Back to Journals » International Journal of Women's Health » Volume 9
Implementing visual cervical cancer screening in Senegal: a cross-sectional study of risk factors and prevalence highlighting service utilization barriers
Authors Dykens JA, Linn AM, Irwin T, Peters KE, Pyra M, Traoré F, Touré Diarra M, Hasnain M, Wallner K, Linn P, Ndiaye Y
Received 21 June 2016
Accepted for publication 5 October 2016
Published 27 January 2017 Volume 2017:9 Pages 59—67
DOI https://doi.org/10.2147/IJWH.S115454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Elie Al-Chaer
J Andrew Dykens,1–4 Annē M Linn,5,6 Tracy Irwin,7 Karen E Peters,8 Maria Pyra,8 Fatoumata Traoré,9 Mariama Touré Diarra,9,☪ Memoona Hasnain,1,10 Katie Wallner,11 Patrick Linn,11 Youssoupha Ndiaye12
1Department of Family Medicine, College of Medicine, 2Center for Global Health, 3Institute for Health Research and Policy, 4Cancer Center, Hospital and Health Sciences System, University of Illinois at Chicago, IL, USA; 5Master’s International Graduate School Program, Peace Corps, Dakar, Senegal; 6Rutgers School of Nursing, Newark, NJ, 7Department of Obstetrics and Gynecology, 8School of Public Health, University of Illinois at Chicago, IL, USA; 9Regional Ministry of Health and Social Affairs, Kédougou, Senegal; 10Foundation for Advancement of International Medical Education and Research, Philadelphia, PA, USA; 11Peace Corps, Dakar, 12Regional Ministry of Health and Social Affairs, Sédhiou, Senegal
☪Mariama Touré Diarra passed away on March 21, 2015
Background: Senegal ranks 15th in the world in incidence of cervical cancer, the number one cause of cancer mortality among women in this country. The estimated participation rate for cervical cancer screening throughout Senegal is very low (6.9% of women 18–69 years old), especially in rural areas and among older age groups (only 1.9% of women above the age of 40 years). There are no reliable estimates of the prevalence of cervical dysplasia or risk factors for cervical dysplasia specific to rural Senegal. The goals of this study were to estimate the prevalence of cervical dysplasia in a rural region using visual inspection of the cervix with acetic acid (VIA) and to assess risk factors for cervical cancer control.
Patients and methods: We conducted a cross-sectional study in which we randomly selected 38 villages across the Kédougou region using a three-stage clustering process. Between October 2013 and March 2014, we collected VIA screening results for women aged 30–50 years and cervical cancer risk factors linked to the screening result.
Results: We screened 509 women; 5.6% of the estimated target population (9,041) in the region. The point prevalence of cervical dysplasia (positive VIA test) was 2.10% (95% confidence interval [CI]: 0.99–3.21). Moreover, 287 women completed the cervical cancer risk factor survey (56.4% response rate) and only 38% stated awareness of cervical cancer; 75.9% of the screened women were less than 40 years of age.
Conclusion: The overall prevalence of dysplasia in this sample was lower than anticipated. Despite both overall awareness and screening uptake being less than expected, our study highlights the need to address challenges in future prevalence estimates. Principally, we identified that the highest-risk women are the ones least likely to seek screening services, thus illustrating a need to fully understand demand-side barriers to accessing health services in this population. Targeted efforts to educate and motivate older women to seek screenings are needed to sustain an effective cervical cancer screening program.
Keywords: gynecologic cancer, cervical cancer screening, risk factors, implementation, global health, visual inspection of the cervix with acetic acid
Introduction
Globally, there are more than half a million new cases of cervical cancer yearly, with nearly 90% of these cases in less developed nations,1 where most women remain undiagnosed and have limited or no access to treatment.2 The cervical cancer incidence rate in the US in 2012 was 8.1 per 100,000 women, while less developed nations had a collective rate of 15.7 per 100,000.3 The cervical cancer incidence rate in Senegal (41.1)4 is more than five times greater than that in the US, and Senegal ranks 15th in the world in the age-standardized incidence rate of cervical cancer.3 When detected at an early stage, invasive cervical cancer is one of the most successfully treated cancers. The 5-year cervical cancer survival rate ranges from 60 to 70% in most countries.5 Limited access to cervical cancer screening and treatment services contributes to a disproportionate amount of morbidity and mortality due to cervical cancer for women living in low- and middle-income countries (LMICs).
However, development of various screening methods adaptable to country contexts has led to clear recommendations for improving cancer control.6–8
Cervical cancer burden in urban areas of Senegal has been studied previously,9–11 along with estimates of human papilloma virus (HPV) prevalence,12 but the prevalence of cervical cancer and dysplasia in rural regions is unclear. This gap in evidence is problematic in raising cervical cancer as a national priority issue.12 Precancer lesion rates detected through visual inspection have been shown to range from 5.7% to 28%, with an overall approximate rate of 10.1% in similar low-income countries.12,13 In Senegal, HPV positivity is higher in older-aged women (aged >45 years) (Table 1) compared to the same in other countries in Africa,5 and the HPV prevalence has been reported as being consistently high among female sex workers (39%–63%).2,3,14,15 In the US, the median age of diagnosis of cervical cancer is 49 years, and the median age of death from cervical cancer is 57 years.14 In Senegal, the incidence of cervical cancer peaks between the ages of 45 and 54 years15 (Table 1).
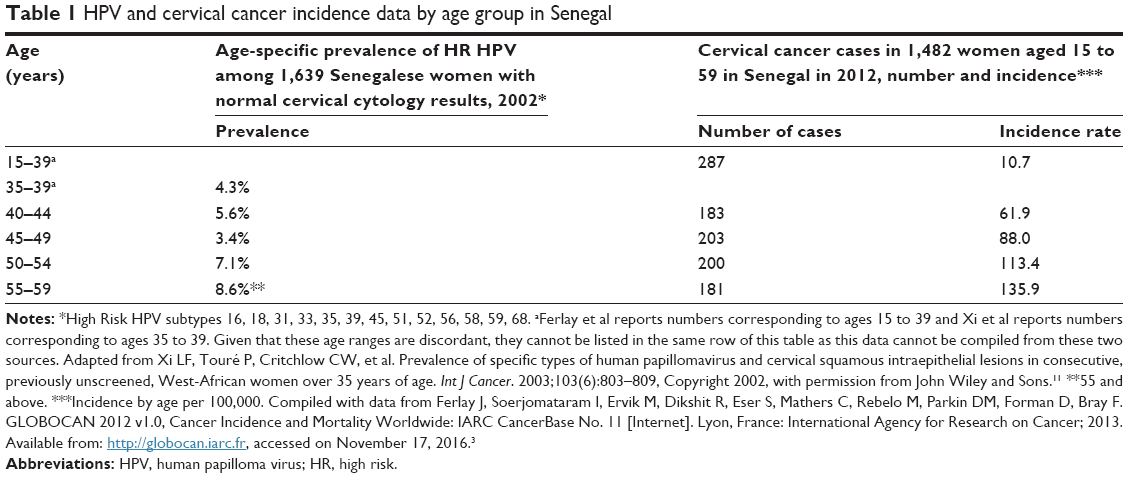 | Table 1 HPV and cervical cancer incidence data by age group in Senegal |
Considering the high incidence of cervical cancer in Senegal, as well as the importance of early diagnosis of cervical dysplasia, the implementation of evidence-based cervical cancer screening programs has been slow to reach the rural regions in Senegal. Screening programs have begun developing in only three of the 13 rural regions since 2010, providing limited services to only 325,000 of the 1,000,000 rural Senegalese women between the ages of 30 and 59 years.16 Despite the high value of cervical cancer screening and treatment, the estimated participation rate for cervical cancer screening in Senegal is very low (6.9% of all women aged 18–69 years). It is especially low in rural areas and in older age groups (1.9% of women aged 40–49 years and 0% of women aged ≥50 years).2 Furthermore, cervical cancer is an indicator of larger health system problems, including poor access to services and lack of culturally competent communication – all factors that disproportionately affect the poorest women.17 This is illustrated by the limited or lack of access to cervical cancer screening for the large majority of rural Senegalese women.
We conducted a study on the prevalence of cervical dysplasia in rural Senegal through a partnership between the Senegal Ministry of Health and Social Affairs (Kédougou Regional Office), Peace Corps Senegal, and the University of Illinois at Chicago.18 The long-term aims of this partnership are to improve access to quality cervical cancer prevention services (a local health system priority, as identified by a 2010 formal assessment). Between 2010 and 2013, the partnership worked to build capacity across Kédougou to ensure access to an estimated 9,041 women in the targeted age group (30–50 years), implemented regional-level cervical cancer clinical guidelines, introduced the EngenderHealth-developed Client-Oriented Provider-Efficient (COPE®) Handbook for quality improvement of the cervical cancer screening process,19–21 and trained 63 health workers in the evidence-based screening technique of visual inspection of the cervix with acetic acid (VIA). Despite multiple community-level information and education campaigns, women were not utilizing the service sufficiently to attain the midterm service goal of screening 70% of eligible women in 5 years. In 2014, we conducted a mass screening campaign to simultaneously reach eligible women, raise awareness in communities, and gather precancer prevalence and cervical cancer risk data to inform the improvement of the developing cervical cancer prevention service.22 Decentralized health systems in resource-limited settings in LMICs have made limited progress in sustaining accessible screening services and reducing disparities in cervical cancer rates over time. Therefore, it is imperative to understand in greater detail the contextual considerations for the implementation and sustainability of screening services. We undertook this study to add to the existing knowledge of the rural Senegal-specific context in order to strengthen the local cervical cancer screening capacity and raise national-level policy stakeholder awareness.
This study utilized VIA, a screening tool with demonstrated utility in low-resource settings, to identify precancerous cervical lesions in Senegal. VIA is performed by applying a vinegar solution to the cervix, followed by a “naked eye” visual inspection to identify (but not discriminate grades of) precancerous lesions, which can then be treated through cryotherapy at the same visit.23 The VIA screening test has a sensitivity of 80% (79%–82%) and a specificity of 92% (range: 91%–92%),24,25 and it has been proven to be safe and cost-effective.24–26 The aims of this study were to estimate the prevalence of cervical dysplasia using VIA and to determine the risk factors for cervical cancer in a rural region of Senegal.
Patients and methods
Research design
We designed a cross-sectional study to screen and survey women in 38 villages in the Kédougou region. Participant recruitment and data collection occurred between October 2013 and April 2014. Participants were screened using VIA and were asked to complete a risk factors questionnaire. The questionnaire contained items designed by a team of Senegalese and US researchers, with direct input from midwives working in the Kédougou region. It identified known cervical cancer risks23,27 and was adapted from findings and tools used in studies in other developing countries.28,29 The questionnaire was pretested on a sample of 15 women at both a rural clinic and a district-level health center in early 2013. The questionnaire was shortened and refined to facilitate the timely gathering of the most pertinent information in a population with a very low literacy rate. We then retested the questionnaire by giving it to Senegalese colleagues (midwives and physicians) to determine whether they interpreted the questions similarly. The fidelity of the data collection process was ensured through data collection standardization and supervision. The institutional review boards of the University of Illinois at Chicago, USA, and Cheikh Anta Diop University in Dakar, Senegal, approved this study. Verbal informed participant consent was obtained using institutional review board-approved guidelines prior to administration of the questionnaire.
Training
From 2011 to 2013, VIA trainers adapted a curriculum from the materials available with the World Health Organization (WHO) and the International Agency for Research on Cancer and conducted a single 6-day train-the-trainer program, certifying four midwives and one physician as Clinical Trainers in VIA. Through five separate trainings, the Clinical Trainers subsequently trained 58 additional health care providers (midwives and nurses), who then assisted in conducting the prevalence study. Training materials were developed in English and French. Prior to the campaign, we systematically trained community health workers at all study sites to provide information and education through individual and group sensitizations and radio broadcasts using WHO-endorsed materials.16
Target population and setting
The WHO recommends a one-time screening for women of ages 40–49 years in areas with limited resources. We expanded the age range to capture a greater number of higher-risk women, including those with initiation of sex at an earlier age and those who were HIV positive. Our target population, therefore, was all women aged 30–50 years in the three health districts (Kédougou, Salémata, and Saraya) of the Kédougou Region in Senegal. The Kédougou health district has eleven zones (each served by a health post staffed by a nurse or midwife) covering a total of 222 villages. Salémata has seven zones with 100 villages, and Saraya has eleven zones with 102 villages. Villages throughout the region are small, with populations ranging between 100 and several thousand. The regional capital of Kédougou contains the only semiurban community, having 16,689 residents living in six neighborhoods. The total population of the Kédougou region is 103,094, according to the 2010–2011 nationwide census data.16 As reported by this census, the distribution of men to women is 87:100 in rural areas, and within the rural areas of Senegal, 16.4% are between the ages of 30 and 50 years.16 Considering these estimates, we estimated the target population of women aged 30–50 years in the Kédougou Region to be 9,041. Representative sampling was performed through a three-stage cluster study with probability proportional to size. The first stage selected nine zones (out of a total of 29), and the second stage selected 38 villages, with three to five villages selected per zone. The third stage of sampling was performed through convenience sampling of women at the village level, with women self-selecting for the screenings. To achieve adequate power, our goal was to survey 75 women per zone, evenly distributed among the villages in each zone.
Inclusion and exclusion criteria
Inclusion criteria consisted of all women living in the Kédougou region between the ages of 30 and 50 years. Exclusion criteria consisted of age outside the target range, having received a hysterectomy (though we encountered none), and women menstruating at the time of the screening. We did not exclude a woman if she was pregnant because VIA is considered safe for pregnant women. Our study protocol specified that if a pregnant woman was tested positive for dysplasia or cancer of the cervix, treatment would be postponed until the postpartum period.
Protocol
A mass cervical cancer awareness and education campaign was conducted by teams in each of the three districts, during which research team personnel traveled to the identified villages. A lead midwife in each district oversaw each team, which was composed of midwives, nurses, community health workers, skilled birth attendants, and Peace Corps volunteers (PCVs). Screenings were performed by the VIA-certified midwives stationed in each of the three districts. Community health workers and skilled birth attendants were organized to educate community members on the purpose, process, and timing of the cervical cancer screenings.
Prior to participating in the screening and the questionnaire, participants were informed in French or a local language (Malinké or Pulaar) that the study surveys were voluntary, would be maintained anonymous, and would not affect their opportunity for obtaining access to cervical cancer prevention or other health services outside of this screening campaign. The majority of screenings took place in small health facilities, but in some villages, screenings were performed on a standard bed or a simple mat, or in villages where the screening took place at the school, they were conducted on a desk. In all cases, a private location, proper equipment (ie, gloves, speculum, forceps, cotton, and vinegar solution), and an adequate light source were used. Strict adherence to proper sanitation protocol was followed (handwashing, glove changes, and equipment sanitizing with bleach solution). We collected deidentified cervical cancer screening results from aggregated village-level data as well as deidentified demographic information from participants. The pretested structured questionnaire included 13 questions regarding demographic information and potential cervical cancer risk factors, including sexual debut, number of sexual partners, history of sexually transmitted infections (STIs), smoking status, and awareness of cervical cancer. Individual screening results were linked to questionnaire data, though this information remained deidentified. At the request of the regional health leadership, we did not include questions regarding a woman’s HIV status given the high sensitivity of this condition in the region.
Statistical analysis
To account for the sampling method, the prevalence rates and confidence intervals for the entire region and for each individual district were calculated using the svyset commands in Stata.30 The probability of selection at each stage was calculated, and we used the finite population correction, because the sampling was done without replacement. In two villages (Thiancombouro and Epingue Bassari), more women were screened than originally estimated to be within the target age group in the village (resulting in greater participation than the expected population at those sites). The estimated populations of these villages were manually reset to 100%. The risk factor data were not linked to the villages or districts. We compared VIA positives and negatives using Fisher’s exact test for categorical variables and two sample t-test for continuous variables, using SAS 9.3.31
Results
Prevalence
We collected data on 509 women screened using VIA in 38 villages. This represents 5.6% of the estimated target population within the region and a participation rate of 21.35% (of the estimated target population of 2,383 in the study villages). The prevalence of cervical dysplasia within the Kédougou Region was 2.10% (95% confidence interval: 0.99–3.21). The prevalence rates in each district were calculated and are listed in Table 2. The prevalence rates in Saraya, Kédougou, and Salémata districts were 4.27, 1.20, and 0.74%, respectively. There were ten VIA-positive lesions and one case of suspected cervical cancer.
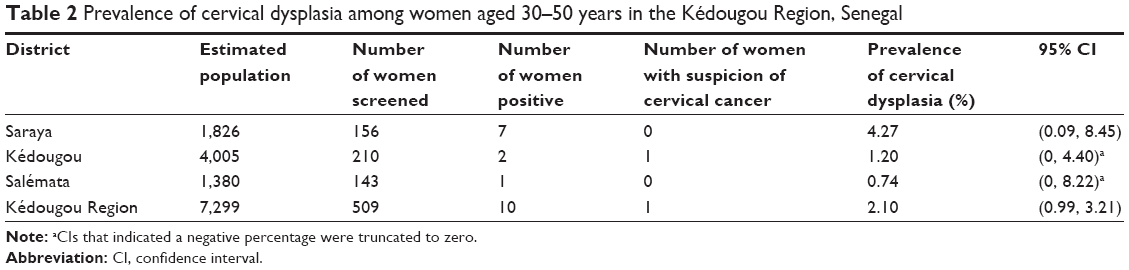 | Table 2 Prevalence of cervical dysplasia among women aged 30–50 years in the Kédougou Region, Senegal |
Risk factors
Data were available for 287 women who completed the cervical cancer risk factor survey (56.4% response rate). As shown in Table 3, the mean age was 35.7 (SD: 5.6) years for the total sample and 33.7 (SD: 2.9) years for women who were VIA positive. Most notably, 75.9% of women in this group were less than 40 years of age. Only 13.8% of women were aged 40–44 years and 10.3% were of age 45–50 years. Moreover, 99.6% of all women had never smoked and 38.2% of all women were aware of cervical cancer. The mean number of births among all women was 4.6 (SD: 2.4), yet 55.6% (five) of the nine women who tested positive for VIA had 0–3 births. The mean age of sexual debut among all women screened was 16.0 (SD: 3.3) years, with 18.2% of all women initiating sexual activity between the ages of 11 and 14 years. The mean age of sexual debut in women who screened positive was 18.8 (SD: 4.9) years. Of the total sample, 72.2% reported having only one lifetime sexual partner, 92.3% reported no more than two lifetime sexual partners, and 43% reported ever having had an STI.
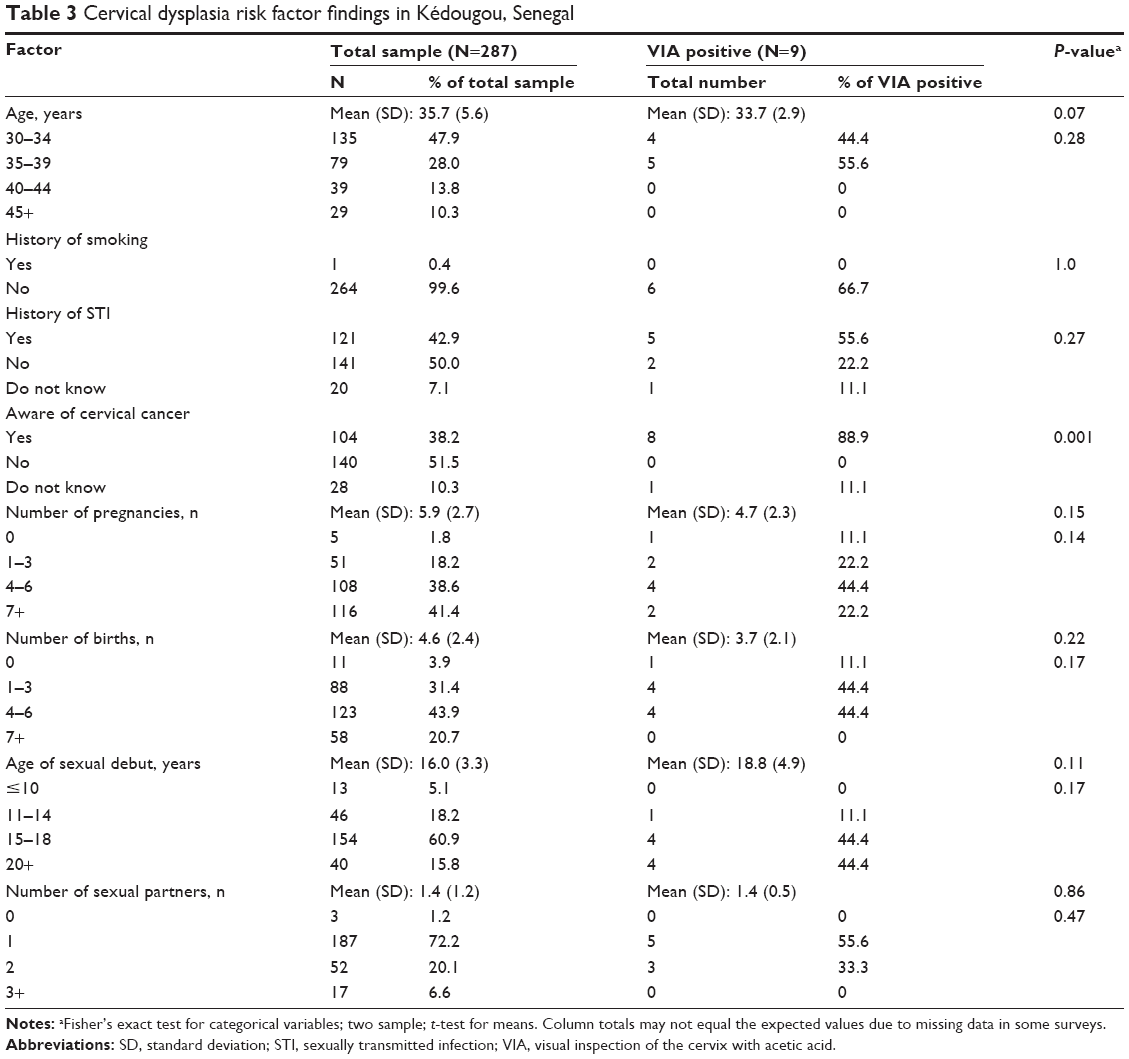 | Table 3 Cervical dysplasia risk factor findings in Kédougou, Senegal |
Discussion
The overall prevalence (2.1%) is lower than what we had anticipated. The participation rate of 21.35%, with low participation by women aged more than 40 years (21.4% of the total sample) may indicate that we had oversampled low-risk women. Of interest, it was noted that all the positive VIA cases were 30–39 years old. Yet, even though the greatest number of screenings were in the 30- to 35-year-old group, with fewer screenings in the 36- to 40-year-old group, our results showed greater numbers of positives as age increased, up to the age of 40 years (consistent with national trends, as shown in Table 1). It is likely that with greater numbers of screening in the 40- to 50-year age group, we would identify higher prevalence in this region. Table 1 illustrates that Senegal national data show increasing HPV rates through age 59 and the highest cervical cancer incidence between the ages of 45 and 54 years.3 These findings, therefore, most strikingly highlight the lack of health services utilization by older, higher-risk women. Further research is needed to fully understand the barriers to accessing health services in older women, which contribute to the apparent disconnect between this portion of the community and the health services. Targeting this age group is critical in the development of a cervical cancer control program.
We did find different prevalence rates (though not statistically significant) in the three districts. The highest prevalence (4.3%), found in Saraya District, is likely due to a developing gold mining industry that is largely isolated to that district. Such mining projects have been associated with increased STI rates due to the presence of migrant workers and increased sex work. Higher STI rates are an established risk factor of cervical dysplasia and cancer. Saraya District also has one of the highest HIV prevalence rates in Senegal,16 another risk factor for cervical cancer.1 Our findings highlight an area of need for cervical cancer prevention and STI reduction.
Given the low number of VIA positives in our study, it is expected that the risk factor data do not reveal any significant correlations. There were trends toward fewer pregnancies and births and later sexual debut among the positives, but additional data would be needed to confirm this. STI rates were high in this sample, with 43% of women reporting ever having had an STI. This highlights STI prevention, detection, and treatment as another potential service need for women in this rural part of Senegal. Furthermore, Table 4 illustrates that the median age of first sexual encounter is lower in Kédougou than nationally and the proportion of women reporting initiation of sex before age 15 is twice as high in Kédougou as that reported nationally.3 These data could illustrate higher risk of HPV exposure and, thus, risk for the development of cervical cancer, as compared to the nation as a whole. In our sample, only 38.2% of women were aware of cervical cancer, highlighting the lack of awareness as another major barrier.
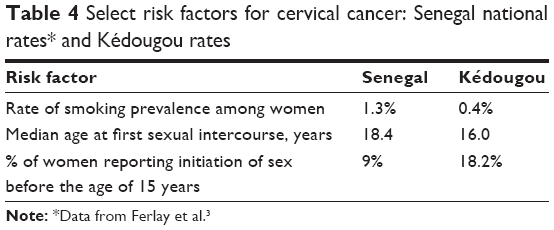 | Table 4 Select risk factors for cervical cancer: Senegal national rates* and Kédougou rates |
Prior to this study, prevalence data for cervical dysplasia were unavailable for the Kédougou region or surrounding rural regions of Senegal. Follow-up studies with efforts at ensuring representative distribution across age groups are needed.
Similar studies will also need to be performed in neighboring regions to confirm the generalizability of the results.
Clinical implications
Clinical implications of this study include the need for capacity building of cervical cancer prevention services in the low-resource rural areas of Senegal. The use of VIA in this setting is practical, is sustainable, and has been shown to be effective through prior studies. However, VIA is not routinely used as an approach for a population-level epidemiological prevalence study. In areas where other screening modalities are not available or are too expensive, VIA may be used for this purpose, as we have demonstrated in this study.
Given this study’s success in screening a representative population across a rural Senegal region, this study also illustrates the utility of a capacity-building approach to implement cervical cancer screening services using the training of trainers and task-sharing (with clinical responsibilities being provided by midwives and nurses) in a rural area with a significant health-care workforce shortage. It is possible through task sharing to build capacity for screening with VIA at the local level. Through the use of this screening approach in routine health care delivery, local health services can affordably conduct population studies while improving their own health services with locally appropriate technology. The training of trainers may facilitate the horizontal scaling of this technology with relative efficiency. Neighboring regions and countries can benefit from the experience of the Kédougou region by means of local collaboration that requires little outside technical support.
Policy implications
In the Kédougou region, these findings will inform the formal integration of cervical cancer screening into the basic health service package. This will be achieved through increased capacity support and the implementation of regional policy for cervical cancer prevention health services. The identification of access barriers for older populations can inform efforts to improve the responsiveness of the cervical cancer screening programs. Community-participatory health services policy development will be used to improve community health service utilization throughout the region. The determination of the prevalence of cervical dysplasia in neighboring regions will further inform the Ministry of Health and Social Affairs of the need for further formal support of cervical cancer prevention services throughout rural Senegal.
Societal and community implications
This study, carried out in partnership with the Peace Corps, illustrates the success that can be achieved through academic institutions partnering with a locally placed development organization for clinical services strengthening projects and research support. This approach links local community members and health care providers and leaders, the US and local academic and research resources, and the US Peace Corps. The Peace Corps is a wide-reaching US governmental development organization that is permanently positioned at the local level and aligned with health services in many LMICs. Being integrated into the communities, PCVs understand the local context and are routinely engaged in community empowerment through participatory activities. Our partnership model uses participatory methods to support the sustainability of health systems while focusing on research into implementation of primary health care services. This study illustrates this partnership approach as an effective means of facilitating implementation research on cervical cancer prevention services in a low-resource setting.
Study strengths, limitations, and lessons learned
The strength of this study includes the acquisition of a large, representative sample of the region. In addition, we are confident of the fidelity of the research process. The reliable, on-the-ground support of PCVs accompanying the screening team on nearly every outing provided an additional layer of research protocol oversight. All the clinicians conducting VIA (as a part of this study) completed a formalized VIA training course and passed a scored, multiple-item written and visual test. This assured a baseline competence for all clinicians. However, a limitation was that no interrater reliability test was conducted among the VIA clinicians as a part of this study.
Another limitation of our study was the relative inexperience of those conducting VIA. Though we did not know the true prevalence of dysplasia in the region, previous evidence illustrates a positive predictive value of 10% with VIA,22 so this must be taken into consideration in interpretation of the results. Validity of the screening results between districts could be improved through improved standardization of screening processes, eg, by conducting the screenings with the same personnel or with oversight by a single highly experienced provider. Photographing the cervical examination of a segment of the overall screened sample would further validate the results across screening teams and districts. A true prevalence rate may be established over time by gathering further data and addressing the challenges identified in this study.
Another major challenge in study implementation was some reluctance of women to participate. This reticence varied by village. Anecdotally, the teams noted that several factors played a role in influencing participation. The comfort and clinical experience of the first few women screened may have played a role in reassuring or discouraging peers from participation in the screening, and village activities such as gardening or weddings prevented some women from attending the mass screening events. Additionally, some villages are known by health workers to be more cautious of seeking health care through the formal health system, with many people trusting only traditional healers in more remote settings. These challenges contributed to the stated low screening participation rate of 21.4%. The survey response rate of 56.4% among those who were screened was also likely due to these considerations, as well as the refusal of many women to remain for an additional task due to the need to return to work, duties, or other activities. Anxieties related to providing personal opinions and views in this sample (with little-to-no previous exposure to research activities) also constitute a potential factor.
Our data were also influenced by the low literacy rate of the sample population and the known trust concerns in a few communities. Detailed demographic information was not sought to limit the number of questions and make the questionnaire feasible and not tedious for the respondents. We did not link questionnaires to community or health structure to respect the concern by the local health service personnel, who desired to ensure participant anonymity and build trust. Therefore, our ability to comprehensively interpret the risk factor data is limited.
A potential bias for this study exists due to the convenience sampling of women at the village level, with women having self-selected for the screenings. In some of the selected villages, the percentage screened of the estimated population was high, thus reducing this bias. However, in villages where there was a low percentage of the estimated population screened, the bias could exist. With this consideration, it is likely that the women who self-selected were not significantly different from the rest of the population. In addition, it is possible that women who self-selected for screening may be more health conscious and less at risk for the development of cervical dysplasia. However, older women, those most likely to be at risk for a positive screen, do not routinely seek care in rural Senegal because they associate the need for health-seeking behavior with pregnancy and childbearing, according to reports from the midwife team. Our small sample in the 40- to 50-year age range could illustrate this bias and may have contributed to an underestimation of study findings.
Conclusion
This study is an effort to advance the science of addressing timely detection and treatment of cervical cancer, a preventable cause of morbidity and mortality for women worldwide, particularly in low-resource settings. The research was conducted in a rural setting in Senegal through a partnership that is dedicated to implementing an evidence-based, technologically appropriate cervical cancer prevention solution, the screen-and-treat method using VIA. Our findings build on prior evidence on the feasibility and utility of VIA as a low-cost screening method.24–26 A training-of-trainers and task-sharing approach has helped the region develop the capacity to implement this service. The prevalence data will be used as a baseline gauge for the advancement and impact of health services in coming years. In addition to prevalence data, we anticipate that findings about the associated cervical cancer individual risk factors can guide future interventional research programs aimed at addressing dysplasia or cervical cancer in this population. Next steps in this work will focus on improving the community utilization of this service and thereby increasing cervical cancer prevention health services utilization across all age groups. To achieve this goal, we will conduct a mixed-methods analysis of the demand-side barriers to initial uptake and sustained utilization of this screening service. Our partnership also aims to build scientific knowledge and inform the implementation of cervical cancer prevention programs in other areas in Senegal, as well as other low-resource areas globally.
Key message
In 2014, The Regional Ministry of Health and Social Affairs, Kédougou, Senegal, assessed regional cervical cancer risk factors and precancer prevalence to inform program implementation. Screening rates were suboptimal, especially among older, higher-risk women, illustrating the need to investigate demand-side access barriers and motivate older women to utilize services, in addition to sustaining an effective cervical cancer screening program.
Acknowledgments
The authors would like to acknowledge and thank the following individuals: Abib Ndiaye, Aziz Kasse, Evrard Kabou, Malick Sarr, Mahmoud Ndiaye, Fatou Ndour, Aissatou Sarr, Diouma Diallo, Ngoné Gueye, Hamidou Thiam, Mamadou Diaw, Chris Hedrick, Vanessa Dickey, Chris Brown, Leah Moriarty, Meera Sarathy, Marielle Goyette, Larocha LaRiviere, Chip Ko, Chris Coox, Matthew Westercamp, John Hickner, Stevan Weine, Michael Fleming, Don Hedeker, Catherine Lind, and Paul Rotert. This study was funded by the Department of Family Medicine, University of Illinois at Chicago.
Author contributions
All authors contributed to the conception and design of the study (JAD, YN, AML, TI, KEP, FT, and MTD) or to the acquisition, analysis, and interpretation of data (MH, MP, KW, PL, FT, and MTD), and drafted the manuscript (JAD, AML, TI, KEP, and MP) or revised it critically for content (YN, MH, KW, PL, FT, and MTD). All authors read and approved the final manuscript. All authors meet the International Committee of Medical Journal Editors authorship criteria. All authors contributed toward data analysis, drafting and critically revising the paper and agree to be accountable for all aspects of the work.
Disclosure
There exist no relevant conflicts of interest in the form of financial interest for any author. No authors hold any patents broadly relevant to this work. A potential perceived conflict of interest based on a relationship is that J Andrew Dykens directs a 501(c)(3) nonprofit organization, Peace Care, which is partially responsible for the development of the partnership between the implicated institutions. Dr Dykens has never been and is not currently compensated in any way for his role with Peace Care. Furthermore, Peace Care has not contributed financially to any aspect of the science or research within this partnership. The role of Peace Care is limited to the partnership development and management. The authors report no other conflicts of interest in this work.
References
Torre LA, Bray F, Siegel RL, Ferlay J, Lortet-Tieulent J, Jemal A. Global cancer statistics, 2012. CA Cancer J Clin. 2015;65(2):87–108. | ||
Forman D, de Martel C, Lacey CJ, et al. Global burden of human papillomavirus and related diseases. Vaccine. 2012;30(suppl 5):F12–F23. | ||
Ferlay J, Soerjomataram I, Ervik M, et al [webpage on the Internet]. GLOBOCAN 2012 v1.1, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. Lyon: International Agency for Research on Cancer; 2015. Available from: http://www.wcrf.org/int/cancer-facts-figures/data-specific-cancers/cervical-cancer-statistics. Accessed October 20, 2016. | ||
Forouzanfar MH, Foreman KJ, Delossantos AM, et al. Breast and cervical cancer in 187 countries between 1980 and 2010: a systematic analysis. Lancet. 2011;378(9801):1461–1484. | ||
Allemani C, Weir HK, Carreira H, et al. Global surveillance of cancer survival 1995–2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet. 2015;385(9972):977–1010. | ||
Brown ML, Goldie SJ, Draisma G [webpage on the Internet]. Chapter 29: health service interventions for cancer control in developing countries. In: Jamison DT, Breman JG, Measham AR, editors. Disease Control Priorities in Developing Countries. 2nd ed. Washington, DC: SRC – GoogleScholar; 2006. Available from: http://www.ncbi.nlm.nih.gov/books/NBK11756/. Accessed October 20, 2016. | ||
World Health Organization. Package of Essential NCD Interventions for Primary Health Care: Cancer, Diabetes, Heart Disease and Stroke, Chronic Respiratory Disease. Geneva: World Health Organization; 2010. | ||
World Health Organization. Cancer Control: Knowledge into Action: WHO Guide for Effective Programmes. Geneva: World Health Organization; 2007:42. | ||
Parkhurst JO, Vulimiri M. Cervical cancer and the global health agenda: insights from multiple policy-analysis frameworks. Glob Public Health. 2013;8(10):1093–1108. | ||
Sankaranarayanan R, Esmy PO, Rajkumar R, et al. Effect of visual screening on cervical cancer incidence and mortality in Tamil Nadu, India: a cluster-randomised trial. Lancet. 2007;370(9585):398–406. | ||
Xi LF, Touré P, Critchlow CW, et al. Prevalence of specific types of human papillomavirus and cervical squamous intraepithelial lesions in consecutive, previously unscreened, West-African women over 35 years of age. Int J Cancer. 2003;103(6):803–809. | ||
Bruni L, Barrionuevo-Rosas L, Albero G, et al [homepage on the Internet]. Human Papillomavirus and Related Diseases in Senegal. Summary Report. ICO Information Centre on HPV and Cancer (HPV Information Centre); 2015. Available from: http://www.hpvcentre.net/. Accessed October 20, 2016. | ||
Langley CL, Benga-De E, Critchlow CW, et al. HIV-1, HIV-2, human papillomavirus infection and cervical neoplasia in high-risk African women. AIDS. 1996;10(4):413–417. | ||
World Health Organization (WHO) [webpage on the Internet]. Senegal-World Health Survey (SEN__WHS_v01_M). 2003. Available from: http://apps.who.int/healthinfo/systems/surveydata/index.php/catalog/87 SRC - GoogleScholar. Accessed October 20, 2016. | ||
Woto-Gaye G, Critchlow C, Kiviat N, Ndiaye PD. [Cytological detection of cervical cancer in black Africa: what are the perspectives?]. Bull Cancer. 1996;83(5):407–409. | ||
Enquête Démographique et de Santé à Indicateurs Multiples au Sénégal (EDS-MICS) 2010–2011. Agence Nationale de la Statistique et de la Démographie (ANSD) [Sénégal] et ICF International. Calverton, MD: ANSD et ICF International; 2012. Available from: http://dhsprogram.com/pubs/pdf/FR258/FR258.pdf. Accessed October 20, 2016. SRC – GoogleScholar. | ||
Freeman HP, Chu KC. Determinants of cancer disparities: barriers to cancer screening, diagnosis, and treatment. Surg Oncol Clin N Am. 2005;14(4):655–669. | ||
Abril EP, Kupczyk M, Zwicke GL, Mastarone GL, Irwin T, Dykens A. Mapping the health communication infrastructure in rural senegal: an assessment to support cervical cancer screening. J Appl Commun Res. 2015;43(2):242–262. | ||
Huezo C, Diaz S. Quality of care in family planning: clients’ rights and providers’ needs. Adv Contracept. 1993;9(2):129–139. | ||
EngenderHealth C. Handbook: A Process for Improving Quality in Health Services. New York: EngenderHealth; 2003. | ||
EngenderHealth. COPE for Cervical Cancer Prevention Services: A Toolbook to Accompany the COPE Handbook®. New York: EngenderHealth; 2004. [EngenderHealth’s Quality Improvement Series]. | ||
Sauvaget C, Fayette J-M, Muwonge R, Wesley R, Sankaranarayanan R. Accuracy of visual inspection with acetic acid for cervical cancer screening. Int J Gynaecol Obstet. 2011;113(1):14–24. | ||
World Health Organization. Comprehensive Cervical Cancer Control: A Guide to Essential Practice. Geneva: World Health Organization; 2015. | ||
Blumenthal PD, Lynne G, Sylvia D, et al; Ghana Cervicare Group. Cervical cancer prevention: safety, acceptability, and feasibility of a single-visit approach in Accra, Ghana. Am J Obstet Gynecol. 2007;196(4):407.e1–407.e9. | ||
Goldie SJ, Kuhn L, Denny L, Pollack A, Wright TC. Policy analysis of cervical cancer screening strategies in low-resource settings: clinical benefits and cost-effectiveness. JAMA. 2001;285(24):3107–3115. | ||
Tergas AI, Gaffikin L, Limpaphayom KK, Charurat E, Eamratsameekool W, Lu E. A single-visit approach to cervical cancer prevention in rural Thailand. Int J Gynaecol Obstet. 2014;126(1):90. | ||
Louie KS, de Sanjose S, Diaz M, et al. Early age at first sexual intercourse and early pregnancy are risk factors for cervical cancer in developing countries. Br J Cancer. 2009;100(7):1191–1197. | ||
Were E, Nyaberi Z, Buziba N. Perceptions of risk and barriers to cervical cancer screening at Moi Teaching and Referral Hospital (MTRH), Eldoret, Kenya. Afr Health Sci. 2011;11(1):58–64. | ||
Thulaseedharan JV, Malila N, Hakama M, et al. Socio demographic and reproductive risk factors for cervical cancer – a large prospective cohort study from rural India. Asian Pac J Cancer Prev. 2012;13(6):2991–2995. | ||
StataCorp. Stata Statistical Software. 13 ed. College Station, TX: StataCorp; 2013. | ||
SAS Institute Inc. Base SAS® 9.3 Procedures Guide. Cary, NC: SAS Institute Inc.; 2011. SRC – GoogleScholar. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.