")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Impact of the Industrialization of Older Adult Care Services on Older Individuals’ Physical and Mental Health: Evidence from China’s Quasi-Natural Experiment
Authors He Y, Ouyang W, Li Z, Wei B
Received 19 June 2023
Accepted for publication 21 September 2023
Published 16 October 2023 Volume 2023:16 Pages 3017—3033
DOI https://doi.org/10.2147/JMDH.S426710
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yang He,1 Wenjing Ouyang,2 Zhenzhen Li,3 Baojian Wei4
1School of Business, Xiangtan University, Xiangtan, 411105, People’s Republic of China; 2Department of Business School, Hunan Normal University, Changsha, 410081, People’s Republic of China; 3Taylor’s University, Subang Jaya, 47500, Malaysia; 4School of Nursing, Shandong First Medical University & Shandong Academy of Medical Sciences, Taian, 271021, People’s Republic of China
Correspondence: Baojian Wei, Changcheng Road, Beijipo Street, Daiyue District, Taian City, People’s Republic of China, Tel +86-15564848382, Email [email protected]
Purpose: Given the increasing longevity of the population, the consolidation of familial structures, and the scarcity of economic resources required to sustain an aging society, the Chinese government faces a complex and urgent challenge in effectively addressing the growing needs of older adults and establishing a long-term care services system that is both sustainable and equitable.
Patients and Methods: This study harnesses the comprehensive CLHLS data from 2011 to 2018 and utilizes the “Pilot Industrialization of Old-Age Service in a Market-Oriented Way” policy as a quasi-natural experiment. Employing the Difference-in-Differences (DID) method, our study aims to evaluate the impact of industrializing older adult care services on the physical and mental health outcomes of older adults in China.
Results: The findings strongly indicate that the government’s adoption of a market-driven fiscal approach within its policies, aimed at attracting social capital and fostering the industrialization of older adult care services, positively influences the physical and mental well-being of the aged population. Furthermore, through heterogeneity analysis, it becomes evident that the health promotion effect is particularly pronounced among older individuals living without a spouse, lacking family care from children or grandchildren, or residing in financially underdeveloped regions.
Conclusion: In summary, these results underscore the potential efficacy of employing financial policy instruments to facilitate the industrialization of older adult care services, thereby advancing the promotion of a society characterized by healthy aging and ensuring equitable health outcomes for older people.
Keywords: industrialization, older adult care, market-driven fiscal policy, physical and mental health, healthy aging, difference-in-differences, Chinese longitudinal healthy longevity survey
Introduction
Globally, the number and proportion of older adults are rapidly expanding because of increased life expectancies and declining fertility rates. Projections indicate that the demographic aged 65 and above will witness an almost twofold surge, surging from 727 million in 2020 to over 1.5 billion in 2050, concurrent with a rise in the proportion of older adults from 9.3% to 16.0% over the same duration.1 Consequently, facilitating suitable and enduring care for older adults has emerged as a paramount concern in public policy and research across the globe.2 The older adult care service industry is a collective term for providing physiological and psychological services for older people. It was first proposed in 2006 when the State Council initially clarified the concept of the older adult care service industry. It is the earliest official document in China to standardize the description of the older adult care service industry.3 The Opinion points out that the older adult care service industry provides regular care and services for older people, meeting their unique living needs. It includes daily care, routine tasks, physical examination, medical assistance, spiritual comfort, psychological care, rehabilitation treatment, and other services. From providing essential services to building an industry supported by traditional home-based, community, and specialized older adult care in new institutions, a socialized service system has been constructed to meet the diversified needs of the older adult population based on targeted care services. China, a nation witnessing a rapid aging process,4 confronts even greater obstacles in addressing the burgeoning demand for older adult care services than other countries.5 However, China faces several hurdles when it comes to addressing these difficulties.
On the one hand, economic development and the implementation of the one-child policy (which was terminated in 2016) have resulted in an upsurge in female employment rates,6 heightened population mobility,7 and an increased prevalence of single-child families.8 These factors have shifted toward nuclear family structures, weakening the traditional family care system. Concurrently, concerns regarding the physical, mental, and economic strain experienced by family caregivers have emerged, exacerbating the burden on the family care system.9,10 As a result, the traditional family care system has been substantially undermined.11 On the other hand, given China’s substantial older adult population and the embryonic stage of its older adult care services, relying solely on government-operated nursing homes and care institutions is not a sustainable recourse.12,13
To fulfill the exigencies of China’s aged population and ensure the enduring viability of older adult care services within the confines of an imperfect welfare structure, insights from developed nations reveal that market engagement in the domain of older adult care service provision is hailed as the most productive course of action.14,15 Nevertheless, the extant body of literature on market participation in the older adult care service industry reflects notable divergence due to conflicting interests between enterprises and the government. Enterprises prioritize maximizing economic gains, whereas the government enhances social welfare.16 Proponents argue that profit-driven private enterprises possess a stronger impetus to allocate resources judiciously and adapt to the varied and fluid needs of the older adult populace.17 They posit that private enterprises display greater adaptability and can furnish cost-effective models of care compared to purely public sectors. However, critics raise apprehensions that private enterprises may prioritize profit-driven objectives at the expense of upholding high standards of older adult care services, potentially leading to a regression in care quality as profit-centric considerations take precedence.18
Furthermore, China’s older adult care service industry presently finds itself in uncertainty and exploration.15 While there exists a burgeoning demand among older adults for these services, an array of economic, social, and cultural factors influence the actual demand for such provisions. Consequently, significant uncertainties enshroud the authentic demand for care services,19,20 amplifying investment risks and financial pressures for prospective investors, compelling many to adopt a cautious stance and defer investment within the older adult care service industry.21 The available literature posits that policy support is pivotal in establishing a sustainable care system by striking a harmonious equilibrium between private and public interests.22,23 Furthermore, policy support is indispensable in tackling enterprises’ financial constraints and nurturing the growth of the older adult care service industry.12
To alleviate the initial dearth of funding encountered by enterprises operating within the older adult care service industry, government support policies typically adopt two approaches: direct subsidies and government-led investment funds.24,25 Direct subsidies extended by governmental entities primarily comprise construction and operational subsidies.12,16,26 Conversely, government-guided investment funds, bolstered by central government backing, strive to allure investments from local authorities, financial institutions, and social capital for ventures fraught with risk, thereby nurturing the growth of burgeoning sectors.27 These investment funds furnish monetary assistance to nascent enterprises and mitigate financing risks that invariably arise during the funding process.28 In contrast to direct subsidies, government-guided investment funds harbor the extraordinary capacity to serve as both an “effective government” and an “effective market”.29 They adopt a market-oriented approach that optimizes the utilization of fiscal resources, engendering a multiplier effect on capital.30 By harnessing public and private resources to the fullest extent possible, they hold the potential to enhance the accessibility of older adult care services.
Moreover, government-guided investment funds exhibit substantial promise in streamlining and elevating the overall structure of the older adult care service industry.31 By selectively identifying enterprises imbued with considerable potential and substantial benefits, these funds can boost the quality and efficiency of older adult care services.32 However, extant studies focusing on the promotion of the older adult care service industry through governmental policies have predominantly addressed providing direct subsidies,16,21,33 Limited attention has been paid to exploring government-guided investment funds. Further research is warranted to investigate government-guided investment funds’ effectiveness and latent advantages within the older adult care service industry.
On August 22, 2014, a collaborative endeavor between the Ministry of Finance and the Ministry of Commerce led to the announcement of the “Notification on Carrying out Pilot Industrialization of Old-Age Service in a Market-Oriented Way”. This proclamation allocated a sum of 2.4 billion Chinese Yuan in guidance funds from the central government, rendering abundant support to the older adult care service industry, mainly facilitating the comprehensive progress in home-based, community-based systems, and life services industries combining medical and nursing care. These funds were distributed equally among the eight provinces and regions, and the designated pilot areas were explicitly directed to promote the industrialization of older adult care services based on market-oriented operation principles. Furthermore, each province was entrusted with establishing an industry fund dedicated to older adult care services, with a matching fund ratio of no less than 1:4. Thus, each province will invest 1.2 billion yuan.34 China has the world’s largest aging population. Therefore, promoting healthy aging initiatives to tackle the challenges associated with an aging society is of critical importance.35,36 By providing guidance funds and encouraging the establishment of industry funds, the government aims to stimulate investment and innovation in the older adult care service industry. Over a year following the initiation of the pilot policy, Hunan province alone has attracted substantial investments totaling nearly 8 billion yuan, catering to the welfare of over 1 million older individuals.37 Therefore, whether these efforts will achieve China’s goal of establishing a sustainable and high-quality older adult care services system and enhancing older individuals’ health and well-being is worth exploring.
This study contributes significantly to an extensive body of literature. First, it addresses issues raised in the ongoing scholarly discourse surrounding the efficacy of market participation in older adult care services. This study applies the “Pilot Industrialization of Old-Age Service in a Market-Oriented Way” policy as a quasi-natural experiment and employs the DID (Difference-in-Differences) methodology. Doing so avoids the endogeneity that often complicates the identification of causal effect between older adult care services and the health outcomes of this cohort. The findings of this study suggest that market participation in the older adult care service industry can significantly improve their physical and mental health. Secondly, research shedding light on the efficacy of government policy tools in promoting sustainable development of the older adult care services sector from an unexamined perspective outside the scope of traditional subsidies and tax incentives is limited. Through careful examination of financial policy, this study will show that the establishment of a market-oriented government guidance fund created in the interest of the older adult care service industry can significantly impact China’s goal of fostering a society that facilitates holistic, healthy aging. This novel perspective offers valuable insights. It clarifies how financial policies can catalyze and spur further development in the older adult care industry. Finally, this study explores the heterogeneous impact of market-driven financial policies supporting the growth of the older adult care service industry on physical and mental health in diverse populations and regions. The analytical framework employed in this study carefully considers several individual characteristics such as age, living arrangements, and family caregiving while shedding light on the regional differences that arise from various factors, including provincial financial subsidies and the pervasive urban-rural dichotomy. Thus, this study delves deeply into the complex impact of policy interventions on older adult health outcomes.
In summary, the insights provided by this study will contribute substantially to the existing literature. They illuminate the positive effects of market participation in older adult care services. Furthermore, they emphasize the significance of financial policy tools beyond subsidies, revealing a wide range of possibilities. Finally, by considering population and regional diversity, this study clarifies the complex factors that impact older adult health. Policymakers and stakeholders who seek to improve care for older adults will benefit substantially from the information it provides.
Materials and Methods
Data Resources
Individual-level data were sourced from the Chinese Longitudinal Healthy Longevity Survey (CLHLS), which was administered in 2011, 2014, and 2018. The CLHLS utilized proportional probability sampling, gathering an array of multidimensional information, including demographic characteristics, socioeconomic conditions, lifestyle factors, family structure, and physical and psychological health.38 The CLHLS draws data from 800 randomly selected counties and cities across 23 provinces, representing approximately 85% of China’s vast populace.
For this study, we obtained a large sample (14,625 participants) aged 60 and above with their presence during at least two interviews.
We procured appropriate data from the China Statistical Yearbook. The data were gathered at the provincial level and included the per capita GDP, the exact number of hospital beds and doctors per 1000 individuals, cataloged for each province.39
Variable Description
Dependent Variable
Evaluating the health status of older adult men and women encompassed two dimensions of self-rated health (SRH) and the domain of psychological well-being. The SRH was quantified using a five-point scale for the question: “How do you rate your health at present?” Those participants who responded with a good or very good were considered to have good physical health, which was scored as 1. Other options were scored 0, representing the state of having poor physical health.40
Within psychological well-being, we examined loneliness, reflecting the older adult’s tendency toward depression and suicidal ideation.41 Participants were asked: “Do you often experience loneliness/bouts of loneliness?”42 Responses of always or often were scored 1. Other options were scored 0.43
Independent Variables
DID was identified as the key independent variable examined in this study, which represented whether the survey participants were located in an area where the policy “Pilot Industrialization of Old-Age Service in a Market-Oriented Way” had been implemented at the time of their interview. The DID variable consisted of two components: “treat” (treatment) and “post” (post-implementation). The “treat” component indicated whether the respondents were located in any of the eight pilot provinces, namely Hunan, Inner Mongolia, Jilin, Jiangxi, Shandong, Anhui, Hubei, and Gansu. These provinces were selected as the treatment group where the policy was implemented, and they served as a basis for comparison. The “post” component indicated whether respondents were interviewed after the policy was implemented, specifically after the year 2015.34 This interaction item represented the change in the treatment effect before and after the policy compared to the control group. By utilizing the Difference-in-Differences (DID) approach, the study aimed to capture the causal effect of the policy on the health outcomes of the participants while controlling for other factors that could potentially influence the results.
Control Variables
Taking into account relevant studies, this study controlled for various demographic and socioeconomic covariates associated with individual health.40,44 The demographic characteristics included the following variables:
Age: A continuous variable representing the age of the participant.
Sex: Categorized as 1 for male and 0 for female.
Marital status: Categorized as 1 for married and living with a spouse, and 0 for separated/divorced/widowed/never married.
Education level: Categorized as 1 for educated and 0 for illiterate.
Living arrangement: Categorized as 1 for living with family members other than the spouse and 0 otherwise.
Number of surviving children: A continuous variable indicating the number of living children the participant has.
Chronic diseases: Assessed based on 24 prevalent diseases among older adults, such as heart disease and diabetes, categorized as “1” if the participant had at least one disease and “0” otherwise.
Smoking: Categorized as 1 for current smokers and 0 otherwise.
Drinking: Categorized as 1 for current drinkers and 0 otherwise.
Regular exercise: Categorized as 1 for engaging in regular exercise and 0 otherwise.
Annual physical examination: Categorized as 1 for undergoing routine physical examination every year and 0 otherwise.
Socioeconomic status variables included:
Adequate economic income: Categorized as 1 if all sources of income were sufficient to cover daily expenses and 0 otherwise.
Economic independence: Categorized as 1 if the participant’s primary source of income is self or spouse, and 0 otherwise.
Social security: Categorized as 1 if the participant had medical and pension insurance and 0 otherwise.
Relative economic level: Categorized from 1 to 5, representing “very difficult”, “relatively difficult”, “average”, “relatively wealthy”, and “very wealthy” economic levels.
Family income: A continuous variable representing annual family income in logarithmic form.
Economic support from children: A continuous variable representing the total cash received from all children/grandchildren during the past year in logarithmic form.
Emotional support from children: Categorized as 1 if older adults primarily confided in their children/grandchildren when having concerns or thoughts, and 0 otherwise.
Residential area type: Categorized as 1 for urban/town area and 0 otherwise.
Furthermore, the study controlled for macro-level environmental variables related to individual health:
Per capita GDP (in yuan): A continuous variable representing the economic output per person, represented in logarithmic form.
Hospital bed count per 100,000 people: A continuous variable indicating the availability of hospital bed count per 100,000 individuals.
Number of doctors per 100,000 people: A continuous variable representing the number of doctors available per 100,000 individuals.
These covariates were incorporated to encapsulate the contextual elements that hold the potential to exert an influence on the outcomes of individual health. The descriptive statistics about the principal variables are elucidated in Table 1, providing a visual representation of their inherent characteristics and distributions.
 |
Table 1 Descriptive Statistics for the Primary Variables |
Econometric Model
To evaluate the inherent influence of market-oriented government financial support on the health outcomes of older adults within the realm of the developing older adult care service industry, this study employed a rigorous and sophisticated analytical approach known as the DID strategy. The model incorporated individual-fixed and year-fixed effects to ensure the utmost precision and accuracy in the estimation process. Within this design, the treatment group comprised older adults hailing from provinces where the policies for Pilot Industrialization of Old-Age Service in a Market-Oriented Way were implemented. In contrast, the control group consisted of their counterparts from other provinces. The estimation equation employed in the analysis is delineated as follows:

Variable yipt represents the health outcomes of individual i residing in province p during year t. The primary explanatory variable of interest, DIDit, is a binary variable assigned a value of 1 if older adults resided in a pilot province and participated in the 2018 survey; otherwise, it was assigned a value of 0. Xipt is the time-varying feature vector of the individual, and Wpt is the time-varying feature vector at the provincial level. Further details regarding these features are provided in Section Control variables. τt is the year fixed effect, ai is the individual fixed effect, and εict is a random error term. To capture the potential correlation among health outcomes of older adults residing in the same province, standard errors are clustered at the provincial level.
Results
Baseline Regression
The baseline regression results for equation (1) are depicted in Table 2. Columns (1) and (3) exclusively incorporate dummy variables signifying the implementation of the pilot policy, while columns (2) and (4) encompass the dynamic interplay of individual time-varying characteristics, provincial time-varying characteristics, individual-fixed effects, and year-fixed effects. Remarkably, the coefficients associated with the pivotal variable consistently demonstrate a positive inclination and attain statistical significance at the exceptional level of 1%, irrespective of the control of other factors. This compelling evidence unequivocally establishes the pivotal role of the pilot policy in elucidating the enhancement of older adults’ well-being. More specifically, the execution of the pilot policy engenders a statistically significant surge of 6.4% in the probability of older adults rating their health as good, concurrently with a noteworthy decline of 7.6% in the probability of experiencing persistent sentiments of solitude.
 |
Table 2 Baseline Regression Results |
Robustness Tests
Parallel Trend Test
The validity of the DID estimation hinges upon the fundamental assumption that the trajectories of the outcome variable in both the treatment and control groups are comparable in the absence of policy intervention, as highlighted by prior research.45 To ensure the utmost credibility and reliability of our research findings, we performed an “Event study” analysis to scrutinize the hypothesis of parallel trends.46 The outcomes of this meticulous examination are meticulously presented in Table 3. Notably, it becomes apparent that prior to the implementation of the policy, there was no statistically significant impact of the policy enforcement on the physical and psychological well-being of older adults, regardless of including other pertinent variables in the analysis. These compelling results affirm the absence of a substantial divergent trend between the provinces that pioneered the execution of the Pilot Industrialization of Old-Age Service in a Market-Oriented Way and those that abstained from its implementation, thereby substantiating the veracity of the parallel trend assumption.
 |
Table 3 Parallel Trend Hypothesis Test |
Placebo Test
A potential concern surrounding this study’s findings pertains to the attribution of the observed enhancements in the health of older individuals to fortuitous circumstances. To address this concern and reinforce the robustness of our conclusions, two placebo-testing methodologies were implemented.
First, a “counterfactual” randomized treatment cohort was established.47 Specifically, of the 32 provincial regions, eight were randomly chosen and designated as the intervention group, assuming their implementation of the Pilot Industrialization of Old-Age Service in a Market-Oriented Manner. At the same time, the remaining provinces were allocated as the control group. As the “pseudo-intervention group” selection was predicated on stochastic processes, it was anticipated that implementing policies would not substantially impact the well-being of older adults. This iterative procedure was replicated 500 times, wherein each regression iteration incorporated all control variables and fixed effects, and Figures 1 and 2 visually present the significance and distribution of the estimated coefficients. These figures reveal that the “pseudo-policy dummy variable” distributions coalesce around the value of 0, with respective mean values of 0.0003 and −0.006. Furthermore, a majority of the p-values associated with this variable surpass 0.1. These findings signify that the enhancements in the health of older individuals cannot be ascribed to fortuitous factors.
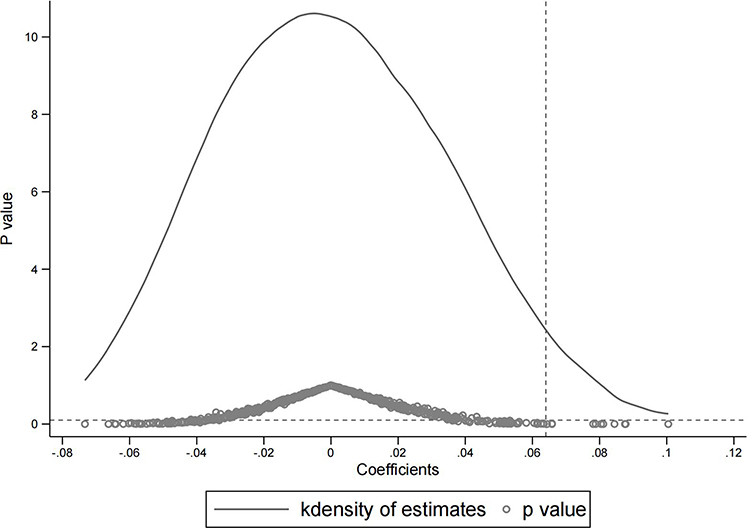 |
Figure 1 Randomized treatment group (SRH). |
 |
Figure 2 Randomized treatment group (Loneliness). |
Second, a “counterfactual” virtual enactment of a policy timeline was devised.48 Specifically, the pre-policy samples were preserved, and the policy’s commencement date was stipulated between 2011 and 2013. In this context, 2011 was regarded as the antecedent phase preceding the policy, while 2014 was designated as the subsequent phase following its implementation. Given the counterfactual nature of the policy timing, it is expected that the simulated policy dummy variables would exert no noteworthy influence on the well-being of older individuals. The scrutiny presented in Table 4 exhibits that the coefficients associated with the “pseudo-policy dummy variable” lack statistical significance concerning physical and psychological health, thereby signifying that the advancements in the health of older adults cannot be ascribed to temporal trends.
 |
Table 4 Virtual Policy Implementation Time |
The outcomes of placebo tests further bolster the resolute conclusion that the policy endeavor of Pilot Industrialization of Old-Age Service in a Market-Oriented Manner has markedly enhanced the well-being of older adults.
Other Robustness Tests
To ensure the veracity of the foundational regression findings, a trio of robustness assessments were conducted.
Firstly, a Logit model was employed for re-estimation (columns 1 and 2 in Table 5). Given that the original dependent variable in the survey constituted a ranking variable, converting it into a binary variable within the 0–1 spectrum posed the potential risk of information loss. To address this concern, a re-estimation was executed employing the original sorting variables in conjunction with the logit model. By comparing the estimation outcomes of the original ordinary least squares (OLS) model and the Logit model, it was ascertained that the direction of the estimated coefficients for the DID analysis remained unaltered. Thus, consistent estimation results were derived from both the alternative model and the benchmark regression analysis, affirming the reliability of the findings.
 |
Table 5 Other Robustness Tests |
Secondly, employing distinct datasets for re-estimation was pursued (columns 3 and 4 in Table 5). Given that the data utilized in this study comprised an unbalanced panel, the inclusion and exclusion of specific samples could potentially impact the outcomes of policy implementation. To assuage this concern, a re-estimation was conducted employing a balanced panel dataset that exclusively encompassed older adults who were interviewed consistently over three successive periods. The outcomes revealed that even after accounting for potential bias stemming from sample selection, the estimated coefficients of policy implementation remained consistently positive, exhibiting statistical significance at the noteworthy level of 1%. This validation affirms the robustness of the original findings.
Thirdly, the inclusion of combined fixed effects encompassing region and year in the foundational regression was pursued (columns 5 and 6 in Table 5). Recognizing the potential influence of latent regional factors that fluctuate over time on the efficacy of the policy, a re-estimation was undertaken to employ a comprehensive fixed-effects approach that incorporated variations at both the regional level (Eastern, Middle, and Western) and the yearly level. The outcomes revealed a persistent and significant positive association between policy implementation and older individuals’ improved physical and mental well-being, even after incorporating joint fixed effects accounting for region and year. This accentuates the invaluable role played by the Pilot Industrialization of Old-Age Service in a Market-Oriented Manner in fostering the health of older adults.
These robustness tests unequivocally affirm the dependability and consistency of the foundational regression results, fortifying the body of evidence supporting the conclusion that the implementation of the pilot policy has exerted a pivotal influence in advancing the health of older individuals.
Heterogeneity Analysis
Individual Characteristics
This study delves into the distinct ramifications of individual characteristics on the health of older adults from three perspectives, as explicated in Table 6, which presents the precise findings of the tests.
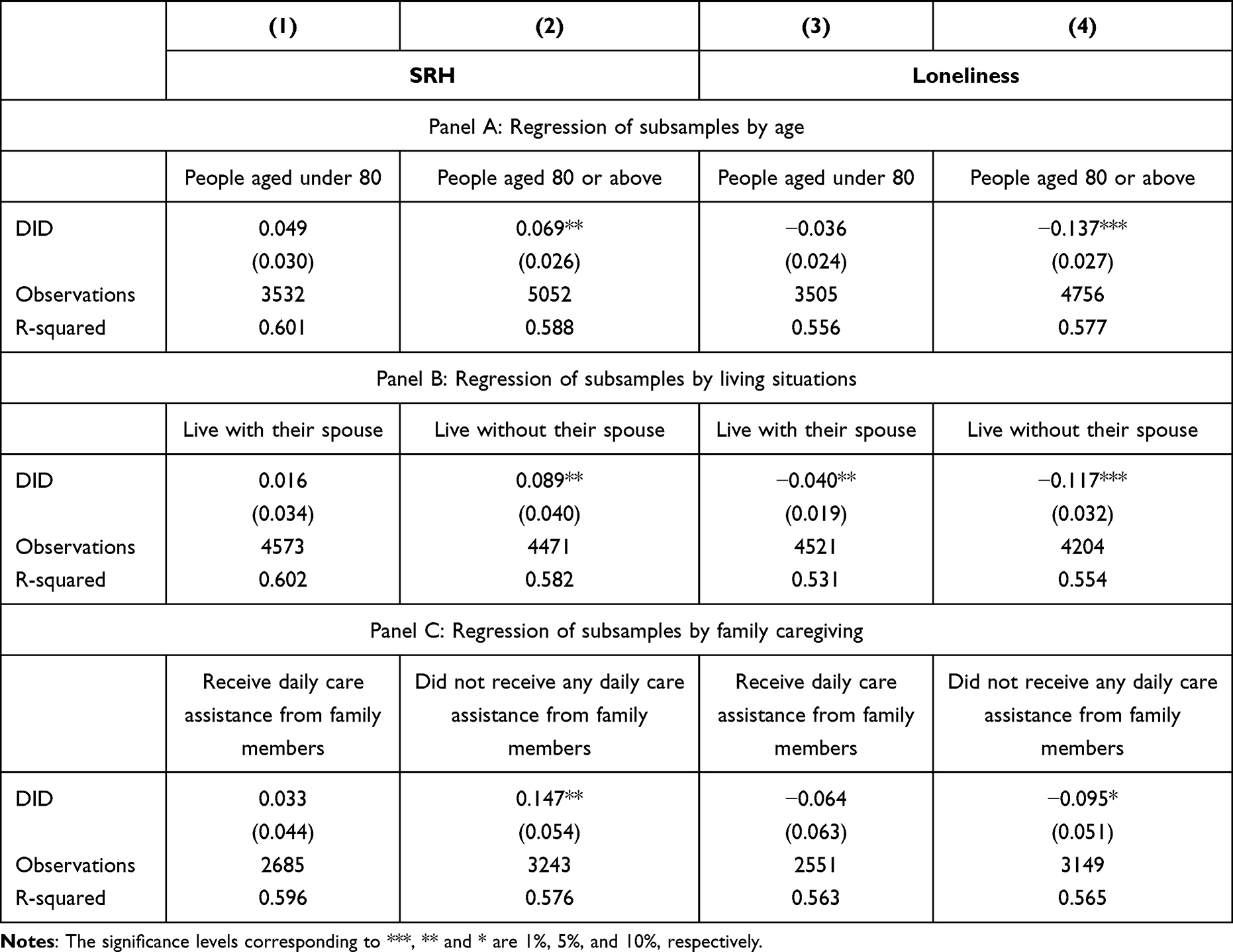 |
Table 6 Heterogeneity Analysis - Individual Characteristics |
Firstly, the sample was stratified into two cohorts based on age, distinguishing those younger and older than 80, and conducted a regression analysis. Panel A of Table 6 unveils that policy implementation exerted a more pronounced influence on enhancing the physical and mental well-being of older adults in the higher-age group. At the same time, no statistically significant impact was observed for those in the lower-age group. These results seamlessly align with existing scholarly literature and real-world expectations, illuminating that formal older adult care services possess more significant potential to ameliorate the health of older individuals grappling with compromised physical functioning.
Secondly, the sample was segmented into two groups based on cohabitation with a spouse, followed by a regression analysis. Panel B demonstrates that policy implementation significantly bolstered the physical and mental health of older adults who did not reside with their spouses while enhancing the psychological equilibrium of those who did cohabit with their spouses. Furthermore, the affirmative influence of policy implementation on the psychological well-being of older adults devoid of spousal cohabitation was notably amplified. These revelatory findings underscore the efficacy of policy implementation in effectively mitigating the detrimental repercussions of marital upheavals on the health of older individuals.
Thirdly, the sample was categorized into two distinct subsets based on whether older adults received daily care assistance from their family members in 2011, which was followed by a regression analysis.49,50 Panel C illuminates that policy implementation exerted a significant positive impact on augmenting the physical and mental health of older adults without any daily care assistance from their family members. However, no statistically significant impact was discerned for those who did receive such support. These insightful findings underscore the partial substitutionary nature of policy implementation in fulfilling the caregiving role typically fulfilled by family members, providing supplementary daily care for older adults who face a dearth of ample support from their children, thus bolstering their physical and mental fortitude.
Overall, these regression analyses predicated on distinct categories of individual characteristics proffer invaluable insights into the divergent ramifications of policy implementation on the health of older adults. The findings elucidate that policy interventions may yield particular advantages for older adults grappling with diminished physical function, those living without their spouses, and those lacking adequate daily care assistance from family members, culminating in the augmentation of their overall well-being.
Regional Characteristics
Ensuring equitable progress in providing older adult care services across regions is paramount in achieving parity and unrestricted accessibility to healthcare for older populations. This study carefully investigates the differences in older adult health outcomes associated with regional characteristics from two perspectives. The specific outcomes of these analyses are meticulously presented in Table 7.
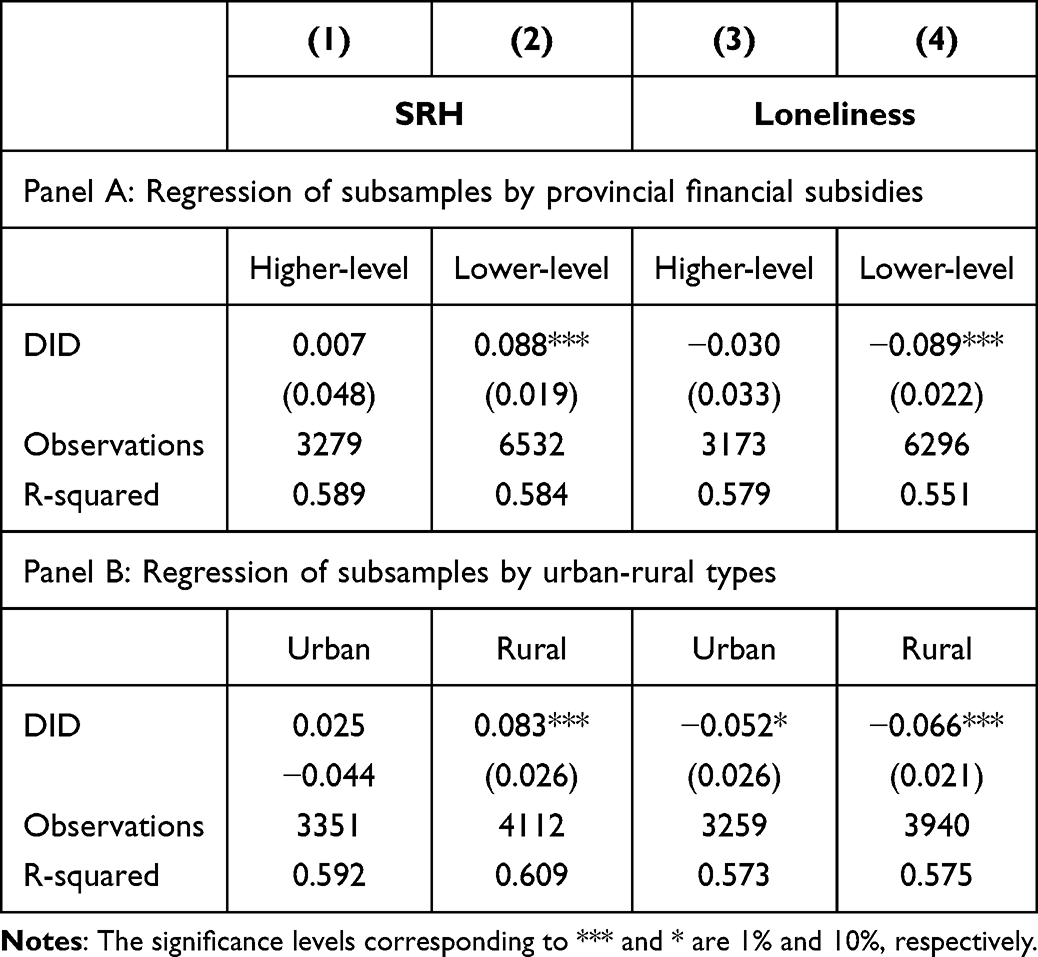 |
Table 7 Heterogeneity Analysis - Regional Characteristics |
Firstly, a grouping regression analysis was conducted based on the province’s average per capita financial subsidy amount in 2011. Panel A of Table 7 astutely illustrates that policy implementation positively influenced older adults’ physical and mental well-being in provinces with lower per capita financial subsidies. Conversely, no discernible association emerged between policy implementation and health enhancement among older adult residents in provinces boasting higher per capita financial subsidies. These findings lucidly suggest that fostering the growth of the older adult care service industry under the guidance of a market-oriented government fund model can effectively galvanize the untapped potential for development within financially deprived regions in the old-age care sector, thereby catalyzing improvements in the health of the older adult populace.
Secondly, a grouping regression analysis was conducted predicated on the urban-rural classification of the older adults’ locales. Panel B indicates that policy implementation significantly engendered psychological well-being and alleviated feelings of isolation among older adults dwelling in rural areas, while no statistically significant effects were observed among their urban counterparts. These consequential findings intimate that advancing the older adult care service industry under the auspices of a market-oriented government fund model can successfully invigorate the latent developmental prospects of underserved rural areas within the old-age care sector, leading to tangible enhancements in the health outcomes for the older adult population.
In summary, the grouping regression analyses predicated on regional characteristics proffer an illuminating perspective on the heterogeneous effects of policy implementation on the health of older adults. The results underscore that policy interventions can potentially ameliorate the health disparities among older individuals, often engendered by economic development disparities. In effect, they lay the groundwork for more equitable and efficacious improvements in the overall health and well-being of the older adult demographic.
Discussion
The study’s meticulous analysis of average effects demonstrates the salutary impact of harnessing market-oriented government guidance funds to enrich the older adult care service industry, thereby fostering a tangible improvement in older adults’ physical and mental well-being. The empirical evidence gleaned from this study carries profound implications, transcending the boundaries of China and extending to other developing nations, underscoring the immense potential for sustainable development within the older adult care service sector through the introduction of market forces. Moreover, the findings herein bestow invaluable insights into other developing nations aspiring to leverage financial policy instruments to nurture the growth of their older adult care service domains.
Furthermore, the probing examination of individual-level heterogeneity effects unveils the significant influence of policy implementation on the physical and mental health of older adults aged 80 years or above, those living in the absence of spousal companionship, and those who lack familial care from their offspring, grandchildren, or other kin. Such findings serve as an emphatic reminder that the implementation of the pilot policy has further contributed to improving the health of vulnerable subgroups within the older adult demographic. Given the rapid expansion of China’s population aged 80 years or above, coupled with the distinctive needs of older adults dwelling alone or as widows,51 policymakers must carefully devise policies and approaches to address the specific challenges faced by these individuals. The individual-level heterogeneity analysis concludes that cultivating the older adult care service industry via a “government-guided and market-oriented operation” model facilitated by government-endorsed investment funds can further engender enhanced health outcomes and equitable advantages for the older adult populace.
Moreover, the scrutiny of regional heterogeneity effects accentuates that older adults inhabiting provinces characterized by lower per capita fiscal expenditures and rural localities experience more pronounced enhancements in their physical and mental well-being consequent to policy implementation. This can be attributed to the adoption of market-oriented government financial support mechanisms, which invigorate social investments.52 Notably, in underdeveloped regions grappling with fiscal constraints, this strategic approach plays a more central role in addressing the dearth of funding afflicting small- and medium-sized enterprises operating within the older adult care service industry and relieving the fiscal onus borne by local governments. In addition, given the prevailing urban-rural dichotomy pervasive within China, characterized by glaring disparities in access to social welfare, nursing resources, and care services for older adult denizens,53 rural areas witness a more substantial older adult population and a languid growth trajectory in the older adult care service industry.54 In light of the discerned regional heterogeneity unveiled through this study, it is strongly advocated that the propulsion of the older adult care service industry be advanced through market-oriented financial policy instruments, which can effectively assuage the health opportunity inequality besetting the older adult populace borne out of economic development disparities between urban and rural areas, as well as between disparate provinces.
In summary, the findings emphatically underscore the potent role of policy implementation in augmenting the well-being of the older adult population and in mitigating the health opportunity disparities engendered by economic development. This research imparts invaluable insights into the efficacy of government-endorsed guidance funds steeped in market-oriented principles, ushering forth positive health outcomes for older adults. Furthermore, it stands as evidence that the market to participate in the elderly care services industry to achieve its sustainable development, casting itself as a veritable reference point for other developing nations in leveraging financial policy instruments to foster the progress of their older adult care sectors.
Japan transformed into an aging society in the 1970s, similar to China in the late 20th century. Both were once “catching up” and “the largest aging society in the world”. This situation seriously challenges the development of Japan’s older adult care service industry. To foster the growth of the older adult care industry and address the initial financing difficulties faced during its early stages, the Japanese government has taken extensive measures to broaden the availability of financing and strengthen support in this domain. Currently, a financing supply system in Japan has been developed, with the government playing a leading role and society as the main support. In contrast, China currently lacks detailed implementation guidelines related to financial policy support. Additionally, the financial products designed to assist different departments within this field fail to adequately capture the distinctive characteristics of each older adult care industry type, leading to a lack of specificity. Consequently, the level of social capital participation remains relatively low. Experience and lessons drawn from the international older adult care service industry, particularly from countries like Japan, have important future implications for the industrial structure of China’s older adult care service industry and a series of policy investments in health development guarantee factors.55 Therefore, we plan to conduct in-depth research on these trends in the future.
Conclusions
The growing older adult population has ushered in an imperative need for comprehensive and tailored older adult care services. In the Chinese context, local government incentive funds have emerged as the primary catalyst for private enterprises to venture into older adult care service provision. However, this initiative has been marred by the exacerbation of regional disparities in economic development, thereby engendering a lopsided industrialization landscape within the old-aged care service sector. Consequently, it becomes paramount to delve into government policies that can efficaciously foster balanced and harmonious growth within this industry. Drawing upon the robust “Pilot Industrialization of Old-Age Service in a Market-Oriented Way” policy and leveraging data sourced from the extensive China Health and Retirement Longitudinal Study (CLHLS) spanning from 2011 to 2018, this study endeavors to unravel the ramifications of market participation bolstered by financial policy instruments on the physical and psychological well-being of China’s venerable older adult population.
The cogent findings of this study resoundingly establish that the cultivation of the older adult care service industry in a market-oriented manner engenders a palpable and substantial amelioration in the overall physical and mental health status of older adults. Furthermore, analysis of individual-level heterogeneity effects sheds luminous insights, revealing that older adults without a spouse and devoid of familial care from children or grandchildren experience magnified health benefits as a direct consequence of the pilot policy. Moreover, the scrutiny of regional-level heterogeneity effects corroborates that older adults inhabiting financially underdeveloped regions reap heightened health dividends owing to the pilot policy’s implementation. These research conclusions decisively affirm that the judicious integration of market-oriented central government guidance funds within the older adult care service industry can reduce health disparities across various geographic regions and demographically diverse groups, thus engendering a resolute stride towards universal health and fostering social equity. This paper’s significant research conclusions have profound implications for policymakers endeavoring to build an ecosystem that seamlessly endows the older adult population with equitable, sustainable, and excellent care services.
Nevertheless, it is incumbent upon us to acknowledge and address the limitations inherent in our study. Primarily, the pilot policy under scrutiny entails the infusion of government investment funds for a minimum duration of five years to fortify the fabric of the older adult care service industry until a state of self-sustenance and robust returns can be attained. Further research must be diligently undertaken to investigate whether the industry can preserve the commendable goal of uplifting older adult health outcomes once fiscal funds are subsequently withdrawn.Moreover, while this study confirms the intrinsic link between developing the older adult care service industry in a market-oriented manner and enhanced health outcomes for this demographic, it does not offer an in-depth examination of the forces behind this relationship or a comprehensive exploration of prospective avenues that could enrich government policies. Future research should address these issues to gain a more profound understanding of this field.
Institutional Review Board Statement
The research described employs secondary data, drawn from the Chinese Longitudinal Healthy Longevity Survey (CLHLS). CLHLS was adopted under the guidance of the Joint Research Ethics Council of Duke and Peking University (IRB00001052-13074) to ensure that it complies with relevant ethical, medical and regulatory requirements. Additionally, the data used in this study were all anonymized prior to use.
Informed Consent Statement
Prior to commencing data collection, all individuals who participated in the CLHLS provided informed consent.
Data Sharing Statement
The data are hosted on the Peking University Open Research Data Platform, available through a persistent URL at https://opendata.pku.edu.cn/dataverse/CHADS.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Xiangtan University.
Acknowledgments
We would like to extend our appreciation to all the investigators and participants involved in the CLHLS.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Research program of Medical and Health Science and Technology Development Plan Project of Shandong province [No. 202103070653].
Disclosure
The authors declare that the research reported in this paper has not been influenced by any apparent conflicting financial interests or personal relationships.
References
1. World population ageing 2020 highlights: living arrangements of older persons. Available from: https://www.un.org/development/desa/pd/news/world-population-ageing-2020-highlights.
2. Pekkarinen S, Melkas H. Welfare state transition in the making: focus on the niche-regime interaction in Finnish elderly care services. Technol Forecast Soc Change. 2019;145:240–253. doi:10.1016/j.techfore.2018.09.015
3. Ding WJ, Xiong B. China’s elderly service industry reform: problems, key points and policy suggestions. J Chin Instit Labor Relat. 2019;33(5):7.
4. Kong T, Yang P. Finding the vulnerable among china’s elderly: identifying measures for effective policy targeting. J Aging Soc Policy. 2019;31:271–290. doi:10.1080/08959420.2018.1485391
5. Zheng X, Lu K, Yan B, Li M. Current situation of public private partnership development for the elderly in China. Open J Soc Sci. 2020;8:165.
6. Sugawara S, Nakamura J. Can formal elderly care stimulate female labor supply? The Japanese Experience. J Jpn Int Econ. 2014;34:98–115. doi:10.1016/j.jjie.2014.05.006
7. Zhan P, Ma X, Li S. Migration, population aging, and income inequality in China. J Asian Econ. 2021;76:101351. doi:10.1016/j.asieco.2021.101351
8. Basten S, Jiang Q. China’s family planning policies: recent reforms and future prospects. Stud Fam Plann. 2014;45(4):493–509. doi:10.1111/j.1728-4465.2014.00003.x
9. Liu S, Li C, Shi Z, et al. Caregiver burden and prevalence of depression, anxiety and sleep disturbances in Alzheimer’s disease caregivers in China. J Clin Nurs. 2017;26(9–10):1291–1300. doi:10.1111/jocn.13601
10. Giles J, Mu R. Elderly parent health and the migration decisions of adult children: evidence from rural China. Demography. 2007;44(2):265–288. doi:10.1353/dem.2007.0010
11. Feng Z, Zhan HJ, Feng X, Liu C, Sun M, Mor V. An industry in the making: the emergence of institutional elder care in urban China. J Am Geriatr Soc. 2011;59(4):738–744. doi:10.1111/j.1532-5415.2011.03330.x
12. Li F, Otani J. Financing elderly people’s long-term care needs: evidence from China. Int J Health Plann Manage. 2018;33(2):479–488. doi:10.1002/hpm.2488
13. Zhou G. The influence of china’s population aging on economic growth. In:
14. Barron DN, West E. The quasi-market for adult residential care in the UK: do for-profit, not-for-profit or public sector residential care and nursing homes provide better quality care? Soc Sci Med. 2017;179:137–146. doi:10.1016/j.socscimed.2017.02.037
15. Luo B, Zhan S. Crossing the river by feeling for the stones: contesting models of marketization and the development of China’s long-term care services. J Chin Gov. 2018;3:438–460. doi:10.1080/23812346.2018.1523296
16. Song H, Yu S, Liu F, Sun X, Sun T. Optimal subsidy support for market-oriented transformation of elderly care: focus on the gap between supply and demand in aging regions of China. Healthcare. 2020;8:441. doi:10.3390/healthcare8040441
17. Stolt R, Winblad U. Mechanisms behind privatization: a case study of private growth in Swedish elderly care. Soc Sci Med. 2009;68:903–911. doi:10.1016/j.socscimed.2008.12.011
18. Bergman MA, Johansson P, Lundberg S, Spagnolo G. Privatization and quality: evidence from elderly care in Sweden. J Health Econ. 2016;49:109–119. doi:10.1016/j.jhealeco.2016.06.010
19. Marinelli M, Zhang J, Ying Z. Present and future trends of sustainable eldercare services in China. J Popul Ageing. 2022;2022:1–29.
20. Wu B, Mao ZF, Zhong R. Long-term care arrangements in rural China: review of recent developments. J Am Med Dir Assoc. 2009;10:472–477. doi:10.1016/j.jamda.2009.07.008
21. Song H, Ji K, Sun T. Subsidy policy selection of elderly care service projects under uncertain actual demand: a real options analysis based on China’s experience. BMC Geriatr. 2022;22:49. doi:10.1186/s12877-021-02690-0
22. Janssen M, Moors EHM. Caring for healthcare entrepreneurs—towards successful entrepreneurial strategies for sustainable innovations in Dutch healthcare. Technol Forecast Soc Change. 2013;80:1360–1374. doi:10.1016/j.techfore.2012.12.003
23. Song H, Yu S, Sun T. Reducing the quality risk of elderly care services in government procurement from market-oriented private providers through ex ante policy design: lessons from the principal-agent theory analysis. BMC Health Serv Res. 2020;20:1–11. doi:10.1186/s12913-020-05994-w
24. Yu J, Zhang L. Evolution of marine ranching policies in china: review, performance and prospects. Sci Total Environ. 2020;737:139782. doi:10.1016/j.scitotenv.2020.139782
25. Dahaj AS, Cozzarin BP. Government venture capital and cross-border investment. Global Fina J. 2019;41:113–127. doi:10.1016/j.gfj.2019.03.001
26. Yue X, Lin Y. Effectiveness of punishment and operating subsidy in supervision of China’s pension PPP Projects: an evolutionary game and simulation analysis. Math Probl Eng. 2019;2019:1–12.
27. Wan X, Teng Z, Song J, Zhai Y, Zhang K. Government guidance fund empowers the supply chain financing decision of marine ranching considering environmental enrichment and friendliness. Animals. 2023;13:897. doi:10.3390/ani13050897
28. Jin X, Ke Y, Chen X. Credit pricing for financing of small and micro enterprises under government credit enhancement: leverage effect or credit constraint effect. J Bus Res. 2022;138:185–192. doi:10.1016/j.jbusres.2021.09.019
29. Cui J, Zhang S, Yin X, Xu K. Determinants of investment timing of government venture capital guiding funds in China. Discrete Dyn Nat Soc. 2021;2021:1–10. doi:10.1155/2021/7140807
30. Zhang W, Guo C. Research on the model, evolution and development of Chinese government guidance fund. J Soc Sci. 2022;3:1131–1146. doi:10.46799/jss.v3i5.359
31. Gong Y, Li P, Shen Z. Research on operating efficiency of government industry guidance fund. Theor Econ Lett. 2020;10:90. doi:10.4236/tel.2020.101006
32. Guo P. Analysis on the mechanism of government guidance fund to promote the optimization of industrial structure. Times Econ Trade. 2017;27:62–65.
33. Jiang T, He Z, Xiang G, Hu T. The impact of government subsidies on private pension enterprises: a decision-making model based on their CSR levels. IEEE Access. 2021;9:167190–167203. doi:10.1109/ACCESS.2021.3136594
34. 2.4 Billion yuan central support for marketization development of pension services industry in 8 pilot provinces. Available from: http://www.gov.cn/xinwen/2014-08/22/content_2738604.htm.
35. Rao K, Qian J, Chen H. Research on healthy aging and elderly health support system. Chin J Health Manag. 2013;7:149–150.
36. Liu Y, Zheng Z, Rao K, Wang S. Annual Report on Elderly Health in China (2018). Beijing, China: Social Sciences Academic Press; 2019.
37. Pension services industry guidance fund status, challenges and suggestions II - development situation. Available from: https://www.sohu.com/a/222513268_759437.
38. Yi Z, Poston DL, Vlosky DA, Gu D. Healthy Longevity in China: Demographic, Socioeconomic, and Psychological Dimensions. Berlin, Germany: Springer Science & Business Media; 2008.
39. Lei X, Bai C, Hong J, Liu H. Long-term care insurance and the well-being of older adults and their families: evidence from China. Soc Sci Med. 2022;296:114745. doi:10.1016/j.socscimed.2022.114745
40. Zhang Z, Mao Y, Shui Y, Deng R, Hu Y. Do community home-based elderly care services improve life satisfaction of Chinese older adults? An empirical analysis based on the 2018 CLHLS Dataset. Int J Environ Res Public Health. 2022;19:15462. doi:10.3390/ijerph192315462
41. Wang G, Jia C, Ma Z, Zhou L. Physical diseases and elderly suicide in rural china: a case–control psychological autopsy study. Aust N Z J Psychiatry. 2022;56:560–568. doi:10.1177/0004867421998804
42. Yang Y, Meng Y. Is China moving toward healthy aging? A Tracking study based on 5 Phases of CLHLS Data. Int J Environ Res Public Health. 2020;17:4343. doi:10.3390/ijerph17124343
43. Song J, Wu H, Lan H, Xu D, Wang W. The influence of disease status on loneliness of the elderly: evidence from rural China. Int J Environ Res Public Health. 2022;19:3023. doi:10.3390/ijerph19053023
44. Dai H, Jia G, Liu K. Health-related quality of life and related factors among elderly people in Jinzhou, China: a cross-sectional study. Public Health 2015, 129, 667–673. doi:10.1016/j.puhe.2015.02.022
45. Kahn ME, Li P, Zhao D. Water pollution progress at borders: the role of changes in China’s political promotion incentives. Am Econ J Econ Policy. 2015;7:223–242. doi:10.1257/pol.20130367
46. Hong Q, Cui L, Hong P. The impact of carbon emissions trading on energy efficiency: evidence from a quasi-experiment in China’s carbon emissions trading pilot. Energy Economics. 2022;110:106025. doi:10.1016/j.eneco.2022.106025
47. Li P, Lu Y, Wang J. Does flattening government improve economic performance? Evidence from China. J Dev Econ. 2016;123:18–37. doi:10.1016/j.jdeveco.2016.07.002
48. Wei Z, Zeng A, Wu Y, Li C. Whether the rules of limiting IPO first day bidding price restrict investors’ speculation?. J Manag World. 2019;35:192–210.
49. Carr D, Springer KW Advances in families and health research in the 21st century. J Marriage Fam 2010, 72, 743–761. doi:10.1111/j.1741-3737.2010.00728.x
50. Robles TF, Kiecolt-Glaser JK. The physiology of marriage: pathways to health. Physiol Behav. 2003;79:409–416. doi:10.1016/S0031-9384(03)00160-4
51. World population prospects 2022. Available from: https://population.un.org/wpp/.
52. Li X, Yang A, Yan H. Priorities and instruments of local elderly care policies in China: text mining and comparative analysis. Front Public Health. 2021;9:647670. doi:10.3389/fpubh.2021.647670
53. Hu B, Wang J. Unmet long-term care needs and depression: the double disadvantage of community-dwelling older people in rural China. Health Soc Care Community. 2019;27:126–138. doi:10.1111/hsc.12630
54. Feng Z, Glinskaya E, Chen H, et al. Long-term care system for older adults in China: policy landscape, challenges, and future prospects. Lancet. 2020;396:1362–1372. doi:10.1016/S0140-6736(20)32136-X
55. Wang XR. The current situation and development trend of the geriatric medical care industry in Japan. Global Sci Technol Economy Outlook. 2013;28(7):6.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.