Back to Journals » Infection and Drug Resistance » Volume 15
In vitro Activity of Isavuconazole and Comparators Against Clinical Isolates of Molds from a Multicenter Study in China
Authors Jing R, Ian M, Xiao M, Sun TS, Zhang G ![]() , Kang W, Guo DW
, Kang W, Guo DW ![]() , Aram JA, Wang J, Utt EA
, Aram JA, Wang J, Utt EA ![]() , Wang Y
, Wang Y ![]() , Xu YC
, Xu YC ![]()
Received 28 January 2022
Accepted for publication 11 April 2022
Published 22 April 2022 Volume 2022:15 Pages 2101—2113
DOI https://doi.org/10.2147/IDR.S360191
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Ran Jing,1– 3 Ian Morrissey,4 Meng Xiao,1,3 Tian-Shu Sun,3,5 Ge Zhang,1,3 Wei Kang,1,3 Da-Wen Guo,6 Jalal A Aram,7 Jeffrey Wang,8 Eric A Utt,7 Yao Wang,1,3 Ying-Chun Xu1– 3
1Department of Laboratory Medicine, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Graduate School, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 3Beijing Key Laboratory for Mechanisms Research and Precision Diagnosis of Invasive Fungal Diseases, Beijing, People’s Republic of China; 4IHMA Europe Sarl, Monthey, Valias, Switzerland; 5Medical Research Center, State Key Laboratory of Complex Severe and Rare Diseases, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 6Department of Laboratory Medicine, the First Clinical Hospital Affiliated to Harbin Medical University, Harbin, Heilongjiang, People’s Republic of China; 7Medical Affairs, Pfizer Inc, Groton, CT, USA; 8Clinical Development, Pfizer, Beijing, People’s Republic of China
Correspondence: Ying-Chun Xu; Yao Wang, Department of Clinical Laboratory, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Number 1, Shuaifuyuan Road, Dongcheng District, Beijing, People’s Republic of China, Fax +86 10 69159766, Email [email protected]; [email protected]
Purpose: Monitoring antifungal susceptibility patterns for new or established antifungals is imperative. Antifungal resistance is frequent in molds, frequently leading to invasive mold infections (IMIs) in immunocompromised patients with high morbidity and mortality. Limited availability of effective antifungals for treatment of IMIs in China is an enormous challenge. The purpose of this study was to monitor in vitro antifungal resistance profiles of mold isolates from China, with a particular focus on evaluating in vitro isavuconazole (ISA) activity against these isolates, contributing to the treatment guidance in clinics.
Methods: We evaluated the in vitro activity of ISA and its comparators (voriconazole [VOR] and amphotericin B [AMB]) against 131 clinical isolates of Aspergillus spp. (n = 105) and Mucorales order (n = 26) collected between 2017 and 2020 from China.
Results: ISA and VOR exhibited similar in vitro activity against Aspergillus spp., with minimum inhibitory concentration (MIC)50 of 1 μg/mL and MIC90 of 2 μg/mL, respectively. Overall, AMB was less active than azoles against Aspergillus spp. (MIC50: 4 μg/mL, MIC90: 8 μg/mL). Against the Mucorales order, ISA demonstrated MIC50 of 0.5 μg/mL and MIC90 of 1 μg/mL; however, one strain each of Mucor circinelloides and Syncephalastrum racemosum were resistant to ISA (MICs: > 8 μg/mL). VOR exhibited little or no activity (MIC50: 8 μg/mL, MIC90: > 8 μg/mL) against the Mucorales order, whereas AMB had MIC50 and MIC90 of 1 μg/mL.
Conclusion: This was the first multicenter, in vitro study conducted in China and demonstrated the excellent activities of ISA against most species of the Mucorales order. MIC indicated an advantage over currently available azole antifungals, positioning ISA as a potential alternative to VOR for clinical management of IMIs. As with other antimicrobials, clinicians should employ stewardship and best practices in relation to potential resistance to new azole antifungals.
Keywords: Mucorales order, Aspergillus species, antifungal susceptibility testing, isavuconazole, resistance
Introduction
Invasive mold infections (IMIs), including invasive aspergillosis (IA) and mucormycosis, cause considerable morbidity, mortality, and economic burden predominantly among immunocompromised individuals worldwide.1–3 IMIs mainly affect immunocompromised patients such as those with hematological malignancies, organ transplants, and those prescribed long-term steroid therapy.4–6 Besides, mucormycosis is also involved in angio-invasion with higher mortality than IA; and infection is increasingly reported in patients with uncontrolled diabetes mellitus.3,6–8
Like other countries, China is also facing an increase in the incidence of IMIs due to rapid economic development and an aging population. This increases the burden on public health and socio-economic systems, and raises health-care costs.3,8 Azoles, mainly voriconazole (VOR), are recommended as primary antifungals for IA treatment.9 However, the emergence of azole-resistant Aspergillus fumigatus is gradually being reported worldwide and is associated with point mutations, particularly in the cyp51 gene.10,11 Amphotericin B (AMB) formulations are used as the mainstay of treatment for mucormycosis,12 despite being associated with a high frequency of treatment-related adverse effects such as nephrotoxicity.13 Therefore, the treatment of IMIs remains a huge challenge worldwide.
The extended-spectrum triazole antifungal, isavuconazole (ISA), was approved in 2015 by the US Food and Drug Administration (FDA) and the European Medicines Agency (EMA) for the treatment of IA and mucormycosis.14,15 Previous studies have reported the excellent activity of ISA against a broad range of yeasts and molds, with lower toxicity than VOR and fewer drug-drug interactions than other azoles.16,17 Considering that ISA is currently unavailable in China, studies on in vitro antifungal activity of ISA against yeast and mold isolates from the region are lacking. We participated in the 2020 Analysis of Resistance in Antifungals (ARIA) Study conducted by IHMA, Europe Sarl. This was the first multicenter study conducted in China to evaluate the in vitro antifungal activity of ISA and its comparators (VOR and AMB) against molds including those belonging to Aspergillus spp. and the Mucorales order. The purpose of the current study was to monitor in vitro antifungal resistance profiles of mold isolates from China between 2017 and 2020, with a particular focus on evaluating in vitro ISA activity against these isolates to contribute to the treatment guidance in the clinics. In those species from which resistant isolates were identified, genetic sequencing along with an alignment for known genetic determinants of resistance (CYP 51s) with reference strains was performed to identify potential associations with ISA resistance.
Materials and Methods
Ethics Statement
This study was approved by the Human Research Ethics Committee of Peking Union Medical College Hospital (HS-2468). An informed consent waiver was granted by Peking Union Medical College Hospital prior to ethics approval, since only in-vitro susceptibility testing of strains isolated from patients was conducted, and no patient-specific information was collected. The results were only used for evaluation of antifungal agents, and no clinical diagnoses were made.
Organisms
A total of 131 clinical filamentous isolates were collected from 2017–2020 under the China Hospital Invasive Fungal Surveillance Net – North China Program (CHIF-NET). These strains were originally isolated from a total of 8 participating regions of northern China, including Beijing, Tianjin, Inner Mongolia, Hebei, Heilongjiang, Jilin, Liaoning, and Shanxi Provinces. All strains were sub-cultured on Sabouraud dextrose agar (SDA) (Thermo Fisher Scientific) and incubated at 28°C for 3–7 days.
Species Identification
All isolates were identified by combining conventional morphological methods and matrix-assisted laser desorption/ionization time of flight mass spectrometry (MALDI-TOF MS), using VITEK® MS (bioMérieux, Marcy-l’Étoile, France) and M-Discover 100 MALDI-TOF MS (Zhuhai Meihua Medical Technology Co., Ltd). One unidentified isolate and two Mucor spp. strains were subsequently identified using molecular sequencing of the internal transcribed spacer (ITS) and/or D1/D2 regions of ribosomal DNA. Nucleotide sequences were then homologically aligned with reliable sequences in the GenBank database (https://www.blast.ncbi.nlm.nih.gov/Blast.cgi) using two reference sequences of M. circinelloides 1006PhL (CYP51F1 and CYP51F5 genes).
Antifungal Susceptibility Testing
In vitro antifungal susceptibility testing of the 131 isolates was performed by the Department of Clinical Laboratory, Peking Union Medical College Hospital (PUMCH), China using the Clinical and Laboratory Standards Institute (CLSI) broth microdilution method (BMD) as described in the CLSI standard M38-A3.18 Frozen 96-well panels provided by IHMA containing three antifungal agents: ISA (0.008–8 μg/mL), VOR (0.008–8 μg/mL) and AMB (0.06–8 μg/mL) were used. After these strains were cultured on SDA and incubated at 28°C for 3–7 days, an adequate amount of conidia was collected using 1 mL of sterile saline with 0.1% Tween-20 (Sigma: P1379). Subsequently, the turbidity of the stock suspension was adjusted to an A530 of between 0.09 and 0.13 for Aspergillus spp. or 0.15 and 0.17 for Mucorales order.18 Thereafter, the suspension was diluted 50-fold in Roswell Park Memorial Institute (RPMI) 1640 (+MOPS) culture medium, after which 100 µL of inoculum was added to the wells of the antifungal panels to give a final inoculum between approximately 2×103 to 2.5×104 colony forming unit (CFU)/mL and the desired test concentrations of antifungal agents in a total volume of 200 µL.18
The minimum inhibitory concentration (MIC), 50% MIC (MIC50) and 90% MIC (MIC90) were determined as defined in the CLSI M38-A3 document.18 For Aspergillus spp., the MICs for ISA and its comparators were observed after 46–50 h of incubation at 35°C. Due to the rapid growth of Mucorales isolates, the incubation time was shorter, and MICs for ISA and its comparators were recorded between 21 h and 26 h.18 Candida parapsilosis ATCC 22019, Candida krusei ATCC 6258, Aspergillus flavus ATCC®204304™ and A. fumigatus ATCC®MYA-3627™ were used as quality control and reference strains.19
Analysis of Mucor circinelloides CYP51s (Sterol 14-Demethylase) Amino Acid Sequences
The homologous sequences of Mucor circinelloides CYP51s (Gene ID: HMPREF1544_03888.1 and HMPREF1544_08704.1) were obtained from FungiDB database (http://FungiDB.org). The paralogs of CYP51s were named CYP51F5 or CYP51F1 according to Nelson’s database nomenclature.20 Using the BLAST program (tblastn), M. circinelloides 1006PhL was identified as the reference strain from Mucor species (GenBank No. AOCY00000000.1); and the amino acid sequences of A. fumigatus CYP51A (GenBank protein ID: AAK73659.1) and CYP51B (GenBank protein ID: AAK73660.1) were used as query sequences. Species-specific primer sequences are presented in Table 1. The sequences of CYP51F5 and CYP51F1 were amplified by Beijing Ruibio BioTech Co., Ltd (Beijing, China). Subsequently, CYP51s amino acids sequences of M. circinelloides strains (M35 and M49) were translated using CLC Sequence Viewer software (version 8.0).
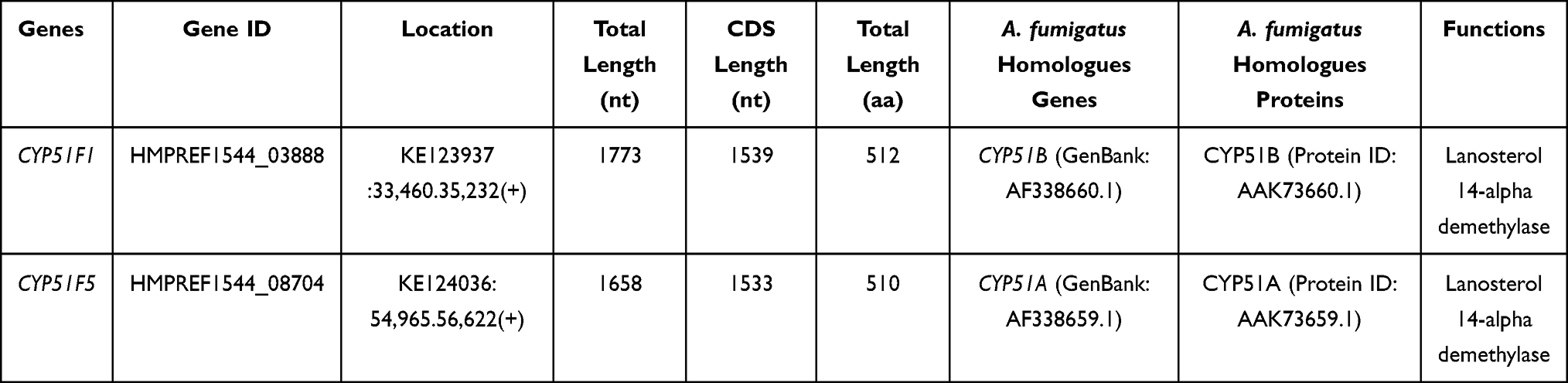 |
Table 1 Molecular Description of CYP51 Homologous Genes Related to Azoles-Resistance in Mucor circinelloides |
To find potential substitutions of CYP51s amino acids likely affecting azole resistance in M. circinelloides, alignment using Saccharomyces cerevisiae S288C Erg11 (reference strain; CYP51 sterol 14-demethylase) was compared with the CYP51s amino acids sequences of M. circinelloides strains (M35 and M49).
Data Analysis
Although several studies have evaluated epidemiological cut-off values (ECVs) for AMB, posaconazole, and itraconazole against a limited number of isolates of Mucorales order,21 ECV values have not been formally established for ISA and VOR against isolates of Mucorales order or may be inapplicable to the interpretation of drug susceptibilities in China due to lack of clinical data in the population from China. Therefore, the MIC50 and MIC90 were calculated for evaluating in vitro activities of these antifungal agents against isolates of Mucorales order. However, ECVs are formally established for VOR, ISA, and AMB against some major Aspergillus spp., such as A. fumigatus, A. flavus, A. niger, and A. terreus22 and were used for susceptibility testing of these organisms.
Results
Species Distribution
A total of 131 clinical isolates were included, comprising 4 different Aspergillus complexes (n = 105) and 5 different species of the Mucorales order (n = 26) (Table 2). The A. fumigatus complex consisted of 71.4% (75/105) of all Aspergillus strains, followed by A. niger complexes (10.5%, 11/105), A. flavus complexes (9.5%, 10/105), and A. terreus complexes (8.6%, 9/105). For strains from the Mucorales order, the predominant genus was Rhizopus (50%, 13/26), of which 84.6% (11/13) were R. oryzae/R. arrhizus, followed by R. microspores and R. stolonifera (1 isolate each). Other common genera were Rhizomucor spp. and Lichtheimia spp. (15.4%, 4/26 each). For Rhizomucor spp., R. pusillus isolates were the most prevalent (n = 3), followed by R. miehei (n = 1), which were identified by using molecular sequencing. For Lichtheimia spp., all isolates were identified as Lichtheimia ramosa (n = 4). Syncephalastrum spp. comprised 11.5% (3/26) of all strains from the Mucorales order, and all of them were identified as S. racemosum. Mucor spp. comprised only 2 isolates, which were identified as M. circinelloides.
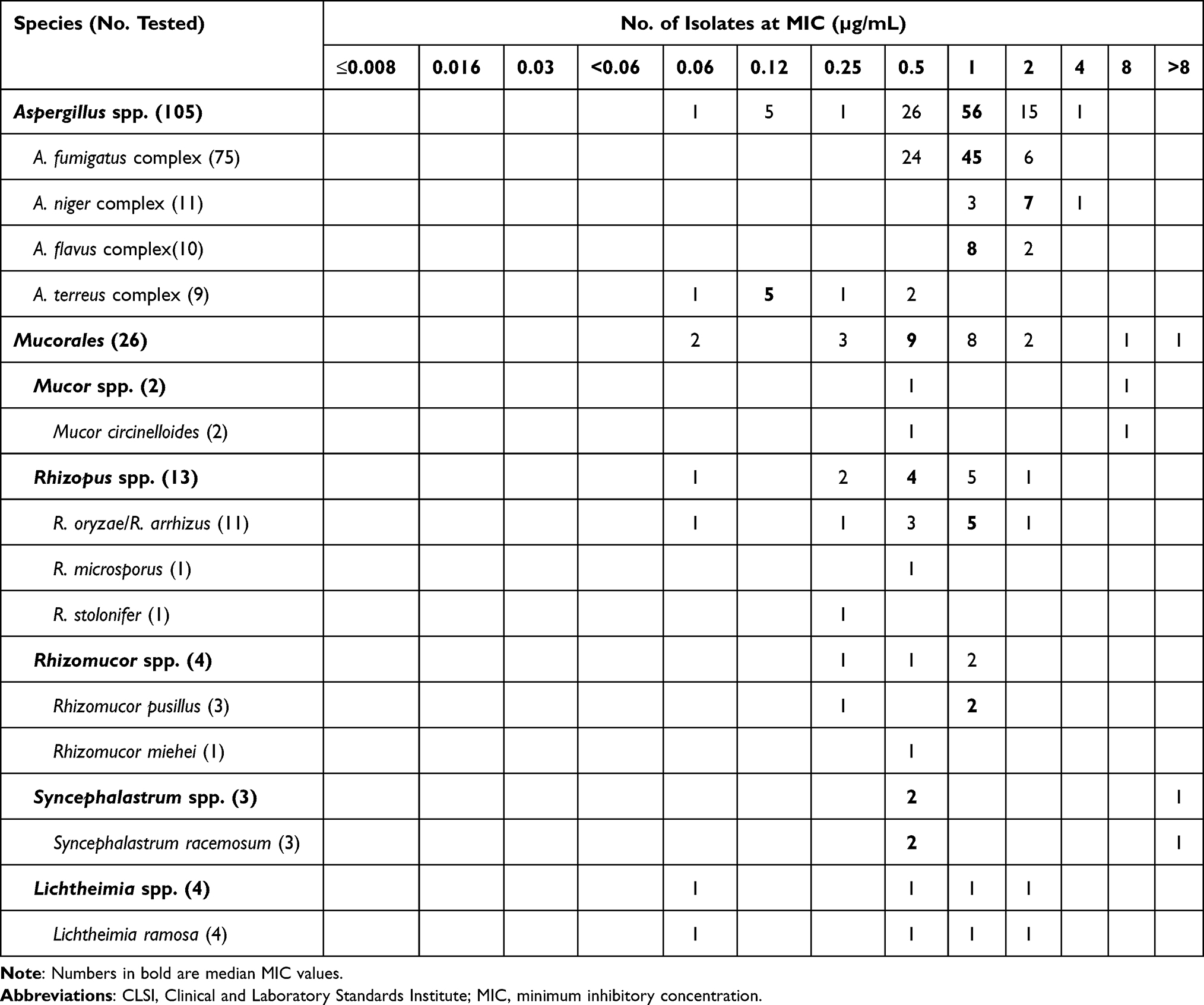 |
Table 2 MIC Distributions for Isavuconazole Against Aspergillus spp. and Species of Mucorales Order Using CLSI Broth Microdilution Methods |
Specimen Distribution
The lower respiratory tract (LRT, i.e., sputum, bronchoalveolar lavage fluid, tracheal aspirate) (75.6%, 99/131) was the primary culture source, followed by secretions (9.2%, 12/131), swabs (i.e., ear, nasopharyngeal, cornea, and skin 6.9%, 9/131), bodily fluids (i.e., blood, pleural fluid, cerebrospinal fluid, and abdominal dialysate; 3.8%, 5/131), pus (n = 3), tissue (n = 2), and stool (n = 1). Of note, more than half (61.5%, 16/26) of the isolates of Mucorales order originated from LRT, with sputum (n = 13) as the most frequent culture source. Of all the isolates of R. arrhizus, one was cultured from blood.
Antifungal Susceptibilities
Isavuconazole Activity Against Aspergillus spp. and Mucorales Order
MIC distributions for ISA against Aspergillus spp. and species of Mucorales order are shown (Table 2). Among the Aspergillus isolates, MICs for ISA ranged from 0.06–4 μg/mL (Table 3). The median MIC (mMIC) for ISA among all Aspergillus spp. was 1 μg/mL, with a low mMIC of 0.12 μg/mL for A. terreus complexes, a high mMIC of 2 μg/mL for A. niger complexes, and the same mMIC value of 1 μg/mL for A. fumigatus complexes (constituted the majority of the isolates identified) and A. flavus complexes (Table 3). Based on the ECVs available, a large proportion of Aspergillus strains in this study were wild-type (WT; MIC ≤ECV; range, 80.0–100.0%) (Table 3).
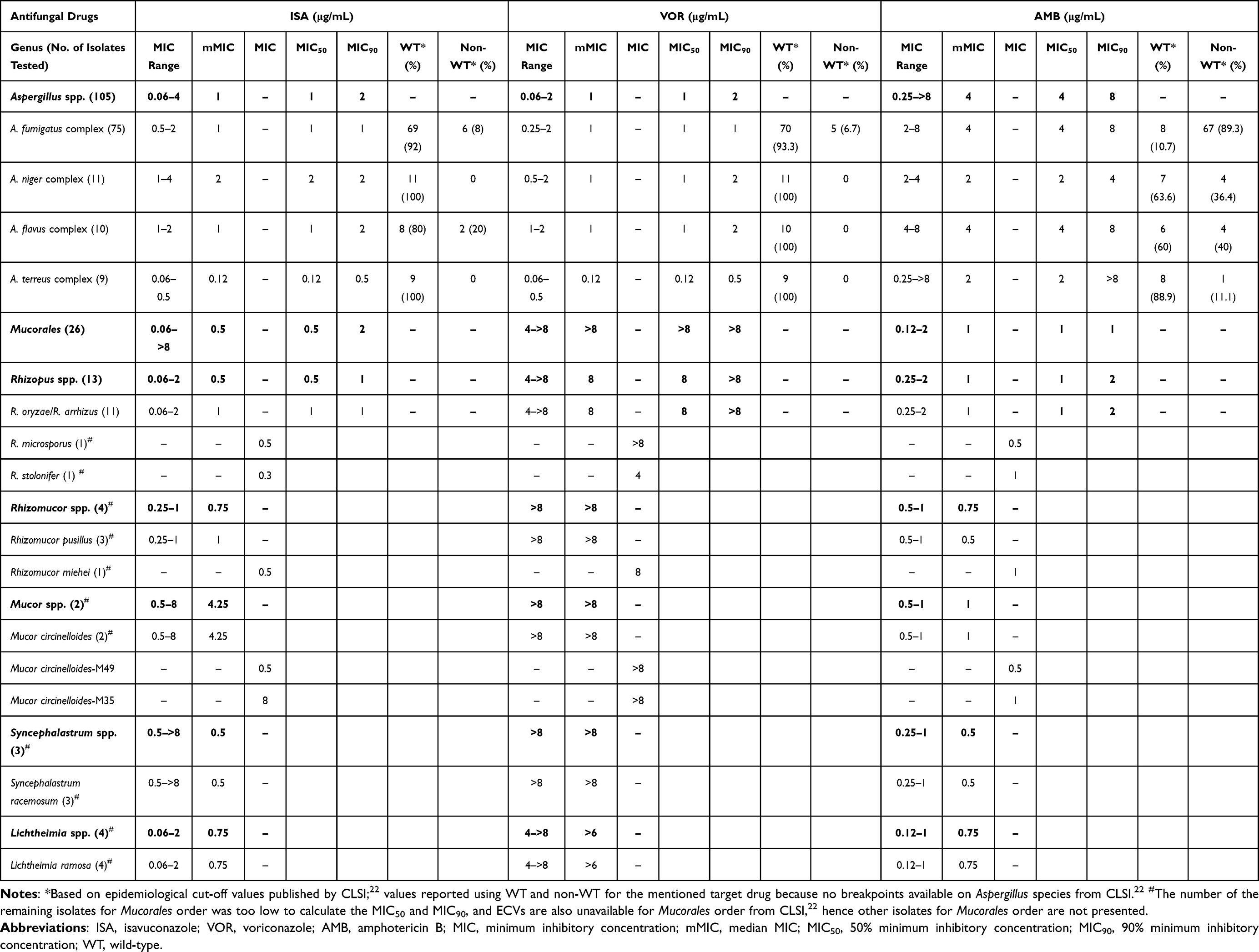 |
Table 3 Antifungal Activity of Isavuconazole and Comparator Antifungal Agents (Voriconazole and Amphotericin B) Against Aspergillus spp. and Species of Mucorales Order Collected in China Between 2017 and 2020 |
In this study, the activity of ISA against isolates of Mucorales order was slightly higher than observed for Aspergillus spp. (MIC50: 1 μg/mL), with a lower MIC50 at 0.5 μg/mL (Table 3). Compared with Aspergillus spp., a lower mMIC value of 0.5–0.75 μg/mL was observed for Rhizopus spp., Rhizomucor spp., Syncephalastrum spp., and Lichtheimia spp. (Table 3). Higher mMIC values of 1 μg/mL were observed for R. oryzae/R. arrhizus and R. pusillus (Table 3).
Activity of Isavuconazole and Comparators (Voriconazole and Amphotericin B Against Aspergillus spp. and Mucorales Order
All MICs of quality control (QC; Candida parapsilosis ATCC 22019, Candida krusei ATCC 6258) and reference strains (A. flavus, A. fumigatus) were within expected limits (Supplementary Table 1). MIC distributions for VOR and AMB against Aspergillus spp. and species of Mucorales order are shown (Tables 4 and 5). The overall MIC50 and MIC90 for both azoles against Aspergillus spp. (n = 105) were 1 μg/mL and 2 μg/mL, respectively (Table 3). WT susceptibility to ISA was 80% and to VOR was 100% among A. flavus, A. niger, and A. terreus complexes. MIC90 for both azoles was lower (1 μg/mL) against A. fumigatus complexes (n = 75) with a WT susceptibility of 90%. Of all Aspergillus spp. studied, A. terreus complex (n = 9) was the most susceptible to ISA and VOR with an MIC50 of 0.12 μg/mL and MIC90 of 0.5 μg/mL. AMB was less active than both azoles against Aspergillus spp., with an MIC50 of 4 μg/mL and MIC90 of 8 μg/mL, particularly against A. fumigatus complexes (89.3% of non-WT were less susceptible).
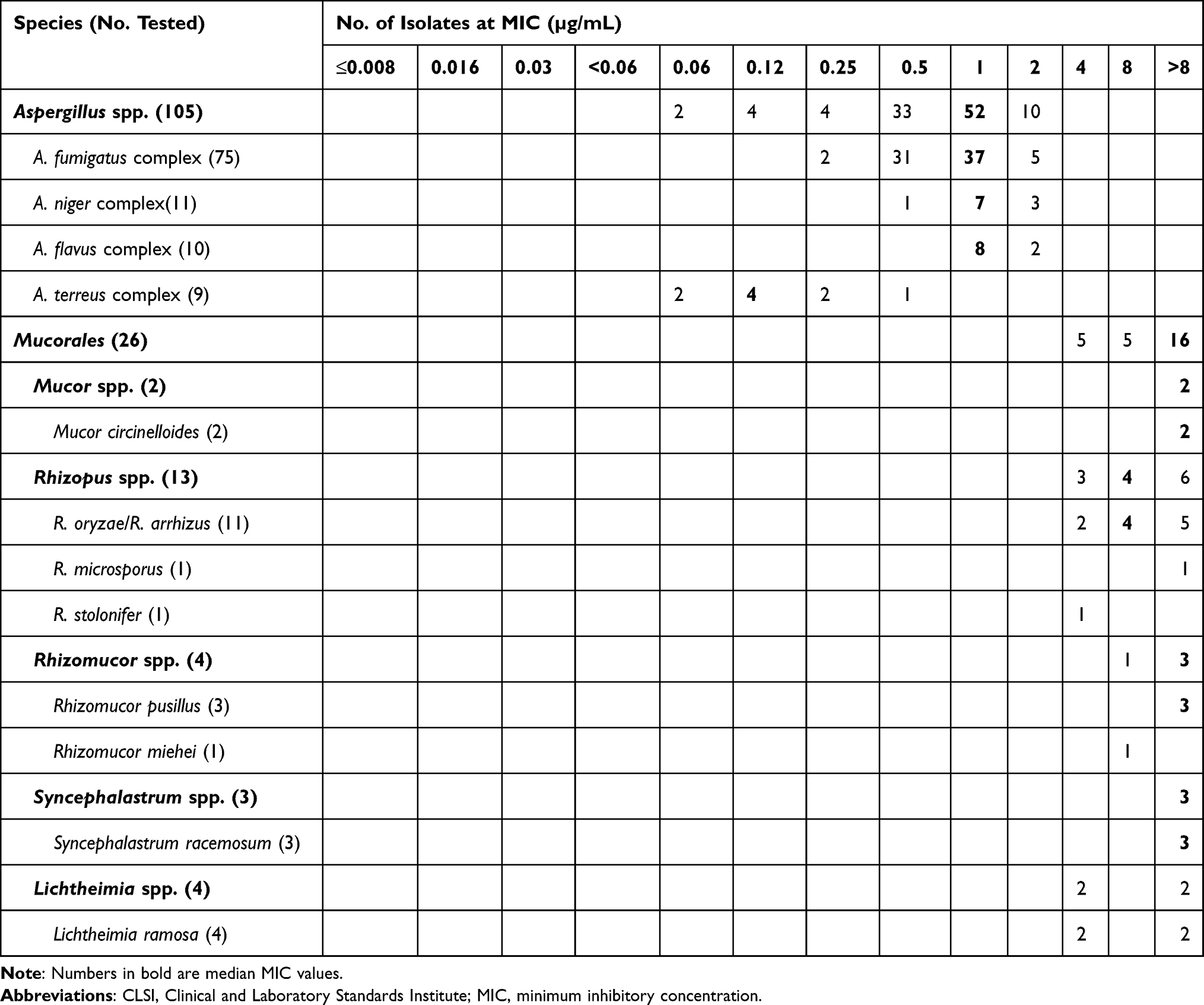 |
Table 4 MIC Distributions for Voriconazole Against Aspergillus spp. and Species of Mucorales Order Using CLSI Broth Microdilution Methods |
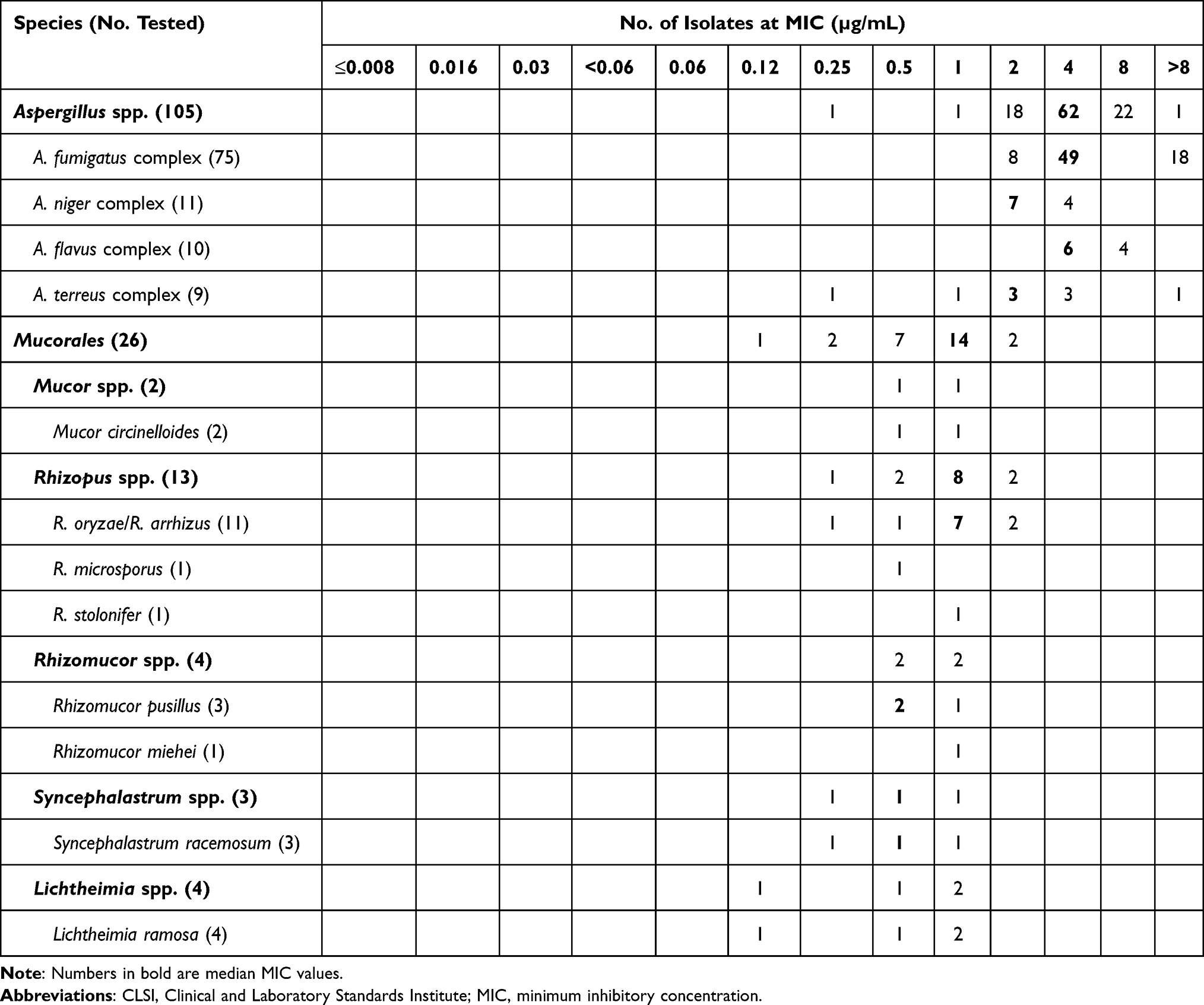 |
Table 5 MIC Distributions for Amphotericin B Against Aspergillus spp. and Species of Mucorales Order Using CLSI Broth Microdilution Methods |
Compared with Aspergillus spp., ISA demonstrated better activity against the isolates of Mucorales order (n = 26) and Rhizopus spp. with an MIC50 of 0.5 μg/mL (Table 3). However, VOR lacked any meaningful activity against the Mucorales order with both MIC50 and MIC90 values of >8 μg/mL across all species (Table 3).
Overall, from in vitro data, AMB was the most active fungistatic-agent against the Mucorales order with an MIC range of 0.12–2 μg/mL, compared with an MIC range of 0.25–>8 μg/mL for Aspergillus spp. (Table 3). Additionally, MIC50 and MIC90 values for Mucorales order were much lower (1 µg/mL) than that of Aspergillus spp. (MIC50: 4 µg/mL; MIC90: 8 µg/mL) (Table 3). Both strains of M. circinelloides (M35 and M49) studied were resistant to VOR (MIC >8 μg/mL). However, ISA demonstrated strong activity against M. circinelloides-M49 (MIC = 0.5 μg/mL) and no activity against M. circinelloides-M35 (MIC = 8 μg/mL) (Table 3). Notably, among three strains of S. racemosum included, ISA demonstrated an MIC of 0.5 μg/mL for two strains; and no in vitro activity against one of strain with an MIC of >8 μg/mL (Table 3).
Genetic Alignment of CYP51s (M. circinelloides Strains)
Molecular description of CYP 51 homologous genes (CYP51F5 and CYP51F1) in M. circinelloides is summarized in Table 1. CYP51F5 and CYP51F1 were originally acquired from A. fumigatus CYP51A and CYP51B, with more than 40% similarity in amino acid sequences. Nucleotide sequences were 1773 bp and 1658 bp and protein sequences were 512 and 510 amino acids in CYP51F1 and CYP51F5, respectively.
We tested if there was a Y129F substitution or other amino acid mutations existed in M. circinelloides CYP51s which possibly affected their intrinsic resistance to ISA and VOR.
Consensus sequences for CYP51F1 and CYP51F5 were aligned against each other. The CYP51s of M. circinelloides-M35, M. circinelloides-M49, and Erg11 of S. cerevisiae S288C were screened for amino acid substitutions previously and confirmed as correlation to resistance to short-tailed azoles (e.g. VOR) in different fungal species (analogous to Y140F in S. cerevisiae).23,24 As depicted in Figure 1, Erg11 of S. cerevisiae S288C and CYP51F1s of both strains of M. circinelloides retained a tyrosine residue (alignment of Y140 for S. cerevisiae and Y130 for M. circinelloides). On the contrary, alignment identified a phenylalanine 129 substitution (Y129F, Y140F S. cerevisiae) conserved in CYP51F5s of both M. circinelloides. There was another V (valine) to A (alanine) substitution (V311 for S. cerevisiae) observed in CYP51F5s (293A for both M. circinelloides). A total of four CYP51s sequences of the two M. circinelloides strains, M35-CYP51A, M49-CYP51A, M35-CYP51B, and M49-CYP51B have been deposited in GenBank (https://www.ncbi.nlm.nih.gov/genbank/; accession numbers OM976985, OM976986, OM976987, and OM976988).
 |
Figure 1 Amino acid sequence alignment of lanosterol 14-α demethylase between Saccharomyces cerevisiae S288C and tested Mucor circinelloides CYP51s. Alignment using Saccharomyces cerevisiae S288C Erg11 (CYP51) as reference, Y140 (a tyrosine residue) is marked in bold, the previously confirmed mutation as correlation to resistance to voriconazole in different fungi species (analogous to Y140F in S. cerevisiae), and the change to phenylalanine (129F) is seen in both M. circinelloides CYP51F5s, displayed in bold and red. Another amino acid mutation of V (valine) to A (alanine) (position V311 in S. cerevisiae, and mutated to 293A for M. circinelloides numbering) potentially related to resistance to voriconazole is also observed in both M. circinelloides CYP51F5s, displayed in bold and red. |
Discussion
Isavuconazole has been indicated for the treatment of IFIs in the USA and Europe since 2015. However, due to limited data from studies in China, it is currently unavailable for the treatment of IFIs in China. This was the first multicenter study to evaluate the in vitro activity of ISA and its comparators (VOR and AMB) against clinical isolates of Aspergillus spp. and Mucorales order in China.
Both azoles exhibited a low MIC50 and MIC90 against combined Aspergillus spp. However, AMB was less active than the azoles against Aspergillus spp. with high MICs. In this study, AMB was less active against Aspergillus species, including A. flavus complexes, A. terreus complexes, and A. fumigatus complexes. It is well-documented that the majority of strains from A. terreus and A. flavus complexes are intrinsically resistant to AMB, and VOR is recommended as the first line of treatment.25 Additionally, A. fumigatus isolates were less susceptible to AMB, with 89.3% of non-WT isolates susceptible to AMB. There are several possibilities for this observation. First, the CLSI range of MICs of AMB to the reference strain (A. fumigatus ATCC®MYA-3627™) was from 0.5–4 µg/mL,19 thus the MIC of AMB against A. fumigatus in our study was in the upper limit of CLSI MIC range. Notably, a study from Canada indicated that 96.4% (188/195) of A. fumigatus isolates were less susceptible to AMB,26 which was higher than our study (89.3%). This suggested that widespread AMB resistance might be gradually trending in many parts of the world including Canada and northern areas of China. Since AMB has been the recommended drug of choice for IA treatment, a large-scale and long-term use might result in an increasing trend of resistance to A. fumigatus. Given that the AMB susceptibility patterns could vary among geographic/ecological populations, Ashu et al. indicated that local clinicians should understand the limitations of the aforementioned recommendations,26 and apply stewardship in the management of AMB. However, whether AMB resistance is also common in other parts of China remains to be investigated in a study with a larger sample size from various regions. Azoles demonstrated contrasting activity against isolates from the Mucorales order, with an MIC50 of 0.5 µg/mL and MIC90 of 1 µg/mL for ISA and an MIC50 of 8 µg/mL and MIC90 of >8 µg/mL for VOR. An MIC50 and MIC90 of 1 µg/mL was reported for AMB.
Rhizopus spp. has been reported as the most frequent cause of mucormycosis worldwide (~48–66%), followed by Mucor spp. (14%) and Lichtheimia spp. (13%)27–29 with R. arrhizus being identified as the most common (33%) sub-species.29 The present study corroborates earlier reports, in that Rhizopus spp. was the most predominant cause of mucormycosis, with fewer Mucor spp. isolated. Moreover, the sites from which isolates were cultured in the current study (i.e., LRT) were also more frequent in the prior study,29 as also reported in an epidemiology and susceptibility study conducted in USA.30
In addition to an increase in the incidence of IMIs globally and in China,1–3,8,31 a gradual increase in patients with COVID-19 co-infected with IA or mucormycosis has also been reported.32–36 The incidence of invasive pulmonary aspergillosis in patients with COVID-19 ranged from 19.4–33.3%.33 Considering the possibility of combined infections as well as limited availability of antifungal agents in China, development of new antifungal drugs is critical for effective treatment. Many isolates of the Mucorales order are resistant to the echinocandin and azole classes of antifungals.37,38 Besides, due to the disadvantages of the currently recommended VOR and available AMB,9,39 there is a need for drugs such as ISA which has been developed as a more effective and safer antifungal azole that may be used to treat a wide range of IMIs.16,17
In the current study, both ISA and AMB demonstrated considerable activity against most species of the Mucorales order and exhibited better activity than VOR. However, similar activities were observed between ISA and VOR against Aspergillus spp., with MICs ranging between 0.06–4 μg/mL. Overall, our findings in clinical isolates of molds from China were consistent with studies conducted in the Netherlands/India and Denmark (Table 6) in that ISA (MIC ranges: 0.125–≥8 μg/mL) and AMB (MIC ranges: ≤0.03–1 μg/mL) exhibited notably increased activity compared with VOR (MIC ranges: 1–≥16 μg/mL) against isolates from the Mucorales order. Notably, Rhizopus spp. strains in China were more susceptible to ISA with MICs between 0.06–2 μg/mL compared with those tested in the Netherlands/India and Denmark with MICs between 0.125–8 μg/mL (Table 6). Strains from the Mucorales order such as M. circinelloides, isolated from the US demonstrated higher MICs for ISA (2–>16 μg/mL) and AMB (≤0.03–8 μg/mL) compared with those from China (ISA: 0.5–8 μg/mL; AMB: 0.5–1 μg/mL) (Table 6).
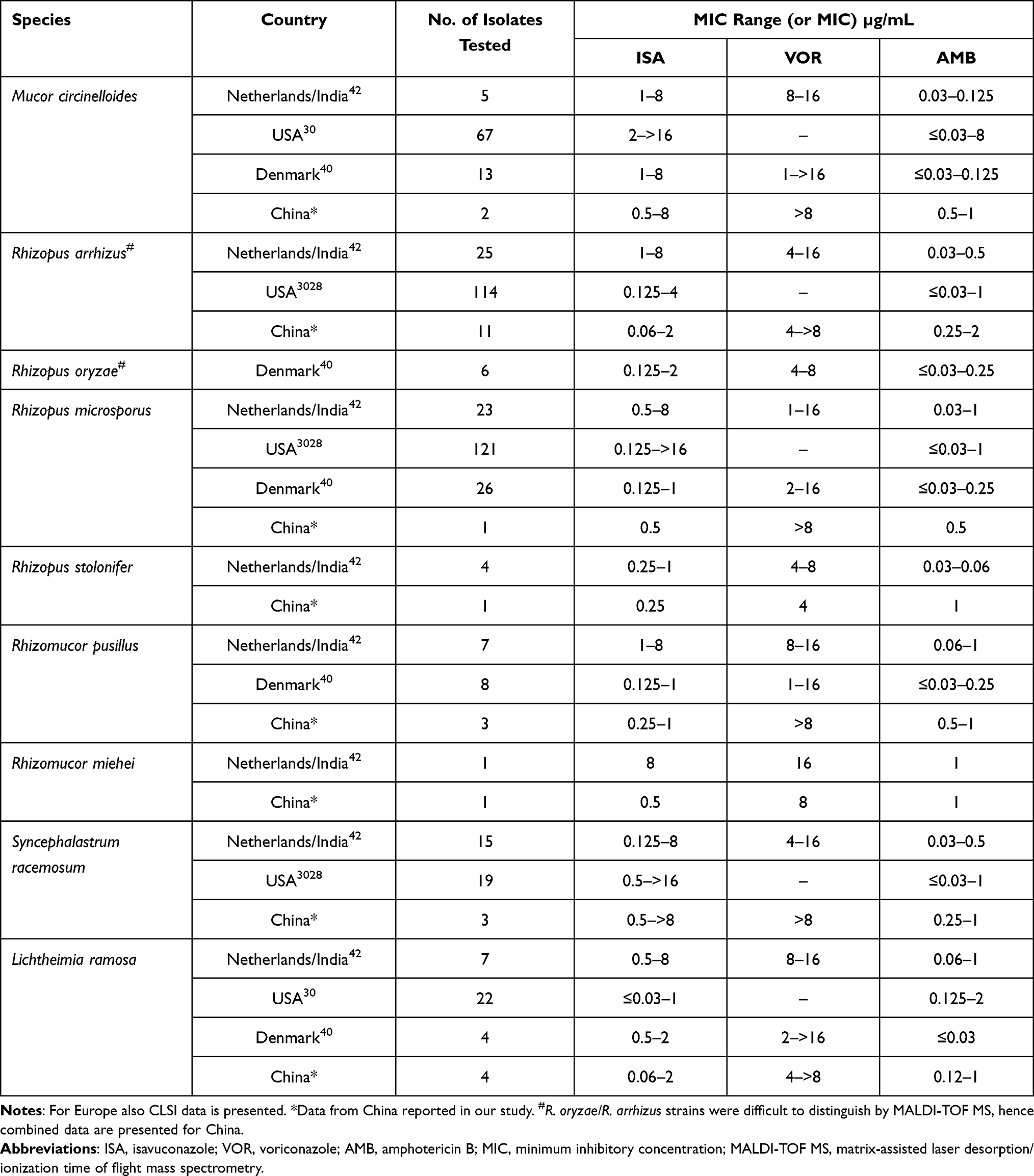 |
Table 6 Review of MICs of Isavuconazole and Comparator Antifungal Agents (Voriconazole and Amphotericin B) MICs of Major Mucorales Order Using CLSI Broth Microdilution Methods Reported in Different Countries |
Of the two M. circinelloides strains identified, M35 was resistant and M49 was sensitive to ISA. These results do not corroborate the results reported by Arendrup et al., in which ISA exhibited in vitro activity against isolates of Mucorales order except for M. circinelloides (13 isolates evaluated).40 Another possible contribution to VOR resistance (short-tailed azoles) by V293A (M. circinelloides) substitution (V311A, S. cerevisiae) was reported in two different functional analysis and structure-based studies.41 There was a V (valine) to A (alanine) substitution (V311 for S. cerevisiae) observed in CYP51F5s (293A for both M. circinelloides). Therefore, results observed in the current study are consistent with a previous study in which the Y129F substitution in M. circinelloides CYP51F5 possibly affected its intrinsic resistance to VOR, with the V293A substitution also potentially playing a role. As ISA belongs to mid-tailed azoles,41 the substitutions on Y129F and V293A in M. circinelloides CYP51F5 found in both M35 and M49 did not appear to be associated with ISA resistance in M. circinelloides-M35.
Despite Syncephalastrum spp. rarely causing mucormycosis and fewer cases reported,29 ISA resistance in one S. racemosum strain was observed in this study. The occurrence of ISA resistance in M. circinelloides and S. racemosum suggested that there may be species-specific differences in susceptibility patterns of several species of Mucorales order. Therefore, rapid identification of infection causing species and improved surveillance is critical to ensure optimal treatment.
Conclusion
ISA exhibited in vitro activity against most clinical isolates from the Mucorales order. Among clinical isolates of Aspergillus spp., similar MICs were reported for ISA and other azoles (VOR). However, as with all antimicrobial agents, clinicians should employ appropriate stewardship to minimize potential resistance to antifungals, and rationally deploy new antifungals in the treatment of IA and mucormycosis.
Abbreviations
AMB, amphotericin B; BMD, broth microdilution; Clinical and Laboratory Standards Institute, CLSI; IA, invasive aspergillosis; IMI, invasive mold infection; ISA, isavuconazole; ITS, internal transcribed spacer; MALDI-TOF MS, matrix-assisted laser desorption/ionization time of flight mass spectrometry; MIC, minimum inhibitory concentration; RPMI, Roswell Park Memorial Institute; SDA, Sabouraud dextrose agar; VOR, voriconazole.
Acknowledgments
The study was performed by the Department of Clinical Laboratory, Peking Union Medical College Hospital, China, and supported by Pfizer Inc. We thank IHMA Europe Sarl, Switzerland for providing technical guidance. Editorial support was provided by Varkha Agrawal (Ph.D., CMPP™) an employee of Pfizer.
Funding
This work was supported by the Pfizer Inc., Special Foundation for National Science and Technology Basic Research Program of China [grant number: 2019FY101204], Fundamental Research Funds for the Central Universities [grant number: 3332020005], and the Beijing Key Clinical Specialty for Laboratory Medicine Excellent Project [grant number: ZK201000]. Sponsors have no role in any of the stages from study design to submission of the paper for publication.
Disclosure
IM received an institutional research grant. JAA, JW, and EAU are current employees of Pfizer and may hold stock/stock options with Pfizer. The authors report no other conflicts of interest in this work.
References
1. Bitar D, Lortholary O, Le Strat Y, et al. Population-Based Analysis of Invasive Fungal Infections, France, 2001–2010. Emerg Infect Dis. 2014;20(7):1149–1155. doi:10.3201/eid2007.140087
2. Donnelley MA, Zhu ES, Thompson GR. Isavuconazole in the treatment of invasive aspergillosis and mucormycosis infections. Infect Drug Resist. 2016;9:79–86.
3. Kontoyiannis DP, Yang H, Song J, et al. Prevalence, clinical and economic burden of mucormycosis-related hospitalizations in the United States: a retrospective study. BMC Infect Dis. 2016;16(1):730.
4. Farmakiotis D, Kontoyiannis DP. Mucormycoses. Infect Dis Clin North Am. 2016;30(1):143–163.
5. Meis JF, Chakrabarti A. Changing epidemiology of an emerging infection: zygomycosis. Clin Microbiol Infect. 2009;15 Suppl 5:10–14.
6. Prakash H, Chakrabarti A. Global Epidemiology of Mucormycosis. J Fungi. 2019;5(1):457.
7. Chakrabarti A, Das A, Mandal J, et al. The rising trend of invasive zygomycosis in patients with uncontrolled diabetes mellitus. Med Mycol. 2006;44:335–342.
8. Liao Y, Chen M, Hartmann T, Yang RY, Liao WQ. Epidemiology of opportunistic invasive fungal infections in China: review of literature. Chin Med J. 2013;126:361–368.
9. Patterson TF, Thompson GR, Denning DW, et al. Practice Guidelines for the Diagnosis and Management of Aspergillosis: 2016 Update by the Infectious Diseases Society of America. Clin Infect Dis. 2016;63:e1–e60.
10. ECDC. European Centre for Disease Prevention and Control. Risk assessment on the impact of environmental usage of triazoles on the development and spread of resistance to medical triazoles in Aspergillus species; 2013. Available from: https://www.ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/risk-assessment-impact-environmental-usage-of-triazoles-on-Aspergillus-spp-resistance-to-medical-triazoles.pdf.
11. van der Linden JW, Arendrup MC, Warris A, et al. Prospective Multicenter International Surveillance of Azole Resistance in Aspergillus fumigatus. Emerg Infect Dis. 2015;21(6):1041–1044. doi:10.3201/eid2106.140717
12. Dannaoui E. Antifungal resistance in mucorales. Int J Antimicrob Agents. 2017;50(5):617–621.
13. Personett HA, Kayhart BM, Barreto EF, et al. Renal Recovery following Liposomal Amphotericin B-Induced Nephrotoxicity. Int J Nephrol. 2019;2019:8629891.
14. EMA. Cresemba; 2021. Available form: https://www.ema.europa.eu/en/medicines/human/EPAR/cresemba;.
15. Drug Trials USFDA. Snapshots: CRESEMBA (aspergillosis); 2020. Available form: https://www.fda.gov/drugs/drug-approvals-and-databases/drug-trials-snapshots-cresemba-aspergillosis.
16. Guillen Vera D, Ruiz Ruigómez M, García Moguel I, Morales Ruiz R, Corbella L, Fernández Rodríguez C. Successful Treatment of Chronic Pulmonary Aspergillosis With Isavuconazole. J Investig Allergol Clin Immunol. 2019;29(6):459–460.
17. McCarthy MW, Moriyama B, Petraitiene R, Walsh TJ, Petraitis V. Clinical Pharmacokinetics and Pharmacodynamics of Isavuconazole. Clin Pharmacokinet. 2018;57(12):1483–1491.
18. CLSI. Clinical and Laboratory Standards Institute. M38 Reference Method for Broth Dilution Antifungal Susceptibility Testing of Filamentous Fungi. Available from. https://clsi.org/media/1894/m38ed3_sample.pdf.
19. CLSI. Clinical and Laboratory Standards Institute. M61 (Ed2), Performance Standards for Antifungal Susceptibility Testing of Filamentous Fungi. Available from: https://clsi.org/standards/products/microbiology/documents/m61/.
20. Nelson DR. The Cytochrome P450 Homepage. Hum Genomics. 2009;4(1):59.
21. Espinel-Ingroff A, Chakrabarti A, Chowdhary A, et al. Multicenter evaluation of MIC distributions for epidemiologic cutoff value definition to detect amphotericin B, posaconazole, and itraconazole resistance among the most clinically relevant species of Mucorales. Antimicrob Agents Chemother. 2015;59(3):1745–1750.
22. CLSI. Clinical and Laboratory Standards Institute. M59, Epidemiological cutoff values for antifungal susceptibility testing. Available from: https://clsi.org/media/1934/m59ed2_sample-updated.pdf.
23. Chau AS, Chen G, McNicholas PM, Mann PA. Molecular basis for enhanced activity of posaconazole against Absidia corymbifera and Rhizopus oryzae. Antimicrob Agents Chemother. 2006;50:3917–3919.
24. Wheat LJ, Connolly P, Smedema M, et al. Activity of newer triazoles against Histoplasma capsulatum from patients with AIDS who failed fluconazole. J Antimicrob Chemother. 2006;57:1235–1239.
25. Rudramurthy SM, Paul RA, Chakrabarti A, Mouton JW, Meis JF. Invasive Aspergillosis by Aspergillus flavus: epidemiology, Diagnosis, Antifungal Resistance, and Management. J Fungi. 2019;5(55):1–33.
26. Ashu EE, Korfanty GA, Samarasinghe H, et al. Widespread amphotericin B-resistant strains of Aspergillus fumigatus in Hamilton, Canada. Infect Drug Resist. 2018;11:1549–1555.
27. Alvarez E, Sutton DA, Cano J, et al. Spectrum of zygomycete species identified in clinically significant specimens in the United States. J Clin Microbiol. 2009;47:1650–1656.
28. Cornely OA, Alastruey-Izquierdo A, Arenz D, et al. Global guideline for the diagnosis and management of mucormycosis: an initiative of the European Confederation of Medical Mycology in cooperation with the Mycoses Study Group Education and Research Consortium. Lancet Infect Dis. 2019;19(12):e405–e421.
29. Jeong W, Keighley C, Wolfe R, et al. The epidemiology and clinical manifestations of mucormycosis: a systematic review and meta-analysis of case reports. Clin Microbiol Infect. 2019;25(1):26–34.
30. Badali H, Cañete-Gibas C, McCarthy D, et al. Epidemiology and Antifungal Susceptibilities of Mucoralean Fungi in Clinical Samples from the United States. J Clin Microbiol. 2021;59:e01230–21.
31. Gong Y, Li C, Wang C, et al. Epidemiology and Mortality-Associated Factors of Invasive Fungal Disease in Elderly Patients: a 20-Year Retrospective Study from Southern China. Infect Drug Resist. 2020;13:711–723.
32. Alanio A, Dellière S, Fodil S, Bretagne S, Mégarbane B. Prevalence of putative invasive pulmonary aspergillosis in critically ill patients with COVID-19. Lancet Resp Med. 2020;8(6):e48–e49.
33. van Arkel ALE, Rijpstra TA, Belderbos HNA, van Wijngaarden P, Verweij PE, Bentvelsen RG. COVID-19-associated Pulmonary Aspergillosis. Am J Respir Crit Care Med. 2020;202(1):132–135.
34. Wang J, Yang Q, Zhang P, Sheng J, Zhou J, Qu T. Clinical characteristics of invasive pulmonary aspergillosis in patients with COVID-19 in Zhejiang, China: a retrospective case series. Crit Care. 2020;24(1):299.
35. Salmanton-García J, Sprute R, Stemler J, et al. COVID-19-Associated Pulmonary Aspergillosis, March-August 2020. Emerg Infect Dis. 2021;27:1077–1086.
36. Pasero D, Sanna S, Liperi C, et al. A challenging complication following SARS-CoV-2 infection: a case of pulmonary mucormycosis. Infection. 2020;1:45. doi:10.1007/s15010-020-01561-x
37. Li Y, Wang H, Hou X, Huang -J-J, Wang P-C, Xu Y-C. Identification by Matrix-Assisted Laser Desorption Ionization–Time of Flight Mass Spectrometry and Antifungal Susceptibility Testing of Non-Aspergillus Molds. Front Microbiol. 2020;11:922.
38. Wiederhold NP. Antifungal resistance: current trends and future strategies to combat. Infect Drug Resist. 2017;10:249–259.
39. Lanternier F, Poiree S, Elie C, et al. Prospective pilot study of high-dose (10 mg/kg/day) liposomal amphotericin B (L-AMB) for the initial treatment of mucormycosis. J Antimicrob Chemother. 2015;70:3116–3123.
40. Arendrup Maiken CJR. In Vitro Activity of Isavuconazole and Comparators against Clinical Isolates of the Mucorales Order. Antimicrob Agents Chemother. 2015;59(12):7735–7742.
41. Caramalho R, Monk BC, Larentis T, Lass-Flörl C, Lackner M. Intrinsic short-tailed azole resistance in mucormycetes is due to an evolutionary conserved aminoacid substitution of the lanosterol 14α-demethylase. Sci Rep. 2017;7:15898.
42. Chowdhary A, Singh PK, Kathuria S, Hagen F, Meis JF. Comparison of the EUCAST and CLSI Broth Microdilution Methods for Testing Isavuconazole, Posaconazole, and Amphotericin B against Molecularly Identified Mucorales Species. Antimicrob Agents Chemother. 2015;59:7882–7887.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.