")
Back to Journals » Infection and Drug Resistance » Volume 14
Importance of Surveillance of New Delhi Metallo-Beta-Lactamase Klebsiella pneumoniae: Molecular Characterization and Clonality of Strains Isolated in the Lazio Region, Italy
Authors Spaziante M, Venditti C, Butera O, Messina F , Di Caro A , Tonziello G, Lanini S, Cataldo MA , Puro V
Received 18 May 2021
Accepted for publication 25 June 2021
Published 8 September 2021 Volume 2021:14 Pages 3659—3665
DOI https://doi.org/10.2147/IDR.S318717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Martina Spaziante,1 Carolina Venditti,2 Ornella Butera,2 Francesco Messina,2 Antonino Di Caro,2 Gilda Tonziello,1 Simone Lanini,1 Maria Adriana Cataldo,1 Vincenzo Puro1
1Emerging Infection Unit and Regional Service for Surveillance and Control of Infectious Diseases (SeRESMI), National Institute for Infectious Diseases “Lazzaro Spallanzani” IRCCS, Rome, Italy; 2Laboratory of Microbiology, National Institute for Infectious Diseases “Lazzaro Spallanzani” IRCCS, Rome, Italy
Correspondence: Maria Adriana Cataldo Tel +39 0655170786
Email [email protected]
Introduction: New Delhi metallo-β-lactamase producing Klebsiella pneumoniae (NDM-Kpn) strains have been causing healthcare-associated infections worldwide. The aim of this study was to describe the molecular mechanisms of antimicrobial resistance and to analyze the clonality of NDM-Kpn isolates collected between January 2019 and June 2020 from patients admitted to hospitals from the Lazio region, Italy.
Methods: We performed a retrospective cohort study. Whole-genome sequencing (WGS) was performed on all NDM-Kpn strains; clonality and genetic relationships were further investigated.
Results: During the surveillance period, 17 NDM-Kpn isolates were obtained from 17 patients admitted to seven different hospitals. Eight different sequence types (STs) were detected: ST147 (n = 4), ST383 (n = 4), ST15 (n = 3), ST11 (n = 2), ST17 (n = 1), ST29 (n = 1), ST307 (n = 1) and the newly identified ST4853 (n = 1). Genetic relationships were further investigated by the WGS-based core genome MLST (cgMLST) scheme, and 5 cluster types (CTs) were identified. Whereas a substantial overall heterogeneity among isolates was detected (8 different STs were identified out of 17 isolates), the strains within each cluster showed a very high level of genome similarity.
Discussion: Our study highlights the key role of surveillance, which allowed taking a picture of a part of the NDM-Kpn strains circulating in Italy, adding further insight into their molecular features.
Keywords: carbapenem-resistant Klebsiella pneumoniae, New Delhi metallo-β-lactamase, surveillance, healthcare-associated infections
Introduction
During the last decade, carbapenem-resistant Enterobacterales (CRE) have become endemic in many countries, representing a major health concern.1 In Enterobacterales and particularly in Klebsiella pneumoniae, acquired Ambler class A (eg, KPC and GES enzymes), class B metallo-beta-lactamase (eg, VIM, IMP and NDM enzymes) and class D carbapenemases (eg, OXA-48-like enzymes) have been described.2 Since its first isolation from a K. pneumoniae clinical isolate in 2008,3 an alarming spread of ceftazidime-avibactam (CZA) resistant NDM-producing Klebsiella pneumoniae isolates has been reported,1 and these strains have been causing healthcare-associated infections worldwide, with an increase of cases across Europe in the last years.4
Recently, an outbreak of NDM-producing Enterobacterales occurred among patients without travel history hospitalized in the Tuscany region, Italy, with a total of 1645 cases of colonization or infection with NDM-CRE reported in the period from 1 November 2018 to 31 October 2019.5,6 Sporadic cases were also reported in four other Italian regions.6
Following the European Centre for Disease Prevention and Control (ECDC) Rapid Risk Assessment “Emergence of resistance to ceftazidime-avibactam in Enterobacteriaceae resistant to carbapenems”,7 the Italian Ministry of Health issued national recommendations for interventions, aimed at ensuring the identification and surveillance of CZA-resistant CRE. Since then, all these cases should be reported to regional surveillance services and isolates sent to reference laboratories. In addition, it is recommended to perform screening rectal swabs to all high-risk patients at hospitalization.
These recommendations are based on the principle that surveillance is the pillar to raise awareness of the emergence of CZA resistance and to limit its further spread. In the aforementioned ECDC risk assessment, a new European WGS-based surveillance module for extensively drug-resistant Enterobacterales was launched with the aim of enabling the identification of mechanisms or gene mutations associated to CZA resistance and helping to monitor its geographic distribution among EU/EEA countries.
Importantly, data coming from deep molecular analysis of CZA-resistant K. pneumoniae strains circulating in Italy are still scarce. In particular, few data on NDM-Kpn strains are available, also due to their sporadic spread.
As regional reference center, we performed a retrospective cohort study with the aim of describing the molecular mechanisms and analyzing the clonality of all NDM-Kpn isolates collected from patients admitted in the Lazio region hospitals that were referred to our laboratory between January 2019 and June 2020.
Materials and Methods
We retrospectively included in the study all inpatients harboring a NDM-Kpn strain; for each patient, the following data were collected: age, gender, nationality, reporting hospital and ward, date of hospital admission, date and site of NDM-Kpn isolation.
For each NDM-Kpn isolate, species identification and antimicrobial susceptibility were obtained by MALDI-TOF MS (bioMérieux, Marcy l’Étoile, France)8 and Phoenix system (Becton Dickinson Diagnostics, CA, USA). Minimum inhibitory concentrations (MICs) for carbapenems, aminoglycosides, trimethoprim/sulfamethoxazole, tigecycline and colistin were interpreted according to European Committee on Antimicrobial Susceptibility Testing (EUCAST) guidelines.9 Phenotypic test for the identification of carbapenemase type was carried out by immunochromatographic assay (NG-test Carba, NG Biotech) that discriminated KPC, IMP, VIM, NDM, and OXA-48-like enzymes.
Whole-genome sequencing (WGS) was performed using Ion Torrent GSS5 (Life Technologies, Carlsbad, California, USA) by constructing single-end libraries with average lengths of 200 bp according to manufacturer’s instructions. All raw reads generated were submitted to the Sequence Read Archive (SRA) under the BioProject accession number PRJNA686854.
Clonality was analysed by the traditional seven housekeeping genes multi-locus sequence type (MLST) extracted from the WGS data (http://bigsdb.pasteur.fr/klebsiella/klebsiella.html). For an in-depth phylogenetic analysis, genetic relationships were further investigated by the validated WGS-based core genome MLST (cgMLST). Sequence quality trimming was carried out as described by Bletz et al,10 de novo assembly was performed by use of the Velvet assembler software (v1.1.04), integrated in the Ridom SeqSphere+ software (version 2.1, Ridom GmbH, Münster, Germany).11 A total of 2358 target genes were used to characterize the gene-by-gene allelic profile of the K. pneumoniae strains, under the assumption that a well-defined cgMLST scheme should cover at least 95% of the genes present in all analysed isolates, compared to the reference strain (GenBank accession no. NZ_CP020067.1). The resulting set of target genes was then used for interpreting the clonal relationship displayed in a minimum spanning tree using the “pairwise ignore missing values” parameter during distance calculations. Genotypically related isolates (distance of ≤15 alleles) were identified within a Complex Type (CT) (https://www.cgmlst.org).
Antimicrobial resistance genes and plasmid replicons were extracted from the WGS data identified by in silico analysis using the ResFinder v3.0 web server (http://www.genomicepidemiology.org). The minimum percentage of sequence identity was set at 99%.
The data reported in this study come from the Regional Public Health Surveillance System and were recorded and analyzed in accordance with the recommendations on the surveillance of CZA-resistant CRE strains issued by the Italian Ministry of Health. All data were analyzed anonymously; the research was carried out according to the principles set out in the Declaration of Helsinki. Informed consent was not required since this was a minimal risk retrospective study.
Results
During the surveillance period, 17 NDM-Kpn isolates were obtained from 17 patients admitted to seven different hospitals (H-1 to H-7), all located in the metropolitan area of Rome. Hospitals where stains were isolated, site of isolation and molecular characterization of isolates are reported in the Table 1. As shown, isolates were collected from different specimens; six out of 17 K. pneumoniae isolates were collected from rectal swabs; the remaining strains were from clinical samples, in particular, three were identified from blood cultures (Table 1).
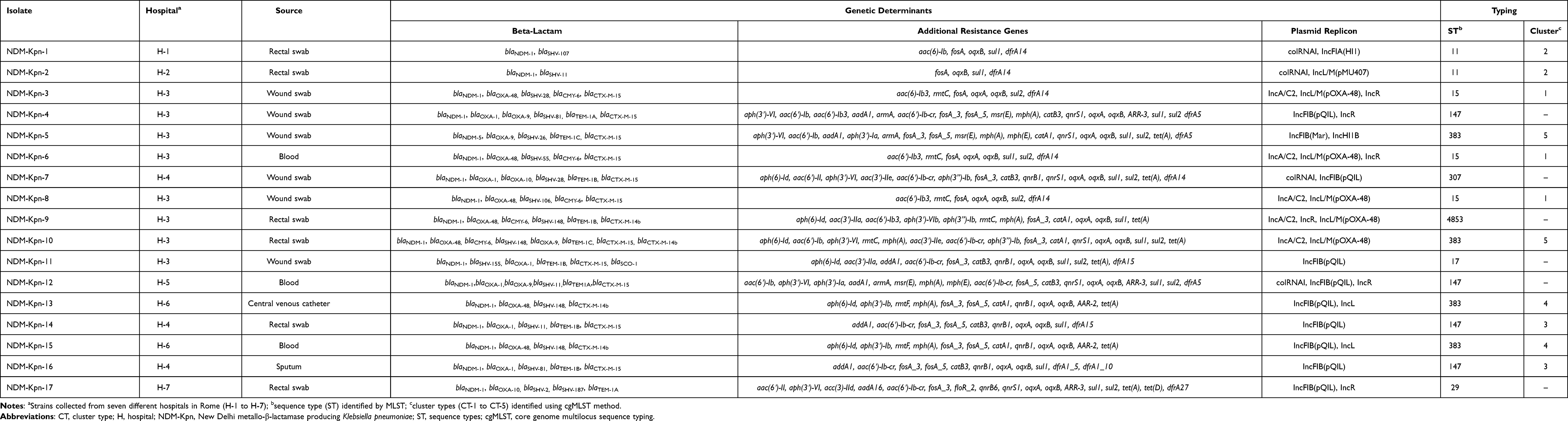 |
Table 1 Molecular Analysis of NDM-Kpn Clinical Isolates |
Eight cases were reported by the same ward of hospital H-3 during a 6-month period; in four cases, the time between hospitalization and isolation of the NDM-Kpn strain was ≤24 hours. All patients hospitalized at H-3 originated from Libya and reported a recent hospitalization in North Africa or Turkey.
Three cases were reported from hospital H-4. Two of them were hospitalized in the same ward and during the same period; the time between hospitalization and isolation of the NDM-Kpn strains was >72 hours.
At hospital H-6 two cases were identified two months apart from each other; the time between hospitalization and isolation of the NDM-Kpn strains was for these cases >72 hours; a patient from H-6 had previously been admitted to a health-care facility in Tuscany region.
Hospitals H-1, H-2, H-5 and H-7 reported only 1 case each during the study period.
As expected, all NDM producing K. pneumoniae isolates were resistant to carbapenems. Antimicrobial susceptibility is shown in Table S1.
Immunochromatographic assay allowed the detection of NDM carbapenemase in all isolates; molecular analysis showed the presence of blaNDM-1 gene variant in 16/17 isolates and of blaNDM-5 gene variant in one isolate. Seven isolates additionally harbored OXA-48-like enzymes, 5/17 isolates the ampC cephalosporinase blaCMY-6 gene, 14/17 the ESBL blaCTX-M gene and in only one isolate the presence of blaSCO-1 gene was documented (Table 1).
Eight different Sequence Types (STs) were identified: ST147 (n=4), ST383 (n=4), ST15 (n=3), ST11 (n=2), ST17 (n=1), ST29 (n=1), ST307 (n=1) and the newly identified ST4853 (n=1).
Clonal relationships within the STs using cgMLST scheme showed the presence of 5 Cluster Types (CTs). As shown in the minimum spanning tree obtained by Ridom pipeline, CT-1 was composed by 3 isolates, while CT-2, CT-3, CT-4 and CT-5 by 2 isolates each. Six strains did not cluster into any group (Figure 1).
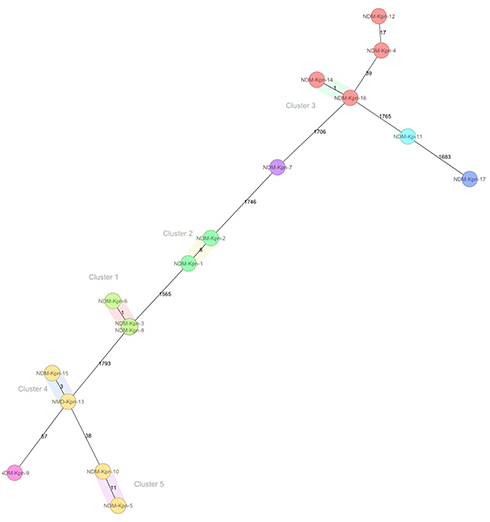 |
Figure 1 Minimum spanning tree based on cgMLST analysis of 17 NDM-producing K. pneumoniae isolates (NDM-Kpn-1 to NDM-Kpn-17), showing 5 cluster types numbered consecutively (1 and 5). Each circle represents an allelic profile, ie sequence type (ST), based on sequence analysis of up to 2358 target genes. Cluster types consist of closely related genotypes (≤ 15 allele differences). The numbers on the connecting lines illustrate the numbers of target genes with different alleles. |
The strains within each cluster showed a very high level of correlation (up to 11 allele differences). The isolates belonging to CT-1 and CT-5 originated from the same hospital (H-3); isolates belonging to CT-4 and CT-3 were also reported from the same hospital (H-6 and H-4, respectively), whereas isolates belonging to CT-2 were isolated from patients from two different hospitals (H-1 and H-2) (Figure 1).
Discussion
Our study describes the epidemiological and molecular features of NDM-Kpn strains circulating in the Lazio region, Italy. During an 18-month surveillance period, 17 patients harbouring NDM-Kpn strains were reported to our Center.
NDM-1 carbapenemase was predominant; in fact, only one strain harbored NDM-5. So far, 32 variants of NDM have been reported.12–15
According to the results of a systematic review on the worldwide spread and genotype distribution of human clinical isolates of NDM-Kpn based on published studies, the 4 most common variants of NDM carbapenemase in K. pneumoniae strains isolated from human samples are NDM-1, NDM-4, NDM-5 and NDM-7. In Europe, the common variants are blaNDM-1 and blaNDM-5.16 Thus, our findings are consistent with available data on the distribution of NDM variants.
Additional enzymes, like OXA-48 and CMY, have been also identified in the majority of cases. Interestingly, 7 out of 17 isolates co-harboured blaNDM-1 and blaOXA-48 genes. The first co-producing OXA-48 and NDM-1 K. pneumoniae was identified in 2015 in Turkey.17 Recently, outbreaks due to these strains have been reported in Iran and Turkey.18,19 According to the results of a nationwide surveillance including 156 K. pneumoniae carbapenem-resistant strains from invasive infections provided from 24 laboratories located in different areas of Italy, in one isolate, blaOXA-48 gene was detected together with blaNDM-1 gene.20
Of note, for one isolate, the presence of blaSCO-1 gene was documented, together with blaNDM-1, blaSHV-155, blaOXA-1 blaTEM-1B and blaCTX-M-15. Since its discovery in 2007,21 the blaSCO-1 gene has been identified in few K. pneumoniae isolates and in other Gram-negatives.22,23 It should be emphasized that the real prevalence of this enzyme might be underestimated because it is not part of any routine screening for resistance genes. The importance of the finding of the blaSCO-1 gene in our small surveillance resides on its representativeness of the risk of transmission of uncommon plasmid-borne resistance genes. This finding further highlights the pillar role of molecular monitoring.
A substantial heterogeneity among isolates was detected; 17 strains belonged to 8 different STs and 5 CTs. Diverse range of STs is reported in different countries with a total of 86 unique STs reported globally for NDM-Kpn.16 In fact, in our study, the heterogeneity was lower among strains isolated from patients coming from the same geographic area. Analysis by cgMLST revealed that NDM-Kpn isolated from 5 patients at H-3 were clonally related; in particular, strains from patients #3, #6 and #8 belonged to ST15 (CT-1), whereas isolates from patient #10 and #5 belonged to ST383, being part of CT-5. ST15 and ST383 are reported in North Africa and Middle East.24–27 The NDM-Kpn strain isolated from patient #4, who also originated from Lybia, harbored ST147, which has been reported in North Africa.28–30 In addition, a new ST (ST4853, an allelic variant of phoE gene, similar to ST383) was identified in our study, isolated from a Libyan patient hospitalized at H-3.
A higher heterogeneity was found among isolates from patients not reporting a recent hospitalization abroad; in fact, five different STs were documented (ST11, ST147, ST383, ST29 and ST307). In particular, in Italy ST307 has been recently identified as an emerging high-risk clone.31,32
Interestingly, in two hospitals (H-6 and H-4) all strains isolated belonged to the same C-T, CT-4 and CT-3, respectively.
The main limitation of our study pertains the possible underestimation of the NDM-Kpn prevalence; we could not assess the level of hospitals’ compliance in reporting patients harboring CZA-resistant Kpn as well as the total number of Kpn strains isolated in the investigated settings. Furthermore, we acknowledge the small sample size of our study; however, we believe that the surveillance data, even if they concern a few strains, are of paramount importance if representative of a specific geographic area.
Conclusion
Our findings are coherent with national data, reporting mainly sporadic cases of NDM-Kpn infections and colonizations.4 They represent a picture of part of the NDM-Kpn strains circulating in Italy, adding further insight into their molecular features. Our findings further emphasize the need for molecular surveillance that represents the basis of any strategy to struggle the spread of antimicrobial resistance.
Acknowledgments
We gratefully acknowledge the colleagues of the Infectious Diseases Prophylaxis Units and of the Public Health and Hygiene Services (SISP) of the Local Health Services (ASL) of Lazio, the microbiology laboratories of participant hospitals as well as all the staff involved in the structures that reported the cases, for the activity carried out to the surveillance and control of invasive CRE infections in the Lazio region.
Funding
This research was funded by Ministero della salute - Ricerca Corrente IRCCS- Linea 1. Progetto 3.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Logan LK, Weinstein RA. The epidemiology of carbapenem-resistant Enterobacteriaceae: the impact and evolution of a global menace. J Infect Dis. 2017;215(suppl_1):S28–S36. doi:10.1093/infdis/jiw282
2. Lee CR, Lee JH, Park KS, Kim YB, Jeong BC, Lee SH. Global dissemination of carbapenemase-producing Klebsiella pneumoniae: epidemiology, genetic context, treatment options and detection methods. Front Microbiol. 2016;7:895.
3. Yong D, Toleman MA, Giske CG, et al. Characterization of a new metallo-β-lactamase gene, blaNDM-1, and a novel erythromycin esterase gene carried on a unique genetic structure in Klebsiella pneumoniae sequence type 14 from India. Antimicrob Agents Chemother. 2009;53:5046–5054. doi:10.1128/AAC.00774-09
4. European Centre for Disease Prevention and Control. Carbapenem-resistant Enterobacteriaceae, second update – 26 September 2019. Stockholm: ECDC; 2019. Available from: https://www.ecdc.europa.eu/en/publications-data/carbapenem-resistant-enterobacteriaceae-second-update.
5. Tavoschi L, Forni S, Porretta A, et al. Prolonged outbreak of New Delhi metallo-beta-lactamase-producing carbapenem-resistant Enterobacterales (NDM-CRE), Tuscany, Italy, 2018 to 2019. Euro Surveill. 2020;25(6):2000085. doi:10.2807/1560-7917.ES.2020.25.6.2000085
6. European Centre for Disease Prevention and Control. Regional outbreak of New Delhi metallo-beta-lactamase producing carbapenem-resistant Enterobacteriaceae, Italy, 2018–2019 – 4 June 2019. Stockholm: ECDC; 2019. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/04-Jun-2019-RRA-Carbapenems%2C%20Enterobacteriaceae-Italy.pdf.
7. European Centre for Disease Prevention and Control. Emergence of resistance to ceftazidime-avibactam in carbapenem-resistant Enterobacteriaceae – 12 June 2018. Stockholm; ECDC; 2018. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/RRA-Emergence-of-resistance-to%20CAZ-AVI-in-CRE-Enterobacteriaceae.pdf.
8. Wimmer JL, Long SW, Cernoch P, et al. Strategy for rapid identification and antibiotic susceptibility testing of gram-negative bacteria directly recovered from positive blood cultures using the Bruker MALDI Biotyper and the BD Phoenix system. J Clin Microbiol. 2012;50(7):2452–2454. doi:10.1128/JCM.00409-12
9. The European Committee on Antimicrobial Susceptibility Testing. Breakpoint tables for interpretation of MICs and zone diameters. Version 9.0; 2019. Available from: http://www.eucast.org.
10. Bletz S, Mellmann A, Rothgänger J, Harmsen D. Ensuring backwards compatibility: traditional genotyping efforts in the era of whole genome sequencing. Clin Microbiol Infect. 2015;21(4):
11. Nurk S, Bankevich A, Antipov D, et al. Assembling genomes and mini-metagenomes from highly chimeric reads. In: Deng M, Jiang R, Sun F, Zhang X, editors. Research in Computational Molecular Biology. RECOMB 2013. Lecture Notes in Computer Science. Vol. 7821. Berlin, Heidelberg: Springer;2013: 158–160.
12. Hammoudi Halat D, Ayoub Moubareck C. The current burden of carbapenemases: review of significant properties and dissemination among Gram-Negative Bacteria. Antibiotics (Basel). 2020;9(4):186. doi:10.3390/antibiotics9040186
13. National Library of Medicine. Pathogen Detection. Available from: https://www.ncbi.nlm.nih.gov/pathogens/isolates#/refgene/NDM.
14. Chakraborty T, Sadek M, Yao Y, et al. Cross-border emergence of Escherichia coli producing the carbapenemase NDM-5 in Switzerland and Germany. J Clin Microbiol. 2021;59(3):e02238–20. doi:10.1128/JCM.02238-20
15. Khalid S, Ahmad N, Ali SM, Khan AU. Outbreak of efficiently transferred carbapenem-resistant blaNDM-producing GramNegative Bacilli Isolated from neonatal intensive care unit of an Indian hospital. Microb Drug Resist. 2020;26(3):284–289. doi:10.1089/mdr.2019.0092
16. Safavi M, Bostanshirin N, Hajikhani B, et al. Global genotype distribution of human clinical isolates of New Delhi metallo-β-lactamase-producing Klebsiella pneumoniae; A systematic review. J Glob Antimicrob Resist. 2020;23(4):420–429. doi:10.1016/j.jgar.2020.10.016
17. Kilic A, Baysallar M. The first Klebsiella pneumoniae isolate co-producing OXA-48 and NDM-1 in Turkey. Ann Lab Med. 2015;35:382–383. doi:10.3343/alm.2015.35.3.382
18. Guducuoglu H, Gursoy NC, Yakupogullari Y, et al. Hospital outbreak of a colistin-resistant, NDM-1- and OXA-48-producing Klebsiella pneumoniae: high mortality from Pandrug resistance. Microb Drug Resist. 2018;24:966–972. doi:10.1089/mdr.2017.0173
19. Duman Y, Ersoy Y, Gursoy NC, Altunisik Toplu S, Otlu B. A silent outbreak due to Klebsiella pneumoniae that co-produced NDM-1 and OXA-48 carbapenemases, and infection control measures. Iran J Basic Med Sci. 2020;23(1):46–50.
20. Di Pilato V, Errico G, Monaco M, et al. The changing epidemiology of carbapenemase-producing Klebsiella pneumoniae in Italy: toward polyclonal evolution with emergence of high-risk lineages. J Antimicrob Chemother. 2021;76(2):355–361. doi:10.1093/jac/dkaa431
21. Poirel L, Corvec S, Rapoport M, et al. Identification of the novel narrow-spectrum beta-lactamase SCO-1 in Acinetobacter spp. From Argentina. Antimicrob Agents Chemother. 2007;51:2179–2184. doi:10.1128/AAC.01600-06
22. Papagiannitsis CC, Tzouvelekis LS, Kotsakis SD, Tzelepi E, Miriagou V. Sequence of pR3521, an IncB plasmid from Escherichia coli encoding ACC-4, SCO-1, and TEM-1 beta-lactamases. Antimicrob Agents Chemother. 2011;55:376–381. doi:10.1128/AAC.00875-10
23. Venditti C, Butera O, Proia A, et al. Reduced susceptibility to carbapenems in a Klebsiella pneumoniae clinical isolate producing SCO-1 and CTX-M-15 β-lactamases together with OmpK35 and OmpK36 Porin deficiency. Antimicrob Agents Chemother. 2020;64(8):e00556–20. doi:10.1128/AAC.00556-20
24. Principe L, Mauri C, Conte V, et al. First report of NDM-1-producing Klebsiella pneumoniae imported from Africa to Italy: evidence of the need for continuous surveillance. J Glob Antimicrob Resist. 2017;8:23–27. doi:10.1016/j.jgar.2016.10.004
25. Jaidane N, Bonnin RA, Mansour W, et al. Genomic insights into colistin-resistant Klebsiella pneumoniae from a Tunisian Teaching Hospital. Antimicrob Agents Chemother. 2018;62(2):e01601–17. doi:10.1128/AAC.01601-17
26. Dziri O, Alonso CA, Dziri R, Gharsa H, Maraoub A, Torres C. Metallo-β-lactamases and class D carbapenemases in south-east Tunisia: implication of mobile genetic elements in their dissemination. Int J Antimicrob Agents. 2018;52(6):871–877. doi:10.1016/j.ijantimicag.2018.06.002
27. Nawfal Dagher T, Azar E, Al-Bayssari C, Chamieh AS, Rolain JM. First detection of colistin-resistant Klebsiella pneumoniae in association with NDM-5 carbapenemase isolated from clinical Lebanese patients. Microb Drug Resist. 2019;25(6):925–930. doi:10.1089/mdr.2018.0383
28. Messaoudi A, Haenni M, Mansour W, et al. ST147 NDM-1-producing Klebsiella pneumoniae spread in two Tunisian hospitals. J Antimicrob Chemother. 2017;72(1):315–316. doi:10.1093/jac/dkw401
29. Izdebski R, Bojarska K, Baraniak A, et al. NDM-1- or OXA-48-producing Enterobacteriaceae colonising Polish tourists following a terrorist attack in Tunis, March 2015. Euro Surveill. 2015;20(23):21150. doi:10.2807/1560-7917.ES2015.20.23.21150
30. Hamzaoui Z, Ocampo-Sosa A, Maamar E, et al. An outbreak of NDM-1-producing Klebsiella pneumoniae, associated with OmpK35 and OmpK36 Porin Loss in Tunisia. Microb Drug Resist. 2018;24(8):1137–1147. doi:10.1089/mdr.2017.0165
31. Loconsole D, Accogli M, De Robertis AL, et al. Emerging high-risk ST101 and ST307 carbapenem-resistant Klebsiella pneumoniae clones from bloodstream infections in Southern Italy. Ann Clin Microbiol Antimicrob. 2020;19(1):24. doi:10.1186/s12941-020-00366-y
32. Villa L, Feudi C, Fortini D, et al. Complete genome sequence of KPC-3- and CTX-M-15-producing Klebsiella pneumoniae sequence type 307. Genome Announc. 2016;4(2):e00213–16. doi:10.1128/genomeA.00213-16
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.