")
Back to Journals » Advances in Medical Education and Practice » Volume 6
Improving medical students' knowledge of genetic disease: a review of current and emerging pedagogical practices
Authors Wolyniak M, Bemis L, Prunuske A
Received 8 July 2015
Accepted for publication 1 October 2015
Published 29 October 2015 Volume 2015:6 Pages 597—607
DOI https://doi.org/10.2147/AMEP.S73644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Michael J Wolyniak,1 Lynne T Bemis,2 Amy J Prunuske2
1Department of Biology, Hampden-Sydney College, Hampden-Sydney, VA, 2Department of Biomedical Sciences, University of Minnesota Medical School, Duluth, MN, USA
Abstract: Genetics is an essential subject to be mastered by health professional students of all types. However, technological advances in genomics and recent pedagogical research have changed the way in which many medical training programs teach genetics to their students. These advances favor a more experience-based education focused primarily on developing student's critical thinking skills. In this review, we examine the current state of genetics education at both the preclinical and clinical levels and the ways in which medical and pedagogical research have guided reforms to current and emerging teaching practices in genetics. We discover exciting trends taking place in which genetics is integrated with other scientific disciplines both horizontally and vertically across medical curricula to emphasize training in scientific critical thinking skills among students via the evaluation of clinical evidence and consultation of online databases. These trends will produce future health professionals with the skills and confidence necessary to embrace the new tools of medical practice that have emerged from scientific advances in genetics, genomics, and bioinformatics.
Keywords: genetics education, medical genetics, pedagogical practice, active learning, problem-based learning
Introduction
DNA encodes the blueprint for life and affects susceptibility to countless diseases, making genetics a foundational subject for all health professions. The interdisciplinary nature of modern molecular biology and the demands of medical entrance examinations like the Medical College Admission Test (MCAT) ensure that genetics will remain a foundational topic for all students aspiring for medical careers. Despite changing trends in required preclinical and clinical program course prerequisites, genetics remains a central and growing requirement for the medical disciplines. Until recently, clinical applications of genetics have been primarily limited to understand the underlying causes of rare diseases inherited in a Mendelian fashion.1 The staggering pace of scientific and technological developments in the last 2 decades, however, has changed the face of what a thorough training regimen in genetics should look like for health professionals.2,3 In 1990, less than 2% of the estimated 7,000 known Mendelian-based human disorders had a well-understood molecular basis. By 2011, this number had skyrocketed to 40%, a jump that is attributable to knowledge gained through the genomics revolution that is rapidly redefining the standard of knowledge necessary for a well-prepared medical professional.4,5 With this increased understanding of human genetics and genomics has also come an improved appreciation of the complex interrelationships between genetic and environmental factors that complicate the diagnosis of genetic diseases. The inheritance patterns of the majority of heritable diseases cannot be explained by a simple Mendelian model.6 Environmental variables, including microbial infection, environmental toxins, and lifestyle choices are all known to impact expressed phenotypes.
Thanks largely to technological advances stemming from the Human Genome Project and the bioinformatics revolution in molecular biology research, a health professional may now follow-up his or her examination of patient family histories with screens for DNA, RNA, and protein markers. However, there remain limitations to current genetic risk prediction models due to gaps in basic understanding of the interactions between components of the genome.7 Also, while there are now online databases and options to obtain personalized genomic information available to both medical professionals and the general public, such resources are only useful if the user has a solid working understanding of modern genetics and genomics.
Taken together, today’s medical professionals have access to a vast array and ever-increasing amount of resources compared with their predecessors for the diagnosis and treatment of their patients based on genetic information. However, have these medical professionals received the necessary training in basic and applied genetics to avail themselves of these resources and use them in a way that best serves their patients? Can they rapidly and efficiently decide what genetic tests are necessary in a given situation? Can they competently use the array of online resources available to them to assist in their efforts? Can they combine Mendelian and molecular information to make an accurate diagnosis and assess disease risk? Can they explain the results of these tests to the patient in a way that is accessible, respectful, and ethical? Can they prescribe and dose treatments that are both medically effective and financially cost-efficient for a particular patient? Built into these questions is the need to have a health care system with clearly defined roles for all health care providers such that primary care physicians are knowledgeable about when and how to coordinate with medical specialists, pharmacists, genetic counselors, and researchers.
As of 2013, approximately 50% of available medical genetics residencies remained vacant, a statistic that is sobering given the increasing need for medical professionals who can bring new genetic technologies into common practice.8 Also, surveys of 3rd and 4th year American and Canadian medical students suggest that only 26% are learning genetics as a part of their formal clinical training while over 50% lack basic competencies related to applying genetic tools to prospective patient care. Of academic family physicians, 54% felt that they were not knowledgeable about available genetic tests.9 Additional competency deficiencies include an understanding of when to recommend a patient to a genetic counselor, an awareness of online genetics resources like the United States National Institutes of Health’s “Online Mendelian Inheritance in Man” (OMIM), and the appropriate situations in which to refer patients to genetics specialists.10,11 While genetics education has not been neglected in medical training per se, recent work in both the biological and pedagogical arenas argues for the use of a more proactive and evidence-based approach based on evaluating clinical evidence and consulting online resources as opposed to simply memorizing content. A challenge facing medical education programs at all levels is to consider these developments and to reflect on the effectiveness of their curriculum in utilizing these best practices for the teaching of genetics as well as other principles of molecular biology. A medical genetics education focused on developing scientific critical thinking skills in health care professionals has the potential not only to increase the number of specialists available to the medical community for genetics-related fields but also to increase the overall proficiency level of all medical professionals in utilizing the vast informational resources available in today’s rapidly evolving medical landscape.8,12 As genomic data become more readily available to medical professionals, it becomes essential that not only specialists but also primary care providers be conversant in how to use modern genetics and genomics tools to make treatment decisions for their patients.3
A proactive approach to develop a medical community equipped with knowledge of the best practices in modern genetics and genomics should be built on a solid foundation in the basic principles of these fields in a student’s undergraduate and preclinical years supplemented with exposure to the evidence-based practices commonly used across medical curricula in professional schools.13 This foundation prepares the trainee for a clinical education that exposes them to the technologies and applications of modern genetic and genomic medicine so that they may proficiently implement these resources in their future practices. Here, we review the latest approaches being taken in medical genetics education to highlight how medical professionals are being equipped to bring the fruits of the modern genetics and genomics revolution to their future patients.
What educational practices will best help future medical professionals to understand and embrace modern genetics and genomics?
There are a number of different approaches to integrate the fundamentals of genetics into the training of future medical professionals. For instance, a student could be asked to take one or more dedicated courses that provide a concentrated view of the principles of genetics and genomics. This approach is effective at delivering the foundational content necessary for understanding modern genomics technologies but may not provide the sustained exposure to these concepts that would engender confidence in applying this knowledge to medical practice. Alternatively, genetics concepts can be integrated longitudinally over several different levels of a medical curriculum. This approach frees up the student to take additional specialized coursework and provides a steady exposure to genetics that instills and sustains confidence in working with modern genomic tools. However, strong coordination and organization among the faculty of a medical program is necessary to ensure that students are exposed to all necessary genetics and genomics concepts over time and that students will be adequately prepared to move on to additional training opportunities at the next level of their careers. Ultimately, striking a balance between these approaches affords the student the best opportunity to receive both breadth and depth to their medical genetics educations and to receive both the knowledge and the confidence necessary to be prepared to embrace modern genetics and genomics in future medical practice.
General pedagogical standards for medical students are largely based on the notion of competency-based education, or an education that focuses on providing students with the knowledge, skills, and attitudes needed to best serve their patients.14,15 In 2009, the American Association of Medical Colleges (AAMC) and the Howard Hughes Medical Institute (HHMI) issued a report entitled “Scientific Foundations for Future Physicians” that outlined competencies rather than a specific slate of courses students need for a career in medicine. This report emphasized the importance of combining a strong foundation in basic sciences content with the critical thinking skills necessary to integrate new scientific discoveries into medical practice.16 In this same spirit at the residency level, the Accreditation Council for Graduate Medical Education (ACGME) and American Board of Medical Specialists (ABMS) emphasize six broad competencies for residency training in the USA, including medical knowledge, patient care, interpersonal and communications skills, practice-based learning and improvement, professionalism, and systems-based practice (Table 1).17 In 2013, these ACGME/ABMS broad competencies were used by the Association of Professors of Human and Medical Genetics (APHMG) to specifically apply the AAMC-HHMI standards to medical genetics education as well as to update their recommended genetics and genomics competencies (Table 2).18 The resulting APHMG core curriculum embraces competency-based education by focusing on developing basic and applied empirical skills in genetics for the medical student as opposed to the memorization of a specific constellation of symptoms associated with particular genetic diseases. The APHMG curriculum also emphasizes making appropriate decisions on ordering particular molecular tests for patients, understanding how to use bioinformatics tools as part of diagnosis and treatment decisions, managing patient symptoms, and making appropriate referrals to specialists. Underpinning the APHMG curriculum is the need to apply ethics and professionalism to all dealings with patients.
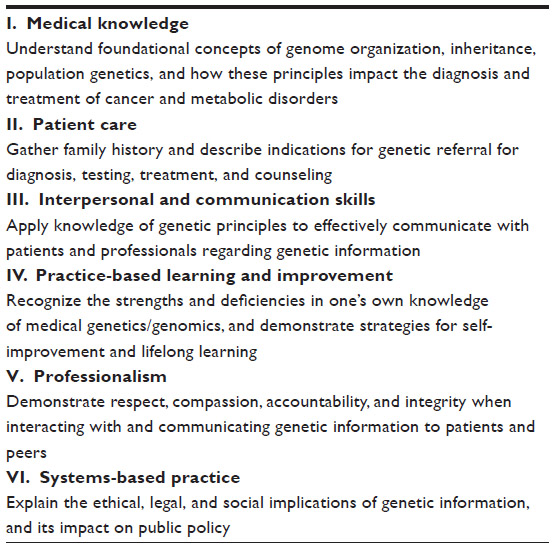 | Table 1 ACGME (Accreditation Council for Graduate Medical Education) competencies related to genetics |
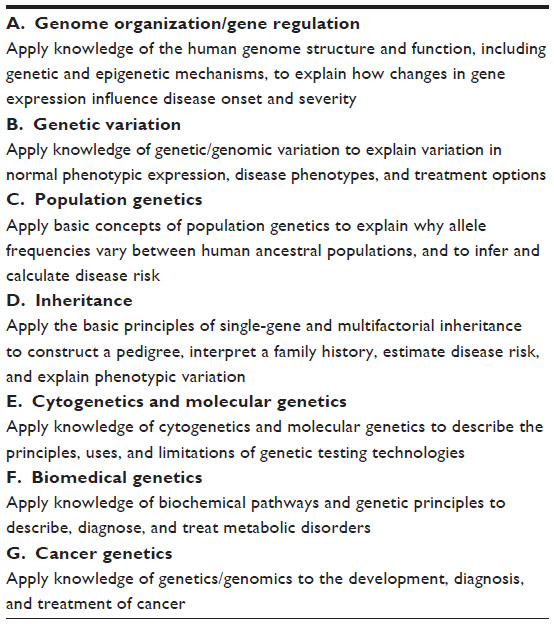 | Table 2 APHMG (Association of Professors of Human and Medical Genetics) Medical Knowledge Competencies |
Taken together, these professional society recommendations suggest a training regimen for future medical professionals emphasizing the development of scientific reasoning skills and the ability to competently utilize the informatics tools of the genomics revolution. These recommendations emphasize the ability of health care professionals to critically think and work through medical problems like a scientist as essential to sustain a competent medical workforce. Thus, a modern and thorough education in genetics for the future medical professional must from its root emphasize scientific reasoning and problem solving as its cornerstone.
Engagement in authentic research to develop practice-based learning skills in preclinical students
The training of a medical professional workforce well-versed in the staggering scientific advances in genetics and genomics of recent years requires physicians to be reflective and to retain a research mindset in order to fully understand how their medical care decisions are impacting the health of their patients. At the preprofessional level, reports like the American Association for the Advancement of Science’s “Vision and Change”19 have driven pedagogical movements in which students engage in actual scientific practice through long-term research opportunities in the classroom.20 The recommendations of “Vision and Change” call for an extension of the essence of evidence-based medical training into undergraduate education. In support of this idea as it applies to medical education, the authors of the previously mentioned AAMC-HHMI report felt that increasing the accessibility of undergraduates to “real science” represented an outstanding way to produce a generation of medical professionals best prepared to utilize the emerging tools of genomic medicine.18
In this spirit, several initiatives have developed in recent years that take a crowdsourcing approach to engage preprofessional students in the authentic research work that will best prepare them for future medical careers.21 For instance, HHMI has supported the development of the Science Education Alliance-Phage Hunters Advancing Genomics and Evolutionary Science (SEA-PHAGES) program in which undergraduates isolate bacteriophages from the environment and perform molecular and bioinformatics characterizations of their discoveries over a two-semester introductory biology course (http://seaphages.org).22 Other institutions have worked with their academic libraries to develop course-based experiences for their preclinical students that engage them with the online databases that are becoming essential to access the full range of available medical knowledge. In these experiences, students work on semester-long research projects based on the synthesis of information from these databases and preparation of a public presentation that summarizes their research. These practices have been shown to both increase students’ base knowledge of genetics principles and promote confidence in doing public presentations on database-based research.23,24 In a similar vein, the Genomics Education Partnership utilizes the study of Drosophila genome evolution to give undergraduates an experience in authentic bioinformatics-based research that can be adjusted to the time commitment and course level needs of instructors at all types of undergraduate institutions. This project provides a thorough exposure to the informatics concepts that underlie modern applications of genomics to making patient diagnoses as well as the chance for the student to develop empirical reasoning through engagement in authentic scientific questions.25 In all of these cases, students have emerged from these programs with more confidence in their abilities to think and act as scientists, an improved ability to utilize online tools to solve scientific problems, and a more solid understanding of the foundations of genetics and genomics.22–25 It is important to note that these examples do not directly engage undergraduates in clinical questions and are not meant to suggest that traditional didactic classroom experiences serve no purpose.26 Nevertheless, they succeed in providing course-based research opportunities that expose students to critical thinking situations that have become increasingly important for adequate preparation for medical careers.
The preprofessional foundation established by a research-based active learning approach to instruction should not be abandoned once a student reaches professional school. Many medical students currently participate in research experiences, usually as electives, and many of these projects are focused on research questions related to molecular medicine.27 At other institutions, the focus is on combining the strengths of biomedical graduate programs and clinical programs to produce medical professionals that have received significant opportunities to engage in research during their training.28 Furthermore, the drive toward precision medicine, where prevention and treatment decisions require integrating individual variations in genetic, phenotypic, and psychosocial characteristics, is currently on the horizon and will require clinical research to inform best practices and clinicians that can competently engage in information management.29
Applying a molecular, evidence-based approach to integrate genetics across medical curricula
A foundational training in genetics at the preclinical level reflective of current research progress in molecular biology emphasizes the molecular foundations of inheritance and takes an interdisciplinary systems biology approach to illustrate the diverse set of parameters that dictate an individual’s expression of phenotype. Many argue that it is at this level where genetics education needs to begin as opposed to the classic approach of simple dominant and recessive Mendelian traits and Punnett squares.2 A genetics-based education based primarily on Mendelian principles does the modern medical student a disservice as it does not acknowledge the complexities of human genetics and inheritance that current research has revealed. As the scientific community continues to expand its knowledge of genomics, protein expression, and ultimately human health, it is critical to use contemporary models based on the latest scientific advances to provide this fundamental knowledge to students in the medical professions. A genetics education based on molecular understandings of genotype and phenotype thus best equips the modern medical professional to accommodate new molecular biology-based diagnostic and treatments into their practices.
Problem-based learning cases, a foundation of the curriculum in many medical schools, are a perfect venue for the integration of modern genetics principles across the foundational disciplines of medicine. In this spirit, a case-study approach is a solid way to provide students at all levels of their medical education with perspective on how the complexities of human genetics reveal themselves in real-life situations. Given the need for enhanced training in bioinformatics and online medical genetics resources among future medical professionals, it is encouraging to note that case-based modules in bioinformatics are being introduced in both preclinical and clinical training programs.30 For instance, cancer biology case studies provide an excellent venue for teaching students about critical concepts like the acquisition of somatic mutations during the cell cycle and how these mutations contribute to cancer progression.8,31 Organizations like the National Center for Case Study Teaching in Science (http://sciencecases.lib.buffalo.edu/cs/) and MedEdPortal (https://www.mededportal.org/) have established themselves as clearinghouses for case studies that can be used to provide an engaging and evidence-based way to teach genetics to future medical professionals. Also, instructors can pair with medical professionals or adopt patient cases from the medical literature to develop new cases most appropriate to a specific classroom. The case study approach can give students practice in creating pedigrees and estimating patient risk as well as the opportunity to discuss the scientific and ethical complexities of genetic counseling and screening.32,33 The success of a problem-based curriculum depends on having a significant number of well-trained facilitators and some schools have found it necessary to use computer-based tutorials or introductory sessions prior to the problem-based learning sessions.34 Regardless, the use of case studies has been shown to improve both fundamental understanding of genetics principles and student confidence in using genetics and genomics tools in future medical practice.32,33
Techniques to implement a hands-on evidence-based genetics curriculum
Evidence-based case study techniques can be applied in a laboratory setting in medical curricula to make the genomic screening of patients and the advent of precision medicine more accessible and realistic to medical students. Case-based virtual laboratories, for instance, have been used with success among 1st-year medical students to illustrate the full range of common and rare issues that can arise with respect to applying genetics in a clinical setting, including selection of diagnostic tests and effectively communicating results to patients.35 Cancer biology once again provides a powerful venue in which to introduce the complexities of genomics with respect to ultimate expression of phenotype. The use of cancer-related case studies and virtual diagnostic laboratories allows medical students across the full gamut of professions to fully grapple with the strengths and limitations of genomic tests and how the final phenotype presented by a patient represents a complex interplay of mutation and environment.36,37
The simple use of concept maps and models in genetics classrooms at all levels is a powerful method to convey and reinforce the fundamentals of genetics and genomics needed for success in today’s medical fields. For instance, a basic understanding of gene expression as expressed by the “Central Dogma” of molecular biology is a critical concept for medical students to master so that they may understand how a genotype is converted into a phenotype and, by extension, how defects in this process can lead to identifiable patient symptoms. An excellent way for students to gain an improved understanding of these concepts is through creating representations of gene expression and “Central Dogma” scenarios either in class or as out-of-class projects. These representations can help students to illustrate the relationship between allelic genotypes and expressed phenotype and can then be applied to disease states (see Figure 1 for an example of such a class activity).
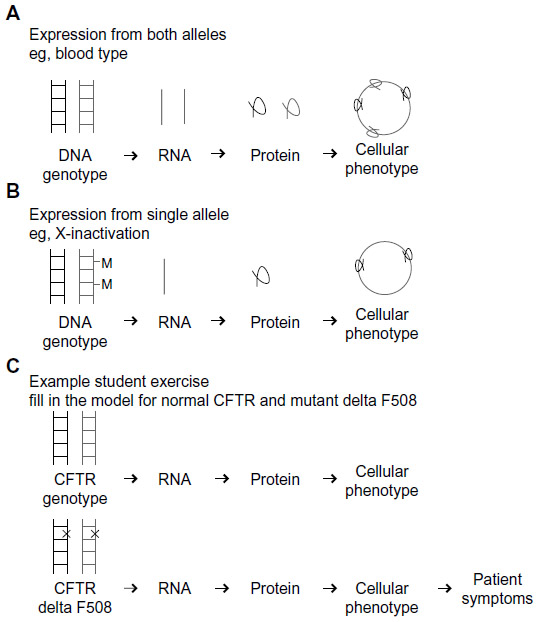 | Figure 1 Sample exercise for teaching basic principles in gene expression. |
With this framework in mind, curricula can be developed to provide students with practice in predicting the consequence of a given genetic mutation on protein expression.30 Students often perceive mutations in genes as rare events triggered by external mutagens, but given the high number of cell divisions stem cells undergo it is a virtual certainty that a baseline level of genetic variation will be generated during normal replication processes and that the number of divisions correlates with cancer risk.38 Mutations that have a significant effect on phenotype are those that dramatically alter the level of the protein product or the ability of the protein to function.31 As a means of conveying these ideas to students, cystic fibrosis provides a classic example of how one of thousands of potential single base pair changes at the DNA level can result in a defect in the cystic fibrosis transmembrane conductance regulator (CFTR) protein product. Knowing which type of mutation a patient has can be determined using online genetics resources (http://omim.org/entry/602421) and is important to establish before prescribing an appropriate treatment. If a patient has a nonsense mutation resulting in a truncated CFTR protein, then it may be possible to treat the disease with a drug called PTC124/Translarna that makes the ribosome less sensitive to stop codons.39 However, other mutations in distinct locations across the CFTR protein can lead to problems in the lung, sweat glands, and pancreas that would not be treatable by PTC124/Translarna.40 Thus, the use of a contextual example such as CFTR can reveal to medical students the great variety of phenotypes that can emerge from different changes affecting a single gene, how one gene can affect different human systems in profoundly different ways, the importance of understanding how to identify particular mutations present in a given gene and where to find more information about what is known about a given mutation, and how particular treatment options will be effective only against diseases deriving from specific mutations in a given gene.
The rapid scientific and technological advances that are constantly occurring in genetics and genomics means that the list of what constitutes a solid foundational understanding of genetics for medical professionals will always be a moving target. The interdisciplinary nature of modern science also makes the field of genetics difficult to define with respect to molecular biology, microbiology, and other related disciplines. The use of medical contexts in the teaching of modern genetics and genomics concepts, however, provides a framework for students to link basic scientific research to clinical advances and to appreciate the power of the genomics revolution.41 The concepts represented in modern genetics and genomics often blur the traditional lines between life science subdisciplines and provide the opportunity for horizontal integration of these concepts across the curriculum, particularly in a system-based curriculum. For instance, research has shown that the competencies of a modern genetics and genomics curriculum for medical professionals can be effectively taught in a primarily microbiology background.42 Many metabolic diseases have an important biochemical component, providing another disciplinary context in which to introduce genetics fundamentals. In this spirit, fundamental concepts in genetics and genomics may be added across an integrated medical curriculum as a demonstration of the interdisciplinary nature of modern scientific practices.
Fundamental concepts of genetics to emphasize in a medical curriculum
Though developing a consensus list of the key concepts in medical genetics may be impossible, there are certain key points that are indispensible and that can be effectively taught using evidence-based methodologies (Table 2 for the broad genetics competencies recommended by the APHMG). An example of this is the origin of the genotype, which is created during reproduction and relies on meiosis to reassort parental chromosomes. This is one of the areas in which students often enter professional school with significant misconceptions and a number of different strategies incorporating active modeling have been developed for teaching chromosome assortment during meiosis.43 It is critical that students develop a sense for how this process leads to the reassortment of alleles, how this processes is integrated into the cell cycle, and how nondisjunction can result in the development of trisomies such as Down Syndrome. Virtual laboratories are available that require students to consider abnormal karyotypes using the Denver classification, defined as the classification of human chromosomes based on size and centromere position.44 These laboratories can give medical students the opportunity to illustrate genetic phenomena for themselves as a key step toward their mastery of the material at hand.
Another key concept based on a more modern understanding of genetics and genomics is how phenotype is influenced by a combination of genetic, epigenetic, and environmental factors that can be hard to collectively predict and interpret. The sequencing of the human genome has created a map over which one can overlay approximately 21,000 genes based on evolutionary homology.45 This represents a figure significantly smaller than was originally predicted, and subsequent research has revealed that a substantial amount of our DNA is transcribed as noncoding RNA. Several research groups have invested their recent efforts in understanding the structure of the genome in terms of how epigenetic regulation through DNA chemical modifications like methylation occurs. These epigenetic regulations greatly complicate traditional Mendelian understandings of how genotype and phenotype are related and how DNA sequence may accurately predict susceptibility to a given disease. For instance, some epigenetic markers are transmitted through generations and accumulate over the course of a lifetime, which means that environmental conditions that occurred during a patient’s great grandfather’s lifetime may impact their own health.46 Epigenetic silencing also results in different chromosomes being shut off in different cell types, creating a mosaicism best illustrated by random X-inactivation in females. Collectively, these genomic complexities make the jobs of medical geneticists quite complex and call into the question the traditional usage of basic Mendelian terms such as “recessive” and “dominant” when making diagnoses.47 As in the CFTR example described before, an evidence-based approach in which case studies illustrate how these genomic and epigenetic phenomena occur in patients provides a good opportunity for students to carefully consider how to best gather information, diagnose, and treat individual patients by combining a patient’s symptoms and expression profile.
As genomics becomes more integrated into mainstream medicine and genomic sequencing becomes more universally accessible, the notion of pharmacogenomics, or the development of drug regimens specifically tailored to individual patients, has increasingly become a reality. While medical science has long appreciated the wide range of side effects from pharmacological treatments that can be exhibited between different patients, genomics has provided the means to better predict these side effects through screening patients for specific markers in the genome. Such information has already been essential in providing safe and effective range of drug treatments for a variety of cancers and cardiovascular diseases.48,49 The importance of ethnicity in prescribing safe and effective drug treatments has also been revealed by the genomics revolution, as specific ethnic groups carry genetic mutations that make them either more or less susceptible to the positive effects of a given treatment as well as potential deleterious side effects.48 Thus, an appreciation of genomics fundamentals will prepare future medical professionals for gene-based drug dosing, a direct and exciting application of the genomics revolution.
Enabling medical students to apply modern genetics and genomics knowledge to successful medical practice
A commonly cited problem among new medical students is a lack of confidence in their abilities to work with genomic databases and other tools of molecular genetics that are increasingly prevalent in medical practice.4,50,51 As seen in Table 3, a diverse array of genetics and genomics databases are available to medical professionals for educational and diagnostic purposes. Thus, medical schools are increasingly adopting curricula that make an effort to vertically incorporate medical genetics and genomics at all levels. This is an exciting development that suggests that medical programs are taking the results of pedagogical research seriously and are adopting best practices in teaching into their curricula. In some cases, this has led to the development of entire genetics academic tracks in medical schools designed both to instill a foundational understanding of modern genetics practices in students and to provide them with access to advanced genetics training through elective coursework and clinical experience.50 In other situations, the use of online genetics resources like OMIM have been integrated into the medical school curriculum at all levels to promote increased confidence among medical trainees in using databases as part of a diagnosis.51 Overall, efforts such as these to more thoroughly integrate molecular genetics and genomics into the medical school curriculum may create the increased interest and improved confidence levels among students necessary to fully incorporate these disciplines into modern medical practice while eliminating current deficits in the number of genetics specialists available to the medical community.8
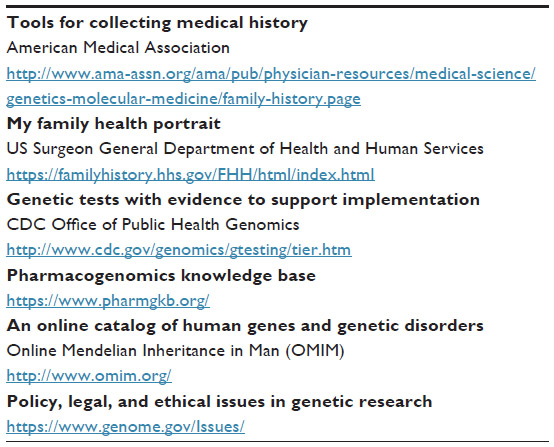 | Table 3 Examples of online resources for teaching genetics |
Communicating genetics information to patients
A foundational knowledge of the tools of genetics and genomics is not useful to the future medical professional if he or she cannot communicate this information to other health providers and patients in an effective and compassionate manner. Several online resources are available to facilitate medical professionals in the dissemination of medical genetic information in language accessible to a general audience. These include GeneReviews (http://www.ncbi.nlm.nih.gov/books/NBK1116/), a service of the United States National Center for Biotechnology Information (NCBI) that provides a clinical perspective on the molecular basis of genetic disorders accompanied by a glossary for patients. The NCBI also provides the Genetic Testing Registry (GTR) (http://www.ncbi.nlm.nih.gov/gtr/), a resource that explains both the procedures behind and locations where one may seek particular genetic tests. Finally, the Genetics Home Reference (http://ghr.nlm.nih.gov) is a service of the United States National Library of Medicine that explains genetic disorders and therapies in general terms while also providing help in locating genetic counselors in particular locations. Knowledge of resources such as these is invaluable in providing medical professionals with a means of helping patients to better understand the difficult medical choices that they may face with respect to their diagnoses and treatments.
In response to pedagogical research, many undergraduate and preclinical classes have increased the amount of time spent working in groups compared with their predecessors to better develop both patient communication and teamwork skills. In many cases, this has led to the use of a more active-learning-based approach in individual classes that can then spread throughout entire departments as more instructors see the benefits of this style of teaching.52 Specifically, the simple incorporation of more group-based work and presentation opportunities alongside case study scenarios has been shown to increase retention of key concepts in genetics, among other subjects, for new medical students.53 In addition, role playing in class and encounters with standardized patient simulations increases student preparedness for facing the critical types of encounters with patients and other personnel that are to be expected in the clinic.54–56
Addressing the ethical, legal, and social implications of genetic information
This paper has argued for a more comprehensive focus on genomics, molecular genetics, and their medical applications as a vital part of a complete and modern medical education. However, this education must also consider the many social and ethical issues introduced by new technologies, including patient privacy, the cost-effective use of health care resources, and patient autonomy in the use of genomic screening.57–59 Teaching these ethical considerations will promote the development of a medical workforce equipped not only with the scientific ability to effectively utilize modern genetics and genomics techniques, but also with the understanding of how to work with these techniques in a manner that best supports the welfare and interests of the patient and society. For instance, the recently emerged CRISPR-Cas9 gene editing system can potentially be used to correct mutations discovered in reproductive cells but also raises many of the same ethical issues originally brought up by gene therapy with respect to when the use of such a system is safe and appropriate.60 Therefore, a study of medical genetics and genomics must embrace not only a scientific understanding of emerging genomics and bioinformatics techniques but also a thorough consideration of the implications such technologies can have on patient welfare.
To engage students in ethical issues, several medical training programs have incorporated the use of personalized genomic testing services into their curricula as relatable examples.61,62 This approach has allowed students to better understand the skepticism and fear that their future patients may have with the donation of DNA for genetic testing as well as the implications of the results.62 Such an approach has been shown to promote a better understanding among students of the complex interactions between genetics and the environment with respect to presentation of phenotype.63 Techniques such as the use of medical students’ own DNA for genomic diagnostic purposes have also allowed students to more personally consider the many ethical issues surrounding the use of new genetics and genomics technologies.61,62 In addition, classroom discussions should also include discussions about the role of the US Food and Drug Administration in the regulation of these technologies.64
The genomics revolution has greatly increased the amount of patient information that can be collected and potentially used for medical and research purposes. As such, students must understand the legal requirements that accompany the accumulation and dissemination of genetic information to their patients. In the USA, the Health Insurance Portability and Accountability Act (HIPAA) requires physicians and researchers to protect the privacy of health information for 50 years after an individual’s death. However, future medical professionals must be trained to consider balancing this requirement against the implications that genetic information may have for patients and their family members.
The storage and usage of genetic information may also be perceived quite differently by different cultural or socioeconomic communities. Medical students must understand that different communities may have different viewpoints on genetic information that may potentially impact participation of a given community in patient care as well as research initiatives.65 A “one size fits all” approach to medical care can in many cases exclude groups that may have historical or social traditions of mistrust toward the medical community. As an example of developing an approach to medicine and public health designed for a specific community, the Mayo Clinic created the Native Cancer Information Resource Center and Learning Exchange (Native CIRCLE) to generate culturally appropriate initiatives on the treatment of cancer as well as other diseases in American Indian and Alaska Native populations.66 Efforts such as this underscore the importance of considerations of the full social and ethical ramifications of modern genetics techniques as an essential part of training for a career in the medical community.
Clinical training for specialized careers in genetics
As previously suggested, the medical community requires both a good working understanding of genetics among all clinicians and an increased number of trained medical genetics specialists. Medical geneticists are specially trained MDs, most of whom have completed a prior residency, or PhDs who are certified by societies like the American Board of Medical Genetics and Genomics (AMBGG). They are trained through programs required to document student exposure to clinical case presentations, medical rounds, and direct clinical contact. These training programs ensure that future medical geneticists have observed physicians and patients in actual clinical encounters so that they are better able to understand the application of genetics and genomics in clinical settings and practices. They are also trained by interacting longitudinally with patients in order to develop an understanding of the impact genetics may have on the patient’s life as well as on the difficulties they may experience when communicating genetics and genomics test results to patients.67 There is also greater realization of the importance of reconsidering foundational science concepts during the clinical years. As with the initial presentation of these concepts, this review can effectively be achieved through case studies with small group discussion.68
Medical genetics is a specialty approved by the ABMS; however, it is one of the 24 specialties with the least yearly certified members, ranging from 129 to 189 between the years 1999 and 2013. This compares with 7.380 certified internal medicine and 3.370 certifications issued by the ABMS in 2013 for internal medicine and family medicine, respectively.69 In the future, perhaps the enriched foundational emphasis in the modern concepts of genetics and genomics across medical curricula advocated for in this paper would lead to an increased interest level in this specialty among medical students. Increasing the number of medical students interested in pursuing clinical medical specialties in genetics will provide more trained professionals for a field that will only increase in demand as medical diagnostics and treatments become more precise and based on personalized molecular biology and bioinformatics.
Conclusion
Examining the current state of genetics education among future medical professionals serves as a reminder that no scientific discipline stands independent of others. Genetics is not meant to be taught either as a separate entity from other scientific disciplines that compose a comprehensive medical education or as a set of facts to be memorized. From the very beginning of one’s medical education, genetics should be presented as a key component of the continuum of disciplines that need to be introduced and developed in medical education through the use of authentic scientific experiences tied to relevant clinical examples. In this way, the next generation of medical professionals will have developed scientific critical thinking skills that allow them to apply foundational genetic knowledge and ethical principles to patient encounters. They will be able to adapt to the rapidly changing practices that are accompanying the genomics revolution, understand the resources of molecular biology and bioinformatics that can serve them in their practice, and treat their patients with confidence, ethical soundness, and compassion.
Disclosure
The authors report no conflicts of interest in this work.
References
Bakhtiar SM, Ali A, Baig SM, Barh D, Miyoshi A, Azevedo V. Identifying human disease genes: advances in molecular genetics and computational approaches. Genet Mol Res. 2014;13(3):5073–5087. | |
Redfield RJ. “Why do we have to learn this stuff?” – a new genetics for 21st century students. PLoS Biol. 2012;10(7):e1001356. | |
Larson EA, Wilke RA. Integration of genomics in primary care. Am J Med. 2015;pii:S0002-9343(15)00452-0. | |
Feero WG, Green ED. Genomics education for health-care professionals in the 21st century. JAMA. 2011;306(9):989–990. | |
Daack-Hirsch S, Jackson B, Belchez CA, et al. Integrating genetics and genomics into nursing curricula: you can do it too! Nurs Clin North Am. 2013;48(4):661–669. | |
Blair DR, Lyttle CS, Mortenson JM, et al. A nondegenerate code of deleterious variants in Mendelian loci contributes to complex disease risk. Cell. 2013;155(1):70–80. | |
Schrodi SJ, Mukherjee S, Shan Y, et al. Genetic-based prediction of disease traits: prediction is very difficult, especially about the future. Front Genet. 2014;5(162):1–18. | |
Cichon M, Feldman GL. Opportunities to improve recruitment into medical genetics residency programs: survey results of program directors and medical genetics residents. Genet Med. 2013;16(5):413–418. | |
Mainous III AG, Johnson SP, Chirina S, Baker R. Academic family physicians’ perception of genetic testing and integration into practice. Fam Med. 2013;45(4):257–262. | |
Pearl PL, Pettiford JM, Combs SE, et al. Assessment of genetics knowledge and skills in medical students: insight for a clinical neurogenetics curriculum. Biochem Mol Biol Educ. 2011;39(3):191–195. | |
Plunkett-Rondeau J, Hyland K, Dasgupta S. Training future physicians in the era of genomic medicine: trends in undergraduate medical genetics education. Genet Med. Epub 2015 Feb 12. doi:10.1038/gim.2014.208. | |
Nelson EA, McGuire AL. The need for medical education reform: genomics and the changing nature of health information. Genome Med. 2010;2:18. | |
Hatala R, Guyatt G. Evaluating the teaching of evidence-based medicine. JAMA. 2002;288(9):1110–1112. | |
Albanese MA, Mejicano G, Mullan P, Kokotailo P, Gruppen L. Defining characteristics of educational competencies. Med Educ. 2008;42(3):248–255. | |
Frank JR, Snell LS, Cate OT, et al. Competency-based medical education: theory to practice. Med Teach. 2010;32(8):638–645. | |
Association of American Medical Colleges-Howard Hughes Medical Institute Committee. Scientific Foundations for Future Physicians. Washington, DC: AAMC-HHMI; 2009. | |
Batalden P, Leach D, Swing S, Dreyfus H, Dreyfus S. General competencies and accreditation in graduate medical education. Health Aff. 2002;21:103–111. | |
Hyland K, Dasgupta S, Garber K, et al. Medical School Core Curriculum in Genetics. Association of Professors of Human and Medical Genetics. April 2013 [cited June 8, 2015]. Available from: http://media.wix.com/ugd/3a7b87_7064376a9eb346cfa1b85bc2f137c48f.pdf. Accessed June 8, 2015. | |
American Association for the Advancement of Science. Vision and Change: A Call to Action. Washington, DC: AAAS; 2010. | |
Ilic D, Tepper K, Misso M. Teaching evidence-based medicine literature searching skills to medical students during the clinical years: a randomized controlled trial. J Med Libr Assoc. 2012;100(3):190–196. | |
Freeman S, Eddy SL, McDonough M, et al. Active learning increases student performance in science, engineering, and mathematics. Proc Natl Acad Sci U S A. 2014;111(23):8410–8415. | |
Jordan TC, Burnett SH, Carson S, et al. A broadly implementable research course in phage discovery and genomics for first-year undergraduate students. mBio. 2014;5(1):e01051–e01113. | |
Tennant MR, Miyamoto MM. The role of medical libraries in undergraduate education: a case study in genetics. J Med Libr Assoc. 2002;90(2):181–193. | |
Tennant MR, Edwards M, Miyamoto MM. Redesigning a library-based genetics class research project through instructional theory and authentic experience. J Med Libr Assoc. 2012;100(2):90–97. | |
Shaffer CD, Alvarez CJ, Bednarski AE, et al. A course-based research experience: how benefits change with increased investment in instructional time. CBE Life Sci Educ. 2014;13(1):111–130. | |
Hora MT. Limitations in experimental design mean that the jury is still out on lecturing. Proc Natl Acad Sci U S A. 2014;111(30):E3024–E3024. | |
Pfarr CM, Bramblett D, Osborne D, et al. A laboratory for education in molecular medicine: a dedicated resource for medical student research. Med Sci Educ. 2013;23(1):108–118. | |
Smith CL, Jarrett M, Bierer SB. Integrating clinical medicine into biomedical graduate education to promote translational research: strategies from two new Ph.D. programs. Acad Med. 2013;88(1):137–143. | |
Jameson JL, Longo, DL. Precision medicine – personalized, problematic, and promising. N Eng J Med. 2015;372(23):2229–2234. | |
Waggoner DJ, Martin CL. Integration of internet-based genetic databases into the medical school pre-clinical and clinical curriculum. Genet Med. 2006;8(6):379–382. | |
Guttmacher AE, Porteous ME, McInerney JD. Educating health-care professionals about genetics and genomics Nat Rev Genet. 2007;8: 151–157. | |
Rogers JC, Taylor ATS. Teaching about genetic testing issues in the undergraduate classroom: a case study. J Genet Counsel. 2011;20: 231–240. | |
Dasgupta S. Differential acceptance of genomic medicine approaches between future and practicing physicians. Med Sci Educ. 2015;25(3):233–236. doi:10.1007/s40670-015-0146-2. | |
Moore CM, Barnett DR. A problem-based learning approach to teaching medical genetics. Am J Hum Genet. 1992;51(4):930. | |
Bean LJ, Fridovich-Keil J, Hegde M, Rudd MK, Garber KB. The virtual diagnostic laboratory: a new way of teaching undergraduate medical students about genetic testing. Genet Med. 2011;13(11):973–977. | |
Farrell CL, Pedigo NG, Messersmith AR. Application of genomic principles to pharmacotherapy of cancer. Am J Pharm Educ. 2014;78(3):55. | |
Polansky M, Ross AC, Coniglio D, Garino A, Hudmon KS. Cancer education in physician assistant programs. J Physician Assist Educ. 2014;25(1):4–11. | |
Tomasetti C, Vogelstein B. Variation in cancer risk among tissues can be explained by the number of stem cell divisions. Science. 2015; 347(6217):78–81. | |
Linde L, Kerem B. Introducing sense into nonsense in treatment in human genetic diseases. Trends Genet. 2008;24(11):552–563. | |
Cutting GR. Cystic fibrosis genetics: from molecular understanding to clinical application. Nat Rev Genet. 2015;16(1):45–56. | |
Sitaraman R. From bedside to blackboard: the benefits of teaching molecular biology within a medical context. Perspect Biol Med. 2012; 55(3):461–466. | |
Shuster M. Can genetics and genomics nursing competencies be successfully taught in a prenursing microbiology course? CBE-Life Sci Educ. 2011;10(2):216–221. | |
Prunuske AJ, Hunter C, Nemeth K. Application of the introductory molecular and cellular biology assessment to health professional students. Med Sci Educ. 2014;24(3):263–271. | |
Toddenroth D, Dugas M, Kennerknecht I. Sorting chromosomes as a software-based exercise. Med Educ. 2010;44(11):1127. | |
Lander E. Initial impact of the sequencing of the human genome. Nature. 2011;470:187–197. | |
Pembrey ME. Time to take epigenetic inheritance seriously. Eur J Hum Genet. 2002;10:669–671. | |
Dobyns WB, Filauro A, Tomson BN, et al. Inheritance of most X-linked traits is not dominant or recessive, just X-linked. Am J Med Genet. 2004; 129A:136–143. | |
Patel JN. Cancer pharmacogenomics: implications on ethnic diversity and drug response. Pharmacogenet Genomics. 2015;25(5):223–230. | |
Roden DM. Cardiovascular pharmacogenomics: current status and future directions. J Hum Genet. Epub 2015 Jul 16. doi:10.1038/jhg.2015.78. | |
Dhar SU, Alford RL, Nelson EA, Potocki L. Enhancing exposure to genetics and genomics through an innovative medical school curriculum. Genet Med. 2012;14(1):163–167. | |
Diehl AC, Reader L, Hamosh A, Bodurtha JN. Horizontal integration of OMIM across the medical school preclinical curriculum for early reinforcement of clinical genetics principles. Genet Med. 2014;17: 158–163. | |
Whiteside A, Brooks DC, Walker JD. Making the case for space: three years of empirical research on learning environments. Educause Q. 2010;33(3):11. | |
Wiznia D, Korom R, Marzuk P, Safdieh J, Grafstein B. PBL 2.0: enhancing problem-based learning through increased student participation. Med Educ Online. 2012;17:17375. | |
McGovern MM, Johnston M, Brown K, Zinberg R, Cohen D. Use of standardized patients in undergraduate medical genetics education. Teach Learn Med. 2006;18(3):203–207. | |
McIlvried DE, Prucka SK, Herbst M, Barger C, Robin NH. Role play to give students practice communication for genetic counseling. Genet Med. 2008;10(10):739–744. | |
Salas R, Steele K, Lin A, Loe C, Gauna L, Jafar-Nejad P. Playback theatre as a tool to enhance communication in medical education. Med Educ Online. 2013;18:22622. | |
Dignam MB, Burhansstipanov L, Bemis L. Successful implementation of genetic education for Native Americans workshops at national conferences. Genetics. 2005;169(2):517–521. | |
Mahoney J. Genetic profiling of medical students. Virtual Mentor. 2012; 14(8):616–621. | |
Nagle E, KaŽoka D. Ethical challenges in teaching genetics for medical students. J Microbiol Biol Educ. 2014;15(2):181–185. | |
Baltimore D, Berg P, Botchan M, et al. A prudent path forward for genomic engineering and germline gene modification. Science. 2015; 348(6230):36–38. | |
Salari K, Karczewski KJ, Hudgins L, Ormond KE. Evidence that personal genome testing enhances student learning in a course on genomics and personalized medicine. PLoS One. 2013;8(7):e68853. | |
Vernez SL, Salari K, Ormond KE, Lee SS. Personal genome testing in medical education: student experiences with genotyping in the classroom. Genome Med. 2013;5(3):24. | |
Seaton A. More genetics for medical students? Occup Med (Lond). 2010;60(8):667. | |
Evans BJ, Burke W, Jarvik GP. The FDA and genomic tests – Getting regulation right. N Engl J Med. 2015;372:2258–2264. | |
Burhansstipanov L, Bemis L, Kaur JS, Bemis G. Sample genetic policy language for research conducted with native communities. J Cancer Educ. 2005;20(1 Suppl):52–57. | |
Carlock D. Native American health: traditional healing and culturally competent health care internet resources. Med Ref Serv Q. 2006;25(3):67–76. | |
ABMGG.org [homepage on the Internet]. Bethesda, MD: American Board of Medical Genetics and Genomics. Number of Certified Specialists in Genetics; [updated June 16, 2015; cited June 18, 2015]. Available from: http://www.abmgg.org/pages/resources_certspecial.shtml. Accessed June 18, 2015. | |
AAFP.org [homepage on the Internet]. Leawood, KS: American Association of Family Physicians. Recommended Curriculum Guidelines for Family Medicine Residents; [updated June 2014; cited August 28, 2015]. Available from: http://www.aafp.org/dam/AAFP/documents/medical_education_residency/program_directors/Reprint258_Genetics/pdf. Accessed August 28, 2015. | |
ABMGG.org [homepage on the Internet]. Bethesda, MD: American Board of Medical Genetics and Genomics. Specialties of Genetics; [updated November 18, 2014;cited June 18, 2015]. Available from: http://www.abmgg.org/pages/training_specialties.shtml. Accessed June 18, 2015. |
 © 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2015 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.