Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Impacts of Huddle Intervention on the Patient Safety Culture of Medical Team Members in Medical Ward: One-Group Pretest-Posttest Design
Authors Lai YH, Wu MJ ![]() , Chen HH
, Chen HH ![]() , Lin SP, Wu CY
, Lin SP, Wu CY ![]() , Chin CS
, Chin CS ![]() , Lin CH, Shiu SI, Lin YC, Chen HC, Hou SC, Chang CW
, Lin CH, Shiu SI, Lin YC, Chen HC, Hou SC, Chang CW
Received 7 August 2023
Accepted for publication 17 November 2023
Published 23 November 2023 Volume 2023:16 Pages 3599—3607
DOI https://doi.org/10.2147/JMDH.S434185
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Scott Fraser
Yi-Hung Lai,1,2 Ming-Ju Wu,3 Hsin-Hua Chen,4,5 Shih-Ping Lin,4,6 Chun-Yi Wu,3,4 Chun-Shih Chin,4,7 Cheng-Hsien Lin,4,8 Sz-Iuan Shiu,4,9 Ying-Cheng Lin,4,9 Hui-Chi Chen,1 Shu-Chin Hou,1 Ching-Wein Chang1
1Department of Nursing, Taichung Veterans General Hospital, Taichung, Taiwan; 2Department of Nursing, National Taipei University of Nursing and Health Sciences, Taipei, Taiwan; 3Division of Nephrology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 4Division of General Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 5Division of Allergy, Immunology and Rheumatology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 6Division of Infection, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 7Division of Chest Medicine, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 8Division of Hematology and Oncology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan; 9Division of Gastroenterology, Department of Internal Medicine, Taichung Veterans General Hospital, Taichung, Taiwan
Correspondence: Ching-Wein Chang, Department of Nursing, Taichung Veterans General Hospital, 1650 Taiwan Boulevard Sect. 4, Taichung, 40705, Taiwan, Email [email protected]
Objective: A huddle is a short, regular meetings to discuss existing or emerging patient safety issues. Hospital administrators can encourage healthcare staff to voluntarily examine the potential occurrence and severity of risks, thereby enhancing awareness of patient safety. The purpose of this study is to explore the effects of huddle intervention on patient safety culture among medical team members and related factors.
Methods: We used a one-group pretest-posttest research design and convenience sampled 109 members of the general internal medicine ward team members from a medical center in central Taiwan. They participated 2 times per week in 15-min huddles from 08:15 to 08:30 in the morning, which lasted for a total of 4 weeks. The process was based on submitted ideas, approved ideas, research ideas and standardization, and data on the safety attitudes questionnaire (SAQ) were collected during the huddles’ intervention pretest and posttest.
Results: After the huddle intervention, we found significantly improved scores for safety attitude, teamwork climate (76.49± 16.13 vs 83.26± 13.39, p < 0.001), safety climate (75.07± 16.07 vs 82.63± 13.72, p < 0.001), job satisfaction (73.67± 19.84 vs 83.39± 17.21, p < 0.001), perceptions of management (77.87± 19.99 vs 84.86± 16.03, p < 0.001) and working conditions (78.96± 18.16 vs 86.18± 14.90, p < 0.001). Correlation analyses on the differences between pretest and posttest showed that age had a significant correlation with safety climate (r = 0.22, p = 0.022) and working conditions (r = 0.20, p = 0.035). The number of times to participate in a huddle had a significant correlation with teamwork climate (r = 0.33, p =< .001), safety climate (r = 0.30, p = 0.002), job satisfaction (r = 0.19, p = 0.043), and work conditions (r = 0.28, p = 0.003).
Conclusion: Huddles improve clinical team members’ understanding of different dimensions and relate factors of safety attitudes. Implementation of the huddles involved standardized process will help hospital administrators understand the steps to parallel expansion to other wards.
Keywords: huddle, patient safety, patient care team
Introduction
The latest huddle practice evidence recommends conducting structured daily huddle, use of a huddle-guiding tool, same time and location and no longer than 15 min,1–4 provides team members with regular meetings each day to connect with each other, to brief periodic reports and to engage frontline staff with leaders to discuss existing or emerging patient safety issues.5 Huddle also supports open communication among clinical, administrative, and technical staff with a blame-free culture that allows for changes to daily workflow, manages crises beforehand, and makes adjustments to improve patient accessibility and staff quality of life.6,7 Chapman et al5 demonstrated that the huddle has increased situational awareness, safety awareness, communication, and teamwork, implementing solutions faster and more efficiently, and is a feasible intervention to improve patient safety.8 Huddles are usually moderated by a member of the team, who may be a leader, manager, or person in charge, whose job is to ensure that the meeting remains focused, runs smoothly, and ensures that all participants have the opportunity to participate. Moderators may rotate from meeting to meeting to ensure that each member participates in the duties of the moderator. Teams can adapt the following Institute for Healthcare Improvement (IHI) standard five-item huddle agenda to their own needs and choose the flow that works best for them, including (1) safety and quality concerns and successes in the past day or shift, (2) safety and quality issues for patients on today’s schedule, (3) review of tracked issues, (4) inputs on other safety and quality issues, and (5) announcements and information to share.3 Therefore, Huddles provide a channel for information dissemination that directly affects a unit. The evidence-based approach to solving the problem of a lack of a structured huddle streamlined the process of finding a solution.
Patient safety in the healthcare process involves necessary measures aimed at preventing and reducing risks, errors, and harm to patients during the course of medical care. This includes preventing mistakes, reducing errors, and avoiding accidents.9 The concept of “patient safety culture” encompasses the essential measures taken during healthcare to prevent or mitigate adverse outcomes or harm to patients, including error, bias, and accidents.10 It is constituted by the values, attitudes, capabilities, and behavioral patterns of individuals and groups, determining an organization’s commitment and actions toward safety.11 Hospital administrators can use patient safety culture to encourage healthcare staff to voluntarily examine the potential occurrence and severity of risks, thereby enhancing awareness of patient safety.12 An ideal patient safety culture scale can help understand the overall safety climate of the unit by evaluating the attitudes of many individuals in the work unit to patient safety and then understanding the patient safety culture of the entire institution.13 The safety attitudes questionnaire (SAQ) was developed by Sexton et al,14 was introduced to Taiwan in 2007 and translated into Chinese by Lee et al.15 In 2009, the Taiwan Medical Association (JCT) extended the survey to all national hospitals, calling it the Taiwan Patient Safety Culture (TPSC) survey.16 Over the past decade, medical institutions in Taiwan have placed great importance on establishing a patient safety culture. The Patient Safety Culture survey reflects the attitudes and perceptions of employees in various professions toward safety culture, becoming one of the ways for medical institutions to enhance the quality of healthcare and reduce the occurrence of medical errors.17
A recent systematic review concluded that “the present body of research related to such huddles demonstrates a generally positive impact on safety”.1,18 Despite the evidence on the impact of huddles on patient outcomes and patient satisfaction,1,8 there is a dearth of literature on the impact of huddles on health care team members’ safety attitudes and their associated factors. However, there is currently no medical unit in Taiwan that uses huddle intervention to explore related research on patient safety culture. Therefore, the primary aim of our study was to explore the effects of huddle intervention on patient safety culture among medical team members. The secondary aim was to explore related factors of huddle intervention on patient safety culture among medical team members and then pose the following research question:
- Impact of huddles intervention on patient safety attitudes of medical team members?
- Are there any associations between basic attributes of team members (age, gender, job category, working years), number of participation in huddles and patient safety attitudes of huddle intervention?
Methods
Research Design
We adopted a quantitative single-group pretest and posttest research design that was approved by the Medical Ethics and Institutional Review Board (No. CE21453B). We used convenience sampling of members of the general internal medicine ward team from a medical center in central Taiwan. Participants included physicians, nurses and other team members at all levels of the unit, such as administrative staff, cleaning staff, orderly staff, nursing students and teachers. Because the training of resident doctors in our hospital rotates every month, it will take a total of seven months from December 1, 2021, to June 30, 2022, to reach a sufficient number of samples. A total of 109 participants were included in this study. The sample number was estimated using G-Power 3.1 statistical software. Referring to Zeng et al19 study on the average differences in scores between pre- and posttests of patient safety attitudes, the α value was set to 0.05, and the power coefficient was 0.8. A total of 109 participants were included in this study.
Intervention Measures
The huddle location is in the ward conference room, and everyone will be required to stand up. This is mainly to force everyone to put down the work at hand, concentrate on sharing, listen to other people’s work progress and obstacles, and solve problems quickly. Team members participated in Huddle twice a week (every Wednesday and Friday), from 08:15 to 08:30 in the morning, each time for 15 min, for a total of 4 weeks, we always started and ended the team huddles on time to ensure reliability and consistency. Each participant filled out the “Safety Attitude Questionnaire” for the pretest within three days before the huddle intervention and completed the posttest within three days after the huddle intervention.
The director of the ward was initially the huddle leader, and then the leadership was rotated among attending physicians in the ward to strengthen their sense of participation. The huddles hold time during the working hours of the hospital in Taiwan, which is the night shift and day shift job handover time, to ensure that the two shift members of the medical team can participate together. Even so, some doctors and nurses are not on duty at huddle time. Therefore, a huddle board was installed in the ward meeting room, and all staff were able to freely post on the board with sticky notes, any issue that needed improvement, and hold was simultaneous with the hybrid for those not attending to boost engagement. The huddle process was placed on the huddle boards, according to the IHI as idea submitted, idea approved, working on idea, and standardizing.3 All staff were able to freely post on the board with sticky notes, any issue that needed improvement, and review focus on issues raised.
Research Tools
Safety Attitude Scale
Since 2007, the Medical Policy Council has adopted Dr. Wei-Chiang Lee’s translated Chinese version of the hospital Safety Attitude Scale (SAQ) as first developed by Dr. Sexton.14 The SAQ has 30 items distributed within 6 dimensions. Specifically, there are 6 items in the dimension teamwork climate; 7 items in safety climate; 5 items in job satisfaction; 4 items in stress recognition; 4 items in perceptions of management; and 4 items in working conditions. Scores are stratified into 5 grades, with 20 representing strongly disagree; 40, somewhat disagree; 60, neutral; 80, somewhat agree; and 100, strongly agree. Teamwork climate is used to assess the degree to which participants feel about the teamwork of peers in the unit. Safety climate is used to assess the degree to which participants feel about the organization’s safety commitment. Job satisfaction is used to evaluate the degree to which participants have positive thoughts about their work compassion. Stress recognition is used to assess the level of awareness of participants of the effects of stress on work performance. Perceptions of management are used to evaluate the degree to which participants agree with the manager’s behavior. Working conditions are used to evaluate how participants feel about the working environment and resources provided.20 SAQ reliability analysis shows that the internal consistency of the six aspects of SAQ is very good (component reliability 0.77∼0.93).15
Data Analyses
The first author is responsible for collecting and processing the basic information of the participants, and the use or publication of the data will keep the privacy of the participants’ information absolutely confidential. Using SPSS (version 24.0) statistical software, our descriptive statistics included number, percentage, median, mean, and standard deviation. For inferential statistical analyses, we used the paired sample t-test, Mann‒Whitney U-test, Kruskal‒Wallis test, and Pearson correlation for verification. Statistical significance was set at p <0.05.
Results
Participant Attributes
The average age of the team members was 28.89 years old (standard deviation, SD: 7.80); gender was predominantly female (66.97%); average working experience was 4.86 years (SD: 7.34); 102 (93.58%) had a university degree or above; and the majority of them were nurses (55.96%); number of participation in huddles average 6 times (Table 1).
 |
Table 1 Participant Attributes (N = 109) |
Patient Safety Attitude
We found that posttest scores of all aspects of patient safety attitudes were higher than those of the pretest, with the only exception being stress recognition. Those improved aspects included teamwork climate (76.49±16.13 vs 83.26±13.39, p < 0.001), safety climate (75.07±16.07 vs 82.63±13.72, p < 0.001), job satisfaction (73.67±19.84 vs 83.39±17.21, p < 0.001), perceptions of management (77.87±19.99 vs 84.86±16.03, p < 0.001), working conditions (78.96±18.16 vs 86.18±14.90, p < 0.001) (Table 2).
 |
Table 2 Patient Safety Attitude (N = 109) |
Correlation Analysis of Participant Attributes and Pretest and Posttest Differences in Safety Attitudes
There is no significant correlation between gender, job category, work experience, and the differences in safety attitudes pretest and posttest (p > 0.05) (Table 3 and Table 4). Therefore, the measurement of safety attitudes at different time points was not affected by gender, job category, or working years. There is a significant positive correlation between age and safety climate (r = 0.22, p = 0.022) and working conditions (r = 0.20, p = 0.035). This means that the older the person was, the higher the score progress of safety climate and working conditions after the huddle intervention. The number of times participating in huddles had a significant positive correlation with teamwork climate, safety climate, job satisfaction and working conditions. That is, the more times participants participated in huddles, the higher the score progress in teamwork climate (r = 0.33, p =<.001), safety climate (r = 0.30, p = 0.002), job satisfaction (r = 0.19, p = 0.043) and working conditions (r = 0.28, p = 0.003) (Table 4).
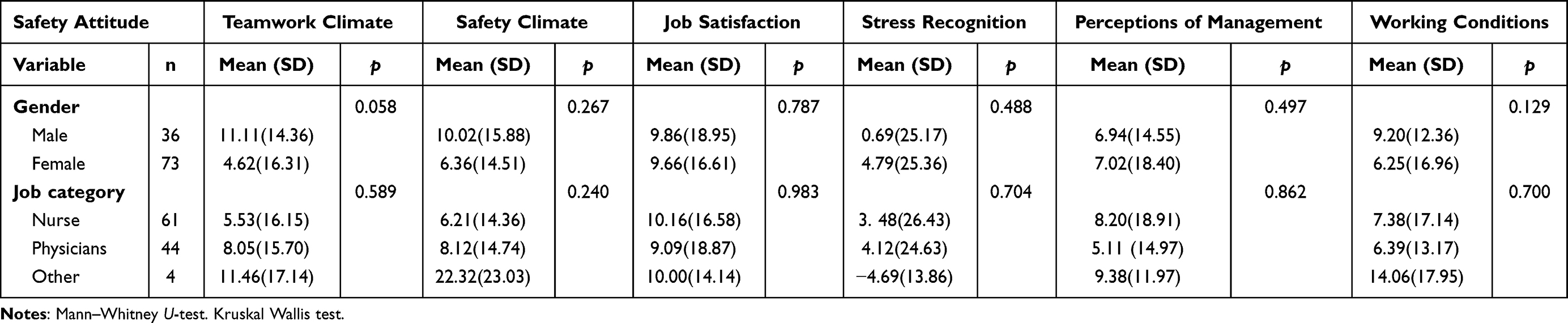 |
Table 3 Correlation Analysis of Gender, Job Category and Pretest and Posttest Differences of Safety Attitude (N = 109) |
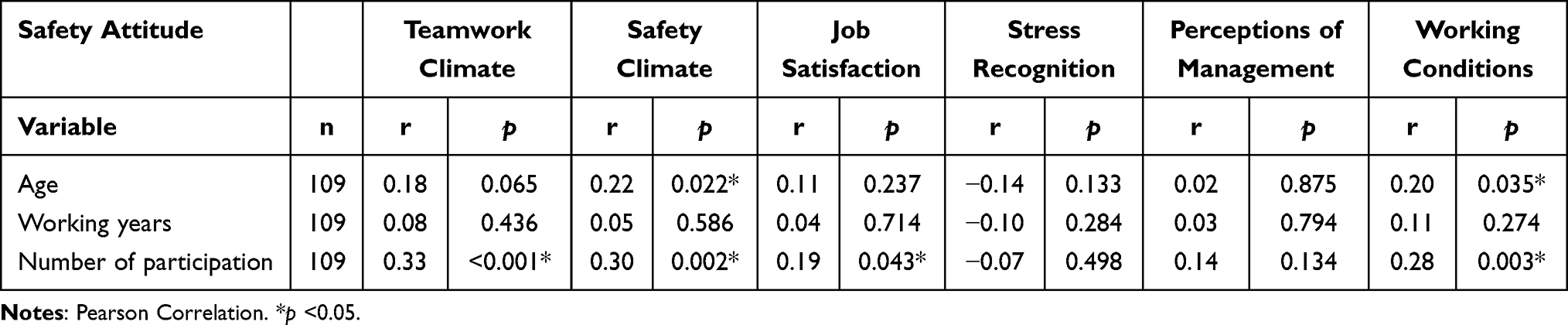 |
Table 4 Correlation Analysis of Age, Working Years, Number of Participation and Pretest and Posttest Differences of Safety Attitude (N = 109) |
Discussion
Huddle runs were held from December 1, 2021, to June 30, 2022, 26 issues were identified and resolved, among them 16 (61%) issues were identified by clinical doctors, 9 (35%) by nurses and medical assistants, and 1 (4%) by nursing students. The majority issues were communication (n = 8, 30.8%), clinical care (n = 7, 26.9%), information technology systems (n = 5, 19.2%), policy documentation (n = 2; 7.7%), equipment/safe environment (n = 2, 7.7%), and others issues (n = 2, 7.2%). Issue example for communication was used ISBAR techniques to communicate with the team when patient status changes. Example for clinical care was malignant fungating wound care responsibilities for cancer patients. We did huddles not daily but twice a week. However, most literature huddles are conducted on a daily basis, 67.7% of studies described huddles used to improve team communication, collaboration, and/or coordination, huddles positively impacted team process outcomes in 67.7% of studies.21 Our research focuses on the agenda of specific safety goals, most of the questions were about communication and clinical care, and the vast majority of staff responded positively at huddles. It was a good start for the whole team to meet and discuss work processes and expectations, which helped us understand and appreciate each other’s work more.
We found that huddle intervention affected the safety attitude of the medical team by improving their Teamwork Climate, Safety Climate, Job Satisfaction, Perceptions of Management, and Working Conditions scores. Our results are consistent with those of Aldawood et al,2 who used Huddle to improve patient safety responsiveness. Regarding teamwork climate, huddles provide more opportunities for team members to meet and discuss certain issues and help increase confidence in patient safety practices to enhance perceptions of peer teamwork within the unit. Sixty-five percent of team members mentioned the benefits of huddles to increase teamwork, and said Nursing and medical staff members mentioned that taking part in the huddle had made them feel more like one team working together on the ward, rather than separate teams.22 It is also consistent with the systematic review that pointed out that huddles have a significant positive impact on teamwork by Rowan et al.8 Regarding safety climate, since huddles hold was simultaneous with hybrid for members on vacation or night shift, the huddle board has appropriate channels to directly respond to issues related to patient safety. Therefore, when problems arise at work, unit personnel are more willing to raise issues and work together to resolve them to gain a level of commitment to organizational safety. Eighty-five percent of teams pointed out that huddles can raise awareness, ensured that a range of perspectives could be clarified within the wider staff group, to avoid misinterpretation of information heard “on the grapevine”, thereby improving an organization’s ability to deal with safety issues.22 Job satisfaction is known to be related to many factors, including decision-making autonomy, effective communication between employees and supervisors, and the ability to express opinions freely.23 These factors can be reached by implementing huddles, thereby improving the degree of positive thinking among colleagues in the unit. This is consistent with the research finding that huddles have a significant positive impact on teamwork and job satisfaction in multidisciplinary healthcare teams; however, the literature also points out that non-huddlers team members express “challenging interpersonal dynamics among team members”8 After implementing huddling, the stress recognition scores of our team members did not increase significantly. The possible reason is that the intervention measures in this study lasted only four weeks. Each person’s ability, personality, life background, stressful events, coping methods, etc., will have a long-term impact on stress cognition and have a greater impact than the surrounding safety culture, and this finding is consistent with those of Zhou et al.20 Regarding perceptions of management, physicians’ participation and leadership are key to the success of huddles. Frontline staff were able to freely discuss daily patient safety issues with unit leaders, making timely improvements. Colleagues in the unit were able to recognize and accept the manager’s behavior. Regarding work conditions, huddles were able to be widely embedded in the daily work of the ward, and team members also proposed that working hours, work remuneration, physical condition loading and psychological needs were also included in the discussion, thus deepening the staff’s feelings about the working environment and resources.
The pretest and posttest differences in safety attitudes after the huddle intervention are not affected by the gender, job category, and working years of the team members. The older the age, the more significant the progress of safety climate and work conditions after huddle intervention. This finding is, however, inconsistent with the study results of Lin et al,24 showing that the younger the age is, the more positive the safety attitude. The possible reason for such a discrepancy is that the older the age, the greater their work familiarity, so they communicate and consult with team members in various departments. When they are good at huddle, they detect problems earlier and come up with solutions. Therefore, they would reduce errors and improve department operations. The number of times participating in the huddle, the greater the improvements in teamwork climate, safety climate, job satisfaction, and work conditions. The possible reason is that with more participation, they are more familiar with the huddle process, and members will be less hesitant in asking questions on potential safety issues. Revising the SOP through consensus and synchronously publicizing results in the unit group helped strengthen teamwork. Frontline staff were authorized by huddles to respond more quickly to patient care and take preventive measures to establish positive organizational safety. Under such an atmosphere, questions raised by any team member were all accepted and valued. Thus, job satisfaction increased, and in the face of excessive workload, seeking reasonable resources at the meeting could improve the working environment.
Limitations and Recommendations
Huddle intervention was implemented in the general internal medicine ward of our hospital with a single group pretest and posttest design. Since there is no control group for comparison, the results of the intervention may be affected by the practice effect of the pretest, sensitivity to posttest content, and fatigue effects. We suggest that future research adopt an experimental and quasi-experimental research design to overcome this weakness. The ward team members who did not implement huddles were included in the study as the control group for comparison to highlight the objective effectiveness of huddles.
Conclusion
Our study found that implementing non-daily huddles, it also improves clinical team members’ understanding of different dimensions and related factors of safety attitudes, will help hospital administrators understand the steps to implement in other ward units and factors that may hinder the development of patient safety culture.
Data Sharing Statement
All data are available upon reasonable request from the corresponding author.
Ethical Approval
The study was approved by the Institutional Review Board at Taichung Veterans General Hospital. This study was conducted in accordance with the World Medical Association (WMA) Declaration of Helsinki. Informed consent was obtained from all subjects involved in the study.
Acknowledgments
The authors would like to thank the team members participating in this study at Taichung Veterans General Hospital. The source of reference for the research questionnaire is the Joint Commission of Taiwan. The Taiwan Patient Safety Culture (TPSC) questionnaire is a national safety cultural network survey system built by reference to the internationally credible Safety Attitude Questionnaire (SAQ) cultural survey tool. The interpretations and conclusions made in this article do not represent the position of the Joint Commission of Taiwan.
Funding
This study has not received any external funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Murphy V. Daily huddle best practice: an evidence-based guide. Worldviews Evid Based Nurs. 2023;20(5):513–518. doi:10.1111/wvn.12668
2. Aldawood F, Kazzaz Y, AlShehri A, Alali H, Al-Surimi K. Enhancing teamwork communication and patient safety responsiveness in a paediatric intensive care unit using the daily safety huddle tool. BMJ Open Qual. 2020;9(1):e000753. doi:10.1136/bmjoq-2019-000753
3. Institute for Healthcare Improvement. Huddles. Available from: http://www.ihi.org/resources/Pages/Tools/Huddles.aspx.
4. Rodriguez HP, Meredith LS, Hamilton AB, Yano EM, Rubenstein LV. Huddle up!: the adoption and use of structured team communication for VA medical home implementation. Health Care Manag Rev. 2015;40(4):286–299. doi:10.1097/hmr.0000000000000036
5. Chapman LR, Molloy L, Wright F, et al. Implementation of situational awareness in the pediatric oncology setting. does a “huddle” work and is it sustainable? J Pediatr Nurs. 2020;50:75–80. doi:10.1016/j.pedn.2019.10.016
6. Stewart EE, Johnson BC. Improve office efficiency in mere minutes. Fam Pract Manag. 2007;14(6):27–29.
7. Menon S, Singh H, Giardina TD, et al. Safety huddles to proactively identify and address electronic health record safety. J Am Med Inform Assoc. 2017;24(2):261–267. doi:10.1093/jamia/ocw153
8. Rowan BL, Anjara S, De Brún A, et al. The impact of huddles on a multidisciplinary healthcare teams’ work engagement, teamwork and job satisfaction: a systematic review. J Eval Clin Pract. 2022;28(3):382–393. doi:10.1111/jep.13648
9. World Health Organization. Patient safety. Available from: https://www.who.int/news-room/fact-sheets/detail/patient-safety.
10. Taiwan Patient Safety Net. Taiwan patient safety reporting system. Available from: https://www.patientsafety.mohw.gov.tw/xmfile?xsmsid=0M098412292297480494.
11. Nieva VF, Sorra J. Safety culture assessment: a tool for improving patient safety in healthcare organizations. Qual Saf Health Care. 2003;12(Suppl 2):ii17–ii23. doi:10.1136/qhc.12.suppl_2.ii17
12. Wu HH. Assessing the patient safety culture in a healthcare organization through safety attitudes questionnaire. Qual J. 2021;57(9):8–11.
13. Lee WC. The applications of safety culture surveys on patient safety improvement. Taiwan Crit Care Med. 2007;8(4):175–183. doi:10.30035/TCCM.200712.00047
14. Sexton JB, Helmreich RL, Neilands TB, et al. The Safety Attitudes Questionnaire: psychometric properties, benchmarking data, and emerging research. BMC Health Serv Res. 2006;6(1):44. doi:10.1186/1472-6963-6-44
15. Lee W, Chen S, Cheng Y, Huang T, Lee C, Lee S. Validation study of the Chinese safety attitude questionnaire in Taiwan. Taiwan J Public Health. 2008;27(3):214–222.
16. Lee WC, Wung HY, Liao HH, et al. Hospital safety culture in Taiwan: a nationwide survey using Chinese version Safety Attitude Questionnaire. BMC Health Serv Res. 2010;10(1):234. doi:10.1186/1472-6963-10-234
17. Jeong HJ, Lee WC, Liao HH, Chu FY, Chen TJ, Wang PC. The Hospital Patient Safety Culture Survey: reform of analysis and visualization methods. Int J Environ Res Public Health. 2019;16(19):3624. doi:10.3390/ijerph16193624
18. Franklin BJ, Gandhi TK, Bates DW, et al. Impact of multidisciplinary team huddles on patient safety: a systematic review and proposed taxonomy. BMJ Qual Saf. 2020;29(10):1–2. doi:10.1136/bmjqs-2019-009911
19. Tseng WC, Cheng CH, Wang TH, Lai SY, Wang YC, Wang PC. Establishment of a patient safety culture in the Radiology Department. Fu-Jen J Med. 2009;7(3):131–139.
20. Chou DW, Lai FT, Li CH, et al. The impact on patient safety culture in the intensive care unit using term resource management. Hospital. 2013;46(4):32–41.
21. Pimentel CB, Snow AL, Carnes SL, et al. Huddles and their effectiveness at the frontlines of clinical care: a scoping review. J Gen Intern Med. 2021;36(9):2772–2783. doi:10.1007/s11606-021-06632-9
22. Stapley E, Sharples E, Lachman P, Lakhanpaul M, Wolpert M, Deighton J. Factors to consider in the introduction of huddles on clinical wards: perceptions of staff on the SAFE programme. Int J Qual Health Care. 2018;30(1):44–49. doi:10.1093/intqhc/mzx162
23. Bhatnagar K, Srivastava K. Job satisfaction in health-care organizations. Ind Psychiatry J. 2012;21(1):75–78. doi:10.4103/0972-6748.110959
24. Lin SM, Chiu YC, Chan SY, et al. The relationship between Hospital Employee Attributes and patient safety culture. Taipei City Med J. 2020;17(1):87–105. doi:10.6200/tcmj.202003_17(1).0008
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.