Back to Journals » Vascular Health and Risk Management » Volume 13
Implementing clinical process management of vascular wounds in a tertiary facility: impact evaluation of a performance improvement project
Authors Avruscio G ![]() , Tocco-Tussardi I
, Tocco-Tussardi I ![]() , Bordignon G, Vindigni V
, Bordignon G, Vindigni V ![]()
Received 15 March 2017
Accepted for publication 29 August 2017
Published 16 October 2017 Volume 2017:13 Pages 393—401
DOI https://doi.org/10.2147/VHRM.S137099
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Amudha Kadirvelu
Giampiero Avruscio,1,* Ilaria Tocco-Tussardi,1,2,* Greta Bordignon,3 Vincenzo Vindigni2
1Angiology Unit, Department of Cardiac, Thoracic and Vascular Sciences, University Hospital of Padova, Padova, Italy; 2Clinic of Plastic and Reconstructive Surgery, Department of Neurosciences, University Hospital of Padova, Padova, Italy; 3Clinical Management, University Hospital of Padova, Padova, Italy
*These authors contributed equally to this work
Background: Chronic vascular wounds have a significant economic and social impact on our society calling for allocation of a great deal of attention and resources. Efforts should be oriented toward the achievement of the most effective and efficient clinical management. The Angiology Unit at the University Hospital of Padova, Italy, developed a performance improvement project to enhance the quality of practice for vascular ulcers.
Methods: The project consisted in a multistep process comprising a critical revision of the previous clinical process management, staff education, tightening connections between operators and services, and creation of a position for a wound care nurse. The previous standard of practice was modified according to the results of revision and the current evidence-based practice.
Results: The new standard of practice reached its full application in September 2015. The number of patients treated and the number of visits in 2015 remained almost unvaried from 2014. However, the total annual expenditure for treating vascular ulcers was reduced by ~60% from the previous year.
Conclusion: Standardization of guidelines and practice is effective in creating an efficient clinical management and in reducing the economic burden of vascular ulcers.
Keywords: chronic wounds, clinical process management, cost-effectiveness, vascular ulcers
Introduction
Vascular ulcers, especially of venous origin, are a relatively common condition in the adult population (1% of the population and 3.6% of people older than 65 years in developed countries) and are associated with significant morbidity, high cost of health care, loss of productivity, and reduced quality of life.1–3 Treatment can be expensive, leading to a large economic burden on health services: the annual cost for chronic venous lesions is estimated to be >1 billion USD in the US and between 400 and 600 million pounds in the UK.1,4,5 In the province of Padova (Veneto region of Italy), the annual health expenditure for 1,421 patients receiving community health assistance is close to EUR 6 million (USD 6,402,060) (mean cost per patient EUR 4,225) and this is around 1% of the health care budget of the province (Ranzi M, unpublished dataset, 2005) (Table 1).
 | Table 1 Prevalence of chronic wound problems among people receiving community health assistance in the province of Padua (IT) (~920,200 inhabitants) Note: *Percent on the total of lesions. |
Recent literature has been reporting encouraging results in the reduction of the economic burden of chronic ulcers coming from performance improvement projects. Implementation of practice through staff education, standardization of therapy, and enforcement of a multidisciplinary approach has been demonstrated to increase efficacy of treatment (reduction in home visits and in the range of products used) and to reduce prevalence, overall controlling costs.6–9
The present paper is the qualitative descriptive report of a project of improvement of practice at Angiology Unit of the University Hospital of Padova. The project was designed in response to an internal audit carried out in 2014, which highlighted a series of critical points in the management of vascular ulcers and a poor control of expenditures.
Materials and methods
Setting
The Angiology Unit provides vascular medicine service for the whole province of Padova (catchment population of ~1 million inhabitants). The unit is the “hub” for vascular ulcers. All major assessments are undertaken at the unit, and all emergencies for the whole province are sent there. Outpatient clinic and a ward referral service are provided. The wound clinic runs on a daily basis, 6–7 patients are seen on average every day. The project was held over an 8-month period (April–December 2015).
Project rationale
Throughout 2014, an internal audit was carried out: the chart audit was developed to assess the evidence-based recommendations for the management of vascular ulcers and to highlight the discrepancies between actual practice and standard in order to identify the changes needed to improve the quality of care. Evidence from observations indicated that physicians and nurses provided care not always consistent with the recommendations, and assessment and decision-making processes were poorly documented. Specifically, patient management followed a standardized protocol. A physician, specialist in Angiology, primarily assessed a new lesion, established the etiology of the wound, and determined the plan for management. Thereafter, wound care was mostly carried out by non-dedicated nurses with great variability in experience on the management of vascular lesions. The nurse consulted the physician if the patient had either a non-healing ulcer or a new skin breakdown. However, the physician was not necessarily the same who had performed the previous clinical evaluation for a variety of reasons (shifts, temporary unavailability, etc.). If the patient was to be seen by a different physician, there would often be disagreement with the previous treatment plan with poor communication between professionals. Further criticalities detected through the audit tool were as follows: a lack of information sharing between medical and nursing staffs on the use rationale of different products/devices; scarce use of electronic medical records although available; and unsatisfying multidisciplinary collaboration because of unclear referral pathways for further assessment if required. Overall, clinical management showed some major inconsistencies and appeared more as a chain of individual and isolated performances instead of a structured and solid team approach.
Phases of the project
The project consisted of four phases (Table 2).
 | Table 2 Synopsis of the project for improvement of clinical management for vascular wounds Notes: Detection of involved health care professionals: Project director: Director of the Angiology Unit at the University Hospital of Padua; Expert A: 1 vascular surgeon and 1 registered nurse who has been working in chronic wound care for 10 years; Expert B: health care specialists (4 specialists in Angiology, 1 vascular surgeon, 1 phlebologist, 1 general surgeon, 1 specialist in long-term hospital care, 1 microbiologist, 1 anesthesiologist, 1 dermatologist, 1 specialist in Forensic Medicine, 1 plastic surgeon, and 1 registered nurse who has been working in chronic wound care for 5 years). |
Phase I: global assessment of wound care system status
We comprehensively analyzed our current standards of practice for both arterial and venous chronic ulcers. This action was performed by medical and nursing staff conjoint meetings where the algorithms of management were reviewed (IA). Critical points in the algorithms were detected (Figures 1 and 2), and staff members were encouraged to make proposals for improvement of management. Also, in the phase we set outcome indicators to be used as a qualitative assessment of the impact of the project on clinical practice:
- Physicians: standardization of clinical data collection; consensus on treatment modalities; harmonization of use rationale for products/devices; and computerization of clinical documentation.
- Nurses: harmonization of knowledge on the management of vascular lesions including dressing products use and compression bandaging among different operators; standardization of practice (measurement of the ankle–brachial pressure index, wound dressing, wound swabbing technique, and measurement of transcutaneous oxygen-transcutaneous carbon dioxide); and increase of use of the computerized patient management system.
- Administrators: increase of knowledge of the multiple needs of patients affected by chronic vascular lesions to promote a holistic care approach and strengthen connections with community care.
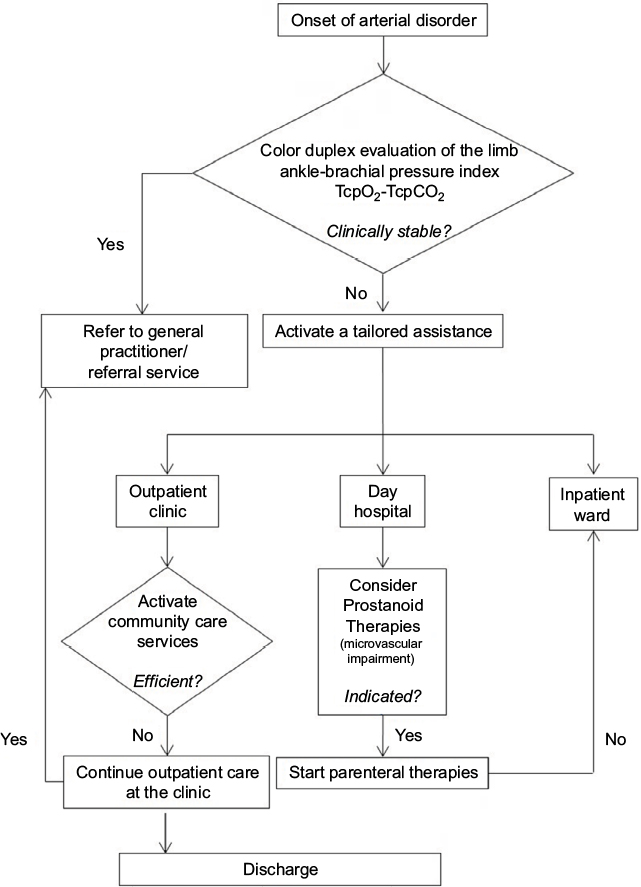 | Figure 1 Algorithm of management for peripheral arterial disease. Abbreviations: TcpO2, transcutaneous oxygen; TcpCO2, transcutaneous carbon dioxide.
|
 | Figure 2 Algorithm of management for venous disease. Note: *Hospitalization was recommended for patients with massive deep venous thrombosis, with symptomatic pulmonary embolism, at high risk of anticoagulant bleeding, or with major comorbidity. |
The following step consisted in assessing the knowledge of the staff on the latest international guidelines for treatment10–12 to set goals for the educational phase (IB). The third step was focused on the assessment of the standards of practice for vascular ulcers in the community (IC). We visited the Community health Centers and met with the service managers for chronic wound care. An audit tool was created to collect information on the standards of practice. The meetings were the occasion not only to collect information and share ideas but also to strengthen the connection and cooperation between different realities operating on the same field.
The concluding step was focused on the education of personnel (ID). From the assessment of knowledge, we highlighted some outdated practice habits by the medical staff and an unstructured knowledge of wound care by the nursing staff. Therefore, the strategy used was to provide the most comprehensive education, update, and training on the assessment, management, and treatment of vascular lesions. The education plan was structured in weekly sessions comprising multidisciplinary meetings with experts, presentation of case studies, wound care algorithms, ulcer management workshops, and hands-on training on compression therapy with experts. The meetings also functioned as a tool to enhance knowledge of the referral figures within the hospital and clear referral modalities were set with service managers.
Phase II: development of a new standardized protocol
Algorithms of practice were implemented according to the criticalities detected in the first phase (IIA). Instructional videos of common procedures (measurement of the ankle–brachial pressure index, wound dressing, wound swabbing technique, and measurement of transcutaneous oxygen-transcutaneous carbon dioxide) were recorded and distributed in order to enhance standardization of practice among different operators of the nursing staff (IIB).
Phase III: application of the new protocol
This phase included the creation of a position for a “wound care nurse” who would devote her activity specifically to wound care in the clinic. This nurse had a sound knowledge and training in caring for patients with compromised skin, gained through enhancement of the baseline knowledge through participation in master classes on ulcers care, courses on proper treatment of vascular ulcers, and a 10-year experience on the field. The wound care nurse would acquire and apply the wound care plan as assessed by the physician and would guide the plan for optimal wound care. She would collect and record all the wound documentation, including regular wound assessment describing the patient’s lesion, and digital images (these were usually acquired at the beginning of the treatment, if the lesion would worsen, and also to document improvement in the healing process). She would also identify opportunities to improve practice as a patient’s wound status would change and would share the findings and review the treatment plan with the staff member who assessed the original findings. Finally, the wound care nurse would give recommendations for therapeutic support and skin care products. The introduction of such a dedicated professional figure was intended to specifically control several important factors that were contributing to a non-performing management of chronic ulcers.
Phase IV: review of outcome indicators
Indicators were reviewed in terms of achievement or failure 3 months after the new standard of practice reached its full application (December 2015) (Table 2). Among proposals for future development, continuous improvement training courses were established to be carried out throughout the whole year starting in 2016 to help maintain and maximize the improvement program’s benefits at our unit.
Results
Table 3 shows the results achieved with referral to outcome indicators. Outcomes expected as results were achieved in almost all cases, even though some actions were still susceptible of improvement.
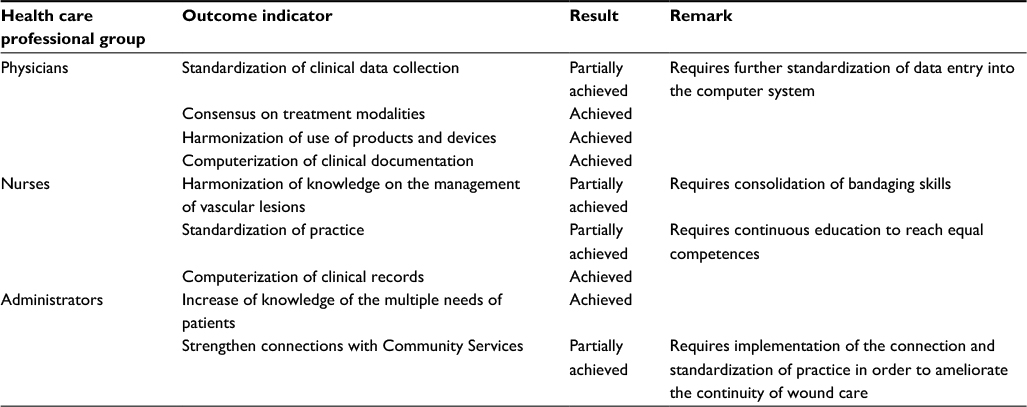 | Table 3 Results of the project with referral to outcome indicators |
In 2015, we treated 319 patients for vascular wound problems and recorded 3,186 admissions to the outpatient wound clinic for evaluation – treatment. These data showed no consistent variation from 2014 (313 patients treated and 3,137 admissions). However, the total annual expenditure for treating vascular ulcers in 2015 was reduced by 56.1% from the previous year. Specifically, the fixed costs as defined by the public health service and the variable costs for wound care were reduced by 18.2% and 86.3%, respectively. While a reduction in the fixed costs is only partially attributable to the project as the provision of basic supplies is regulated by a strict hospital policy on prices, the cut in the order of extra materials, eg, advanced dressing between the year before and after the project, is most certainly a direct improvement of practice. Results regarding costs are showed in detail in Table 4. For 2016, only partial data on total costs related to wound care were available. The number of patients treated and admissions showed slight variations (288 and 3,165, respectively), but the annual expenditure was further reduced (4.7% from 2015), confirming a continuity in cost savings.
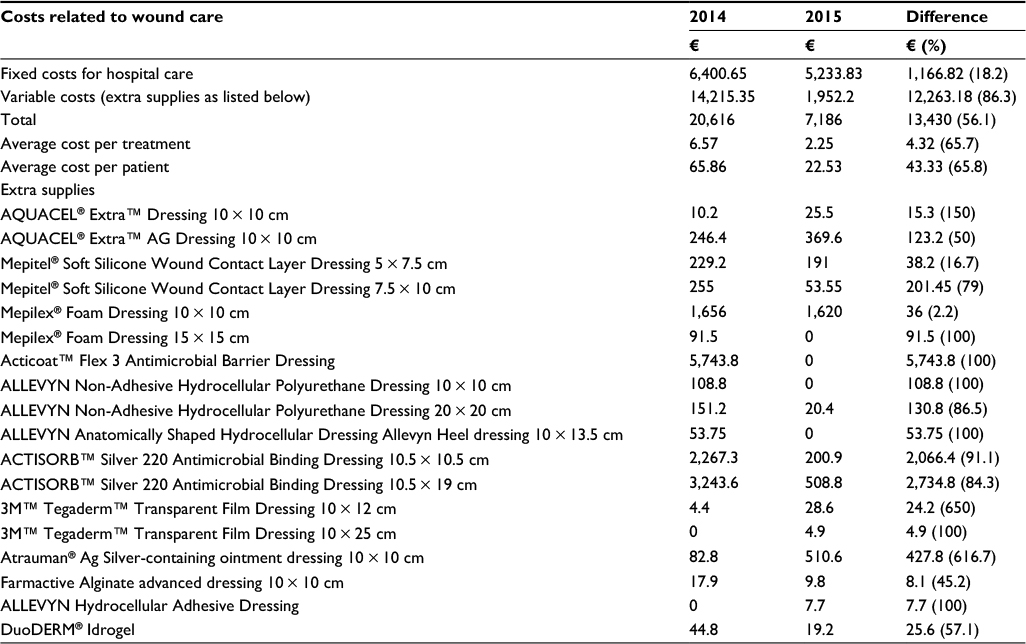 | Table 4 Difference in costs related to wound care between the year before and the year after the project |
Discussion
The complexity of management of vascular lesions and the relevance of the issue under a health, social, and economic point of view have prompted the competent authorities to try and develop the most efficient standards of management and treatment. Approaches and concepts for the optimal treatment of vascular wounds have been multiple. Therapies have been progressively uniformed from the development and update of international guidelines available. The products and devices on the market have increased progressively in number and quality. The realization of comprehensive and multidisciplinary treatment structures has been promoted and already achieved in some countries.13–16
From our experience, the centrality of progress in clinical practice for vascular wounds is represented by the empowerment of knowledge and the integration of competencies. These primary goals allow reaching optimal clinical practice through appropriate and consistent management by each operator and a fruitful collaboration between different professional figures. In our unit this led to a significant reduction of costs in agreement with results from other centers where performance-implementation projects were carried out.6–8,17–19 Our results were also particularly encouraging as the new standardized practice had been fully applied for only 3 months before annual expenditure was calculated. The process of revision led also to the development of evidence-based practice guidelines in March 2017 (unpublished data), which will be soon available for online consultation for all the staff members of the hospital. We encourage treatment facilities to perform critical revision of clinical management in order to highlight area of improvement and to enhance the service, rationalize resources, and to impact final outcome.
With specific regard to Italy, full integration of hospital care into the national health care organization is of vital importance for the care of patients affected by chronic vascular lesions. As described earlier, patient care is managed by different services: first by the tertiary hospital, where the Angiology and Vascular Surgery Units are based, and then separately by the Community Services. Health districts are covered with general practitioners, nurses, social workers, administrative personnel, and other medical specialists.
Among other activities, the health district provides for chronic wound care through outpatient clinics and home assistance. Once discharged from the tertiary hospital, patients are often referred for continuity of care to the district services. Therefore, they should ideally function as a natural prosecution of hospital care. However, this is not always possible for a variety of reasons (health care planning, health care financing, and framework regulations). The social care in Italy is free of charge for citizens. State funding goes directly from the Italian State to the municipalities. Sometimes municipalities themselves manage their own social services, otherwise they may entrust funds directly to the local health authorities. Further complexities exist, as the patient is usually old and fragile, may not be supported by the presence of family members/caregivers, and may need further specialized treatment. All this means that establishing services that will operate across the boundaries between acute and community care can be difficult. Nonetheless, it should not be forgotten that patients are the weak ring of the chain in the process and can suffer the consequences of an unraveled assistance model, not only between hospital and Community Services but sometimes even within the same facility. In order to supply the optimal standard of care it is therefore imperative to review and enhance practice on different levels, from the reality of a unit to the relationships with the different health care organizations involved.20 As far as our unit is concerned, this will constitute the future development of the implementation process. In order to do so we plan on setting collaboration with the national health system to enhance data collection and audit on the incidence and prevalence of vascular wounds across the province. Recently, all the health district of the province has been brought under the same jurisdiction. We are confident this will further enhance connection, a common standard of practice, and an active role of community services. The coordination function of the national system is of vital importance for the establishment of a relevant and solid system.
The current report has several limitations. It is a qualitative and singe-center study, which limits the potential of our conclusions. Furthermore, because of the relatively recent introduction of the new standard of practice we could not detect a correlation between the new routine and healing rate, and our conclusions are necessarily limited. Nonetheless, the reduction in costs for wound management resulted from an improvement in practice, as the characteristics of the patient population referring to our clinic (age, gender, comorbidities, wound etiology, and dimension) remained stable between the year before and the year after the project and are in line with the data presented in Table 1.
Conclusion
Overall, this survey emphasized the importance of education and cooperation to reach an efficient clinical management through standardization of practice. An optimized wound-care system is also effective in reducing the economic burden of vascular ulcers. The comprehensive program discussed in this article seems to confirm that total costs may be reduced when the individual patient has access to a harmonized and efficient group of health care workers.
Acknowledgments
The authors would like to thank G Camporese, MD, RC Martini, MD, G Salmistraro, MD, and MA Scomparin, MD, who served as scientific advisors; E Baracco, RN, M Bettella, RN, L Cacco, RN, N Griggio, RN, S Morandin, RN, F Nalin, RN, A Noventa, RN, O Scarpazza, RN, C Tonello, RN, and P Zulian, RN, who provided and cared for the study; C Napoli, L Bissoli, E Farinazzo, and B Rossato, who provided technical administrative support.
Disclosure
The authors report no conflicts of interest in this work.
References
Lal BK. Venous ulcers of the lower extremity: definition, epidemiology, and economic and social burdens. Semin Vasc Surg. 2015;28(1):3–5. | ||
Green J, Jester R, McKinley R, Pooler A. The impact of chronic venous leg ulcers: a systematic review. J Wound Care. 2014;23(12):601–612. | ||
Gordon P, Widener JM, Heffline M. Venous leg ulcers: impact and dysfunction of the venous system. J Vasc Nurs. 2015;33(2):54–59. | ||
Markova A, Mostow EN. US skin disease assessment: ulcer and wound care. Dermatol Clin. 2012;30(1):107–111. | ||
Rabe E, Pannier F. Societal costs of chronic venous disease in CEAP C4, C5, C6 disease. Phlebology. 2010;25(suppl 1):64–67. | ||
Hanna-Bull D. Preventing heel pressure ulcers: sustained quality improvement initiative in a Canadian acute care facility. J Wound Ostomy Continence Nurs. 2016;43(2):129–132. | ||
Armour-Burton T, Fields W, Outlaw L, Deleon E. The Healthy Skin Project: changing nursing practice to prevent and treat hospital-acquired pressure ulcers. Crit Care Nurse. 2013;33(3):32–39. | ||
Chicano SG, Drolshagen C. Reducing hospital-acquired pressure ulcers. J Wound Ostomy Continence Nurs. 2009;36(1):45–50. | ||
Blaszczyk J, Majewski M, Sato F. Make a difference: standardize your heel care practice. Ostomy Wound Manage. 1998;44(5):32–40. | ||
Alavi A, Sibbald RG, Phillips TJ, et al. What’s new: management of venous leg ulcers: treating venous leg ulcers. J Am Acad Dermatol. 2016;74(4):643–664; quiz 665–666. | ||
Alavi A, Sibbald RG, Phillips TJ, et al. What’s new: management of venous leg ulcers: approach to venous leg ulcers. J Am Acad Dermatol. 2016;74(4):627–640; quiz 641–642. | ||
Kirsner RS. The Wound Healing Society chronic wound ulcer healing guidelines update of the 2006 guidelines – blending old with new. Wound Repair Regen. 2016;24(1):110–111. | ||
Gray BL. Developing a model for clinical practice. J Wound Care. 1996;5:428–432. | ||
Gottrup F, Holstein P, Jorgensen B, Lohmann M, Karlsmar T. A new concept of a multidisciplinary wound healing center and a national expert function of wound healing. Arch Surg. 2001;136:765–772. | ||
Gottrup F. A specialized wound-healing center concept: importance of a multidisciplinary department structure and surgical treatment facilities in the treatment of chronic wounds. Am J Surg. 2004;187(5A):38S–43S. | ||
Granick MS, McGowan E, Long CD. Outcome assessment of an in-hospital cross-functional wound care team. Plast Reconstr Surg. 1998;101(5):1243–1247. | ||
Morehead D, Blain B. Driving hospital-acquired pressure ulcers to zero. Crit Care Nurs Clin North Am. 2014;26(4):559–567. | ||
McElhinny ML, Hooper C. Reducing hospital-acquired heel ulcer rates in an acute care facility: an evaluation of a nurse-driven performance improvement project. J Wound Ostomy Continence Nurs. 2008;35(1):79–83. | ||
Hiser B, Rochette J, Philbin S, Lowerhouse N, Terburgh C, Pietsch C. Implementing a pressure ulcer prevention program and enhancing the role of the CWOCN: impact on outcomes. Ostomy Wound Manage. 2006;52(2):48–59. | ||
Mooij MC, Huisman LC. Chronic leg ulcer: does a patient always get a correct diagnosis and adequate treatment? Phlebology. 2016;31(1 suppl):68–73. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.