Back to Journals » Advances in Medical Education and Practice » Volume 14
Impact of Training in Serious Illness Communication and Work Life Balance on Physicians’ Self-Efficacy, Clinical Practice and Perception of Roles
Authors Funding E ![]() , Viftrup DT
, Viftrup DT ![]() , Knudsen MB
, Knudsen MB ![]() , Haunstrup LM, Tolver A, Clemmensen SN
, Haunstrup LM, Tolver A, Clemmensen SN
Received 3 February 2023
Accepted for publication 4 May 2023
Published 31 May 2023 Volume 2023:14 Pages 547—555
DOI https://doi.org/10.2147/AMEP.S406570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Eva Funding,1,2 Dorte Toudal Viftrup,3 Mark Bech Knudsen,4 Laura Mors Haunstrup,5 Anders Tolver,4 Stine Novrup Clemmensen1
1Department of Hematology, Rigshospitalet, Copenhagen, Denmark; 2Institute of Clinical Medicine, University of Copenhagen, Copenhagen, Denmark; 3Department of Public Health, University of Southern Denmark, Odense, Denmark; 4Data Science Lab, Department of Mathematical Sciences, University of Copenhagen, Copenhagen, Denmark; 5Department of Hematology, Aalborg University Hospital, Aalborg, Denmark
Correspondence: Eva Funding, Department of Hematology, Rigshospitalet, Copenhagen, Denmark, Email [email protected]
Purpose: Serious illness communication is a core task in hemato-oncology that require advanced communication skills and can be emotionally demanding. A 2-day course was implemented as a mandatory part of the 5-year hematology specialist training program in Denmark in 2021. The aim of this study was to assess the quantitative and qualitative effect of course participation on self-efficacy in serious illness communication and measure the prevalence of burnout among physicians in hematology specialist training.
Methods: For quantitative assessment course participants answered three questionnaires: Self-efficacy Advance care planning (ACP), Self-efficacy Existential communication (EC) and the Copenhagen Burnout Inventory at baseline, 4 and 12 weeks after the course. The control group answered the questionnaires once. Qualitative assessment was performed as structured group interviews with course participants 4 weeks after the course, transcribed, coded, and transformed into themes.
Results: All self-efficacy EC scores and 12 out of 17 self-efficacy ACP scores improved after the course, though mostly non-significant. Course participants reported altered clinical practice and perception of role as a physician. The physicians’ confidence that they could find the time to discuss ACP were low and remained low. The prevalence of burnout was high. Burnout levels were non-significantly lower after the course.
Conclusion: A mandatory course of formal training can increase physician self-efficacy in serious illness communication and alter clinical practice and perception of roles. The high level of burnout among physicians in hemato-oncology calls for institutional interventions in addition to training.
Keywords: hemato-oncology, communication skills training, burnout, mixed methods study
Introduction
Communication with patients exposed to serious illness and facing life and death decisions is a core task in hemato-oncology as well as in primary care, internal medicine and surgery.1 In Denmark, communication skills training is an integrated part of the pregraduate curriculum in medical school, practicing basic communication skills, active listening, and delivering bad news. After graduation these skills must be transferred to daily clinical practice, where direct observation with feed-back from a mentor is limited to rare occasions. It is widely recognized that healthcare professionals involved in end-of-life care should be trained to improve their communication skills.2–6 In the 5-year hematology specialist training in Denmark, the formal training focus is on medical and academic expertise. Meanwhile, the complexity of patient communication increase in parallel with the growing expertise and responsibility during specialist training. Serious illness communication and end of life care raise existential questions, not thoroughly addressed in the basic training as an undergraduate student. Physicians who feel insufficiently trained in communication skills are at a higher risk of burnout than those who feel sufficiently trained.7–10
Therefore, a 2-day course of formal training was implemented as a mandatory part of the hematology specialist training program in Denmark in 2021. The method and content of the course can be adapted to specialists in any field engaged in end-of-life care. The course consisted of two times four hours of communication exercises, targeting serious illness communication with focus on discussing patients’ and caregivers’ goals of care, worries, values, and hope. Professional actors performed as patients in “improvised theatre”, and participants took turns acting while their peers watched, with time-outs for group discussion and reflection. This was combined with sessions aiming to create reflection on participants own existential values, work-life balance, symptoms and management of burnout and work overload, and training in debriefing with peers after traumatic events.
Mata et al reviewed the effect of communication skills training on health professional´s self-efficacy in a meta-analysis from 2021, identifying 8 experimental studies with varying methods of teaching and assessment.6 The authors recommend valid and diversified evaluation in future programs to complement existing data. The use of actors and psychologists in this course increase cost and add to the importance of evaluation.
The aim of this study was to assess the quantitative and qualitative effect of a mandatory course on self-efficacy in conducting goals of care with patients, to optimize future courses and promote implementation of mandatory communication training of hospital physicians. Furthermore, to measure the prevalence of burnout among physicians in hematology specialist training in Denmark.
Materials and Methods
Participants
All physicians in haematology specialist training in Denmark in 2021 were invited to participate in the study. 17 out of 77 physicians in specialist training were allocated to the first 2-day course “Communication in haematology” in October 2021 and 15 participated in the study. Non-course participants served as controls, and 28 out of the remaining 60 specialist trainees participated. Participation in the study was voluntary. According to Danish legislation, review board approval is not required for surveys and interviews.
Data Collection
Electronic questionnaires were distributed and collected via REDCap™, hosted by the Capital Region, Copenhagen, Denmark, according to standard data protection requirements for scientific studies. Interviews were conducted virtually, digitally recorded, and transcribed verbatim. The study was approved by the Capital Region data protection knowledge centre.
Assessment of Self-Efficacy
Two validated questionnaires were used, “Self-efficacy advance care planning (ACP)” consisting of 17 items and a control question, and “Self-efficacy existential communication (EC)” where 6 out of 8 items were included in this study.11,12 Each item consists of two questions; “How confident are you that you can…?” and “How important is it for you to be able to…in your daily professional work?” on a scale from 1 to 5. Two self-efficacy EC items on religious concerns were left out, as religion was not a focus for the course. The self-efficacy EC scores are presented for each item separately, whereas self-efficacy ACP is presented as a single score based on the average of all 17 items, in addition to scores for each item.
Assessment of Burnout
Burnout was assessed with the Copenhagen burnout inventory (CBI), consisting of three scales: personal burnout, work-related burnout, and patient-related burnout, containing 6–7 items with a score up to 100.13 The score on a scale is the average of the scores for each item. An average score of 50 or more in a scale is a moderate to high degree of burnout.13,14
Course participants answered the self-efficacy and burnout questionnaires one week before the course (n=15), 4 weeks after (n=12) and 12 weeks after (n=14). Controls answered the questionnaires once (n=27). Prevalence was calculated based on answers from controls and participants before the course.
Statistical Analysis
For course participants who answered the survey both before and after the course, change in self-efficacy was evaluated using a Wilcoxon signed-rank test to avoid misspecification due to non-normality of data. Controls were compared with course participants 4 weeks after the course using the Wilcoxon rank-sum test. Statistical analysis was performed using R version 4.2.1.
Qualitative Assessment
On the last day of the course the participants were invited to take part in focus group interviews. 12 out of 17 participants signed up to participate in one of two online interviews on different dates to their convenience. The interviews took place four weeks after completion of the course. On the days of the interviews, only nine participants (5 female, 4 male) were able to attend. The focus group interviews took approximately 60 minutes and were organized with a moderator guide focusing on whether the course had influenced or changed anything in the daily practice and communication of the participants, and which aspects of the course had contributed to change and in what way. The importance of the participants’ own descriptions during the interviews were emphasized, and the moderator guide introduced less sensitive questions first and subsequently more sensitive questions in order to facilitate disclosure of the participants’ personal experience and perspectives. The second author moderated both focus group interviews. The interviews were audio-recorded and transcribed verbatim in agreement with Reflexive Thematic Analysis by Braun and Clark.15
Results
Course participants were slightly older than controls (mean age 39 versus 37 years), had been physicians longer (mean timespan 10 versus 8 years) and had been in specialist training longer (mean year of training 4.0 versus 3.2 years). The gender distribution was 10 female (67%) and 5 male (33%) course participants, compared to 16 female (59%) and 11 male (41%) controls.
Self-Efficacy
For course participants, mean scores for self-efficacy and perceived importance of each item on the EC scale before and after the course are shown in Figure 1. The mean efficacy score in EC increased for all 6 questions, whereas the mean score of perceived importance score increased in 4 out of 6 questions. The change in scores in self-efficacy EC reached statistical significance for item 1 and 3 (Table 1), concerning patients’ existential concerns and needs and the physician’s ability to endure situations without an answer or a solution. Compared to controls, course participants scored significantly higher in item 5; the ability to work with own barriers to discuss existential issues. Of note, the scores for importance of EC were already high before the course, mean score 4.2–4.8, leaving little room for improvement.
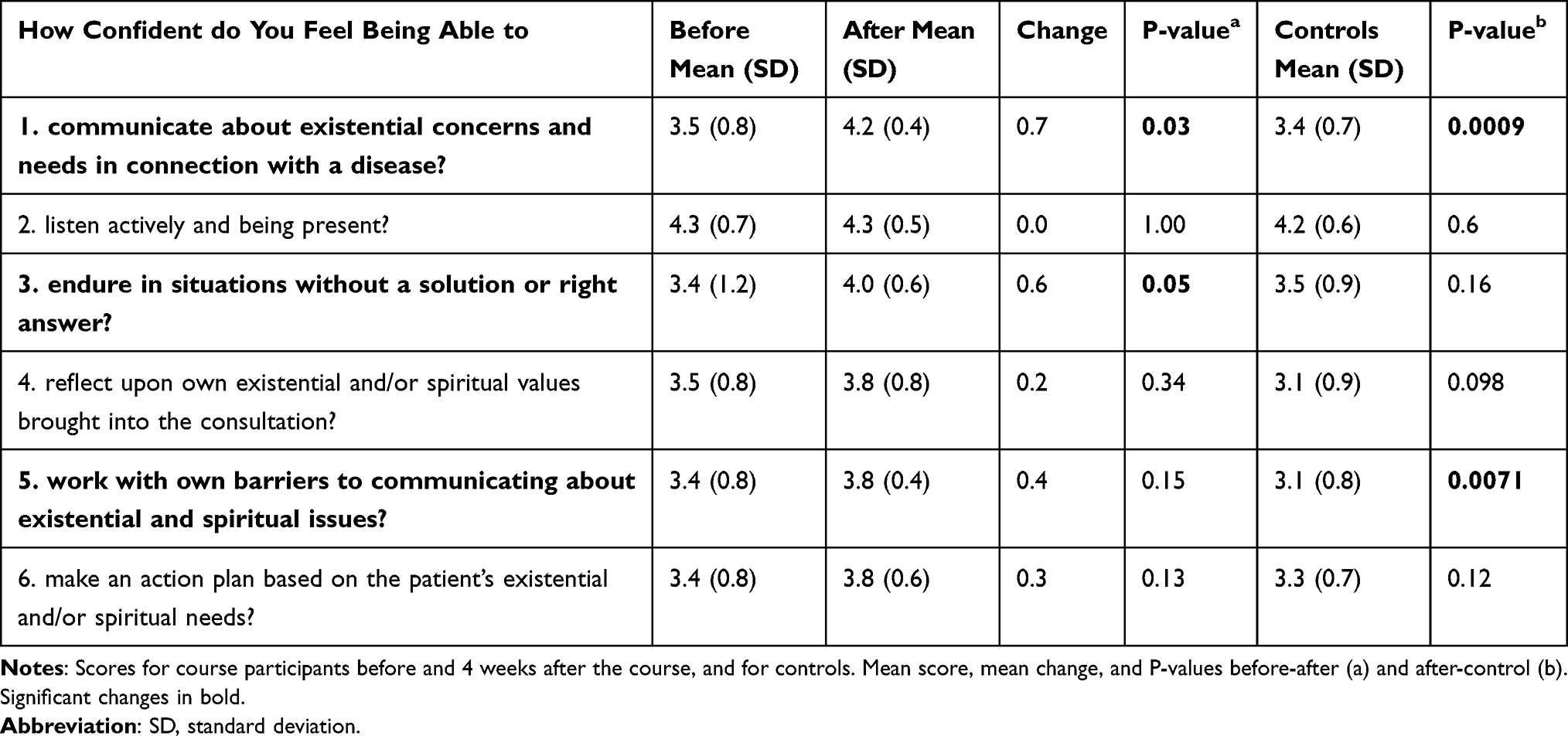 |
Table 1 Self-Efficacy Existential Communication |
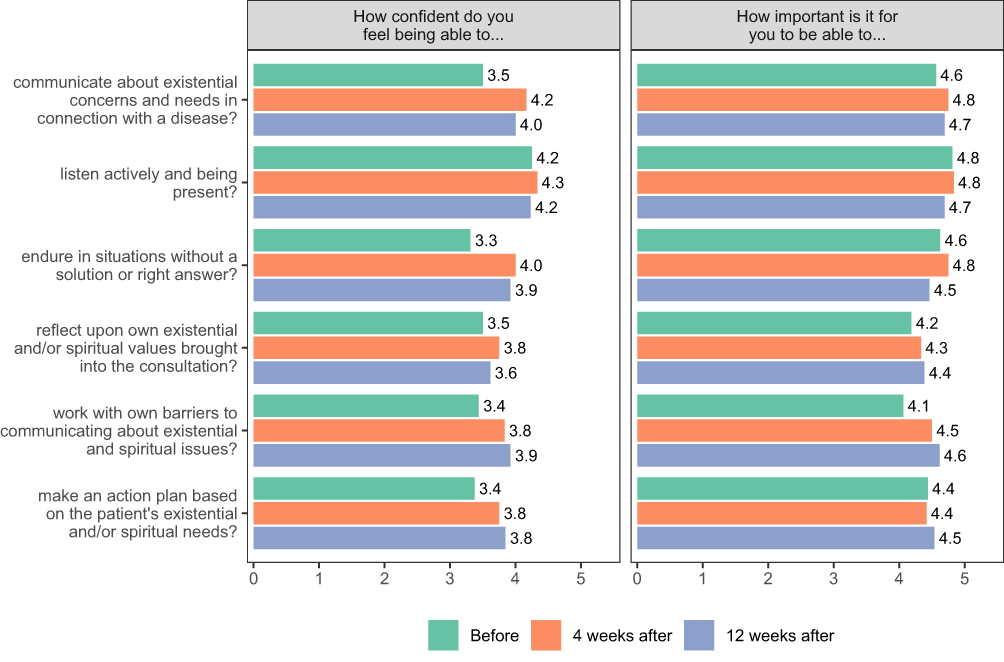 |
Figure 1 Self-efficacy existential communication Mean self-efficacy scores for course participants before and 4 and 12 weeks after the course. |
Mean scores for the 17 items of the self-efficacy ACP scale before and after the course are shown in Table 2. The mean self-efficacy score for course participants improved in 14 out of 17 items but decreased or remained unchanged in 4 items (question 2, 4, 6 and 8). The mean change for each item in the ACP scale only reached statistical significance in item 14; the confidence to openly discuss insecurities with the patient, and compared to the control group, course participants had a significantly higher score in item 9, the confidence to ensure that patients treatment preferences would be honored. The single item ACP score increased non-significantly from 3.5 to 3.7 after the course, compared to 3.5 for the control group. The increase is confirmed by the control question (item 18) increasing from a mean score of 3.5 to 3.6, compared to 3.1 for controls.
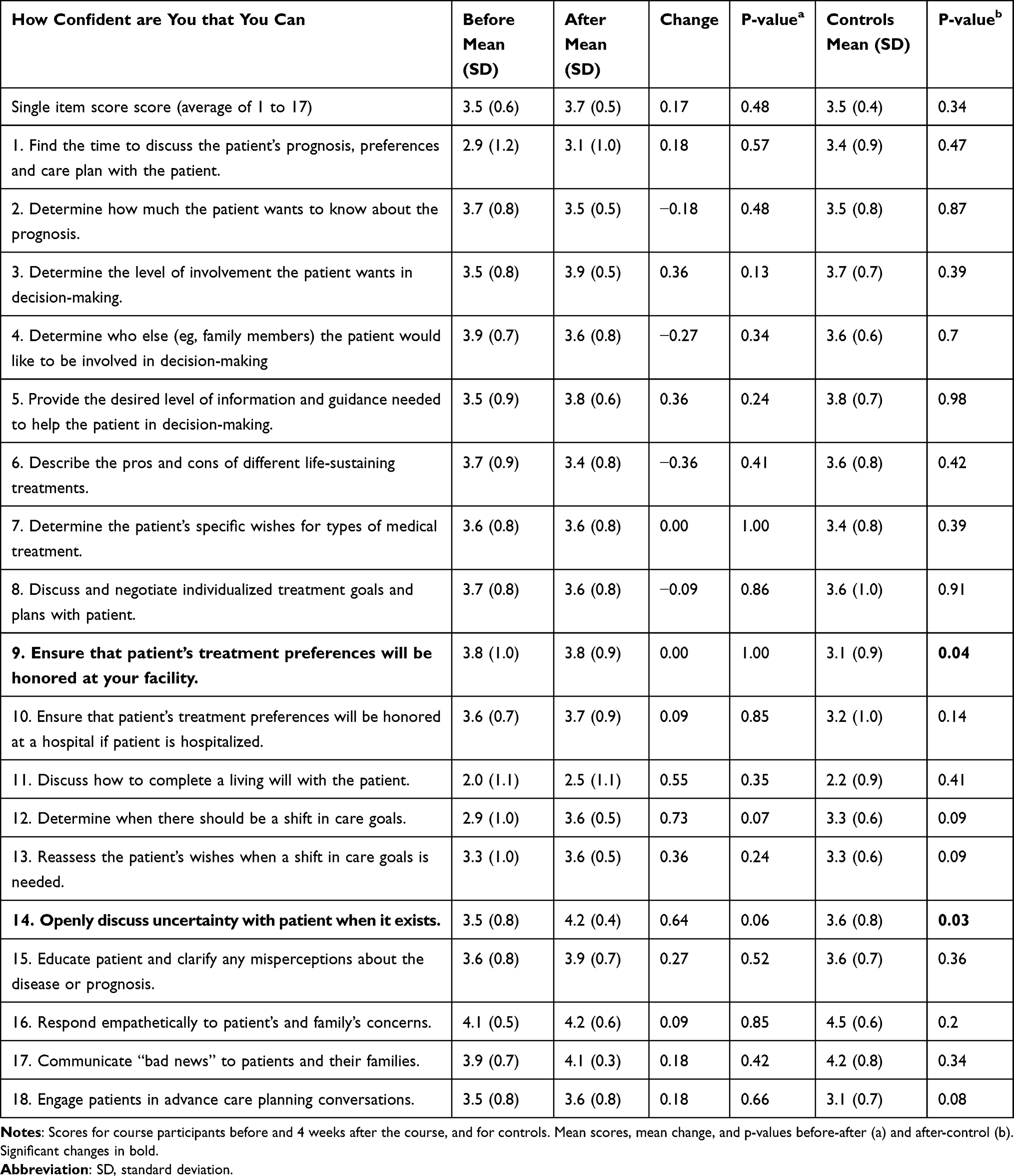 |
Table 2 Self-Efficacy Advance Care Planning |
Self-efficacy scores were not significantly correlated with gender, age or seniority, expressed as years being a physician and years in specialist training.
Burnout
For course participants completing the burnout questionnaire more than once, there were no significant difference in mean score before and after the course, nor in comparison with the control group. Mean burnout scores are shown in Table 3. The prevalence of moderate to severe burnout with a score of 50 or higher were respectively 10% (n=4) for patient-related burnout, 29% (n=12) for work-related burnout, and 37% for personal burnout (n=15). Only 12% (n=5) reported no symptoms of personal burnout (score under 25). Burnout was not significantly associated with gender, age, nor seniority.
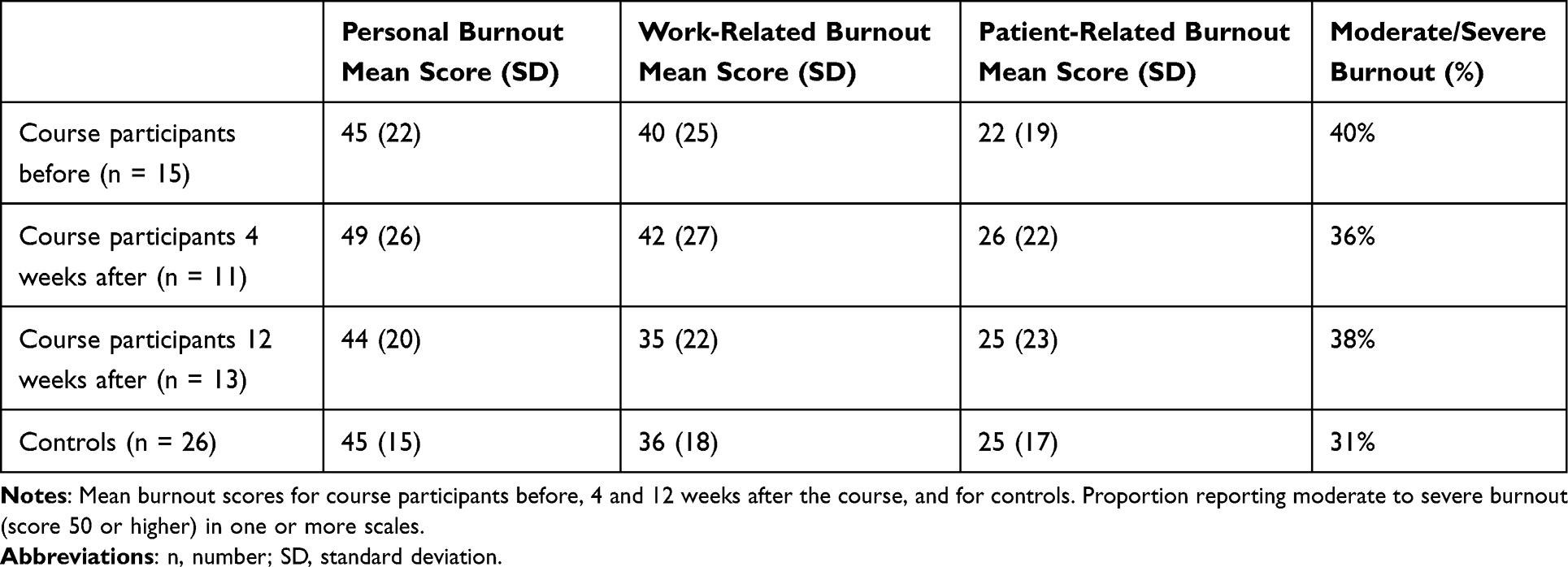 |
Table 3 Burnout |
Qualitative Evaluation
The analysis was carried out in six steps. In step one, the second author became familiar with the dataset and made initial notes. In step two, data were organized into systematic meaning units. The initial notes of each description and meaning unit were transformed into short phrases, and these were discussed between the first and second author and formed into initial codes. In step three, the initial codes were analyzed and transformed into three overall themes across all descriptions in line with the idiographic approach. In step four, these three themes were reviewed, modified, and developed by three authors. In step five, the essence of the themes as well as subthemes were identified. The final writing of the analysis and results was carried out in step six. The three overall themes are: 1) specific changes in practice, 2) self-awareness, and 3) sense of security in the course. Quotes from the participants are shown in Table 4.
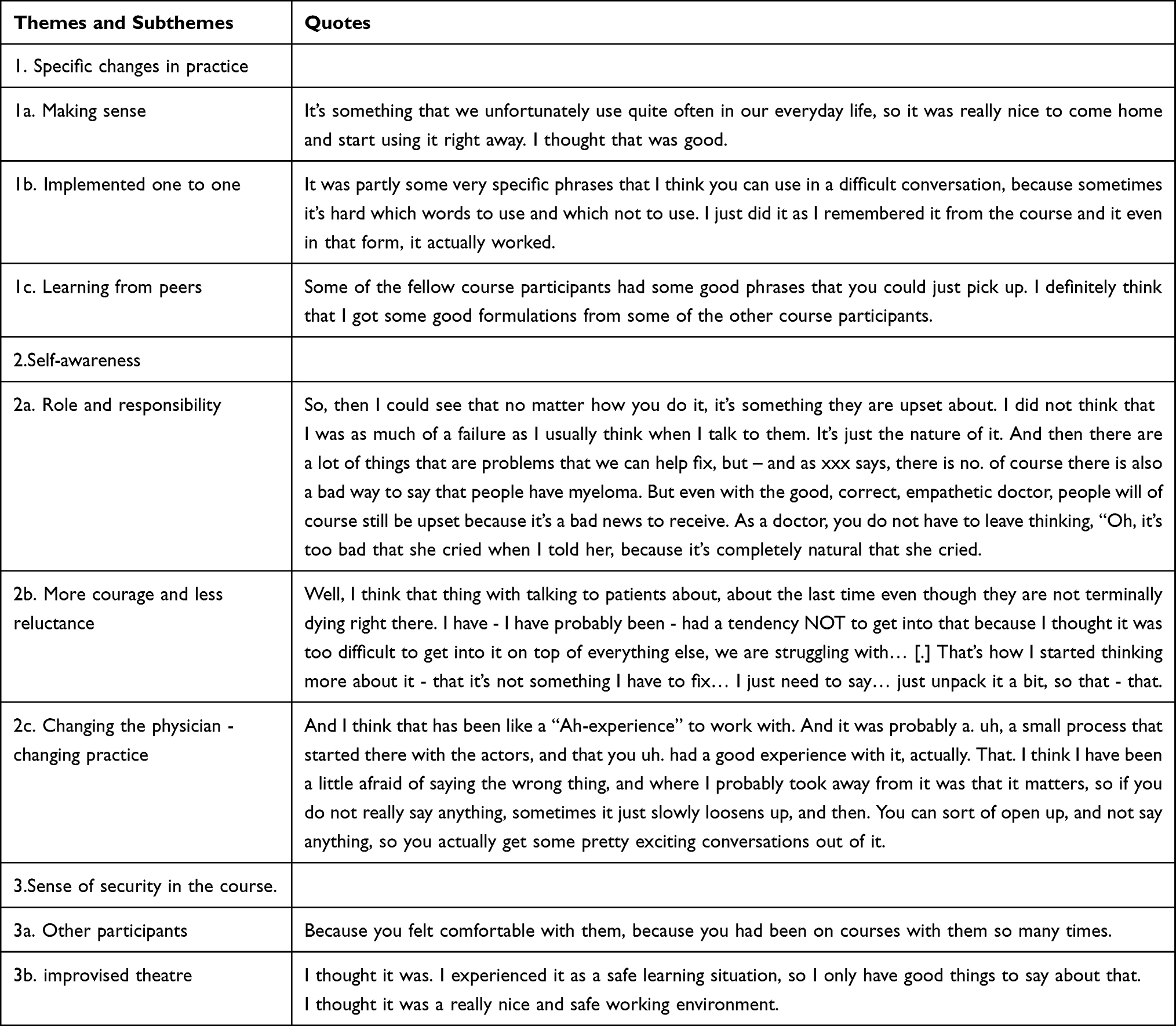 |
Table 4 Qualitative Assessment |
Specific Changes in Practice
The first theme involved how the participants had implemented aspects from the course directly in their own practice. The theme comprised three subthemes. They explained how specific aspects of the course made sense in their clinical practice. They could immediately see how the teaching was relevant for specific situations in clinical practice, and they had implemented several aspects of the course one to one in clinical practice, for example specific sentences learned during the improvised theatre. They explained how they had learned from their peers. This referred to specific sentences or reflections from practices of their peers, that they had implemented in their own practice.
Self-Awareness
The second theme involved how the course had facilitated a change in the participants self-awareness. It comprised three subthemes. They explained how after the course their views upon their role and responsibility in relation to patients had changed. Participants explained that they had become more accepting of the things they could not “fix”, such as patients’ and relatives’ sadness and grief. They had begun seeing their role as more supporting and comforting than curing the incurable of the patient’s illness. They also explained how they experienced having more courage and less reluctance for communicating difficult topics with patients. They summed it up in the third subtheme as how the course by changing their perceived role as a physician subsequently had changed their practice.
Sense of Security in the Course
The third theme comprised two subthemes involving the importance of the participants feeling secure during the course. They believed benefit from the course was caused by a sense of security in the course. This security was both in relation to the other participants in the course as well as particularly feeling safe during the improvised theatre. The participants emphasized how important it was for them to feel secure, or else they did not think they would have profited from the course.
Discussion
We implemented a 2-day course with a curriculum consistent with the “education for life” model as recently proposed by the health Policy for education of health professionals.16 The course curriculum comprised training in patient centered communication, combined with reflections on how healthcare professionals can learn to live their own life, preserve mental wellbeing, and prevent burnout.
This study, combining validated quantitative questionnaires with qualitative interviews, demonstrate the value of mixed methods. Method triangulation by using different methods to collect data concerning the same phenomenon increase the validity of the results.17 The qualitative methodology add depth and understanding of the subject.18 Despite the low number of participants, the improvement in self-efficacy scores after the course, though mostly non-significant, show a trend towards improved self-efficacy in serious illness communication, and the convergence with the interviews consolidate this observation. The items with significant increase in self-efficacy were concordant between the EC and ACP self-efficacy scales, addressing the ability to endure situations without a solution and discuss insecurity. This were in line with the altered perception of role as a physician described in the interviews, accepting the things they could not “fix” and seeing their role as more supporting and comforting, with more courage and less reluctance to discuss difficult topics. The confidence that they could find the time to discuss ACP were low and remained low. The themes emerging in the interviews provide valuable guidance for future courses, and document that a two-day course has the capability of changing both participants’ perception of their role as a physician and their clinical practice.
Exercises were conducted in groups of maximum eight, and this, together with previous acquaintance with their peers, ensured the sense of security that was fundamental for participants.
The course was mandatory and 75% of participants answered all questionnaires, reducing selection bias. This was not the case for the interviews and controls, were only a subgroup participated.
The self-efficacy scores were not significantly associated with seniority, as all participants were undergoing specialist training in hemato-oncology, and therefore within a 5-year range of experience. The mean scores increased after the course in all 6 self-efficacy questions in the EC scale, whereas 13 out of 17 items and the single item score on the ACP scale showed increase in mean score. This could be chance findings, and calls for reproduction in future courses, increasing the number of participants. The control group only answered the questionnaires once, and it was therefore not possible to assess if variation between timepoints occurred to a similar degree in this group. The ACP scale is a very comprehensive assessment of efficacy in advance care planning but was not designed to evaluate this intervention, and not all subjects in the scale were included in the course curriculum. The items with the lowest scores were “finding the time to discuss ACP” and “discuss how to fill out a living will”, the former addressing an organizational issue, and the latter not addressed in the course. An improvement in all 17 items could therefore not be expected. A further weakness in self-assessment of efficacy in communication is the lacking patient perspective but was not within scope of this study.
We found a prevalence of moderate to severe personal and work-related burnout of respectively 37% and 29%. This is high, compared to a recent survey of Danish vascular surgeons, reporting moderate to severe personal burnout in 28% and work-related burnout in 16%.19 The prevalence of moderate to severe patient related burnout was lower but still high compared to vascular surgeons (10% vs 4%). Of note, no participants reported severe patient related burnout (score of 75 or higher) in the present study. A score over 50 has been shown to predict future sickness absence, sleep problems, use of painkillers, and intention to quit.14 The high scores for work related and personal burnout underscore the relevance of addressing burnout in hematology specialist training. A meta-analysis of interventions to reduce burnout has shown that institutional interventions are more effective than individual-focused interventions.7
Conclusion
The study shows that a short mandatory course of formal training can increase physician self-efficacy in serious illness communication and alter clinical practice and perception of roles. The prevalence of burnout was high. Future research should aim to confirm the effectiveness in a larger study not restricted to hemato-oncology. The self-efficacy ACP and EC scales can be used for evaluation, though we suggest tailoring or selecting self-efficacy questions to fit the content of the intervention or course. Qualitative assessment with structured interviews adds value to questionnaires.
The physicians’ confidence in their ability to find time to conduct ACP conversations remained low, and constitutes an organizational barrier, as described by Andersson and Sandgren in their recent study of organizational readiness to change.20 The high level of burnout among physicians in hemato-oncology calls for institutional interventions in addition to training. A work organization allocating time to conduct goals of care conversations could be one the means.
Funding
The study received financial support from the Danish Health Authority.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fulmer T, Escobedo M, Berman A, Koren MJ, Hernández S, Hult A. Physicians’ Views on Advance Care Planning and End-of-Life Care Conversations. J Am Geriatr Soc. 2018;66(6):1201–1205. doi:10.1111/jgs.15374
2. Berkhof M, van Rijssen HJ, Schellart AJ, Anema JR, van der Beek AJ. Effective training strategies for teaching communication skills to physicians: an overview of systematic reviews. Patient Educ Couns. 2011;84(2):152–162. doi:10.1016/j.pec.2010.06.010
3. Chung HO, Oczkowski SJ, Hanvey L, Mbuagbaw L, You JJ. Educational interventions to train healthcare professionals in end-of-life communication: a systematic review and meta-analysis. BMC Med Educ. 2016;16:131. doi:10.1186/s12909-016-0653-x
4. Moore PM, Rivera S, Bravo-Soto GA, Olivares C, Lawrie TA. Communication skills training for healthcare professionals working with people who have cancer. Cochrane Database Syst Rev. 2018;7(7):CD003751. doi:10.1002/14651858.CD003751.pub4
5. Paladino J, Bernacki R, Neville BA, et al. Evaluating an Intervention to Improve Communication Between Oncology Clinicians and Patients With Life-Limiting Cancer: a Cluster Randomized Clinical Trial of the Serious Illness Care Program. JAMA Oncol. 2019;5(6):801–809. doi:10.1001/jamaoncol.2019.0292
6. Mata ÁNS, de Azevedo KPM, Braga LP, et al. Training in communication skills for self-efficacy of health professionals: a systematic review. Hum Resour Health. 2021;19(1):30. doi:10.1186/s12960-021-00574-3
7. West CP, Dyrbye LN, Erwin PJ, Shanafelt TD. Interventions to prevent and reduce physician burnout: a systematic review and meta-analysis. Lancet. 2016;388(10057):2272–2281. doi:10.1016/S0140-6736(16)31279-X
8. Boissy A, Windover AK, Bokar D, et al. Communication Skills Training for Physicians Improves Patient Satisfaction. J Gen Intern Med. 2016;31(7):755–761. doi:10.1007/s11606-016-3597-2
9. Messerotti A, Banchelli F, Ferrari S, et al. Investigating the association between physician’s self-efficacy regarding communication skills and risk of “burnout”. Health Qual Life Outcomes. 2020;18(1):271. doi:10.1186/s12955-020-01504-y
10. Wert K, Donaldson AM, Dinh TA, et al. Communication Training Helps to Reduce Burnout During COVID-19 Pandemic. Health Serv Res Manag Epidemiol. 2023;10:233339282211480. doi:10.1177/23333928221148079
11. Hvidt EA, Ammentorp J, Søndergaard J, Timmermann C, Hansen DG, Hvidt NC. Developing and evaluating a course programme to enhance existential communication with cancer patients in general practice. Scand J Prim Health Care. 2018;36(2):142–151. doi:10.1080/02813432.2018.1459235
12. Baughman KR, Ludwick R, Fischbein R, et al. Development of a Scale to Assess Physician Advance Care Planning Self-Efficacy. Am J Hosp Palliat Care. 2017;34(5):435–441. doi:10.1177/1049909115625612
13. Kristensen TS, Borritz M, Villadsen E, Christensen KB. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress. 2005;19(3):192–207. doi:10.1080/02678370500297720
14. Borritz M, Rugulies R, Bjorner JB, Villadsen E, Mikkelsen OA, Kristensen TS. Burnout among employees in human service work: design and baseline findings of the PUMA study. Scand J Public Health. 2006;34(1):49–58. doi:10.1080/14034940510032275
15. Braun V, Clarke V. Reflecting on reflexive thematic analysis. Qualitative Research in Sport. Exercise and Health. 2019;11(4):589–597. doi:10.1080/2159676X.2019.1628806
16. Frenk J, Chen LC, Chandran L, et al. Challenges and opportunities for educating health professionals after the COVID-19 pandemic. Lancet. 2022;400(10362):1539–1556. doi:10.1016/S0140-6736(22)02092-X
17. Carter N, Bryant-Lukosius D, DiCenso A, Blythe J, Neville AJ. The use of triangulation in qualitative research. Oncol Nurs Forum. 2014;41(5):545–547. doi:10.1188/14.ONF.545-547
18. Stige B, Malterud K, Midtgarden T. Toward an agenda for evaluation of qualitative research. Qual Health Res. 2009;19(10):1504–1516. doi:10.1177/1049732309348501
19. Møller CM, Clausen T, Aust B, Eiberg JP. A cross-sectional national study of burnout and psychosocial work environment in vascular surgery in Denmark. J Vasc Surg. 2022;75(5):1750–1759. doi:10.1016/j.jvs.2021.11.042
20. Andersson S, Sandgren A. Organizational readiness to implement the Serious Illness Care Program in hospital settings in Sweden. BMC Health Serv Res. 2022;22(1):539. doi:10.1186/s12913-022-07923-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.