Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Implementation and Outcomes of a Standardized Multidisciplinary Treatment Outpatient Model in Two Pediatric Tertiary Hospitals
Authors Wang M, Ye C, Gao X, Qian Y, Feng T ![]() , Shi Y
, Shi Y
Received 13 February 2026
Accepted for publication 2 April 2026
Published 9 April 2026 Volume 2026:19 599215
DOI https://doi.org/10.2147/JMDH.S599215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Tilakavati Karupaiah
Miao Wang,1,* Chengjie Ye,2,* Xuan Gao,3 Yuping Qian,3 Tianxing Feng,4 Yu Shi3
1Department of Medical Affairs, Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Information and Data Center, National Children’s Medical Center, Children’s Hospital of Fudan University, Shanghai, People’s Republic of China; 3Outpatient and Emergency Management Office, National Children’s Medical Center, Children’s Hospital of Fudan University, Shanghai, People’s Republic of China; 4Department of Medical Affairs, Shanghai Clinical Research and Trial Center, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu Shi, Outpatient and Emergency Management Office, National Children’s Medical Center, Children’s Hospital of Fudan University, Shanghai, People’s Republic of China, Email [email protected] Tianxing Feng, Department of Medical Affairs, Shanghai Clinical Research and Trial Center, Shanghai, People’s Republic of China, Email [email protected]
Objective: This study aims to investigate the implementation and outcomes of the Multidisciplinary Treatment (MDT) outpatient model in two pediatric tertiary hospitals, guided by the standardized “Three Fixed Elements and Four Dedicated Processes” operational plan.
Methods: A retrospective analysis was conducted on the MDT outpatient services at the Children’s Hospital of Fudan University and Shanghai Children’s Hospital, School of Medicine, Shanghai Jiao Tong University, from 2018 to 2025.
Results: During the study period, MDT outpatient services at two pediatric hospitals showed substantial growth, serving 15,813 patients with complex and rare conditions. Annual service volume increased from 304 to 5,174, and the number of MDT clinics expanded from 13 to 53, reflecting enhanced service capacity and efficiency. Specialty coverage developed in three phases, incorporating core clinical departments and integrated supportive services. Operational consistency was maintained through a “Three Fixed Elements and Four Dedicated Processes” framework, with performance monitored via a five-dimension management system tracking clinic volume, protocol standardization, expert participation, record quality, and patient satisfaction.
Conclusion: The management model effectively enhances multidisciplinary focus, strengthens outpatient clinic construction, and facilitates continuous patient management and successful interdisciplinary collaboration. The study demonstrates the model’s success in building a scalable, standardized, and patient-centered MDT system for pediatric complex care.
Keywords: multidisciplinary team, pediatrics, outpatient clinic, standardized management, rare diseases
Background
The discipline layouts and specialization divisions of comprehensive hospitals are becoming increasingly better due to the rapid growth of modern medicine. However, this growth has created new challenges for some patients,1 such as compilated and difficult medical care, especially for individuals with multiple ailments, undiscovered conditions, or those requiring interdisciplinary teamwork. For example, patients with undetected diseases,2 difficult-to-diagnose ailments, and tumors sometimes must transfer between departments and cope with a variety of challenges, such as lengthy cycles, low efficiency, high costs, and challenging diagnosis and treatment. To enhance coordination and communication across various healthcare teams, a multidisciplinary team may be employed.3,4 One important way to deal with the aforementioned problems in this situation is through the interdisciplinary diagnostic and therapeutic approach.
The phrase of MDT refers to a concept in which clinical multidisciplinary teams work together to discuss a specific case, develop standardized and personalized best diagnosis and treatment plans, and then implement those plans either independently or in concert by relevant disciplines.5 In recent years, the country has produced several relevant policies and considered the development of the MDT model.6 In 2023, for example, the National Health Commission published “Notice on Carrying out the Comprehensive Action to Improve Medical Quality (2023–2025)” and “Notice on Carrying out the Theme Activities to Improve Medical Experience and Enhance Patient Experience,” both of which emphasized the significance of “putting patients at the center,” actively promoting the MDT model, and opening MDT clinics to better serve the public’s growing needs.
With varying degrees of success, a few hospitals have established centers for the diagnosis and treatment of uncommon diseases and have carried out interdisciplinary diagnosis and therapy.7,8 Current experiences, however, often have distinctive hospital features, and their generalizability and reproducibility are questionable. Many institutions do not seem to be able to improve their MDT diagnosis and treatment capabilities currently.
Since 2017, Children’s hospital of Fudan University and Shanghai Children’s Hospital have both used MDT management, with noteworthy results. This paper will analyze the status of development, management style, advantages, and challenges of MDT clinics in the two hospitals to provide useful resources for optimizing medical services and improving patient experience. Additionally, it will investigate related solutions and potential future development paths.
Methods
MDT Outpatient Mode of Operation
The MDT outpatient model is coordinated by an MDT project leader and a dedicated project secretary, the latter being primarily responsible for patient administration and daily operational management. To ensure standardized and high-quality service delivery across all MDT clinics, both hospitals have implemented a structured operational framework referred to as the “Three Fixed Elements and Four Dedicated Processes”. The Three Fixed Elements establish core operational consistency by maintaining a fixed Schedule for regular clinic sessions, utilizing a fixed Location for all consultations, and engaging a fixed Team comprising a stable core of specialist departments dedicated to each disease-specific program. Complementing this, the Four Dedicated Processes ensure systematic management: dedicated Coordination through an assigned project secretary; dedicated Patient Files that consolidate individual medical records; dedicated Disease Registries organized by condition to enable standardized tracking; and dedicated Funding earmarked specifically to support MDT activities. This framework is reinforced through regular MDT clinics, scheduled secretary meetings, and periodic assessments and evaluations.
Operationally, the MDT process is initiated when a patient or attending physician submits an application, with patients able to self-schedule via online platforms. The project secretary subsequently collects and organizes the patient’s medical records in advance. Upon verification that the patient meets referral criteria and that documentation is complete, the fixed expert team convenes at the scheduled time and location to conduct the multidisciplinary consultation, culminating in a coordinated, patient-specific diagnostic and therapeutic plan (Figure 1).
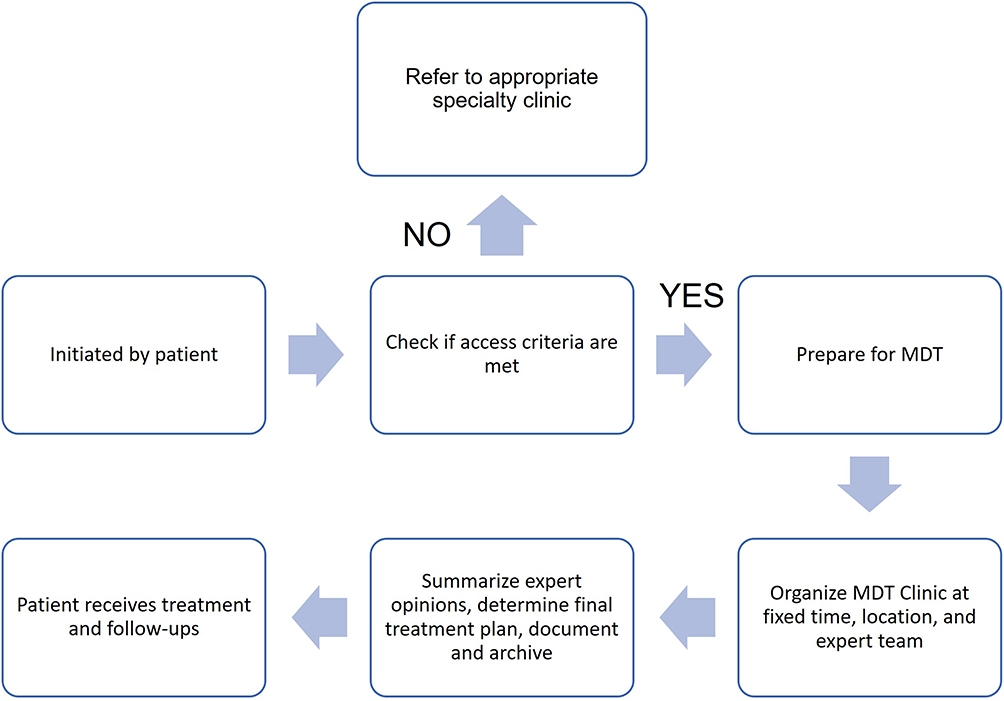 |
Figure 1 Flowchart of Multidisciplinary Treatment (MDT) Patient Management Process. |
Results
MDT Clinic Patient Profile
Between 2018 and 2025, Children’s hospital of Fudan University and Shanghai Children’s Hospital provided MDT outpatient services to 15813 patients with difficult and rare conditions. The yearly number of MDT services staff went from 304 in 2018 to 5174 in 2025, an increase of around 16 times, and the number of MDT clinics increased from 13 to 53, a more than threefold increase, demonstrating a considerable improvement in outpatient service efficiency. This development is particularly apparent after 2023, which may be due to the market’s high demand expansion and the MDT mode’s continuous optimization (Figure 2).
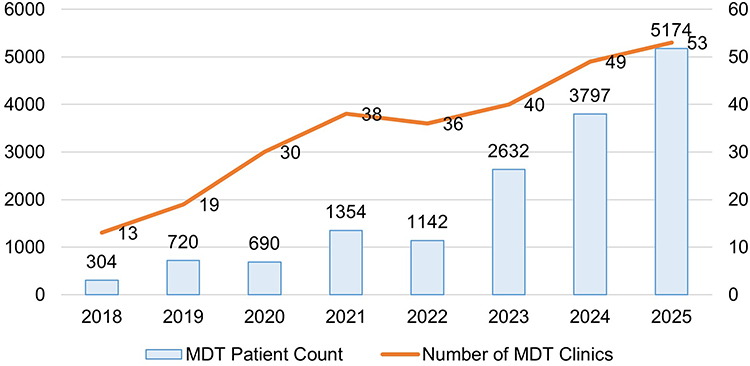 |
Figure 2 Trends in MDT Patient Count and Number of MDT Clinics (2018–2025). |
Coverage of MDT Clinic Specialty Areas
The expert coverage of the MDT outpatient department at both hospitals has gone through three stages of development. Taking the Children’s Hospital of Fudan University as an example, rheumatology, general surgery, endocrinology, neurology, psychology, digestion, hematology, and orthopedics are among the first specialties covered in 2018. We started a phase of quick supplementation between 2019 and 2020 with the addition of departments such as Hepatology, Respiratory Medicine, Cardiology, Immunology, Pediatrics, Stomatology, Urology, and Neonatology. Since 2021, the MDT specialty system has expanded to include nursing teams, nephrology, cardiology, infection, and rehabilitation (Figure 3).
 |
Figure 3 Expansion Timeline of Multidisciplinary Treatment Departments (2018–2025). |
Neurology and general surgery are tied for top place in terms of the number of MDT clinics, each with six. MDT in neurology mostly addresses challenging conditions such refractory epilepsy, whereas the majority of MDT in general surgery focuses on gastrointestinal cancers and related gastrointestinal issues (Figure 4).
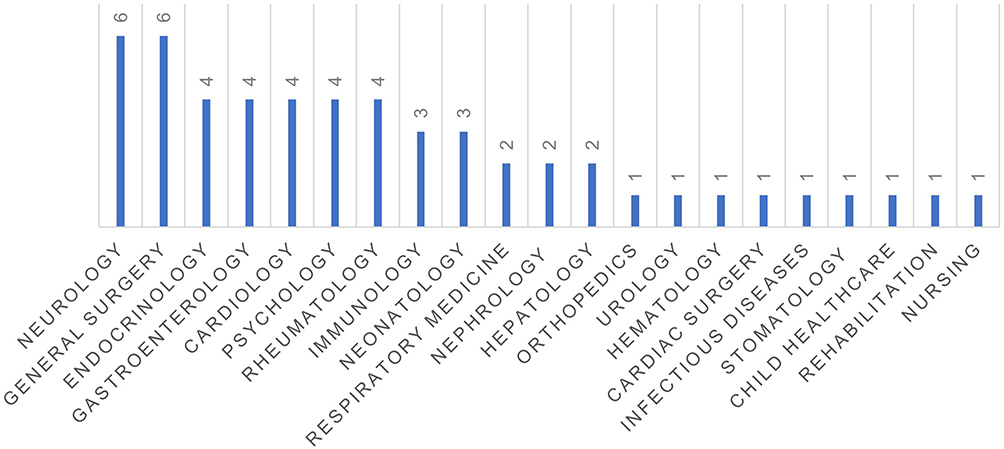 |
Figure 4 Number of Departments Involved in MDT Services Across Different Medical Specialties. |
According to the MDT outpatient data ranking among the top ten in terms of outpatient volume in 2025, the gastroenterology department holds four seats (inflammatory bowel disease, difficulty defecating, infant milk allergy, and digestive endoscopy) and ranks first with an absolute business volume advantage of 840 people. This demonstrates both the department’s fundamental stance and the scope and depth of its implementation throughout our MDT system. The two outpatient clinics for children solid tumors and biliary atresia on the list show general surgery’s excellent fit for addressing pediatric surgical severe cases, with business volumes ranking second and fourth, respectively. Despite being relatively small, the single volume focuses on the difficult and difficult diagnostic domains. Additionally, two seats are occupied by the clinical immunology and allergy departments (immunodeficiency, unexplained fever) (Table 1).
 |
Table 1 Top 10 MDT Clinics by Outpatient Volume in 2025 |
Table 2 lists the participating and leading departments from the 53 MDT clinics in each of the two hospitals. Data shows that of the 24 MDTs (including neurology, general surgery, endocrinology, etc)., nutrition is the most often involved department. This emphasizes how important nutritional assistance is for treating a wide range of diseases holistically. Participating in 18 MDTs (including neurology, general surgery, cardiology, etc.), the second-ranked radiology/imaging department is mainly responsible for diagnostic and imaging evaluation activities. The rehabilitation department’s involvement in 12 MDTs, including those in neurology, cardiology, psychiatry, etc., demonstrated the significance of rehabilitation treatment. Additionally, neurology has participated in ten MDTs (including dentistry, psychiatry, and others), demonstrating its extensive interdisciplinary collaboration. From a pattern viewpoint, many MDTs focus on treating chronic illnesses, genetic disorders, or complicated symptoms (such as allergies, malignancies, or epilepsy). Internal medicine, surgery, auxiliary departments (such as nutrition and rehabilitation), and psychological support services are frequently integrated.
 |
Table 2 Overview of 53 Multidisciplinary Treatment (MDT) Clinics by Lead Department and Participating Units |
Discussion
Since its introduction in the United States in the 1990s, the MDT paradigm has become the standard for clinical diagnosis and treatment in developed countries in both Europe and North America.9,10 For instance, the UK’s National Health Service mandated MDT-based management for all cancer patients in 2007, a policy now reflected in numerous international oncology guidelines.11,12 This report provides a systematic analysis of the establishment and management of the MDT outpatient service at our institution from 2016 onward.
The promotion of MDT services is explicitly advocated in key national health policies, such as the National Health Commission’s 2019 work plan for service improvement.13 Furthermore, the 2022 edition of China’s Evaluation Standards for Tertiary Hospitals formally recognizes MDT as a core component of medical quality and patient safety, specifically encouraging the establishment of MDT clinics for complex, multi-system diseases.14,15 In response, our hospitals implemented a multi-channel appointment system via phone, in-person, online platforms, and physician referral to streamline patient access and enhance operational efficiency.
To address the common constraint of dedicated physical space, the hospitals established a centrally managed MDT consultation center. The development of the service was guided by a structured “Three Fixed Elements and Four Dedicated Processes” management framework. The operation is further reinforced by a complementary “Five-Dimension Performance Management” for long-term oversight. This integrated system facilitates the synchronized monitoring of key performance indicators across five critical domains: the growth in MDT clinic volume, the standardization level of diagnostic and therapeutic protocols, expert participation rates, the quality of electronic medical records, and patient satisfaction metrics. This comprehensive evaluation mechanism, supported by targeted incentives, promotes consistent engagement from clinical departments and fosters sustained improvement in the quality of MDT care delivery.
Beyond improving efficiency and reducing patient inconvenience, the MDT clinic model delivers comprehensive, precise, and personalized treatment plans. More significantly, by breaking down traditional disciplinary silos, it enhances diagnostic accuracy and treatment efficacy for complex conditions like tumors, rare diseases, and other difficult cases, ultimately improving patient outcomes.16,17 The hospitals have successfully built a scalable, standardized, and patient-centered MDT outpatient system, with strategic expansion into high-need specialties and deep integration of supportive services.
The primary challenge moving forward is integrating a full life-cycle management concept into the MDT process. Current MDT practice in China often focuses on the acute diagnostic and treatment phase, with gaps in long-term health management and follow-up. To address this, we recommend leveraging health information platforms to create integrated MDT service chains that cover diagnosis, treatment, rehabilitation, and follow-up, thereby extending the team’s long-term impact. It must be acknowledged that MDT clinics in China are still in a developmental stage, requiring improvements in financing models, operational workflows, quality control, and clinician engagement. Future development should focus on digital integration of MDT services, such as through cloud-based multidisciplinary platforms or synchronized tele-MDT systems, to improve accessibility and coordination.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by Ethics Committee of Children’s Hospital of Fudan University (Approval No. (2023) 152).
Data Sharing Statement
The datasets used and/or analyzed during the current study available from the corresponding author Dr. Yu Shi on reasonable request. The data are not publicly available due to privacy restrictions.
Informed Consent Statement
As this study involved a retrospective analysis of anonymized data from the Hospital Information System, the requirement for written informed consent was waived by the Institutional Review Board.
Acknowledgment
The authors acknowledge all the participants joining the training program.
Author Contributions
Dr. Miao Wang and Mr Chengjie Ye share the first author and contribute equally to this manuscript. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
M.W. discloses support for the research of this work from Health Commission of Putuo District (grant number PTELT-2024-18). Y.Q. discloses support for the research of this work from Shanghai Hospital Development Center Foundation (grant number SHDC12024623). The funders played no role in study design, collection, analysis, interpretation of data, writing of the report, or the decision to submit the paper for publication.
Disclosure
All authors declare no financial or non-financial competing interests.
References
1. Curic E, Ewans L, Pysar R, et al. International Undiagnosed Diseases Programs (UDPs): components and outcomes. Orphanet J Rare Dis. 2023;18(1):348. doi:10.1186/s13023-023-02966-1
2. Shi Y, Miao S, Yuan Y, et al. Accelerating rare disease detection: an experience of multidisciplinary team model in undiagnosed diseases program in a children’s hospital. Front Public Health. 2024;12:1373649. doi:10.3389/fpubh.2024.1373649
3. Epstein NE. Multidisciplinary in-hospital teams improve patient outcomes: a review. Surg Neurol Int. 2014;5(Suppl 7):S295–9. doi:10.4103/2152-7806.139612
4. Moodley N, Weidler EM, Ochoa B, et al. Satisfaction with multidisciplinary team structure and function in a pediatric outpatient clinic. J Pediatr Surg. 2025;60(3):162103. doi:10.1016/j.jpedsurg.2024.162103
5. Rowan BL, Anjara S, De Brún A, et al. The impact of huddles on a multidisciplinary healthcare teams’ work engagement, teamwork and job satisfaction: a systematic review. J Eval Clin Pract. 2022;28(3):382–393. doi:10.1111/jep.13648
6. Yang C, Hu S, Ye D, et al. Evaluating price and availability of essential medicines in China: a mixed cross-sectional and longitudinal study. Front Pharmacol. 2020;11:602421. doi:10.3389/fphar.2020.602421
7. Wohlgemuth WA, Wölfle K, Schuster T, et al. Hereditary vascular malformations: classification, symptoms, diagnostics and prognosis. Zentralbl Chir. 2012;137(5):440–445. Norwegian. doi:10.1055/s-0030-1262546
8. Jiang Y, Huang H, Zhao G, et al. Seven-year exclusivity and beyond for drugs of rare diseases in China. Front Pharmacol. 2023;14:1223056. doi:10.3389/fphar.2023.1223056
9. Takahara M. Sialendoscopy for the management of sialolithiasis in Japan. Auris Nasus Larynx. 2025;52(6):764–768. doi:10.1016/j.anl.2025.10.004
10. Hotez P, Bottazzi ME, Strub-Wourgaft N, et al. A new patient registry for chagas disease. PLoS Negl Trop Dis. 2020;14(10):e0008418. doi:10.1371/journal.pntd.0008418
11. Wang H, He Q, Guo Y, et al. Empirical study on the operational status and key influencing factors of outpatient multidisciplinary (MDT) service model: a cross-sectional study in Sichuan Province, China. J Multidiscip Healthc. 2025;18:4431–4442. doi:10.2147/JMDH.S528489
12. Brown S, Bate J. National advisory panels for paediatric cancer in the UK as an example of rare cancer multidisciplinary team meetings. Rare Tumors. 2021;13:20363613211052503. doi:10.1177/20363613211052503
13. Chen Y, Xiang J, Liu D, et al. Multidisciplinary team consultation for resectable gastric cancer: a propensity score matching analysis. J Cancer. 2021;12(7):1907–1914. doi:10.7150/jca.53365
14. Zhong X, Zeng X, Zhao L, et al. Clinicians’ knowledge and understanding regarding multidisciplinary treatment implementation: a study in municipal public class III grade A hospitals in Southwest China. BMC Med Educ. 2023;23(1):916. doi:10.1186/s12909-023-04891-0
15. Shao Y, Li Q, Bian M, et al. A multi-center study on the implementation and challenges of nursing three-level ward rounds in tertiary hospitals in Shanxi Province. J Multidiscip Healthc. 2024;17:4441–4452. doi:10.2147/JMDH.S474702
16. Soroush S, Lim S, Beniwal P, et al. Optimising prostate cancer pathways: improving post-biopsy waiting times in a tertiary centre. BJUI Compass. 2025;6(7):e70045. doi:10.1002/bco2.70045
17. Huang Q, Changxu L, Ruijun T, et al. Multidisciplinary team for the diagnosis and treatment of 2 cases of primary intestinal yolk sac tumor. Cancer Biol Med. 2018;15(4):461–467. doi:10.20892/j.issn.2095-3941.2018.0054
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Practice of Multidisciplinary Team-Guided Comprehensive Management for Pediatric Patients with Fabry Disease: A Single-Center Case Series
Liu Y, Liu X, Yang M, Wang Q, Xu W, Zeng J, Han T, Mao H, Qian S
Journal of Multidisciplinary Healthcare 2026, 19:537644
Published Date: 27 January 2026