Back to Journals » International Journal of General Medicine » Volume 16
Improving the Efficiency of Medication Reconciliation in Two Taiwanese Hospitals by Using the Taiwan National Health Insurance PharmaCloud Medication System
Authors Huang PP, Poon SYK ![]() , Chang SH, Kuo CW, Chien MW, Chen CC, Chiang SC
, Chang SH, Kuo CW, Chien MW, Chen CC, Chiang SC
Received 15 September 2022
Accepted for publication 9 January 2023
Published 19 January 2023 Volume 2023:16 Pages 211—220
DOI https://doi.org/10.2147/IJGM.S389683
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Luca Testarelli
Pei-Pei Huang,1,* Samantha Yun-Kai Poon,2,* Shao-Hsuan Chang,3 Chien-Wen Kuo,4 Ming-Wen Chien,1 Chien-Chih Chen,5 Shao-Chin Chiang2,6
1Division of Outpatient Pharmacy, Department of Pharmacy, Cheng Hsin General Hospital, Taipei, Taiwan; 2Department of Pharmacy, College of Pharmaceutical Sciences, National Yang Ming Chiao Tung University (Yang Ming Campus), Taipei, Taiwan; 3Department of Pharmaceutical Outcomes and Policy, College of Pharmacy, University of Florida, Gainesville, FL, USA; 4Department of Pharmacy, Cheng Hsin General Hospital, Taipei, Taiwan; 5Division of Colorectal Surgery, Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan; 6Department of Pharmacy, Koo Foundation Sun Yat-Sen Cancer Center, Taipei, Taiwan
*These authors contributed equally to this work
Correspondence: Shao-Chin Chiang, Department of Pharmacy, College of Pharmaceutical Sciences, National Yang Ming Chiao Tung University (Yang Ming Campus), Taipei, Taiwan, Tel +886-983641216, Email [email protected]; [email protected]
Purpose: Medication reconciliation (MedRec) is a process to ensure complete and accurate communication of patient medication information throughout care transitions to prevent medication errors. Hospitals in Taiwan have stride to implement a universal protocol for MedRec. To establish a feasible protocol indigenously, the World Health Organization (WHO) protocol was incorporated with the Taiwan National Health Insurance (NHI) PharmaCloud patient medication profile. The efficiency and error detection capability of this modified protocol was evaluated in two hospitals.
Methods: A prospective, non-randomized, unblinded, multicenter cohort study was conducted. Subjects were recruited among patients admitted for colorectal or orthopedic surgery with at least 4 or more chronic drugs. To obtain the best possible medication history (BPMH), the control group was conducted according to the WHO protocol, and the experimental group used the modified WHO protocol with the medication data from the PharmaCloud system. The time spent on the two protocols was recorded. Admission and discharge orders were reconciled against the BPMH to identify any discrepancies. Discrepancies were evaluated by appropriateness, prescribing intentions, and types of inappropriateness. The levels of potential harm were classified for inappropriate discrepancies.
Results: The mean time to obtain BPMH in the control group was 34.3± 10.8 minutes and in the experimental group 27.5± 11.5 minutes (P = 0.01). The experimental group had more subjects with discrepancies (87.9%) than the control (58.3%) (p < 0.001). The discrepancies in both admission and discharge orders for the experimental group (84.5 and 67.2%) were higher than those of the control (47.9 and 37.5%). Many inappropriate discrepancies were classified as the potential harm of level 2 (77.8%).
Conclusion: Through the establishment of BPMH with the medication data from the Taiwan NHI PharmaCloud, MedRec could be achieved with greater efficiency and error detection capability in both the admission and discharge order validation processes.
Keywords: medication reconciliation, prescription discrepancy, PharmaCloud, best possible medication history, BPMH
Introduction
Medication reconciliation (MedRec) is a process to ensure that accurate and complete patient medication information is consistently communicated throughout care transitions so that all changes in medications are carefully evaluated. It is a process that requires tremendous and multidisciplinary effort across an implementing organization. Currently, one of the challenges faced by many institutions is to acquire the best possible medication history (BPMH) accurately and efficiently. The BPMH is defined as a medication list obtained by a healthcare provider that includes all current medications before the transition through several different sources of information.1–3
The typical sources of obtaining BPMH are: (1) a report directly from the patient or his/her family caregivers, (2) the institutional electronic medical record (EMR) system, and (3) the medication profile provided by a third-party payer. For a MedRec process compliant with the WHO protocol to obtain BPMH, patient involvement is heavily relied on. However, self-reported information is often found to be insufficient and inaccurate.4,5 The hospital EMR system does not have cross-institutional access. The third-party insurer may be able to provide cross-institutional information, but the information could cover only a limited region.
According to a 2016 US review that discussed the problems of MedRec,6 as many as 46 minutes are required to obtain a BPMH from patients at admission, resulting in some estimated personnel costs of up to USD 46 per patient (calculated from the mean pharmacist hourly wage in 2021). This would equate to 9 full-time personnel of 500 beds with an estimated 23,500 annual admissions.7,8
It is laborious to be fully compliant with the WHO protocol for MedRec, which requires operational, cultural change and process redesign at multiple levels. Hospitals are required to invest a large number of resources in personnel and information systems. Institutions may not deliver tangible results due to partial implementation in the process. This is why, although the importance of MedRec has been emphasized in many publications, its actual implementation is still complex and challenging.
The Taiwan National Health Insurance Administration (NHIA) introduced PharmaCloud in 2013, which is an electronic platform that provides NHI-covered medication profiles for an individual patient and can be accessed by prescribers and pharmacists upon the patient’s authorization. A few studies in Taiwan demonstrated the potential benefits of PharmaCloud on various medication-related topics, such as reducing medication duplication, expenses, and wastage.9–11 Nevertheless, ensuring patient safety with the completeness and precision of the BPMH by using PhamaCloud has not yet been published.
Currently, healthcare institutions in Taiwan have yet to fully implement a universal protocol for medication reconciliation. To establish the critical steps of collecting BPMH in this indigenous protocol, the purpose of this study is to evaluate the efficiency and error detection capability of medication reconciliation with and without the aid of PharmaCloud in two hospitals in Taiwan.
Methods
Study Design
This was a prospective, non-randomized, unblinded, multicenter cohort study with a control group and an experimental group. All procedures of the two groups were the same; the only difference was the inclusion of the PharmaCloud system for the experimental group. An eligible patient or one of their family caregivers was provided with informed consent to participate in the study through a designated pharmacist, who was trained to collect data for the study.
Participant Criteria
Potential participants were screened from the daily inpatient admission list according to the following criteria:
Inclusion criteria: (1) 20 years of age or older; (2) at least four preadmission medications for chronic diseases; 3) scheduled for colorectal or orthopedic surgery within 48 hours;
Exclusion criteria: (1) discharged against medical advice; (2) transferred to another hospital during the same hospitalization; (3) unable to communicate and did not have a family caregiver for the interview.
Data Collection
Data were collected from August 2019 to July 2020. There were significant delays and disruptions due to COVID-19 pandemic restrictions. As pandemic control, some scheduled surgeries were canceled, the stay of family caregivers in the patient ward was restricted, and more patients and guardians declined the invitation to participate to avoid the risk of infection. The recruitment of subjects was carried out at two locations in Taipei, Taiwan, ie, the Cheng Hsin General Hospital (CHGH) and the Koo Foundation Sun Yat-Sen Cancer Center (KFSYSCC). Patients scheduled for orthopedic surgery at CHGH and cancer patients scheduled for colorectal surgery at KFSYSCC were recruited.
Obtaining the BPMH
In the control group, the WHO protocol of MedRec was carried out in which the designated pharmacist obtained the BPMH through the hospital EMR and patient interviews. In the experimental group, not only was the WHO protocol followed, the PharmaCloud was also used to obtain the BPMH. The PharmaCloud medication profile was downloaded from the cloud database built by NHIA to the hospital EMR system and then the designated pharmacist recorded the medications in a standard form. The completed BPMHs were attached to the EMR system for the prescribers’ reference.
Data collected for a BPMH: date of birth, sex, weight and height, date of admission, known allergies, and complete information for each drug prescription, including date of a prescription, generic drug name, indication, strength, route, dose, frequency, duration, and prescribing institution. To clarify the actual usage by the patient before admission, the actual dose and the date and time of the last dose taken by the patient were also recorded. Additionally, to evaluate the efficiency of the procedure, the time spent in preparation before interviewing a patient, including creating the patient’s basic profile according to their EMR, declared supplementary records, and transferred notes; for the experimental group, this also included the time to download the patient’s PharmaCloud medication history, and for the subsequent interview to be recorded. All data were collected within 24 hours of admission.
Verification of Prescriptions
The prescribers developed an admission order according to the patient’s conditions and BPMH. The order was then sent to designated pharmacists for validation, where it was compared with the BPMH to identify any discrepancies. Discrepancies were communicated to the prescribers, and their appropriateness was also evaluated and documented. The following information was collected: the appropriateness of the discrepancies (appropriate vs inappropriate), the prescribing intentions (intentional vs unintentional), and the types of inappropriate discrepancies (omission, alteration, or others). An inappropriate discrepancy would cause harm to the patient. Intentional discrepancy is defined as the prescriber making the decision consciously in medication changes. For the discharge order, the same procedures as described above were also followed.
Expert Validation
Two experts, one from each hospital, were assigned to evaluate the appropriateness, prescribing intentions, and the types of discrepancies in admission and discharge orders from both hospitals. In addition, they independently determined the level of potential harm from inappropriate discrepancies according to the criteria modified from the National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) index.12 There were three levels of harm, that is, level 1: discrepancies will not cause disease progression or discomfort to the patient; level 2: discrepancies may cause mild discomfort to the patient; and level 3: discrepancies may cause disease progression or death. When a disagreement between the two experts occurred, a third was consulted for a final decision.
Data Analysis
The results were represented by numbers and percentages. The time that designated pharmacists spent to obtain BPMHs and the age of the subjects were expressed as mean ± standard deviation (SD). Differences between groups were compared using the Chi-square test or t-test where appropriate. A p value of <0.05 was interpreted as significant. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 24 (IBM Corp., Armonk, NY, USA).
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board of KFSYSCC (code: 20190108A, approved on February 13, 2019), CHGH (code: (687)180A-03, approved on March 26, 2019), and NYCU (IRB No. YM108075E, approved on June 1, 2019).
Results
There were 116 patients recruited and interviewed, and 107 were included in the final analysis. Nine patients scheduled for colorectal surgery were excluded due to changes in their disease course, including deaths (3 patients) and changes in treatment plans (6 patients). Eight were from the control group and 1 from the experimental group. Due to the cancer progression of the patients, they were no longer deemed fit to continue with surgical procedures, and the full MedRec process could not be completed. Forty-eight participants (44.9%) were assigned to the control group and 59 to the experimental group (55.1%). The mean age of the total population was 69.1 ±11.4 and most of the subjects were in the age group 68 to 80 (48.6%). The group of patients in orthopedic surgery was significantly larger in number than that in colorectal surgery (p = 0.02) (Table 1).
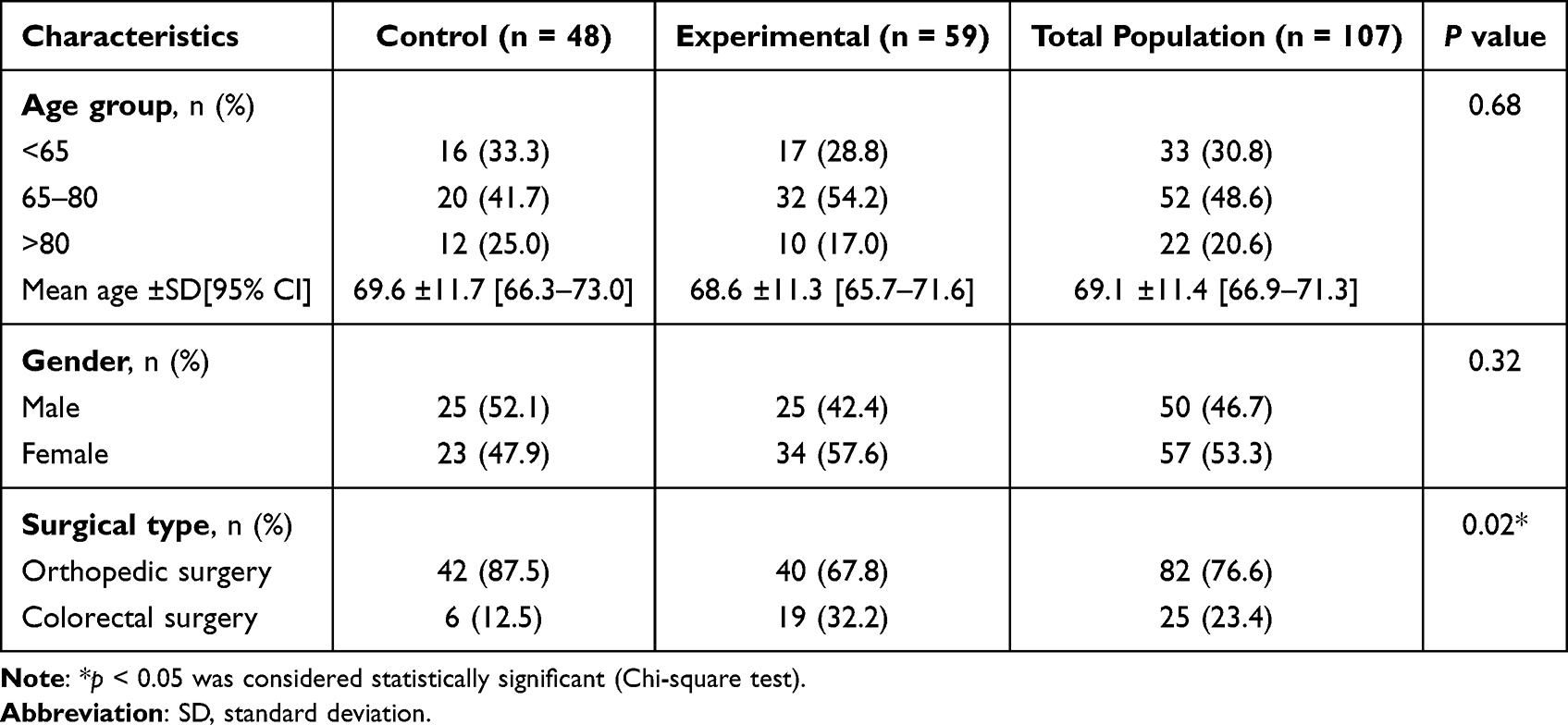 |
Table 1 Demographic Characteristics of the Study Population |
Table 2 detailed the time taken to obtain BPMHs, including the preparation and interview processes. The mean preparation time for the control (9.9 ± 4.4 minutes) and the experimental (10.9 ± 7.1 minutes) was similar without significant differences. However, for the interview time, the control group (24.4 ± 9.1 minutes) had taken up a longer time than the experimental group (16.6 ± 8.1 minutes), with a difference of 7.8 minutes (P = 0.03). The total time spent by the control group and the experimental group had a mean of 34.3 ± 10.8 minutes and 27.5 ± 11.5 minutes, respectively, and a difference of 6.8 minutes (P = 0.01).
 |
Table 2 The Time Spent to Obtain BPMH |
Out of the 107 subjects, 81 patients had medication discrepancies (75.7%) with 125 identified medication discrepancies (admission, n = 70, 56.0%, vs discharge, n = 55, 44.0%). The experimental group showed a higher percentage of subjects with medication discrepancies (87.9%) than the control group (58.3%) (P < 0.001) (Figure 1). Both groups (Figure 2) had a higher percentage of discrepancies at admission than at discharge (control: 47.9% vs 37.5%; experimental: 84.5% vs 67.2%). The discrepancies in the admission order for the experimental group (84.5%) were significantly higher than for the control (47.9%) (P = 0.001), and a similar pattern was observed for the discharge order (control 37.5 vs experimental 67.2%) (P = 0.02).
 |
Figure 1 The percentage of subjects with at least one medication discrepancy (n = 107). |
 |
Figure 2 The percentages of admission and discharge orders with discrepancies. |
Of the 125 discrepancies (from both admission and discharge orders), 27 were inappropriate (21.6%). Table 3 provided detailed information on 18 patients with at least one inappropriate discrepancy. In terms of the type of inappropriate discrepancies, similar patterns were observed in both the control and experimental groups. There were 8 inappropriate discrepancies identified in the control groups, including 2 ‘omissions’ and 6 “others”. Nineteen inappropriate discrepancies were identified in the experimental group, where 11 were “omission” and 8 were “others”. None was found to be an “alteration”. Regardless of the study groups, the 14 inappropriate discrepancies in the category “others” consisted of the following reasons: (1) patients insisted not to take the prescribed medication (9 cases), (2) patients forgot to bring their chronic medications and refused to take the products of the same active ingredient provided by the hospitals (1 case), (3) the prescribers omitted the medications because the drugs were considered unnecessary, eg, drugs for symptomatic relief (3 cases), (4) the prescriber was notified by the designated pharmacist regarding the discrepancies and agreed, but the intended order was still not prescribed (1 case).
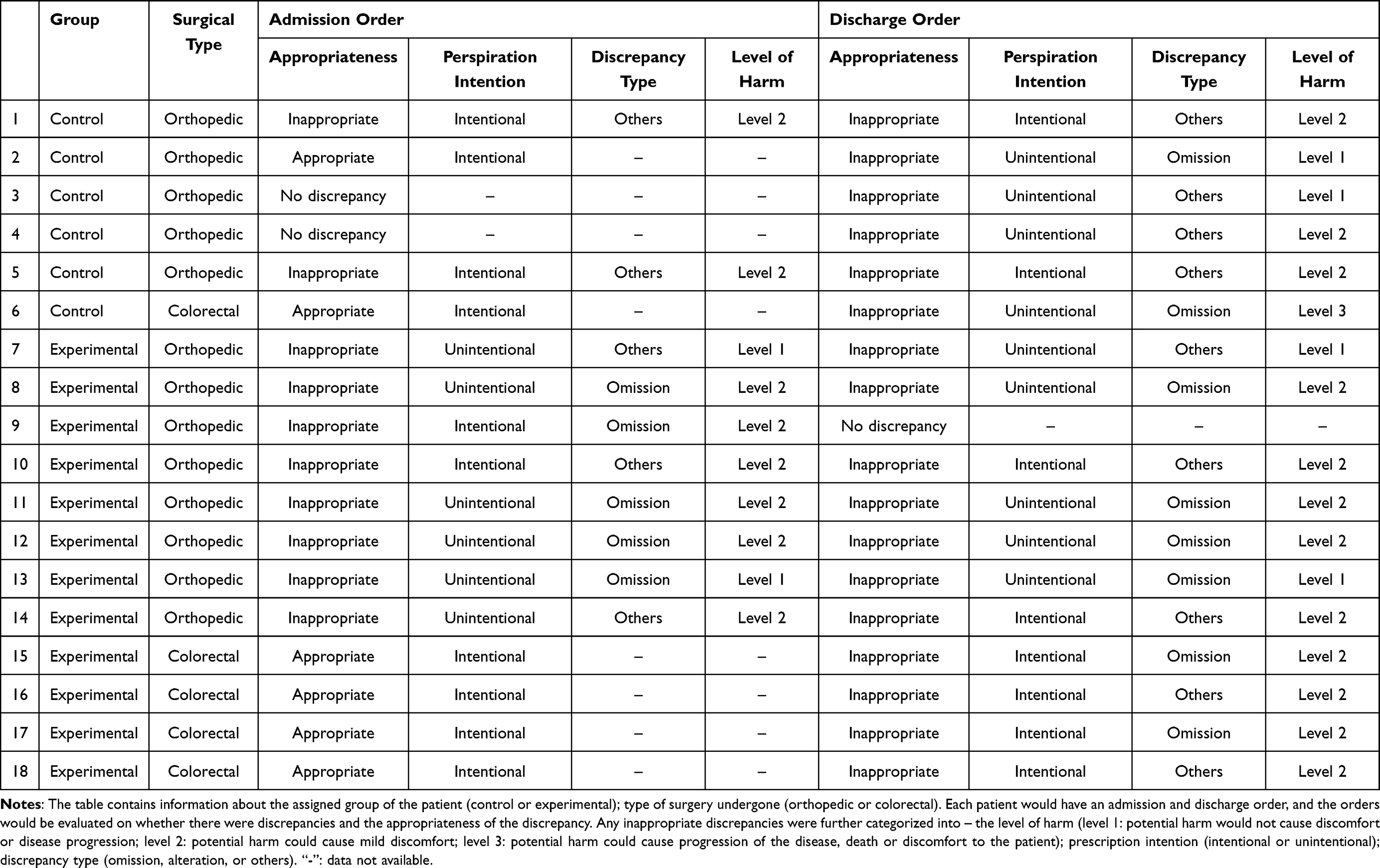 |
Table 3 List of Patients with at Least One Inappropriate Discrepancy |
Of all medication discrepancies, regardless of their appropriateness, 83.8% were deemed “intentional” and 16.2% were “unintentional”. The control group had an equal number of intentional and unintentional discrepancies, while the experimental group had more unintentional than intentional discrepancies (Table 3). No significant differences were observed between the groups and between admission and discharge orders.
For the levels of potential harm of the 27 inappropriate discrepancies (Table 3), we observed that level 2 was the majority (n = 20, 74.1%), and more than half of these level 2 discrepancies were intentional (n=12, 60.0%). An unintentional discrepancy in the discharge order in the control group was considered as level 3. The subject was reported to be diabetic and the physician mistakenly omitted an antihyperglycemic agent.
Discussion
To our knowledge, this is the first study to implement MedRec with the combination of the WHO protocol and the Taiwan NHI PharmaCloud system in hospitalized surgical patients. Through this study, we aspired to establish a standardized protocol that could be applied nationwide. The most common approach recognized in the literature is the use of in-house EMRs.6,13,14 It allows healthcare providers to have rapid access to pre-admission information as a basis to create BPMH. However, the EMR has weaknesses: (1) it requires institutional commitment and expenditures toward integration of the EMR system to accommodate MedRec practices; (2) it could not universally share information with other institutions and is unable to extract data from others.6 The PharmaCloud is unique and universally available nationwide for healthcare providers, and the system has become a tool used by NHIA to reduce the rate of medication duplication.15
Our investigation demonstrates the efficiency of using PharmaCloud to support the performance of MedRec in obtaining BPMH. We observe that the time to interview patients in the experimental group requires 8 minutes less than in the control group. Although downloading the subject’s PharmaCloud medication history takes time, it was especially instrumental in the interview sessions. Therefore, the reduced interview time contributed to a shorter total time spent in the experimental group to obtain BPMH than in the control group.
From the evaluation of the discrepancies, we observed that the subjects in the experimental group had a higher rate of discrepancy (87.9%) compared to the control (58.3%) (Figure 1). We believe this was due to the completeness of BPMH obtained through WHO standard procedures with the addition of the PharmaCloud system, which enables clinicians to identify more errors compared to traditional methodology purely through institutional EMR and interviews.
Through the discrepancies of the admission and discharge orders (Figure 2), we have demonstrated that although both groups reported a higher discrepancy in admission than in discharge orders, the difference was more prominent in the experimental group (experimental 84.5% vs control 67.2%). Other studies have suggested that discrepancies occur more frequently at hospital admissions; Tam et al’s16 systematic review found that discrepancies at the time of admission were common, up to 67.0% of occurrence; Cornish et al17 reported that 53.6% of their subjects had at least one unintended medication discrepancy; Ashcroft et al’s study18 showed that medication errors were 70% more likely to occur at admission than in other prescribing stages.
When examining all 27 inappropriate discrepancies, almost half of them were omissions. Surgical patients may require more consideration in medication modifications before the invasive procedures. Some medications are temporarily stopped due to the possible risk of surgery, so potential errors in not resuming also exists. Regarding the prescription intentions (Table 3), inappropriate discrepancies are more often classified as “unintentional”. Between 50.0 and 70.0% of the patients were reported to have experienced medication errors caused by unintended discrepancies during care transitions.19,20
Of all inappropriate discrepancies, the majority were classified as level 2 harm (74.1%, Table 3), which can cause mild discomfort to the patient. The systematic review conducted by Kwan et al3 pointed out that unintentional discrepancies would not necessarily cause serious harm to patients. It was also true in our case, except for one case of level 3 harm mentioned previously. In 2013, the Taipei Municipal Wanfang Hospital conducted a one-year study on medication reconciliation led by pharmacists. The study reported that approximately 8.0% of the patients had at least one medication error and approximately 19.0% of the medication errors had the potential to cause serious harm to the patients. In 2017, a Jordanian teaching hospital published a prospective observational study21 reporting that 47.0% of patients on the medicine wards had at least one “unintentional” medication error, and 46.0% of patients had at least one medication error. According to their analysis, these unintentional errors pose potential harm to patients or worsen disease progression, and increase the risks of harm to the elderly.
Although not the main objective of our study, during data collection, we observed that on average patients had approximately 58.2% of their medications and supplements obtained from other institutions or community pharmacies and approximately 71.0% of patients had at least one drug or diet supplement acquired from other sources. We believe that simply relying on data from a single health institute is not enough to protect hospitalized patients. From Taiwan’s example, with the NHIA providing an accessible PharmaCloud medication profile, we want to encourage the idea of having cross-regional and cross-institutional medication profile integrations. For countries without universal healthcare coverage, the government should promote health insurance company cooperations and allow the availability of an integrated medication profile for medication reconciliation. We believe that this could greatly improve patient medication use safety. The European Collaborative Action on Medication Errors and Traceability (ECAMET) recommended the introduction of medication traceability with various systems, such as electronic prescriptions, barcode medication administration, and automated dispensing cabinets, and, most essentially, complete connectivity for all systems.22
Also a prominent example from the Netherlands, all Dutch citizens are encouraged to register at a regular community pharmacy locally under the health insurance scheme. As the pharmacy has records of a patient’s prescription and medication use history, the pharmacist can check for any possible medication errors or prescription conflicts. General practitioners and hospitals could also access this information.23,24 The data content and exchange of the Dutch health claim data are well-established and have clear custodianship, and they aimed to create a data infrastructure with nationally coordinated authorization and privacy design.25 Similarly, the NHS from England has recently introduced the Summary Care Record (SCR) in community pharmacies, under patient authorization, pharmacists have instant access to patient information to prevent prescription errors, such as allergies and current medication prescriptions.26,27
Currently, patients with chronic diseases in Taiwan were able to refill their medications from NHI-registered community pharmacies. However, there is no data exchange mechanism between hospitals and community pharmacies, so data on over-the-counter medications for acute symptoms and dietary supplements are not available for MedRec in hospitals. It is also critical that patients are encouraged to authorize healthcare institutions to use their medication profiles on the PharmaCloud, so that the accuracy and efficiency of BPMH could be improved with the written promise of the institutions to protect the confidentiality of personal data.
Limitations
Some obvious drawbacks in using the PharmaCloud medication profile are: (1) it only contains NHI-covered medications and no out-of-pocket medications are recorded; (2) the database could not be accessed if the patient did not give their consent to the hospital; (3) it contains incomplete prescription information, eg, lack of information on doses, difficulty in differentiating combination products, and the problem with mistakenly duplicated upload of prescriptions by a few prescribers from local clinics intermittently.
There was an unbalanced number of patients recruited between the two hospitals. The characteristics of the subjects of the two hospitals were also slightly different. Thus, there is a potential to skew the trend and the results presented. The general hospital recruited patients from the orthopedic ward and the cancer center recruited cancer patients scheduled for colorectal surgery. Although the procedures of data collection and the formation of BPMH were the same, the effect of the pandemic was especially prominent for the cancer center as mentioned previously in the method section. Due to tighter control of COVID-19 restrictions, and the increased risk of complications in cancer patients, recruitment was greatly affected. Discrepancies were observed in the characteristic of surgical types. It is important to mention that generalization of the study results should be managed with caution.
Conclusion
With the aid of NHIA’s PharmaCloud, MedRec could be achieved with significantly higher efficiency and greater error detection capabilities in the admission and discharge order validation processes. It is necessary to incorporate the collection of patients medication profiles from the cross-institutional platform into the standard operating procedures of MedRec.
Acknowledgments
Special thanks to Professor Yu Ko (Taipei Medical University, Department of Clinical Pharmacy) for her assistance in establishing the study design. The authors thank all members of the Department of Pharmacy at KFSYSCC and CHGH who participated in the study. Jia-Yu Lin, RPh, is acknowledged for data collection at KFSYSCC. This study was supported by the Cheng-Yang project (project No. CY10814), a collaboration between the National Yang Ming Chiao Tung University (Yang Ming Campus), and the Cheng Hsin General Hospital.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. High 5s project standard operating protocol. Assuring accuracy of medication information at transitions in care: medication reconciliation. Available from: https://www.who.int/publications/m/item/high5s-standard-operating-protocol-medication-reconciliation.
2. Johnston R, Saulnier L, Gould O. Best possible medication history in the emergency department: comparing pharmacy technicians and pharmacists. Can J Hosp Pharm. 2010;63(5):359–365. doi:10.4212/cjhp.v63i5.947
3. Kwan JL, Lo L, Sampson M, Shojania KG. Medication reconciliation during transitions of care as a patient safety strategy: a systematic review. Ann Intern Med. 2013;158(5 Pt 2):397–403. doi:10.7326/0003-4819-158-5-201303051-00006
4. Goldman N, Lin IF, Weinstein M, Lin YH. Evaluating the quality of self-reports of hypertension and diabetes. J Clin Epidemiol. 2003;56(2):148–154. doi:10.1016/s0895-4356(02)00580-2
5. Gnjidic D, Du W, Pearson SA, Hilmer SN, Banks E. Ascertainment of self-reported prescription medication use compared with pharmaceutical claims data. Public Health Res Pract. 2017;27(4):27341702. doi:10.17061/phrp27341702
6. Pevnick JM, Shane R, Schnipper JL. The problem with medication reconciliation. BMJ Qual Saf. 2016;25(9):726–730. doi:10.1136/bmjqs-2015-004734
7. Meguerditchian A, Krotneva S, Reidel K, Huang A, Tamblyn R. Medication reconciliation at admission and discharge: a time and motion study. BMC Health Serv Res. 2013;13:485. doi:10.1186/1472-6963-13-485
8. Bureau of Labor Statistics, U.S. Department of Labor, occupational outlook handbook, pharmacists; 2021. Available from: https://www.bls.gov/ooh/healthcare/pharmacists.htm.
9. National Health Insurance Administration. NHI 21 Cloud Service. Available from: https://www.nhi.gov.tw/english/News_Content.aspx?n=996D1B4B5DC48343&sms=F0EAFEB716DE7FFA&s=24F7904DFB5F77AA.
10. National Health Insurance Administration. Physicians taking advantage of the NHI pharmacloud system to reduce inappropriate waste of resources. Available from: https://www.nhi.gov.tw/English/News_Content.aspx?n=996D1B4B5DC48343&sms=F0EAFEB716DE7FFA&s=678FD6BB7AB0BB1E.
11. Liao LL, Liao KM, Huang HF. The early results analysis of PharmaCloud system. J Healthc Qual. 2016;10:67–72.
12. National Coordinating Council for Medication Error Reporting and Prevention (NCC MERP) index. Medication error index: NCC MERP index for categorizing medication errors. Avilable from: https://www.nccmerp.org/sites/default/files/index-color-2021-draft-change-10-2022.pdf.
13. Wiebe N, Otero Varela L, Niven DJ, Ronksley PE, Iragorri N, Quan H. Evaluation of interventions to improve inpatient hospital documentation within electronic health records: a systematic review. J Am Med Inform Assoc. 2019;26(11):1389–1400. doi:10.1093/jamia/ocz081
14. Horsky J, Drucker EA, Ramelson HZ. Higher accuracy of complex medication reconciliation through improved design of electronic tools. J Am Med Inform Assoc. 2018;25(5):465–475. doi:10.1093/jamia/ocx127
15. Fang YY, Wu JS, Hsu CC. The effectiveness of medication safety for using PharmaCloud system. J Taiwan Taiwan Pharmacy. 2014;30(3):107–112.
16. Tam VC, Knowles SR, Cornish PL, Fine N, Marchesano R, Etchells EE. Frequency, type and clinical importance of medication history errors at admission to hospital: a systematic review. CMAJ. 2005;173(5):510–515. doi:10.1503/cmaj.045311
17. Cornish PL, Knowles SR, Marchesano R, et al. Unintended medication discrepancies at the time of hospital admission. Arch Intern Med. 2005;165(4):424–429. doi:10.1001/archinte.165.4.424
18. Ashcroft DM, Lewis PJ, Tully MP, et al. Prevalence, nature, severity and risk factors for prescribing errors in hospital inpatients: prospective study in 20 UK hospitals. Drug Saf. 2015;38(9):833–843. doi:10.1007/s40264-015-0320-x
19. Dong PTX, Pham VTT, Nguyen TT, Nguyen HTL, Hua S, Li SC. Unintentional medication discrepancies at admission among elderly inpatients with chronic medical conditions in Vietnam: a single-centre observational study. Drugs. 2022;9(1):141–151. doi:10.1007/s40801-021-00274-3
20. Vira T, Colquhoun M, Etchells E. Reconcilable differences: correcting medication errors at hospital admission and discharge. Qual Saf Health Care. 2006;15(2):122–126. doi:10.1136/qshc.2005.015347
21. Salameh L, Abu Farha R, Basheti I. Identification of medication discrepancies during hospital admission in Jordan: prevalence and risk factors. Saudi Pharm J. 2018;26(1):125–132. doi:10.1016/j.jsps.2017.10.002
22. ECAMET. The urgent need to reduce medication errors in hospitals to prevent patient and second victim harm. Available from: https://eaasm.eu/wp-content/uploads/ECAMET-White-Paper-Call-to-Action-March-2022-v3.pdf.
23. Wammes J, Stadhouders N, Westert G. International Healthcare system profiles. Netherlands; 2020. Available from: https://www.commonwealthfund.org/international-health-policy-center/countries/netherlands.
24. Van Der Luit CD, De Jong IR, Ebbens MM, et al. Frequency of occurrence of medication discrepancies and associated risk factors in cases of acute hospital admission. Pharm Pract. 2018;16(4):1301. doi:10.18549/PharmPract.2018.04.1301
25. OECD. Towards an Integrated Health Information System in the Netherlands. Paris: OECD Publishing; 2022.
26. NHS Digital. Benefits and uses of summary care records in community pharmacy. Available from: https://digital.nhs.uk/services/summary-care-records-scr/summary-care-record-scr-in-community-pharmacy/benefits-and-uses-of-scr-in-community-pharmacy.
27. NHS Digital. Summary care record in community pharmacy. Available from: https://digital.nhs.uk/services/summary-care-records-scr/summary-care-record-scr-in-community-pharmacy.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Obstacles and Opportunities in Information Transfer Regarding Medications at Discharge – A Focus Group Study with Hospital Physicians
Glans M, Midlöv P, Kragh Ekstam A, Bondesson Å, Brorsson A
Drug, Healthcare and Patient Safety 2022, 14:61-73
Published Date: 17 May 2022
Opioid Utilization and Management in the Setting of Stewardship During Inpatient Rehab Care
Murphy L, Leblanc K, Badr S, Ching E, Mao L, Steenhof N, Hamandi B, Rubin B, Seto A, Furlan AD
Drug, Healthcare and Patient Safety 2022, 14:161-170
Published Date: 11 September 2022
The Impact of Real-Time Documentation of In-Hospital Medication Changes on Preventing Undocumented Discrepancies at Discharge and Improving Physician-Pharmacist Communication: A Retrospective Cohort Study and Survey
Kim WY, Baek A, Kim Y, Suh Y, Lee E, Lee EE, Lee JY, Lee J, Park HS, Kim ES, Lim Y, Kim NH, Ohn JH, Kim S, Ryu J, Kim HW
Journal of Multidisciplinary Healthcare 2024, 17:2999-3010
Published Date: 25 June 2024
Effectiveness of Quality Use of Medicines (QUM) Programs and Strategies in Saudi Arabia: A Narrative Review
Aldhafeeri F, Wilson A, Larkin S, Aldhafeeri FM
Drug, Healthcare and Patient Safety 2025, 17:87-96
Published Date: 24 March 2025