Back to Journals » Patient Preference and Adherence » Volume 19
Impact of the Information-Motivation-Behavioral Skills Model Based Medication Literacy Intervention on Medication Self-Management Capacity in Stroke Patients: A Randomized Controlled Trial
Authors Ma L, Liu Z, Chen X, Zhang Q, Chu T, Chen X, Zhang J, Sun R, Wu Y ![]()
Received 24 July 2025
Accepted for publication 18 November 2025
Published 27 November 2025 Volume 2025:19 Pages 3785—3805
DOI https://doi.org/10.2147/PPA.S555955
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ramón Morillo-Verdugo
Linlin Ma,1,2,* Zhimin Liu,3,* Xueru Chen,2 Qian Zhang,2 Tianyu Chu,2 Xian Chen,2 Jiajia Zhang,2 Renjuan Sun,1 Yibo Wu4
1Department of Neurology, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China; 2Wuxi School of Medicine, Jiangnan University, Wuxi, People’s Republic of China; 3Department of Neurology, Binzhou People’s Hospital Affliction to Shandong First Medical University, Binzhou, People’s Republic of China; 4Obstetrics, Gynecology and Reproduction Research Center, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renjuan Sun, Department of Neurology, Affiliated Hospital of Jiangnan University, Wuxi, People’s Republic of China, Email [email protected] Yibo Wu, Obstetrics, Gynecology and Reproduction Research Center, Affiliated Hospital of Jiangnan Universit, Wuxi, People’s Republic of China, Email [email protected]
Purpose: This study aimed to evaluate the effectiveness of a multidisciplinary collaborative medication literacy intervention, grounded in the Information-Motivation-Behavioral Skills (IMB) model, on the medication self-management capacity, stroke-related knowledge, medication literacy, medication adherence, and health status of stroke patients.
Patients and Methods: This single-blind, two-arm RCT in a Wuxi tertiary hospital enrolled 127 participants, randomized into intervention (n = 63) and control groups (n = 64). The intervention group received a medication literacy intervention based on the Information-Motivation-Behavioral Skills (IMB) model through multidisciplinary collaboration, while the patients in the control group received standard care and follow-up after discharge. The primary outcome measure was medication self-management capacity, while secondary outcome measures included stroke-related knowledge, medication literacy, medication adherence, blood pressure, lipid levels, and unplanned readmission rates. The generalized estimating equation (GEE) model was employed to assess the effectiveness of the intervention.
Results: Compared with the control group, the intervention group showed significant improvement in medication self-management capacity (βday of discharge = 1.41, p = 0.045, Cohen’s d = 0.31; β4 weeks = 2.74, p = 0.003, Cohen’s d = 0.52; β12 weeks = 3.46, p = 0.003, Cohen’s d = 0.74). Significant improvements were also observed in stroke-related knowledge (β4 weeks = 2.67, p < 0.001; β12 weeks = 3.97, p < 0.001), medication literacy (β4 weeks = 1.22, p < 0.001; β12 weeks = 1.18, p < 0.001), medication compliance (β4 weeks = 1.07, p = 0.034; β12 weeks = 1.45, p = 0.013), and blood pressure reduction (p < 0.05). The intervention did not significantly affect blood lipids or unplanned readmission rates (p > 0.05). The sensitivity analysis using the PP method indicated that the obtained results were comparable to the ITT results, suggesting that the preliminary research results and conclusions of the medication literacy intervention based on multidisciplinary collaboration were reliable.
Conclusion: The medication literacy intervention based on the Information-Motivation-Behavioral Skills (IMB) model effectively enhances the medication self-management capacity of stroke patients. It positively influences several outcomes, including stroke-related knowledge, medication literacy, medication adherence, blood pressure.
Keywords: medication literacy, medication adherence, stroke, intervention studies
Introduction
Stroke has long been recognized as a group of diseases arising from vascular lesions in the brain, primarily categorized into two types: ischemic stroke and hemorrhagic stroke.1 The “Global Stroke Fact Sheet”, published by the World Stroke Organization (WSO) in 2022, revealed that stroke has become the second leading cause of death globally, with approximately 6.5 million fatalities attributed to it annually.2 Currently, the treatment and prevention of predominantly depend on pharmacotherapy. However, due to the intrinsic nature of stroke and the various complications arising from brain tissue damage, patients predominantly require a prolonged regimen of multiple medications. Previous research has indicated that elderly commonly patients are typically administered a diverse array of drugs during hospitalization, with usage ranging from 5 to 34 different medications,3 Furthermore, during the rehabilitation phase post-discharge, it has been reported that 60% of commonly patients continue to require more than five medications concurrently.4 The combination of multiple medications commonly complicates the treatment regimen,5 thereby increasing the challenges associated with long-term medication management. Consequently, ensuring the safe and continuous administration of medications for stroke patients remains a significant challenge for healthcare professionals.
The World Health Organization (WHO) has long emphasized that medication self-management is an indispensable component of health management,6 which is recognized as crucial for disease control, reducing complications, improving quality of life, and minimizing the risk of recurrence in stroke patients.7 However, the current state of medication self-management in stroke patients presents numerous challenges. A study examining the self-management capabilities of stroke patients revealed that particularly poor medication self-management abilities were present,8 with missed medications or medication errors being prevalent.9 Intermittent medication adherence was identified as the most common issue during the home rehabilitation phase. Various factors may limit medication self-management in stroke patients, including advanced age,10 insufficient and biased medication knowledge,11,12 inadequate social support,13 and poor medication adherence. Clearly, inadequate medication self-management can lead not only to poor medication adherence and an increased risk of adverse medication reactions but also to the recurrence or exacerbation of the disease, such as subsequent strokes and worsening neurological deficits. Therefore, healthcare professionals must prioritize the medication self-management of stroke patients and implement targeted intervention strategies.
Numerous existing studies have demonstrated that enhancing medication literacy can improve medication adherence14 and reduce adverse medication reactions,15 thereby standardizing patients’ medication self-management behaviors regarding medication. Specifically, medication literacy is defined as the ability of individuals to effectively obtain, evaluate and apply medication-related information throughout the medication process, enabling them to make informed health decisions and maintain or promote their health.16 For stroke patients, medication literacy encompasses not only the understanding of fundamental information such as medication names, dosages, and timing of administration, but also awareness of side effects, medication interactions, and necessary adjustments to medications during recovery. Currently, medication literacy interventions including health education and technical guidance have a positive impact on the outcome of medication self-management. For instance, Smith17 conducted five lectures on health behavior skill changes for stroke patients, integrating individual assessments with group interventions, which resulted in significant improvements in medication adherence and patients’ self-efficacy. Similarly, Solmaz18 found that, with the assistance of intelligent auxiliary tools, patients’ disease-related knowledge levels could be enhanced, leading to significant improvements in medication adherence and an overall elevation in medication self-management. Although most current intervention studies on medication literacy focus on elderly patients with chronic diseases, such as myocardial infarction,19 there is a notable lack of intervention studies addressing medication literacy specifically for stroke patients.
Medication literacy interventions aimed at enhancing medication self-management are more likely to succeed when grounded in a theoretical framework. The Information-Motivation-Behavioral Skills Model, proposed by Fisher20 in 1992, is widely acknowledged as a robust behavior change theory. This model underscores the causal relationships among information, motivation, and behavioral skills, positing that these three factors interact to collectively influence individual behavior change. Specifically, accurate information provides a rationale for behavior change, motivation propels individuals to take action, and behavioral skills facilitate the effective implementation of that action. When these three components reach a sufficient level, individuals are more inclined to experience behavior change. To date, interventions based on the IMB model have demonstrated efficacy in improving patients’ health behaviors, including adherence to treatment in chronic obstructive pulmonary disease,21 coronary heart disease,22 diabetes,23 and other chronic diseases. However, there is a notable absence of such applications aimed at enhancing medication self-management among stroke patients.
To fill the research gap in this field, we have identified medication literacy as a pivotal focus. Utilizing the IMB model as the theoretical framework, we have established a multidisciplinary team comprising nurses, doctors and pharmacists. This team will provide medication literacy interventions for patients, aiming to effectively enhance the medication literacy levels of stroke patients through this program. Our objective is to standardize their medication self-management behaviors, thereby improve health-related outcomes.
Materials and Methods
Theoretical Framework
The IMB model provided the theoretical basis for this study (Figure 1). Specifically, a multidisciplinary collaboration team, consisting of nurses, physicians, and pharmacists, was established. Utilizing the IMB model as the intervention framework, the team aimed to provide patients with a comprehensive four-dimensional medication literacy intervention. This research framework was proposed based on the findings from a literature review and an investigation of the current situation.
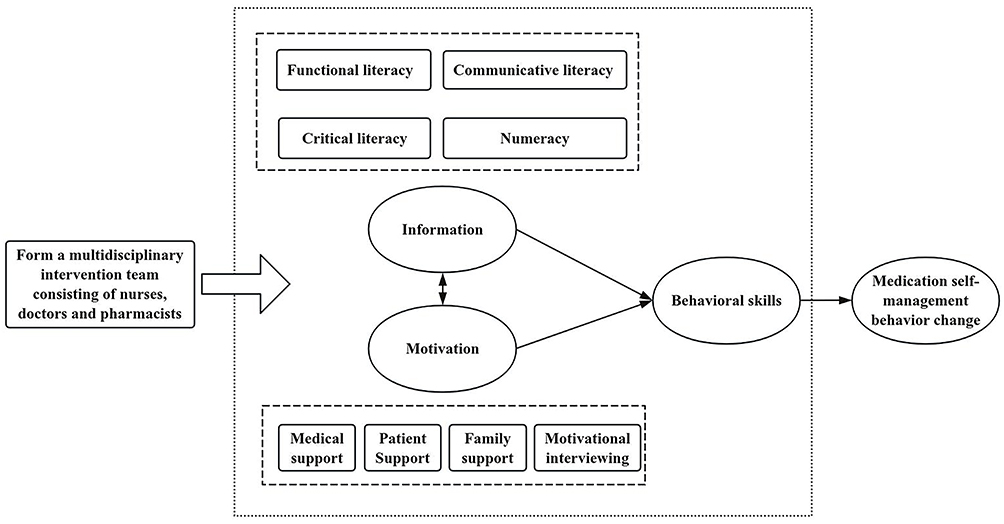 |
Figure 1 Information-Motivation-Behavioral Skills (IMB) model (adaptation to our research). |
Study Design and Setting
This study was conducted as a three-month, single-blind, two-arm randomized controlled trial to compare the effects of an IMB model-based medication literacy intervention with those of usual care on medication self-management in stroke patients. This study was carried out in a tertiary hospital located in Wuxi, Jiangsu Province. The study protocol received approval from the Research Ethics Committee of the Affiliated Hospital of Jiangnan University (LS2023063) and was registered with the Chinese Clinical Trial Registry (ChiCTR2400084673). Informed consent was obtained from all participants.
Participants
From June 2024 to August 2024, inpatients diagnosed with stroke were recruited from the Department of Neurology at a Class III Grade A hospital in Wuxi using convenience sampling. Participants were eligible for the study if they met specific inclusion and exclusion criteria. The inclusion criteria were as follows: ① age ≥60 years old; ② patients who met the diagnostic criteria for stroke and were confirmed by head CT or MRI; ③ Barthel Index (BI) >60 points,24 indicating a certain level of self-care ability; ④ hospital stay of ≥7 days; ⑤ clear cognitive status with adequate communication skills; ⑥ voluntary participation. The exclusion criteria were: ① patients with hearing impairment, speech impairment, dementia, or cognitive impairment who could not cooperate with the researchers; ② severe dysfunction of lungs, heart, liver, or kidneys; ③ participation in other similar studies.
Sample Size
Sample size estimation was conducted based on the results of a previous randomized controlled trial,25 which identified an effect size (Cohen’s d) of 0.58 for the difference in medication self-management levels between the two groups. A minimum of 48 participants per group was determined to be necessary, as calculated with G*Power 3.1 software (Germany), to ensure that the study achieved at least 80% power to reject the null hypothesis at a significance level of 0.05. Furthermore, accounting for a 20% sample dropout rate, the final required sample size was adjusted to 127 participants, comprising 63 individuals in the intervention group and 64 in the control group.
Interventions
Intervention Group
Prior to the intervention, a multi-professional team comprising nurses, physicians, and pharmacists was established. Stroke specialist nurses served as the primary executioner of the intervention program, delivering comprehensive medication care services. They also acted as a communication bridge between physicians and pharmacists, accurately conveying physicians’ treatment intentions and pharmacists’ medication recommendations, thereby facilitating effective communication. Similarly, cardiovascular specialist nurses provided patients with health education regarding hypertension, hyperlipidemia, hyperglycemia, and other prevalent conditions. They offered personalized medication education and guided patients in regularly monitoring blood pressure, blood glucose and other relevant indicators. Concurrently, physicians conducted comprehensive assessments of stroke patients, developed individualized treatment plans, and selected the most appropriate medications and treatment strategies based on the patients’ specific conditions, complications, and overall health status. As key experts in medication therapy management, pharmacists were tasked with reviewing the patient’s medication regimens to ensure the rationality, safety, and efficacy of medication selection. Furthermore, pharmacists provide patients with detailed medication counseling, including information on medication of action, potential side effects, and possible interactions, to enhance patients’ understanding of their treatment.
Development of the intervention: The initial draft of the intervention program was developed based on findings from a comprehensive literature review and a cross-sectional survey. This draft was further refined in alignment with the theoretical framework of the IMB model. Subsequently, two rounds of Delphi expert consultations were conducted to revise and enhance the preliminary plan. Prior to the formal implementation of the intervention, the final draft of the medication literacy intervention plan, grounded in the IMB model, was formulated based on feedback from the pre-experiment. This plan encompasses a total of seven themes: (1) build relationships to assess needs, (2) access and exchange of disease information, (3) application of medication information understanding, (4) medication management skills were improved, (5) medication guidance at discharge, (6) medication management behaviors were strengthened, and (7) follow-up.
Implementation of the intervention: The intervention was implemented over a total duration of 12 weeks, consisting of four inpatient group sessions, two individual sessions. Additionally, three follow-up telephone calls were conducted to reinforce the intervention. Each group session lasted between 30 to 40 minutes and was conducted in the neurology training room, while the one-to-one intervention lasted was 15 to 20 minutes, conducted either at the patient’s bedside or in the outpatient department.
The theme of the first session was to build relationships to assess needs. Aimed to build a trusting relationship with the patient and evaluate their needs. The researchers first provided a comprehensive explanation of the research’s purpose, process, expected benefits, and potential risks to the participants, who then signed a written informed consent form after fully understanding the information. Subsequently, the researchers guided the patients in describing their medication experiences to gain insights into their medication usage and any associated problems.
The theme of the second session focused on the access and exchange of disease information. The stroke specialist nurse educated the patients about stroke-related knowledge to help them develop an accurate perception of their condition.
The theme of the third session focused on the application of medication information understanding. The objective was to educate the patient about the relevant knowledge concerning stroke medications and to enhance family support in fostering accurate medication beliefs. The stroke specialist nurse provided informational guidance, and the intervention’s primary content was integrated with QR code health education videos and cards detailing common stroke medications. Additionally, the head nurse of the neurology department developed a family system assessment form for the patient. The neurology doctor introduced available community resources, such as community pharmacy clinics and family-contracted doctors, to assist the patient in establishing a social support network. Furthermore, the pharmacist offered behavioral skills guidance through scenario simulation and role-playing.
The theme of the fourth session was the enhancement of medication management skills. The head nurse of the neurology department emphasized the importance of adhering to medication for secondary stroke prevention. Concurrently, the cardiovascular specialist nurse instructed the patient on the safe use of medication aids and guided them in accurately measuring blood pressure, monitoring blood sugar, and administering insulin, thereby improving the patient’s communication skills.
The theme of the fifth session centered on medication guidance at discharge. The aim was to educate the patient about home medication practices, provide discharge medication instructions, and enhance the patient’s self-efficacy. The stroke specialist nurse delivered guidance on medication safety and conducted motivational sessions to encourage the patient to express their genuine thoughts and feelings regarding medication use and the challenges they faced. The neurology doctor assisted in identifying the types and causes of the patient’s medication issues and provided tailored solutions based on the patient’s specific circumstances, incorporating physical demonstrations and medication logs for behavioral skills training.
The theme of the sixth session focused on reinforcing medication management behaviors, with the objective of standardizing patients’ medication self-management during their home stay. Stroke specialist nurses and cardiovascular specialist nurses regularly shared approximately 10-minute health education videos about stroke health in the “Stroke Medication Management WeChat Group”. Additionally, doctors and pharmacists addressed questions within the group to clarify doubts raised by patients and their caregivers. During outpatient follow-ups, pharmacists reviewed patients’ medication logs and provided scientifically-based recommendations for any missed doses or adverse reactions.
The theme of the seventh session was follow-up, aimed at assessing patients’ home medication management subsequent to the completion of the medication literacy intervention based on the IMB model. Researchers conducted monthly telephone follow-ups and provided corrective guidance for any medication issues that arose during the patients’ home stay.
Before the study commenced, the intervention personnel underwent training on implementing the intervention measures. Following each intervention, the personnel responsible for the corresponding topic were required to submit an intervention checklist to ensure the thoroughness of the intervention content. If the completion rate of the intervention checklist reached 20%, additional training for the intervention personnel would be considered. Detailed information is provided in Table 1.
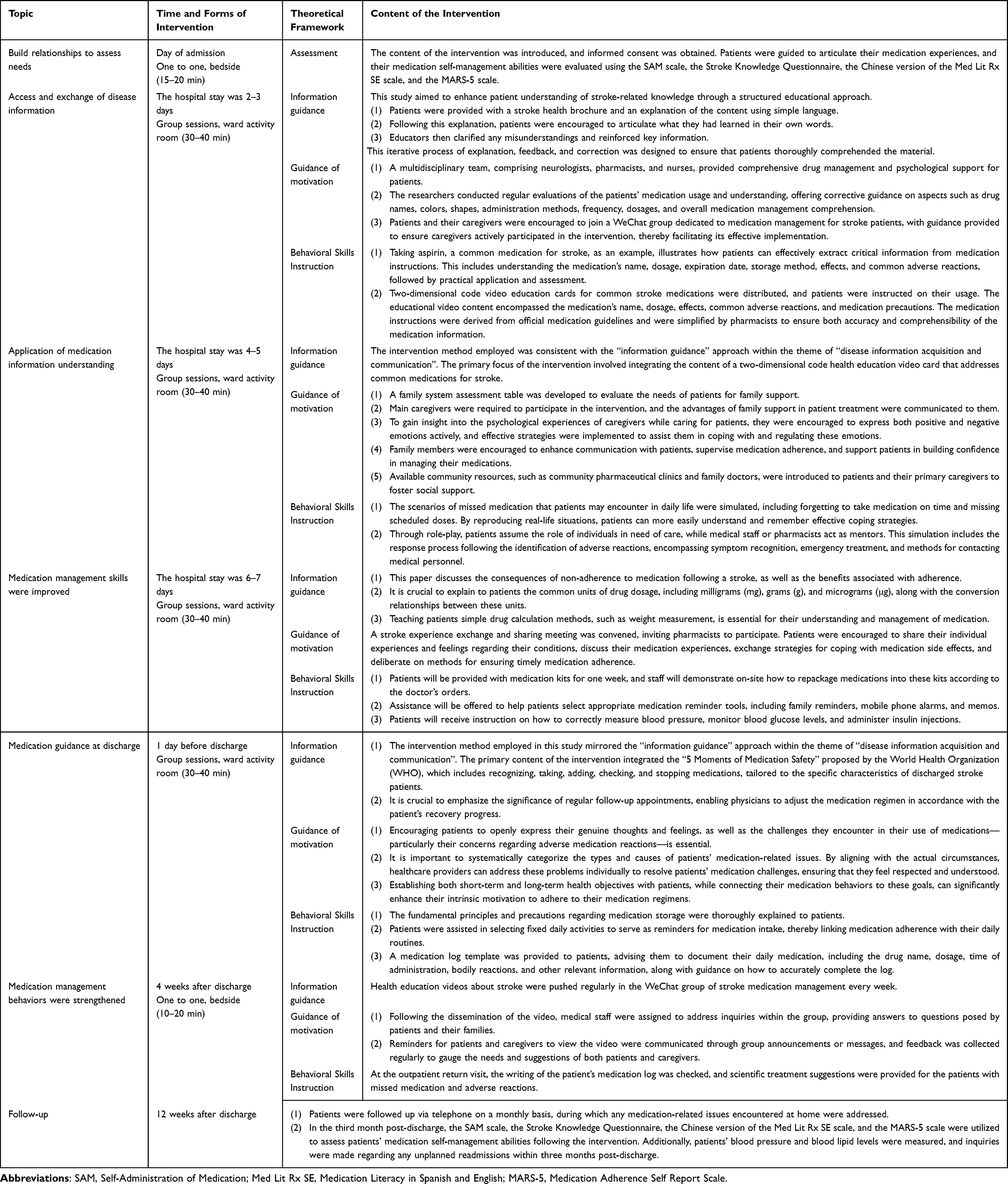 |
Table 1 Details of Medication Literacy Intervention Based on the IMB Model |
Control Group
Patients in the control group received standard nursing care and discharge follow-up. The specific nursing interventions encompassed the diagnosis and treatment of stroke-related conditions, which primarily included: (1) medication observation and condition monitoring; (2) nursing care for stroke symptoms; (3) daily living assistance; (4) discharge health education, along with consultation services regarding the patient’s condition and medication management. Following discharge, two follow-up visits were conducted at one and three months.
This study implemented multi-dimensional preventive measures to mitigate the risks of cross-contamination associated with shared personnel and resources. Firstly, specialized training was conducted for the intervention personnel, and data collectors were instructed to standardize their data collection practices. The roles of the medical teams and researchers were clearly delineated between the intervention group and the control group, with specific personnel designated to implement the intervention for each group. Secondly, the intervention environment and teaching aids were thoroughly cleaned and organized after each intervention. Thirdly, access to the “Stroke Patient Medication Management WeChat Group” was restricted exclusively to the intervention group. Finally, the independence of the group-based intervention was emphasized to both patients and their primary caregivers prior to the intervention, as well as during each intervention and follow-up, with a strict prohibition on the communication of intervention-related content between the groups.
Outcome Measures
Data were collected at four time points: baseline (T0), day of discharge (T1), week 4 (T2), week 12 (T3). The primary outcome was medication self-management capacity, which was assessed by the Self-Administration of Medication Tool (SAM). The secondary outcomes included stroke-related knowledge, medication literacy, medication adherence, blood pressure, blood lipid levels, and the rate of unplanned readmission.
Medication Self-Management Capacity
The Self-Administration of Medication Tool (SAM) was developed by Manias et al26 and subsequently translated into Chinese by Lin et al.27 SAM is primarily designed to comprehensively evaluate patients’ capacity for self-managing their medications. It encompasses three dimensions: capable to self-medicate (11 items), knowledge about medications (7 items), and experience with self-medication (6 items), totaling 24 items. Each item is scored using a 5-point Likert scale, which includes responses such as “never”, “rarely”, “sometimes”, “often”, and “always”, with corresponding scores ranging from 0 to 4. Higher scores indicate better medication self-management. Scores equal to or greater than 60 are considered indicative of competent medication management, while scores below 60 suggest incompetence. The Cronbach’s α coefficient of the scale is 0.913.
Stroke-Related Knowledge
The stroke-knowledge questionnaire was developed by Yao Qiping,28 a Chinese scholar, encompassing six dimensions: preemptive symptoms, emergency treatment, risk factors, safe medication, behavior, and rehabilitation knowledge, totaling 40 items. A dichotomous scoring system was utilized, assigning 1 point for a correct answer and 0 points for an incorrect answer or “do not know” response. The total score ranged from 0 to 40, with higher scores indicating a greater level of knowledge mastery. The Cronbach’s α coefficient of the questionnaire is 0.893.
Medication Literacy
The Medication Literacy in Spanish and English (Med Lit Rx SE) was developed by Sauceda et al29 and adapted into Chinese by Zheng Feng et al30 in 2016. This scale simulates four medication use scenarios and consists of 14 items, scored on a 2-point scale, with a maximum score of 14. The medication literacy level of the evaluated individual can be objectively assessed, with higher scores indicating greater levels of medication literacy. The specific evaluation criteria are as follows: a total score exceeding 10 points indicates a high level of medication literacy; a score between 4 and 10 points signifies a medium level; and a score below 4 points reflects poor medication literacy. The scale has been utilized in studies involving populations such as kidney transplant recipients31 and individuals with coronary heart disease.32 The Cronbach’s α coefficient of the scale is 0.937.
Medication Adherence
We used the five-item version of the Medication Adherence Self Report Scale (MARS) to evaluate adherence to stroke medication.33 The MARS consists of five general statements about non-adherent behavior on a 5-point Likert scale (1 = always, 2 = often, 3 = sometimes, 4 = rarely, 5 = never), The total score is the sum of the five individual items. A high score indicates a high level of medication adherence. The Chinese version of MARS demonstrated good internal consistency (Cronbach’s α coefficient was 0.870).34
Blood Pressure, Blood Lipids
Systolic blood pressure (SBP), diastolic blood pressure (DBP), triglyceride (TG), and total cholesterol (TC) levels were obtained from the patients’ electronic medical records at the time of admission and subsequently measured again 12 weeks after discharge for analysis.
Unplanned Readmissions
The study defined unplanned readmissions within 12 weeks post-discharge as those resulting from patient deterioration, complications, or other health issues related to stroke. In this study, patients were primarily queried about readmissions through follow-up telephone calls, and their responses were subsequently verified against the hospital’s electronic medical records (EMR) or hospitalization information system (HIS).
Randomization, Allocation Concealment and Blinding
Participants were randomly assigned in a 1:1 ratio to either the intervention group or the control group through simple randomization. This process was conducted using computer-generated random numbers by a research assistant who was unaware of the study’s details. The random numbers and group assignments were sealed in opaque envelopes, which were opened by research assistants after they had assessed the baseline data from participants who provided written informed consent. Given the nature of the intervention, intervention nurses and study participants could not be blinded. However, the outcome assessors and data analysts were blinded to the allocation.
Statistical Analysis
All data were analyzed using IBM SPSS Statistics 27.0 software (IBM Corporation, Armonk, New York, USA). Prior to conducting the statistical analysis, an assessment of outliers and normality tests was performed on the research data. The sample size for this study comprised 127 participants. Given that a sample size of ≥ 50 makes the Kolmogorov–Smirnov test an appropriate method for normality testing,35 this study utilized this test. Quantitative data exhibiting a normal distribution were presented as mean ± standard deviation, while categorical data were reported as frequencies and percentages. Independent sample t-tests and chi-square tests were employed for comparisons between groups. Both primary and secondary outcomes were analyzed according to the intention-to-treat (ITT) principle. Little’s Missing Completely at Random (MCAR) test was conducted to perform to evaluate the nature of missing data. The generalized estimating equation (GEE) model was utilized to evaluate the impact of the intervention on medication self-management capacity, stroke-related knowledge scores, medication literacy, and medication adherence scores. This model is capable of explaining repeated measurement data with internal correlations and is applicable to datasets with missing values due to loss to follow-up.36 It can manage missing data using the quasi-likelihood method without requiring interpolation, under the assumption that the data are missing completely at random.37 Thus, it is particularly suitable for intention-to-treat analysis. The control group (group = 0) and the baseline measurement group (T0) were designated as the reference categories for the GEE model. The interaction term between time and group (group * time) was employed to measure differences and changes in each variable across time points among the groups. Given that we could not identify known prognostic factors for the main outcomes of this study in the target population from the literature, and considering that baseline characteristics were generally comparable among the different groups, we opted not to adjust the baseline covariates in the GEE analysis. Continuous outcome measures were assessed using Cohen’s d (standardized mean difference) to estimate effect size.38 A two-sided p-value < 0.05 was considered statistically significant. To determine the robustness of the research findings, a sensitivity analysis (per-protocol analysis) was conducted in this study.39
Results
Participant Flow
A total of 219 stroke patients were screened prior to the commencement of the study, of which 127 eligible participants were included and randomly assigned to either the intervention group (n = 63) or the control group (n = 64). The CONSORT flowchart is shown in Figure 2. Data collection was completed for 119 participants at T1, 111 at T2, and 104 at T3, the reasons for the dropouts in the intervention group included being transferred to other hospitals, refusal to answer, work commitments, and loss of interest in the study. For the control group, the main reasons for dropout were refusal to answer and loss of contact.
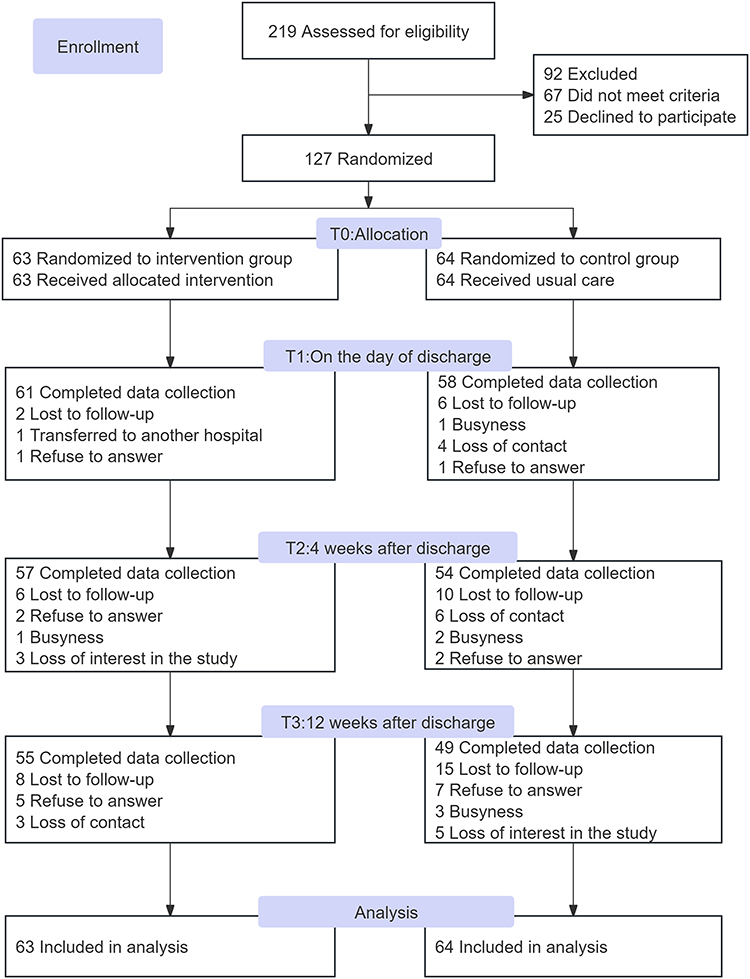 |
Figure 2 The CONSORT flowchart. |
The attrition rate at T3 was 18.1%. In No statistically significant differences were observed in baseline characteristics regarding socio-demographic features and outcome variables between participants who completed the study and those who dropped out (as shown in Supplementary Material Table 1), implying the attrition bias is minimal.
Baseline Characteristics
The mean age of the 127 participants was 67.47 years, with more than half being female (52.0%). Additionally, 70.9% of the participants had received junior high school education or higher. A significant majority, 88.2%, lived with their families, while a minor proportion were unemployed, and the per capita monthly household income was below 3000 yuan. All participants were covered by health insurance. In terms of medical characteristics, the majority of participants had ischemic stroke (89.8%), and 52.8% reported no family history of stroke. Most participants had a disease duration exceeding one year (61.4%) and were prescribed fewer than five types of medication (55.1%). Furthermore, 62.2% of participants took medication twice or more per day without guidance. All patients demonstrated certain self-care abilities. Overall, the mean systolic blood pressure was elevated at 152.07 mmHg, while the mean diastolic blood pressure was 83.51 mmHg. The mean triglyceride level was 1.39 mmol/L, and the total cholesterol level was 3.89 mmol/L, both of which fell within normal ranges. There were no statistically significant differences in baseline characteristics between the two groups (Table 2).
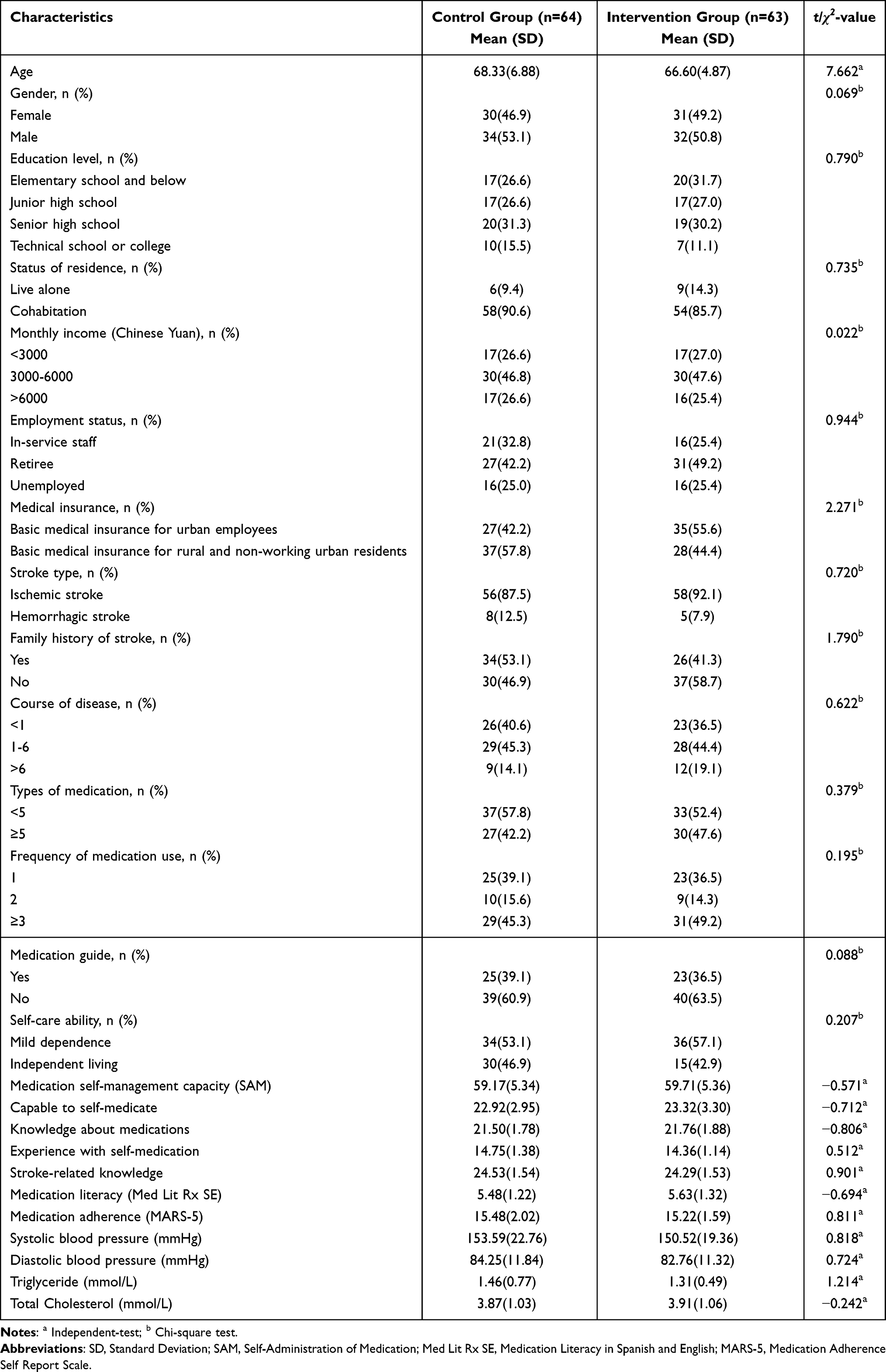 |
Table 2 Baseline Socio-Demographic and Clinical Characteristics for the Intervention and Control Groups |
Outcomes
Effects of the Intervention on Medication Self-Management Capacity
Table 3 and Figure 3A present the research results of the primary outcomes. Little’s test for completely random missingness indicated a non-significant result (p = 0.101), suggesting that the data were missing completely at random. In comparison to the control group, the intervention group demonstrated a significant improvement in medication self-management ability, as measured by the SAM scale at T1 (β = 1.41, p = 0.045). This positive effect was sustained at T2 and T3 (T2: β = 2.74, p = 0.003; T3: β = 3.46, p = 0.003). The effect sizes at T1, T2, and T3 were 0.31, 0.52, and 0.74, respectively, indicating that the medication literacy intervention had a small to moderate effect on enhancing medication self-management. The Generalized Estimating Equations (GEE) results revealed significant interaction effects between the groups and time for the ability to self-medicate (T2: β = 0.98, p = 0.034; T3: β = 1.78, p = 0.010) and experience with self-medication (T2: β = 1.19, p = 0.021; T3: β = 1.14, p = 0.048) at T2 and T3, but no interaction effect was observed at T1. Notably, there were no significant differences in medication-related cognition scores between the two groups at T1, T2, or T3. Figure 3A illustrates the changes in medication self-management capacity scores for the two groups across different intervention time points.
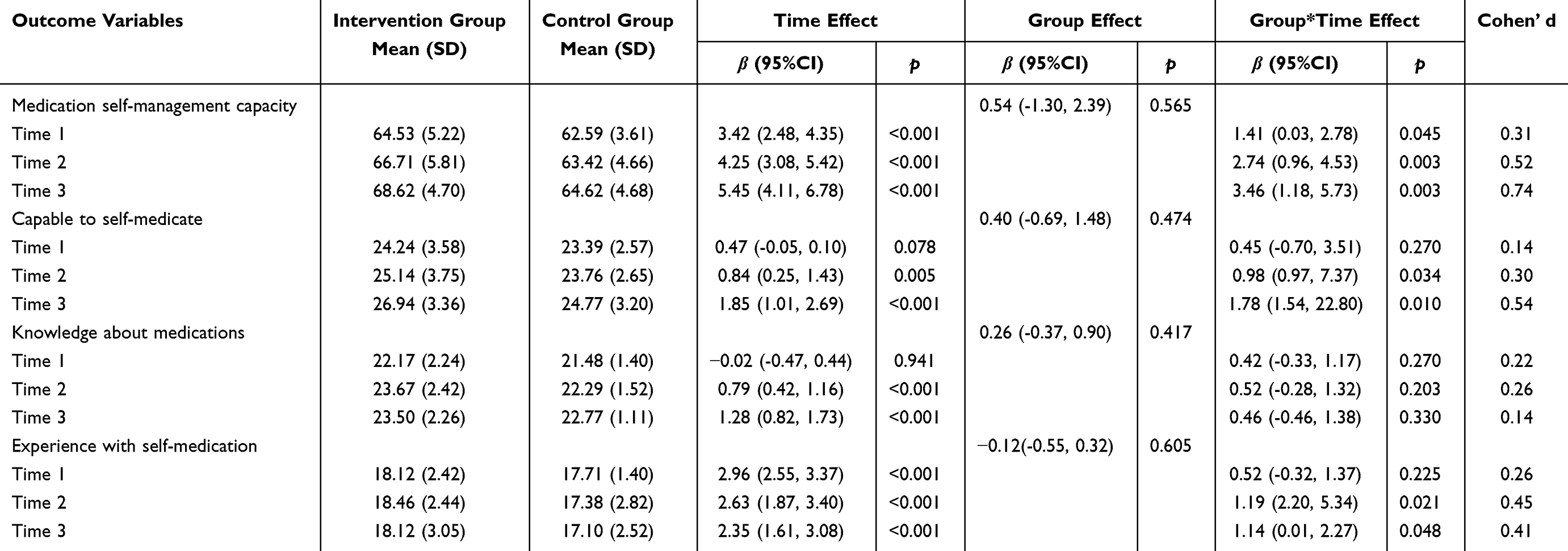 |
Table 3 Generalized Estimating Equation Models of the Comparison of Medication Self-Management Capacity Between the Intervention and Control Groups |
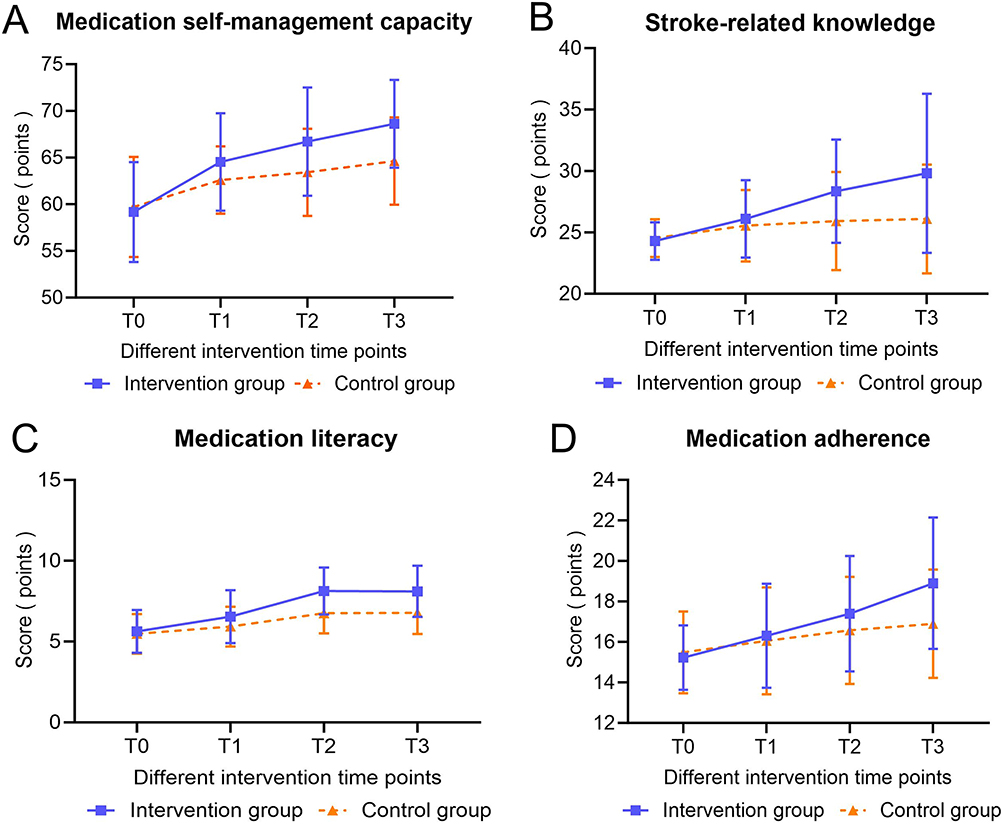 |
Figure 3 Changes in the scores of the medication (A) self-management capacity, (B) stroke-related knowledge, (C) medication literacy and (D) medication adherence of patients were observed. |
Effects of the Intervention on the Level of Stroke-Related Knowledge, Medication Literacy and Medication Adherence
Compared to routine care, the medication literacy intervention significantly enhanced medication literacy (T2: Cohen’s d = 0.89; T3: Cohen’s d = 0.81), demonstrated a moderate effect in improving stroke-related knowledge (T2: Cohen’s d = 0.65; T3: Cohen’s d = 0.71), and showed a small to medium effect on medication adherence (T2: Cohen’s d = 0.39; T3: Cohen’s d = 0.49). At T2 and T3, the intervention group exhibited statistically significant differences in stroke-related knowledge (T2: β = 2.67, p < 0.001; T3: β = 3.97, p < 0.001), medication literacy (T2: β = 1.22, p < 0.001; T3: β = 1.18, p < 0.001), and medication adherence (T2: β = 1.07, p = 0.034; T3: β = 1.45, p = 0.013) when compared to the control group. At T1, the effect sizes for stroke-related knowledge, medication literacy, and medication adherence were minimal, measuring 0.27, 0.32, and 0.19, respectively. Generalized estimating equation (GEE) analysis in Table 4 indicated no significant interaction between group and time for stroke-related knowledge (β = 0.81, p = 0.172), medication literacy (β = 0.46, p = 0.082), and medication adherence scores (β = 0.50, p = 0.278) at T1. Figure 3B–D respectively illustrate the changes in stroke-related knowledge, medication literacy and medication adherence scores for the two groups at different intervention time points.
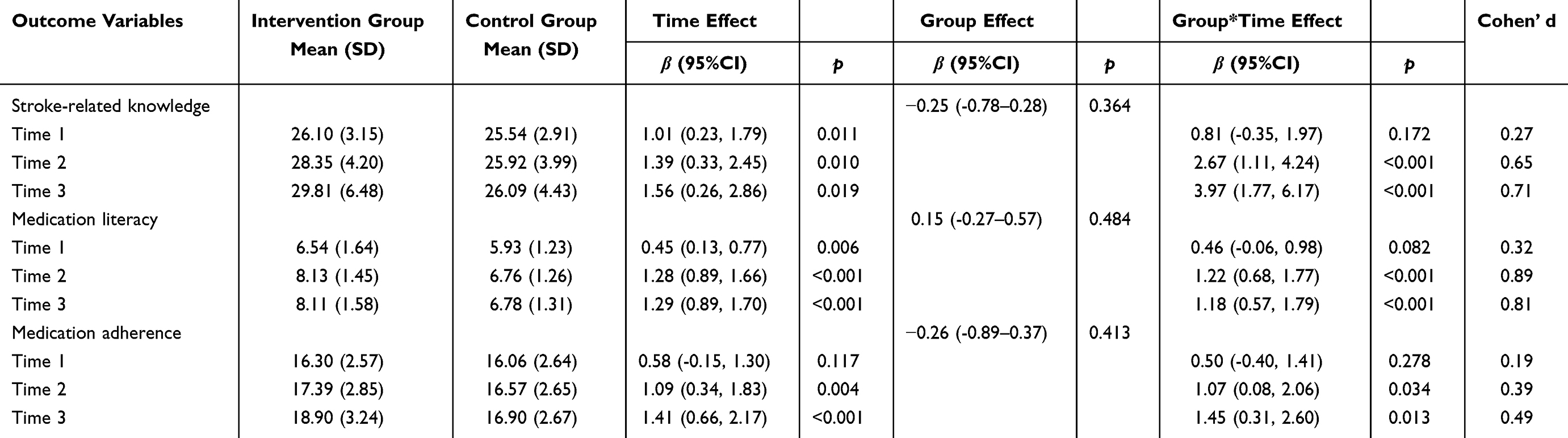 |
Table 4 Generalized Estimating Equation Models of the Comparison of Stroke-Related Knowledge, Medication Literacy and Medication Adherence Between the Intervention and Control Groups |
Effects of the Intervention on Blood Pressure, Blood Lipids, and Unplanned Readmission Rates
The effects of the intervention on blood pressure, blood lipids, and unplanned readmission rates are presented in Table 5 and Table 6. Compared to the control group, both SBP and DBP were significantly lower in the intervention group at T3, with effect sizes of 0.16 and 0.37, respectively. This indicates that the intervention had a mild to moderate effect on blood pressure. However, no significant changes were observed in the levels of TG, TC, or the rate of unplanned readmission in the intervention group (p > 0.05).
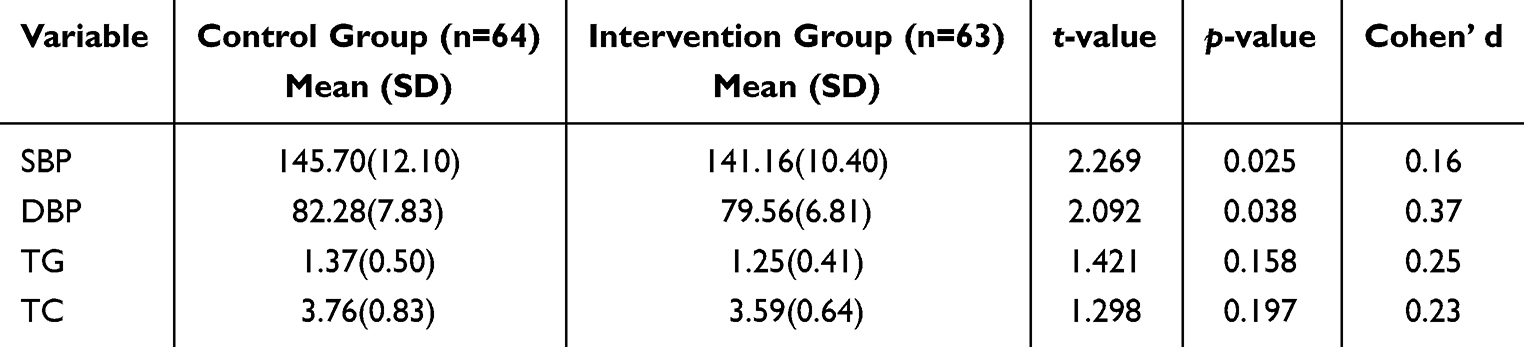 |
Table 5 Pairwise Comparison of Blood Pressure and Blood Lipids Between the Two Groups After Intervention |
 |
Table 6 Pairwise Comparison of Unplanned Hospital Readmission Rates Between the Two Groups After Intervention |
Sensitivity Analysis
Sensitivity analysis is essential for evaluating the robustness of research findings derived from the original data.40 The sensitivity analysis performed using the per-protocol (PP) approach demonstrated that both the primary and secondary outcome indicators yielded results comparable to those obtained from the main analysis based on ITT. This confirmed that the research results and conclusions regarding initial effectiveness of the medication literacy intervention, grounded in multidisciplinary collaboration, were reliable (Supplementary Table 2).
Discussion
The effectiveness of a medication literacy intervention program based on the IMB model for patients with stroke was evaluated in terms of medication-related and health-related outcomes. We found that the intervention produced statistically significant positive effects on enhancing patients’ short-term medication self-management capacity. Additionally, improvements were observed in stroke-related knowledge, medication literacy, medication adherence, and blood pressure. However, the intervention did not yield statistically significant effects on blood lipid levels, including triglycerides and total cholesterol, nor did it affect the rate of unplanned readmission.
The medication literacy intervention based on the IMB model significantly enhanced the participants’ capacity for medication self-management. From the time of admission to 12 weeks post-discharge, the medication self-management levels of stroke patients exhibited a continuous upward trend following the intervention, aligning with the findings of Van.41 Studies have shown that low memory and executive function are linked to inadequate medication self-management.42 Due to the neurological dysfunction associated with the condition, 30% to 60% of stroke patients experience varying degrees of memory decline, attention deficits, and executive dysfunction,43 which severely impairs their ability to manage medications effectively. Consequently, effective medication self-management necessitates a series of cognitive processes, particularly memory and executive functions.
Our study provided patients with essential information about medications through health education. Additionally, we delivered educational videos featuring QR codes for common medications used in stroke management, allowing patients to scan the codes and watch the videos multiple times to reinforce their understanding and facilitate long-term memory retention. Furthermore, we conducted motivational interviews and offered behavioral skills guidance, including training patients to utilize medication reminder tools. This approach enabled patients to acquire specific medication management skills, while their executive functioning improved through simulated scenarios and case analyses. Moreover, a retrospective study examining the correlation between pharmacist-provided medication guidance and medication self-management revealed that the success of medication self-management remains closely tied to the guidance provided by pharmacists, particularly among hospitalized older adults undergoing rehabilitation.44 Ernawati et al45 further illustrated that pharmacist involvement significantly enhances patients’ medication adherence and self-management capabilities, while also reducing the incidence of medication-related problems. Collectively, these findings, along with our current study, underscore the effectiveness of a multidisciplinary intervention team, including pharmacists, in enhancing medication self-management.
The current study highlights that at both the 4th and 12th weeks following the intervention, there was a significant increase in stroke related knowledge among stroke patients, aligning with the findings of previous research.46 This effect can be attributed to several potential mechanisms: our study utilized a feedback method47 to provide informational guidance to patients, coupled with motivational interviewing. This approach empowered patients to better recognize their own abilities and potential, thereby enhancing their self-efficacy in disease management. Consequently, the improvement in self-efficacy encourages patients to engage more actively in learning and rehabilitation activities, continuously strengthening their health awareness and maintaining focus on disease knowledge post-intervention, which facilitates effective self-management of their conditions. It is anticipated that this increase in knowledge will positively influence patients’ attitudes towards medication, foster a scientific understanding of “active medication”, and subsequently enhance medication literacy and adherence.
A cross-sectional survey48 has confirmed that medication literacy is a crucial factor influencing medication adherence, with a significant positive correlation between the two. Specifically, the intervention notably improved participants’ medication literacy, which directly or indirectly enhanced the patients’ medication adherence. Thus, the effectiveness of the intervention can be elucidated through the IMB model.49 Our intervention significantly augmented patients’ disease knowledge reserves. Building upon this foundation, we systematically enhanced patients’ medication literacy levels through targeted guidance and scenario simulation training, alleviating the burden of medication use and ultimately improving adherence. Similarly, previous studies based on the IMB model have identified comparable intervention mechanisms. Mirzaei-Alavijeh et al50 implemented an incentive education course grounded in the IMB model for elderly patients with type 2 diabetes, confirming that this intervention could enhance medication literacy by improving medication knowledge and self-efficacy, thus leading to better adherence. Jia et al51 furthermore demonstrated that providing essential information, motivation, and behavioral skills during the intervention significantly improves patients’ medication adherence, warranting clinical promotion and application. Furthermore, considering that polypharmacy and complex medication regimens are prevalent factors contributing to poor patient adherence,52 this study suggests that introducing medication management auxiliary tools (such as smart reminder devices and dose-separated medicine boxes) can simplify the medication process, aiding patients in understanding and executing their treatment plans, thereby continuously enhancing medication adherence.
Blood pressure serves as a critical indicator for evaluating the health status of stroke patients, with its management directly impacting medication adherence53 and treatment efficacy.54 Consequently, standardized blood pressure monitoring and management can effectively prevent both the occurrence and recurrence of strokes, thereby enhancing patient prognosis. In our study, we observed that motivational information delivered through phone calls and brief standardized medication reminder messages can contribute to lowering blood pressure. These messages are crucial for stroke patients, as they facilitate positive changes in blood pressure when patients are adequately informed and motivated. However, it is noteworthy that, despite the observed reductions in both systolic and diastolic blood pressures among participants, the systolic blood pressure of some patients remained above the normal range. Relevant literature indicates that lifestyle management is a vital component of hypertension treatment.55 Although medication literacy intervention can help patients recognize the detrimental effects of unhealthy lifestyles, the absence of comprehensive guidance and interventions addressing lifestyle factors - such as diet, exercise, and psychological well - being - poses challenges for achieving significant changes in short term, thereby impacting blood pressure control.
Dyslipidemia is a significant risk factor for stroke. Research indicates that for every 1 mmol/L increase in total cholesterol, the risk of stroke rises by 25%.56 Unfortunately, during the follow-up period, although lipid levels decreased, no statistically significant differences were observed. This outcome may be attributed to the complexities involved in lipid management. The management of lipids in stroke patients relies not only on pharmacological treatment but is also influenced by various factors.57 While medication literacy interventions can significantly enhance patients’ self-management of medications, the control of lipid levels is closely related to patients’ dietary, physical activity, genetic predispositions, and comorbidity. Consequently, it is challenging to comprehensively address all key aspects of lipid management through medication literacy interventions alone.
Readmission is one of the most frequently used indices of quality of care. Hospital readmissions, particularly unplanned ones, are regarded as unpredictable outcomes of care.58 The readmission rate for stroke patients is notably elevated compared to restriction diseases,59 with polypharmacy being a common reason for readmission among elderly stroke patients. A retrospective study60 found that elderly patients aged 65 and older who were discharged experienced readmissions due to medication-related issues within 30 days post-discharge, accounting for approximately 20% to 40% of total readmissions during this period. Therefore, effective pre-discharge care planning and post-discharge medication management are essential to reduce the readmission rate among stroke patients. Unfortunately, while this study can enhance patients’ medication self-management capacity and effectively reduce complications such as infections and thrombosis resulting from medication errors or poor control of risk factors, it fails to significantly decrease the unplanned readmission rate among stroke patients. This restriction is attributed to the complex health status of patients, the diversity of readmission incentives, and the integration challenges within the medical system. Future efforts should focus on developing a comprehensive intervention model that includes “medication literacy, psychological support, rehabilitation nursing, and multidisciplinary follow-up”, as well as optimizing the allocation of medical resources to more comprehensively reduce the risk of readmission.
This study identified a differential dropout rate at the T3 stage, with the control group exhibiting a dropout rate of 23.4%, compared to 15.9% in the intervention group. This dropout pattern may either attenuate or exaggerate the intervention effect, potentially leading to a deviation of the research conclusions from the actual situation.61 To assess the stability of the research findings, we conducted a sensitivity analysis. Initially, we employed ITT analysis as the primary method, adhering strictly to the principle of including all randomly assigned subjects in the analysis according to their original groups. This approach objectively reflects the intervention effect under varying dropout rates within the actual research context.62 Subsequently, the PP analysis conducted as part of the sensitivity analysis corroborated the findings of the ITT analysis, with both approaches yielding consistent conclusions. Importantly, there were no significant differences in key baseline characteristics between the dropouts and the completers, suggesting that the dropout situation was not influenced by the observed confounding factors. In conclusion, despite the observed differential dropout phenomenon, the consistency of the sensitivity analysis results and the verification of the causes of dropout indicate that the main conclusions of this study are robust.
It is noteworthy that, despite the implementation of certain prevention and control measures in this study, potential risks of cross-contamination may still persist. Specifically, the direction of contamination is primarily evidenced by the control group receiving partial intervention-related information, which may diminish the observed outcome differences between the intervention and control groups, thereby leading to an underestimation of the true efficacy of the intervention measures. Nonetheless, an analysis of the actual prevention and control measures suggests that the extent of such impact is limited. On one hand, the control group did not engage in core intervention sessions, such as group guidance, role-playing, and WeChat group notifications, and could only access fragmented information, which hampers the achievement of a comprehensive intervention effect. On the other hand, the ITT analysis incorporated all randomized patients; thus, even if minor cross-contamination occurred, its influence on the overall results has been partially alleviated through the ITT principle. Furthermore, the consistency between the results of the PP analysis, conducted as a sensitivity analysis, and the ITT analysis further corroborates the robustness of the conclusions, indicating that potential cross-contamination did not systematically affect the core findings. Future multi-center studies could enhance prevention and control strategies by implementing grouping based on different hospitals and designating dedicated medical teams to assume full responsibility throughout the study, thereby reducing cross-contamination risks linked to shared resources and more accurately validating the efficacy of the intervention measures.63
Limitations
Despite its strengths, this study has several limitations. Firstly, due to resource constraints, the research was conducted at a university-affiliated hospital in Wuxi City, which may limit the generalizability of the results. Conducting multi-center studies would enhance the robustness of our findings. Secondly, the 12-week follow-up period is relatively short; we believe that an endpoint exceeding six months would provide more conclusive evidence regarding the long-term benefits of the multidisciplinary drug literacy intervention based on the IMB model. Thirdly, the study’s participant population did not include patients with cognitive dysfunction or severe physical disabilities, meaning the applicability of the intervention plan to these groups remains unverified. Future research should consider designing stratified intervention strategies and formulating targeted measures based on the varying functional conditions of patients, such as implementing a family collaborative care model. Finally, the high dropout rate, particularly in the control group, may have compromised the study’s ability to detect differences between the groups.
Conclusion
This study has demonstrated that a medication literacy intervention based on the IMB model can effectively enhance the medication self-management capacity of stroke patients. Furthermore, these interventions positively influence the knowledge levels, medication literacy, and adherence of stroke patients, as well as their health conditions, including blood pressure. However, our research found no significant beneficial effects on blood lipid levels or unplanned readmission rates. Future research should focus on developing a comprehensive intervention model that integrates medication literacy, psychological support, rehabilitation care, and multidisciplinary follow-up. Additionally, long-term, multi-center studies are necessary to validate our findings and provide robust evidence regarding the effectiveness of IMB model-based medication literacy interventions for stroke patients supported by a multidisciplinary team.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and received approval from the Research Ethics Committee of the Affiliated Hospital of Jiangnan University (No.LS2023063). Additionally, it was registered with the Chinese Clinical Trial Registry (ChiCTR2400084673).
Data Sharing Statement
Upon reasonable request, communicating the correspondence author (Yibo Wu) may present data in favor of the results of this research.
Acknowledgments
The authors thank all participants in this study for their support.
Funding
This work was supported by grants from the Wuxi Taihu Lake Talent Plan Leading Talents in Medical and Health Professions (Mading academician, 4532001THMD), General Project of Wuxi Health Commission (M202408, M202418).
Disclosure
All of the authors had no any personal, financial, commercial, or academic conflicts of interest separately for this work.
References
1. Zeng S, Li L, Li J, He X. Two-stage DRG grouping of cerebral infarction based on comorbidity and complications classification. Front Public Health. 2025;13:1513744. doi:10.3389/fpubh.2025.1513744
2. Feigin VL, Brainin M, Norrving B, et al. World stroke organization (WSO): Global stroke fact sheet 2022. Int J Stroke. 2022;17(1):18–29. doi:10.1177/17474930211065917
3. Barow E, Probst AC, Pinnschmidt H, et al. Effect of comorbidity burden and polypharmacy on poor functional outcome in acute ischemic stroke. Clin Neuroradiol. 2023;33(1):147–154. doi:10.1007/s00062-022-01193-8
4. Matsumoto A, Yoshimura Y, Nagano F, et al. Polypharmacy and potentially inappropriate medications in stroke rehabilitation: prevalence and association with outcomes. Int J Clin Pharm. 2022;44(3):749–761. doi:10.1007/s11096-022-01416-5
5. George J, Phun YT, Bailey MJ, Kong DC, Stewart K. Development and validation of the medication regimen complexity index. Ann Pharmacother. 2004;38(9):1369–1376. doi:10.1345/aph.1D479
6. Tabi K, Randhawa AS, Choi F, et al. Mobile apps for medication management: review and analysis. JMIR mHealth uHealth. 2019;7(9):e13608. doi:10.2196/13608
7. Mafruhah OR, Huang YM, Lin HW. Impacts of medication non-adherence to major modifiable stroke-related diseases on stroke prevention and mortality: a meta-analysis. J Neurol. 2023;270(5):2504–2516. doi:10.1007/s00415-023-11601-9
8. Li Y, Zhang S, Song J, Tuo M, Sun C, Yang F. Effects of self-management intervention programs based on the health belief model and planned behavior theory on self-management behavior and quality of life in middle-aged stroke patients. Evid Based Complement Alternat Med. 2021;2021:8911143. doi:10.1155/2021/8911143
9. Suzuki R, Uchiya T, Nakamura A, et al. Analysis of factors contributing to medication errors during self-management of medication in the rehabilitation ward: a case control study. BMC Health Serv Res. 2022;22(1):292. doi:10.1186/s12913-022-07679-y
10. Erickson JM, Kamke-Jordan A, Lancaster IJ, et al. Medication self-management behaviors of adolescents and young adults with cancer. Support Care Cancer. 2023;31(7):
11. Menkin JA, McCreath HE, Song SY, et al. “Worth the Walk”: culturally tailored stroke risk factor reduction intervention in community senior centers. J Am Heart Assoc. 2019;8(6):e011088. doi:10.1161/jaha.118.011088
12. Jang DE, Zuñiga JA. Factors associated with medication persistence among ischemic stroke patients: a systematic review. Neurol Res. 2020;42(7):537–546. doi:10.1080/01616412.2020.1754640
13. Huang J, Ding SL, Xiong SY, Liu ZP. Medication adherence and associated factors in patients with type 2 diabetes: a structural equation model. Front Public Health. 2021;9:
14. Wang WN, Luan WY, Zhang ZX, Mei YX. Association between medication literacy and medication adherence and the mediating effect of self-efficacy in older people with multimorbidity. BMC Geriatr. 2023;23(1):
15. Gentizon J, Bovet E, Rapp E, Mabire C. Medication literacy in hospitalized older adults: concept development. Health Lit Res Pract. 2022;6(2):e70–e83. doi:10.3928/24748307-20220309-02
16. Pouliot A, Vaillancourt R, Stacey D, Suter P. Defining and identifying concepts of medication literacy: an international perspective. Res Social Adm Pharm. 2018;14(9):797–804. doi:10.1016/j.sapharm.2017.11.005
17. Smith S, Parkinson J, Caitens T, Sanders A, Murphy L, Hamilton K. Promoting adherence to stroke secondary prevention behaviours by imparting behaviour change skills: protocol for a single-arm pilot trial of living well after stroke. BMJ Open. 2023;13(1):e068003. doi:10.1136/bmjopen-2022-068003
18. Solmaz T, Altay B. The role of training and medication reminder wristwatch in adherence to treatment in geriatric patients diagnosed with hypertension: a randomized controlled trial. Geriatr Gerontol Int. 2024;24(11):1189–1195. doi:10.1111/ggi.14999
19. Jing W, Liting W, Youhong H, Yanling H, Qiuqiong Q, Yuemei X. Application research on health education prescription for empowering authorization combined with drug literacy in patients with myocardial infarction. J Nurses Training. 2025;40(01):34–38. doi:10.16821/j.cnki.hsjx.2025.01.007
20. Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychol Bull. 1992;111(3):455–474. doi:10.1037/0033-2909.111.3.455
21. Kuang J, Li Y, Deng S, Su J, Gong S, Wang Y. Effect of information-motivation-behavior skills on adherence of continuous positive airway pressure therapy in patients with obstructive sleep apnea hypopnea syndrome. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2022;47(4):479–487. doi:10.11817/j.issn.1672-7347.2022.210590
22. Li M, Zhu H. Application of intervention of information motivation behavior skill (IMB) model in the cardiac rehabilitation of patients with coronary heart disease. Pak J Med Sci. 2022;38(6):1627–1632. doi:10.12669/pjms.38.6.5721
23. Yao X, Zhang L, Du J, Gao L. Effect of information-motivation-behavioral model based on protection motivation theory on the psychological resilience and quality of life of patients with type 2 DM. Psychiatr Q. 2021;92(1):49–62. doi:10.1007/s11126-020-09783-w
24. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. doi:10.1016/0895-4356(89)90065-6
25. Appalasamy JR, Tha KK, Quek KF, Ramaiah SS, Joseph JP, Md Zain AZ. The effectiveness of culturally tailored video narratives on medication understanding and use self-efficacy among stroke patients: a randomized controlled trial study protocol. Medicine. 2018;97(22):e10876. doi:10.1097/md.0000000000010876
26. Manias E, Beanland CJ, Riley RG, Hutchinson AM. Development and validation of the self-administration of medication tool. Ann Pharmacother. 2006;40(6):1064–1073. doi:10.1345/aph.1G677
27. Lin B, Mei Y, Ma F, Zhang Z, Chen Q, Wang S. Testing the validity and reliability of the self-administration of Medication (SAM) instrument in Chinese chronic disease patients: a cross-cultural adaptation. Int J Nurs Pract. 2018;24(2):e12625. doi:10.1111/ijn.12625
28. Yao Q. The Effects of Self-Management Intervention on KAP and Subjective Well-Being of Convalescent Cerebral Apoplexy Patients. Southeast University; 2016.
29. Sauceda JA, Loya AM, Sias JJ, Taylor T, Wiebe JS, Rivera JO. Medication literacy in Spanish and English: psychometric evaluation of a new assessment tool. J Am Pharm Assoc. 2012;52(6):e231–40. doi:10.1331/JAPhA.2012.11264
30. Feng Z, Zhuqing Z, Siqing D, Aijing L, Zina L. Modification and evaluation of assessment of medication literacy. J Central South Univ. 2016;41(11):1226–1231.
31. Wang L, Fang C, Nie M, Zhu L, Liu S, Li H. Mediating role of inner strength in the relationship between medication literacy and medication adherence among kidney transplant patients. Zhong Nan Da Xue Xue Bao Yi Xue Ban. 2024;49(6):961–971. doi:10.11817/j.issn.1672-7347.2024.240215
32. Qu J, Zhou T, Xue M, Sun H, Shen Y, Liu Y. Relationship between medication literacy and frailty in elderly inpatients with coronary heart disease: a cross-sectional study in China. Front Pharmacol. 2021;12:691983. doi:10.3389/fphar.2021.691983
33. Mahler C, Hermann K, Horne R, et al. Assessing reported adherence to pharmacological treatment recommendations. Translation and evaluation of the medication adherence report scale (Mars) in Germany. J Eval Clin Pract. 2010;16(3):574–579. doi:10.1111/j.1365-2753.2009.01169.x
34. T Q, Y L. Reliability and validity of the Chinese version of medication adherence report scale for asthma. Chin J Nurs. 2014;49(5):621–624.
35. Mishra P, Pandey CM, Singh U, Gupta A, Sahu C, Keshri A. Descriptive statistics and normality tests for statistical data. Ann Card Anaesth. 2019;22(1):67–72. doi:10.4103/aca.ACA_157_18
36. Constantine RJ, Andel R, Tandon R. Trends in adult antipsychotic polypharmacy: progress and challenges in Florida’s Medicaid program. Community Ment Health J. 2010;46(6):523–530. doi:10.1007/s10597-009-9288-2
37. Marks D, Bisset L, Comans T, et al. Increasing capacity for the treatment of common musculoskeletal problems: a non-inferiority RCT and economic analysis of corticosteroid injection for shoulder pain comparing a Physiotherapist and Orthopaedic surgeon. PLoS One. 2016;11(9):e0162679. doi:10.1371/journal.pone.0162679
38. Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. 2013;4:863. doi:10.3389/fpsyg.2013.00863
39. Ranganathan P, Pramesh CS, Aggarwal R. Common pitfalls in statistical analysis: intention-to-treat versus per-protocol analysis. Perspect Clin Res. 2016;7(3):144–146. doi:10.4103/2229-3485.184823
40. Thabane L, Mbuagbaw L, Zhang S, et al. A tutorial on sensitivity analyses in clinical trials: the what, why, when and how. BMC Med Res Methodol. 2013;13:92. doi:10.1186/1471-2288-13-92
41. Van der Linden L, Hias J, Walgraeve K, Flamaing J, Tournoy J, Spriet I. Clinical pharmacy services in older inpatients: an evidence-based review. Drugs Aging. 2020;37(3):161–174. doi:10.1007/s40266-019-00733-1
42. Sumida CA, Van Etten EJ, Lopez FV, et al. Medication management capacity and its neurocognitive correlates in Huntington’s disease. Arch Clin Neuropsychol. 2019;34(7):1121–1126. doi:10.1093/arclin/acy093
43. Milosevich E, Kusec A, Pendlebury ST, Demeyere N. Domain-specific cognitive impairments, mood and quality of life 6 months after stroke. Disabil Rehabil. 2025;47(2):435–444. doi:10.1080/09638288.2024.2340121
44. Kose E, Endo H, Hori H, et al. Pharmacist medication instructions are associated with continued medication self-management in older adults: a retrospective observational study. J Pharm Health Care Sci. 2021;7(1):11. doi:10.1186/s40780-021-00194-y
45. Ernawati I, Munif Yasin N, Setyopranoto I, Ikawati Z. The role of pharmacists’ interventions in increasing medication adherence of patients with Epilepsy: a scoping review. J Prev Med Public Health. 2024;57(3):212–222. doi:10.3961/jpmph.23.592
46. Widjaja KK, Chulavatnatol S, Suansanae T, et al. Knowledge of stroke and medication adherence among patients with recurrent stroke or transient ischemic attack in Indonesia: a multi-center, cross-sectional study. Int J Clin Pharm. 2021;43(3):666–672. doi:10.1007/s11096-020-01178-y
47. Shen D, Huang W, Wei S, Zhu Y, Shi B. The impact of Teach-back method on preoperative anxiety and surgical cooperation in elderly patients undergoing outpatient ophthalmology surgery: a randomized clinical trial. Medicine. 2023;102(8):e32931. doi:10.1097/md.0000000000032931
48. Coskun S, Bagcivan G. Associated factors with treatment adherence of patients diagnosed with chronic disease: relationship with health literacy. Appl Nurs Res. 2021;57:151368. doi:10.1016/j.apnr.2020.151368
49. Yang C, Hui Z, Zeng D, et al. A community-based nurse-led medication self-management intervention in the improvement of medication adherence in older patients with multimorbidity: protocol for a randomised controlled trial. BMC Geriatr. 2021;21(1):152. doi:10.1186/s12877-021-02097-x
50. Mirzaei-Alavijeh M, Yarmoradi S, Khashij S, Jalilian F. Application of the information-motivation-behavioral skills model to improve medication adherence among older adults with type 2 diabetes: findings from a quasi-experimental study in Kermanshah, Iran. BMC Geriatr. 2025;25(1):328. doi:10.1186/s12877-025-06000-w
51. Jia X, Zhou S, Luo D, Zhao X, Zhou Y, Cui YM. Effect of pharmacist-led interventions on medication adherence and inhalation technique in adult patients with asthma or COPD: a systematic review and meta-analysis. J Clin Pharm Ther. 2020;45(5):904–917. doi:10.1111/jcpt.13126
52. Pevnick JM, Anderson LJ, Chirumamilla S, et al. Tools and tactics for postdischarge medication management interventions. Am J Health Syst Pharm. 2021;78(7):619–632. doi:10.1093/ajhp/zxab010
53. Gwadry-Sridhar FH, Manias E, Lal L, et al. Impact of interventions on medication adherence and blood pressure control in patients with essential hypertension: a systematic review by the ISPOR medication adherence and persistence special interest group. Value Health. 2013;16(5):863–871. doi:10.1016/j.jval.2013.03.1631
54. Shi M, Liu Y, Wang S, et al. Blood pressure control and antihypertensive medication use after discharge and prognosis of ischemic stroke. J Hypertens. 2023;41(11):1730–1737. doi:10.1097/hjh.0000000000003523
55. de Boer IH, Bangalore S, Benetos A, et al. Diabetes and hypertension: a position statement by the American Diabetes Association. Diabetes Care. 2017;40(9):1273–1284. doi:10.2337/dci17-0026
56. Zhao Y, Wang Z, Ji R, Zhang Y, Wang Y, Yu K. Relationship between carotid atherosclerosis and lipoprotein (a) in patients with acute ischemic stroke. Front Neurol. 2024;15:1383771. doi:10.3389/fneur.2024.1383771
57. Xu J, Li ZX. Scientific statement on the long-term lipid management in patients with ischemic stroke and transient ischemic attack in China. Chin J Stroke. 2024;19(04):440–451.
58. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. doi:10.1056/NEJMsa0803563
59. Lee SA, Park EC, Shin J, Ju YJ, Choi Y, Lee HY. Patient and hospital factors associated with 30-day unplanned readmission in patients with stroke. J Investig Med. 2019;67(1):52–58. doi:10.1136/jim-2018-000748
60. Murad H, Basheikh M, Zayed M, Albeladi R, Alsayed Y. The association between medication non-adherence and early and late readmission rates for patients with acute coronary syndrome. Int J Gen Med. 2022;15:6791–6799. doi:10.2147/ijgm.S376926
61. Kristman V, Manno M, Côté P. Loss to follow-up in cohort studies: how much is too much? Eur J Epidemiol. 2004;19(8):751–760. doi:10.1023/b:ejep.0000036568.02655.f8
62. Gupta SK. Intention-to-treat concept: a review. Perspect Clin Res. 2011;2(3):109–112. doi:10.4103/2229-3485.83221
63. Bennasar-Veny M, Colom-Rosselló M, Abbate M, et al. Impact of an adapted diabetes prevention program in a spanish primary care setting: protocol for a type II hybrid effectiveness-implementation cluster-randomized trial (ALADIM). Implement Sci. 2025;20(1):27. doi:10.1186/s13012-025-01438-3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.