drug at the concentration of 1/4× MIC, 1/8× MIC, 1/16× MIC, 1/32× MIC, 1/64× MIC and 1/128× MIC, respectively. To determine whether the susceptible breakpoint concentration of ceftazidime-avibactam (8 mg/L) could reduce meropenem or aztreonam MICs to their respective susceptible breakpoint concentrations, the time-kill assays were examined at the concentration of 4 or 8 mg/L of ceftazidime-avibactam plus the concentration of 2, 4 or 8 mg/L of aztreonam or meropenem. All tests were performed in duplicate. Bactericidal activity was defined as a decrease of ≥3 log10 CFU/mL in colony count compared to the initial inoculum. Synergistic effect was defined as a ≥2 log10 CFU/mL reduction in colony count at 24 h compared with the most active single drugs.16
Statistical Analysis
Statistical analysis was performed using GraphPad Prism (Version 9.1.1, San Diego, California USA).
Results
Meropenem-Based Combination with Ertapenem, Amikacin, Tigecycline, or Polymyxin B Was Ineffective Against CREs with High-Level Resistance to Carbapenems
CR1-blaKPC-2 and CR2-blaNDM-1 were highly resistant to meropenem (MICs ≥128 mg/L) and ertapenem (MICs ≥128 mg/L) according to the Clinical and Laboratory Standards Institute (CLSI) guidelines in 2022.17 (Table 1). Meropenem plus ertapenem did not show synergistic effects but displayed additive, indifferent, and antagonistic effects against 25% (4/16), 43.8% (7/16), and 31.3% (5/16) of the strains, respectively (Table 1).
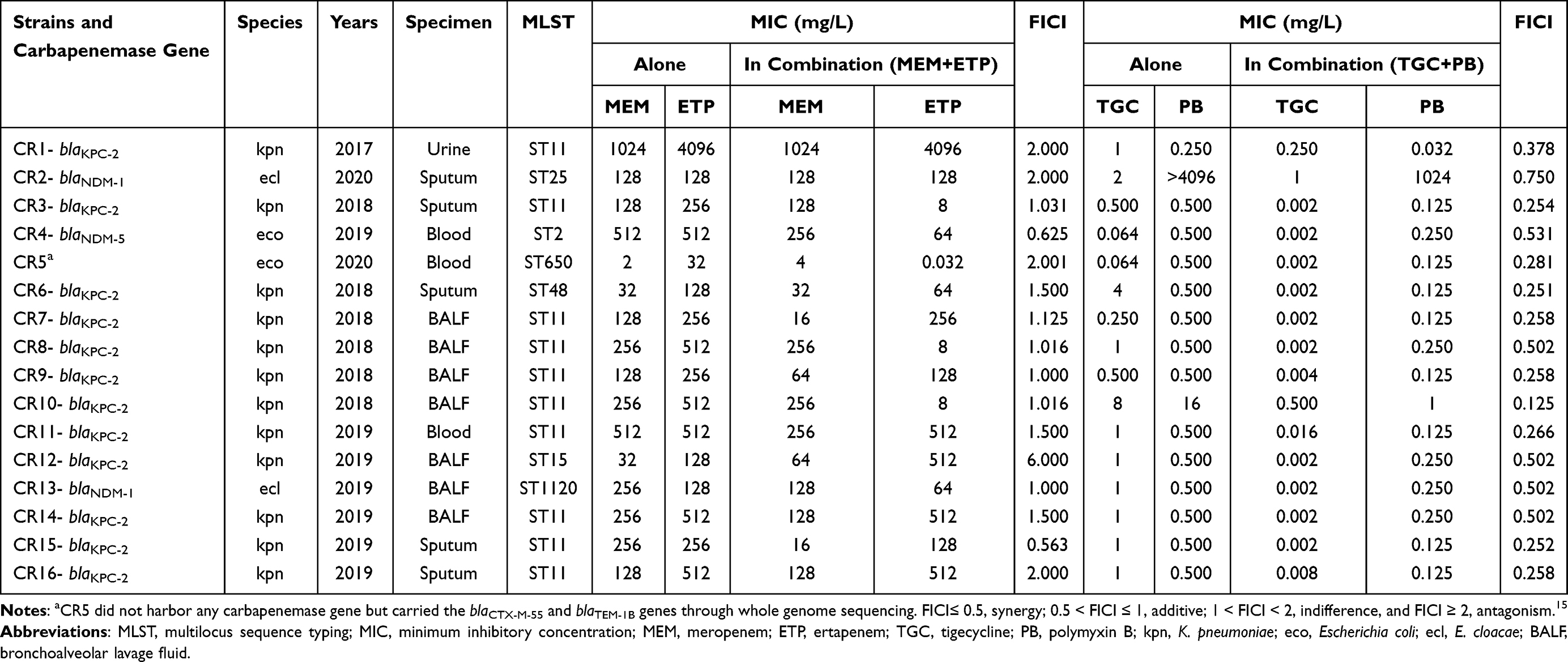 |
Table 1 Characteristics of Genotypic Background, MICs, and Synergy Detecting Results of Meropenem Plus Ertapenem and Tigecycline Plus Polymyxin B by Checkerboard Assays Against 16 CRE |
CR1-blaKPC-2 was highly resistant to amikacin (MIC >4096 mg/L), whereas CR2-blaNDM-1 was susceptible (MIC = 8 mg/L). Synergistic effects were not observed for meropenem combined with amikacin for these two strains (FICI were 2.000 and 0.625, respectively, Data not shown).
CR1-blaKPC-2 was susceptible to polymyxin B (MIC = 0.25 mg/L), whereas CR2-blaNDM-1 was highly resistant (MIC >4096 mg/L). Meropenem plus polymyxin B showed an indifferent effect against CR1-blaKPC-2 (FICI = 1.001). Although this combination demonstrated a synergistic effect against CR2-blaNDM-1 (FICI = 0.375), synergy only decreased the meropenem MIC from 128 to 16 mg/L and polymyxin B from >4096 to 1024 mg/L (Data not shown).
Both CR1-blaKPC-2 (MIC = 1 mg/L) and CR2-blaNDM-1 (MIC = 2 mg/L) were susceptible to tigecycline according to the US Food and Drug Administration standard (www.fda.gov). Synergistic effects were not observed when meropenem was combined with tigecycline (FICI of CR1-blaKPC-2 and CR2-blaNDM-1 were 1.001 and 1.000, respectively, Data not shown).
Tigecycline Combined with Ceftazidime-Avibactam Was Ineffective Against CREs with High-Level Resistance to Carbapenems
Ceftazidime-avibactam showed indifferent and antagonistic effects against 50% (5/10) and 50% (5/10) of the strains that were susceptible to both tigecycline and ceftazidime-avibactam, respectively (Table 2). For four strains susceptible to tigecycline and resistant to ceftazidime-avibactam, ceftazidime-avibactam plus tigecycline showed synergistic, indifferent, and antagonistic effects against 25% (1/4), 50% (2/4), and 25% (1/4) of the strains, respectively. For two strains susceptible to ceftazidime-avibactam and non-susceptible to tigecycline, ceftazidime-avibactam plus tigecycline showed antagonistic effects (Table 2).
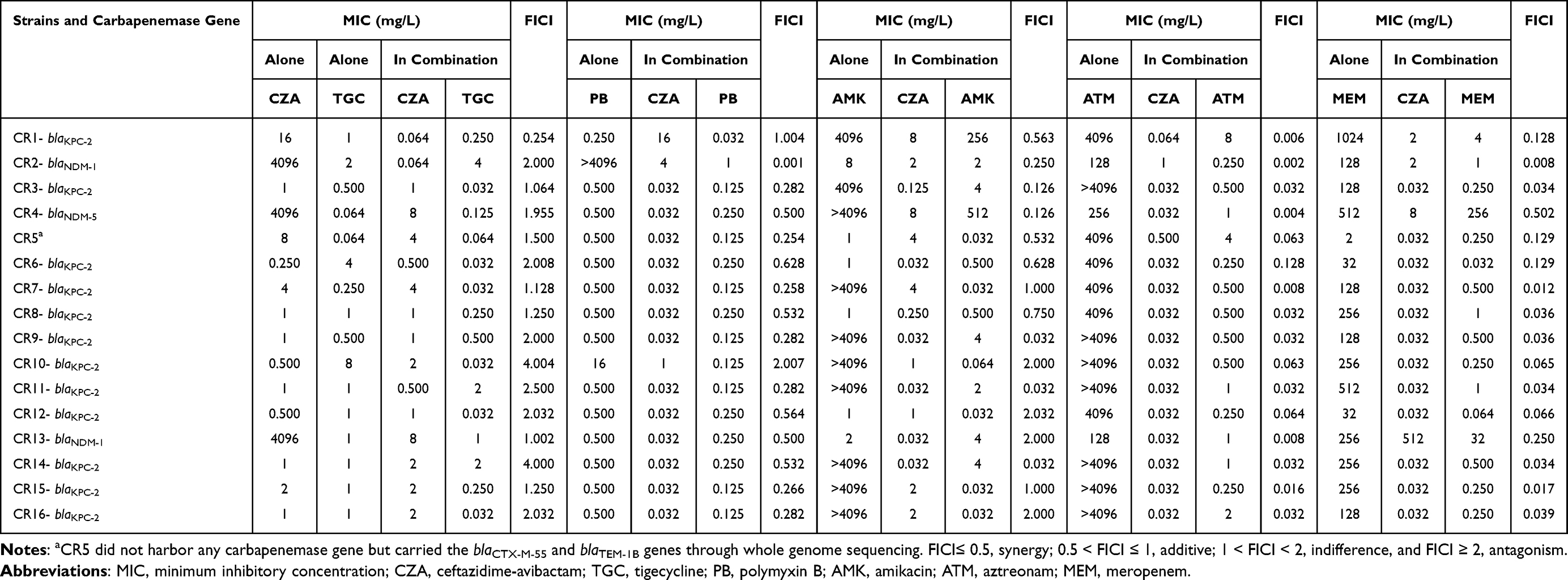 |
Table 2 MICs and Synergy Detecting Results of Ceftazidime-Avibactam in Combination with Tigecycline, Polymyxin B, Amikacin, Aztreonam, or Meropenem by Checkerboard Assays Against 16 CRE |
Polymyxin B Combined with Tigecycline or Ceftazidime-Avibactam Showed Moderate Synergy Rates Against CREs
For the 13 strains susceptible to both polymyxin B and tigecycline, polymyxin B plus tigecycline showed synergistic effects against 61.5% (8/13) and additive effects against 38.5% (5/13) of them, respectively (Table 1). This combination also showed synergistic effects against CR6-blaKPC-2, which exhibited intermediate to tigecycline (4 mg/L) and was susceptible to polymyxin B. Although CR10-blaKPC-2 showed low-level resistance to polymyxin B (MIC = 16 mg/L) and tigecycline (MIC = 8 mg/L), polymyxin B plus tigecycline showed a synergistic effect, reducing the MIC of polymyxin B from 16 to 1 mg/L and that of tigecycline from 8 to 0.5 mg/L. However, for CR2-blaNDM-1 with high-level resistance to polymyxin B (MIC >4096 mg/L) and susceptibility to tigecycline (MIC = 2 mg/L), this combination only showed additive effects, where the MIC of tigecycline was reduced from 2 to 1 mg/L and that of polymyxin B from >4096 to 1024 mg/L.
Polymyxin B plus ceftazidime-avibactam showed synergistic and additive activities against 63.6% (7/11) and 36.4% (4/11) of the strains susceptible to both polymyxin B and ceftazidime-avibactam, respectively (Table 2). For ceftazidime-avibactam-resistant and polymyxin B-susceptible strains, polymyxin B plus ceftazidime-avibactam showed synergistic and indifferent effects against 66.6% (2/3) and 33.3% (1/3) strains, respectively. This combination also showed synergistic effects against CR2-blaNDM-1 with high-level resistance to polymyxin B (MIC >4096 mg/L) and ceftazidime-avibactam (MIC = 4096 mg/L). Synergy reduced the polymyxin B MIC from >4096 to 1 mg/L and that of ceftazidime-avibactam from 4096 to 4 mg/L.
Ceftazidime-Avibactam Combined with Amikacin Showed Partial Synergistic Activity Against CREs with High-Level Resistance to Carbapenems
Ceftazidime-avibactam plus amikacin showed no synergistic effect against strains susceptible to both drugs (Table 2). For eight ceftazidime-avibactam-susceptible and high-level amikacin-resistant strains (amikacin MICs ≥4096 mg/L), ceftazidime-avibactam combined with amikacin showed synergistic effects against 50% (4/8) strains, reducing amikacin MICs to ≤4 mg/L. For CR4-blaNDM-5 with ceftazidime-avibactam and amikacin MICs of ≥4096 mg/L, the ceftazidime-avibactam plus amikacin combination only reduced the ceftazidime-avibactam MIC to 8 mg/L and that of amikacin to 512 mg/L.
Ceftazidime-Avibactam-Based Combinations with Aztreonam or Meropenem Showed Excellent Synergistic Activities
Excellent synergistic effects were observed for ceftazidime-avibactam plus aztreonam or meropenem against 100% (16/16) or 93.8% (15/16) of CREs in the checkerboard assays, 81.3% (13/16) of which the meropenem MICs were ≥128 mg/L and 25% (4/16) were resistant to ceftazidime-avibactam (ceftazidime-avibactam MICs of three blaNDM-producing strains were 4096 mg/L) (Table 2).
In time-kill assays, for CR1-blaKPC-2 with a ceftazidime-avibactam MIC of 16 mg/L, 1/32× MIC ceftazidime-avibactam plus 1/32× MIC aztreonam (128 mg/L) showed excellent bactericidal effects with a 3.97 log10 CFU/mL reduction in bacterial population after 24 h of incubation (Figure 1A). For CR2-blaNDM-1 with a ceftazidime-avibactam MIC of 4096 mg/L, 1/64× MIC ceftazidime-avibactam (64 mg/L) plus 1/64× MIC aztreonam (2 mg/L) displayed a bactericidal effect with a 4.48 log10 CFU/mL reduction in bacterial population after 24 h of incubation (Figure 1B). For CR1-blaKPC-2, 1/32× MIC ceftazidime-avibactam (0.5 mg/L) plus 1/32× MIC meropenem (32 mg/L) showed excellent bactericidal effects with a 5.93 log10 CFU/mL reduction at 24 h (Figure 1C). For CR2-blaNDM-1, 1/4× MIC ceftazidime-avibactam (1024 mg/L) plus 1/4× MIC meropenem (32 mg/L) showed a synergistic but not bactericidal effect, with a 2.8 log10 CFU/mL reduction compared to that of single drugs at 24 h (Figure 1D).
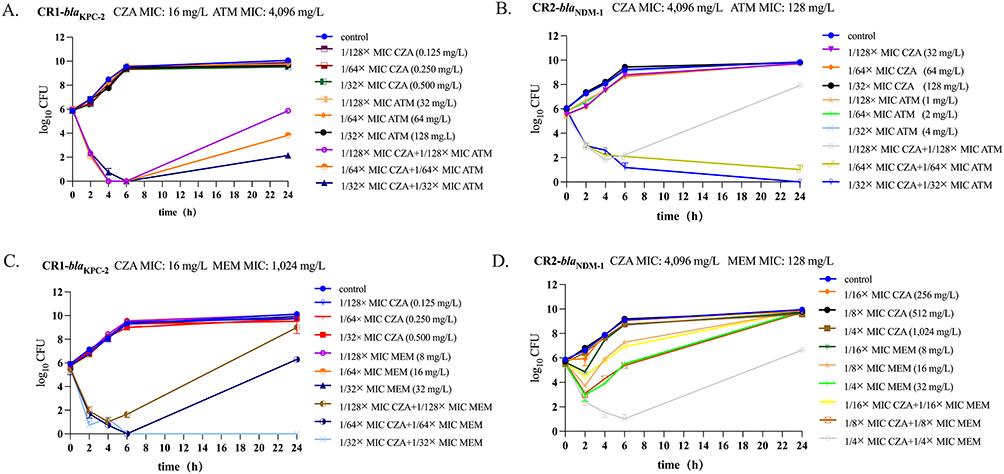 |
Figure 1 Time-kill assays against CR1-blaKPC-2 and CR2-blaNDM-1 in incubation with ceftazidime-avibactam (CZA) alone and ceftazidime-avibactam (CZA) in combination with aztreonam (ATM) or meropenem (MEM). Curves represent average concentrations of duplicate experiments. (A) CZA in combination with ATM against CR1-blaKPC-2 via time-kill assays at the concentration of 1/128× MIC CZA plus 1/128× MIC ATM, 1/64× MIC CZA plus 1/64× MIC ATM and 1/32× MIC CZA plus 1/32× MIC ATM. (B) CZA in combination with ATM against CR2-blaNDM-1 via time-kill assays at the concentration of 1/128× MIC CZA plus 1/128× MIC ATM, 1/64× MIC CZA plus 1/64× MIC ATM and 1/32× MIC CZA plus 1/32× MIC ATM. (C) CZA in combination with MEM against CR1-blaKPC-2 via time-kill assays at the concentration of 1/128× MIC CZA plus 1/128× MIC MEM, 1/64× MIC CZA plus 1/64× MIC MEM, and 1/32× MIC CZA plus 1/32× MIC MEM. (D) CZA in combination with MEM against CR2-blaNDM-1 via time-kill assays at the concentration of 1/16× MIC CZA plus 1/16× MIC MEM, 1/8× MIC CZA plus 1/8× MIC MEM, and 1/4× MIC CZA plus 1/4× MIC MEM. |
Ceftazidime-Avibactam Has Potential to Restore Aztreonam Susceptibility and Reduce the MICs of Meropenem to 8 Mg/L
For CR1-blaKPC-2 and CR2-blaNDM-1, additional time-kill assays were performed to explore whether treatment with the susceptible breakpoint concentration of ceftazidime-avibactam (8 mg/L) could reduce meropenem or aztreonam MICs to their respective susceptible breakpoint concentrations (the susceptible breakpoint concentrations of meropenem and aztreonam were 1 mg/L and 4 mg/L, respectively, according to the CLSI guidelines in 2022).
Bactericidal effects were observed for the combination of 1/4× MIC ceftazidime-avibactam (4 mg/L) plus 1/512× MIC aztreonam (8 mg/L) against CR1-blaKPC-2 (Table 3). For CR2-blaNDM-1, 1/1024× MIC ceftazidime-avibactam (4 mg/L) plus 1/64× MIC aztreonam (2 mg/L) showed bactericidal effects that started at 2 h and lasted until 24 h (Table 3).
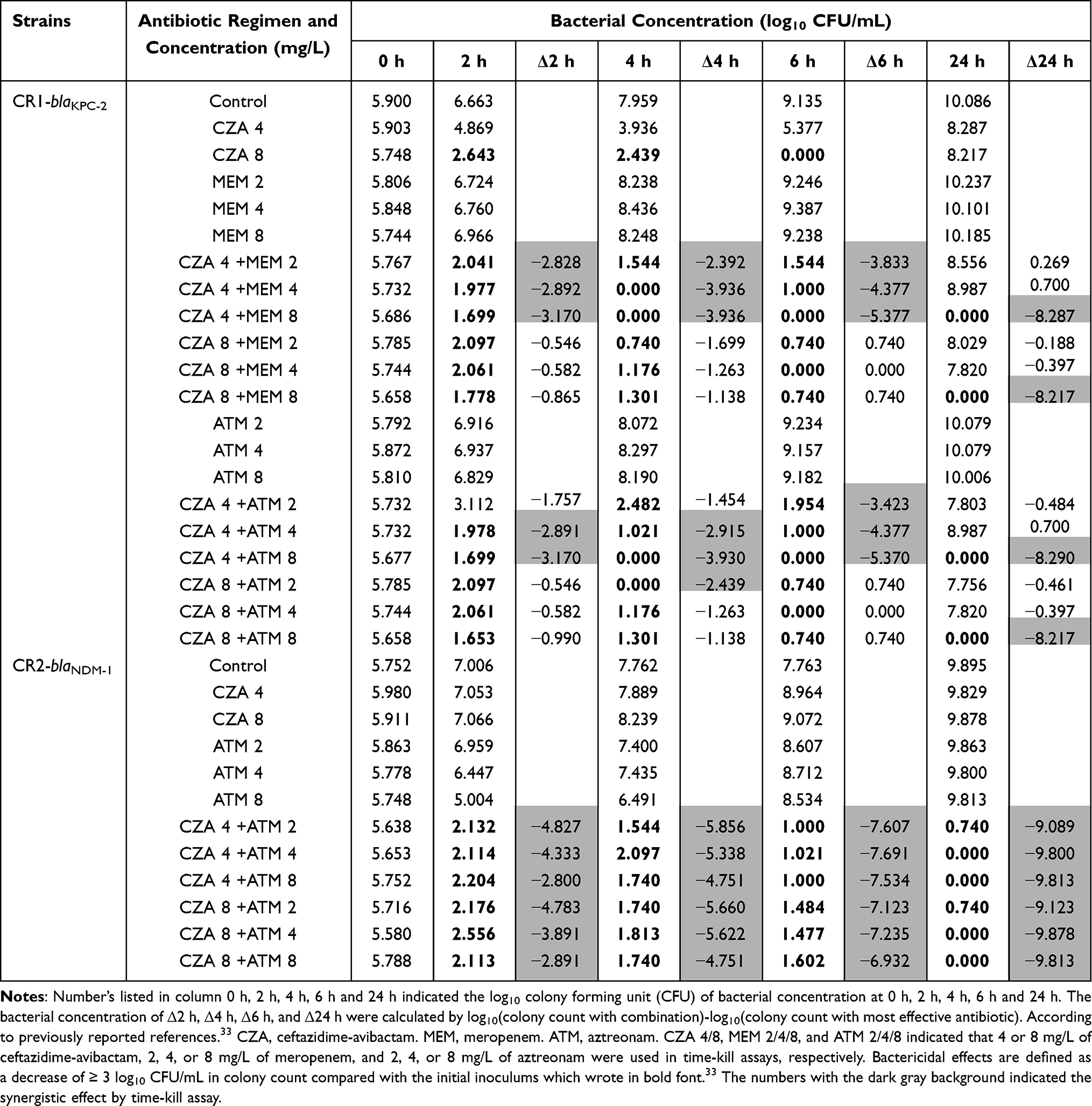 |
Table 3 Time-Kill Assays Against CR1-blaKPC-2 and CR2-blaNDM-1 at the Concentration of 4 or 8 Mg/L of Ceftazidime-Avibactam in Combination with 2, 4, or 8 Mg/L of Meropenem or Aztreonam |
For CR1-blaKPC-2, 1/4× MIC ceftazidime-avibactam (4 mg/L) plus 1/128× MIC meropenem (8 mg/L) showed bactericidal effects with a 5.68 log10 CFU/mL reduction after 24 h of incubation (Table 3). However, 1/2× MIC ceftazidime-avibactam (8 mg/L) plus 1/256× MIC or 1/512× MIC (2 or 4 mg/L) meropenem showed indifferent activity (Data not shown).
Discussion
Combination therapy is recommended as an effective measure to treat CRE infections because of limited salvage therapy drugs.5,18 However, identifying potential combination drugs is challenging.4,19 Thus, we evaluated the synergistic activity of meropenem, tigecycline, polymyxin, and ceftazidime-avibactam-based combinations to explore in vitro evidence of the combined use of these antibiotics.
A double-carbapenem combination has been suggested to treat CRE infections.4 Previous studies have shown that the double-carbapenem regimen has great synergy against 100% (33/33) of carbapenemase-producing K. pneumoniae isolates with meropenem MICs ≤128 mg/L.20 In this study, indifferent and antagonistic effects were observed against three strains with meropenem MICs <128 mg/L. For the 13 strains with meropenem MICs ≥128 mg/L, meropenem plus ertapenem did not display synergism but rather additive effects against 38.5% (5/13) of the strains and indifferent and/or antagonistic effects against 61.5% (8/13) of the strains. Thus, meropenem plus ertapenem might be not recommended for the treatment of CREs.
In our previous longitudinal large-scale CRE network in China, 1801 CRE isolates showed high susceptibility to colistin (96.9%), tigecycline (89.7%), and amikacin (54.5%).2 Thus, tigecycline, polymyxin B or amikacin combined with meropenem was a good choice to treat CRE infections. A previous study from our research group showed that meropenem combined with tigecycline or polymyxin shows low synergy against 4% (1/25) or 20% (5/25) of CREs with meropenem MICs >16 mg/L, respectively.10 Meropenem plus amikacin has a synergistic effect and maintains bactericidal activity against 100% (4/4) of MBL- and KPC-producing E. cloacae strains susceptible to amikacin.21 In this study, the meropenem-based combination with amikacin, tigecycline, and polymyxin B did not show synergistic effects but rather additive and indifferent effects against CREs with high-level resistance to carbapenem. It is suggested that when combating strains with high-level resistance to carbapenems, amikacin, tigecycline, or polymyxin B in combination with meropenem may be ineffective.
Because of the results showing high susceptibility to tigecycline and polymyxin B in the CRE network surveillance conducted in China,2 these two drug combinations were potential candidates to combat CRE infections. In this study, this drug combination showed synergistic effects against 61.5% (8/13) of polymyxin B-and-tigecycline-susceptible strains. The combination showed synergistic effects against two tigecycline-non-susceptible KPC producers but was ineffective against one high-level polymyxin B-resistant NDM producer. This indicated that tigecycline combined with polymyxin B could be considered when strains have low-level resistance to polymyxin B or tigecycline but could be not suitable for high-level polymyxin B-resistant strains.
As international consensus guidelines suggest, an average steady-state concentration of approximately 2–4 mg/L polymyxin B is a safe and effective concentration range.22 Previous studies have shown that ceftazidime-avibactam plus polymyxin B shows synergistic effects against 69.4% (25/36) of isolates with polymyxin B MICs ≥4 mg/L.23 In this study, polymyxin B plus ceftazidime-avibactam showed synergistic effects against 63.6% (7/11) of the strains susceptible to both drugs. Synergistic effects were also observed in the three ceftazidime-avibactam-resistant NDM producers. For CR2-blaNDM-1 with high-level resistance to polymyxin and ceftazidime-avibactam (MIC ≥4096 mg/L), ceftazidime-avibactam plus polymyxin B also showed synergistic effects and could restore susceptibility to these two drugs, with ≥4096-fold MIC reductions. These results imply that ceftazidime-avibactam plus polymyxin B may be a potential clinical option to combat high-level polymyxin B-and-ceftazidime-avibactam-resistant CRE infections, which could reduce polymyxin B concentrations to safe and effective levels.
Combination therapy is recommended to prevent the emergence of ceftazidime-avibactam resistance. Ceftazidime-avibactam plus tigecycline showed low synergy percentages against 12.5% (1/8) of KPC-producing K. pneumoniae and none of the NDM-producing K. pneumoniae strains.24 This study also confirmed that tigecycline plus ceftazidime-avibactam displayed low synergistic effects [43.8% (7/16) of strains with indifferent effects and 50% (8/16) with antagonistic effects] against KPC- and NDM-producing CREs. Even if the strains were susceptible to both drugs, the combination still showed no synergistic antibacterial effect. Thus, ceftazidime-avibactam and tigecycline combinations should be used with caution.
Amikacin, an aminoglycoside, is recommended for therapy against CRE when used in combination with other effective antibiotics.16 Tao et al reported that ceftazidime-avibactam combined with amikacin showed a synergistic effect against 47.6% (10/21) of ceftazidime-avibactam-resistant Gram-negative isolates.16 In this study, ceftazidime-avibactam plus amikacin showed synergy against 37.5% (6/16) of CREs, four of which were susceptible to ceftazidime-avibactam and resistant to amikacin with MICs ≥4096 mg/L. This indicated that ceftazidime-avibactam plus amikacin could be suitable for the treatment of CRE infections caused by strains susceptible to ceftazidime-avibactam and with high levels of resistance to amikacin.
Ceftazidime-avibactam plus meropenem showed synergistic effects against both ceftazidime-avibactam-susceptible and ceftazidime-avibactam-resistant CREs. This combination showed excellent synergistic activities against all ceftazidime-avibactam-susceptible CREs and 75% (3/4) of ceftazidime-avibactam-resistant CREs. These results were consistent with that of Gaibani et al, who also found that ceftazidime-avibactam combined with meropenem showed a 100% (13/13) synergistic effect.12 Extended infusion of meropenem can achieve an ideal concentration in vivo in critically ill patients and is increasingly recommended to treat CRE infections when the meropenem MICs of the isolated strains are ≤8 mg/L.25,26 In this study, added with the susceptible breakpoint concentration of ceftazidime-avibactam (8 mg/L) did not reduce the meropenem MIC to its susceptible breakpoint (1 mg/L) but still reduced it to 8 mg/L, although the strains were highly resistant to meropenem (MIC ≥128 mg/L). The synergistic mechanism of ceftazidime-avibactam and meropenem may be related to the increased affinity of bacteria penicillin-binding proteins (PBPs) to these two drugs, because meropenem tends to exhibit highly-affinity binding to PBP2 for inhibiting the bacteria cell wall synthesis, while PBP3 with high affinity to ceftazidime.27,28 In addition, avibactam could protect meropenem from hydrolyzing by serine β-lactamases including serine-carbapenemases.
The combination of ceftazidime-avibactam and aztreonam is particularly effective against MBL producers, such as NDM-producing bacteria.29 Previous studies have shown that ceftazidime-avibactam combined with aztreonam shows synergistic effects against 97.5% (39/40) of the strains, including NDM producers and MBL and KPC co-producers.30 Another research also found that the FICI values of ceftazidime-avibactam combined with aztreonam against 37 NDM-, IMP-, KPC+IMP- or KPC+NDM-co-producing isolates with ceftazidime-avibactam MICs ≥128 mg/L were all below 0.51.31 In this study, when combined with aztreonam, ceftazidime-avibactam exhibited excellent synergistic activity with 100% synergism in checkerboard assays, which could be used as the preferred combination to treat CRE strains, although the MICs of meropenem reached 128 mg/L or even higher. In time-kill assays, ceftazidime-avibactam combined with aztreonam reduced the ceftazidime-avibactam and aztreonam MIC of CR2-blaNDM-1 to the susceptible breakpoint (4 mg/L) or lower. Due to aztreonam not hydrolyzed by MBLs and avibactam protecting aztreonam/ceftazidime from inactivating by serine β-lactamases including serine-carbapenemases, ceftazidime-avibactam combined with aztreonam could overcome the limitation of ceftazidime-avibactam ineffectiveness against MBL-producing strains.32 Taken together, ceftazidime-avibactam combined with aztreonam could have potential for use in therapeutic strategies against CREs with high-level carbapenem resistance.
This study provides in vitro evidence of dual-drug combinations against high-level carbapenem-resistant CRE strains. Among all combinations, ceftazidime-avibactam plus aztreonam and ceftazidime-avibactam plus meropenem showed the best in vitro synergistic antibacterial activities against CREs with high-level resistance to carbapenems. It was further found that the susceptible breakpoint (8 mg/L) or low concentrations of ceftazidime-avibactam (4 mg/L) plus aztreonam (2 mg/L) or meropenem (8 mg/L) had excellent in vitro efficacy, reducing the aztreonam and meropenem MIC values to the susceptible breakpoint (4 mg/L) and 8 mg/L, respectively.
This study had some limitations. Firstly, tests were only performed during in vitro combinations; therefore, in vivo experiments are needed to further verify the synergistic activities observed. Secondly, the drug synergistic mechanisms, particularly for ceftazidime-avibactam plus meropenem, remain unclear and require further investigation.
Conclusion
Ceftazidime-avibactam plus aztreonam or meropenem could be effective against CRE regardless of whether the strains are highly or poorly resistant to carbapenems and/or ceftazidime-avibactam.
Acknowledgments
This research was funded by the National Natural Science Foundation of China (grant number 81971975) and the National Key Research and Development Program of China (grant number 2018YFC1200102). The authors acknowledge Chunlei Wang from China-Japan Friendship Hospital for providing CRE isolates.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Palacios-Baena ZR, Giannella M, Manissero D, et al. Risk factors for carbapenem-resistant Gram-negative bacterial infections: a systematic review. Clin Microbiol Infect. 2021;27(2):228–235. doi:10.1016/j.cmi.2020.10.016
2. Wang Q, Wang X, Wang J, et al. Phenotypic and genotypic characterization of carbapenem-resistant Enterobacteriaceae: data from a longitudinal large-scale CRE study in China (2012-2016). Clin Infect Dis. 2018;67(suppl_2):S196–S205.
3. Stojowska-Swędrzyńska K, Łupkowska A, Kuczyńska-Wiśnik D, et al. Antibiotic heteroresistance in Klebsiella pneumoniae. Int J Mol Sci. 2021;23(1): 449.
4. Lu J, Qing Y, Dong N, et al. Effectiveness of a double-carbapenem combinations against carbapenem-resistant Gram-negative bacteria. Saudi Pharm J. 2022;30(6):849–855.
5. Rodríguez-Baño J, Gutiérrez-Gutiérrez B, Machuca I, et al. Treatment of infections caused by extended-spectrum-beta-lactamase-, AmpC-, and carbapenemase-producing Enterobacteriaceae. Clin Microbiol Rev. 2018;31(2):e00079–17.
6. Zhang J, Yu L, Fu Y, et al. Tigecycline in combination with other antibiotics against clinical isolates of carbapenem-resistant Klebsiella pneumoniae in vitro. Ann Palliat Med. 2019;8(5):622–631.
7. Crémieux AC, Dinh A, Nordmann P, et al. Efficacy of colistin alone and in various combinations for the treatment of experimental osteomyelitis due to carbapenemase-producing Klebsiella pneumoniae. J Antimicrob Chemother. 2019;74(9):2666–2675.
8. Toledo PV, Aranha Junior AA, Arend LN, et al. The activity of antimicrobial combinations against KPC-2-producing Klebsiella pneumoniae in a rat model and time-kill assay. Antimicrob Agents Chemother. 2015;59(7):4301–4304.
9. Paul M, Daikos GL, Durante-Mangoni E, et al. Colistin alone versus colistin plus meropenem for treatment of severe infections caused by carbapenem-resistant Gram-negative bacteria: an open-label, randomised controlled trial. Lancet Infect Dis. 2018;18(4):391–400.
10. Zhou C, Wang Q, Jin L, et al. In vitro synergistic activity of antimicrobial combinations against blaKPC and blaNDM-Producing Enterobacterales with blaIMP or mcr genes. Front Microbiol. 2020;11:533209.
11. Zhang W, Guo Y, Li J, et al. In vitro and in vivo bactericidal activity of ceftazidime-avibactam against Carbapenemase-producing Klebsiella pneumoniae. Antimicrob Resist Infect Control. 2018;7:142.
12. Gaibani P, Lewis RE, Volpe SL, et al. In vitro interaction of ceftazidime-avibactam in combination with different antimicrobials against KPC-producing Klebsiella pneumoniae clinical isolates. Int J Infect Dis. 2017;65:1–3.
13. Clinical and Laboratory Standards Institute. M7-A10. Methods for Dilution Antimicrobial Susceptibility Tests for Bacteria That Grow Aerobically; Approved Standard.
14. Bankevich A, Nurk S, Antipov D, et al. SPAdes: a new genome assembly algorithm and its applications to single-cell sequencing. J Computational Biol. 2012;19(5):455–477.
15. European Committee for Antimicrobial Susceptibility Testing (EUCAST) of the European Society of Clinical Microbiology and Infectious Dieases (ESCMID). EUCAST Definitive Document E.Def 1.2, May 2000: terminology relating to methods for the determination of susceptibility of bacteria to antimicrobial agents. Clin Microbiol Infect. 2000;6(9):503–508.
16. Chen T, Xu W, Yu K, et al. In vitro activity of ceftazidime-avibactam alone and in combination with amikacin against colistin-resistant Gram-negative pathogens. Microb Drug Resist. 2021;27(3):401–409.
17. Clinical and Laboratory Standards Institute. Performance Standards for Antimicrobial Susceptibility Testing, Document. M100. Wayne, PA: CLSI; 2022:36–47.
18. Murray CJ, Ikuta KS, Sharara F, et al. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet. 2022;399(10325):629–655.
19. Mouton JW. Combination therapy as a tool to prevent emergence of bacterial resistance. Infection. 1999;27(Suppl 2):S24–8.
20. Oliva A, Scorzolini L, Cipolla A, et al. In vitro evaluation of different antimicrobial combinations against carbapenemase-producing Klebsiella pneumoniae: the activity of the double-carbapenem regimen is related to meropenem MIC value. J Antimicrob Chemother. 2017;72(7):1981–1984.
21. Kulengowski B, Rutter WC, Campion JJ, et al. Effect of increasing meropenem MIC on the killing activity of meropenem in combination with amikacin or polymyxin B against MBL- and KPC-producing Enterobacter cloacae. Diagn Microbiol Infect Dis. 2018;92(3):262–266.
22. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins: endorsed by the American College of Clinical Pharmacy (ACCP), European Society of Clinical Microbiology and Infectious Diseases (ESCMID), Infectious Diseases Society of America (IDSA), International Society for Anti-infective Pharmacology (ISAP), Society of Critical Care Medicine (SCCM), and Society of Infectious Diseases Pharmacists (SIDP). Pharmacotherapy. 2019;39(1):10–39.
23. Li Y, Guo S, Li X, et al. Evaluation of the in vitro synergy of polymyxin B-based combinations against polymyxin B -resistant Gram-negative bacilli. Microb Pathog. 2022;166:105517.
24. Ojdana D, Gutowska A, Sacha P, et al. Activity of ceftazidime-avibactam alone and in combination with ertapenem, fosfomycin, and tigecycline against carbapenemase-producing Klebsiella pneumoniae. Microb Drug Resist. 2019;25(9):1357–1364.
25. Lawandi A, Leite GC, Cheng MP, et al. Assessment of piperacillin-tazobactam-meropenem synergy against serine carbapenemase-producing Enterobacterales using Time-Kill assays. Antimicrob Agents Chemother. 2021;65(4):e02317–20.
26. Cojutti P, Sartor A, Righi E, et al. Population Pharmacokinetics of high-dose continuous-Infusion meropenem and considerations for use in the treatment of infections due to KPC-producing Klebsiella pneumoniae. Antimicrob Agents Chemother. 2017;61:e00794–17.
27. Zhang Y, Kashikar A, Brown CA, et al. Unusual Escherichia coli PBP 3 insertion sequence identified from a collection of carbapenem-resistant Enterobacteriaceae tested in vitro with a combination of ceftazidime-, ceftaroline-, or aztreonam-avibactam. Antimicrob Agents Chemother. 2017;61(8):e00389–17.
28. Sutaria DS, Moya B, Green KB, et al. First Penicillin-Binding Protein occupancy patterns of β-Lactams and β-Lactamase inhibitors in Klebsiella pneumoniae. Antimicrob Agents Chemother. 2018;62(6):e00282–18.
29. Meini S, Viaggi B, Tascini C. Mono vs. combo regimens with novel beta-lactam/beta-lactamase inhibitor combinations for the treatment of infections due to carbapenemase-producing Enterobacterales: insights from the literature. Infection. 2021;49(3):411–421.
30. Maraki S, Mavromanolaki VE, Moraitis P, et al. Ceftazidime-avibactam, meropenen-vaborbactam, and imipenem-relebactam in combination with aztreonam against multidrug-resistant, metallo-β-lactamase-producing Klebsiella pneumoniae. Eur J Clin Microbiol Infect Dis. 2021;40(8):1755–1759.
31. Lu G, Tang H, Xia Z, et al. In vitro and in vivo antimicrobial activities of ceftazidime/avibactam alone or in combination with aztreonam against carbapenem-resistant Enterobacterales. Infect Drug Resist. 2022;15:7107–7116.
32. Temkin E, Torre-Cisneros J, Beovic B, et al. Ceftazidime-Avibactam as salvage therapy for infections caused by carbapenem-resistant organisms. Antimicrob Agents Chemother. 2017;61(2):e01964–16.
33. Wistrand-Yuen P, Olsson A, Skarp KP, et al. Evaluation of polymyxin B in combination with 13 other antibiotics against carbapenemase-producing Klebsiella pneumoniae in time-lapse microscopy and time-kill experiments. Clin Microbiol Infect. 2020;26:1214–1221.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Simple Disk Stacking Plus Micro-Elution Method for Rapid Detection of the Synergistic Effect of Aztreonam and Ceftazidime/Avibactam Against Metallo-β-Lactamase Producing Enterobacterales
Liu Z, Hang X, Yan T, Chu W, Gong Z, Liu Y, Dai Y, Yang M, Li J, Zhou Q
Infection and Drug Resistance 2023, 16:1537-1543
Published Date: 15 March 2023
Aztreonam Acts as a Synergist for Ceftazidime/Avibactam Against Carbapenem-Resistant Enterobacteriaceae (CRE) of Various Carbapenemase Phenotypes in Southwestern China
Ruan X, Gong Z, Zeng M, Zhong Z, Chen Y, Wei F, Lei C, Zhu Y, Qin X, Li M
Infection and Drug Resistance 2025, 18:2243-2253
Published Date: 3 May 2025
A Tentative Clinical Study: Colistin Combined with Ceftazidime/Avibactam in the Treatment of Carbapenem-Resistant Gram-Negative Bacilli Infection

Zhang R, Zheng Z, Lu Y, Shi K, Lin Z, Tang S, Shao Z, Yang X, Liu J
Infection and Drug Resistance 2025, 18:3977-3991
Published Date: 9 August 2025
Combination of Ceftazidime-Avibactam and Meropenem for the Treatment of Pneumonia and Bloodstream Infections Caused by Pan-Drug Resistant Pseudomonas aeruginosa ST244: A Case Report
Kang Y, Kang S, Cui J
Infection and Drug Resistance 2026, 19:575082
Published Date: 17 April 2026