")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Impacts of the Early COVID-19 Response on Allied Health Staff Within an Australian Tertiary Health Service: A Qualitative Study
Authors Angus RL , Wenke R , Burrett S, Mahoney J , Roberts S
Received 4 July 2023
Accepted for publication 6 November 2023
Published 6 December 2023 Volume 2023:16 Pages 3833—3846
DOI https://doi.org/10.2147/JMDH.S428710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rebecca L Angus,1 Rachel Wenke,1 Sara Burrett,1 Jill Mahoney,1 Shelley Roberts1,2
1Allied Health and Rehabilitation Services, Gold Coast Hospital and Health Service, Southport, QLD, Australia; 2School of Health Sciences and Social Work, Griffith University, Southport, QLD, Australia
Correspondence: Rebecca L Angus, Allied Health and Rehabilitation Services, Gold Coast Hospital and Health Service, Southport, QLD, 4215, Australia, Tel +6 175 687 8314, Email [email protected]
Purpose: Understanding the experiences and needs of healthcare workers is crucial in strengthening healthcare system resilience during times of change. We aimed to explore allied health (AH) professionals’ perceptions of the impacts of the COVID-19 pandemic response on their work experiences.
Participants and Methods: Qualitative descriptive study using thematic analysis of semi-structured interviews with AH professionals employed in a large Australian health service.
Results: Four themes were conceptualized from interviews of 21 AH clinicians and consolidated with six AH managers. Impacts were at personal, service, and systems levels. An overarching theme of “acceptance of circumstances due to the pandemic” influenced experiences within each level. Service changes included service cessation, remote service delivery, new COVID-19 protocols and role or work location alterations. Some staff were empowered in making practice changes, while others lost research or career opportunities. Despite low COVID-19-related hospitalizations and fatalities, staff reported stresses from workload changes and fear for self or loved ones. Open, clear communication assisted in alleviating anxiety, while perceived involvement in decision making and administrative and/or technical support for implementation of new processes facilitated change management processes.
Conclusion: The study demonstrates the impacts of the COVID-19 pandemic response on AH professionals. Gleaned in a context with limited community disease transmission and without the challenges of providing care for large numbers of COVID-19 patients, the findings have implications for change management within health services in any context in which rapid change is required. The wellbeing of the workforce should be forefront. Clear communication is critical, with staff involved in decision-making where possible. The needs of vulnerable staff should be considered with clear processes and eligibility guidelines to ensure provision of appropriate support and transparency of decision making. Workloads should be monitored, and adequate infrastructure, technical support and training provided for new initiatives or processes.
Keywords: allied health professionals, change management, hospital, COVID-19, healthcare workers
Introduction
The emergence of the SARS-CoV-2 virus and the eventual declaration of the COVID-19 pandemic by the World Health Organization in March 2020 resulted in massive social and economic upheaval as actions were taken to limit spread of the virus and manage care for those infected. In Australia, international and many internal state borders were closed, and quarantine procedures were introduced.1 Health services engaged in rapid preparations for the anticipated rise in cases seen in many other countries around the world. Non-urgent elective surgeries and specialist outpatient services were suspended. Other service changes including the expansion of telehealth, enhanced physical distancing and visitor restrictions were made to reduce transmission of SARS-CoV-2 within the health workforce and the wider community by minimizing foot traffic through hospitals and reducing person-to-person contact.2
While change is a constant in healthcare, it is also notoriously challenging, with the implementation of new practices, services or altered models of care often slow or ineffective. Barriers to change include the complexity of healthcare organizations, political and funding pressures, organizational culture and factors related to individual practitioners and the other stakeholders involved.3 Despite this, multiple rapid changes were enacted in health services the world over during the early stages of the pandemic. Understanding the experiences and needs of healthcare workers is crucial in strengthening healthcare system resilience during times of change. In Queensland, the effectiveness of disease transmission strategies created a unique environment to explore this. The setting differed from that common elsewhere where staff faced service changes while simultaneously juggling responsibilities to care for large numbers of COVID-19 patients. Further, although numerous studies have now documented the impacts of the COVID-19 pandemic on health care workers, most have focused on doctors and nurses.4 Allied health (AH) encompasses a range of disciplines outside of medicine, nursing and dentistry. Practitioners are university qualified and have specialist expertise in preventing, diagnosing and treating various conditions and illnesses. In Australia, in excess of one quarter of the health workforce are AH professionals.5 Understanding the experiences of such a large proportion of the health workforce is important for developing systems resilience.
The aim of this study was to explore the perceptions of AH professionals on the impacts of the COVID-19 response on their work while employed within an Australian health service during the first year of the pandemic. Specifically, we sought to understand the impacts these staff faced personally, the effects on their work and patient care, and their experience of change management at a systems level during the pandemic.
Materials and Methods
Study Design
This qualitative descriptive study used semi-structured interviews of hospital-based AH professionals. The study was performed in accordance with the Declaration of Helsinki, with ethical approval granted by the Gold Coast Hospital and Health Service Human Research Ethics Committee (HREC/2020/QGC/67379). Reporting of this study follows the consolidated criteria for reporting qualitative research.6
Setting
The study was conducted across a tertiary health service in southeast Queensland, Australia, providing publicly funded inpatient and outpatient services to a local population of 650,000 people. Gold Coast Hospital and Health Service (GCHHS) has an AH workforce of 1200 and delivers services across two large hospitals (~1250 beds total), a day (surgical) hospital, and several community outpatient hubs. The health service had a pandemic preparedness plan in place prior to the onset of the COVID-19 pandemic and was a designated COVID-19 management facility, providing treatment to affected patients during the study period. Located close to the New South Wales border, the service both employs and services residents of two States, thus was acutely impacted by border closures enacted to contain spread of SARS-CoV-2.
Participants and Recruitment
All AH professionals (eg, audiology, dietetics, occupational therapy, pharmacy, physiotherapy, podiatry, psychology, social work, speech pathology) employed at our health service were eligible for participation. Potential participants were approached by direct email. As we were particularly interested in the impacts of service changes and the change management process, a purposive sampling strategy was used, with staff experiencing role and/or service delivery changes identified through discussions with AH discipline leads and via snowball sampling from interviewed participants. To capture a range of views and experience, additional recruitment was via open invitation disseminated through health service-wide email channels/newsletters and tearoom notice boards. A participant information sheet was emailed, and written informed consent was collected from those agreeing to an interview. Participants were advised that responses were confidential, would not affect their employment, and that information would be de-identified prior to team analysis and later publication.
Positionality of Researchers
The multidisciplinary study team comprised AH professionals in health service management (SB – social work), workforce development (JM – physiotherapy), and research roles (RLA, SR – dietetics, RW – speech pathology). RLA, RW and SR also held research doctorates and had experience in qualitative research methods including semi-structured interviews and thematic analysis. All were female and employed within GCHHS. During analysis, the researchers had a combined insider and outsider perspective,7 as team members worked within the same organization, disciplines and timeframe of experience as participants, but not in clinical roles. Interviews were conducted by RLA. Participants were aware of research team members’ roles in the health service, and in some cases, the interviewer was previously known to the participant.
Data Collection
Semi-structured interviews were selected to enable flexible exploration of topics and issues of interest and maximize the richness of data collected.8 An interview guide designed to elicit open-ended responses from participants was developed based on the professional experience and discussion amongst the research team. Questions were organized under three domains, exploring: 1) Impact of the pandemic response on individual staff/roles; 2) Innovations resulting from the response (technology, work arrangements); and 3) Changes to service delivery (and how they were implemented) (Supplementary File 1). Demographic information was collected directly from participants prior to interview. Face-to-face or video-conference interviews were conducted in private with only interviewer and participant(s) present, either individually or as small focus groups (where participants worked in similar caseloads) according to participant preference. The interviewer used prompts and probing techniques as necessary for in depth exploration of areas of interest, while remaining open to new topics. Field notes were completed immediately after interviews to capture non-verbal content and contextualize data. Interviews were audio recorded and transcribed verbatim. The interviewer returned transcripts to clinician participants for checking, with the option to redact or clarify any items before these were shared with the remainder of the research team. Only the interviewer was aware of the identities of participants. For data triangulation, a second round of interviews were conducted with managers from various AH disciplines using a modified interview guide designed to probe themes arising in the clinician interviews. Interviews with clinicians were conducted between October 2020 and January 2021, and AH managers between June and November 2021.
Data Analysis
Thematic analysis was undertaken via the six-step process of data familiarization; initial code generation; identification of potential themes; review of themes; defining/naming themes; and writing up of findings.9 Each transcript was inductively coded by at least two researchers (SR, RW, JM, RLA), with one researcher (RLA) coding all transcripts for continuity. An initial thematic framework was developed by discussion between all team members after interviewing the first six participants and was refined after 15 participants. Data saturation was recognized when all data from the subsequent four interviews were able to be coded within these themes, thus, recruitment was ceased. NVivo software (QSR International Pty Ltd) was used to facilitate data organization and coding.
Results
Interviews were conducted with 26 AH professionals, comprising 19 clinicians and seven managers from six disciplines (Table 1). All clinicians approached consented to participate, and all those who self-nominated were interviewed. Clinician participants worked in inpatient, outpatient, and community settings across a range of clinical areas. Managers from dietetics, occupational therapy, physiotherapy, social work, and speech pathology also participated. The participant gender ratio reflected that of AH professionals in our health service. Interviews averaged 28 minutes for clinicians and 37 minutes for managers.
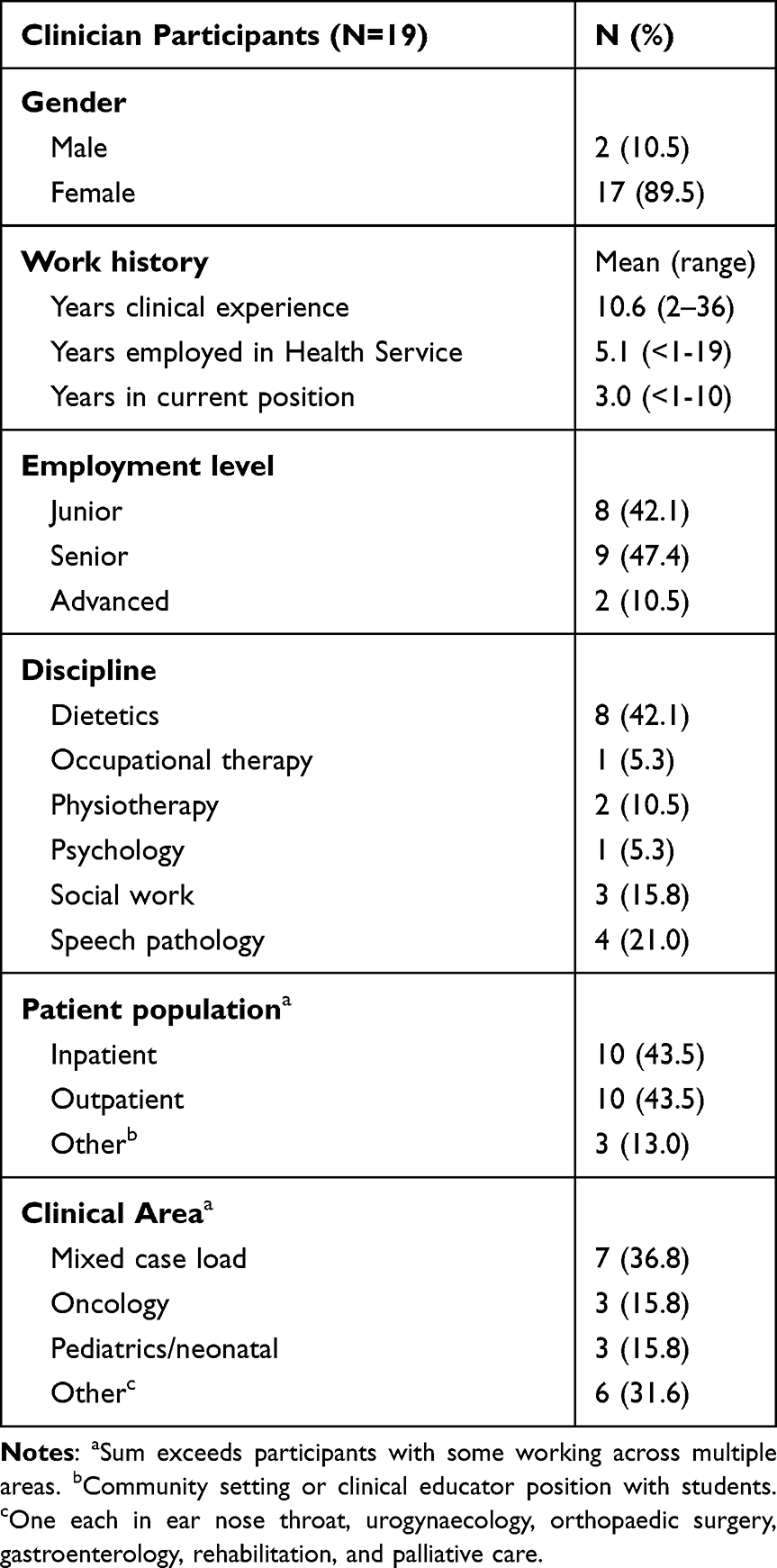 |
Table 1 Demographics of Clinician Participants |
The changes to clinician roles and service provision occurring as a result of the pandemic response were descriptively grouped into four categories (Table 2). The impacts of the health service’s COVID-19 response were experienced by AH professionals at service, personal, and systems levels. The subthemes generated within each level are shown in Figure 1. A fourth theme, “Acceptance due to pandemic circumstance”, overlaid all other themes, influencing the responses and findings within these. Exemplar quotes for each theme and subtheme are provided in Supplementary File 2.
 |
Table 2 Changes to AH Professional Roles and Service Provision During the Early COVID-19 Pandemic Response |
 |
Figure 1 Themes generated from participant interviews. |
Theme 1: Service Level – Impacts on Service Provision
Standard of Care and Perceived Impacts on Patients
Participants perceived both positive and negative aspects of changes on the standard of care provided to patients. Many clinicians were worried that patients were missing out on care because of closures or reduced services:
It sucks that patients miss out on therapy. I could see frustration levels really high in lots of my colleagues… Everyone was really struggling. Participant 16.
Others were concerned about effects on the quality of the holistic patient and/or family experience resulting from reduced visitor and support person access imposed by hospital visitor restrictions and State border closures.
I was not able to really provide that kind of level of support for family because we were constantly just trying to manage the distress around them being able to visit their loved ones and the restrictions around that. Participant 17.
AH clinicians described adverse effects of personal protective equipment (ie, face masks) and remote service delivery on rapport building and the ability to conduct and provide usual assessments, care, and interventions. For example, they indicated this resulted in less robust bedside or clinic assessments. However, telehealth also provided some advantages, giving clinicians extra information about the home environment, and the ability to provide real-time feedback to patients on behaviors within the home context.
I got parents to go and open up the fridge and find out how much calcium is in the soymilk that they are using, show me what high fat options they had in the cupboard. It was great. Then we can say “pull that out, give it to them”. It was awesome. Participant 3
AH clinicians reported varying degrees of patient satisfaction with telehealth. They indicated that many patients appreciated the convenience and/or safety aspects for themselves in not needing to attend a clinic appointment. However, they described that other patients struggled with the technology or disliked not being seen in person, especially in services where assessments of interventions were more difficult to provide remotely. Several managers commented on the benefits of telehealth in providing patients with options for receiving care, indicating that the option to receive consultations via telehealth had been continued in various services, despite the later removal of hospital attendance restrictions.
We have learnt a lot through the pandemic in terms of generating different ideas around how we can provide clinical services and I think one of them definitely was telehealth options and providing people with those options. Participant 26, Manager
Workload Changes
Workload changes were experienced by many AH professionals. Some service alterations provided increased efficiencies. For example, greater patient awareness of telehealth resulted in increased responses to telephone calls, reducing the need for multiple contact attempts. This was particularly evident during lockdown periods where patients were at home and engaged in fewer other activities. However, workloads increased in clinics where staff typically relied on patient failure to attend some scheduled appointments for time to complete clinical notes, letters, and referrals.
We had reduced numbers of cancellations, reduced numbers of FTAs [fails to attend] … we were seeing more patients as a result of the change from in-person to telehealth or teleconferencing. So clinical load increased and also… I, as a clinician, was making contact with patients to change their appointments over from in-person to phone or teleconferencing and the time burden that’s associated with that is significant. Participant 14
Other reasons for increased workload included staff experiencing role changes needing to learn new skills, systems and/or administrative procedures to support telehealth, or develop new methods of assessing or providing care to patients. During the earlier stages of the pandemic, patient numbers across the health service were substantially reduced for various reasons including closure of many outpatient clinics and cessation of elective surgeries. Some managers indicated that these lulls in activity had allowed project work to be undertaken in preparation for expected future COVID-19 case surges. This included development of resources for alternative methods of providing service, or feasibility evaluation of remote service delivery. The time was also used to upskill staff in areas of anticipated need for COVID-19 treatment.
In some areas such as newborn care and palliative care, the impact of decreased patient numbers on workload was offset by increased levels of patient distress. This was due to external stressors on patients including reduced access to family support and hospital visitor restrictions.
You spend so much time with one family, where usually you probably would not have, but they needed much more support because it was more distressing. Participant 4
Systems were refined over time to ensure that individuals were not tasked with exhaustive workloads, with this particularly evident in staff allocations for the management of COVID-19 positive patients. Decreased tolerance for work attendance with any symptoms of illness resulted in increased staff absences, further impacting workloads. This strained staffing levels and creating additional management challenges for providing optimal patient care. One manager described a further aspect of the situation:
…the expectation of the public that we are going to save everyone, that the public will get the same care that they are used to, and that the health system has an endless amount of money, which they do not, so something’s got to give. Participant 25, Manager
And commented on how these views might affect health service staff:
Are we expected to provide the same service? I do not think we can. We can do the best we can, but I am not going to ask staff to work every day, long days, not take holidays, not take weekends, because they will get sick. Participant 25, Manager
Theme 2: Personal Level: Impacts on Individual Staff
Opportunity Changes
The health service’s pandemic response created both positive and negative changes to opportunities for AH professionals. Service changes provided some clinicians with the opportunity to innovate in developing new models for clinical care, which in some cases resulted in new or expedited research opportunities. Conversely, many research projects were put on hold as part of system-wide changes to consolidate staffing and services to suppress virus transmission or to prepare the health service for the anticipated rise in COVID-19 cases. Several participants experienced increases in job satisfaction through the opportunities arising for innovation or to extend themselves within new roles:
It was a very energizing, interesting time to be working… It was really showing the workforce how resilient and adaptable we could be to still meet needs. Participant 15
However, unprompted comments expressing discontent relating to reduced opportunities for interpersonal interactions were common, with participants indicating this led to decreased job satisfaction.
Definitely less work satisfaction for me. I am a people person. I love being with people. I love interacting with my colleagues, with my MDTs [multi-disciplinary teams]. I love connecting with patients in-person. Participant 18
I sat in a room with no windows and talk to them on the phone and type on my computer and yeah, and came out every now and then and said “let me out of my cupboard! I need to get out of the cupboard!” Participant 5
Those not employed in permanent roles reported distress related to reduced job security or lost opportunity for career progression.
People are flooding into the hospital looking for that job security of the public system. I definitely thought I would get one of two permanent positions and I did not. That was pretty gutting. Participant 9
Managers acknowledged the unusually low staff turnover during the early pandemic period. However, by mid-2021, managers from many disciplines were struggling to attract and retain suitably qualified staff. A combination of external and internal factors, including additional budgetary constraints and human resources changes contributed to the situation, with managers indicating this as a significant current stressor within the workplace.
Emotional Response, Vulnerability, and Support
Many staff experienced emotional turmoil related to the threat of COVID-19 to their personal safety or the safety of loved ones. Some expressed relief at service changes that reduced their risk of exposure to the virus, such as the transition to telehealth services rather than seeing patients in person, using personal protective equipment, or working in areas not requiring direct patient contact.
I was pretty happy with the change, because again it meant less patient contact, which again at the time - The social distancing and avoiding people as much as possible - it was nice. I felt very safe. Participant 1
While some participants felt cared for, others expressed distress about the perceived lack of support received from the health service:
(It’s) not a safe place for someone that’s immunocompromised to work… I did not feel safe. I was not supported at all… You should not be made to feel like you are difficult or being challenging when you are just really trying to do the right thing by yourself and your family… it was one of the most stressful times I have ever had in my working career. Participant 7
There was notable variation in the perception of staff vulnerability and the success in accommodating this. Some managers expressed surprise at the level of concern and were skeptical about the true vulnerability of all staff claiming this status, while others appreciated the bravery of vulnerable colleagues in continuing to attend work. Some managers suggested there were no vulnerable staff within their discipline, or that all had been accommodated without issue. However, in other areas, high numbers of vulnerable individuals created difficulties in staffing activities requiring direct patient contact. Fairness of treatment was of particular concern for staff who identified as part of vulnerable populations. Managers described challenges in balancing the maintenance of open lines of communication amongst teams, with the privacy of the staff requiring accommodation.
Staff within the team are not aware of the challenges that we went through in the background and situation that we had to manage. I personally advocated for my staff. Staff do not know that. What they see is that “my line manager wasn’t supportive of my situation” and I am still dealing with those aftermaths… a year later. P23, Manager
Theme 3: Systems Level: Process of Change Management
Communication of Information
AH disciplines generally increased the frequency of internal communications during the early pandemic period, both within leadership groups and across teams. Managers noted the high utility of the Microsoft Teams virtual meeting platform, valuing the efficiencies provided by this. Nearly all participants thought the health service Executive leadership team provided comprehensive and accessible organization-wide communications through daily emails and online staff forums. However, there were some disruptions in information flow. Forum presentations often advised staff to speak with their line manager for further information, but this information had not always been provided, resulting in wasted time for managers to seek this out. At the team level, communication about plans within particular services varied extensively. Some clinicians felt very well informed of all relevant information and as a result were content with changes. Others felt that communication was disorganized, not timely or inconsistent, and consequently felt unprepared for changes.
The communication was all very last minute. No one knew anything, it was not well organized… I know there was lots of really upset staff here. I personally saw a few people in tears. Participant 16
The difficulty of working within continually changing regulations was noted by many participants, with most believing the onus was on the individual to keep up with current requirements. Participants described contradictory guidance in State-wide, local health service and department/managerial level communications. They felt challenged by this lack of consistency, especially when dealing with patients and families.
We were caught out a lot… there was period there where things were changing daily in terms of two visitors, one visitor… Participant 17
There was conflicting messaging around working from home options. Participants described requests to work from home being denied at the team level, despite State-wide health system guidance encouraging this. Managers noted that rapid policy changes meant that processes and equipment considerations were not well defined in the early stages of the pandemic. Further, operational requirements for continued onsite patient care, and additional complications in protections for vulnerable staff (as outlined in subtheme 2.2), challenged the accommodation of all work-from-home requests.
Involvement in Decision Making
The level of clinician involvement in decision making around changes to service provision differed substantially, both within and between disciplines, depending on the team or clinical area involved. Some decisions were made at AH discipline level, and others at clinical multidisciplinary team level (eg, within a hospital ward). In outpatient services, some clinicians were directed to offer appointments only by telehealth; others were given opportunity to decide if, when and for which patients telehealth would be offered; while others were denied their requests to transition their services to telehealth. Some clinician participants acknowledged receiving clear information about changes and reasons for these, but wished they’d had more opportunity to be involved in discussions about options and received reassurance and acknowledgement of their specific situations. Staff who felt involved in decision making reported positive experiences of the process.
I was involved in discussions with the directors… They were pretty good involving me in that as well and we spoke through the various different options. Participant 13
Support for Work Activity
There were varied levels of support for staff across different aspects of service change. The rapid change to remote service delivery meant workplace instructions were not always available. However, while the increased flexibility during this period may have contributed some level of risk, reduced protocol complexities and increased flexibility in choice of systems for providing telehealth consultations enhanced the user-friendliness of remote service delivery for clinicians. Access to IT support, including expertise in establishing technologies, as well as to physical resources such as webcams, was crucial to the smooth transition to providing services via telehealth.
I met with the digital engagement people. We had a bit of a briefing about what I wanted to achieve. They were a great team. I do not think I would’ve been able to do that on my own. Participant 6
Equally important was administrative support in booking, preparing, and assisting patients in utilizing the necessary technology. Participants who did not have access to this described increased workloads combined with challenges and frustrations experienced by clinicians and patients. Managers recognized the time-consuming nature of these tasks and acknowledged inefficiencies regarding the resultant additional workload placed on some clinicians.
Theme 4: Acceptance of Pandemic Circumstance
It is what it is… if this is what we need to do for a time to keep everybody safe and healthy, well, that’s what we will do. Participant 5
The extraordinary circumstances of the pandemic appeared to provide a level of acceptance for changes that otherwise would not have existed. This was expressed in staffs’ acceptance of sudden changes to their work environment, roles, and processes; and across the entire health service in tolerating change, including risks such as altering the patient care provided. Potential benefits of this were noted in the COVID-19 restrictions and requirements providing impetus for progress on long discussed change that previously seemed difficult to achieve:
I do feel that there were some very positive things to come about it because, previously, I’d felt like telehealth was not really an option. But now, it is. Participant 11
Within all manager interviews, this theme of acceptance was more powerfully expressed as a sense of embracing change. Managers described their pleasure at the “can do” attitude of many staff, their commitment, and the teamwork they observed to make change happen. They commented on how the health service had become more flexible and responsive to change as a result of the pandemic. When asked what had assisted in managing change, one participant reflected on the value of the emergent change philosophy used:
It’s about relationships, it’s about communication, it’s about transparency. It’s about keeping that open and allowing people an opportunity to come up with ideas that you can then trial, versus “here’s the idea, this is how it must be”. P24, Manager
Participants also described a high level of patient acceptance for enacted changes, including reduced services or restricted access to aspects of their or their loved ones’ care.
It felt like we were all working together and so however the service was delivered it felt like families were appreciative of the connection and the services they had. Participant 3
As the pandemic progressed, however, an increase in patient frustrations was noted with some restrictions such as visitor limits or processes (eg, being required to wear masks during therapies).
Discussion
This study explored the experiences of AH professionals employed in a large Australian hospital and health service during the early stages of the COVID-19 pandemic. Experiences were conceptualized within themes at three levels: Impacts on individual staff (personal level), impacts on service provision (service level), and the process of change management (systems level). A fourth theme of acceptance due to pandemic circumstance overlaid and influenced the experiences within each level. The findings provide unique insights into AH professionals’ experiences yielding implications for managing rapid health system change in response to pandemic threat, and more broadly in change management and supporting resilience in the health care workforce.
This study highlighted the many changes that the COVID-19 response imposed on AH services. Globally, healthcare utilization reduced by around one-third during the early months of the pandemic.10 With a low incidence of COVID-19 in Australia, this lull enabled health services to make various service changes in preparation for future expected patient waves, as was also apparent in our study. The extraordinary nature of the pandemic supported transformation, with health services appearing to hold an increased appetite for risk within the need to make swift changes. In our health service, as elsewhere, one of the most evident changes was the rapid transition to telehealth for the provision of many services. The utility of this in providing efficiencies for both patients and the health service, along with various disadvantages and challenges, were noted by many participants and align with previous research.11–13 Of key importance was providing administrative and technical support to book patients, enabling clinicians to learn new systems, and thus continuing to provide quality patient care without development of unsustainable clinician workloads. While the pandemic provided the impetus for rapid change, increasing red tape has now been noted in some centres,14 and the challenge will be in maintaining and improving the systems put in place.15,16 The onus is on health professionals and health service managers to capitalize on the benefits and advances that have been made and convert these into permanent improvements in health service delivery.
Effective control of the spread of SARS-CoV2 in Queensland meant that by the end of 2021 when data collection for our study was completed, there was no community transmission and only seven fatalities due to COVID-19 had been recorded state-wide over the previous two years.17 Despite this, health service staff still experienced significant pandemic-related stressors. Staffing numbers were strained due to reduced tolerance for work attendance with any symptoms of illness. Workloads increased due to the need for new skills and systems to support changes to service provision, and the greater support needs of patients and family members impacted by public health imposed border closures, and travel and visitor restrictions. The impacts of visitor restrictions on patients, as well as the burden on healthcare workers from the increased need to inform family members have been observed in various other settings.18 Our participants also described reduced workplace satisfaction because of decreased contact with patients and colleagues. This is perhaps unsurprising given people who are drawn to these person-orientated professions tend to have personality traits focused on relationship building.19 Concerns regarding the loss of personal connection have been similarly reported in other studies of allied health personnel over the pandemic period.20,21
Proximity to infected patients can pose threats to the health and lives of healthcare workers. In a study conducted in our hospital in 2006, 53% of staff indicated they would not attend work in the event of respiratory pandemic admissions in the absence of effective vaccines and/or antiviral medications.22 While the vast majority of staff did in fact continue to attend in this very circumstance in 2020, it was evident from our participants’ stories that many were distressed by the situation. Indeed, although our health service provided care for a relatively small number of COVID-19 patients during the study period, participants experienced similar fear for the safety of self and loved ones as described by health care workers in regions with a much higher burden of active COVID-19 cases.20,23–25 Widespread mental health effects were noted within Australian rural healthcare workforces which also experienced comparatively low COVID-19 case numbers.26 This and other studies noted an association of mental health symptoms with those working in allied health and of female gender, the predominant demographic of our study participants.26–28 An apparent contributor to distress was the disparity participants felt in the treatment of vulnerable staff, highlighting the importance of open communication and equity in management strategies. A recent study emphasized the role of organizational support on the resilience and coping of nursing staff during the pandemic, and this may also be imperative to enable sustainability in an environment of growing workforce shortages in the allied health context.29
In Queensland, decisions to temporarily suspend all non-urgent specialist outpatient services in public hospital and health services were made at the state-wide level.30 For the remaining services, risks to staff and patients and the consequent need for operational changes differed substantially between disciplines and clinical areas. Moral distress at the inability to provide care at the usual level was evident for some participants, as has been noted in other studies of health care workers during the pandemic.14,20,31–33 Amongst our participants, it was apparent that those either actively involved in or well informed about decision making for operational changes had higher contentment with the eventual outcomes. Similarly, the greater involvement of managerial staff in decision making may explain the perceived differences in accepting versus embracing change described by clinicians and managers, respectively. This observation is in alignment with numerous theoretical frameworks in change management,34–37 with inclusion of employees at all levels of the organisation in change decisions an important and commonly reported strategy in the literature in this area.38 The centrality of providing all members of an organisation with clear communication about change is also a feature of major change management models.38 Clear communication is particularly essential in times of difficulty, and the importance of maintaining these between leadership and the workforce to create shared understanding of new processes, procedures and changing priorities has been recognized elsewhere in healthcare during the COVID-19 pandemic.39
Strengths and Limitations
This study was conducted within a single health service in southeast Queensland Australia, so findings may not be generalizable to other countries or locales with different circumstances during the pandemic. While the study was open to all AH professionals at multiple sites across a large regional area, it is possible that some perspectives were not captured; however, data were collected until four subsequent interviews yielded no new themes. The research team held diverse roles and took an insider-outsider perspective, enabling an in-depth understanding of contextual factors and influences, alongside organizational and professional knowledge to reduce the likelihood of participant responses being misunderstood, while the degree of separation for some team members as non-clinician outsiders provided a complementary external viewpoint. Careful attention to confidentiality, anonymization and the use of participant checking supported confidence in participants sharing their stories honestly and openly. Triangulation of clinician data with manager interviews provided a second data point to increase confidence in findings. Targeted recruitment of staff in areas with notable service change ensured varied experiences in this were captured, while a widely circulated open invitation enabled participation of staff with a diverse range of experience. The latter may have prompted self-selection by individuals who had felt more impacted by the COVID-19 response, however, did successfully capture the views of people with extremes of both positive and negative experience.
Conclusion
This study provides a unique perspective, examining the impacts of the pandemic response and the wider impacts of the pandemic on AH professionals, in a context without community transmission of the disease and the challenges of providing care for large numbers of COVID-19 patients. Consequently, the study has implications for change management within health services in any context in which rapid change is required. The needs of the workforce must be considered at the forefront, and the mental health needs of staff prioritized. Clear communication channels are critical, and staff should feel involved in decision-making where possible. Consideration for the needs of vulnerable staff should be conducted with clear processes and eligibility guidelines to ensure both provision of appropriate support and transparency of decision making. Workloads should be monitored, and adequate support provided; for example, infrastructure, technical support and training for new initiatives or processes. Future research should evaluate the new methods of health service delivery developed and operationalized during the pandemic, assessing acceptability, safety, and cost-effectiveness.
Data Sharing Statement
The datasets generated during this study are not available due to the sensitive and personal nature of the information contained. Data may be available upon justified request from the corresponding author with restrictions and following ethical approval.
Ethics Approval and Informed Consent
This study was performed in accordance with the Declaration of Helsinki. Ethical approval was granted by the Gold Coast Hospital and Health Service Human Research Ethics Committee (HREC/2020/QGC/67379). All participants provided written and informed consent prior to study involvement.
Acknowledgments
The authors thank the interview participants for giving up their time to take part in this study. This paper was presented at the Australian 15th National Allied Health Conference as a poster presentation with interim findings, abstract available at https://nahc.com.au/8730.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Gold Coast Health Study, Education and Research Trust Account (SERTA).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Australian Government. Australian Health Sector Emergency Response Plan for Novel Coronavirus (COVID-19). Department of Health, Commonwealth of Australia: Canberra, Australia. Available from: https://www.health.gov.au/sites/default/files/documents/2020/02/australian-health-sector-emergency-response-plan-for-novel-coronavirus-covid-19_2.pdf.
2. Stobart A, Duckett S. Australia’s Response to COVID-19. Health Econ Policy Law. 2022;17(1):95–106. doi:10.1017/S1744133121000244
3. Grol R, Wensing M, Eccles M, Davis D, editors. Improving Patient Care: The Implementation of Change in Health Care. John Wiley & Sons, Ltd; 2013.
4. Chemali S, Mari-Sáez A, El Bcheraoui C, Weishaar H. Health care workers’ experiences during the COVID-19 pandemic: a scoping review. Hum Resour Health. 2022;20(1):27. doi:10.1186/s12960-022-00724-1
5. Allied Health Professions Australia. What is Allied Health? Melbourne, Victoria. Available from: https://ahpa.com.au/what-is-allied-health/.
6. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
7. Dwyer SC, Buckle JL. The Space Between: on Being an Insider-Outsider in Qualitative Research. Int J Qual Methods. 2009;8(1):54–63. doi:10.1177/160940690900800105
8. Galletta A. Mastering the Semi Structured Interview and Beyond: From Research Design to Analysis and Publication. New York: NYU Press; 2013.
9. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
10. Moynihan R, Sanders S, Michaleff ZA, et al. Impact of COVID-19 pandemic on utilisation of healthcare services: a systematic review. BMJ Open. 2021;11(3):e045343. doi:10.1136/bmjopen-2020-045343
11. Cottrell M, Burns CL, Jones A, et al. Sustaining allied health telehealth services beyond the rapid response to COVID-19: learning from patient and staff experiences at a large quaternary hospital. J Telemed Telecare. 2021;27(10):615–624. doi:10.1177/1357633X211041517
12. Eddison N, Leone E, Healy A, Royse C, Chockalingam N. The potential impact of allied health professional telehealth consultations on health inequities and the burden of treatment. Int J Equity Health. 2022;21(1):91. doi:10.1186/s12939-022-01689-2
13. Tukur M, Saad G, AlShagathrh FM, Househ M, Agus M. Telehealth interventions during COVID-19 pandemic: a scoping review of applications, challenges, privacy and security issues. BMJ Health Care Inform. 2023;30(1). doi:10.1136/bmjhci-2022-100676
14. Borek AJ, Pilbeam C, Mableson H, et al. Experiences and concerns of health workers throughout the first year of the COVID-19 pandemic in the UK: a longitudinal qualitative interview study. PLoS One. 2022;17(3):e0264906. doi:10.1371/journal.pone.0264906
15. Thomas EE, Taylor ML, Ward EC, et al. Beyond forced telehealth adoption: a framework to sustain telehealth among allied health services. J Telemed Telecare. 2022:1357633X221074499.
16. Wong A, Bhyat R, Srivastava S, Lomax LB, Appireddy R, Lomax L. Patient Care in the COVID-19 Pandemic: the Use of Virtual Care. J Med Internet Res. 2021;23(1):e20621. doi:10.2196/20621
17. Australian Government. Coronavirus (COVID-19) at a glance – 31 December 2021. Department of Health and Aged Care. Commonwealth of Australia. Available from: https://www.health.gov.au/resources/publications/coronavirus-covid-19-at-A-glance-31-december-2021?language=en.
18. Hugelius K, Harada N, Marutani M. Consequences of visiting restrictions during the COVID-19 pandemic: an integrative review. Int J Nurs Stud. 2021;121:104000. doi:10.1016/j.ijnurstu.2021.104000
19. Campbell N, Eley DS, McAllister L. Investigating personality and conceptualising allied health as person or technique oriented. Aust Health Rev. 2014;38(1):86–92. doi:10.1071/AH13109
20. Digby R, Winton Brown T, Finlayson F, Dobson H, Bucknall T. Hospital staff well‐being during the first wave of COVID‐19: staff perspectives. Int J Ment Health Nurs. 2021;30(2):440–450. doi:10.1111/inm.12804
21. Goff SL, Wallace K, Putnam N, et al. A Qualitative Study of Health Workers’ Experiences During Early Surges in the COVID-19 Pandemic in the U.S. Implications for Ongoing Occupational Health Challenges Front Public Health. 2022;10:780711.
22. Martinese F, Keijzers G, Grant S, Lind J. How would Australian hospital staff react to an avian influenza admission, or an influenza pandemic? Emerg Med Australas. 2009;21(1):12–24. doi:10.1111/j.1742-6723.2008.01143.x
23. Huerta-González S, Selva-Medrano D, López-Espuela F, Caro-Alonso P, Novo A, Rodríguez-Martín B. The Psychological Impact of COVID-19 on Front Line Nurses: a Synthesis of Qualitative Evidence. Int J Environ Res Public Health. 2021;18(24):12975. doi:10.3390/ijerph182412975
24. Qureshi I, Gogoi M, Al-Oraibi A, et al. Factors influencing the mental health of an ethnically diverse healthcare workforce during COVID-19: a qualitative study in the United Kingdom. Eur J Psychotraumatol. 2022;13(2):2105577. doi:10.1080/20008066.2022.2105577
25. Koontalay A, Suksatan W, Prabsangob K, Sadang JM. Healthcare Workers’ Burdens During the COVID-19 Pandemic: a Qualitative Systematic Review. J Multidiscip Healthc. 2021;14:3015–3025. doi:10.2147/JMDH.S330041
26. Tham R, Pascoe A, Willis K, Kay M, Smallwood N. Differences in psychosocial distress among rural and metropolitan health care workers during the COVID 19 pandemic. Aust J Rural Health. 2022;30(5):683–696. doi:10.1111/ajr.12873
27. Gillen P, Neill RD, Mallett J, et al. Wellbeing and coping of UK nurses, midwives and allied health professionals during COVID-19-A cross-sectional study. PLoS One. 2022;17(9):e0274036. doi:10.1371/journal.pone.0274036
28. Smallwood N, Karimi L, Bismark M, et al. High levels of psychosocial distress among Australian frontline healthcare workers during the COVID-19 pandemic: a cross-sectional survey. Gen Psychiatr. 2021;34(5):e100577. doi:10.1136/gpsych-2021-100577
29. Ahmed FR, Bani-Issa W, Timmins F, et al. Managing during the COVID-19 pandemic: a cross-sectional study of health care workers’ perceived organizational support and its consequences on their compassion, resilience and turnover intention. J Nurs Manag. 2022;30(7):2642–2652. doi:10.1111/jonm.13824
30. State of Queensland (Queensland Health). Unleashing the potential: an open and equitable health system Healthcare for Queenslanders in a pandemic ready world. Reform Planning Group - Final Report. Brisbane, Queensland; 2020. Available from: https://www.health.qld.gov.au/__data/assets/pdf_file/0029/1143479/Unleashing-The-Potential-An-open-and-equitable-health-system.pdf.
31. Bradshaw A, Dunleavy L, Garner I, et al. Experiences of staff providing specialist palliative care during COVID-19: a multiple qualitative case study. J R Soc Med. 2022;115(6):220–230. doi:10.1177/01410768221077366
32. Castle M, O’Hagan R, Anderberg E, Wangman A, Harrington H, Dhakal L. About face: regional allied health professional early adaptation during the COVID-19 pandemic. Aust J Prim Health. 2022;28(2):110–116. doi:10.1071/PY21150
33. Smallwood N, Pascoe A, Karimi L, Willis K. Moral Distress and Perceived Community Views Are Associated with Mental Health Symptoms in Frontline Health Workers during the COVID-19 Pandemic. Int J Environ Res Public Health. 2021;18(16):56.
34. Kotter J. Leading Change. Boston: Harvard Business Review Press; 2012.
35. Bridges W. Managing Transitions: Making the Most of Change. Reading, Massachusetts: Perseus Books; 1991.
36. Lewin K. Field Theory in Social Science: Selected Theoretical Papers. New York: Harper & Brothers Publishers; 1951.
37. Hiatt J. ADKAR: A Model for Change in Business, Government, and Our Community. Loveland, Colorado: Prosci Learning Publications; 2006.
38. Phillips J, Klein JD. Change Management: from Theory to Practice. TechTrends. 2023;67(1):189–197. doi:10.1007/s11528-022-00775-0
39. Osgood JM, Froude JW, Daye SP, et al. Cross-Cutting Lessons Learned During the COVID-19 Pandemic-The Walter Reed Army Institute of Research Experience. Mil Med. 2023;188(1–2):158–165. doi:10.1093/milmed/usab438
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.