")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Implementation of the Admission Process of Patients Under the Public Crisis Situation of COVID-19 Pandemic: A Real-World Case Study
Authors Zhang X , Yang Z , Chen J , Zhang C , Zhang J
Received 4 April 2023
Accepted for publication 3 July 2023
Published 11 July 2023 Volume 2023:16 Pages 1905—1914
DOI https://doi.org/10.2147/JMDH.S415678
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Xiaohong Zhang,1 Ziyan Yang,2 Jiaqi Chen,1 Cuiling Zhang,3 Junyan Zhang4
1Nursing Department, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China; 2College of Nursing, Shanxi Medical University, Taiyuan, People’s Republic of China; 3Department of Digestive Oncology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China; 4Department of Clinical Epidemiology and Evidence-based Medicine, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, Taiyuan, People’s Republic of China
Correspondence: Cuiling Zhang, Department of Digestive Oncology, Shanxi Bethune Hospital, Shanxi Academy of Medical Sciences, Tongji Shanxi Hospital, Third Hospital of Shanxi Medical University, NO. 99, Longcheng Street, Xiaodian District, Taiyuan, 030032, People’s Republic of China, Tel +86-13753482546, Email [email protected]
Purpose: To clarify the implementation of the admission process under the public crisis of COVID-19 pandemic.
Methods: A real-world study was conducted to collect data on the normal and public crisis situations at a tertiary hospital in China and understand the views of 18 head nurses on the necessity of the admission process in public crisis situations. Independent t-test and chi-square test were used to analyze the work data in two situations; Spearman correlation analysis was performed to determine the correlation of work data with two situations of process implementation, and differences between the head nurses’ views of necessity of the admission process and actual implementation under public crisis situations were analyzed.
Results: Significant differences were observed in the working data between the normal and public crisis situations (P < 0.05), and the implementation of the admission process was not in place. The number of nurses on duty was positively correlated with each item of admission process (P < 0.05), the rest of work data were negatively correlated with each item in the admission process (P < 0.05), and there was a significant difference between the necessity of each item in the admission process and the actual implementation results (P < 0.05).
Conclusion: Public crisis leads to the lack of implementation of admission process, and the original admission process and quality control standards are not applicable during the public crisis situation.
Keywords: public crisis, COVID-19 infection, admission process, nursing management, process reengineering, real-world study
Introduction
In December, 2022, China’s State Council issued the “Notice on Further Optimizing the Implementation of Prevention and Control Measures for COVID-19 epidemic Situation” to accelerate the restoration of normal social activities.1 The National Health Commission renamed novel coronavirus pneumonia as COVID-19 infection.2 Since the beginning of December 2022, the focus of epidemic prevention and control in China has shifted from “preventing infection” to “preventing severe disease, reducing death, and ensuring health”.2 Under such condition, the number of patients admitted to Shanxi Bethune Hospital, China, because of COVID-19 infection has increased sharply; the number of beds in the respiratory medicine department cannot meet the needs of inpatients, and the whole hospital has begun to admit patients with COVID-19 infection across specialties. Medical staff are extensively infected at the same time, and the highest number of people who cannot come for work in a single day is 50%. Therefore, there is a serious shortage of nursing staff. Therefore, how to ensure effective treatment for every hospitalized patient is a challenge being faced by every nursing manager.
The patient admission process which is the first process after the patient is hospitalized3 refers to a series of orderly work steps that patients need to complete before entering the medical institution for hospitalization.3 It starts with the patient entering the ward4 and has an important position in hospital management. In 2015, China proposed the” On Further Deepening Quality Care and Improving Nursing Services, which aims to standardize nursing behavior and promote the development of quality care.4 Specifically, it standardized patient admission processes to improve the appearance of nursing services and meet patients’ needs in hospital; subsequently, it has developed into a guiding regulation to be implemented by hospitals.4
The public crisis situation refers to the situation of emergency encountered in the public sphere, including earthquake, hurricane, flood, SARS, and COVID-19 pandemic.5–9 Its outbreak will affect the process specification that was originally being followed, interfere with normal work and life, and heavily affected healthcare systems.10 An increasing number of people getting infected with COVID-19 is also a public crisis event.11 Since early December 2022, the number of infected patients in the whole society has been increasing, with the increase being 16 times compared with the control period and the infection rate among medical staff is as high as 70%.12 A large number of nurses in our hospital are unable to work, resulting in newly admitted patients not being treated in a timely manner after admission. Studies have reported that in the situation of public crisis, various factors will cause failure in implementing the original work processes, which need to be optimized, and the evaluation criteria need to be updated.13–18 However, no similar research on the implementation of workflow and quality control standards is available in view of the current public crisis.
Real-world study (RWS)19 is a research method that uses the data in real medical world to reflect the actual situation. This ensures that researchers can understand the implementation of standards and norms in the real medical process, and the research evidence is more practical and reliable. RWS can be used to evaluate the accessibility of patients’ clinical treatment and treatment compliance.20 Moreover, it can determine problems such as inadequate medical-care services and rare adverse effects discovery21 to provide a basis for further implementation of medical and health guidelines, policies, standards, and norms.
Therefore, in this paper, we analyzed relevant data to conduct real-world research. The objectives of this study were as follows: 1. To understand the implementation of the admission process of patients with COVID-19, which is a part of cross-professional centralized treatment in our hospital under the public crisis situation of COVID-19 infection; 2. To clarify whether the standardized admission process in our hospital is suitable for this public crisis and its influencing factors. 3. To understand whether the quality evaluation standard of our hospital for standardized admission process is suitable for this public crisis. This study is expected to provide reference for the optimization of admission process of patients with COVID-19 and for the standardized management of other public crisis events.
Research Data and Methods
Data
Since early December 2022, patients with new coronavirus infections have been admitted to the respiratory medicine department. With the sudden increase in the number of coronavirus cases, beds in the respiratory medicine department can no longer meet the clinical requirements. Consequently, the hospital has decided to coordinate medical resources and arrange other internal medicine departments for admission and treatment. Therefore, this study included 16 wards of Shanxi Bethune Hospital of China that did not admit patients with the first diagnosis of pneumonia under normal conditions but intensively admitted patients with COVID-19 infection from December 2022. Of the 16 wards, 8, 3, 1, 1, 1, and 2 were oncology, neurology, rheumatology and immunology, nephrology, gastroenterology, and endocrinology departments, respectively. The research data were derived from the inpatient working day report, nursing staff schedule, electronic medical record system, and nursing quality control system of Shanxi Bethune Hospital, China. The data obtained from the working day report include the total number of inpatients, daily admitted patients, and critically ill patients. The data obtained from the nursing staff schedule include the number of nurses on duty and the number of nurses on duty with illness. The data obtained by the electronic medical record system include the number of long-term and temporary medical orders at the time of admission. The data obtained by the nursing quality control system include the implementation rate of the admission process.
Methods
Data Retrieval and Collation
This study uses data from real medical work to analyze actual consultations and patient conditions under real conditions to better understand the implementation of standard norms in real medical processes and obtain authentic and reliable evidence.22,23 Real world data were retrieval from the inpatient working day report, nursing staff schedule, electronic medical record system, and nursing quality control system in Shanxi Bethune Hospital: the inpatient working day report was obtained from the medical office, the nursing staff schedule and nursing quality control system data were obtained from the nursing department, and the electronic medical record system data were obtained from the patient case room. Data from September 19, 2022, to September 25, 2022 were collected as the data under normal situation, whereas those from December 29, 2022, to January 4, 2023, were used as the data in the situation of public crisis. The data were organized using Excel 2021. Summed the everyday total number of inpatients, critical patients, daily admitted patients, all nurses on duty, sick nurses on duty, long-term medical orders at the time of admission, and temporary medical orders at the time of admission in six departments under these two situations to prepare for the next analysis.
Questionnaires
Data collection was performed using the Questionnaire Star tool, which is an electronic questionnaire collection tool commonly used in China; this tool is operated online and facilitates quick data collection. The standardized admission process in “Further Deepening Quality Nursing and Improving Nursing Service” was made into a quiz star to understand the necessity of implementing each item of the admission process of 18 head nurses in 16 wards under the public crisis situation. The process includes six dimensions: special person reception, admission introduction, admission evaluation, hygiene and cleanliness, psychological support, and timely treatment and is evaluated in terms of whether it is necessary or unnecessary. For details about the questionnaire, please see the Appendix. The questionnaire survey was anonymously conducted, and the purpose and significance of the study were explained to the head nurses in detail before the survey. The subjects could withdraw at any time. If the questionnaire was completed and submitted, it was regarded as the subject’s informed consent to participate in the study.
Statistical Analysis
Most of the clinical work reports and database data are recorded by Excel. Therefore, we used Excel 2021 for preliminary data collation and accounting the data, and SPSS26.0 was used for statistical analysis. The general information of the departments conformed to the normal distribution by Shapiro–Wilk test and are expressed as the mean ± SD. Two independent samples t-test was used to compare the two groups, and the Mann–Whitney U-test was used to test the robustness of the results against departures from normality. The implementation of the admission process in two states were expressed as the number of cases and percentages, and chi-square test was used for comparison between the groups. When all expected counts (expected cell frequencies 100.0%) were >5, Pearson’s chi-square test was used. With at least one expected count (expected cell frequencies ≥ 25.0%) < 5 but > 1, continuity correction was used. For the minimum expected count of <1, Fisher’s exact probability method was used. Spearman correlation analysis was conducted between the statistically considerable variables in the general data and implementing each item in the admission process under the two situations, and the correlation coefficient was used to assess the degree of correlation between the items. The correlation coefficients (r) < 0 and > 0 indicated negative and positive correlations, respectively, and 95% confidence intervals were used to estimate the overall parameter truthfulness. The implementation of each item in the admission process was tested for discrepancies with the survey results of the head nurses’ views of necessity for implementation. A P value < 0.05 was considered significant. Part of the data for this study was obtained from the hospital database and daily work data, which was recorded in detail; the data were complete and accurate. The other part was obtained from the questionnaire and checked at the end, thereby ensuring that there were no outliers or missing values.
Results
General Information
Table 1 presents the independent samples t-test results for general information of the 16 wards. Between the normal and public crisis situations, no considerable difference was observed in terms of the total number of hospitalized patients and patients admitted daily. However, the number of critically ill patients, all nurses on the job, sick nurses on the job, long-term medical orders at the time of admission, and temporary medical orders at the time of admission were all compared at P < 0.001, and the difference was statistically significant at the test level ɑ = 0.05. Table 2 shows the results of the comparison using the Mann–Whitney U-test. The number of critically ill patients, the total number of nurses on duty, the number of nurses on duty with illness, the number of long-term medical orders at the time of admission, and the number of temporary medical orders at the time of admission in two states were compared at P < 0.05. The results were consistent with those of the two independent samples t-test, indicating that the public crisis state led to a upward trend in the number of critically ill patients, the number of long-term medical orders at the time of admission, the number of nurses on duty with illness, and the number of temporary medical orders at the time of admission and downward in the number of nurses in duty.
 |
Table 1 Comparison of General Information of Departments Under the Normal and Public Crisis Situations |
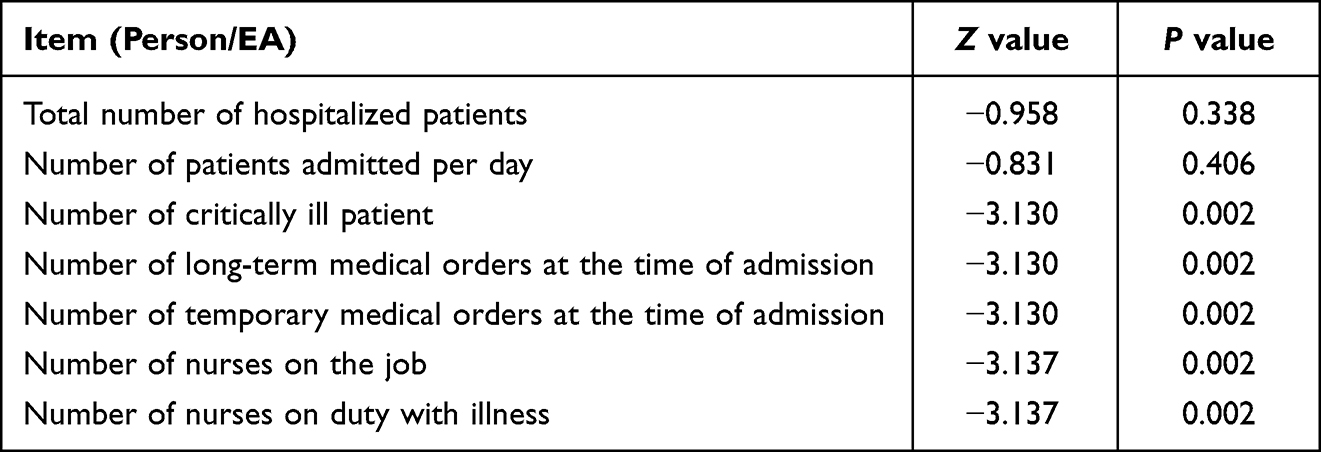 |
Table 2 U-Test of General Data of Departments in Two States |
Necessity of the Implementation of Each Item of Admission Process Under the Public Crisis Situation
The results of the survey of 18 head nurses in 16 wards on the necessity of implementing each item of the admission process under public crisis situation are shown in Table 3. Among them, the necessity of timely treatment was 94.4%, and the necessity of admission evaluation was 88.9%, indicating that timely treatment and admission evaluation were of high importance, and priority should be given in public crisis situations.
 |
Table 3 The Necessity of the Implementation of Each Item in Admission Process |
Analysis of the Implementation of Admission Process
Comparison of the Implementation of Admission Process Under the Two Situations
Table 4 shows the implementation rate of each item in the admission process in the normal state and the public crisis state. According to the Chi-square test, the implementation rates of special person reception, admission introduction, admission evaluation, hygiene and cleanliness, psychological support, and timely treatment differed significantly between the two states (all P value < 0.05). It shows that the implementation rate of the items in the public crisis state is significantly lower than that in the normal state, with the actual implementation rate of hygienic and cleanliness being only 1.5%, and the admission process in the public crisis state is poorly implemented.
 |
Table 4 The Implementation of Admission Process Under the Two Situations |
Correlation Analysis of Implementing Each Item in Admission Process and General Data
Table 5 depicts the correlations for the implementation of each item in admission process under the two situations and statistically considerable general data and 95% confidence intervals. Spearman correlation analysis showed that the number of critically ill patients, nurses on duty with illness, and long-term and temporary medical orders at the time of admission were negatively correlated with each item in the admission process. However, the number of nurses on duty was positively correlated with each item. It can be inferred that in the public crisis state, the number of critically ill patients, the number of nurses on duty with illness, the number of long-term medical orders at the time of admission, and the number of temporary medical orders at the time of admission will lead to poor implementation of the admission process, whereas the increase in the number of nurses on duty will promote the implementation of the admission process.
 |
Table 5 Correlation Analysis Between Each Item in Admission Process and General Data |
Difference Test Between the Head Nurse’s Opinions on the Necessity of Each Item in the Admission Process Under the Public Crisis Situation and Actual Implementation
Table 6 shows the difference between the head nurse’s opinion on the necessity of the six items of admission process under the public crisis situation and actual implementation. It was statistically significant, with all P values < 0.05. It shows that the head nurse’s opinion on the necessity of each item of admission process is inconsistent with the actual implementation, and the public crisis state has a greater impact on the implementation of the admission process.
 |
Table 6 Difference in the Head Nurse’s Opinion on the Necessity of Admission Process and Actual Implementation |
Discussion
The Standard Patient Admission Process is Not in Place Under Public Crisis Situation of COVID-19 Infection
The implementation rate of each item in the admission process of patients with COVID-19 was clearly lower than that under the normal situation (Table 4). It is suggested that the admission process is not properly implemented in the public crisis situation. For example, the implementation rate of special person reception is 100% in the normal situation but only 7.7% in the public crisis situation. The correlation analysis (Table 5) revealed that the inadequate implementation of the admission process was positively related to the increase in the number of critically ill patients, nurses on the job with illness, and long-term and temporary medical orders at the time of admission but negatively related to the decrease in the number of all nurses on the job. In “On Further Deepening Quality Nursing and Improving Nursing Service”, the admission process is standardized, which includes six items: special person reception, admission introduction, admission evaluation, hygiene and cleanliness, psychological support, and timely treatment.4 Although the implementation rate of “timely treatment” was the highest under public crisis, it was only 65.4%, and the lowest implementation rate was for “hygiene and cleanliness” (1.5%). This indicated that under the public crisis situation, many factors affect the implementation rate of admission process. This finding is consistent with that of the study by Houghton.15 Nurses are professionals who have the most frequent contact with patients. Assessment of their reasonable workflow is related to patients’ condition after treatment and satisfaction with the medical process, so if there is any carelessness, patients’ medical experience will be poor.24 In this public crisis of COVID-19 infection, although the total number of hospitalized patients and those admitted daily were not considerably different compared with those under the normal situation, the number of critically ill patients was high, which increased the nurses’ workload related to their treatment and care. However, the number of nurses on the job would decrease, and the nurses with illness would be unable to work under the condition of incomplete recovery. This may lead to the inadequate implementation of the admission process. Therefore, nursing managers at all levels should not only pay attention to the implementation rate but also consider whether the existing processes and standards are appropriate.
The Admission Process Should Be Reengineered Under the Public Crisis Situation of COVID-19 Infection
Overall, 18 head nurses thought that the necessity of each item of the admission process in the public crisis state ranged from 39% to 94.4%, indicating that all six items of admission process need not be entirely implemented (Table 3). The necessity for timely treatment and admission evaluation was the highest, at 94.4% and 88.9% respectively, indicating that nurse leaders were more concerned with both timely treatment and admission evaluation. The head nurses perceived the necessity of admission process as high, while actual implementation was poor (Table 6), indicating that the objective factors, rather than the subjective factors, affect the implementation of the admission process. The admission process regulated in “Further Deepening Quality Nursing and Improving Nursing Service”4 is a standard process, which is not suitable under public crisis situations and needs to be reengineered. This is consistent with the findings of studies by Gowda14 and Song.18 Process reengineering refers to the process of rebuilding and optimizing the original workflow using modern management means.25 In recent years, the application of process reengineering has produced a series of changes in nursing management;18 However, the process that conforms to reality and meets the needs should be formulated according to the specific situation.26 Since 2020, the number of deaths from infection worldwide has been increasing dramatically, and countries have made changes accordingly, including optimizing healthcare systems and developing crisis management plans to improve the resilience of healthcare systems that have struggled to adapt as well as to continuously optimize crisis management strategies in response to subsequent emergencies, making dynamic system changes.27,28 The ICU of a hospital in Saudi Arabia has optimized its workflow in terms of supplies, personnel, and bed management to ensure effective care for patients with severe COVID-19 and other critical illnesses.29 In the anti-infection phase of COVID-19 pandemic, a hospital in Nanjing optimized the infusion process, which reduced the physical and mental burden and workload of nurses, improved work efficiency and patient satisfaction, and saved medical costs.18 Nursing managers should fully understand the peculiarities of the public crisis situation of COVID-19 infection compared with any general public crisis situation while conducting process reengineering. First, most of the hospitalized patients are critically ill. Second, most patients are elderly patients. Third, the hospital disrupted the disciplinary boundaries for cross-disciplinary treatment, and some nurses lacked knowledge and skills in arterial specimen collection and prone position treatment. Fourth, the medical staff were infected on a large scale at the same time, which led to the decrease in the number of nursing staff. Fifth, some nurses with illness could not work efficiently. Sixth, the treatment and nursing measures of patients on the day of admission were considerably increased compared with the normal situation. These problems should be considered by nursing managers during process reengineering, and it is necessary to combine the current reality and highlight the key points.26
The Original Quality Evaluation Criteria for Admission of Patients Should Be Adjusted Under the Public Crisis Situation of COVID-19 Infection
The implementation rate is obviously reduced when the nursing quality assessment standard under normal situation is used to assess the nursing quality under public crisis situation (Table 4). For example, the rate of implementation of hygiene and cleanliness was only 1.5% when evaluated using the service quality criteria for the admission process in the normal state. This indicated that the quality control standard under normal situation may not be suitable for public crisis situation of COVID-19 infection. This is consistent with the finding of the study by Babroudi.13 As the key link of nursing quality management, nursing quality evaluation is the basis for nursing management and the standard of evaluating nursing service and the guide for nurses’ work.30 Through the problems discovered during many earthquakes, Japan has continuously optimized the seismic evaluation standards, thus making the seismic capacity of buildings constantly stable and reducing the losses caused by earthquakes.17 In current public crisis situation, the focus of the government is to prevent serious illnesses and reduce the number of deaths. Accordingly, the assessment standard of nursing quality should be adjusted. Moreover, according to the results of investigation of head nurses and quality inspection, “hygiene and cleanliness”, “psychological support”, and “admission introduction” were not the focus at that time, and the focus should be placed on “timely treatment” and “admission evaluation”, which are closely related to “preventing serious illness and reducing death”. Nursing managers can take the following measures when adjusting quality control standards. First, important content can be given a higher score when weighted. Second, the inspection of unimportant terms in quality inspection can be ignored. Because nursing managers’ evaluation results of nursing quality which is the guide of nurses’ work quality will be linked to nurses’ performance appraisal,31 and the nurse’s work focus will vary with the quality evaluation criteria. So nursing managers should start with the adjustment of quality control standards to make nurses further understand their work priorities.
Limitations
This study has some limitations. The implementation of admission process may be affected by many factors. This study only used the existing data and considered the number of critically ill patients, nurses on the job, and doctors’ orders. In the next study, we aim to adopt various research methods to conduct a comprehensive analysis.
Conclusion
This study focuses on the implementation of the public crisis admission process. Based on the real-world research, the study reports on the standard patient admission process and identified that the admission process in public crisis situations should focus on the more important aspects of timely treatment and admission assessment, which is in line with the focus of China’s work on new coronavirus infection cases. At the same time, it shows that original quality evaluation standard of patient admission are not applicable in the public crisis situation of COVID-19 pandemic. The study reminds nursing managers that in the public crisis situation, process reengineering should be conducted while considering the situation at that time. Moreover, the quality evaluation standard should be readjusted so that nurses can focus on effective treatment for patients in the situation of shortage of nurses, poor health condition, and large number of critically ill patients. The reengineering can provide a reference for the optimization of the subsequent admission process.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Approval
This study was approved by the Institutional Review Board of Shanxi Bethune hospital of China (YXLL-2023-011) and conducted in accordance with the Declaration of Helsinki. All patients provided informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no financially supporting body for this article.
Disclosure
There is no conflict of interest in publishing this article.
References
1. Central people’s Government of the People’s Republic of China. Notice on further optimizing the implementation of prevention and control measures for COVID-19 epidemic situation; 2022. In Chinese. Available from: http://www.gov.cn/xinwen/2022-12/07/content_5730443.htm.
2. Central people’s Government of the People’s Republic of China. Major adjustment! Covid-19’s infection will be adjusted from “Class B A tube” to “Class B tube”; 2022. In Chinese. Available from: http://www.gov.cn/xinwen/2022-12/27/content_5733672.htm.
3. Ortiga B, Salazar A, Jovell A, Escarrabill J, Marca G, Corbella X. Standardizing admission and discharge processes to improve patient flow: a cross sectional study. BMC Health Serv Res. 2012;12(1):180. doi:10.1186/1472-6963-12-180
4. People’s Republic of China (PRC) National Health and Wellness Committee. Notice on further deepening quality nursing and improving nursing service. 2015. In Chinese. Available from: http://www.nhc.gov.cn/yzygj/ylzcxx/201503/8d18fd8cdb224e06956a61362fad1e5a.shtml.
5. Li M. Public health crises in comparison: China’s epidemic response policies from SARS to COVID-19. Glob Public Health. 2021;16(8–9):1223–1236. doi:10.1080/17441692.2021.1919735
6. Maršanić VB, Dobrović N, Tadić MF, Flander GB. 2020 Double crisis in Croatia: earthquakes in the time of COVID-19. Eur Child Adolesc Psychiatry. 2021;30(8):1309–1313. doi:10.1007/s00787-021-01785-8
7. Nadeem A, Sahito AM, Shahid S. Flood Crisis in Pakistan: a mass destruction to economy and fragile health care systems. Med Confl Surviv. 2022;38(1):1–5. doi:10.1080/13623699.2022.2157587
8. Rauchfleisch A, Vogler D, Eisenegger M. Public sphere in crisis mode: how the COVID-19 pandemic influenced public discourse and user behaviour in the Swiss Twitter-sphere. Javnost. 2021;28(2):129–148. doi:10.1080/13183222.2021.1923622
9. Vera-Burgos CM, Griffin Padgett DR. Using Twitter for crisis communications in a natural disaster: hurricane Harvey. Heliyon. 2020;6(9):e04804. doi:10.1016/j.heliyon.2020.e04804
10. Kim SA, Kim S, Kim G, et al. A multivalent vaccine based on ferritin nanocage elicits potent protective immune responses against SARS-CoV-2 mutations. Int J Mol Sci. 2022;23(11):6123 doi:10.3390/ijms23116123.
11. Mousavi S, Anjomshoa M. COVID-19 in Yemen: a crisis within crises. Int J Equity Health. 2020;19(1):120. doi:10.1186/s12939-020-01231-2
12. Chinese Philanthropist. The number of patients has increased dramatically, and medical staff have been infected in a large area, so medical resources are facing challenges; 2022. In Chinese. Available from: https://news.sina.com.cn/s/2022-12-14/doc-imxwsfhr6428267.shtml.
13. Babroudi NEP, Sabri-Laghaie K, Ghoushchi NG. Re-evaluation of the healthcare service quality criteria for the Covid-19 pandemic: z-number fuzzy cognitive map. Appl Soft Comput. 2021;112:107775. doi:10.1016/j.asoc.2021.107775
14. Gowda NR, Siddharth V, Inquillabi K, Sharma DK. War on waste: challenges and experiences in COVID-19 waste management. Disaster Med Public Health Prep. 2021;1–13. doi:10.1017/dmp.2021.171
15. Houghton C, Meskell P, Delaney H, et al. Barriers and facilitators to healthcare workers’ adherence with infection prevention and control (IPC) guidelines for respiratory infectious diseases: a rapid qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;4(4):D13582. doi:10.1002/14651858.CD013582
16. Mohammadpour M, Sadeghkhani O, Bastani P, Ravangard R, Rezaee R. Iranian’s healthcare system challenges during natural disasters: the qualitative case study of Kermanshah earthquake. BMC Emerg Med. 2020;20(1):75. doi:10.1186/s12873-020-00359-2
17. Okada T. Development and present status of seismic evaluation and seismic retrofit of existing reinforced concrete buildings in Japan. Proc Jpn Acad Ser B Phys Biol Sci. 2021;97(7):402–422. doi:10.2183/pjab.97.021
18. Song Y, Wang W, Zhang L, Sha L, Lu G. Optimization of the intravenous infusion workflow in the isolation ward for patients with coronavirus disease 2019. Int J Nurs Sci. 2020;7(2):148–152. doi:10.1016/j.ijnss.2020.03.009
19. Sherman RE, Anderson SA, Dal Pan GJ, et al. Real-world evidence - what is it and what can it tell us? N Engl J Med. 2016;375(23):2293–2297. doi:10.1056/NEJMsb1609216
20. Nandi M, Asthana AK, Asthana AK. Audit of cancer patients from eastern Uttar Pradesh (UP), India: a university hospital based two year retrospective analysis. Asian Pac J Cancer Prev. 2013;14(9):4993–4998. doi:10.7314/APJCP.2013.14.9.4993
21. Chen D. Real-world studies: bridging the gap between trial-assessed efficacy and routine care. J Biomed Res. 2022;36(3):147–154. doi:10.7555/JBR.36.20220040
22. Luo J, Xu H, Liu B. Real world research: a complementary method to establish the effectiveness of acupuncture. BMC Complement Altern Med. 2015;15(1):153. doi:10.1186/s12906-015-0676-6
23. Zhang L, Li H, Wang T, Wang R, Cheng L, Wang G. Real-world study: a powerful tool for malignant tumor research in general surgery. Cancers. 2022;14(21):5408. doi:10.3390/cancers14215408
24. Tsai H, Huang SW, Hung YL, Hsu YS, Huang CC. Use of the smart lean method to conduct high-quality integrated perioperative management prior to hospitalization. Int J Environ Res Public Health. 2021;18(24):13391. doi:10.3390/ijerph182413391
25. Liu Y, Liu H, Khalaf OI. Utilization of nursing defect management evaluation and deep learning in nursing process reengineering optimization. Comput Math Methods Med. 2021;2021:8019385. doi:10.1155/2021/8019385
26. Pelt CE, Campbell KL, Gililland JM, et al. The rapid response to the COVID-19 pandemic by the arthroplasty divisions at two academic referral centers. J Arthroplasty. 2020;35(7S):S10–S14. doi:10.1016/j.arth.2020.04.030
27. Abbas J. Crisis management, transnational healthcare challenges and opportunities: the intersection of COVID-19 pandemic and global mental health. Res Global. 2021;3:100037. doi:10.1016/j.resglo.2021.100037
28. Haldane VA-O, De Foo CA-O, Abdalla SM, et al. Health systems resilience in managing the COVID-19 pandemic: lessons from 28 countries. Nat Med. 2021;27(6):964–980. doi:10.1038/s41591-021-01381-y
29. Al-Dorzi HM, Aldawood AS, Almatrood A, et al. Managing critical care during COVID-19 pandemic: the experience of an ICU of a tertiary care hospital. J Infect Public Health. 2021;14(11):1635–1641. doi:10.1016/j.jiph.2021.09.018
30. Duan X, Shi Y. Current status of quality evaluation of nursing care through director review and reflection from the nursing quality control centers. Int J Clin Exp Med. 2014;7(10):3737–3745.
31. Moradi T, Mehraban MA, Moeini M. Comparison of the perceptions of managers and nursing staff toward performance appraisal. Iran J Nurs Midwifery Res. 2017;22(2):128–134. doi:10.4103/ijnmr.IJNMR_142_15
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.