")
Back to Journals » International Journal of General Medicine » Volume 16
Impact of the COVID-19 Pandemic on Initiation of Antibiotic Treatment After Performing a Blood Culture and Intervention by the Antimicrobial Stewardship Team
Authors Kubota S, Sasano H , Suzuki M, Fukui Y, Chonan M, Kawakami T, Tabe Y, Miida T, Kimura T , Naito T
Received 17 May 2023
Accepted for publication 26 July 2023
Published 23 August 2023 Volume 2023:16 Pages 3713—3719
DOI https://doi.org/10.2147/IJGM.S418558
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Sanae Kubota,1 Hiroshi Sasano,2,3 Mai Suzuki,3 Yukiko Fukui,3 Masayoshi Chonan,4 Takaaki Kawakami,4 Yoko Tabe,5 Takashi Miida,5 Toshimi Kimura,1 Toshio Naito3
1Department of Pharmacy, Juntendo University Hospital, Tokyo, Japan; 2Department of Pharmacy, Juntendo Tokyo Koto Geriatric Medical Center, Tokyo, Japan; 3Department of General Medicine, Juntendo University Faculty of Medicine, Tokyo, Japan; 4Department of Clinical Laboratory, Juntendo University Hospital, Tokyo, Japan; 5Department of Clinical Laboratory Medicine, Juntendo University Faculty of Medicine, Tokyo, Japan
Correspondence: Hiroshi Sasano, Department of General Medicine, Juntendo University Faculty of Medicine, Hongo 2-1-1, Bunkyo-ku, Tokyo, 113-8421, Japan, Tel +81 03-5802-1190, Email [email protected]
Purpose: Whether the coronavirus disease 2019 (COVID-19) pandemic had any effect on the time between blood culture collection and administration of antibiotics in the outpatient Department of Emergency Medicine in a single university hospital in Japan was investigated, and the intervention carried out by the antimicrobial stewardship team (AST) to promote the appropriate use of antibiotics was examined.
Patients and Methods: The monthly percentage of patients who visited the outpatient Department of Emergency Medicine between January 2019 and December 2021 and received an intravenous antibiotic within 3 hours of blood culture collection was calculated. The AST calculated a quality indicator (QI) based on the results of the investigation and started QI monitoring and hospital feedback.
Results: From January 2020 to March 2021 (the third COVID-19 wave), the implementation rate of antibiotic administration within 3 hours after blood culture collection decreased as the COVID-19 pandemic spread, and the implementation rate tended to increase as the number of COVID-19-positive patients decreased. However, when the AST started monitoring and feedback from April 2021, although there was a temporary decline in the early stages of the fifth wave when the scale of infection was large, the implementation rate rose and was maintained by AST intervention. (the fourth and the fifth COVID-19 waves) (P< 0.01). Also, the implementation rate was significantly lower during the COVID-19 pandemic than during the non- pandemic (P< 0.05).
Conclusion: The early COVID-19 pandemic may have affected the delay in time from blood culture collection to antibiotic administration. Later, in recurring COVID-19 pandemics, AST intervention eliminated this problem. When a bacterial infection such as sepsis is suspected, delayed treatment can be prevented by promptly collecting a blood culture, irrespective of concerns about COVID-19 infection. Calculating the QI may promote AST activities and the appropriate use of antibiotics.
Keywords: coronavirus disease 2019, bacteremia, administration of antibiotics, quality indicator
Introduction
Each year, 30 million cases of sepsis occur worldwide, and six million cases are estimated to die; sepsis therefore remains one of the most fatal conditions.1 Sepsis is a time-sensitive illness, and its prognosis can improve if an early diagnosis is made, and appropriate treatment is carried out.1 The 2016 Surviving Sepsis Campaign Guidelines (SSCG) state that antibiotic treatment should be started within 1 hour of identifying sepsis; however, the 2021 revision to the guidelines recommends that antibiotics be administered immediately, ideally within 1 hour when there is the possibility of septic shock or in adults with a high likelihood of developing sepsis, and within 3 hours when there is possible sepsis without shock.2 In the Japanese Antimicrobial Stewardship Guidelines, monitoring recommendations include the time to administration of the first antibiotics.3 However, coronavirus disease 2019 (COVID-19) spread rapidly throughout the world from the end of 2019 and was declared a global pandemic by the WHO in March 2020. Japan likewise declared a state of emergency in April 2020, and caring for COVID-19 patients became the focus of many healthcare facilities, which impacted routine care practices.4 Further measures were taken, such as reducing outpatient care services and adjusting the flow of day-to-day work to ensure the safety of patients and medical professionals. Due to these measures, chest computed tomography scans were performed to rule out COVID-19 when symptomatic patients with fever visited outpatient departments, which consequently caused delays in the diagnosis and treatment of bacteremia.5
The COVID-19 pandemic also caused delay in perform a physical examination. It is possible that these delays may have contributed to delayed initial treatment with antibiotics following blood culture collection after visiting hospitals, but no studies that focused on whether the COVID-19 pandemic impacted the time between blood culture collection and initial treatment with antibiotics could be identified.
In the present study, first whether the COVID-19 pandemic impacted the time between blood culture collection and antibiotic treatment in the Department of Emergency Medicine of a single university hospital in Japan was investigated. Second, with the aim of right time blood culture collect and administering antibiotics without delay regardless of the COVID-19 pandemic, referring to guideline2 and previous report,6 the implementation rate of intravenous antibiotics within 3 hours of blood culture collection was then set as a new quality indicator (QI). Finally, the effect of data monitoring and hospital feedback by the antimicrobial stewardship team (AST) was subsequently evaluated.
Materials and Methods
Data were retrospectively extracted from the medical records of patients administered intravenous antibiotics after collection of a blood culture during their visit to the outpatient Department of Emergency Medicine at Juntendo University Hospital between January 1, 2019 and December 31, 2021. The percentages of cases in which procedures from blood culture collection to administration of intravenous antibiotics were carried out within 3 hours were calculated by month, and the figures from before and after the COVID-19 pandemic were compared using the mean pre-COVID-19 implementation rate for 2019 as the baseline. The exclusion criteria were (1) unknown time of blood culture collection and (2) patients whose blood culture collection and intravenous antibiotic administration took place on consecutive days. The details investigated were the patients’ age, sex, presence or absence of a positive blood culture (and bacterial species if positive), diagnosis at the time of blood culture collection, the quick Sequential Organ Failure Assessment (qSOFA) score (blood pressure, respiratory rate, level of consciousness), time of blood culture collection, and time of administration of intravenous antibiotics.
The AST has set QIs for treatment of Infectious Diseases and implemented antimicrobial stewardship within hospitals.7 Therefore, a new QI was set based on this investigation’s results, and data monitoring and hospital feedback were started from April 2021.
This study used SPSS for windows Ver.29 for data processing, Welch’s t-tests were used for comparisons between before and after AST intervention groups, at COVID-19 pandemic spread duration. Also, it was used for comparisons between pandemic and non-pandemic COVID-19 duration on the implementation rate of intravenous antibiotics within 3 hours of blood culture collection. A value of P< 0.05 was considered statistically significant.
This study was conducted with the approval of the Juntendo University School of Medicine Research Ethics Committee (E22-0204-H01). Because this study used data from existing electronic medical records, the requirement for written, informed consent was waived. The purpose of the study and the opportunity to opt out were provided on the Juntendo University website. This study complies with the Declaration of Helsinki.
Results
Table 1 shows the data of the target patients. The total number of patients with antibiotics administered by the Department of Emergency Medicine at Juntendo University Hospital was 573 in 2019, 512 in 2020, and 547 in 2021. Number of emergency patients with blood cultures collection before antibiotics administered was 570 in 2019, 499 in 2020, and 545 in 2021. Of these, the number of positive blood cultures was 121 in 2019, 130 in 2020, and 126 in 2021. The main diagnoses at the time of blood culture collection were urinary tract infection, pneumonia, and cholangitis. The number of patients with a positive blood culture whose qSOFA score was 2 or higher, indicating an increased risk of sepsis, was 27 in 2019, 36 in 2020, and 28 in 2021.
 |
Table 1 Participants’ Characteristics |
The trend in the rate of patients administered intravenous antibiotics within 3 hours of blood culture collection (hereinafter “implementation rate”) and the collection of 2 sets of blood cultures rate is shown in Figure 1. The collection rate of two sets of blood cultures was maintained at a high level. On the other hand, the average annual implementation rate in 2019 was 88%. From January 2020 to March 2021 (1st to 3rd waves) after the COVID-19 pandemic spread, monthly trends in the blood culture collection rate showed a decrease with COVID-19, and then an increase as the number of COVID-19-positive patients decreased. However, when the AST started monitoring and feedback from April 2021, although there was a temporary decline in the early stages of the fifth wave when the scale of infection was large, the implementation rate rose and was maintained by AST intervention. (the fourth and the fifth COVID-19 waves) (P<0.01) (Figure 2). Also, non-pandemic period (January 2019-March 2020), the average implementation rate was 89%, while the average implementation rate was 85.1% significantly lower in the pandemic period (first wave: April-May 2020, 2nd wave: July-August 2020, 3rd wave: November 2020-March 2021, 4th wave: April-May 2021, 5th wave: July-October 2021) (P<0.05) (Figure 3).
 |
Figure 1 Antibacterial agent administration rate within 3 hours after blood culture: 2019–2021. |
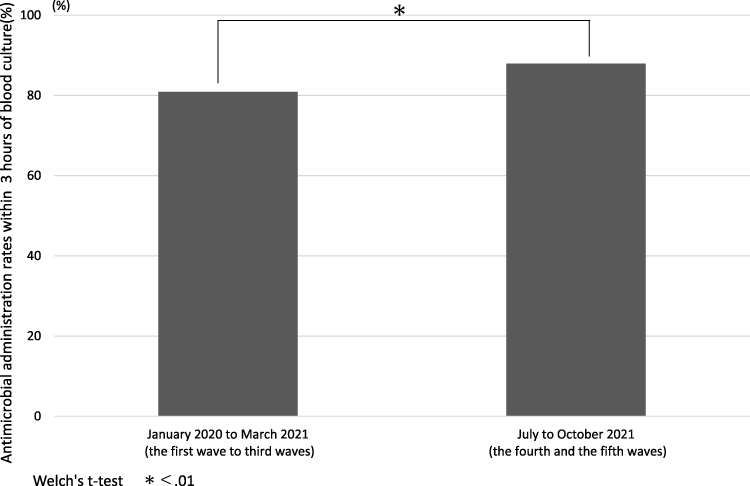 |
Figure 2 Comparison of antimicrobial administration rates within 3 hours of blood culture before and after AST intervention. |
 |
Figure 3 Comparison of antimicrobial administration rates within 3 hours of blood culture before and after COVID-19 pandemic. |
Discussion
Sepsis involves dysregulation of the host’s biological response to infection and causes life-threatening organ damage. When infection is suspected, a patient usually has symptoms, including a fever exceeding 38.5 °C, a dry cough, shortness of breath, and diarrhea. In patients with a severe febrile illness, a blood culture to rule out bacterial infection is absolutely necessary.8 Also, to maximize the chances of identifying culprit pathogens, blood cultures should be done before antibiotics are administered.9
Bacteremia has a particularly high mortality, and early administration of antibiotics is proven to reduce mortality.10 Rüddel et al reported that delayed start of treatment for infection increased 28-day mortality in patients with sepsis or septic shock, and that delay to administration of antibiotics increased the risk of mortality and the risk of progression from sepsis to septic shock, irrespective of the presence or absence of septic shock,11 which also suggests the importance of prompt administration of antibiotics after blood culture collection when infection is suspected.
The qSOFA score is used to screen for sepsis outside the ICU. In a previous study, 70% of patients without an infectious disease with a qSOFA score of 2 or higher had a poor prognosis. On the other hand, less than 30% of patients with an infectious disease had a qSOFA score of 2 or higher; they point out that the presence or absence of infectious disease should therefore not be judged based on the qSOFA score alone.12 The latest guidelines state that, as a general rule, screening for sepsis should not be carried out using the qSOFA score alone.2 The present investigation showed results consistent with those of an earlier study for the number of blood culture collection patients with a qSOFA score of 2 or higher each year (4.7% in 2019, 7.0% in 2020, and 5.1% in 2021). This suggests the importance of not assessing patients using the qSOFA score alone and promptly administering antibiotics after blood culture collection in cases of suspected sepsis.
The 2012 UK Surviving Sepsis Campaign recommends de-escalation of antibiotics based on the microbiological findings of a blood culture conducted before administering antibiotics.13 Overuse of broad-spectrum antibiotics can be a risk factor for the development of resistant pathogens, and blood culture collection also appears to be important from the perspective of antimicrobial stewardship. Based on these recommendations, a high blood culture collection rate of 92% has been reported in the field of intensive care medicine in Japan.14 However, the authors could find no academic papers on blood culture collection rates outside the field of intensive care medicine, which means that the current situation regarding antimicrobial stewardship is unclear. Outside of Japan, the development of QIs is being promoted to evaluate the appropriate use of antibiotics, and QIs are reported to be effective in improving antimicrobial stewardship in routine clinical care.15 A QI is defined as “a measurable element of practice performance with evidence or consensus that it can be used to assess the quality of care provided”.16 The AST of our hospital has therefore set “the rate of implementation of intravenous antibiotics within 3 hours of blood culture collection” as a QI and has started feedback on blood culture collection rates and awareness-raising activities via a newsletter.
Immediately after COVID-19 was declared a global pandemic, blood culture collection rates showed a downward trend. This was likely due to disruption of the medical system caused by COVID-19, the threat to the mental and physical health of healthcare professionals,17 and the consequent impact on clinical diagnoses.5 If infectious disease is suspected, it was no change in our hospital policy of “blood cultures collection before antibiotics are administred”. But, the results of the present investigation also suggest that prioritizing tests to rule out COVID-19 in patients with symptoms of fever and disruption to the medical system caused by COVID-19 contributed to the decrease in the blood culture collection rate. However, no large decrease in the blood culture collection rate was seen from June 2021, when awareness-raising activities were started, despite the continued spread of the pandemic.
In addition, the implementation rate of intravenous antibiotics within 3 hours of blood culture collection was 88% before COVID-19 became a global pandemic. This is better than the report that 73.9% of patients diagnosed with sepsis in Japanese Emergency Departments received antibiotics within 3 hours.18 Thereafter, AST awareness-raising activities were able to improve it to the same level as the average implementation rate in 2019 from June 2021.
We believe that setting a QI and visualization through feedback contributed to maintaining the blood culture collection rate and contributed to recovery of the implementation rate of intravenous antibiotics within 3 hours of blood culture collection.
A limitation of the present investigation was that the QI, ie, the implementation rate of intravenous antibiotics within 3 hours of blood culture collection, only partly assessed the appropriate use of antibiotics. Therefore, the evaluation of the process, such as the rate of antibiotic de-escalation based on blood culture results and the rate of antibiotic discontinuation, was not included. Furthermore, the study was conducted in a single university hospital in Japan. This means that evaluation of the process is needed, as described above, in addition to the blood culture implementation rate and time to treatment start, in addition to the blood culture implementation rate and time to treatment start. Clinical outcomes of patients associated with this process also need to be assessed, in addition to the process of appropriate antibiotic use.
Conclusion
In conclusion, the early COVID-19 pandemic may have affected the delay in time from blood culture collection to antibiotic administration. Later, in recurring COVID-19 pandemics, AST intervention eliminated this problem. When a bacterial infection such as sepsis is suspected, delayed treatment can be prevented by promptly collecting a blood culture, irrespective of concerns about COVID-19 infection. Calculating the QI may promote AST activities and the appropriate use of antibiotics.
Acknowledgments
The authors would like to thank Mr. Toshihiro Yoshizawa in the Department of Pharmacy, Juntendo University Hospital, and Mr. Toshihiro Takahashi in the Department of Clinical Laboratory, Juntendo University Hospital, for their study support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work did not receive any grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Candel FJ, Borges Sá M, Belda S, et al. Current aspects in sepsis approach. Turning things around. Rev Esp Quimioter. 2018;31:298–315. doi:10.1097/EJA.0000000000000798
2. Evans L, Rhodes A, Alhazzani W, et al. Executive summary: surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock 2021. Crit Care Med. 2021;49:1974–1982. doi:10.1097/CCM.0000000000005357
3. The Eight Societies Joint Committee for enhancement of antimicrobial stewardship. Guidance for implementing an antimicrobial stewardship program in Japan. Jpn J Chemother. 2017;65:650–687. Japanese.
4. Yan Y, Tomooka K, Naito T, Tanigawa T. Decreased number of inpatients with community-acquired pneumonia during the COVID-19 pandemic: a large multicenter study in Japan. J Infect Chemother. 2022;28:709–713. doi:10.1016/j.jiac.2022.01.013
5. Miyagami T, Uehara Y, Harada T, et al. Delayed treatment of bacteremia during the COVID-19 pandemic. Diagnosis. 2021;19:327–332. doi:10.1515/dx-2020-0114
6. Nadia A, Erick O, Patricia MS, et al. Prehospital antibiotics in the ambulance for sepsis: a multicentre, open label, randomised trial. Lancet Respir Med. 2018;6:40–50. doi:10.1016/S2213-2600(17)30469-1
7. Sasano H, Yoshizawa T, Kawakami T, et al. Improvements in quality indicators for the treatment of infectious diseases with intervention by an antimicrobial stewardship team. J Hosp Gen Med. 2021;3:1–10.
8. Mormeneo BS, Palacián RMP, Moreno HM, Villuendas UMC. Bacteremia during COVID-19 pandemic in a tertiary hospital in Spain. Enferm Infecc Microbiol Clin. 2022;40:183–186. doi:10.1016/j.eimc.2021.01.015
9. Matthew PC, Robert S, Katryn P, et al. Blood culture results before and after antimicrobial administration in patients with severe manifestations of sepsis: a diagnostic study. Ann Intern Med. 2019;171:547–554. doi:10.7326/M19-1696
10. Papadimitriou-Olivgeris M, Psychogiou R, Garessus J, et al. Predictors of mortality of bloodstream infections among internal medicine patients in a Swiss hospital: role of quick sequential organ failure assessment. Eur J Intern Med. 2019;65:86–92. doi:10.1016/j.ejim.2019.05.003
11. Rüddel H, Thomas-Rüddel DO, Reinhart K, et al. Adverse effects of delayed antimicrobial treatment and surgical source control in adults with sepsis: results of a planned secondary analysis of a cluster-randomized controlled trial. Crit Care. 2022;26:51. doi:10.1186/s13054-022-03901-9
12. Seymour CW, Liu VX, Iwashyna TJ, et al. Assessment of clinical criteria for sepsis: for the third international consensus definitions for sepsis and septic shock (sepsis-3). JAMA. 2016;315(8):762–774. doi:10.1001/jama.2016.0288
13. Dellinger RP, Levy MM, Rhodes A, et al. Surviving sepsis campaign: international guidelines for management of severe sepsis and septic shock: 2012. Crit Care Med. 2013;41:580–637. doi:10.1097/CCM.0b013e31827e83af
14. Abe T, Ogura H, Shiraishi A, et al. Characteristics, management, and in-hospital mortality among patients with severe sepsis in intensive care units in Japan: the FORECAST study. Crit Care. 2018;22:322. doi:10.1186/s13054-018-2186-7
15. van den Bosch CM, Hulscher ME, Natsch S, et al. Development of quality indicators for antimicrobial treatment in adults with sepsis. BMC Infect Dis. 2014;14:345. doi:10.1186/1471-2334-14-345
16. Lawrence M, Olesen F. Indicators of quality in health care. Eur J Gen Pract. 1997;3:103–108. doi:10.3109/13814789709160336
17. Harada T, Watari T, Miyagami T, Watanuki S, Shimzu T, Hiroshige J. COVID blindness: delayed diagnosis of aseptic meningitis in the COVID-19 era. Eur J Case Rep Intern Med. 2020;7:001940. doi:10.12890/2020_001940
18. Abe T, Kushimoto S, Tokuda Y, et al. Implementation of earlier antibiotic administration in patients with severe sepsis and septic shock in Japan: a descriptive analysis of a prospective observational study. Crit Care. 2019;23:360. doi:10.1186/s13054-019-2644-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.