")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Impact on patient satisfaction and importance of medical intake and office staff in a multidisciplinary, one-stop shop transgender program in Indianapolis, Indiana
Authors Nowaskie DZ , Fogel RS, Fogel JM
Received 24 May 2019
Accepted for publication 2 July 2019
Published 15 August 2019 Volume 2019:12 Pages 665—673
DOI https://doi.org/10.2147/JMDH.S216969
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dustin Z Nowaskie, 1 Rachel S Fogel, 2 Janine M Fogel 3
1Department of Psychiatry, Indiana University School of Medicine, Indianapolis, IN, USA; 2Center for Virology and Vaccine Research, Beth Israel Deaconess Medical Center, Boston, MA, USA; 3Transgender Health & Wellness Program, Eskenazi Health, Indianapolis, IN, USA
Background: Historically, the transgender population has postponed seeking primary care due to discrimination within social and medical settings. Very few studies have considered patient satisfaction with transgender care and whether there are differences in staff satisfaction. This cross-sectional study focuses on the satisfaction of transgender patients who receive primary care at a comprehensive, “one-stop shop” program in Indianapolis, IN, USA.
Methods: Sixty-two patients completed a patient satisfaction survey. Items consisted of 5-point Likert scales with anchors of satisfaction, caring, competence, and doctor recommendation.
Results: Overall, there were positive responses to all items, ranging from moderately high to very high. There was high overall satisfaction in the program’s trans-friendliness, office visits, and “one-stop shop” model. Lower scoring items concerned medical intake with appointment making and timing. There were no statistical differences across age, gender, education, duration at the program, and number of visits in the past 12 months. There were clear differences between how respondents viewed the care and competence of the program’s staff. In particular, the doctor was viewed most positively and office staff least positively with medical staff rated in-between.
Conclusion: There is high patient satisfaction with this comprehensive, “one-stop shop” care model among the transgender population. We recommend that transgender programs routinely conduct quality improvement measures, maintain sufficient workforce coverage, and provide cultural competency training which should include appropriate care standards and patient-centered concerns regarding appointment making and burdens associated with timing, traveling, and cost.
Keywords: cultural competency, minority health, multidisciplinary research, patient satisfaction, quality of care, transgender persons
Corrigendum for this paper has been published
Background
In the United States (US), nearly 1.4 million adults (0.6% of the population) identify as transgender.1 Social and medical inequality, marginalization, and discrimination continue to pervade transgender communities.2–4 Recent survey data suggest that 63% of the transgender people experience some form of serious discrimination.3 As proposed under the minority stress model, this outward prejudice and marginalization can eventually lead to internalization of chronic psychosocial stress and results in poor health outcomes.5–7 Of particular importance, the transgender community often reports more negative life experiences and poorer quality of life than the general population and lesbian, gay, and bisexual populations.3,5,8,9
Historically, the transgender population has postponed seeking primary care due to discrimination and stigmatization within both social and medical settings.10–14 The 2011 National Transgender Discrimination Survey (NTDS) and 2015 US Transgender Survey (USTS) found that approximately 20–30% of the transgender people postpone seeking medical care when sick due to discrimination and nearly 30–50% delay care due to affordability. Additionally, up to 20% of the transgender people encounter refusal of care, 30% endure harassment, and 50% report teaching their providers about appropriate transgender care.3,8 Several other studies also cite that transgender individuals are more likely to report negative health care experiences.15 In comparison to general civilian populations in the US, reported rates of delaying care by transgender people are often much higher.15,16 Although decreasing rates of perceived negativity suggest a more accepting, transgender-competent health system, clear shortcomings regarding provider knowledge and patient inequality perpetuate within the transgender community.14,17–20
Patient satisfaction
Surveys are frequently exploited to evaluate patient satisfaction with medical care and can be a reliable tool for quality improvement within medical practices.21–27 This utility is especially true for comprehensive care.28 Satisfaction however is often not operationally defined and patients perceive satisfaction differently with regard to provider care, office staff, and health accessibility.22,23 Many studies assessing patient satisfaction within family medicine clinics have found a recurring contention, ie, while overall satisfaction scores tend to be favorable, poorly perceived access to care can result in points of dissatisfaction.29–31 It is because of these incongruences in satisfaction that modifications to procedures and staff education are necessary. This approach theoretically could result in better care.
While transgender-related research is scarce, very few studies have considered patient satisfaction with the transgender-specific health care that is received. Although data are limited, those studies have published comparable results of high patient satisfaction. Bockting et al assessed satisfaction over time at a sexual health clinic in the US.32 The researchers found very few differences between transgender and other sexual health patients. However, upon reviewing data early in the study, they modified areas in need of improvement, including staff’s friendliness and phone call handling, and noted a significant increase in satisfaction in subsequent years. At this clinic, overall satisfaction with services varied between 80% and 97%. Other gender identity clinics in the United Kingdom and Australia have found equally high patient satisfaction scores.33–35
To add to the literature on transgender programs in the US, this cross-sectional study focuses on the satisfaction of transgender patients who receive primary care at a relatively new outpatient multidisciplinary program, the Eskenazi Transgender Health and Wellness Program. Due to the program’s recent initiation, we initially implemented a satisfaction survey to assess quality and needs for improvement. We evaluated whether this comprehensive, “one-stop shop” care model promotes high patient satisfaction levels and especially high overall satisfaction. To determine potential incongruences in staff satisfaction, we compared perceptions of the doctor, medical staff, and office staff at the program. We hypothesized that respondents would endorse high satisfaction scores but report lower satisfaction with the nuances of medical intake. We also posited that respondents would endorse the doctor more positively than medical staff and office staff.
Methods
Participants
The survey was administered to returning patients who seek care at the Eskenazi Transgender Health and Wellness Program in Indianapolis, Indiana.
Transgender Health and Wellness Program at Eskenazi Health
The Eskenazi Transgender Health and Wellness Program is a multidisciplinary medical and surgical program that provides comprehensive, culturally competent health care services and providers exclusively for transgender and gender-nonconforming adults. It is the first of its kind to serve the transgender population of Indiana and surrounding areas. Staff in the adult program consists of family medicine providers, plastic surgeon, psychiatric nurse practitioner, licensed practical nurse, therapists, speech pathologists, dietitians, attorneys, medical assistant, hospital chaplain, and patient care coordinator. As a “one-stop shop” model, the program offers medical, surgical, and mental health care services including primary care, hormone replacement therapy, surgeries, psychiatry, social work services, vocal feminization/masculinization, medical nutrition, legal aid, and care coordination including pre/post-operative support and linkage with support groups.
Instrument
A patient satisfaction survey was adapted from the American Academy of Family Physicians (AAFP) Patient Satisfaction Survey.27,36 The original version is a self-reporting, anonymous survey that measures patient satisfaction with different aspects of health care. In particular, there are demographic items and items consisting of 5-point Likert scales with the anchors of satisfaction, caring, and doctor recommendation. For example, satisfaction items have the options of “extremely dissatisfied”, “very dissatisfied”, “satisfied”, “very satisfied”, and “extremely satisfied”. To our knowledge, this survey has not yet been tested or validated in past studies.
We modified the AAFP survey into a self-reporting, anonymous transgender-specific battery of demographic items and items considering of 5-point Likert scales with the anchors of satisfaction, caring, competence, and doctor recommendation. In order to capture overall satisfaction, we replaced two of the original AAFP survey items with questions pertaining to general office visits and trans-friendliness and added one item about helpfulness of the program’s “one-stop shop” model.27 All items also had the option of “N/A”.
Procedure
This study was reviewed by the Indiana University Institutional Review Board (IRB), regarded as a quality improvement project, and deemed exempt from further IRB review (protocol number: 1,611,038,141). The survey was distributed by program staff to all returning patients at the transgender program between August 2015 and January 2017. Surveys were collected at the completion of each visit. Participation was voluntary and anonymous. A study information sheet was provided to patients, and completion of the survey constituted consent of participation. Data were then entered and evaluated by a blinded reviewer not involved in patient care. As this survey was anonymous, there was no identifying information attached to responses. Data were restricted to authorized study personnel and stored on a secure, password-protected computer.
Analysis
Results were analyzed using IBM SPSS Statistics 23. Frequencies were computed for demographic items and means were computed for survey items. Satisfaction rate was defined as the frequency of positive satisfaction responses (ie, scores of 3, 4, or 5) and computed for survey items. Independent variables were collapsed into two groups, ie, age (<30 and >30), gender (transgender female and transgender male), education (high school and college), duration at the program (0–4 months and >4 months), and number of visits (1–3 times and >3 times). Differences in mean scores were analyzed using independent samples t-tests. Paired samples t-tests were conducted to assess differences in satisfaction with the program’s staff. Spearman’s correlation coefficients between survey items and staff satisfaction scores were calculated. Specifically, correlations were computed between the survey items related to medical intake and survey items related to staff satisfaction in caring and competence. For all analyses, “N/A” responses were excluded; other excluded responses concerned missing data.
Results
Patient demographics
A total of 62 patients completed the anonymous survey (Table 1). Respondents varied in age (56.4% were under 30 years old and 43.5% were over 30 years old) and identified as either transgender female (male-to-female/MTF, 56.4%) or transgender male (female-to-male/FTM, 41.9%). Most respondents’ education consisted of at least some college (79.0%). Majority had been patients at the transgender program for more than 4 months (83.8%), while many had been to the program more than 3 times in the past 12 months (61.2%).
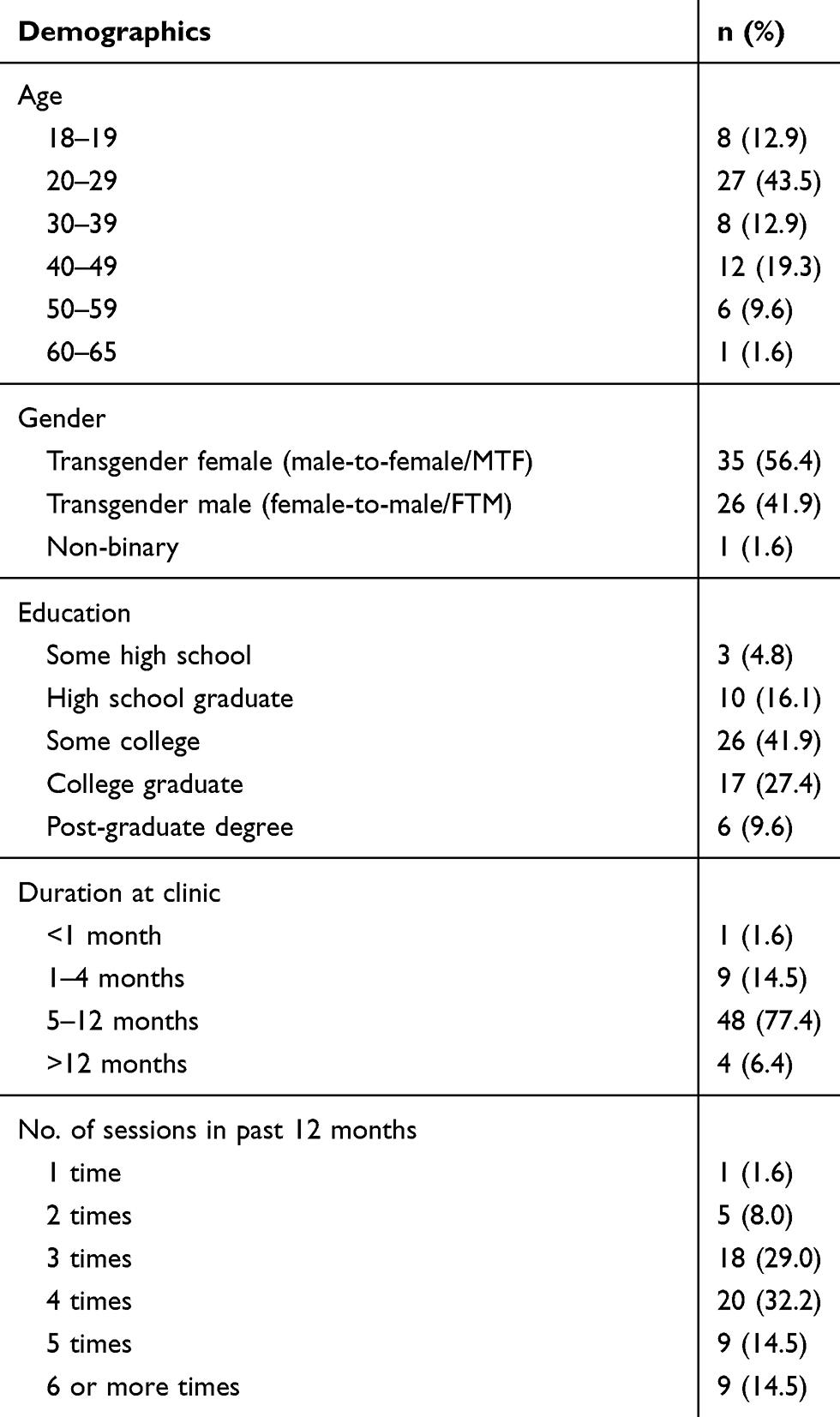 |
Table 1 Patient demographics (N=62) |
Item score means and frequencies
Overall, there were positive responses to all survey items (Table 2). Average survey responses ranged from moderately high (Q3, M=3.96, SD=0.94) to very high (Q19, M=4.90, SD=0.30). For overall patient satisfaction items (Q4, Q10, and Q20), responses were highly positive (M=4.62, SD=0.63; M=4.61, SD=0.58; M=4.80, SD=0.51, respectively). Frequencies revealed high satisfaction rates as well. Thirteen of the 20 items had a 100% satisfaction rate. For the other seven items (Q1, Q3, Q5, Q6, Q7, Q15, Q18), satisfaction rates varied between 92.3% (Q5) and 98.4% (Q1). There were no statistical differences of survey responses across age, gender, education, duration at the program, and number of visits in the past 12 months.
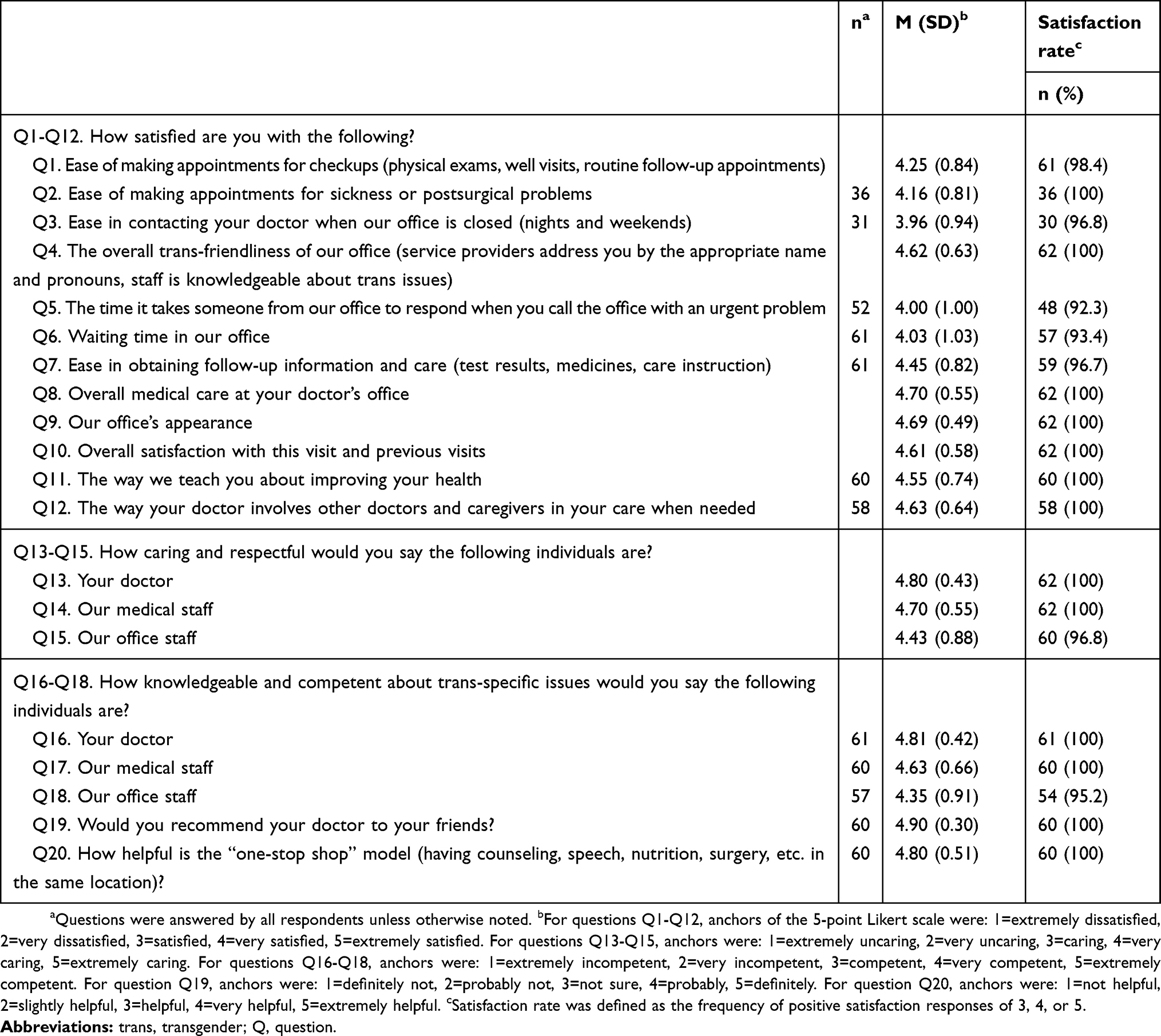 |
Table 2 Survey item means and satisfaction rates (N=62) |
Comparison of satisfaction with the doctor, medical staff, and office staff
There were clear differences between how respondents viewed the care (Q13-Q15) and competence (Q16-Q18) of the program’s staff (Figure 1). Doctors were viewed most positively and office staff least positively with medical staff rated in-between. Concerning conveyed care and respect, doctors (M=4.80, SD=0.43) were rated more positively than both medical staff (M=4.70, SD=0.55); t(61)=2.18, p=0.03, and office staff (M=4.43, SD=0.88); t(61)=4.00, p=<0.001, while medical staff were rated more positively than office staff; t(61)=3.73, p=<0.001. In regard to provided knowledge and competence, doctors (M=4.83, SD=0.41) received higher scores than both medical staff (M=4.63, SD=0.66); t(59)=3.49, p=0.001, and office staff (M=4.35, SD=0.91); t(56)=4.88, p=<0.001, while medical staff had higher scores than office staff; t(56)=4.22, p=<0.001.
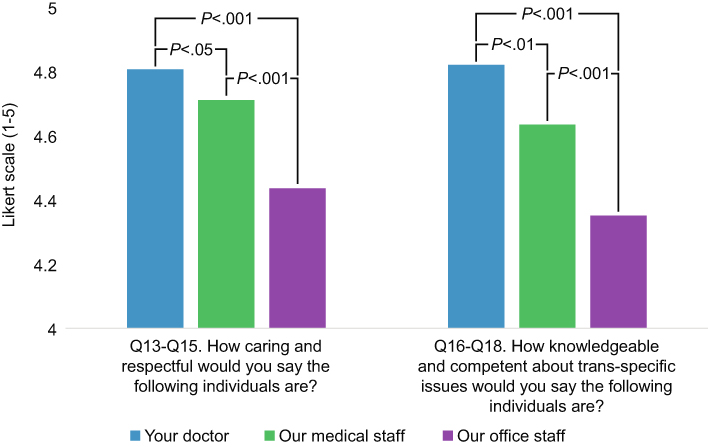 |
Figure 1 Patient respondents view the care and competence of the Eskenazi Transgender Health and Wellness Program’s staff differently. For both care/respect and knowledge/competence, doctors were viewed most positively and office staff least positively with medical staff rated in-between. Data shown as means. Means and standard deviations for care/respect and knowledge/competence, respectively: doctor (M=4.80, SD=0.43; M=4.83, SD=0.41), medical staff (M=4.70, SD=0.55; M=4.63, SD=0.66), and office staff (M=4.43, SD=0.88; M=4.35, SD=0.91). |
Correlations between satisfaction with survey items (in particular, medical intake items) and staff revealed a similar trend (Table 3). In general, the five medical intake items (Q1, Q2, Q3, Q5, and Q6) were significantly correlated with staff satisfaction in regard to caring and competence. For medical staff and office staff, all medical intake/caring satisfaction and medical intake/competence satisfaction correlations were statistically significant. For the doctor, one medical intake/caring satisfaction correlation (Q2) and two medical intake/competence satisfaction correlations (Q1 and Q2) did not reach statistical significance. Medical intake/caring satisfaction correlations were all of stronger strength for office staff than for the doctor; these correlations were also stronger for office staff than for medical staff, except for three items (Q1, Q3, and Q5). Medical intake/competence satisfaction correlations were stronger for office staff than for both the doctor and medical staff. For all other correlations between the other nine survey items and staff satisfaction scores, a pattern was not identified (all correlations except six had p-values<0.001, data not shown).
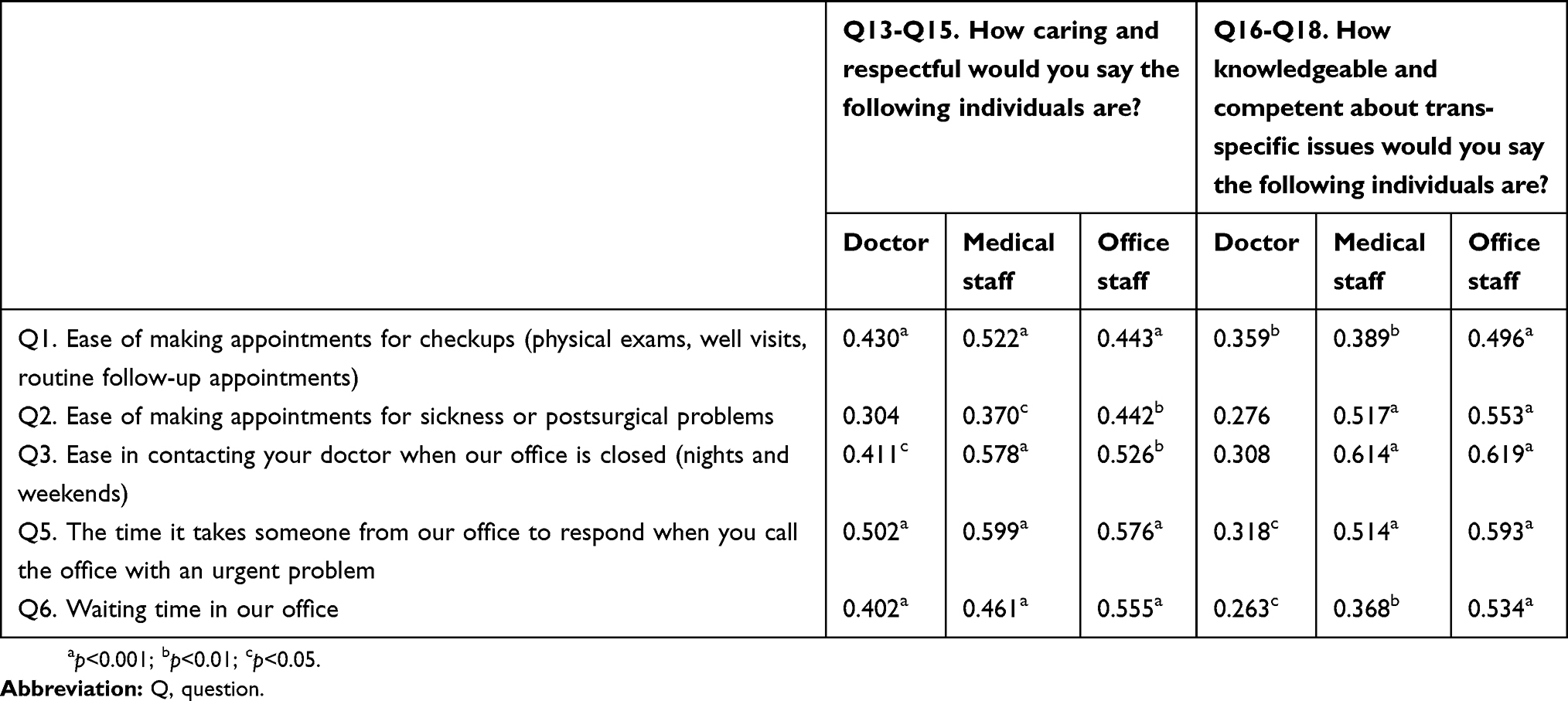 |
Table 3 Spearman’s correlation coefficients between satisfaction with medical intake and staff |
Discussion
Utilizing a satisfaction survey, we found that in general patients were highly satisfied with the care provided by the Eskenazi Transgender Health and Wellness Program. These results are analogous to past studies that have found high patient satisfaction among the transgender population.32–35 At the multidisciplinary program, patients often spend several hours per visit interacting with a variety of health care providers. Appropriating an integrative stance toward standard care, we hypothesized that the multidisciplinary program would be well received by transgender patients. However, a half day of care and support could equally be perceived as onerous, overwhelming, and consequentially not superior to standard health care visits. Hence, an inquiry concerned the general impression of the program. Respondents expressed high overall satisfaction in trans-friendliness, office visits, and the program’s “one-stop shop” model (Q4, Q10, and Q20). Perhaps such satisfaction is rooted in the types of unique services provided that would otherwise require a referral from a primary care provider—ie, counseling, speech therapy, nutrition, and surgery. We believe that the comprehensive nature of the program is likely a contributing factor to the high satisfaction observed and we highly recommend this model to other transgender care programs. Although this study was unable to offer a comparison group, another study by Bockting et al found no differences in overall satisfaction with health services between transgender and other sexual health patients.32 This study also did not assess whether there were differences in satisfaction between services at the program, eg, primary care versus legal aid. However, satisfaction with different health services may differ. Erasmus et al, for example, reported varying satisfaction across service type, eg, psychiatry, endocrinology, surgery, voice therapy, and social work.34 Therefore, transgender care programs should consider comparing satisfaction between nature of care (eg, standard vs multidisciplinary care) and across specific services to evaluate for possible subtle differences. Such an analytical approach would provide valuable, detailed information to better improve patient satisfaction and health outcomes.
A predilection to respond very positively may be compounded by many factors. Research has shown that patients tend to report moderate to very high satisfaction levels.22,29–35 The positivity among the program’s patient population may not be a function of the actual care provided but actually the appreciation of a once nonexistent resource. Eskenazi Health is the only transgender-specific program in the entire state, and patients may have responded highly because they are finally receiving patient-centered care (ie, any care is better than no care). Eskenazi also serves low-income populations. Because health care accessibility is heavily rooted in socioeconomic status, care postponement is more likely to occur in transgender people without income, health insurance, and means to obtain appropriate care.12 To this end, low-income transgender people report lower quality of life than their high-income counterparts.37 Now that an avenue to access and afford patient-centered care exists for the transgender population, respondents may have simply expressed gratitude for such a long-awaited, coveted resource or may have conveyed a fear that poor quality measures would jeopardize the program’s continuation.
Of interest are those survey items that received lower scores. Lower satisfaction levels and rates were typically associated with the nuances of medical intake rather than medical care. The five least endorsed items concerned medical intake such as appointment making (Q1, Q2, and Q3) and timing (Q5 and Q6). These results are comparable to previous studies that have also shown distress in making, traveling, and waiting for appointments.27,29–32,34 In addition, we found incongruences in reported satisfaction of the program’s staff. Interestingly, doctors were viewed most positively and office staff least positively with medical staff rated in-between. Perhaps less satisfaction in the care and competence of office staff originates from the perception of office staff’s minimal transgender health care experience and training. While we did not ascertain and quantify the competence of the doctor, medical staff, and office staff, it is reasonable to infer that respondents may entrust more confidence in the care provided by the doctor, whose practice relies on direct patient interaction. Another rationale of the observed incongruences among the program’s staff concerns the duties and responsibilities of office staff, ie, medical intake. Correlations between satisfaction with medical intake and the program’s staff were of stronger strength with office staff than the doctor. This disparity implies that dissatisfaction with medical intake correlates less strongly to perceptions of the doctor’s caring and competence than to perceptions of the office staff’s caring and competence. Consequently, if patients are dissatisfied with appointment making and timing, they may internalize and associate this contention with office staff’s care and competence. On the contrary, patients seem to weakly associate medical intake satisfaction with perceptions of their doctor. In summary, patients may perceive care with strong associations: the doctor provides only care and office staff carries out only medical intake. Therefore, dissatisfaction with appointment making and timing may not necessarily weaken perceptions of the doctor but it may have serious implications for perceptions of other staff members.
While there is a paucity of specific resources at individual and structural levels and subsequent perceived inaccessibility and unaffordability among the transgender population, additional barriers to appointment making and waiting time even further restrict transgender people’s access to quality care, their satisfaction, and ultimately their retention as patients.3,8,15–17,38 Although the former inequality is a universal issue that must be alleviated nationwide, the latter can be efficiently mitigated with better training of office staff about these specific issues. Current improvement efforts at the transgender program include hiring another more physicians, therapists, and patient care coordinators in order to reduce the wait time for appointments and providing training to office staff in order to improve cultural competency. Other transgender care programs should highly consider reviewing perceptions of medical intake and staff with their patients. By acknowledging appointment making and timing as a determinant of care, efforts can then be directed to establish better efficiency and productivity and balance patient satisfaction across all staff. For example, providing open availability with an adequate provider workforce and sufficient coverage at the front desk can relieve some medical intake dissatisfaction. Likewise, conducting quality improvement measures and delivering cultural competency training to staff, especially front office workers, can provide valuable information. This patient-centered approach can promote staff appreciation of patient-specific concerns. Such quality improvement will hopefully improve patient satisfaction with their received care and lead to better health outcomes for the transgender community.
Limitations
There are several noteworthy limitations to this study. For instance, although this survey is adapted from the AAFP’s Patient Satisfaction Survey and parallels other satisfaction surveys, this instrument has not yet been validated across many studies nor was it validated in this study. Of further note, the constructed Likert scales do not reflect neutrality. For example, we did not include a moderate or neutral option, eg, “neither satisfied or dissatisfied”, thus giving respondents two negative choices and three positive choices. This imbalance possibly skewed respondents to choose more positively than they otherwise would have if a neutral option was available. In addition, this study is also limited by subject recruitment relying on convenience sampling as well as a small sample size. Because the program only treats transgender patients, this study was unable to offer a comparison group. Likewise, the program is a relatively new practice and we have not yet compared satisfaction over time after instituting quality improvements.
Conclusions
While medical care is paramount to care programs’ reputations and eventual health outcomes, health care is truly initiated at the front desk. During a time when medical discrimination is common within the transgender community, a culturally competent model involves one where all staff are respectful, unbiased, and qualified to provide patient-centered care. To ensure these important qualities are witnessed across all personnel, we recommend that transgender programs routinely conduct quality improvement measures, maintain sufficient workforce coverage, and provide cultural competency training about appropriate care standards and patient-centered concerns regarding appointment making and burdens associated with timing, traveling, and cost. Only then, through an integrative perspective, can we start to deconstruct the medical inequalities of the transgender community.
Significance of work
There are very few transgender-specific programs in the United States. Only a handful of studies have considered patient satisfaction with the care provided to the transgender community. This study focuses on patient satisfaction within Indiana’s first transgender-specific outpatient program. This study reports very positive results overall and acknowledges the least endorsed items as issues surrounding medical intake. This study emphasizes the importance of efficient medical intake (ie, ease of appointment making, waiting time, and timing of office replies) on patient satisfaction. Extending these results, this study makes recommendations to existing and future transgender-specific programs on how to improve patient satisfaction.
Credentials
Dustin Nowaskie, MD: Dustin is a second-year psychiatry resident at the Department of Psychiatry of the Indiana University School of Medicine. He has specific interests in LGBTQ care and is the founder of the nonprofit 501(c)(3) organization OutCare Health.
Rachel Fogel, BA: Rachel is a clinical research assistant at the Center for Virology and Vaccine Research of the Beth Israel Deaconess Medical Center. She is currently applying to medical school and has an interest in global women’s health.
Janine Fogel, MD: Janine is a family medicine physician at Eskenazi Health. She is the founder of the first and only transgender program in Indiana.
Acknowledgments
The authors wish to acknowledge and thank all the staff at the Eskenazi Transgender Health and Wellness Program for their help in the creation and distribution of the survey used in this study. Because this study was a quality improvement project and not considered research, the study was exempt from review by the Indiana University Institutional Review Board. There was no source of funding for this study.
Disclosure
The authors of this study report no conflicts of interests or competing affiliations, financial agreements, or other involvements with any company whose product figures in the manuscript, and no conflicts of interest in regard to this work.
References
1. Flores AR, Herman JL, Gates GJ, Brown TNT; Williams Institute. How many Adults Identify as Transgender in the United States? 2016. Available from: http://williamsinstitute.law.ucla.edu/wp-content/uploads/How-Many-Adults-Identify-as-Transgender-in-the-United-States.pdf.
2. Daniel H, Butkus R. Lesbian, gay, bisexual, and transgender health disparities: executive summary of a policy position paper from the American college of physicians. Ann Intern Med. 2015;163:135–137. doi:10.7326/M14-2482
3. Grant JM, Mottet LA, Tanis J, et al. National Center for Transgender Equality and National Gay and Lesbian Task Force. Injustice at Every Turn: A Report of the National Transgender Discrimination Survey. 2011. Available from: www.transequality.org/sites/default/files/docs/resources/NTDS_Report.pdf.
4. Institute of Medicine. The Health of Lesbian, Gay, Bisexual, and Transgender People: Building a Foundation for Better Understanding. Washington, DC: The National Academies Press; 2011.
5. Carmel TC, Erickson-Schroth L. Mental health and the transgender population. J Psychosoc Nurs Ment Health Serv. 2016;54:44–48. doi:10.3928/02793695-20161208-09
6. Meyer IH. Prejudice as stress: conceptual and measurement problems. Am J Public Health. 2003;93:262–265. doi:10.2105/ajph.93.2.262
7. Redfern JS, Barnes A, Chang J. Psychosocial, HIV, and health care management issues impacting transgender individuals. Am J Orthopsychiatry. 2016;86:366–372. doi:10.1037/ort0000190
8. James SE, Herman JL, Rankin S, et al. National center for transgender equality. The Report of the 2015 U.S. Transgender Survey; 2016. Available from: www.transequality.org/sites/default/files/docs/usts/USTS%20Full%20Report%20-%20FINAL%201.6.17.pdf.
9. McNamara MC, Ng H. Best practices in LGBT care: a guide for primary care physicians. Cleve Clin J Med. 2016;83:531–541. doi:10.3949/ccjm.83a.15148
10. Bauer GR, Hammond R, Travers R, Kaay M, Hohenadel KM, Boyce M. “I don’t think this is theoretical; this is our lives”: how erasure impacts health care for transgender people. J Assoc Nurses AIDS Care. 2009;20:348–361. doi:10.1016/j.jana.2009.07.004
11. Bradford J, Reisner SL, Honnold JA, Xavier J. Experiences of transgender-related discrimination and implications of health: results from the virginia transgender health initiative study. Am J Public Health. 2013;103:1820–1829. doi:10.2105/AJPH.2012.300796
12. Cruz TM. Assessing access to care for transgender and gender nonconforming people: a consideration of diversity in combating discrimination. Soc Sci Med. 2014;110:65–73. doi:10.1016/j.socscimed.2014.03.032
13. Drescher J, Cohen-Kettenis P, Winter S. Minding the body: situating gender identity diagnoses in the ICD-11. In Rev Psychiatry. 2012;24:568–577. doi:10.3109/09540261.2012.741575
14. Poteat T, German D, Kerrigan D. Managing uncertainty: a grounded theory of stigma in transgender health care encounters. Soc Sci Med. 2013;84:22–29. doi:10.1016/j.socscimed.2013.02.019
15. Macapagal K, Bhatia R, Greene GJ. Differences in healthcare access, use, and experiences within a community sample of racially diverse lesbian, gay, bisexual, transgender, and questioning emerging adults. LGBT Health. 2016;3:434–442. doi:10.1089/lgbt.2015.0124
16. Centers for Disease Control and Prevention. QuickStats: percentage of adults aged 18–64 years who delayed or did not receive medical care during the past 12 months because of cost, by year—national health interview survey, United States, 2005–2014. Morb Mortal Wkly Rep. 2016;65:251. doi:10.15585/mmwr.mm6509a6
17. Sanchez NF, Sanchez JP, Danoff A. Health care utilization, barriers to care, and hormone usage among male-to-female transgender persons in New York City. Am J Public Health. 2009;99:713–719. doi:10.2105/AJPH.2007.132035
18. Selix NW, Rowniak S. Provision of patient-centered transgender care. J Midwifery Womens Health. 2016;61:744–751. doi:10.1111/jmwh.12518
19. Shetty G, Sanchez JA, Lancaster JM, Wilson LE, Quinn GP, Schabath MB. Oncology healthcare providers’ knowledge, attitudes, and practice behaviors regarding LGBT health. Patient Educ Couns. 2016;99:1676–1684. doi:10.1016/j.pec.2016.05.004
20. Snelgrove JW, Jasudavisius AM, Rowe BW, Head EM, Bauer GR. “Completely out-at-sea” with “two-gender medicine”: a qualitative analysis of physician-side barriers to providing healthcare for transgender patients. BMC Health Serv Res. 2012;12:110. doi:10.1186/1472-6963-12-110
21. Ford RC, Bach SA, Fottler MD. Methods of measuring patient satisfaction in health care organizations. Health Care Manage Rev. 1997;22:74–89.
22. Hall JA, Dornan MC. Meta-analysis of satisfaction with medical care: description of research domain and analysis of overall satisfaction levels. Soc Sci Med. 1988;27:637–644.
23. Harris LE, Swindle RW, Mungai SM, Weinberger M, Tierney WM. Measuring patient satisfaction for quality improvement. Med Care. 1999;37:1207–1213.
24. Ingram BL, Chung RS. Client satisfaction data and quality improvement planning in managed care organizations. Health Care Manage Rev. 1997;22:40–52.
25. Pascoe GC. Patient satisfaction in primary health care: a literature review and analysis. Eval Program Plann. 1983;6:185–210.
26. Rosenthal GE, Shannon SE. The use of perceptions in the evaluation of health-care delivery systems. Med Care. 1997;35:58–68. doi:10.1097/00005650-199711001-00007
27. White B. Measuring patient satisfaction: how to do it and why to bother. Fam Pract Manag. 1999;6:40–44.
28. Asadi-Lari M, Tamburini M, Gray D. Patients’ needs, satisfaction, and health related quality of life: towards a comprehensive model. Health Qual Life Outcomes. 2004;2:32. doi:10.1186/1477-7525-2-32
29. Carroll JC, Talbot Y, Permaul J, et al. Academic family health teams: part 2: patient perceptions of access. Can Fam Physician. 2016;62:e31–e39.
30. Howard M, Agarwal G, Hilts L. Patient satisfaction with access in two inter professional academic family medicine clinics. Fam Pract. 2009;26:407–412. doi:10.1093/fampra/cmp049
31. Wetmore S, Boisvert L, Graham E, et al. Patient satisfaction with access and continuity of care in a multidisciplinary academic family medicine clinic. Can Fam Physician. 2014;60:e230–e236.
32. Bockting W, Robinson B, Benner A, Scheltema K. Patient satisfaction with transgender health services. J Sex Marital Ther. 2004;30:277–294. doi:10.1080/00926230490422467
33. Davies A, Bouman WP, Richards C, et al. Patient satisfaction with gender identity clinic services in the United Kingdom. Sex Relation Ther. 2013;28:400–418. doi:10.1080/14681994.2013.834321
34. Erasmus J, Bagga H, Harte F. Assessing patient satisfaction with a multidisciplinary gender dysphoria clinic in Melbourne. Australas Psychiatry. 2015;23:158–162. doi:10.1177/1039856214566829
35. Wylie KR, Fitter J, Bragg A. The experience of service users with regard to satisfaction with clinical services. Sex Relation Ther. 2009;24:163–174. doi:10.1080/14681990903002730
36. American Academy of Family Physicians. Patient Surveys/Questionnaires. Patient Satisfaction Survey; 2017. Available from: www.aafp.org/fpm/toolBox/viewToolType.htm?toolTypeId=23.
37. Motmans J, Meier P, Ponnet K, T’Sjoen G. Female and male transgender quality of life: socioeconomic and medical differences. J Sex Med. 2012;9:743–750. doi:10.1111/j.1743-6109.2011.02569.x
38. White Hughto JM, Reisner SL, Pachankis JE. Transgender stigma and health: a critical review of stigma determinants, mechanisms, and interventions. Soc Sci Med. 2015;147:222–231. doi:10.1016/j.socscimed.2015.11.010
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.