Back to Journals » International Journal of General Medicine » Volume 18
Impact of Workload and Shift Characteristics on Diagnostic Resource Utilization Among Emergency Medicine Residents
Authors Cakmak S ![]() , Bas RK, Hokenek NM, Sakul AA
, Bas RK, Hokenek NM, Sakul AA
Received 10 September 2025
Accepted for publication 10 December 2025
Published 17 December 2025 Volume 2025:18 Pages 7615—7626
DOI https://doi.org/10.2147/IJGM.S562179
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Woon-Man Kung
Sumeyye Cakmak,1 Raif Kaan Bas,2 Nihat Mujdat Hokenek,1 Ayse Arzu Sakul2
1Department of Emergency Medicine, University of Health Sciences, Istanbul Cam and Sakura City Research and Training Hospital, Istanbul, Turkey; 2Department of Medical Pharmacology, Istanbul Medipol University, Faculty of Medicine, Istanbul, Turkey
Correspondence: Sumeyye Cakmak, University of Health Sciences, Istanbul Cam and Sakura City Research and Training Hospital, g-434 Street, Basaksehir/Istanbul, 34480, Turkey, Tel +90 (212) 909 60 00, Email [email protected]
Purpose: This study aimed to investigate the impact of shift characteristics, resident workload, and physician attributes on diagnostic expenditures in low-acuity patients (green triage category) emergency department (ED) patients.
Methods: A retrospective cross-sectional analysis was conducted in a high-volume tertiary ED over one month, including 22,427 green-triage visits managed by 71 emergency medicine residents. Resident characteristics (age, gender, seniority, shift group, post-night shift status), patient demographics, and diagnostic expenditures (laboratory, imaging, electronic medication orders, total cost) were extracted from the hospital information system. Non-parametric tests were used for group comparisons given non-normal distribution patterns, and cost determinants were analyzed using a Gamma generalized linear model with a log-link function.
Results: Diagnostic expenditures demonstrated significant variability across physician and patient characteristics. Female residents were associated with higher laboratory (1.27 vs 0.87 USD; p< 0.001), imaging (1.35 vs 1.01 USD; p< 0.001), and medication-order costs (p< 0.001). Compared with junior residents, mid-level trainees generated the highest total expenditures, whereas senior residents exhibited a cost-attenuating effect (exp(β)=0.74). Unadjusted analyses indicated greater total spending during night shifts (2.8 USD vs 2.39– 2.43 USD; p=0.011); however, after adjustment for resident- and patient-level covariates, night-shift status was associated with lower expenditures (exp(β)=0.76). Post-night-shift status independently correlated with reduced laboratory and medication-order costs. Resident workload showed a strong inverse association with expenditures, with increasing daily patient volume linked to lower total diagnostic costs (rho=– 0.226; p< 0.001). Among patient factors, advancing age increased total cost by approximately 6% per year (exp(β)=1.06). Repeat ED utilization emerged as the most powerful cost determinant, with each additional prior visit associated with more than a threefold increase in diagnostic spending (exp(β)> 3; p< 0.001). Female patients consistently incurred higher costs across all categories (p< 0.001).
Conclusion: Diagnostic spending in low-acuity ED encounters is shaped by both clinical and operational dynamics. Resident workload, seniority level, and gender independently influence cost patterns, while patient age and repeat admissions are strong drivers of increased expenditures. These findings highlight several potentially modifiable determinants—particularly workload distribution and trainee supervision—that may support more cost-conscious diagnostic practices in busy emergency departments.
Keywords: workload, triage, retrospective study, emergency diagnostic efficiency, healthcare system, diagnostic costs
Introduction
Emergency departments (EDs) are crucial components of healthcare systems, providing immediate care for acute and life-threatening conditions and serving as a safety net for individuals lacking regular access to medical services.1,2 Despite this vital role, EDs face increasing operational and financial burdens due to crowding and resource strain. A 2009 US study reported a net surplus of $6.1 billion generated by ED services, illustrating both high demand and systemic stress.3
A major driver of crowding is the growing number of non-urgent visits, which account for 6.7% to 89% of all ED encounters.4 First described in the 1970s, these visits—typically classified as “green triage”—represent low-acuity presentations.5,6 However, recent studies have shown that some low-acuity cases still require diagnostic testing, specialist consultation, or even hospitalization.7 Inappropriate ED utilization contributes to delays in care, higher costs, lower patient satisfaction, and increased risk of adverse outcomes.8–10 Patient preference alone does not explain this trend; structural and system-level barriers such as access limitations and inefficiencies also play major roles.11 Redirecting such cases to alternative care settings could reduce expenditures by up to $4.4 billion annually in the US healthcare system.12
Beyond patient-related factors, operational conditions—such as shift timing and workload—significantly influence clinical decision-making.13,14 Rea et al demonstrated that test ordering and length of stay vary according to when patients present during a physician’s shift.15 However, few studies have investigated how these operational pressures affect resident physicians, who constitute the primary frontline workforce in EDs. The relationship between resident characteristics (eg, seniority, gender, post-call status) and diagnostic expenditures in low-acuity encounters remains insufficiently understood.
This study therefore investigates diagnostic test ordering patterns among resident physicians managing green-triage patients in a high-volume tertiary ED. By examining how physician attributes and workload relate to laboratory, imaging, and electronic order costs, we aim to identify modifiable factors that could inform targeted interventions to optimize diagnostic efficiency and reduce unnecessary healthcare spending.
Method
Study Design and Setting
The researchers performed a retrospective cross-sectional investigation in the emergency department of a teaching and research hospital from March 1, 2025, to March 31, 2025. The study evaluated the diagnostic test ordering practices of resident physicians and analyzed the costs linked to their testing methodologies.
Setting and Triage System
The emergency department at Cam and Sakura City Hospital is among the largest in Istanbul, accommodating around 500,000 people and 5000 ambulances each year. The triage system in the emergency department integrates components of the Emergency Severity Index triage system (Figure 1). Triage is performed by trained triage nurses under an ESI-adapted institutional protocol, with emergency physician supervision when necessary. If, upon subsequent clinical evaluation, the attending resident or supervising physician considers the triage category inaccurate, it can be corrected in the hospital information system. For analytical purposes, we used each patient’s final (revised) triage category as recorded in the system. In our study, Groups 1 and 2 corresponded to the red triage category, Group 3 to yellow, and Groups 4 and 5 to green. A small subset of green-triage patients could still require a limited diagnostic evaluation.
 |
Figure 1 Emergency Severity Index (ESI)–adapted triage flow used in the study. |
The emergency department has three shifts, each lasting eight hours: morning (08:00–16:00), evening (16:00–24:00), and night (24:00–08:00). The working hours in the designated region are uniform throughout all shifts.
Study Population
The study included 22,427 patients and 71 resident physicians throughout the research period. The patients were assigned triage categories ranging from green according to the emergency triage protocol. The daily number of patients per assistant found in our study reflects the total number of green triage patient records registered for each assistant in the hospital information system. It should be noted that this includes not only in-depth examinations but also low-priority cases that undergo brief assessments. Residents were stratified into three seniority tiers —first-year juniors (64.4%), second- and third-year mid-level residents (33.8%), and fourth-year seniors (1.8%)—following a classification approach aligned with established frameworks in emergency medicine residency training.16 The residents undergo a seniority examination biannually, and those who succeed are elevated in rank. The researchers recorded demographic data regarding the residents, encompassing their age, gender, work hours (morning, evening, night), and their condition post-night shifts. Residents following a 24-hour-on/24-hour-off duty schedule were classified as being in the post-night shift status group, indicating they had recently completed a night shift before their subsequent workday.
Inclusion Criteria
Must be a resident in the Emergency Department. Patients assigned to the green triage category upon arrival to the emergency department. Availability of complete data in the hospital information system.
Exclusion Criteria
Patients and residents that could not be reached for data collection. Patients presenting with yellow or red triage categories were excluded from the analysis. Psychiatric patients were excluded because such cases are evaluated and managed within a dedicated psychiatric emergency unit rather than the general emergency department. Pediatric patients presenting with non-traumatic complaints were excluded, as these cases are managed by a separate pediatric emergency unit under the pediatric department rather than the emergency medicine department.
Data Collection
Data were obtained through a retrospective review of the hospital information system. Information collected included patient demographic characteristics (age, gender), resident demographic variables (age, gender, seniority level), shift details, individual patient volume per resident, laboratory test expenditures, medication order costs, and total diagnostic expenses.
All cost data also were extracted from the hospital information system, including laboratory, imaging, and medication order expenditures. The cost of each investigation was determined based on the 2025 Turkish Health Implementation Guideline unit prices. Costs were recorded in Turkish Lira (TRY) and converted to US dollars (USD) using the average Central Bank exchange rate for March 2025 (1 USD = 40 TRY).
Variables
The dependent variables included laboratory test expenses, imaging expenses, medication order expenses, and total diagnostic expenses for each patient visit. Medication order cost represents the total cost of all medications electronically prescribed and administered within the hospital for each patient during their emergency department visit, as recorded in the hospital information system’s electronic drug order module.
Total diagnostic cost as a total cost was analyzed as a continuous variable. This composite cost measure represented the sum of three components recorded for each patient encounter: (1) laboratory test expenditures, (2) imaging test expenditures, and (3) medication order costs. Because total cost values were strictly positive and showed a right-skewed distribution, they were modeled using a Generalized Linear Model (Gamma distribution with a log-link). Exponentiated coefficients (exp(β)) from this model are interpreted as multiplicative effects (cost ratios) associated with each predictor.
The independent variables included resident seniority, resident gender, resident age, resident’s shift group, resident’s post-night shift work status, daily patient count seen by the resident, patient age, patient gender, and frequency of repeat admissions.
Statistical Analysis
The distributional properties of continuous variables were evaluated using the Shapiro–Wilk test and Q–Q plots. As most variables violated the assumption of normality, non-parametric methods were applied. Group comparisons were performed using the Mann–Whitney U-test for two independent groups and the Kruskal–Wallis test for more than two groups. Continuous variables were summarized as median and interquartile range (median; Q1–Q3), with means reported when informative. Associations between continuous variables were assessed using Spearman rank correlation, and correlation coefficients (ρ) with corresponding p-values were reported.
Because total cost values were strictly positive and exhibited marked right-skewness, determinants of cost were analyzed using a Generalized Linear Model (GLM) with a Gamma distribution and log-link. Observations with zero total cost were replaced with 0.01 USD, consistent with recommendations for maintaining the positive domain required for Gamma log-link models. The model included resident seniority, resident gender, shift group, patient gender, patient age, resident age, post-night-shift status, daily patient volume, and repeat admission count as independent variables. Model fit was evaluated using Null Deviance, Residual Deviance, and Akaike Information Criterion (AIC). All analyses were conducted using the StatsModels package in Python, and statistical significance was set at p < 0.05.
Results
Descriptive Analysis
The study included 22,427 patients and 71 resident physicians attending to them. During the specified month, the emergency department conducted a total of 41,958 patient examinations, comprising 22,427 (53.4%) in the green zone. Among the 22,427 patients assessed in the emergency department with green triage included in the study, 53.7% were female and 46.3% were male. The median age of the studied patients was determined to be 36 years. Among the 22,427 patients assessed, 42.0% were attended to by resident physicians during the morning shift, 42.3% during the evening shift, and 15.7% during the night shift. 12.6% of patient examinations conducted by resident doctors occurred during post-shift hours.
38.3% of the residents were female, 61.7% were male, and the breakdown of seniority was as follows: junior 38%, intermediate senior 47.9%, and senior 14.1%. The median age of the residents was 29 (IQR: 28–32) years. The median number of patients per resident in the green area daily was 129 (IQR: 94–154), indicating the number of patients individually assessed by the residents each day (minimum: 1; maximum: 264 patients/day). The median cost of laboratory tests was determined to be 0 USD (IQR: 0–0), imaging costs at 0 USD (IQR: 0–0), medication order costs at 0 USD (IQR: 0–0.19), and the overall cost at 0.1 USD (IQR: 0–1.12), with a minimum cost of 0 USD and a maximum cost of 226.13 USD. (Table 1).
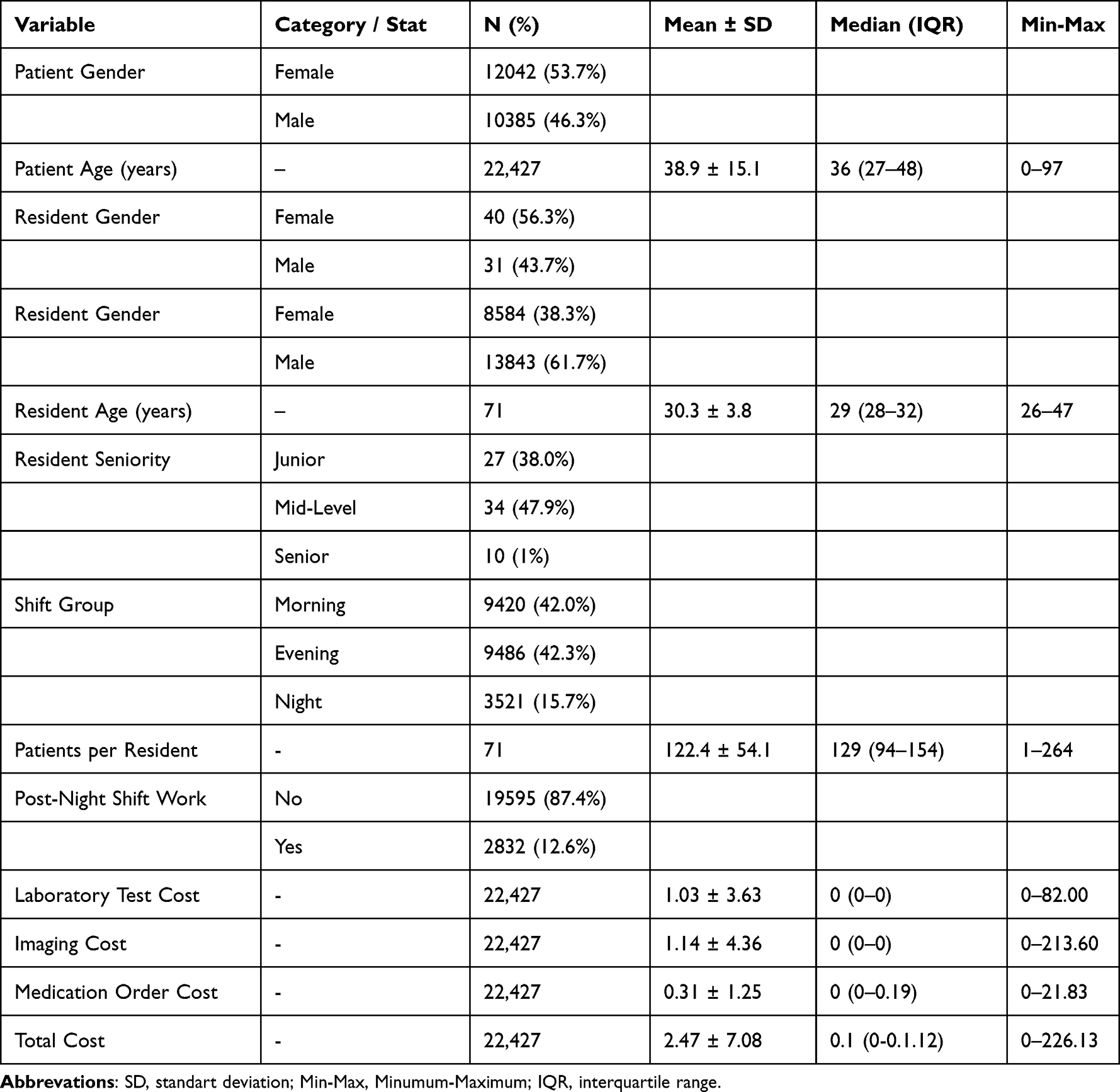 |
Table 1 Descriptive Characteristics of the Study Population |
Comparison of Costs According to Demographic and Clinical Variables
Laboratory test expenditures varied significantly across shift groups, with the highest average costs observed during the night shift (p < 0.001). No significant differences were found across resident seniority levels (p = 0.322). When assessed by resident gender, laboratory test costs were significantly higher among male residents compared with female residents (1.27 USD vs 0.87 USD; p < 0.001). Residents working post-night shift generated lower laboratory expenses, and this reduction reached statistical significance (p = 0.022). Spearman correlation analyses demonstrated that laboratory test costs were negatively correlated with the total daily number of patients evaluated by the resident (ρ = –0.199, p < 0.001), indicating that higher workload was associated with reduced per-patient laboratory expenditures. Conversely, laboratory costs showed significant positive correlations with repeat admission frequency (ρ = 0.065, p < 0.001) and patient age (ρ = 0.122, p < 0.001). Laboratory expenditures were also significantly higher among female patients than male patients (p < 0.001, Table 2).
 |
Table 2 Univariate Analysis of Laboratory Test, Imaging, Medication Order, and Total Costs According to Clinical and Demographic Variables |
Imaging Cost
Imaging costs demonstrated no significant variation across shift groups (p = 0.196) or seniority levels (p = 0.708). In contrast, female residents were associated with significantly higher imaging expenditures compared with male residents (1.35 USD vs 1.01 USD; p < 0.001), Post–night-shift status was not significantly associated with imaging costs (p = 0.105). Imaging expenditures showed positive correlations with repeat admission frequency (p < 0.001) and patient age (p < 0.001). Additionally, imaging costs were significantly higher among female patients compared with male patients (p = 0.031; Table 2).
Medication Order Cost
Medication order costs varied significantly across shift groups (p < 0.001), with higher mean expenditures during night shifts (0.43 USD) compared with morning (0.27 USD) and evening (0.31 USD) shifts. A significant difference was also observed across seniority levels (p = 0.030), whereby intermediate-level residents demonstrated the highest mean medication order cost (0.34 USD).
Medication order costs were higher among female residents compared with male residents (p < 0.001). Post-night shift work was associated with a statistically significant reduction in these costs (p = 0.019). Medication order cost demonstrated positive correlations with resident age (p < 0.001) and the frequency of repeat admissions (p < 0.001), whereas negative correlations were observed with the daily patient count (p < 0.001). Furthermore, medication order costs were significantly higher among female patients than male patients (p < 0.001; Table 2).
Total Cost
A statistically significant difference in overall costs was seen among shift groups (p<0.001), with the average total cost for the night shift (2.8 USD) exceeding that of the morning (2.43 USD) and evening (2.39 USD) shifts.
Junior residents had significantly higher total costs compared to senior residents (p=0.008). The overall expense was markedly more for patients attended to by female residents in contrast to those attended to by male residents (p<0.001).
The cost was found to be significantly lower when residents worked the day after a night shift (p<0.001). Statistically significant positive correlation was identified between resident age and total cost (rho=0.02, p<0.001). Furthermore, there was a statistically significant negative correlation between daily patient count and total costs (rho=–0.226, p<0.001), indicating that higher patient volumes were associated with lower costs per patient. Significant positive relationships were identified between the frequency of repeat admissions (rho=0.068, p<0.001), patient age (rho=0.121, p<0.001), and overall cost. It was also determined that total costs were significantly higher for female patients compared to male patients (p<0.001).
The total cost differed significantly between shift groups, with higher costs observed in the night shift compared to other shifts (p<0.001). Second-year residents were associated with approximately 38% higher costs compared to first-year residents (exp(β)≈1.38), while third-year residents showed a 26% reduction in costs (exp(β)≈0.74). Patients evaluated by male residents had about 26% lower costs than those evaluated by female residents (exp(β)≈0.74). Costs were approximately 24% lower in the third shift compared to the first shift (exp(β)≈0.76).
A one-year increase in patient age was associated with a 6% increase in total cost (exp(β)≈1.06). Increased daily patient volume per resident was significantly correlated with lower costs. Each additional repeat admission increased the total cost by nearly threefold (exp(β)>3). Working the day after a night shift was linked to a modest but significant cost reduction. In multivariable analysis, after adjusting for all covariates, the night shift itself did not have an independent effect on cost (Table 3).
 |
Table 3 Generalized Linear Model (GLM) Gamma (Log-Link) Regression Results for Determinants of Total Cost |
Discussion
This study expands the current understanding of how physician-specific characteristics and real-time operational factors jointly shape diagnostic resource use in low-acuity emergency department (ED) settings. Drawing from a large, real-world dataset of over 22,000 green-triage patient encounters managed by 71 emergency medicine residents, we identified clinically significant patterns that reflect both adaptive and potentially avoidable variation in test-ordering behavior.
Our findings suggest that increased resident workload, as indexed by daily patient volume, is inversely associated with per-patient diagnostic expenditures—particularly for laboratory testing—consistent with prior evidence demonstrating “efficiency under pressure” behaviors in the face of rising demand.1 This result contrasts with most prior studies, which have typically shown that greater workload is linked to increased test ordering and higher costs.14,15
Moreover, the inverse association between cumulative patient volume and diagnostic intensity per case aligns with the concept of diagnostic fatigue. As physicians move through their shifts, cognitive bandwidth narrows, and test ordering appears to decline—a trend supported by prior behavioral and cognitive load models in ED practice.17–19 Still, such reductions may not uniformly equate to higher-value care; rather, they may reflect a fatigue-driven truncation of diagnostic reasoning.20
Our data also underscore the strong influence of physician seniority and gender on diagnostic expenditures. Relative to junior residents, mid-level residents demonstrated significantly higher total costs, with expenditures approximately 38% greater (exp(β) ≈1.38; p<0.001). Conversely, senior residents exhibited a cost-reducing effect, incurring expenditures roughly 26% lower than juniors (exp(β) ≈0.74; p=0.035). This stratification confirms that training stage is a crucial determinant of resource utilization, suggesting that the initial phases of residency training may be associated with elevated diagnostic spending before efficiency gains are realized in the final stages.5,16 This is consistent with evidence from Emergency Department (ED) settings globally, where increased physician experience is associated with the use of fewer diagnostic procedures, particularly for nonurgent patients, resulting in better use of resources.21 Although senior physicians may spend more time on orders and disposition, their increased clinical experience correlates with a reduction in procedures like radiography and CT scans and is associated with a lower ED mortality rate.7,22
Regarding other demographic variables, the main effect of resident age showed a slight inverse association with costs (β=−0.0108; exp(β) ≈0.9893; p=0.030), indicating that older residents generally trend toward marginally lower expenditures.23
Additionally, resident gender proved to be a statistically significant determinant of total diagnostic cost. Contrary to some prior literature, female residents in our study demonstrated higher adjusted diagnostic costs compared to their male counterparts, whose costs were approximately 26% lower in the multivariate model (exp(β) ≈0.74; p<0.001).
Temporal factors demonstrated a complex relationship with diagnostic behavior. While univariate analysis suggested higher costs during night shifts, the multivariate GLM analysis indicated that after controlling for confounding variables (such as patient age and repeat admission count), being in the night shift actually correlated with an approximate 54% reduction in total cost compared to the morning shift (exp(β)≈0.46; p<0.001). This reversal suggests that the raw, higher costs observed at night are primarily driven by the specific, high-cost patient characteristics and complexity arriving during those hours, rather than the shift itself. Additionally, consistent with potential duty-hour protection mechanisms or limited fatigue-related variability, post-night shift status was found to be statistically insignificant in determining total diagnostic cost in the final multivariate model (p=0.213). Although experience has been proposed as a factor influencing diagnostic behavior, robust evidence linking seniority to reduced imaging use (and concomitantly lower mortality) is lacking, and our findings contribute novel data to this underexplored area.24
Of particular note, patients with repeat ED admissions experienced significantly higher diagnostic expenditures. Our multivariate analysis identified repeat admission count as one of the strongest predictors of cost, demonstrating that each additional admission increased total diagnostic costs by approximately 40.6% (exp(β)≈1.4063; p<0.001). This significant positive correlation (ρ=0.068; p<0.001) is consistent with literature highlighting the substantial healthcare cost and resource utilization burden contributed by frequent ED utilizers.25 While this high expenditure may reflect increased provider caution or perceived complexity associated with frequently returning patients, resulting in heightened test intensity, potentially driven by the substitution of tests for time under high-demand settings,15 it also reinforces prior findings that increased test intensity in the ED can propagate downstream utilization. This finding highlights the potential utility of integrating prior ED visit data into clinical decision support tools aimed at guiding diagnostic stewardship, particularly given the documented effectiveness of multidisciplinary care models in managing these high-need patient populations.25
Ultimately, this study illustrates that test ordering is not merely the product of individual clinician preferences, but rather the result of dynamic, intersecting factors including workload configuration, shift timing, resident experience, and patient-specific characteristics.26 As EDs confront ongoing pressures to deliver high-quality, cost-effective care, recognizing and addressing the contextual forces behind resource utilization will be essential.27 Future work should focus on real-time analytics, feedback dashboards, and structured mentorship interventions to optimize diagnostic efficiency without compromising patient safety.
Limitations
The most significant strength of this study is its large dataset, encompassing over 22,000 patients and 71 resident physicians, which enabled robust multivariate regression analyses. However, limitations exist. As a single-center study, the generalizability of our results may be limited. The retrospective design allows us to identify correlations but not to establish definitive causal relationships. Furthermore, the inability to control for clinical variables like case-mix complexity within the green triage category requires cautious interpretation. Also, although triage levels were verified and, when necessary, corrected by the evaluating physicians, the possibility of residual mis-triage cannot be completely excluded. Finally, this study analyzed only cost data; whether lower costs are associated with different clinical outcomes (eg, missed diagnoses, 72-hour readmissions) is beyond its scope.
Conclusion
In conclusion, this study identifies and correlates the variables of physician workload, gender, seniority, and environmental factors, providing helpful tips for enhancing resource allocation and clinical efficiency. Future research should aim for multi-center, prospective designs that integrate clinical outcome data to deepen the understanding of these multifaceted relationships.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare no conflicts of interest.
References
1. Soltani M, Batt RJ, Bavafa H, Patterson BW. Does what happens in the ED stay in the ED? The effects of emergency department physician workload on post-ED care use. Manuf Serv Oper Manag. 2022;24(6):3079–3098. doi:10.1287/msom.2022.1110
2. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316
3. Wilson M, Cutler D. Emergency department profits are likely to continue as the Affordable Care Act expands coverage. Health Aff. 2014;33(5):792–799. doi:10.1377/hlthaff.2013.0754
4. Uscher-Pines L, Pines J, Kellermann A, Gillen E, Mehrotra A. Emergency department visits for nonurgent conditions: a systematic literature review. Am J Manag Care. 2013;19(1):47–59.
5. Lees RE, Steele R, Spaso R. Primary care for nontraumatic illness at the emergency department and the family physician’s office. Can Med Assoc J. 1976;114:333–337.
6. Liggins K. Inappropriate attendance at accident and emergency departments: a literature review. J Adv Nurs. 1993;18(7):1141–1145. doi:10.1046/j.1365-2648.1993.18071141.x
7. Dong SL, Bullard MJ, Meurer DP, et al. Predictive validity of a computerized emergency triage tool. Acad Emerg Med. 2007;14(1):16–21. doi:10.1197/j.aem.2006.08.021
8. Derlet RW, Richards JR. Overcrowding in the nation’s emergency departments: complex causes and disturbing effects. Ann Emerg Med. 2000;35(1):63–68. doi:10.1016/S0196-0644(00)70105-3
9. Jepson GMH. How do primary health care systems compare across Western Europe? Pharm J. 2001;267:269–273.
10. Siddiqui S, Ogbeide DO. Utilization of emergency services in a community hospital. Saudi Med J. 2002;23(1):69–72.
11. Durand AC, Palazzolo S, Tanti-Hardouin N, Gerbeaux P, Sambuc R, Gentile S. Nonurgent patients in emergency departments: rational or irresponsible consumers? Perceptions of professionals and patients. BMC Res Notes. 2012;5:525. doi:10.1186/1756-0500-5-525
12. Weinick RM, Burns RM, Mehrotra A. Many emergency department visits could be managed at urgent care centers and retail clinics. Health Aff. 2010;29(9):1630–1636. doi:10.1377/hlthaff.2009.0748
13. Anderson D, Golden B, Jank W, Wasil E. The impact of hospital utilization on patient readmission rate. Health Care Manag Sci. 2012;15(1):29–36. doi:10.1007/s10729-011-9178-3
14. Chan DC. The efficiency of slacking off: evidence from the emergency department. Econometrica. 2018;86(3):997–1030. doi:10.3982/ECTA13565
15. Rea D, Anderson D, Bjarnadottir M. Emergency department physicians alter their ordering behavior based on available time. SSRN [Preprint]. 2024 Jul 26 [cited 2025 Nov 27]. Available from: https://ssrn.com/abstract=4907055.
16. Chiu IM, Syue YJ, Kung CT, et al. The influence of resident seniority on supervised practice in the emergency department. Medicine. 2017;96(4):e5987. doi:10.1097/MD.0000000000005987
17. Ergün-Şahin B, Güneş ED, Kocabıyıkoğlu A, Keskin A. How does workload affect test ordering behavior of physicians? An empirical investigation. Prod Oper Manag. 2022;31(6):2664–2680. doi:10.1111/poms.13711
18. Danziger S, Levav J, Avnaim-Pesso L. Extraneous factors in judicial decisions. Proc Natl Acad Sci U S A. 2011;108(17):6889–6892. doi:10.1073/pnas.1018033108
19. Ibanez M, Toffel MW. How scheduling can bias quality assessment: evidence from food-safety inspections. Manag Sci. 2020;66(6):2396–2416. doi:10.1287/mnsc.2019.3318
20. Westbrook JI, Raban MZ, Walter SR, et al. Task errors by emergency physicians are associated with interruptions, multitasking, fatigue and working memory capacity: a prospective, direct observation study. BMJ Qual Saf. 2018;27(8):655–663. doi:10.1136/bmjqs-2017-007333
21. McDonald N, Antkowiak PS, Burke R, Chiu DT, Stenson BA, Sanchez LD. Emergency physician resource utilization varies by years of experience. J Am Coll Emerg Physicians Open. 2024;5(2):e13162. doi:10.1002/emp2.13162
22. Li CJ, Syue YJ, Tsai TC, Wu KH, Lee CH, Lin YR. The impact of emergency physician seniority on clinical efficiency, emergency department resource use, patient outcomes, and disposition accuracy. Medicine. 2016;95(6):e2706. doi:10.1097/MD.0000000000002706
23. Querin LB, McGary A, Hodgson NR, Allen R, Martini WA. Association between physician age and imaging utilization in emergency department abdominal pain evaluation. J Emerg Med. 2025;72:9–16. doi:10.1016/j.jemermed.2024.11.016
24. Klein RP, Velan G, Razee H, et al. Factors affecting diagnostic imaging decision-making in the emergency department during day and night shifts. Emerg Med J. 2025;42(8):511–518. doi:10.1136/emermed-2024-214416
25. Wang R, Lukose K, Ensz OS, Revere L, Hammarlund N. Emergency department visit frequency and health care costs following implementation of an integrated practice unit for frequent utilizers. Acad Emerg Med. 2024;31(11):1112–1120. doi:10.1111/acem.14973
26. Klein RP, O’Brien BC, Razee H, et al. Factors affecting diagnostic imaging decision making in the emergency department. Emerg Med J. 2025;42(8):511–517.
27. Perrone PM, Deda L, Comotti A, Agostoni C, Castaldi S, Milani GP. Impact of time of shift on diagnostic service requests in a pediatric emergency department. Intern Emerg Med. 2025. doi:10.1007/s11739-025-03954-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Validity of an Ocular Emergency Triage System Compared to the Existing Grading System at the Emergency Unit of a Tertiary Eye Hospital in Saudi Arabia
AlSamnan M, AlAmry M, aldossari S, Talea M, Khandekar R, AlGhadeer H
Clinical Ophthalmology 2023, 17:527-534
Published Date: 8 February 2023