Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Implementation of the Allied Health Assistant Workforce in the Australian Context: An Integrative Review
Authors Pearce C ![]() , Phillips R
, Phillips R ![]() , Richardson A, Volker N, Mitterfellner R
, Richardson A, Volker N, Mitterfellner R ![]()
Received 28 August 2025
Accepted for publication 2 December 2025
Published 13 December 2025 Volume 2025:18 Pages 7979—8004
DOI https://doi.org/10.2147/JMDH.S561660
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Claire Pearce,1 Rebecca Phillips,1,2 Andy Richardson,2 Nerida Volker,3 Rachael Mitterfellner1,2
1Discipline of Occupational Therapy, University of Canberra, Canberra, ACT, Australia; 2Canberra Health Services, ACT Government, Canberra, ACT, Australia; 3Health and Human Services, TAFE NSW, Sydney, NSW, Australia
Correspondence: Claire Pearce, Clinical Education and Research Centre, University of Canberra Hospital, Guraguma Street, Bruce, ACT, 2617, Australia, Tel +61 2 6206 8452, Email [email protected]
Abstract: The Allied Health Assistant (AHA) workforce plays a critical role in enhancing the capacity, efficiency, and accessibility of allied health services across Australia. Considering significant structural reforms in sectors in which AHAs are employed, including the introduction of the National Disability Insurance Scheme (NDIS) and changes to aged care funding, this integrative review synthesizes current evidence on the utilization of AHAs across diverse settings, disciplines, and sectors. A comprehensive search of peer-reviewed and government literature from 2007 to 2025 identified 38 studies and 18 policy documents. A concept analysis identified four key concepts: service efficiency and quality, capacity building through training, contextual and structural determinants of role implementation, and tensions between role innovation and professional boundaries. Findings highlight the positive impact of AHAs on therapy access and service delivery, the importance of context-specific training and supervision, and the need for supportive organizational structures. Despite growing recognition of the AHA role, gaps remain in outcome-focused research, particularly in mental health, disability, and aged care settings. This review underscores the need for targeted workforce strategies and policy development to optimize the integration and sustainability of the AHA workforce in Australia’s evolving health landscape.
Plain English Summary: This review looks at how Allied Health Assistants (AHAs) help deliver healthcare in Australia. AHAs work under the guidance of qualified health professionals to support therapy and improve access to care. The review covers research and government documents from 2007 to 2025. The authors found that AHAs make a positive difference in four main areas:.Improving Services: AHAs help more people get therapy and allow health professionals to do more of the tasks they are trained to do. This leads to better care and more efficient services.Training and Support: AHAs need training that fits their specific work setting. While formal qualifications are useful, hands-on training at work is often more effective. Supervisors also need training to guide AHAs properly.Workplace Conditions: Where AHAs work, such as in cities or rural areas, affects how well they can do their job. Clear guidelines, good supervision, and supportive workplaces help AHAs succeed.Balancing Roles: Some health professionals worry that AHAs might take over parts of their job. AHAs often have limited chances to grow in their careers, which can lead to high staff turnover.
The review shows that AHAs are valuable, but more research is needed, especially in mental health, disability, and aged care. To make the most of AHAs, services that employ AHAs should invest in training, create flexible job roles, and build a culture that supports teamwork.
Keywords: allied health assistant, workforce utilization, training & supervision, allied health professions, scope of practice, health system
Introduction
The Allied Health Assistant (AHA) workforce plays an increasingly important role in supporting the delivery of allied health services across the Australian healthcare system.1 AHAs work under the delegation and supervision of qualified allied health professionals (AHPs) to deliver care that enhances service capacity, accessibility, and efficiency.2 Following the 2007 development of the Certificate IV in Allied Health Assistance, a vocational qualification that provides specialized skills and knowledge, a significant body of research and policy development between 2010 and 2015 focused on strengthening the AHA workforce by clarifying training pathways, qualifications, and the parameters for supervision and delegation.3,4 Government-supported initiatives during this period helped define the value of the AHA role and contributed to a more consistent understanding of the AHA scope of practice across healthcare settings.4
Much of the foundational work to develop the assistant workforce focused on acute and subacute public health settings where most AHAs were employed. However, since then, there have been major structural reforms in the Australian health, aged care and disability services landscape. This has included the introduction of the National Disability Insurance Scheme (NDIS) in 2013 and changes to the aged care funding model,5 which have significantly altered service delivery models and workforce composition across settings.6 In the context of the NDIS, AHA roles have expanded within disability services; however, this expansion has occurred largely in the absence of a robust evidence base or clear policy guidance.1 Likewise, the integration of AHAs into mental health services remains under-explored. This is despite the potential for AHAs to support workforce sustainability, expand service delivery, improve access, enable AHPs to practice at full or extended scope, and to enhance care quality, job satisfaction and staff retention in this area.2,7
The growing complexity and ongoing reform activities across these sectors and the increasing use of the AHA workforce raises important questions regarding consistency in role definition, training quality, and delegation and supervision frameworks across sectors and allied health professions. Given this complexity, there is a clear need to synthesize current knowledge regarding the utilization of AHAs in the Australian context. This integrative review aims to examine how the AHA workforce is being utilized across various settings, disciplines, and sectors, with the goal of identifying current practices, gaps in the literature, and implications for workforce policy and service delivery.
Review Aims and Objectives
This review aimed to understand how the AHA workforce is being utilized within the Australian context.
The research objectives were to:
- Identify and describe research undertaken in relation to AHAs in the Australian context, considering the types of allied health professions working with AHAs, as well as the clinical and geographical settings represented.
- Identify and describe how research undertaken in relation to AHAs in the Australian context references government documents, policy, frameworks and training.
- Synthesize the key findings of research undertaken in relation to AHAs in the Australian context to identify gaps in the research, and implications for workforce policy and service delivery.
Methods
The research undertaken in relation to AHAs comprises diverse methodologies and is often focused on small sample sizes and/or one service setting. This, combined with the aim of the review being to appraise the evidence relating to utilization rather than to examine definitive outcome measures, led the authors to select the integrative review as the most appropriate approach.8,9 An integrative review provided the opportunity to present a thorough and holistic understanding of the utilization of AHAs in the Australian context, to provide a synthesis of the current body of knowledge and to identify gaps to guide future research in terms of theory, methodology, and practice.
An integrative review approach consists of five steps: problem identification, literature search, data evaluation (quality appraisal), data analysis and presentation of results.8
Problem Identification
A preliminary literature review was undertaken to identify key concepts and variables of interest. Subsequently, the research team convened to establish the review’s aims, guiding questions, and scope. The team comprised individuals with diverse expertise and experience related to the AHA workforce, including: a professional lead with a decade of experience working as an AHA; a member of the Board of Directors of the Allied Health Assistants’ National Association (AHANA); an occupational therapist working in a leadership position in mental health, justice health, and alcohol and drug services; a senior occupational therapist working within an outpatient rehabilitation setting; and an occupational therapy academic with clinical and research experience related to the AHA workforce.
Literature Search: Search Strategy
A comprehensive search strategy was developed in consultation with two research librarians to capture studies exploring the utilization of the AHA workforce in Australia. The identification of suitable search terms was an iterative process, informed by extant literature and previous reviews on AHAs that were reviewed during the problem identification phase.
Relevant keywords, search terms, and wildcard symbols were applied to each database (see Supplementary File 1 for the complete search strategy). Complete inclusion and exclusion criteria are described in Table 1.
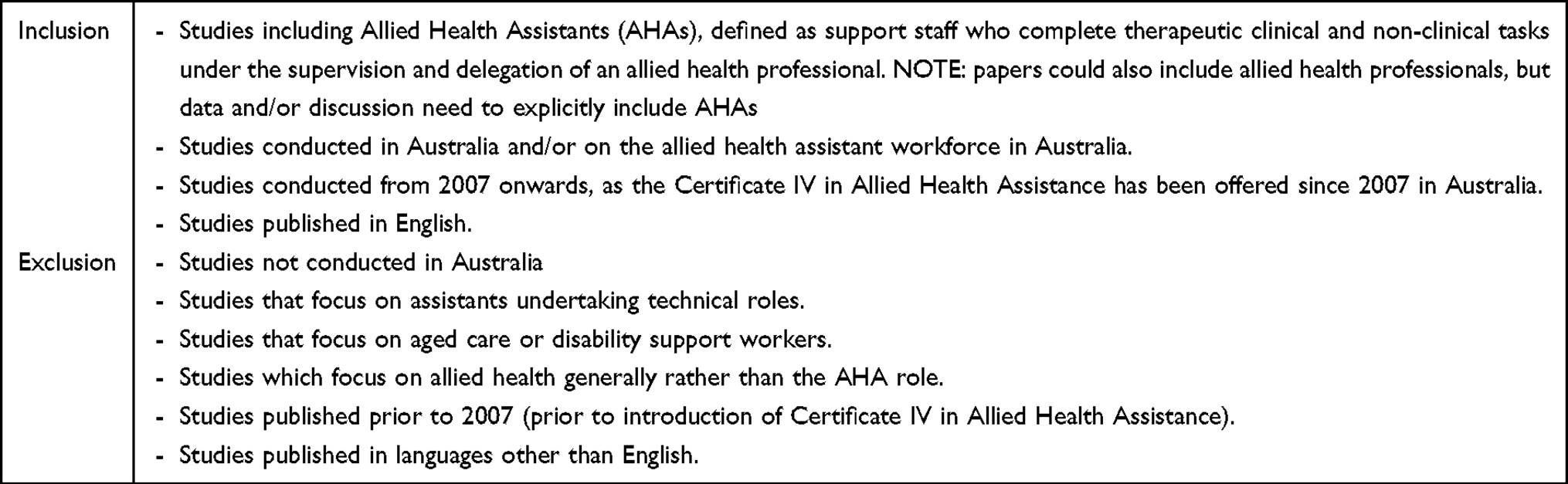 |
Table 1 Inclusion and Exclusion Criteria |
Appropriate studies published between January 2007—June 2025, were retrieved from MEDLINE, CINAHL, PsycINFO, SCOPUS, Web of Science Core Collection, and the Cochrane Central Register of Controlled Trials (CENTRAL). This timeframe was chosen to capture studies published after the Certificate IV in Allied Health Assistance became available in Australia. These were retrieved from Trove and ProQuest. A further search was undertaken using the Google Advanced Search function (see Supplementary File 2). This aimed to identify publicly available government documents relating to the allied health assistant workforce. An initial search primarily identified job advertisements, so further filters were applied to focus on government documents. This resulted in 18 documents. This search and identified documents are summarized in Supplementary File 2.
Screening
Three of the authors were involved in the screening process (CP, RP, RM) as listed in Figure 1. Two reviewers independently screened titles and abstracts based on the inclusion and exclusion criteria, with a third reviewer resolving any conflicts. This process was repeated with a full text screen. Articles focusing on medical, scientific, or technician assistant roles such as imaging assistants, dental assistants, pharmacy assistants, and laboratory technicians were excluded from this review due to the substantial differences in scope, training, and functional responsibilities compared to traditional allied health assistant roles which focus primarily on direct therapeutic interventions. Including scientific assistants would have introduced significant heterogeneity, limiting the relevance and applicability of findings to the allied health assistant workforce.
 |
Figure 1 PRISMA flow chart showing screening and selection process for Utilization of the allied health assistant workforce in the Australian context: an integrative review. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg. 2021;88,105,906. |
Two reviewers independently screened all articles using Covidence. Where discrepancies concerning the eligibility of an article occurred, a meeting was held to determine consensus. If consensus could not be reached, a third reviewer was consulted to make the final decision.
Quality Appraisal
The Quality Assessment for Diverse Studies (QuADS) tool was used independently by two of three authors (CP, RP, RM) to assess the methodological quality of included studies, due to its applicability across qualitative, quantitative, and mixed method studies.10 The maximum score that could be attributed for each category was 3 and there are 13 categories giving a maximum score of 39. Disagreements were resolved via discussion, or by a third author (RM). The QuADS tool was chosen due to its applicability to methodologically diverse studies and its focus on the theoretical underpinnings, clarity of aims, methodology, stakeholder involvement, and reported strengths and limitations. One reviewer was an author of an included article and was purposefully not assigned to appraise this study. Results were analyzed narratively, and no studies were discarded based on low scoring to maintain inclusivity and comprehensiveness, as suggested by Oermann and Knafl.11 The quality appraisal did not include the government documents.
Data Extraction and Analysis
To extract data from the peer reviewed literature, a data extraction table was developed by three reviewers (CP, RP, RM). This data extraction table was initially piloted by each reviewer on three studies selected at random and then further refined following discussion. For each of the included studies, key data were extracted into the data extraction table by one reviewer then checked by a second reviewer for accuracy. As summarized in Table 2, data extraction focused on the study design, as well as the allied health profession(s) represented, the clinical setting and geographical location. As this review aims to inform policy and practice, reference to government documents, policy, frameworks and training of AHAs was also noted.
 |
Table 2 Data Extraction Table |
Analysis of the article findings was structured using inductive content analysis to identify, organize, and interpret patterns and themes within the included literature findings. Content analysis is a suitable approach within an integrative review when including qualitative and mixed-methods data to maintain a balance between data-driven analysis and interpretive understanding.46 For this review, content analysis commenced following data extraction when articles were re-read by two independent reviewers, with a particular focus on the results, discussion and conclusion. Notes were made before the three reviewers met to discuss and summarize. This was followed by the generation of codes with subcategories47 as summarized in Table 3.
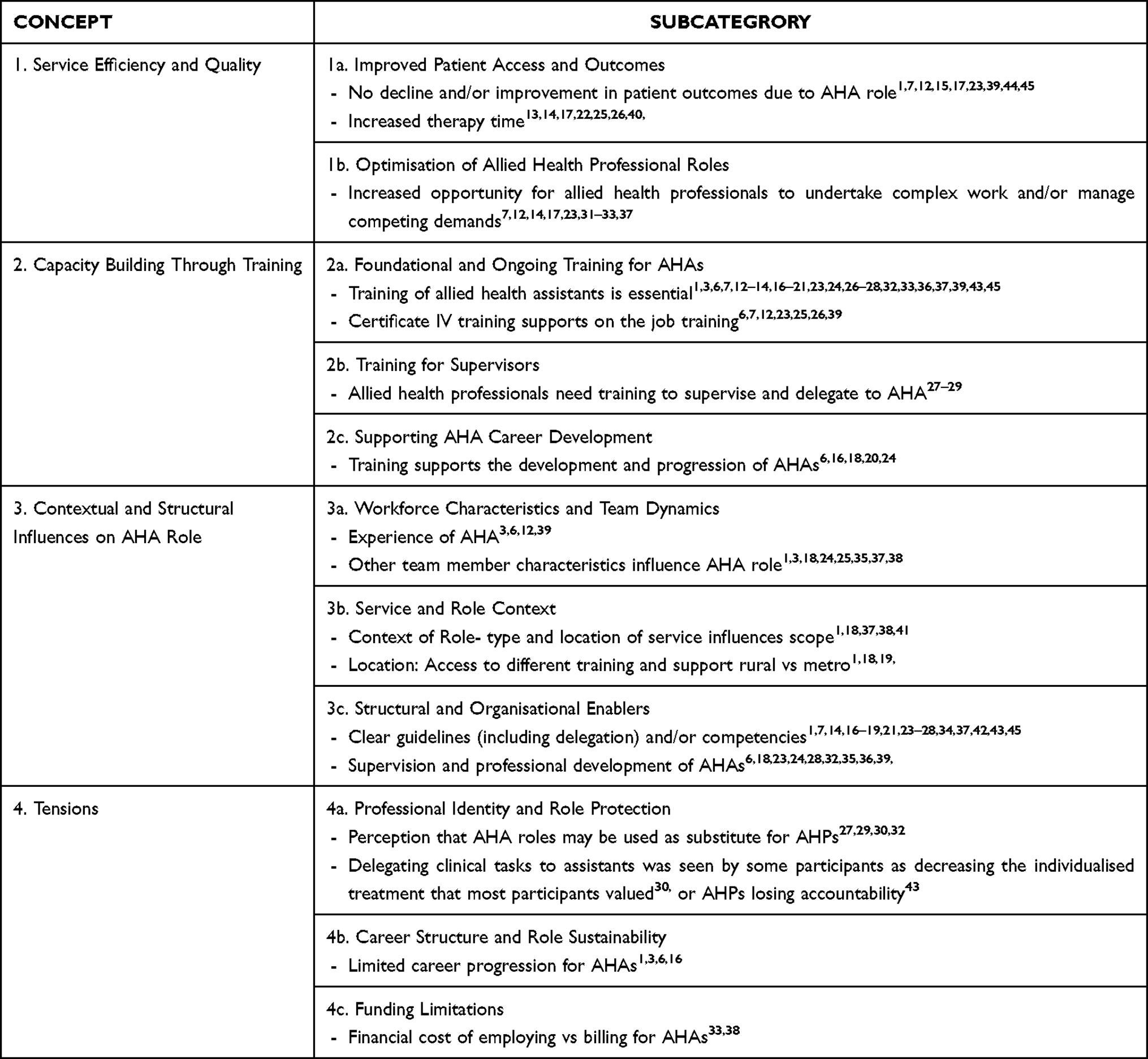 |
Table 3 Content Analysis |
For the government documents, a data extraction table was developed to summarize the core content of each document, as shown in Table 4. The coding framework created based on indicative content analysis of the empirical research was applied using deductive content analysis to the government documents.
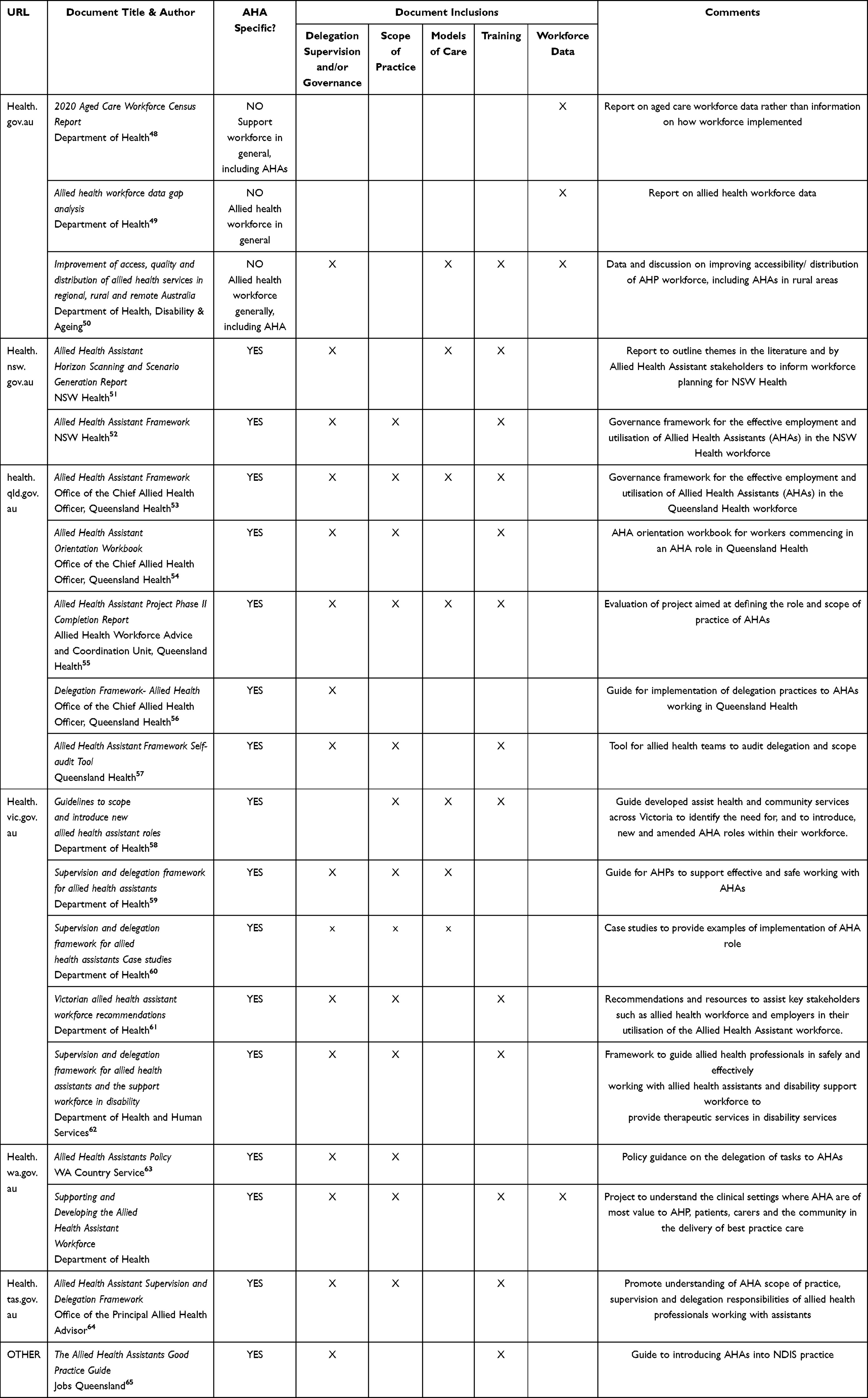 |
Table 4 Government Documents Data Extraction |
Results
Study Characteristics
The search identified 38 articles that met the inclusion criteria, as illustrated in Figure 1. Most articles reviewed took a qualitative (18/38) or mixed-methods (10/38) approach, with the remaining 10 consisting of nine quantitative studies and one literature review. Sample sizes ranged from interviews with small numbers of AHPs and AHAs from one profession or one team (n=21), to sampling large numbers of staff and/or patients across several health settings (n= 17). The clinical setting was predominantly public health care services, with only three explicitly including services external to public health care.1,6,33 Ten of the included studies included a focus on rural, remote, or regional settings.13,18,19,22,26,27,29–31,33,40,41
The search of government websites identified 19 documents. Three were generated by the federal Department of Health, so are explicable across all states and territories. The remaining 16 were from five state governments.
The allied health professions considered included occupational therapy, physiotherapy, speech and language therapy, dietetics, podiatry, social work and medical imaging. All states and territories were represented in the data, with the greatest volume of research undertaken in Queensland;12,14,18,26,31,34–37,42,43 Victoria;1,6,16,22,32,38–41 the Australian Capital Territory3,15,23–25 and New South Wales.20,27,29,30
Data Quality
The methodological and reporting quality of the included studies varied. The average overall QuADS score for the studies included in this review was 28.5 (range 12–34) out of a total possible score of 39 (based on a maximum score of 3 for each of the 13 criterion). Studies tended to score highest on the statement of research aim/s (mean of 2.6), research setting and target population (mean of 2.8), appropriate study design (mean of 2.6), description of data collection (mean of 2.4), and method of analysis criterion (mean of 2.5). The lowest scoring criterion at an average of 1.3 and 1.4, respectively, were “Justification for analytic method selected”; and “Evidence that the research stakeholders have been considered in research design or conduct”, indicating that there was typically limited justification for the method of analysis, and limited stakeholder involvement in the design or conduct of the studies. Articles with lower overall QuADS scores (ie Isbel et al (2014), Pearce & Pagett (2015), Phillips et al (2021) and Stute (2013)) commonly exhibited methodological limitations in relation to unclear sampling strategies, a lack of clarity regarding the appropriateness of the data collection and analytical methods employed to address the aims or outcomes of interest, and limited discussion of strengths or limitations. The full quality appraisal evaluations are presented in Table 5.
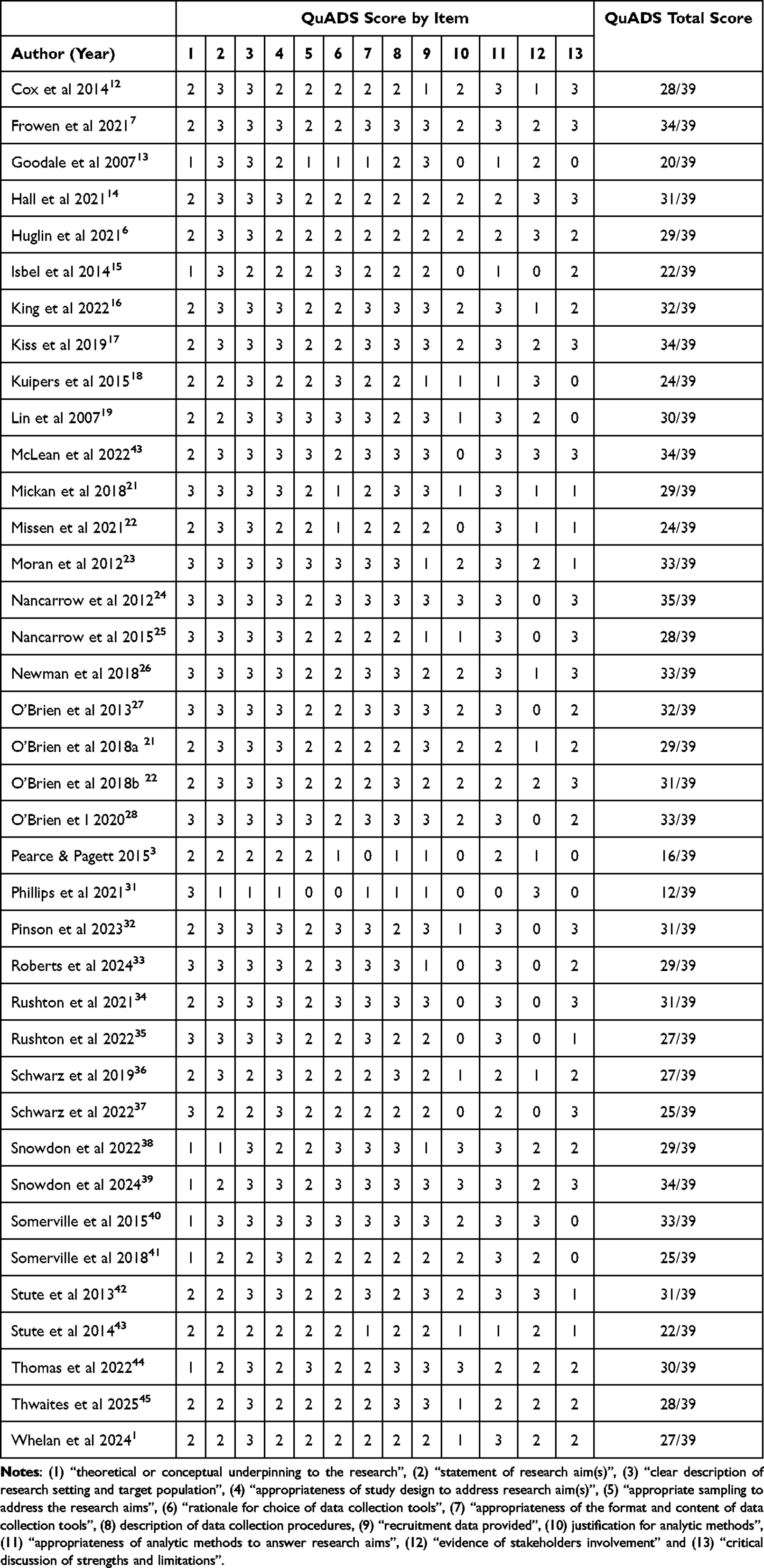 |
Table 5 Quality Appraisal of the Reviewed Studies Using the Quality Assessment for Diverse Studies Tool (QuADS) |
Content Analysis
A review of the study results and discussions identified four concepts that impact the utilization of AHAs in Australia. The concepts with subcategories are summarized in Table 3.
Concept 1: Service Efficiency and Quality
Most of the studies focused on the characteristics of the AHA workforce rather than the impact of the AHA role. Of those that did attempt to measure service efficiency and quality, all found a positive impact, both in terms of clinical outcomes not changing when compared to AHP delivered care,7,12,15,17,23,36,39,44,45 and access to therapy, with the availability of the AHA increasing overall therapy time.13,14,17,22,25,26,40 The AHA role may also provide an opportunity to free up allied health professional time to undertake more complex work and manage competing demands.7,12,14,17,22,25,26,40 One study highlighted a perception that AHAs would not lead to increased capacity for allied health professionals, due to the increased demands of training and supervising the AHAs.27 However, it is noted that this qualitative study was undertaken in a rural setting where the AHA role was more novel and included a small number of speech and language pathologists who, as a profession, were less represented in the studies.
The government documents, while acknowledging the value of AHAs, did not focus specifically on efficiency or quality, but rather on the pragmatics of incorporating the AHA role. Two of the documents which specifically considered workforce data, provided numbers of AHAs in relation to other professions48,49 but this does not necessarily support services to understand what the impacts are in relation to efficiency or quality.
Concept 2: Capacity Building Through Training
A significant proportion of the included studies identified training as a key concept. Fundamentally, there was a consensus that context-specific and ongoing training of AHAs is essential for the role to be safe and effective.1,3,6,7,12–14,16–21,23–28,32,33,36,37,39,43,45 As determined by the search parameters of this review, whilst all the studies were undertaken after the introduction of the Certificate III and IV in Allied Health Assistance, currently the only formal qualifications available for AHAs, only a small proportion of the studies explicitly referenced the training as being a tool to support, not replace, on the job training.6,7,12,23,25,26,39 The remaining studies did not explicitly identify if AHAs had or were required to have a Certificate IV. Training was framed as being both important for the safety and quality of service delivery, as well as supporting the development and career progression of AHAs.6,16,18,20,24 One study investigated the option of moving formal training from the vocational sector to the university sector but found that role-specific training delivered in the work setting was more impactful than formal training so this change was not warranted.21 Whilst many studies acknowledged supervision and delegation as being important to the success of the AHA role, only O’Brien et al’s27,28,30 work examining speech and language pathology assistant roles explicitly addressed training for supervisors of AHAs. With limited formal training in delegation and supervision skills AHPs often feel underprepared to supervise AHAs. Suggested actions include embedding supervision competencies into undergraduate curricula, ensuring structured support and clear role boundaries in workplace settings, and advocating for professional bodies to provide guidelines and training resources.
Of the 18 government documents identified, the majority addressed training to varying levels of detail including mentioning the Certificate IV in Allied Health Assistance,51–53,58–62,64–67 as well as highlighting the need for on the job and/or role specific training.
Concept 3: Contextual and Structural Influences on AHA Role
The generalizability of the studies included in this review are limited by factors including sample size and sample variance. However, there were common contextual and structural determinants which may inform the AHA role. Whilst the AHA role does not have a requirement for completion of compulsory training in the same way as allied health professionals, the experience of the AHA needs to be considered when determining how the role is utilized, including scope and degree of autonomy.3,6,12,39 Other team member characteristics, including their previous experience of supervision and delegation and attitude towards the AHA role also influence implementation.1,3,18,24,25,35,37,38 The type of service and location, particularly in terms of rural versus metropolitan also have an impact on both determining the scope of the AHA role1,18,37,38 and the access to training and support for the AHA,1,18,19,41 with studies considering AHAs working in rural or regional areas identifying reduced access to robust governance structures, on-site clinical supervision and formal training compared to their metropolitan counterparts.1,18,19,41
At a health service level, there are structural and organizational factors which when present, enable the successful implementation of the AHA role. These included clearly documented guidelines governing factors such as delegation and AHA competencies,1,7,14,16–19,21,23–28,34,37,42,43,45 as well as framing the processes for supervision of AHAs and recommendations for their ongoing professional development.6,18,23,24,28,32,35,36,39
This concept was a feature of all the government documents, the intent of which was to provide practical guidance regarding incorporating AHAs into a service. This included documents which focused on workforce data, with the intent of providing an overview of workforce size and configuration, so that gaps might be identified, along with opportunities to expand service offerings.48,49
Concept 4: Tensions
The AHA role is framed as one that can support health services to deliver increased frequency, volume and quality of care, while creating capacity for allied health professionals to deliver care specific to their scope of practice. However, there is tension between this potential for innovation and a perceived threat to the professional identity and role of the allied health professions. There continues to be a perception in some professions that AHAs will be employed to substitute, rather than support or complement, allied health professions.27,29,30,32 It is to be noted that these studies were conducted with allied health professions that have only more recently begun to incorporate the assistant role. It is important to consider the other factors which may impact on the successful implementation of an AHA role into a service including the impact of limited career progression for AHAs,1,3,6,16 which can lead to a high turnover of position holders, negating the important impact of AHA experience as highlighted in Concept 3.
As with all health and social care systems, finances need to be considered. This was not an element that was prominent within this review, which may reflect the limited research undertaken outside of the public health care system. In some areas of service delivery, particularly the National Disability Insurance Scheme (NDIS), the funding model presented challenges for employers in balancing cost-effective service provision through the utilization of AHAs with the need to generate sufficient billable hours to offset the costs of their employment and training.33,38 This concept was not a feature of the government documents which focused on services with block funding and considered the AHA role as being an opportunity to provide efficiencies within this funding model.
Discussion
The AHA role is well established within the Australian health and social care context, across a range of allied health professions.1,6 The role is aimed at implementing services based on the clinical reasoning of allied health professionals rather than delivering autonomous care.2 As such, it can be difficult to explicitly evidence specific clinical outcomes of AHA interventions. However, as demonstrated in the synthesis of evidence included in this review, it is possible to understand the positive contribution of AHAs to service efficiency, access and quality. Studies that broadly evaluated clinical outcomes and therapy access reported improvements in both domains,7,12,15,17,23,36,39,44,45 suggesting that AHAs enhance the capacity of health services to deliver timely and effective care. Importantly, the presence of AHAs was associated with increased therapy time and the ability of allied health professionals to focus on tasks specific to their scope of practice.13,14,17,22,25,26,40
Whilst the literature reveals a gap in robust outcome-focused research, it is important to consider the learnings that may be garnered from studies examining workforce characteristics and context factors. Training emerged as a critical enabler of safe and effective AHA practice, with services developing bespoke packages to allow for contextual factors such as AHA and supervisor experience, clinical setting and geographical location.12,17,25,36,43 While the Certificate III and IV in Allied Health Assistance provides a foundational qualification, the literature underscores the importance of ongoing, context-specific training to support role development and service quality. Notably, on-the-job training was frequently cited as more impactful than formal education alone. It was suggested that this was due to the existing qualification package not being fit for purpose but stemmed more from the breadth of settings and individualized role requirements for AHAs within these settings.
Despite the centrality of supervision and delegation to the successful implementation of the AHA role, few studies addressed the training needs of allied health professionals in supervisory relationships with AHAs. This may reflect the time frame and setting of most of the included studies, as public health care services have access to supervision and delegation policies and guidelines developed at a state level. However, with the expansion of the AHA role into services funded through the NDIS and ongoing aged care reforms, considering the skills of the delegating allied health professionals will be central to ensuring consistent and safe utilization of the AHA role across these settings. Whilst not specifically addressed within the literature, consideration needs to be given to incorporating supervision and delegation to AHAs as a competency for all entry level AHPs.
The four concepts identified in this review align with those proposed in a recent study looking at opportunities to promote the AHA workforce across all sectors in Victoria. This mixed-methods study proposed four interrelated factors- system, training, individual and workplace- as being the core contributing factors to the utilization of AHAs.6 Whilst not a core concept within this framework or within the literature, it is important to also continue to address any concerns raised in relation to professional identity and role boundaries. Some AHPs perceive AHAs as a threat to their scope of practice, particularly in disciplines where the assistant role is less frequently utilized.27,29,30,32 This tension may hinder the full realization of the AHA role’s benefits. Additionally, limited career progression opportunities for AHAs contribute to workforce instability, undermining the value of experience and continuity.
Despite many of the government documents identifying mental health as a practice area in which AHAs currently work, no studies were identified that examined the implementation of AHAs within mental health, justice health, or alcohol and drug services in the Australian context. This represents a significant gap in knowledge regarding how AHAs can be effectively utilized to provide safe and effective services within the mental health sector in Australia.
Similarly, though underexplored in the literature, financial considerations will also shape the development and utilization of AHAs, especially in emerging funding models such as the NDIS and changes implemented under the new Aged Care Act. Within the Australian landscape, these sectors provide vital services to support people to live well in the community, thereby reducing demand on already overstretched health services. To staff these services, as reflected in the National Allied Health Workforce Strategy,68 the various sectors will need to develop innovative models of care supported by staffing models that are safe, efficient and sustainable. Whilst definitive figures are not available, according to the Allied Health Assistant National Association, 50% of their members work in disability services.50
A recent scoping review69 aimed to understand the governance arrangements for therapy assistants and support workers within the disability sector, with a specific focus on rural and remote communities in Australia and internationally.69 Whilst acknowledging that it considered international settings and a broader workforce, it is of note that the review did draw similar conclusions, namely that training and supervision along with contextual factors impact the effectiveness of support roles within the disability sector.
The evidence elucidated through this review provides further guidance on how to ensure that the AHA workforce plays an effective part in the health and social care workforce. Whilst there is a dearth of published evidence in the mental health and disability sectors, there are opportunities to integrate the core elements identified through this review to support expansion of the AHA role into these sectors.
Strengths and Limitations
This review used a comprehensive search strategy involving seven academic databases, and searches for grey literature on government websites, and with input from two health research librarians.
This review primarily presented research and policy relating to public health care services. There may be AHA documentation available that is not publicly available but as this review only accessed published literature, not all areas of health and social care could be fully considered. The heterogeneous nature of the research methodologies and methods means this review cannot draw definitive conclusions but rather present a synthesis of the evidence. As the review was based on research and documents relating to the Australian context, generalizability to international settings may be limited.
Conclusion
This review underscores the factors that support the integration of the AHA role in the Australian health system. While the evidence points to clear benefits in terms of service efficiency, quality of care, and workforce capacity, the successful integration of AHAs depends on a range of interrelated factors. Effective training, supportive organizational structures, and context-specific implementation strategies are essential to maximize the value of the AHA role. To optimize the contribution of AHAs, policy and practice must address these identified enablers and barriers. This includes investing in training for both AHAs and their supervisors, developing flexible role descriptions that accommodate local needs, and fostering a culture that values the complementary nature of the AHA role. As the healthcare system continues to evolve, and new funding models are introduced, AHAs have the potential to play an increasingly vital role in delivering accessible, high-quality care. Expanding research into the cost-effectiveness and long-term outcomes of AHA integration, particularly within disability services, mental health and aged care, will be essential to inform sustainable workforce planning.
Author Contributions
All authors developed the study aims and method. RM conducted literature search. RM, CP and RP undertook article screening, quality appraisal and data extraction. CP undertook data analysis in consultation with RM and RP. CP drafted introduction, results and discussion. All authors contributed to final version of manuscript, contributing to introduction, results, discussion and conclusion and approved final version for submission.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Whelan L, McLean S, Edwards A, king J, Farlie MK. The evaluation of health, disability and aged care-sector engagement with resources designed to support optimisation of the allied health assistant workforce: a qualitative study. BMC Health Serv Res. 2024;24(1):848. doi:10.1186/s12913-024-11253-z
2. Lizarondo L, Saravana K, Lisa H, Skidmore D. Allied health assistants and what they do: a systematic review of the literature. J Multidisciplinary Healthcare. 2010;3(null):143–153. doi:10.2147/JMDH.S12106
3. Pearce C, Pagett L. Advanced allied health assistants: an emerging workforce. Aust Health Rev. 2015;39(3):260. doi:10.1071/AH14253
4. Victorian Department of Health. Supervision and delegation framework for allied health assistants and the support workforce in disability. Melbourne: 2018.
5. Department of Health Disability and Ageing. About the Support at Home Program 2025. Available from: https://www.health.gov.au/our-work/support-at-home/about.
6. Huglin J, Whelan L, McLean S, et al. Exploring utilisation of the allied health assistant workforce in the Victorian health, aged care and disability sectors. BMC Health Serv Res. 2021;21(1). doi:10.1186/s12913-021-07171-z
7. Frowen J, Hughes R, Kiss N. Introduction of a speech-language pathology assistant role for swallow screening in a head and neck radiotherapy clinic. Int J Speech Lang Pathol. 2021;23(4):441–451. doi:10.1080/17549507.2020.1800818
8. Whittemore R, Knafl K. The integrative review: updated methodology. J Adv Nurs. 2005;52(5):546–553. doi:10.1111/j.1365-2648.2005.03621.x
9. Toronto CE. Overview of the integrative review. In: Toronto CE, Remington R, editors. A Step-by-Step Guide to Conducting an Integrative Review.
10. Harrison R, Jones B, Gardner P, Lawton R. Quality assessment with diverse studies (QuADS): an appraisal tool for methodological and reporting quality in systematic reviews of mixed- or multi-method studies. BMC Health Serv Res. 2021;21(1):144. doi:10.1186/s12913-021-06122-y
11. Oermann MH, Knafl KA. Strategies for completing a successful integrative review. Nurse Author Ed. 2021;31:65–68. doi:10.1111/nae2.30
12. Cox RJ, Mills VJ, Fleming J, Nalder E. Implementation of an advanced occupational therapy assistant‐led groups programme in aged care rehabilitation. Austr Occup Ther J. 2014;61(3):187–193. doi:10.1111/1440-1630.12105
13. Goodale BJ, Spitz S, Beattie NJ, Lin IB. Training rural and remote therapy assistants in Western Australia. Rural Remote Health. 2007;7(3):774.
14. Hall K, Maxwell L, Cobb R, et al. Physiotherapy service provision in a specialist adult cystic fibrosis service: a pre-post design study with the inclusion of an allied health assistant. Chron Respir Dis. 2021;18:14799731211017895. doi:10.1177/14799731211017895
15. Isbel S, Pearce C, Kohlhagen L. An allied health assistant helps reduce difficulties faced by older people when returning home from hospital. Asia Pacific J Health Manag. 2014;9(2):59–65.
16. King OA, Pinson JA, Dennett A, Williams C, Davis A, Snowdon DA. Allied health assistants’ perspectives of their role in healthcare settings: a qualitative study. Health Soc Care Community. 2022;30. doi:10.1111/hsc.13874
17. Kiss N, Gilliland S, Quinn P, Atkins L, Black J, Frowen J. Evaluating the effectiveness of a nutrition assistant role in a head and neck cancer clinic. Nutr Diet. 2019;76(1):21–27. doi:10.1111/1747-0080.12462
18. Kuipers P, Hurwood A, McBride LJ. Audit of allied health assistant roles: suggestions for improving quality in rural settings. Aust J Rural Health. 2015;23(3):185–188. doi:10.1111/ajr.12161
19. Lin I, Goodale B, Villanueva K, Spitz S. Supporting an emerging workforce: characteristics of rural and remote therapy assistants in Western Australia. Aust J Rural Health. 2007;15(5):334–339. doi:10.1111/j.1440-1584.2007.00917.x
20. McLean C, Turner N, Dragicevich H, Lee C, Desmares-Matters M. Evaluation of a structured nutrition competence program for dietitian assistants. J Allied Health. 2022;51(1):38–42.
21. Mickan S, Golenko X, Buys N. Educational needs and workplace opportunities of allied health assistants: a qualitative pilot. Focus Health Prof Educ. 2018;19(3):52. doi:10.11157/fohpe.v19i3.251
22. Missen K, Mills A, McDonald G, Di Corleto E, Telling L, Davey A. Evaluation of an assessment model to reduce waitlist times for occupational therapy in a rural community health setting. Aust J Rural Health. 2021;29(6):987–992. doi:10.1111/ajr.12806
23. Moran AM, Nancarrow SA, Wiseman L, et al. Assisting role redesign: a qualitative evaluation of the implementation of a podiatry assistant role to a community health setting utilising a traineeship approach. J Foot Ankle Res. 2012;5(1). doi:10.1186/1757-1146-5-30
24. Nancarrow S, Moran A, Wiseman L, Pighills AC, Murphy K. Assessing the implementation process and outcomes of newly introduced assistant roles: a qualitative study to examine the utility of the Calderdale Framework as an appraisal tool. J Multidisciplinary Healthcare. 2012;5:307–317. doi:10.2147/JMDH.S35493
25. Nancarrow SA, Moran A, Sullivan R. Mechanisms for the effective implementation of an allied health assistant trainee: a qualitative study of a speech language pathology assistant. Aust Health Rev. 2015;39(1):101–108. doi:10.1071/AH14053
26. Newman CS, Cornwell PL, Young AM, Ward EC, McErlain AL. Accuracy and confidence of allied health assistants administering the subjective global assessment on inpatients in a rural setting: a preliminary feasibility study. Nutr Diet. 2018;75(1):129–136. doi:10.1111/1747-0080.12370
27. O’Brien R, Byrne N, Mitchell R, Ferguson A. Rural speech-language pathologists’ perceptions of working with allied health assistants. Int J Speech-Lang Pathol. 2013;15(6):613–622. doi:10.3109/17549507.2012.759623
28. O’Brien R, Mitchell R, Byrne N. What value can allied health assistants bring to speech-language pathology practice? J Clin Pract Speech. 2020;22(1):29–33. doi:10.1080/22087168.2020.12370281
29. O’Brien R, Mitchell R, Byrne N. The role of speech-language pathology professional identity in response to workforce redesign. J Clin Pract Speech. 2018;20(2):50–56.
30. O’Brien R, Mitchell R, Byrne N. Paradoxical perceptions towards the introduction of assistants in speech‐language pathology and potential impact on consumers. Scand J Caring Sci. 2018;32(1):117–127. doi:10.1111/scs.12437
31. Phillips D, Matheson L, Pain T, Kingston GA. Development of an occupational-therapy-led paediatric burn telehealth review clinic. Rural Remote Health. 2021;21(3). doi:10.22605/RRH6223
32. Pinson J-A, King OA, Dennett AM, Davis A, Williams CM, Snowdon DA. Exploring the role of medical imaging assistants in Australian medical imaging departments: a mixed-methods study. J Med Radiation Sci. 2023;70(1):46–55. doi:10.1002/jmrs.623
33. Roberts L, Staley B, Callanan J, Logan K. Building the private practice workforce in the Northern Territory: barriers and facilitators for implementation of the allied health assistant role. Austr J Rural Health. 2024;32(6):1173–1184. doi:10.1111/ajr.13187
34. Rushton A, Young A, Keller H, Bauer J, Bell J. Delegation opportunities for malnutrition care activities to dietitian assistants—findings of a multi-site survey. Healthcare. 2021;9(4):446. doi:10.3390/healthcare9040446
35. Rushton A, Bauer J, Young A, Keller H, Bell J. Barriers and enablers to delegating malnutrition care activities to dietitian assistants. Nutrients. 2022;14(5):1037.
36. Schwarz M, Ward EC, Cornwell P, Coccetti A, Kalapac N. Evaluating the feasibility and validity of using trained allied health assistants to assist in mealtime monitoring of dysphagic patients. Dysphagia. 2019;34(3):350–359. doi:10.1007/s00455-018-9947-y
37. Schwarz M, Ward EC, Cornwell P, Coccetti A. Dysphagia screening using an allied health assistant delegation model: service considerations for implementation. Disability Rehabil. 2022;44(8):1275–1283. doi:10.1080/09638288.2020.1800109
38. Snowdon DA, King OA, Dennett A, et al. Delegation of patient related tasks to allied health assistants: a time motion study. BMC Health Serv Res. 2022;22(1):1–8. doi:10.1186/s12913-022-08642-7
39. Snowdon DA, Vincent P, Callisaya ML, et al. Allied health assistant management of people with Hip fracture is feasible and may improve patient adherence to hip fracture mobilisation guidelines: a feasibility randomised controlled trial. Physiotherapy. 2024;124:51–64. doi:10.1016/j.physio.2024.05.002
40. Somerville L, Davis A, Elliott AL, Terrill D, Austin N, Philip K. Building allied health workforce capacity: a strategic approach to workforce innovation. Aust Health Rev. 2015;39(3):264–270. doi:10.1071/AH14211
41. Somerville L, Davis A, Milne S, Terrill D, Philip K. Exploration of an allied health workforce redesign model: quantifying the work of allied health assistants in a community workforce. Aust Health Rev. 2018;42(4):469–474. doi:10.1071/AH16266
42. Stute M, Hurwood A, Hulcombe J, Kuipers P. Defining the role and scope of practice of allied health assistants within Queensland public health services. Aust Health Rev. 2013;37(5):602–606. doi:10.1071/AH13042
43. Stute M, Hurwood A, Hulcombe J, Kuipers P. Pilot implementation of allied health assistant roles within publicly funded health services in Queensland, Australia: results of a workplace audit. BMC Health Serv Res. 2014;14(1):258. doi:10.1186/1472-6963-14-258
44. Thomas J, Lawless C, Christie A, Kuhr O, Miller M. In patients admitted to a home rehabilitation service, is remote completion of the patient-generated subjective global assessment physical examination using still images captured by allied health assistants a valid alternative to an in-person physical examination? J Acad Nutr Diet. 2022;122(12):2320–2329.
45. Thwaites C, Shaw L, Lui R, et al. Boosting hospital falls prevention using health assistant staff alongside usual care. Patient Educ Couns. 2025;130:108464. doi:10.1016/j.pec.2024.108464
46. Dwyer PA. Analysis and synthesis. In: Toronto CE, Remington R, editors. A Step-by-Step Guide to Conducting an Integrative Review.
47. Cameron J, Roxburgh M, Taylor J, Lauder W. An integrative literature review of student retention in programmes of nursing and midwifery education: why do students stay? J Clin Nurs. 2011;20(9–10):1372–1382. doi:10.1111/j.1365-2702.2010.03336.x
48. Australian Government. 2020 Aged Care Workforce Census Report. Department of Health, editor. 2023.
49. Australian Government. Allied Health Workforce Data Gap Analysis. Department of Health, editor. Sydney, NSW; 2022.
50. Allied Health Assistant National Association. AHANA’s Feedback on the Draft National Allied Health Workforce Strategy. 2025.
51. NSW Government. Allied Health Assistant Horizon Scanning and Scenario Generation Report. NSW Ministry of Health, editor. 2022.
52. NSW Government. Allied Health Assistant Framework. Workforce Planning and Talent Development, editor. 2020.
53. Office of the Chief Allied Health Officer. Allied Health Assistant Framework. Queensland Health, editor. Brisbane; 2022.
54. Office of the Chief Allied Health Officer. Allied Health Assistant Orientation Workbook. Queensland Health, editor. Brisbane; 2022.
55. Allied Health Workforce Advice and Coordination Unit. Allied Health Assistant Project Phase II Completion Report. Q. Health, editor. Brisbane;2008
56. Office of the Chief Allied Health Officer. Delegation Framework Allied Health Assistant. Clinical Excellence Queensland, editor. 2022.
57. Queensland Health. Allied Health Assistant Framework Self-Audit Tool. Queensland Government, editor. 2022.
58. Alfred Health. Guidelines to Scope and Introduce New Allied Health Assistant Roles. Victoria Department of Health, editor. 2012.
59. Victorian Department of Health. Supervision and Delegation Framework for Allied Health Assistants. Government V, editor. Melbourne;2023.
60. Victorian Department of Health. Supervision and Delegation Framework for Allied Health Assistants. Case Studies. Government V, editor. 2012.
61. Victorian Department of Health. Victorian Allied Health Assistant Workforce Recommendations. Victorian Government, editor. 2023.
62. Department of Health and Human Services. Supervision and Delegation Framework for Allied Health Assistants and the Support Workforce in Disability. Victoria State Government, editor.. 2018.
63. WA Country Health Service. Allied Health Assistants Policy. Government of Western Australia, editor. 2020.
64. Office of the Chief Health Professions Office. Supporting and Developing the Allied Health Assistant Workforce. In: Western Australia Department of Health, editor. 2015.
65. Workability Qld. The Allied HealthAssistants Good Practice Guide. An evidence-based guide for employers on introducing Allied Health Assistants to deliver quality NDIS services. 2022.
66. Allied Health Workforce Advice and Coordination Unit. Allied Health Assistant Project Phase II Completion Report. Health Q. editor. Brisbanen;2011.
67. Chief Nurse and Allied Health Principal Allied Health Adviser. Allied Health Assistant Supervision and Delegation Framework. Tasmanian Department of Health and Human Services, editor. 2012.
68. Department of Health Disability and Ageing. National Allied Health Workforce Strategy: australian Government. 2025. Available from: https://www.health.gov.au/our-work/national-allied-health-workforce-strategy.
69. Moran A, Bulkeley K, Johnsson G, Tam E, Maloney C. Models of governance of disability therapy support workers in rural and remote settings: a systematic scoping review. Int J Environ Res Public Health. 2024;21(6):693. doi:10.3390/ijerph21060693
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.