")
Back to Journals » Infection and Drug Resistance » Volume 16
In vitro Efficacy Evaluation of Leading Brands of Ciprofloxacin Tablets Found in Bishoftu City Against Salmonella Isolates, Central Ethiopia
Received 6 February 2023
Accepted for publication 10 March 2023
Published 14 March 2023 Volume 2023:16 Pages 1433—1440
DOI https://doi.org/10.2147/IDR.S402640
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Kenboni Geleta,1 Takele Beyene Tufa2
1SPANA Ethiopia Project of the College of Veterinary Medicine and Agriculture, Addis Ababa University, Bishoftu, Ethiopia; 2Department of Biomedical Sciences, College of Veterinary Medicine and Agriculture, Addis Ababa University, Bishoftu, Ethiopia
Correspondence: Takele Beyene Tufa, Tel +251 911 532131, Email [email protected]
Purpose: Salmonella Enteritidis (SE) and Salmonella Typhimurium (STM) are the serovars most frequently associated with human illness. Ciprofloxacin is most widely used to manage cases in adults. The present study aimed to evaluate the in vitro antibacterial activity of leading brands of ciprofloxacin (tablets) marketed in Bishoftu city against SE and STM serovars, and field isolates of Salmonella (non-serotyped) from dairy milk in central Ethiopia.
Methods: Five most widely prescribed ciprofloxacin brands (A-E) were subjected to in vitro efficacy evaluation against Salmonella isolates by using the disc diffusion method. The zone of inhibition (ZI) of the tested brands was compared with the standard disc and interpreted as susceptible, intermediate, and resistant.
Results: Out of 27 replicates (SE, STM, and field Salmonella isolates each = 9) tested for efficacy, the result revealed the mean ZI of the brands varies for all tested isolates (p < 0.05). The highest mean was recorded for Brand E (24.7± 0.71, 24.3± 0.50, and 19.5± 2.69) and lowest for Brand A (22.0± 0.87, 21.0± 0.87, and 10.7± 1.4) for field Salmonella isolates, STM and SE, respectively. All SE were resistant to four brands (Brand A-D) whereas 67% and 33% of them were resistant and intermediate to Brand E, respectively. Similarly, 33% of STM were resistant to Brand A while all the STM were intermediate to other brands. Furthermore, all non-serotyped field isolates of Salmonella were intermediate to all five tested ciprofloxacin brands with variable ranges of mean of ZI (p< 0.05).
Conclusion: The study revealed that Brand E was found to have relatively better efficacy against SE than other brands. The current study warrants a need for periodic surveillance of both the quality and efficacy of antibiotics to improve patient well-being and minimize the risk of antimicrobial resistance.
Keywords: antibacterial activity, ciprofloxacin brands, disc diffusion, resistance, Salmonella isolates
Introduction
Ciprofloxacin, a synthetic group of fluoroquinolones,1 is one of the most important antibiotic medications needed in the basic healthcare system. It is available in the list of essential medicines of the World Health Organization (WHO)2 and Ethiopia.3 It is available as a generic medication4 and is a first-line drug to manage enteric fever caused by the serovars most frequently associated with human illness [Salmonella Enteritidis (SE) and Salmonella Typhimurium (STM)].5
Generic drugs play key roles in decreasing health care costs,6,7 and they must be chemically and biopharmaceutically equivalent in comparison to the innovator drug.4,8 However, their qualities are in doubt in the case of resource-poor and developing countries.9 Generic antibiotics are widely used in healthcare facilities, which have become increasing the development of resistance by many common pathogens.8 The emergence of multidrug-resistant (MDR) strains became a major issue, resulting in the widespread use of ciprofloxacin as first-line therapy for adults infected with Salmonella species as well as MDR S. Typhi and S. Paratyphi.10–12 Reports indicate that inferior quality or substandard drugs are circulating in the market in the different developing world, and selling of such drugs has been widely reported in Africa, Asia, and Latin America.13 In 2003, the WHO reported that about 28% of fake antibiotics were reported between 1999 and 2002.14
The clinical efficacy of drug products can be ensured when their quality is reliable and reproducible.15,16 One under-recognized driver of antimicrobial resistance (AMR) is substandard and falsified (SF) or poor-quality medicines which can favor the selection of antibiotic-resistant strains9,17 and treatment failure.18 Substandard medicines are those that fail to meet standards or specifications of quality, while falsified medicines deliberately or even fraudulently misrepresent their identity, composition, or source.19 In various developing countries, poor-quality medicines is a public health concern and may have a significant impact on the national clinical and economic burden.20 A comprehensive analysis conducted in 2018 found that more than 12% of antibiotics circulating in low- and middle-income countries (LMICs) are SF medicines,13 suggesting a need for drug manufacturers to test their products during and after manufacturing to ensure the requisite quality.16
Despite the above facts, the information on the in vitro antibacterial activity of commonly used brands of ciprofloxacin in Bishoftu city in particular, and in Ethiopia in general, is absent. Thus, the availability of recent information is important to know the present trends of ciprofloxacin brands against pathogenic Salmonella strains, where ciprofloxacin is the first-line drug for the treatment of adult human salmonellosis. Therefore, this study aimed to evaluate and compare the efficacy of five leading brands of ciprofloxacin tablets commonly used in Bishoftu city, central Ethiopia against Salmonella serovars most frequently associated with human illness.
Materials and Methods
Study Area
The study was conducted in Bishoftu city, central Ethiopia. Laboratory investigation was also conducted in the veterinary pharmacology laboratory of the College of Veterinary Medicine and Agriculture, Addis Ababa University. The town is located in central Ethiopia and about 47km southeast of Addis Ababa at an elevation of 1920 meters. The area is characterized by mild subtropical with the average minimum and maximum temperatures ranging from 5.5°C and 23.5°C, respectively. The city is home to multi-government institutions including two General Hospitals and six health centers and commercial dairy and chicken farms.
Test Organisms
The test pathogens used in this study were obtained from the National Veterinary Institute (S. Enteritidis [SE] and S. Typhimurium [STM]) and the randomly selected non-serotyped Salmonella species isolated from milk of smallholder dairy farms in Modjo town, central Ethiopia. The organisms were refreshed on Nutrient Agar media. The media was prepared according to the manufacturer’s specifications21 and fresh cultures were used for the sensitivity test.
Drugs, Media, and Reagents
Five commercially available leading brands of ciprofloxacin hydrochloride tablets, each with a label of 500mg, were purchased from a single retail registered pharmacy in Bishoftu city, central Ethiopia. These brands are the leading products commonly prescribed by health professionals to treat salmonellosis in adults and vary in their prices. Detailed information about the brands is shown in Table 1 and Table 2. Unless otherwise specified, all the media and reagents used were of standard grade and obtained from chemical and media importer companies in Ethiopia. Media used in this study included Rappaport Vassiliadis Salmonella Enrichment Broth, Xylose lysine Desoxycholate agar (XLD), Salmonella Shigella (SS) agar, Nutrient Agar (NA), Tryptone soya broth and Mueller–Hinton agar.
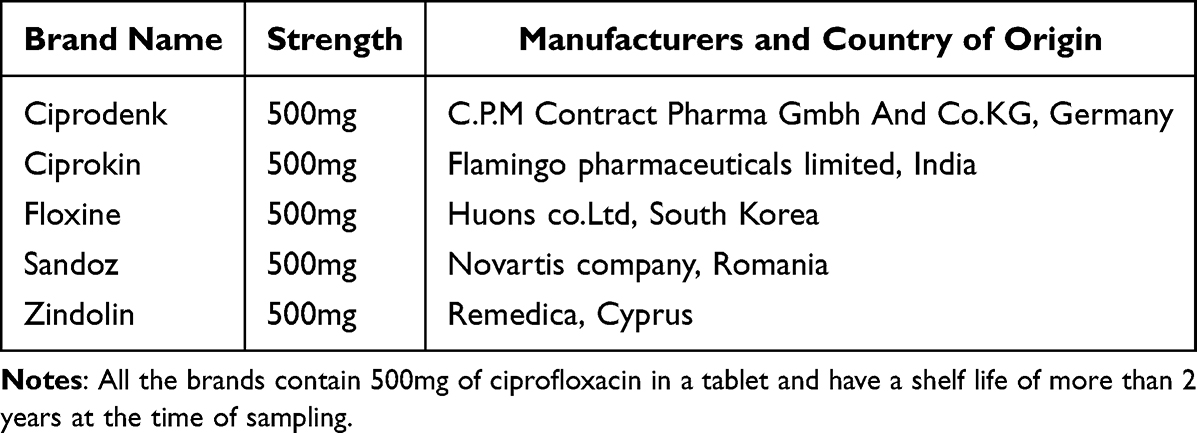 |
Table 1 Brands of Ciprofloxacin Tested for Efficacy |
 |
Table 2 Prices (in ETB) of Different Brands of Ciprofloxacin Sold in Bishoftu City, Ethiopia |
Preparation of Antibiotic Discs
Antibiotic discs were prepared following the recommendations of Vineetha et al.22 The stock and working solutions were prepared for each brand using distilled water as per the recommendation by CLSI (2020) for ciprofloxacin.23 The average weight of the tablet for each brand was determined by expecting 500mg of active ingredient present in a tablet. The known weight of the antibiotic for each brand was dissolved in sterile distilled water (100mg/2mL) to obtain the stock solution. First, the ciprofloxacin tablet was powdered and 100mg was weighed and dissolved in 2mL of sterile distilled water to prepare a stock solution that contains (50mg/mL) or (50µg/μL) concentrations. Then, the stock solution was diluted at the time of disc preparation to obtain the working solution. The concentrations of antibiotic solutions were expressed in μg/μL. The working solution was prepared using the dilution formula:

where, C1 = Concentration of stock solution, V1 = Volume of stock solution; C2 = Concentration of working solution and V2 = Volume of working solution.
Then, to prepare 2mL (V2) of the working solution which contains a concentration of 5μg/20μL (C2 = 0.25μg/μL) from a stock solution of 50μg/μL concentration (C1), we measured 10μL (V1) volume of stock solution with micro-pipette and added on a test tube containing 2mL of sterilized distilled water. A paper disc of 6mm diameter can absorb 20μL of solutions during impregnation.22 Hence, we measured 20μL from 0.25μg/μL working solution to obtain 5μg of ciprofloxacin (0.25μg concentration of drug in 1μL of working solution, 0.25μg/μL × 20μL = 5μg).
Impregnation of discs was done after discs of approximately 6mm diameter were prepared from a Whatman No.1 filter paper using a hole-punching machine. The discs were wrapped in aluminum foil and sterilized in the hot oven at 180°C for 1 h. The impregnated discs were placed in petri-dishes approximately 5mm apart. Using a mechanical pipette, a fixed volume of 20μL (which contains 5μg of the active ingredient) was loaded on each disc. This concentration was equivalent to the recommended standards according to guidelines of Clinical and Laboratory Standard Institute (CLSI).23 Finally, without covering the petri-dishes, the discs were allowed to dry in a clean incubator at 37°C for 4 h. After drying, 30–35 discs were placed in small sterile air-tight labeled containers with CaCl2 (desiccant) at the bottom. The discs were stored in a freezer at −20°C. The discs were removed from the freezer 2 h prior to usage so that the amount of condensation that may occur when warm room air reaches the cold containers.22
Inoculum Preparation and Inoculation
The disc diffusion test was adopted following previous analysis24 using tryptone soy broth and nutrient broth. Colonies of the non-serotyped Salmonella isolates, S. Enteritidis (SE) and S. Typhimurium (STM) were inoculated into 5mL of the broths and incubated at 35°C. A turbidimeter was used to monitor the turbidity of the broth cultures. Immediately the turbidity exceeded the McFarland 0.5 standard, the incubation was stopped. The broth culture was then diluted 1:10 with a freshly prepared nutrient broth to give the amount of approximately 1–2×108 CFU/mL (colonies per millimeter).25
After proper turbidity equivalent to the density of a McFarland 0.5 standard was achieved, a new sterile cotton swab was submerged in the suspension, lifted out and the excess fluid was removed by pressing and rotating the swab against the wall of the tube. The swab was then used to inoculate the entire surface of the supplemented Mueller Hinton (MH) agar plate three times, rotating the plate 60 degrees between each inoculation. The inoculum was allowed to dry before the discs are placed on the plates. The discs were placed on the agar with sterile forceps and tapped gently to ensure adherence to the agar. The plates containing the disks were incubated at 35°C for 16 to 18 h in an inverted position in a 5% CO2 incubator.22
In vitro Antimicrobial Efficacy Evaluation
The antimicrobial efficacy of five brands of ciprofloxacin sold in the Bishoftu markets was evaluated on SE, STM and other non-serotyped Salmonella isolates using the agar-disc diffusion method following the Performance Standards for Antimicrobial Susceptibility Testing guidelines recommended by CLSI (2020).23 MH agar (Oxoid, UK) was used for sensitivity analysis as it shows good batch-to-batch uniformity.26 This medium is also effective to grow only the target bacterial species for study by inhibiting the growth of other alternative bacterial species.26 The disc diffusion method is based on the determination of the zone of inhibition (ZI) proportional to the bacterial susceptibility to the antimicrobial present in the disc. The diameter of this ZI around the antimicrobial disc depends on the concentration of antibiotics in the disc and its diffusibility.27 The ZI diameter breakpoints around the discs were measured to the nearest whole millimeter using a digital caliper, and the isolates were classified as susceptible (≥31), intermediate (21–30), and resistant (≤20) according to the interpretative standards where the breakpoints for ciprofloxacin are based on a dosage regimen of 400 mg IV or 500mg orally administered every 12 h.23
Data Analysis
The raw data were entered and managed in a Microsoft Excel 365 worksheet and descriptive statistics and graphical presentation were utilized to summarize the data. STATA version 17 statistical software was used to analyze the standard deviations (SD) and 95% confidence interval. Pearson’s chi-square test was used to detect the association between parameters ZI and drug efficacy. To consider a result to be statistically significant 95% CI and p-value <0.05 was taken.
Results
The efficacy of five brands of ciprofloxacin tablets commonly sold in pharmacies found in Bishoftu city was determined using the diameter of ZI on SE and STM serovars and non-serotyped Salmonella species isolated from cow milk. A total of 27 isolates of Salmonella were tested for susceptibility to brands of ciprofloxacin. To test the individual brand efficacy, the mean of ZI against SE, STM and other non-serotyped Salmonella isolates was measured, and the results were compared with the value set to standard Ciprofloxacin 0.5 µg disc (Table 3).
 |
Table 3 Mean Zone of Inhibition of Different Brands of Ciprofloxacin Against Salmonella Serovars and Non-Serotyped Field Isolates |
The results of the current study revealed that the activity of five brands of ciprofloxacin significantly varies among the tested Salmonella strains (p < 0.05) (Table 3). Of the brands tested for efficacy, the highest mean ZI (24.7±0.71, 24.3±0.50, and 19.5±2.69) was recorded for Brand E against all tested isolates (non-serotyped field Salmonella isolates, STM and SE, respectively). Conversely, the lowest ZI was recorded for Brand A (22.0±0.87, 21.0±0.87, and 10.7±1.4) for non-serotyped field Salmonella isolates, STM and SE, respectively (Table 3).
The study result indicated that of 9 SE tested against different brands of Ciprofloxacin tablets, all (100%) of SE were resistant to four brands (Brand A-D) while 6 (67%) were resistant and 3 (33%) were intermediate susceptible to Brand E (Table 4). Similarly, of 9 STM tested against five brands, 33% and 67% of them were resistant and intermediate susceptible to Brand A, respectively, while all the STM were intermediate to the other four brands (Brand B-E). Furthermore, the current results of efficacy evaluation of ciprofloxacin brands against non-serotyped field isolates of Salmonella indicated that all of them were intermediate susceptible to all five brands (Brand A, B, C, D, and E), respectively, with the increasing zone of inhibition (Table 4).
 |
Table 4 Antibiotic Susceptibility Profile of S. Enteritidis, S. Typhimurium and Non-Serotyped Salmonella Isolated from Dairy Farms (n = 27) Against Brands of Ciprofloxacin |
The susceptibility of isolates to the standard Ciprofloxacin 5µg disc showed that 56% of SE, 89% of STM and 78% of non-serotyped Salmonella isolates were intermediate susceptible, while 44% of SE demonstrated resistance; and 10% of STM and 22% of non-serotyped Salmonella isolates showed susceptible (Table 4). Though the clinical interpretation of the breakpoints of brands of ciprofloxacin did not show any difference for non-serotyped Salmonella isolates, the study finding indicated there was a statistically significant difference in the antimicrobial efficacy among the tested brands compared to the standard (p < 0.05) (Table 4).
Discussion
Antibiotics must be safe, effective and of acceptable quality to use in both human and veterinary medicines.28–31 A generic version of a drug must use the same active ingredient(s) as the brand name drug and it must meet the same quality and safety standards.32 To the best of our knowledge, this study is the first report from Ethiopia that evaluated the efficacy of leading brands of ciprofloxacin against S. Enteritidis, S. Typhimurium, and animal food source non-serotyped Salmonella isolates. Furthermore, no published and/or accessible study was conducted elsewhere on in vitro efficacy evaluation of different brands of ciprofloxacin on different Salmonella species. Hence, the study result in this discussion could not be compared with previous study findings. However, the specific mean ZI diameter for different brands of ciprofloxacin were compared with commercially available standard ciprofloxacin disc.
Our study on the comparative antibacterial activity evaluation of five brands of ciprofloxacin showed a considerable difference in mean of ZI diameter among the brands. In our current study we found that Brand E was found to have higher mean ZI diameter than all brands of Ciprofloxacin tested on S. Typhimurium, S. Enteritidis and non-serotyped field Salmonella isolates. Similarly, the present findings showed Brand E has comparable efficacy against S. Enteritidis compared to the ciprofloxacin standard disc. The amount of active ingredients found in Brand E compared to other brands could be a reason for higher mean ZI, which directly correlates with the efficacy of drugs. The findings also demonstrated that the efficacy of Brand D, Brand C, Brand B, and Brand A (Brand D-A) tested against S. Enteritidis was low (resistant) with decreasing the mean ZI diameter, respectively. On top of this, all non-serotyped field Salmonella isolates were intermediate susceptible to all brands (Brand E, D, C, B and A) with a decreasing order of mean of ZI diameter, respectively. Similar results were also recorded for the susceptibility profile of S. Typhimurium (intermediate) with 33% resistance and 67% intermediate were recorded for Brand A. The current study findings indicate that there is difference in efficacy among five brands of ciprofloxacin sold in Ethiopia. Relatively better efficacy is expected from Brand E against salmonellosis caused by S. Enteritidis, whereas the efficacy increases from Brand A to Brand E or (Brand A < Brand B < Brand C < Brand D < Brand E) against S. Typhimurium and non-serotyped field Salmonella isolates.
The efficacy of different brands of ciprofloxacin tested in this study was directly related to the percent of inhibition to the test organism ie, the more the drug inhibits the test bacteria, the higher the efficacy of the drug.33 In this study, we observed differences in efficacies of brands of Ciprofloxacin sold in Bishoftu, Ethiopia, which differs in their effectiveness depending on their brands or manufacturers. This is due to the difference in their manufacturing process and/or the active ingredient of the drugs is believed to be the major factor.16 This difference in the quality of drugs can create a great difference in the price of drugs in the market.
The findings of the current study revealed that drugs with lower prices show lower mean of ZI diameter and drugs with higher prices found with better efficacy as indicated in Table 2 and Table 3. The study showed Brand E, with the highest price of 280.00 ETB per full dosage regimen (Table 2), was found the highest mean ZI diameter and first-ranked efficacious drug that showed 33% intermediate susceptibility of S. Enteritidis to the drug as compared to other brands. Whereas Brand A with price of 30 ETB (ie, cheapest of all brands) was found the least mean of ZI diameter with 100% resistance of S. Enteritidis to the drug. This could be due to the difference in the quality of active ingredients found in these different brands of Ciprofloxacin. Our current study is supported by other previous report.34
The differences in mean of ZI diameter among different brands of some antibiotics constitute a potential danger both to human and animal health. Most developing and underdeveloped countries are suffering from the direct and indirect effects of poor-quality drugs to a high degree.16 Administering fake and/or low-quality drugs could result in therapeutic failure, toxicity or allergic reactions due to their content, drug resistance, prolonged illness, high cost of treatment, and even mortality which all can directly or indirectly influence public health. This is directly related to most societies found in such countries that can afford (highly use) low-cost drugs. As recorded from this study, brands of drugs with low mean ZI diameter and efficacy were imported and sold at lower prices. This finding is indicating variations in the amount of active ingredients in each brand. Our finding negates The Food and Drug Administration (FDA) of the US suggests that generic drug products must contain identical amounts of the same active drug ingredient as the brand name product.35
The current study has some limitations. First, we used in vitro antimicrobial activity assay against Salmonella serovars and non-serotyped milk isolates of Salmonella using disc diffusion method. Hence, the findings may differ for the MIC method. Second, we used the clinical breakpoints set by CLSI (2020), which is high mean ZI for interpretation as disc diffusion might not be good indicators for assessing fluoroquinolones susceptibility or resistance in Salmonella spp. However, the variations in mean of ZI diameter of brands of ciprofloxacin observed in current study are good predictor of efficacy variation among tested brands. Third, the diffusability of the active ingredients of brands of ciprofloxacin impregnated on Whatman paper may vary compared with commercial disc as the dispersion of the particles of each brand are affected by the diluents in the tablet. This may also have effects on efficacy evaluation findings.
Conclusion
The current study revealed variations in mean of ZI diameter of leading brands of ciprofloxacin against the tested Salmonella isolates. The highest mean ZI diameter was recorded for Brand E, whereas the lowest was recorded for Brand A. Comparatively, brand E was found to be more efficacious against the tested SE, STM, and non-serotyped Salmonella isolates than other brands. The significant differences in the mean ZI diameter among the tested brands could be associated with differences in the level of active ingredients, which constitute a potential danger to human health as result in therapeutic failure and drug resistance. Hence, the current study warrants a need for periodic surveillance of both the quality and efficacy of antibiotics to improve patient well-being and minimize the risk of antimicrobial resistance.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval
This study was approved by the institutional ethics committee of the College of Veterinary Medicine and Agriculture of Addis Ababa University (VM/ERC/01/13/12/2020).
Acknowledgments
The authors acknowledge Private Pharmacy found in Bishoftu city for supplying the drugs and the National Veterinary Institute for supplying bacteria isolates.
Funding
The study was financially supported by the Office of Research and Technology Transfer of Addis Ababa University (CEVMed Thematic Research: VPRTT/PY-045/2019).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Thai T, Salisbury BH, Zito PM. Ciprofloxacin. StatPearls; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535454/.
2. WHO. WHO model list of essential medicines - 22nd list. World Heal Organ. 2021. Available from: https://www.who.int/publications/i/item/WHO-MHP-HPS-EML-2021.02.
3. EFDA. Ethiopian Essential Medicines List. Ministry of Health/Ethiopian Food and Drug Authority; 2020:6.
4. Meredith P. Bioequivalence and Other Unresolved Issues in Generic Drug Substitution. Clin Ther. 2003;25(11):2875–2890. doi:10.1016/S0149-2918(03)80340-5
5. Sánchez-Vargas FM, Abu-El-Haija MA, Gómez-Duarte OG. Salmonella infections: an update on epidemiology, management, and prevention. Travel Med Infect Dis. 2011;9(6):263–277. doi:10.1016/J.TMAID.2011.11.001
6. King DR, Kanavos P. Encouraging the use of generic medicines: implications for transition economies - PubMed. Croat Med J. 2002;43(4):462–469.
7. ASPE. Expanding the Use of Generic Drugs: ASPE Issue Brief. ASPE Issue Br; 2010:1–13.
8. Finch R. Generic antibiotics, antibiotic resistance, and drug licensing. Lancet Infect Dis. 2010;10(11):754. doi:10.1016/S1473-3099(10)70246-2
9. Taylor RB, Shakoor O, Behrens RH, et al. Pharmacopoeial quality of drugs supplied by Nigerian pharmacies. Lancet. 2001;357:1933–1936. doi:10.1016/S0140-6736(00)05065-0
10. Butler T, Sridhar CB, Daga MK, et al. Treatment of typhoid fever with azithromycin versus chloramphenicol in a randomized multicentre trial in India. J Antimicrob Chemother. 1999;44(2):243–250. doi:10.1093/jac/44.2.243
11. Effa EE, Lassi ZS, Critchley JA, et al. Fluoroquinolones for treating typhoid and paratyphoid fever (enteric fever). Cochrane Database Syst Rev. 2011;2011:10. doi:10.1002/14651858.CD004530.PUB4
12. Umair M, Siddiqui SA. Antibiotic susceptibility patterns of salmonella typhi and salmonella paratyphi in a tertiary care hospital in Islamabad. Cureus. 2020;12:9. doi:10.7759/CUREUS.10228
13. Ozawa S, Evans DR, Bessias S, et al. Prevalence and estimated economic burden of substandard and falsified medicines in low- and middle-income countries: a systematic review and meta-analysis. JAMA Netw open. 2018;1(4):e181662. doi:10.1001/jamanetworkopen.2018.1662
14. Delepierre A, Gayot A, Carpentier A. Update on counterfeit antibiotics worldwide; Public health risks. Médecine Mal Infect. 2012;42(6):247–255. doi:10.1016/J.MEDMAL.2012.04.007
15. MSF. Drug Quality and Storage. MSF Medical Guidelines; 2022. Available from: https://medicalguidelines.msf.org/en/viewport/EssDr/english/drug-quality-and-storage-16688167.html.
16. WHO. Quality assurance of pharmaceuticals: a compendium of guidelines and related materials; 2007. Available from: https://www.who.int/medicines/areas/quality_safety/quality_assurance/QualityAssurancePharmVol2.pdf.
17. Newton P, Proux S, Green M, Smithuis F, Nosten F, White NJ. Fake artesunate in Southeast Asia. Lancet. 2001;357:1948–1950. doi:10.1016/S0140-6736(00)05085-6
18. Zabala GA, Bellingham K, Vidhamaly V, et al. Substandard and falsified antibiotics: neglected drivers of antimicrobial resistance? BMJ Glob Heal. 2022;7(8):8587. doi:10.1136/BMJGH-2022-008587
19. Pisani E. WHO Global Surveillance and Monitoring System for Substandard and Falsified Medical Products. Geneva: World Health Organization; 2017.
20. Johnston A, Holt DW. Substandard drugs: a potential crisis for public health. Br J Clin Pharmacol. 2014;78(2):218–243. doi:10.1111/bcp.12298
21. HIMEDIA. Nutrient agar: technical data M001. HiMedia Laboratories Technical Data; 2022. Available from: https://www.himedialabs.com/TD/M001.pdf.
22. Vineetha N, Vignesh R, Sridhar D. Preparation, standardization of antibiotic discs and study of resistance pattern for first-line antibiotics in isolates from clinical samples. Int J Appl Res. 2015;1(11):624–631.
23. Clinical and Laboratory Standards Institute (CLSI). Performance Standards for Antimicrobial Susceptibility Testing. In: Weinstein M, Lewis J, Bobenchik A, editors. CLSI Supplement M100. Vol M100-Ed30.
24. Berhe S, Beyene T, Jibat T, Tadese W. Comparative efficacy evaluation of six brands of amoxicillin against S. aureus isolated from subclinical mastitic milking dairy cows in bishoftu. Adv Dairy Res. 2017;5:169.
25. Quinn P, Carter M, Markey B, Carter G. Clinical Veterinary Microbiology. Aust Vet J. 2002;72(6):96–344. doi:10.1111/j.1751-0813.1995.tb03534.x
26. Okonko IO, Fajobi EA, Ogunnusi TA, Ogunjobi AA. Antimicrobial chemotherapy and sustainable development: the past, the current trend, and the future. African J Biomed Res. 2009;11:235–250.
27. OIE (World Organization for Animal Health). Guideline 2.1. Laboratory Methodologies for Bacterial Antimicrobial Susceptibility Testing. Paris, France: OIE Terrestrial Animal Health Code; 2012.
28. FDA. The FDA’s drug review process: ensuring drugs are safe and effective. FDA. U.S.Food & Drug Administration; 2017. Available from: https://www.fda.gov/drugs/information-consumers-and-patients-drugs/fdas-drug-review-process-ensuring-drugs-are-safe-and-effective.
29. Bihari M. Are generic drugs as safe and effective as brand-name? Verywell health; 2022. Available from: https://www.verywellhealth.com/generic-drug-safety-and-effectiveness-1738890.
30. Eshetie TC, Marcum ZA, Schmader KE, Gray SL. Medication use quality and safety in older adults: 2020 update. J Am Geriatr Soc. 2022;70(2):389–397. doi:10.1111/JGS.17603
31. FDA. FDA regulation of animal drugs. FDA. U.S.Food and Drug Administration; 2022. Avilable from: https://www.fda.gov/animal-veterinary/resources-you/fda-regulation-animal-drugs.
32. FDA. Generic drug facts. U.S. Food & Drug Administration; 2021. Avilable from: https://www.fda.gov/drugs/generic-drugs/generic-drug-facts.
33. Paul M. Assessment of commonly available antimicrobial agents. A study from Ilala Tanzania. Tanzania Med Students’ Assoc. 2009;16:16–22.
34. Azoulay P. Do pharmaceutical sales respond to scientific evidence? J Econ Manag Strateg. 2002;11(4):551–594. doi:10.1162/105864002320757262
35. FDA. Abbreviated New Drug Application (ANDA); 2019. Available from: https://www.fda.gov/drugs/types-applications/abbreviated-new-drug-application-anda.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.