Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Impact of Plan-Do-Study-Act Cycle-Based Quality Improvement on Head-of-Bed Elevation Compliance, Cuff Pressure Management and Ventilator-Associated Pneumonia in Intensive Care Units: A Before-After Study
Authors Zhong X, Li T, Lin L, Zhou L, Yang Y, Hu J ![]()
Received 6 March 2026
Accepted for publication 7 June 2026
Published 8 July 2026 Volume 2026:19 607474
DOI https://doi.org/10.2147/JMDH.S607474
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Judith Johnson
Xiu Zhong1, Ting Li1, Li Lin1, Lu Zhou1, Yi Yang1, Juan Hu2
1Department of Emergency, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China; 2Department of Respiratory and Critical Care Medicine, The Affiliated Hospital of Southwest Medical University, Luzhou, Sichuan, 646000, People’s Republic of China
Correspondence: Juan Hu, Department of Respiratory and Critical Care Medicine, The Affiliated Hospital of Southwest Medical University, 25th Taiping Street, Jiangyang District, Luzhou, Sichuan, 646000, People’s Republic of China, Email [email protected]
Objective: This study aimed to evaluate the association between Plan-Do-Study-Act (PDSA) cycle-based quality improvement measures and the correct implementation rate of head-of-bed elevation, artificial airway cuff pressure compliance, and ventilator-associated pneumonia (VAP) incidence in mechanically ventilated patients, and to identify independent influencing factors of the two core care indicators.
Methods: A total of 4305 patients receiving mechanical ventilation for ≥48 hours in the Emergency Intensive Care Unit (EICU) and Respiratory Intensive Care Unit (RICU) were enrolled, divided into the pre-implementation group (n=2163, Jan-Dec 2024) and the post-implementation group (n=2142, Jan-Dec 2025). The post-implementation group received comprehensive improvement measures based on the PDSA cycle, including standardized monitoring, normalized measuring tools and continuous quality control. The two indicators’ compliance rates and VAP incidence were compared between groups. Univariate and multivariate Logistic regression analyses were used to identify influencing factors, and Spearman correlation analysis was performed to explore the relationship between indicator compliance and VAP incidence.
Results: The post-implementation group had significantly higher compliance rates of both indicators and lower VAP incidence (all P<0.05). Both indicators were significantly negatively correlated with VAP incidence (all P<0.001). APACHE II score ≥25, mechanical ventilation ≥10 days, patient agitation and delirium, and insufficient nursing staffing were independent risk factors for lower compliance rates, while standardized processes and quality monitoring were independent protective factors (all P<0.05).
Conclusion: PDSA cycle-based comprehensive quality improvement measures were associated with improved compliance rates of head-of-bed elevation and artificial airway cuff pressure in mechanically ventilated patients, and lower VAP incidence. Standardized procedures and continuous quality monitoring are key to maintaining high compliance of these two core VAP prevention indicators.
Keywords: PDSA cycle, ventilator-associated pneumonia, head-of-bed elevation, cuff pressure, nursing quality improvement, compliance rate
Introduction
Ventilator-associated pneumonia (VAP) is the most common nosocomial infection in patients with artificial airways receiving mechanical ventilation.1 Its occurrence significantly prolongs mechanical ventilation duration and hospital stay, increases medical resource consumption, and raises in-hospital mortality, making it a key challenge in nosocomial infection control and nursing quality management in critical care settings.2 Head-of-bed elevation at 30°~45° and maintenance of artificial airway cuff pressure at 25~30 cmH2O are two core preventive measures strongly recommended by international and domestic VAP prevention guidelines, and critical links to block VAP pathogenesis.3 Head-of-bed elevation reduces gastroesophageal reflux and microaspiration of oropharyngeal secretions by altering patient position, thereby lowering the risk of lower respiratory tract colonization by pathogenic bacteria. This operation requires no additional equipment and is a cost-effective VAP prevention measure. The maintenance of artificial airway cuff pressure within the optimal range of 25~30 cmH2O is the core point of airway barrier management. This pressure value can not only ensure the close fit between the cuff and the airway wall, effectively block the secretions retained above the cuff from falling into the lower respiratory tract, but also avoid airway mucosal ischemic injury caused by excessive pressure or sealing failure due to insufficient pressure, which is the core quality control indicator for artificial airway management.4,5 The standardized implementation and high-quality management of these two indicators are the important foundation for VAP prevention and control, and their clinical compliance rate directly affects the overall effect of VAP prevention and control, and is also an important sensitive indicator for evaluating the nursing quality of Emergency Intensive Care Unit (EICU) and Respiratory Intensive Care Unit (RICU).6
In recent years, although hospitals worldwide have increasingly emphasized standardized VAP prevention and control, suboptimal compliance with core preventive measures remains a persistent global challenge. International multicenter studies have reported that the correct execution rate of head-of-bed elevation ranges from 45% to 78% across different regions, while cuff pressure compliance rates vary between 32% and 65% in low- and middle-income countries (LMICs) and 58% to 82% in high-income countries.7–9 Even in well-resourced healthcare settings, compliance rates often fail to meet guideline-recommended targets due to systemic barriers, staff workload constraints, and inconsistent implementation protocols. In China, despite growing national attention to VAP prevention and control, similar issues persist, with low correct execution rates of head-of-bed elevation and non-standard cuff pressure monitoring still prevalent in clinical practice. The traditional management model is mainly based on single training or phased supervision, lacking systematic root cause analysis, targeted improvement strategies and sustainable quality control mechanisms, leading to poor clinical compliance with preventive measures and difficulty in achieving the ideal effect of VAP prevention and control.10,11
The Plan-Do-Study-Act (PDSA) cycle is an iterative scientific quality improvement method. Through closed-loop management of formulating improvement plans by stages, implementing improvement measures, analyzing implementation effects and optimizing improvement strategies, it can accurately solve quality problems in clinical practice.12,13 It has been widely used in many fields such as the continuous improvement of hospital nursing quality and nosocomial infection control, and can effectively improve the standardization and compliance of clinical measure implementation.14,15 This study was conducted in a complex clinical environment where multiple simultaneous practice changes may have contributed to the observed outcomes. This inherent characteristic of real-world quality improvement research should be considered when interpreting the results of the before-after study design, which is susceptible to temporal confounding but provides pragmatic evidence for translating evidence into routine clinical practice. In view of this, this study took the PDSA cycle as a quality improvement tool, systematically analyzed the causes and formulated improvement countermeasures for the existing problems in the management of head-of-bed elevation and artificial airway cuff pressure in our hospital’s EICU and RICU. By analyzing the nursing quality monitoring data and clinical outcomes of mechanically ventilated patients in our hospital’s EICU and RICU from 2024 to 2025, it aimed to verify the effect of the PDSA cycle on improving the compliance rates of the two core prevention and control indicators, clarify their independent influencing factors, and evaluate the impact of the compliance rates of the two indicators on the incidence of VAP, so as to provide empirical evidence for further optimizing the VAP prevention strategy and establishing a long-term mechanism for the continuous improvement of artificial airway nursing quality.
Materials and Methods
Study Subjects
Patients who received mechanical ventilation for ≥48 hours in the EICU and RICU of our hospital from January 2024 to December 2024 were selected as the pre-implementation group, and those who received mechanical ventilation in the same units from January 2025 to December 2025 were the post-implementation group. The sample size included all eligible patients admitted to the EICU and RICU during the study periods. Inclusion criteria: (1) Aged ≥18 years; (2) Underwent orotracheal/nasotracheal intubation or tracheotomy for mechanical ventilation; (3) Complete clinical data and nursing quality monitoring data. Exclusion criteria: (1) Contraindications to head-of-bed elevation (such as severe hypotension, increased intracranial pressure, spinal cord injury, etc).; (2) Duration of mechanical ventilation <48 hours; (3) Patients receiving hospice care or with abandoned treatment. This study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of The Affiliated Hospital of Southwest Medical University (Approval No.: KY2025694). A total of 4305 patients were finally enrolled, including 2163 in the pre-implementation group and 2142 in the post-implementation group.
Study Methods
The pre-implementation group adopted the traditional nursing management model: routine theoretical training on VAP prevention and control was carried out, there was no unified standardized process for head-of-bed elevation and cuff pressure monitoring, which were implemented by nurses based on clinical experience; quality control was mainly based on quarterly random checks, and there was no unified electronic traceability system for monitoring results.
The post-implementation group adopted a quality improvement model based on the PDSA cycle. A quality improvement team consisting of 3 physicians and 6 nurses from EICU and RICU, 2 nursing department quality control specialists, 2 hospital information department staff and 1 clinical pharmacist was established, and targeted improvements were implemented in strict accordance with the four stages of the PDSA cycle. The specific measures were as follows:
(1) Plan stage (root cause analysis): By retrospectively analyzing the 2024 nursing quality monitoring data, bedside field observations and semi-structured interviews with nursing staff, combined with the fishbone diagram root cause analysis method (Figure 1), the core problems of poor implementation of the two measures were identified: ① Non-standard monitoring processes, failing to meet the standard of monitoring at least once every 6–8 hours specified in WS/T 661–2023 Specifications for Artificial Airway Cuff Management (p.12); ② Improper use of measuring tools, relying on subjective judgment methods such as digital palpation with large pressure measurement errors; ③ Lack of an effective quality supervision and control mechanism, with no closed-loop management for problem rectification; ④ Insufficient knowledge and understanding among medical and nursing staff regarding the importance of these measures in preventing VAP (Table 1 and Figure 2).
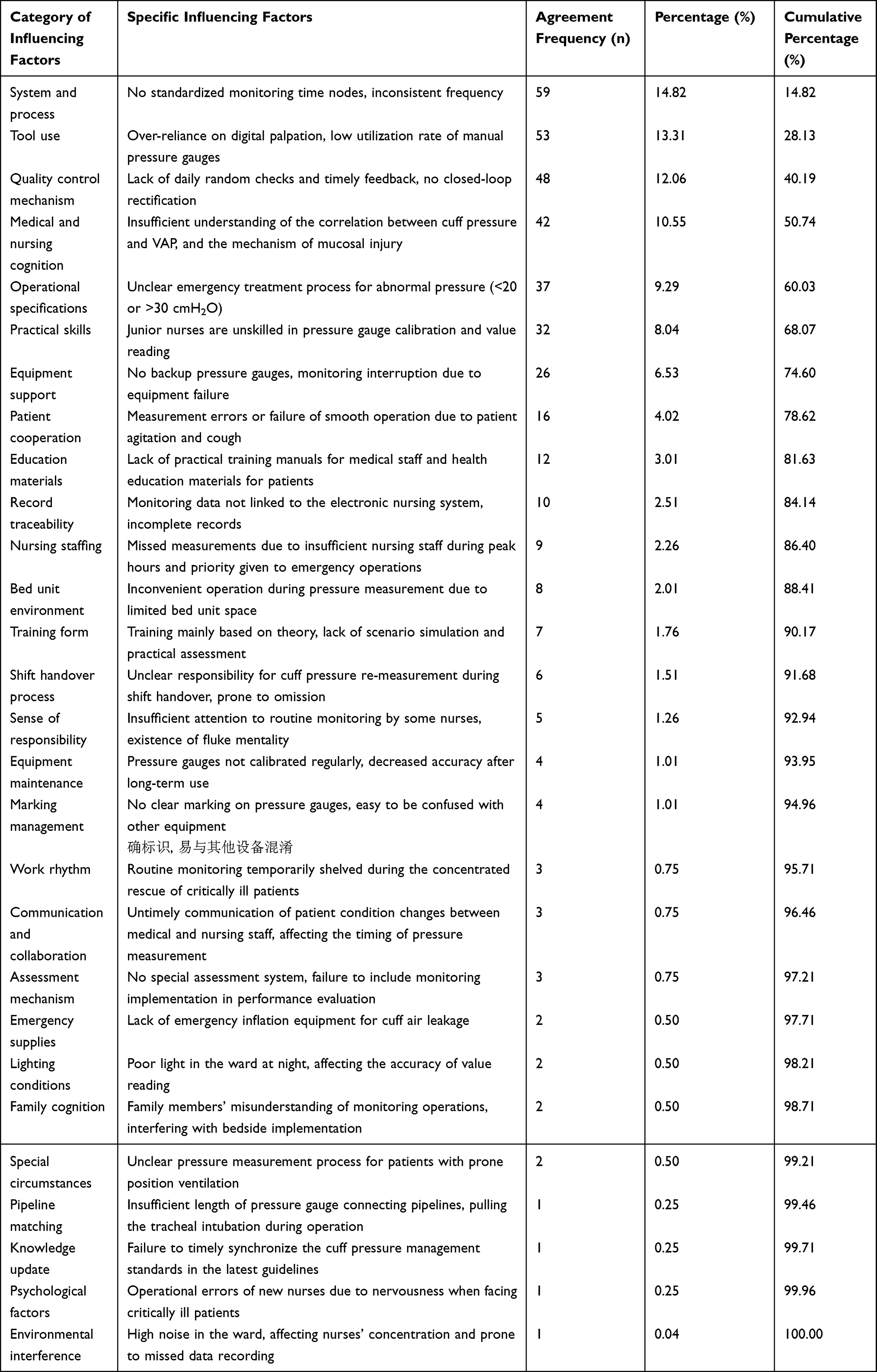 |
Table 1 Survey Results of Influencing Factors for Head-of-Bed Elevation and Cuff Pressure Management |
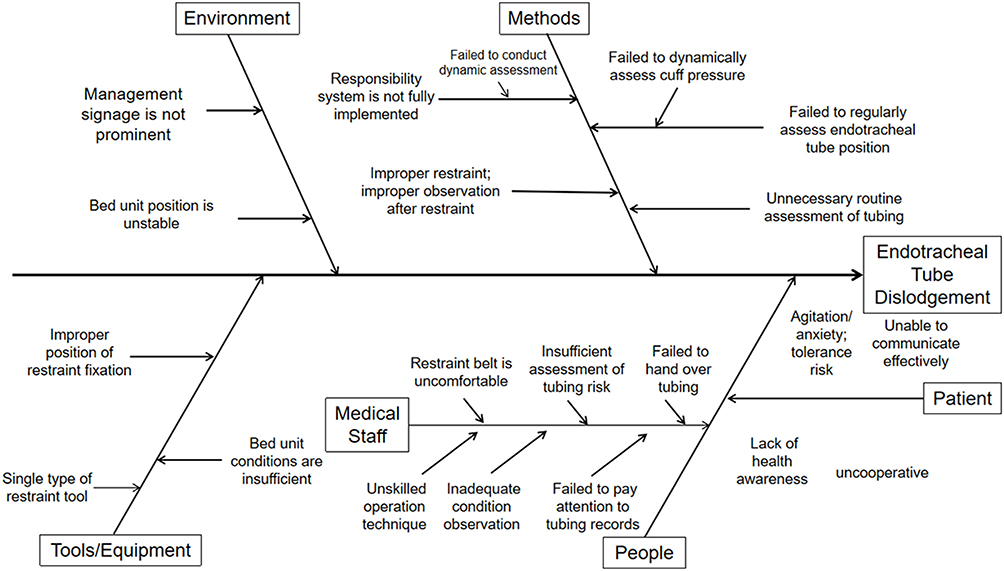 |
Figure 1 Fishbone diagram of root cause analysis for poor implementation of head-of-bed elevation and cuff pressure management. Abbreviation: VAP, ventilator-associated pneumonia. |
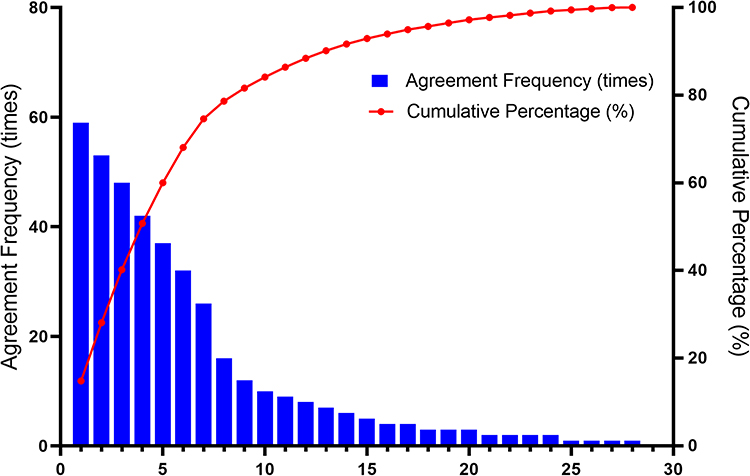 |
Figure 2 Pareto chart of survey results of influencing factors for head-of-bed elevation and cuff pressure management. |
(2) Do stage (implementation of the improved plan): ① Standardized monitoring process: A dual system of monitoring every 4–8 hours + re-measurement during shift handover was formulated, and four core monitoring time nodes were fixed: 8:00 for N-A (night to morning) shift handover, 12:00 for the extra shift, 16:00 for A-P (afternoon to evening) shift handover and 0:00 for P-N (evening to night) shift handover. Monitoring results were recorded in the electronic nursing system in real time to achieve full-process traceability; ② Normalized measuring tools: Precision manual cuff pressure gauges were uniformly equipped, digital palpation was completely eliminated, and hands-on operation training on tool use was organized for all staff; ③ Intensified special training: Special training on VAP prevention guidelines, cuff pressure management standards, standardized processes and emergency treatment specifications was carried out with a model of theory + hands-on operation + scenario simulation, and the qualified rate of post-training assessment reached 100%.
(3) Study stage (effect analysis): The compliance rate data of the two measures in the first 3 months of the implementation stage were summarized and compared with the same period before the implementation. The difficult problems in process implementation (such as unskilled operation of junior nurses, missed measurements due to insufficient staffing during peak hours) were analyzed, and targeted optimization plans were formulated.
(4) Act stage (quality control consolidation): A long-term mechanism for continuous quality control was established: ① Daily random checks: Head nurses and the quality control team randomly checked the cuff pressure monitoring records of 20% of patients every day to verify the measurement time, numerical accuracy and record integrity; ② Monthly analysis: Special sensitive indicator data were summarized monthly to analyze the change trend of the compliance rates of the two measures, and special rectification meetings were held for abnormal problems; ③ Rewards and punishments linkage: The results of random checks and monthly analysis were linked to the performance of nursing staff to strengthen implementation compliance; ④ Dynamic optimization: The monitoring process was continuously improved according to actual clinical problems, such as supplementing the pressure measurement specifications for patients with prone position ventilation and configuring backup pressure gauges.
Observation Indicators
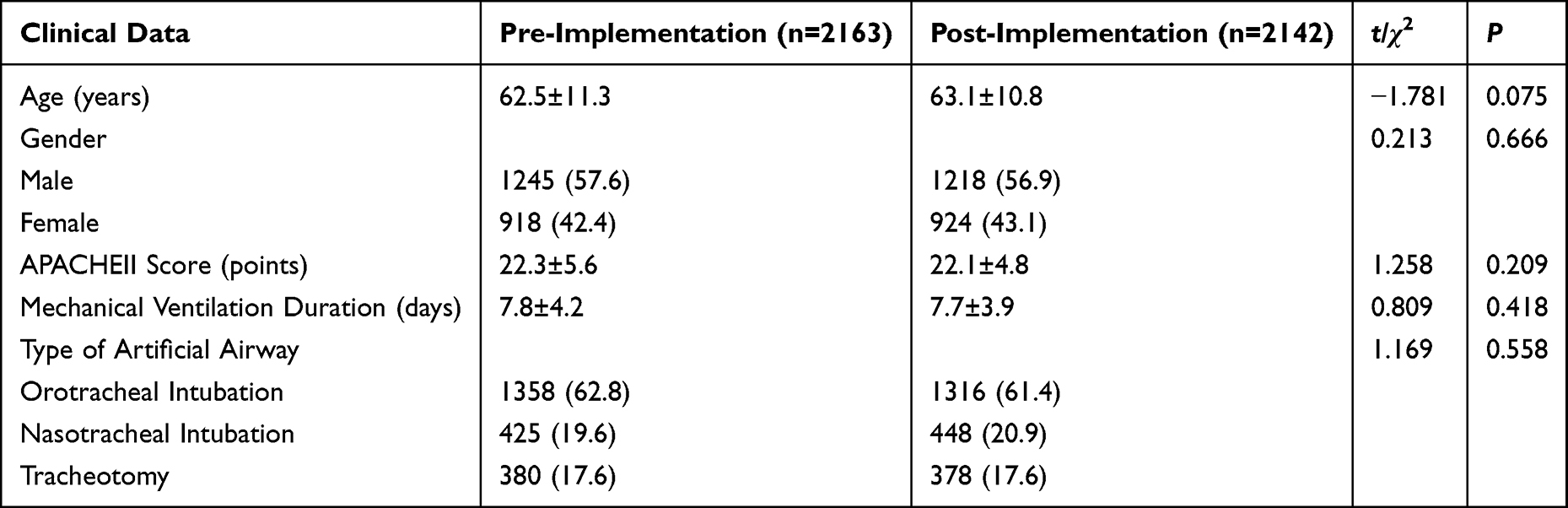
1. General data: Gender, age, Acute Physiology and Chronic Health Evaluation II (APACHEII) score, mechanical ventilation duration, and type of artificial airway were collected from the hospital’s electronic medical record system.
2. Correct execution rate of head-of-bed elevation in mechanically ventilated patients: Calculated by the formula “Number of mechanically ventilated patients with correctly executed head-of-bed elevation (30°–45°) within a certain period/Total number of mechanically ventilated patients during the same period × 100%”. Measured and recorded by responsible nurses using an angle ruler daily, and randomly verified by head nurses.
3. Compliance rate of artificial airway cuff pressure: Calculated by the formula “Number of patients with artificial airway whose measured cuff pressure is within 25–30 cmH2O within a certain period/Total number of patients with artificial airway during the same period × 100%”. Systematic monitoring was not conducted before April 2024; manual cuff pressure gauges were used from April 2024 (finger palpation was eliminated); the “monitoring every 4–8 hours + re-measurement during shift handover” system was implemented from 2025, and measurement data were recorded in the electronic nursing system in real time.
4. VAP incidence: Independently determined by two full-time infection control specialists who were blinded to the group allocation of patients according to the diagnostic criteria in the “Diagnosis and Treatment Guidelines for Hospital-Acquired Pneumonia and Ventilator-Associated Pneumonia in Chinese Adults (2018 Edition)”,16 and VAP occurrence during mechanical ventilation was recorded.
Quality Control
A unified Nursing Quality Data Collection Form was formulated, and two researchers received unified training and could participate in data extraction only after passing the post-training assessment; data were extracted independently by two persons and cross-checked after extraction, and discrepancies were resolved through group discussion or consultation with third-party experts in critical care medicine; logical verification was conducted on the collected data to ensure a reasonable numerical range and consistent records, avoiding entry errors; the quality control team supervised the entire research process to ensure that the research process met the design requirements and reduce bias.
Statistical Analysis
SPSS 26.0 statistical software was used for data analysis. Measurement data conforming to normal distribution were expressed as mean ± standard deviation ( ), and inter-group comparison was performed using t-test; data not conforming to normal distribution were expressed as median (interquartile range) [M (Q1, Q3)], and inter-group comparison was performed using Wilcoxon rank-sum test. Categorical data were expressed as count (percentage) [n (%)], and inter-group comparison was performed using χ2-test. Univariate analysis was used to screen potential factors influencing the compliance rates of the two core measures (head-of-bed elevation correct implementation rate and artificial airway cuff pressure compliance rate). Variables with P<0.05 in univariate analysis were included in the multivariate Logistic regression model to identify independent influencing factors for head-of-bed elevation correct implementation rate ≥90% and artificial airway cuff pressure compliance rate ≥90%, respectively. Spearman correlation analysis was used to explore the correlation between the compliance rates of the two measures and VAP incidence. The sample size included all eligible patients admitted to the EICU and RICU during the study periods. A P<0.05 was considered statistically significant.
), and inter-group comparison was performed using t-test; data not conforming to normal distribution were expressed as median (interquartile range) [M (Q1, Q3)], and inter-group comparison was performed using Wilcoxon rank-sum test. Categorical data were expressed as count (percentage) [n (%)], and inter-group comparison was performed using χ2-test. Univariate analysis was used to screen potential factors influencing the compliance rates of the two core measures (head-of-bed elevation correct implementation rate and artificial airway cuff pressure compliance rate). Variables with P<0.05 in univariate analysis were included in the multivariate Logistic regression model to identify independent influencing factors for head-of-bed elevation correct implementation rate ≥90% and artificial airway cuff pressure compliance rate ≥90%, respectively. Spearman correlation analysis was used to explore the correlation between the compliance rates of the two measures and VAP incidence. The sample size included all eligible patients admitted to the EICU and RICU during the study periods. A P<0.05 was considered statistically significant.
Results
Baseline Characteristics of Study Subjects
There were no statistically significant differences in baseline data such as gender, age, APACHEII score, mechanical ventilation duration, and type of artificial airway between the two groups (P>0.05), indicating comparability. (Table 2).
 |

Temporal Change Trends of the Compliance Rates of the Two Core Nursing Measures and the Incidence of VAP
Before the implementation, the annual average correct execution rate of head-of-bed elevation was 1751/2163 (80.95%), and the annual average compliance rate of artificial airway cuff pressure was 1705/2163 (78.84%), with both indicators below 90% throughout the year. After the implementation, the compliance rates of the two measures remained at a stable and high level: the correct execution rate of head-of-bed elevation was stable at 91.76%~96.99% with an annual average of 2017/2142 (94.16%), and the compliance rate of artificial airway cuff pressure was stable at 90.91%~96.55% with an annual average of 2016/2142 (94.10%). The annual average values of the two indicators were significantly higher than those before the implementation (χ2=156.324, df=1, P<0.001; χ2=172.589, df=1, P<0.001). The mean incidence of VAP was 227/2163 (10.52%) before the implementation and 83/2142 (3.87%) after the implementation, with a statistically significant difference between the two groups (χ2=43.986, df=1, P<0.001, OR=0.342, 95% CI: 0.263–0.445) (Figure 3).
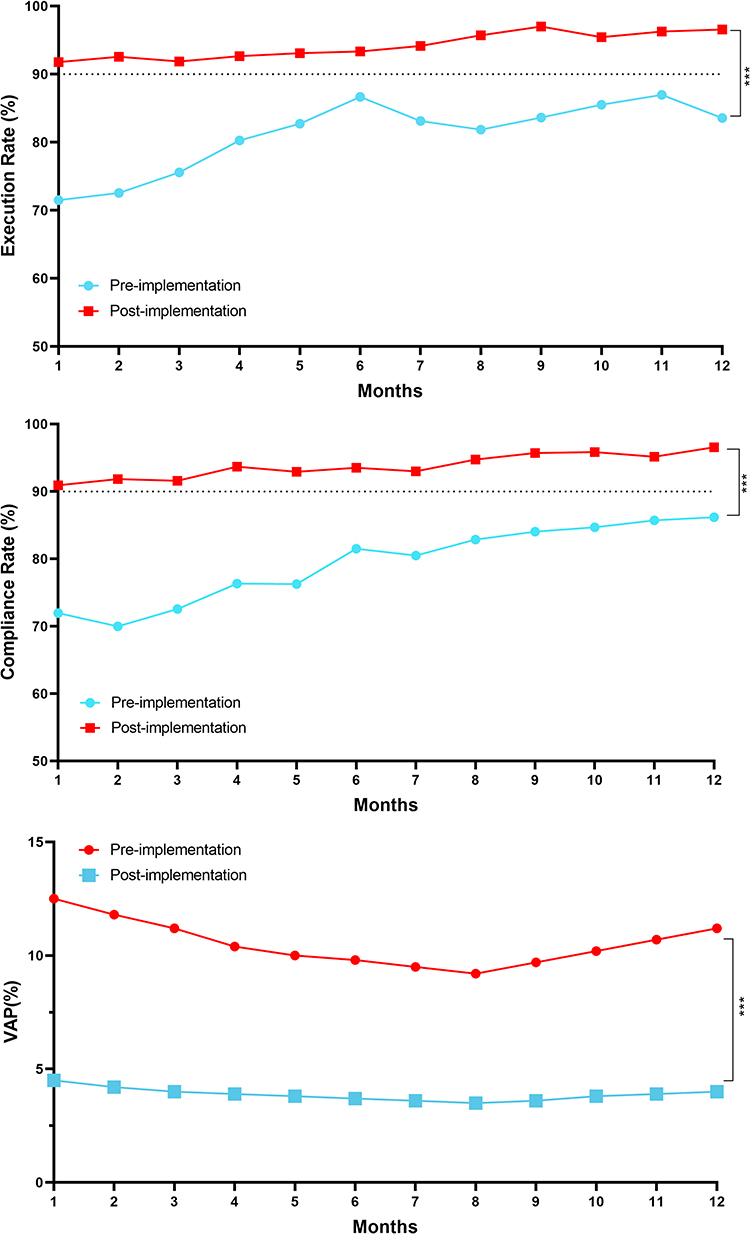 |
Figure 3 Line chart of the correct execution rate of head-of-bed elevation, cuff pressure compliance rate and VAP incidence from January to December 2024 (pre-implementation) and 2025 (post-implementation). Abbreviation: VAP, ventilator-associated pneumonia. |
Correlation Between the Compliance Rates of the Two Core Nursing Measures and the Incidence of VAP
Spearman correlation analysis showed that the correct execution rate of head-of-bed elevation was significantly negatively correlated with the incidence of VAP (r=−0.782, P<0.001), and the compliance rate of artificial airway cuff pressure was also significantly negatively correlated with the incidence of VAP (r=−0.765, P<0.001), indicating that the higher the compliance rates of the two measures, the lower the incidence of VAP (Figure 4).
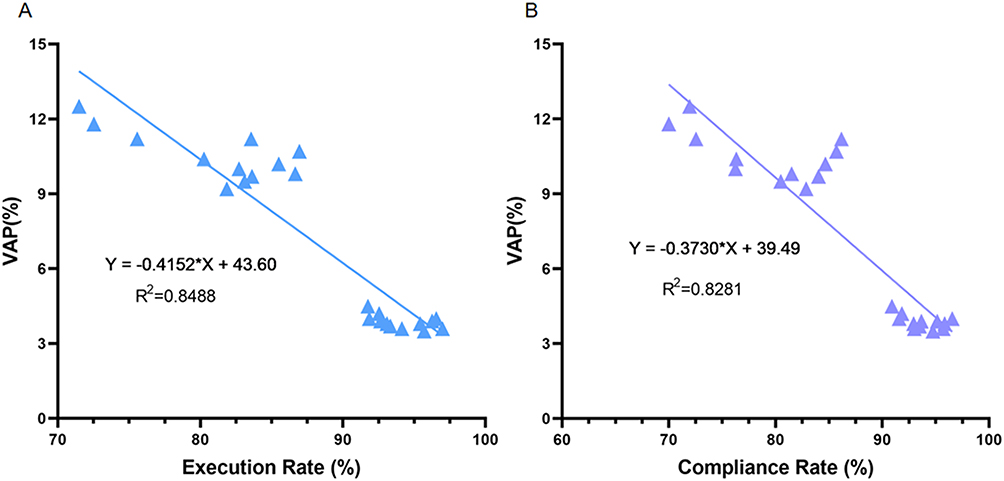 |
Figure 4 Scatter plots of the correlation between (A) head-of-bed elevation correct execution rate and VAP incidence, and (B) cuff pressure compliance rate and VAP incidence from January to December 2024 (pre-implementation) and 2025 (post-implementation). Abbreviation: VAP, ventilator-associated pneumonia. |
Factors Influencing the Combined Compliance Rate of the Two Core Nursing Measures
Univariate Analysis
With the correct implementation rate of head-of-bed elevation and cuff pressure compliance rate ≥90% as the dependent variables respectively, univariate analysis results showed that APACHE II score, duration of mechanical ventilation, patient agitation and delirium, type of artificial airway, implementation of standardized procedures, conduct of quality monitoring and nursing staffing were significantly correlated with the correct implementation rate of head-of-bed elevation (P<0.05), while age had no significant effect on it (P>0.05). APACHE II score, duration of mechanical ventilation, patient agitation and delirium, implementation of standardized procedures, conduct of quality monitoring and nursing staffing were significantly correlated with the cuff pressure compliance rate (P<0.05), while age and type of artificial airway had no significant effect on it (P>0.05) (Tables 3 and 4).
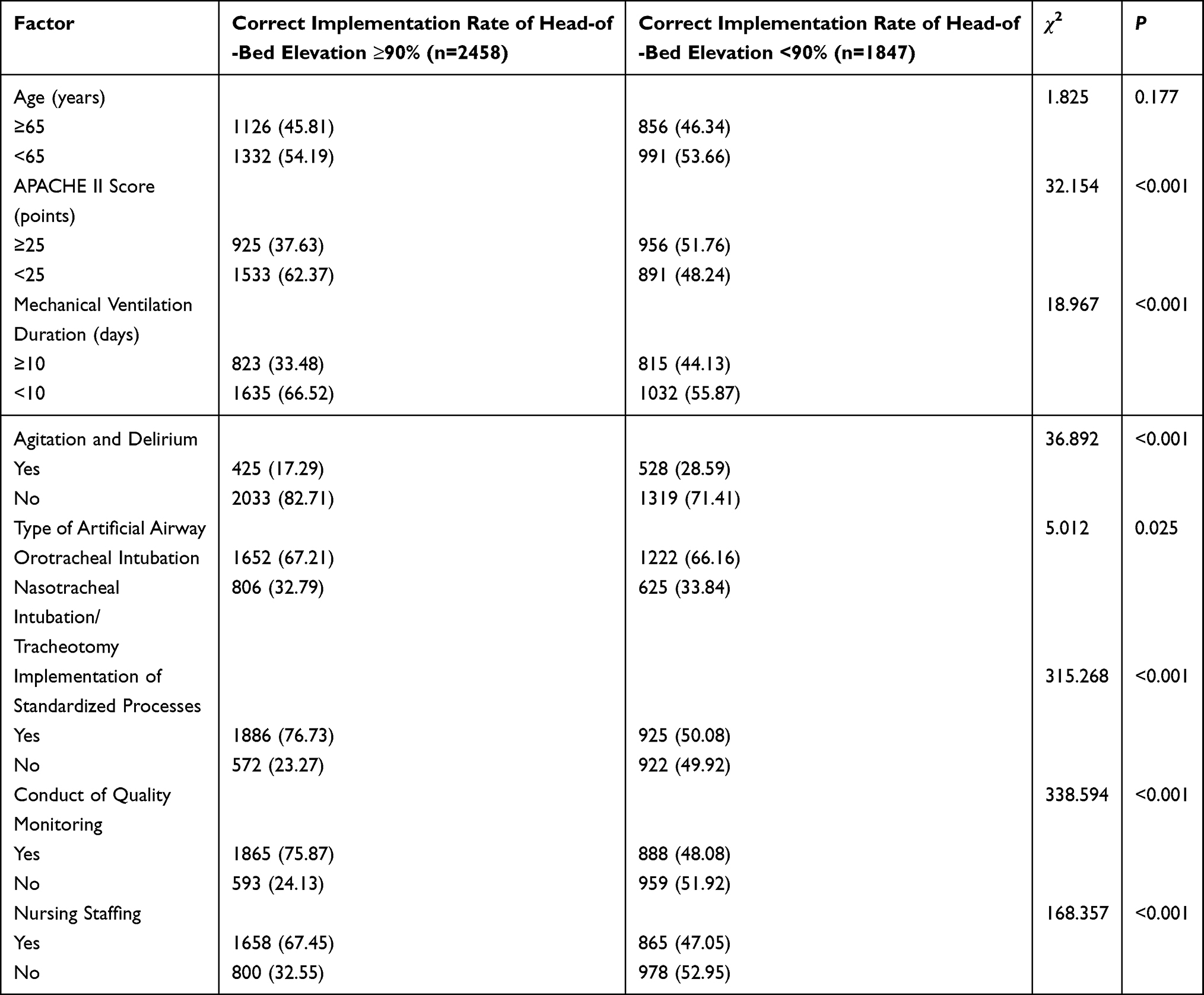 |
Table 3 Univariate Analysis of Influencing Factors for the Correct Implementation Rate of Head-of-Bed Elevation [n (%)] |
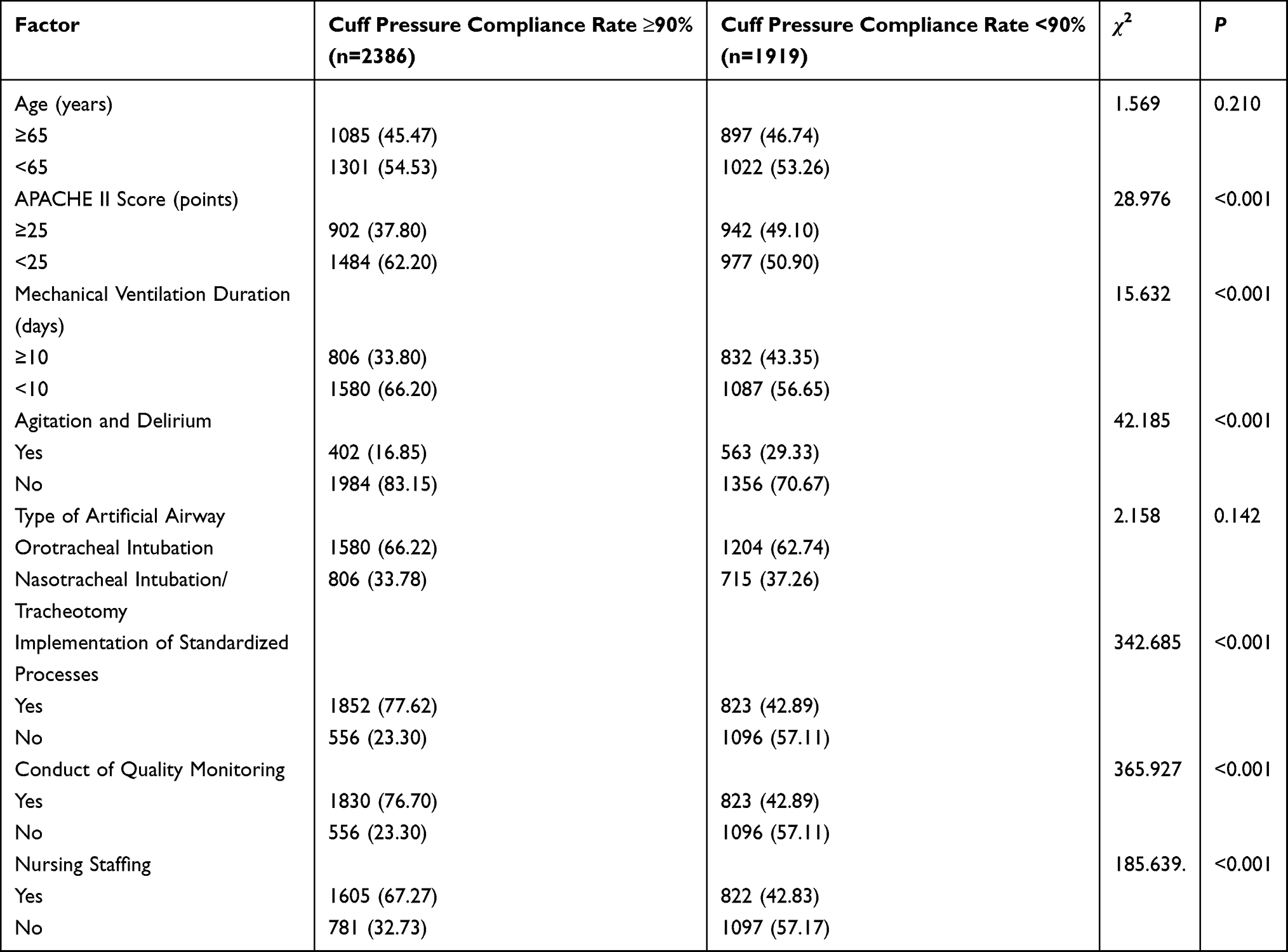 |
Table 4 Univariate Analysis of Influencing Factors for the Cuff Pressure Compliance Rate [n (%)] |
Multivariate Logistic Regression Analysis
Variables with P<0.05 in univariate analysis were included in the multivariate Logistic regression model. The results showed that APACHEII score ≥25 points (OR=1.331, 95% CI: 1.165–1.520, Wald χ2=16.258, df=1, P<0.001; OR=1.367, 95% CI: 1.201–1.557, Wald χ2=20.587, df=1, P<0.001), duration of mechanical ventilation ≥10 days (OR=1.295, 95% CI: 1.128–1.487, Wald χ2=12.587, df=1, P<0.001; OR=1.316, 95% CI: 1.152–1.503, Wald χ2=15.126, df=1, P<0.001), patient agitation and delirium (OR=1.445, 95% CI: 1.238–1.688, Wald χ2=20.169, df=1, P<0.001; OR=1.510, 95% CI: 1.305–1.748, Wald χ2=27.895, df=1, P<0.001), and insufficient nursing staffing (OR=2.191, 95% CI: 1.920–2.505, Wald χ2=124.896, df=1, P<0.001; OR=2.285, 95% CI: 2.005–2.612, Wald χ2=146.985, df=1, P<0.001) were independent risk factors for reducing the correct implementation rate of head-of-bed elevation and the cuff pressure compliance rate; the implementation of standardized procedures (OR=0.324, 95% CI: 0.282–0.372, Wald χ2=238.569, df=1, P<0.001; OR=0.311, 95% CI: 0.271–0.357, Wald χ2=279.658, df=1, P<0.001) and the conduct of quality monitoring (OR=0.319, 95% CI: 0.276–0.368, Wald χ2=233.897, df=1, P<0.001; OR=0.306, 95% CI: 0.267–0.351, Wald χ2=269.357, df=1, P<0.001) were independent protective factors for improving the correct implementation rate of head-of-bed elevation and the cuff pressure compliance rate, and the type of artificial airway was not an independent influencing factor (P>0.05) (Tables 5 and 6).
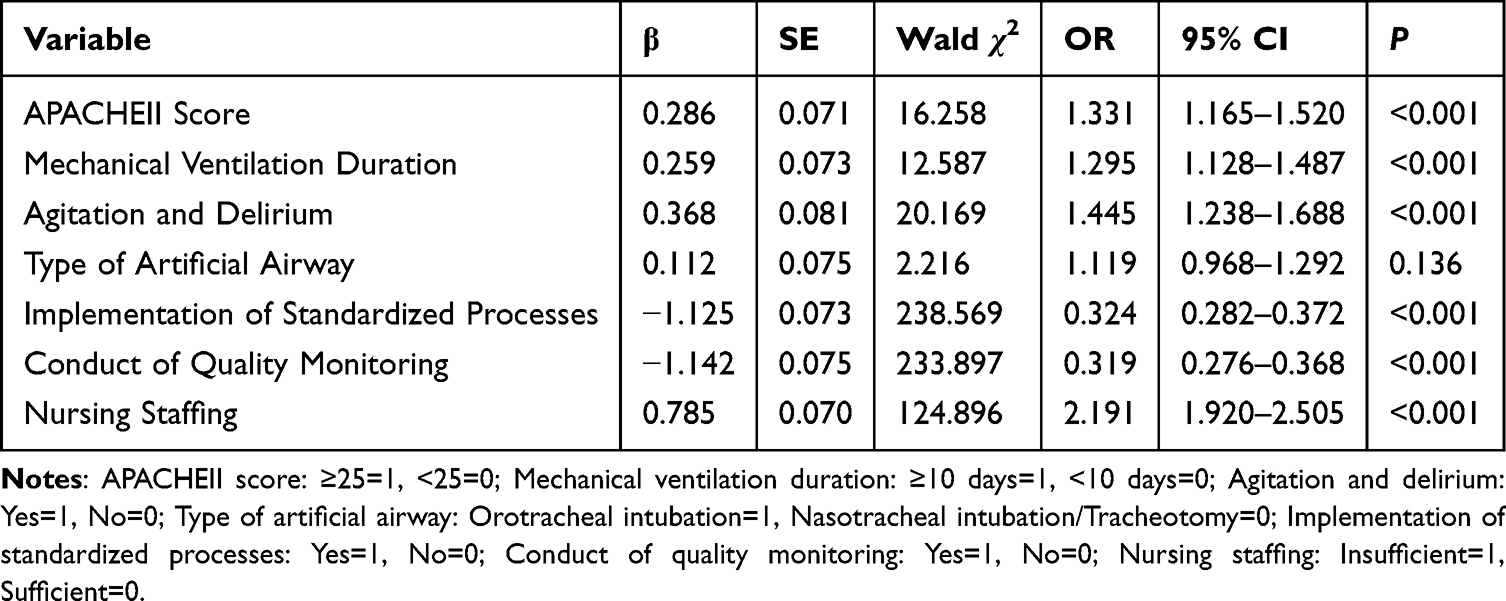 |
Table 5 Multivariate Logistic Regression Analysis of Influencing Factors for the Correct Implementation Rate of Head-of-Bed Elevation |
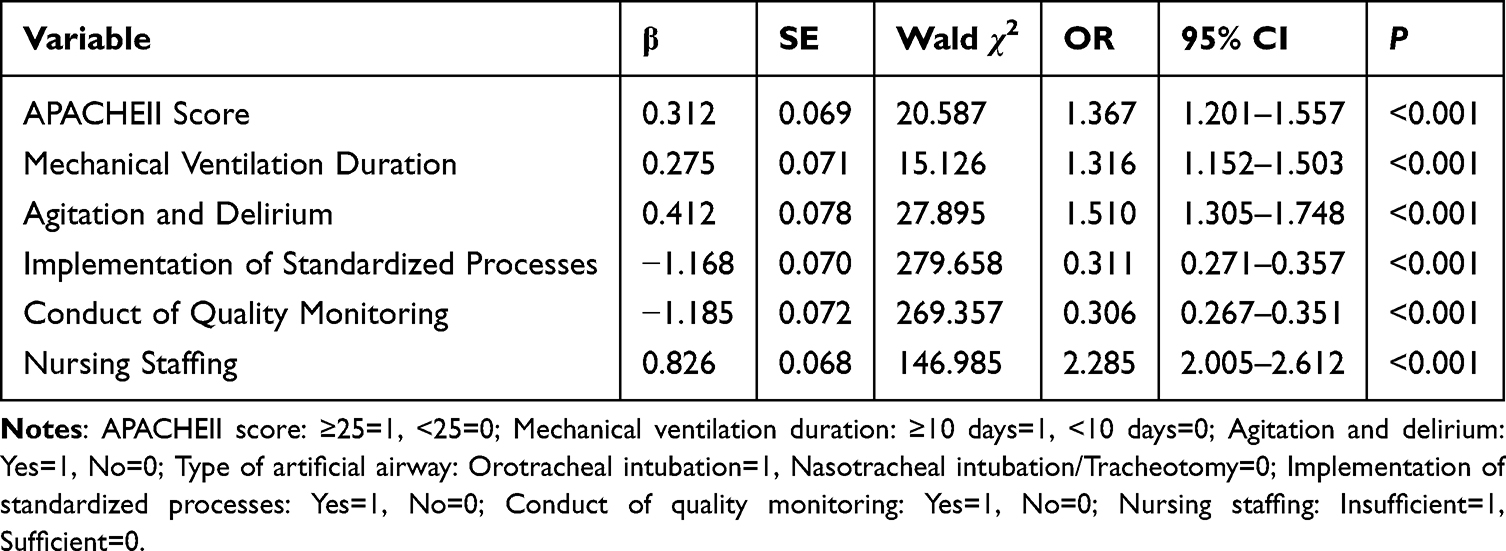 |
Table 6 Multivariate Logistic Regression Analysis of Influencing Factors for the Artificial Airway Cuff Pressure Compliance Rate |
Discussion
This study used the PDSA cycle as a quality improvement tool and implemented full-process improved plans for the existing problems in the management of head-of-bed elevation and artificial airway cuff pressure in our hospital’s EICU and RICU, achieving significant improvements in the compliance rates of the two core VAP preventive measures and a substantial decrease in the incidence of VAP. The results showed that after the implementation of the intervention, the compliance rates of both head-of-bed elevation and cuff pressure increased significantly and remained at a stable high level, while the incidence of VAP decreased markedly. These findings support the potential application value of the PDSA cycle in the continuous improvement of nursing quality, consistent with the conclusion of the systematic review by Martinez-Reviejo et al2 that structured quality improvement strategies can enhance the implementation effect of VAP preventive measures.
From the perspective of the management optimization of the two core indicators, artificial airway cuff pressure management is a weak link in clinical VAP prevention and control. A survey of 194 tertiary hospital ICUs in China found that only 58% of departments could maintain a cuff pressure compliance rate of over 80%, with a manual pressure measurement error rate of up to 15%.6 In contrast, this study standardized the use of precision manual cuff pressure gauges and eliminated subjective finger palpation, stabilizing the cuff pressure compliance rate at a high level. In addition, a systematic review by Mastrogianni et al17 pointed out that the effect of nursing bundle interventions depends on “process operability”. This study refined the guideline-recommended monitoring every 6–8 hours to monitoring every 4–8 hours + re-measurement during shift handover and specified specific time points, transforming abstract guideline requirements into actionable behavioral norms for nurses. This optimization addresses the shortcoming of vague processes in previous bundle interventions and provides key support for improving measure adherence.
Multivariate Logistic regression analysis showed that APACHE II score ≥25 points, duration of mechanical ventilation ≥10 days, patient agitation and delirium, and insufficient nursing staffing were the common independent risk factors for reducing the compliance rates of the two indicators, which was consistent with clinical practice. Critically ill patients with an APACHE II score ≥25 points are often accompanied by multiple organ dysfunction. Postural adjustment of head-of-bed elevation may cause hemodynamic fluctuations, and the operation of cuff pressure monitoring may also interfere with the stability of patients’ vital signs. Nurses tend to prioritize “maintaining the stability of vital signs” over “implementing preventive measures” in the trade-off, which is consistent with the research conclusion of Wang et al5 It also suggests that clinical individualized indicator implementation plans should be formulated for critically ill patients to implement standardized operations as much as possible on the premise of ensuring the stability of vital signs. For patients with mechanical ventilation duration ≥10 days, nurses tend to shift their work focus to dominant indicators such as airway humidification and infection control due to the “nursing fatigue effect”, while basic preventive measures such as head-of-bed elevation and cuff pressure monitoring are easily ignored.18 Güner et al4 also reported a negative correlation between the duration of mechanical ventilation and the correct implementation rate of head-of-bed elevation, confirming that the implementation of basic nursing measures for patients with long-term mechanical ventilation needs to strengthen special quality control. Patient agitation and delirium were another important risk factor, consistent with the findings reported in previous studies.19 This is because agitation not only makes it difficult to maintain the position of head-of-bed elevation, but also causes displacement of the cuff pipeline and interruption of pressure measurement operations, and even the measured pressure value deviates from the real level due to the patient’s struggle. It suggests that clinical timely sedation, physical restraint and other intervention measures should be taken for patients with agitation and delirium to ensure the standardized implementation of the two indicators.20 Consistent with the findings of this study, international research has also identified insufficient nursing staffing as a major barrier to high-quality VAP prevention care.21 Because patients in the ICU have severe conditions and high nursing needs, when staffing is insufficient, nurses tend to choose time-saving and subjective operations to replace standardized operations. This result is highly consistent with the conclusion of Shao et al6 that staffing shortage reduces the cuff pressure compliance rate by 15%–20%, suggesting that the quality improvement of ICU VAP prevention and control cannot only focus on the measures themselves, but also needs to be supported by a dynamic staffing allocation plan based on the severity of patients’ conditions, rather than a fixed “nurse-patient ratio” standard. Only by dynamically adjusting staffing according to the patients’ disease grading and the difficulty of nursing operations can the implementation of basic nursing measures be fundamentally guaranteed, which provides a new thinking direction for the optimization of nursing management.7 It is important to note that while the present study demonstrates the significant impact of compliance with these core care processes on VAP incidence, patient prognosis is determined not only by nursing practices but also by the patient’s underlying physiological status. In this context, bedside, easily applicable parameters such as the Shock Index (SI), Modified Shock Index (MSI), and Age Shock Index (ASI) have been shown to be significant predictors of mortality in critically ill patients and can provide valuable guidance for clinical decision-making.22 Integrating these physiological indicators into routine risk assessment alongside process compliance monitoring may help identify high-risk patients more accurately and implement targeted interventions to improve overall patient outcomes.
At the same time, this study clarified that the implementation of standardized procedures and the conduct of quality monitoring are the common independent protective factors for improving the compliance rates of the two indicators (all OR values < 0.325), and the protective effect on the cuff pressure compliance rate is slightly higher than that on the head-of-bed elevation. The reason is that the operation standardization of cuff pressure monitoring is higher, and procedure consolidation and quality monitoring can more directly reduce subjective operation errors, while the implementation of head-of-bed elevation is slightly interfered by individual factors such as patients’ postural tolerance and bed unit environment. This difference provides a basis for formulating targeted clinical optimization strategies: for the implementation of head-of-bed elevation, an individualized postural assessment link can be added, and the elevation angle can be adjusted and effectively fixed according to the patient’s condition and body shape to reduce postural deviation; for cuff pressure management, procedure consolidation and regular equipment calibration can be further strengthened, the frequency of pressure gauge calibration can be increased, and standby pressure measurement equipment can be configured to continuously improve the accuracy of monitoring.8 In addition, univariate analysis showed that the type of artificial airway was correlated with the correct implementation rate of head-of-bed elevation, but this effect was offset by other strong factors in multivariate analysis, confirming that the type of artificial airway is not an independent influencing factor of the two indicators. It suggests that there is no need to formulate differentiated implementation standards according to the type of artificial airway in clinical practice, and standardized management requirements can be uniformly implemented to reduce the complexity of nursing operations and improve the compliance of measure implementation.23
Spearman correlation analysis accurately quantified the correlation between the two core indicators and the incidence of VAP, confirming that both the correct implementation rate of head-of-bed elevation and the compliance rate of artificial airway cuff pressure are significantly and strongly negatively correlated with the incidence of VAP, that is, the incidence of VAP will decrease by a corresponding margin for every 1 percentage point increase in the compliance rates of the two indicators, which clarifies the core value of the two indicators in VAP prevention and control. From the perspective of pathophysiological mechanism, the two indicators achieve the synergistic effect of VAP prevention from two dimensions of upstream block and airway barrier: head-of-bed elevation at 30°–45° reduces gastroesophageal reflux and microaspiration, reducing the risk of oropharyngeal colonizing bacteria invading the lower respiratory tract from the source,24 maintaining the cuff pressure at 25~30 cmH2O effectively seals the airway and prevents secretions above the cuff from falling into the lungs.25 Both are core measures to block the key pathogenesis of VAP, and their standardized implementation is an important foundation for reducing the incidence of VAP. Mastrogianni et al17 pointed out that VAP prevention bundle measures can significantly reduce the infection rate, but did not clarify the prevention and control value of a single core indicator. This study focused on two core indicators strongly recommended by guidelines and confirmed that improving their compliance rates through the PDSA cycle can achieve a substantial decrease in the incidence of VAP. This finding has important practical implications for resource-limited settings: prioritizing these two easily implementable, cost-effective core indicators through standardized, continuous management may represent a pragmatic starting point to reduce VAP risk, particularly when resources are insufficient to implement full comprehensive bundles. It is critical to emphasize that these data support the independent value of these two indicators, but do not negate the potential benefits of more comprehensive VAP prevention bundles in settings where they can be fully implemented and sustained.26,27
Compared with previous studies,9,28 the innovations of this study are mainly reflected in three aspects: first, a full-process quality improvement plan for the two core indicators was formed with the PDSA cycle as a tool, forming a closed-loop management from root cause analysis and measure implementation to effect monitoring and long-term consolidation, which provides a replicable and operable practical path for clinical promotion and application; second, it uses 2-year complete time-series data to show the dynamic variation trends of measure compliance rates, indicating that the implementation difficulties of different measures vary and targeted optimization of intervention strategies is needed; third, it quantifies the interaction between patient-level and nursing-level factors through multivariate analysis, providing empirical evidence for formulating individualized and systematic quality improvement plans in clinical practice.
Limitations
This study has several important limitations that should be acknowledged. First, it was a single-center before-after observational study, which is vulnerable to temporal confounding factors such as secular trends in clinical practice, infection control strategies, staffing changes and case mix variations that may have contributed to the observed outcomes independently of the PDSA intervention. Second, the intervention was multicomponent, making it impossible to determine which specific component drove the observed improvements in compliance and VAP incidence. Third, important clinical variables such as sedation level, enteral nutrition practices and antibiotic use were not included in the analysis, which may have introduced residual confounding. Fourth, formal interrupted time series analysis was not performed, which would have provided a more robust evaluation of the system-level intervention. Finally, the long-term sustainability of the intervention beyond 2025 was not tracked. In the future, multi-center and prospective studies are needed to further verify the conclusions of this study and include more confounding factors for analysis to provide more comprehensive empirical evidence for VAP prevention and control.
Conclusion
PDSA cycle-based comprehensive quality improvement measures including standardized monitoring procedures, standardized measuring tools and continuous quality control were associated with improved compliance rates of head-of-bed elevation and artificial airway cuff pressure in mechanically ventilated patients, maintained the two indicators at a stable high level, and lower VAP incidence. Patient agitation and delirium, insufficient nursing staffing, high APACHE II score and long duration of mechanical ventilation are the main risk factors affecting the compliance rates of the two measures, while the implementation of standardized procedures and continuous quality control are important protective factors. Both the correct implementation rate of head-of-bed elevation and the compliance rate of artificial airway cuff pressure are significantly and strongly negatively correlated with the incidence of VAP. Strengthening the standardized implementation of these two core indicators has important clinical significance for improving patient prognosis, enhancing nursing quality and reducing medical burdens.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon request.
Ethics Approval and Consent to Participate
This study was a quality improvement before-after study using the PDSA cycle. It was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of The Affiliated Hospital of Southwest Medical University (Approval No.: KY2025694). A waiver of informed consent was granted. A waiver of informed consent was granted because this was a retrospective study using de-identified electronic medical record data that did not involve any direct intervention with patients or alteration of standard clinical care. All patient data were stored in a password-protected electronic system with access restricted only to the research team, and all identifying information was removed prior to analysis to ensure patient confidentiality.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was not funded by any organization.
Disclosure
The authors declared that they have no conflicts of interest regarding this work.
References
1. Goodfellow LT, Miller AG, Varekojis SM, LaVita CJ, Glogowski JT, Hess DR. AARC clinical practice guideline: patient-ventilator assessment. Respiratory Care. 2024;69(8):1042–16. doi:10.4187/respcare.12007
2. Martinez-Reviejo R, Tejada S, Jansson M, et al. Prevention of ventilator-associated pneumonia through care bundles: a systematic review and meta-analysis. J Intensive Med. 2023;3(4):352–364. doi:10.1016/j.jointm.2023.04.004
3. Rosenthal VD, Memish ZA, Bearman G. Preventing ventilator-associated pneumonia: a position paper of the international society for infectious diseases, 2024 update. Int J Infect Dis. 2025;151:107305. doi:10.1016/j.ijid.2024.107305
4. Güner CK, Kutlutürkan S. Role of head-of-bed elevation in preventing ventilator-associated pneumonia bed elevation and pneumonia. Nurs Crit Care. 2022;27(5):635–645. doi:10.1111/nicc.12633
5. Wang S, Lu M, Xu Y, Wang S, Wei L. [Study on mechanical ventilation pressure under continuous cuff pressure monitoring in critical patients]. Zhonghua wei Zhong Bing Ji Jiu Yi xue. 2020;32(10):1257–1259. doi:10.3760/cma.j.cn121430-20200714-00523
6. Xin S, Xia W, Chenxia L, et al. Investigation and analysis of nursing prevention and control of ventilator-associated pneumonia in ICUs of 194 tertiary hospitals. Chin J Nurs. 2023;2617–2623.
7. Bankanie V, Outwater AH, Wan L, Yinglan L. Assessment of knowledge and compliance to evidence-based guidelines for VAP prevention among ICU nurses in Tanzania. BMC Nurs. 2021;20(1):209. doi:10.1186/s12912-021-00735-8
8. Al-Harthi F, Al-Noumani H, Matua GA, Al-Abri H, Joseph A. Nurses’ compliance to ventilator-associated pneumonia prevention bundle and its effect on patient outcomes in intensive care units. Nurs Crit Care. 2025;30(3):e70043. doi:10.1111/nicc.70043
9. Giang BTH, Matsubara C, Okamoto T, et al. The development of a 10-item ventilator-associated pneumonia care bundle in the general intensive care unit of a tertiary hospital in Vietnam: lessons learned. Healthcare. 2025;13(5). doi:10.3390/healthcare13050443
10. Miron M, Blaj M, Ristescu AI, et al. Hospital-acquired pneumonia and ventilator-associated pneumonia: a literature review. Microorganisms. 2024;12(1):213. doi:10.3390/microorganisms12010213
11. Sharma J, Mohanty S. Ventilator-associated pneumonia: a persistent menace in the ICU. Indian J Crit Care Med. 2025;29(4):285–286. doi:10.5005/jp-journals-10071-24945
12. Sangani D, Krupadev V, Crawford M, Deere B, Hendel R. A quality improvement initiative for increasing cardiac rehabilitation referrals using plan-do-study-act (PDSA) methodology. Am J Med. 2022;135(4):512–516. doi:10.1016/j.amjmed.2021.10.027
13. Shebrain S, Cookenmaster C, Ajine M, et al. The plan-do-study-act (PDSA): an iterative approach to optimize residents performance in the American board of surgery in-training exam (ABSITE). J Surg Educ. 2024;81(10):1452–1461. doi:10.1016/j.jsurg.2024.06.022
14. Baandrup L, Dons AM, Bartholdy KV, Holm KO, Hageman I. Changing prescribing practice for rapid tranquillization-a quality improvement project based on the plan-do-study-act method. Soc Psychiatr Psychiatric Epidemiol. 2024;59(5):781–788. doi:10.1007/s00127-023-02461-9
15. Ohta R, Kato K, Sano C. Improving pneumococcal vaccination coverage among older adults in a rural hospital: a plan-do-study-act (PDSA)-based quality improvement project. Cureus. 2025;17(11):e97353. doi:10.7759/cureus.97353
16. Shi Y, Huang Y, Zhang TT, et al. Chinese guidelines for the diagnosis and treatment of hospital-acquired pneumonia and ventilator-associated pneumonia in adults (2018 Edition). J Thoracic Dis. 2019;11(6):2581–2616. doi:10.21037/jtd.2019.06.09
17. Mastrogianni M, Katsoulas T, Galanis P, Korompeli A, Myrianthefs P. The impact of care bundles on ventilator-associated pneumonia (VAP) prevention in adult ICUs: a systematic review. Antibiotics. 2023;12(2). doi:10.3390/antibiotics12020227
18. Arumugam Y, Arulappan J, Nandakumar SM. Impact of modified ventilator-associated pneumonia prevention bundle on clinical parameters and outcomes among mechanically ventilated patients: an interventional study. Nurs Crit Care. 2026;31(1):e70265. doi:10.1111/nicc.70265
19. Prieto-Alvarado DE, Parada-Gereda HM, Molano D, Martinez YL, Tafurt GPR, Masclans JR. Risk factors and outcomes of ventilator-associated pneumonia in patients with traumatic brain injury: a systematic review and meta-analysis. J Crit Care. 2025;85:154922. doi:10.1016/j.jcrc.2024.154922
20. Moltrasio M, Sacco A, Corrada E, et al. Agitation and delirium in intensive cardiac care unit. A multicenter prospective registry. Eur Heart J. 2020;41(Supplement_2). doi:10.1093/ehjci/ehaa946.1834
21. Nemet M, Gmehlin CG, Vukoja M, Dong Y, Gajic O, Tekin A. Ventilator-associated pneumonia in low- and middle-income vs high-income countries: the role of ventilator bundle, ventilation practices, and health care staffing. Chest. 2025;167(6):1628–1638. doi:10.1016/j.chest.2025.01.002
22. Uluç KJKÜSBD. Prognostic value of shock index, modified shock index, and age shock index in patients with sepsis in the intensive care unit. 2024.
23. Tan JH, Che CC, Tang LY, Chong MC. Predictors of self-reported practice in ventilator-associated pneumonia (VAP) prevention among critical care nurses in Sarawak public hospitals. PLoS One. 2025;20(12):e0325637. doi:10.1371/journal.pone.0325637
24. Albarqouni L, Moynihan R, Clark J, Scott AM, Duggan A, Del Mar C. Head of bed elevation to relieve gastroesophageal reflux symptoms: a systematic review. BMC Family Pract. 2021;22(1):24. doi:10.1186/s12875-021-01369-0
25. Maertens B, Lin F, Chen Y, Rello J, Lathyris D, Blot S. Effectiveness of continuous cuff pressure control in preventing ventilator-associated pneumonia: a systematic review and meta-analysis of randomized controlled trials. Crit Care Med. 2022;50(10):1430–1439. doi:10.1097/ccm.0000000000005630
26. Jin J, Zou Q, Liu H, Zeng F, Chu Y, Chen X. [Design and application of intelligent management system of artificial airway airbag pressure in intensive care]. Zhongguo Yi Liao Qi Xie Za Zhi. 2021;45(6):645–649. doi:10.3969/j.issn.1671-7104.2021.06.012
27. Lian C, Zhang J, Wang P, Mao W. Impact of head-of-bed elevation angle on the development of pressure ulcers and pneumonia in patients on mechanical ventilation: a systematic review and meta-analysis. BMC Pulm Med. 2024;24(1):462. doi:10.1186/s12890-024-03270-9
28. Ait Hssain A, Vahedian-Azimi A, Ibrahim AS, Hassan IF, Azoulay E, Darmon M. Incidence, risk factors and outcomes of nosocomial infection in adult patients supported by extracorporeal membrane oxygenation: a systematic review and meta-analysis. Crit Care. 2024;28(1):158. doi:10.1186/s13054-024-04946-8
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.