")
Back to Journals » Journal of Pain Research » Volume 16
Impact of Patient Subgroups on the Efficacy and Safety of Methylnaltrexone for Opioid-Induced Constipation in Patients with Advanced Illness
Authors Mehta N, Slatkin NE, Israel RJ, Stambler N , Shah ED
Received 2 May 2023
Accepted for publication 25 September 2023
Published 20 October 2023 Volume 2023:16 Pages 3529—3543
DOI https://doi.org/10.2147/JPR.S416307
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Neel Mehta,1,* Neal E Slatkin,2,3,* Robert J Israel,4,* Nancy Stambler,5,* Eric D Shah6,*
1Department of Anesthesiology, Weill Cornell School of Medicine, New York, NY, USA; 2School of Medicine, University of California Riverside, Riverside, CA, USA; 3Medical Affairs, Salix Pharmaceuticals, Bridgewater, NJ, USA; 4Clinical and Medical Affairs, Bausch Health US LLC, Bridgewater, NJ, USA; 5Clinical Research, Progenics Pharmaceuticals, a Subsidiary of Lantheus Holdings Inc, North Billerica, MA, USA; 6Division of Gastroenterology and Hepatology, University of Michigan, Michigan Medicine, Ann Arbor, MI, USA
*These authors contributed equally to this work
Correspondence: Eric D Shah, Division of Gastroenterology and Hepatology, University of Michigan | Michigan Medicine, 300 N Ingalls Street, Ann Arbor, MI, 48109, USA, Tel +1 877 285-7788, Email [email protected]
Purpose: We evaluated the impact of baseline patient characteristics on safety and efficacy of methylnaltrexone, a peripherally acting μ-opioid receptor antagonist, in patients with advanced illness with opioid-induced constipation (OIC).
Patients and Methods: This analysis pooled data from 2 randomized, double-blind, placebo-controlled studies (study 302: NCT00402038; study 4000: NCT00672477) in patients with advanced illness, including cancer, and OIC. Patients were randomized to receive subcutaneous methylnaltrexone (study 302: 0.15 mg/kg; study 4000: 8 or 12 mg based on weight) or placebo every other day for 2 weeks. The proportions of patients achieving rescue-free laxation within 4 or 24 hours after the first dose of study drug were assessed in patient subgroups stratified by baseline age, Eastern Cooperative Oncology Group (ECOG) performance status, cancer status, laxative type, and opioid requirement. Treatment-emergent adverse events (TEAEs) were evaluated.
Results: Overall, 363 patients were included in this analysis (methylnaltrexone, 178; placebo, 185). Mean (SD) age was 66.3 (13.7) years and 48.5% were men overall. A significantly greater proportion of patients receiving methylnaltrexone versus placebo achieved rescue-free laxation within 4 hours (111/178 [62.4%] vs 31/185 [16.8%]; P< 0.0001) and 24 hours (135/178 [75.8%] vs 81/185 [43.8%]; P< 0.0001) of the first dose. These trends were consistent across all subgroups. Most patients experienced ≥ 1 TEAE in the overall population (methylnaltrexone, 82.1%; placebo, 76.2%), which remained consistent when stratified by baseline characteristics. More than half of TEAEs were gastrointestinal in nature. Abdominal pain was more common in patients receiving methylnaltrexone than placebo across baseline characteristic subgroups.
Conclusion: Methylnaltrexone treatment was superior to placebo in achieving rescue-free laxation within 4 and 24 hours after the first dose, irrespective of patients’ cancer status, baseline ECOG performance status, or baseline opioid or laxative use. The methylnaltrexone safety profile remained consistent across baseline characteristic subgroups.
Keywords: methylnaltrexone, opioid-induced constipation, μ-opioid receptor antagonist
Introduction
Opioid-induced constipation (OIC) is a condition associated with abdominal discomfort and pain and is a common adverse event of opioid use.1–3 Patients often develop tolerance to other side effects of opioid use, such as nausea and vomiting, but some patients do not develop tolerance to constipation with opioid use.4 Additionally, OIC is associated with disruption of opioid therapy when patients skip or discontinue opioid doses, longer duration of opioid therapy, greater use of healthcare resources, and higher healthcare costs.5 Therefore, an effective treatment is important for alleviating the burden of OIC.
OIC is believed to occur because of opioid binding to peripheral μ-opioid receptors in the gastrointestinal tract, leading to abnormal modulation of mucosal secretion and fluid absorption.1 Peripherally acting μ-opioid receptor antagonists (PAMORAs) block µ-opioid receptors in the gastrointestinal tract. PAMORAs have limited ability to cross the blood–brain barrier, thereby reversing μ-opioid binding in the gut without compromising the effects of opioid analgesia.1,6
Methylnaltrexone is a PAMORA approved for the treatment of OIC in adults with chronic noncancer pain, including patients with chronic pain related to previous cancer or its treatment who do not require frequent (eg, weekly) opioid dosage escalation, and for the treatment of OIC in adults with advanced illness or pain caused by active cancer who require opioid dosage escalation for palliative care.7 Pivotal clinical trials in patients with serious and advanced illnesses demonstrated the superior efficacy of methylnaltrexone over placebo in achieving rescue-free laxation responses within 4 and 24 hours after the first dose and within 4 hours after ≥2 of the first 4 doses.8,9 Whether certain patient characteristics, such as age and cancer status, influence the likelihood that a patient will respond to methylnaltrexone remains unknown. Using pooled data from 2 pivotal methylnaltrexone trials, we conducted a post hoc analysis to evaluate whether baseline patient characteristics impact safety, tolerability, and efficacy of methylnaltrexone among patients with advanced illness and OIC.
Methods
Study Design
This was a post hoc analysis of pooled data from 2 multicenter, double-blind, randomized, placebo-controlled clinical trials of methylnaltrexone, including the phase 3 302 (NCT00402038) study and the phase 4 4000 study (NCT00672477) (Figure 1).9,10 In study 302, patients were randomized 1:1 to receive subcutaneous injections of methylnaltrexone 0.15 mg/kg or placebo every other day (QOD) for 14 days, with the opportunity to increase the dose to 0.30 mg/kg on day 9 in patients with <3 rescue-free laxations at the discretion of the investigator.9 After completion of the double-blind treatment period, patients could enroll in the 3-month open-label extension phase, in which they could receive methylnaltrexone as needed up to every 24 hours. Study 4000 included patients randomized 1:1 to receive subcutaneous methylnaltrexone 8 mg or 12 mg for patients weighing 38 kg to <62 kg or ≥62 kg, respectively, or placebo administered QOD for a maximum of 7 doses/14 days, with the option to enroll in a 10-week open-label extension portion.10 The 2 studies were approved by either a central or a local institutional review board and followed Good Clinical Practice and Declaration of Helsinki principles. Each patient provided written informed consent before enrollment in the studies.
 |
Figure 1 Study design. Abbreviations: d, day; QOD, every other day; R, randomization. |
Study Population
In both studies, eligible patients were aged ≥18 years with a diagnosis of advanced illness, which was defined as terminal disease incurable cancer or other end-stage diseases with a life expectancy of ≥1 month. Patients were receiving opioids routinely for discomfort or pain management for ≥2 weeks and taking a stable regimen of opioids (defined as no reduction in opioid dose of ≥50%) and laxatives for ≥3 days before the first dose. OIC was defined as either <3 bowel movements during the previous week and no clinically significant laxation in the 24 hours before the first dose of study drug or no clinically significant laxation within 48 hours before the first dose of study drug.
Exclusion Criteria
Key exclusion criteria included history of methylnaltrexone treatment, any disease process suggestive of mechanical bowel obstruction, an indwelling peritoneal catheter, clinically active diverticular disease, evidence of fecal impaction, peritonitis, acute surgical abdomen, any potential nonopioid cause of bowel dysfunction (in the opinion of the investigator), body weight <38 kg, and history of fecal ostomy.
Assessments
Efficacy assessments in both studies included the proportion of patients achieving rescue-free laxation within 4 or 24 hours after the first dose of study drug or within 4 hours of ≥2 of the first 4 doses and median time to rescue-free laxation within 4 or 24 hours after the first dose. Rescue-free laxation was defined as a bowel movement without use of any rescue medication or procedure within 4 hours before the bowel movement. In the current analysis, outcomes were assessed in patient subgroups stratified by baseline age (<65 vs ≥65), cancer status, Eastern Cooperative Oncology Group (ECOG) performance status (≤2 vs >2), opioid requirement (oral morphine equivalent dose <80 mg/day, 80 to <150 mg/day, and ≥150 mg/day), and laxative type (osmotic agents, stimulants, or stool softeners). Patients could receive more than one type of laxative. The ECOG performance status scale is a measure of a patient’s functioning with scores ranging from 0 (fully active, able to carry on all predisease performance without restriction) to 5 (dead).11 Data were collected from patient diaries in study 4000 and electronic health records in both studies. Treatment-emergent adverse events (TEAEs), gastrointestinal TEAEs, and abdominal pain were evaluated at all postbaseline visits in the pooled population and in the patient subgroups defined by age, cancer status, ECOG performance status, opioid requirement, and laxative type.
Statistical Analysis
Efficacy analyses for both studies were performed on the intention-to-treat population, defined as patients who received ≥1 dose of study medication. Response rates for patients achieving rescue-free laxation within 4 and 24 hours were compared across treatment groups using the Cochran-Mantel-Haenszel test, and P-values based on chi-squared tests were generated to compare placebo and methylnaltrexone. Time to rescue-free laxation was estimated using Kaplan–Meier methods and compared using Log rank tests. Nominal levels of significance were set at P<0.05, with no adjustments for multiplicity. Safety analyses were performed on the safety population, which consisted of patients who received ≥1 dose of study medication and 1 patient who received methylnaltrexone in an unblinded fashion and was included only in the safety analyses. TEAEs were described for each treatment group using summary statistics.
Results
Baseline Characteristics
A total of 364 patients received ≥1 dose of study medication. One patient received methylnaltrexone in an unblinded fashion and was included only in the safety analysis. Thus, the pooled efficacy analyses included 363 patients (methylnaltrexone, 178; placebo, 185). Overall, patients had a mean age of 66.3 years, 48.5% were men, and approximately two-thirds had a cancer diagnosis; most patients had an ECOG performance status score ≥2. The mean oral morphine equivalent dose was 374.5 mg/day, and almost all patients were taking ≥1 laxative at baseline. Demographic and clinical characteristics were similar between the methylnaltrexone and placebo groups (Table 1).
 |
Table 1 Patient Demographic and Baseline Characteristics (Intention-to-Treat Population) |
Efficacy
A significantly greater proportion of patients receiving the first dose of methylnaltrexone versus placebo achieved rescue-free laxation within 4 hours (111/178 [62.4%] vs 31/185 [16.8%]; P<0.0001) and 24 hours (135/178 [75.8%] vs 81/185 [43.8%]; P<0.0001). This pattern was consistent across patient subgroups stratified by baseline age, cancer status, ECOG performance status, opioid requirement, and laxative type (Figure 2A and B). Additionally, a significantly greater proportion of patients treated with methylnaltrexone versus placebo achieved rescue-free laxation within 4 hours of ≥2 of the first 4 doses across all subgroups (methylnaltrexone, 52.4%–69.2%; placebo, 4.1%–14.3%; P<0.001 for all) (Figure 2C).
 |
Figure 2 Rescue-free laxation (A) within 4 hours after the first dose, (B) within 24 hours after the first dose, and (C) within 4 hours of ≥2 of the first 4 doses by patient subgroups. Intention-to-treat population. Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; RFL, rescue-free laxation. Note: P-values based on chi-squared test. |
Overall median time to rescue-free laxation for the 4-hour interval was 1.1 hours for methylnaltrexone and >4 hours for placebo (P<0.0001). For the 24-hour interval, median time to rescue-free laxation was 1.1 hours for methylnaltrexone and 23.6 hours for placebo (P<0.0001). Median time to rescue-free laxation was significantly shorter (P<0.05) with methylnaltrexone than with placebo for both the 4-hour and 24-hour intervals regardless of baseline age, cancer status, ECOG performance status, OED, and laxative type (Table 2).
 |
Table 2 Median Time to Rescue-Free Laxation Within 4 Hours and 24 Hours of First Dose (Intention-to-Treat Population) |
Safety
Most of the patients in both treatment groups (methylnaltrexone, 82.1%; placebo, 76.2%) experienced ≥1 TEAEs, which were mostly gastrointestinal (eg, abdominal pain, nausea, flatulence) (Table 3). The overall incidence of TEAEs was similar between methylnaltrexone and placebo and generally similar across subgroups, although patients who had a cancer diagnosis had a slightly higher incidence of TEAEs than those without cancer (Figure 3). The most common TEAEs were gastrointestinal (including nausea, abdominal pain, and flatulence) and were reported in 38.0–62.4% of patients receiving methylnaltrexone or placebo across subgroups (Figure 4A). Abdominal pain was more common in patients receiving methylnaltrexone than placebo across subgroups (methylnaltrexone, 15.8%–29.5%; placebo, 8.8–14.6%) (Figure 4B).
 |
Table 3 Treatment-Emergent Adverse Events Occurring in ≥5% of Patients in Placebo and Methylnaltrexone Treatment Groups (Safety Population) |
 |
Figure 3 Overall incidence of TEAEs by patient subgroups. Safety population. Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; TEAE, treatment-emergent adverse event. |
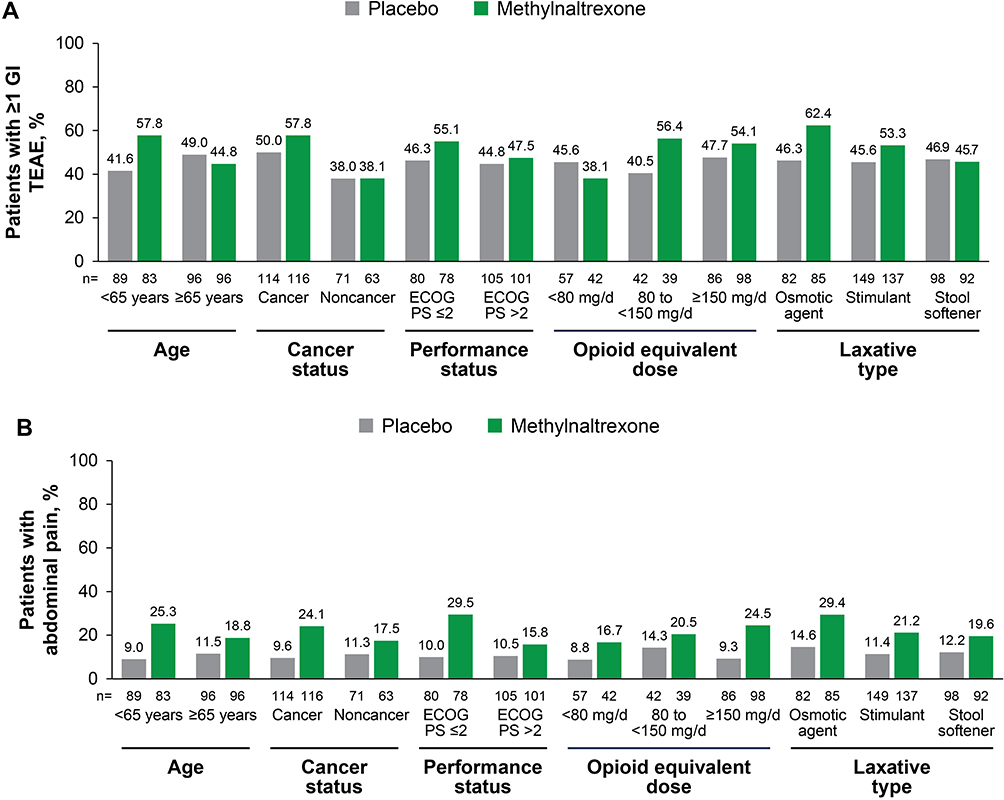 |
Figure 4 Incidence of (A) GI TEAEs and (B) TEAEs of abdominal pain by patient subgroups. Safety population. Abbreviations: ECOG PS, Eastern Cooperative Oncology Group performance status; GI, gastrointestinal; TEAE, treatment-emergent adverse event. |
Patient Disposition
A total of 82/364 (22.5%) patients discontinued the studies. The most common reasons for discontinuation included adverse events (methylnaltrexone, 6.7%; placebo, 5.4%), death (methylnaltrexone, 6.7%; placebo, 8.1%), and patient withdrawal (methylnaltrexone, 2.8%; placebo, 4.3%). The vast majority (48/51) of the deaths in the 2 studies were attributed to underlying illness (previously described).9,10 Some variation in patient disposition was seen when stratified by patient baseline characteristic subgroups, including age, cancer status, ECOG performance status, opioid requirement, and laxative type (Table 4). Discontinuations tended to be higher in patients who were aged <65 years (vs ≥65 years), in patients with cancer (vs without cancer), and in patients with higher opioid equivalent doses (OEDs; vs lower doses).
 |
Table 4 Patient Disposition Stratified by Baseline Parameters (Safety Population) |
Discussion
To our knowledge, this is the first evaluation to demonstrate the safety and efficacy of methylnaltrexone for the treatment of OIC in patients with advanced illness who are receiving palliative care across patient characteristics, including age, cancer status, ECOG performance status, opioid requirement, and concurrent laxative use. Methylnaltrexone was significantly more effective than placebo in achieving rescue-free laxation within 4 and 24 hours of the first dose and within 4 hours of ≥2 of the first 4 doses, irrespective of baseline patient characteristics. Time to rescue-free laxation was also significantly faster with methylnaltrexone compared to placebo and was generally similar across subgroups. Methylnaltrexone was generally well tolerated, with the most common TEAEs being gastrointestinal, which may be a consequence of restored laxation. The safety profile was similar to that in prior studies of methylnaltrexone.8–10,12 Rates of abdominal pain were higher with methylnaltrexone versus placebo across all subgroups. Abdominal pain associated with methylnaltrexone treatment has previously been reported to typically be mild to moderate in severity and to correspond with a laxation response to treatment.13 The incidence of abdominal pain usually decreases with subsequent methylnaltrexone dosing.13
The elderly are more prone to constipation due to a variety of factors, such as use of opioids for chronic pain and having a sedentary lifestyle, and are at greater risk of developing complications from constipation.14 Our study showed that age did not affect the efficacy of methylnaltrexone. The overall rates of TEAEs were also similar between age categories (<65 years versus ≥65 years). Likewise, there has been no observed difference in the effectiveness or safety of the PAMORA naloxegol between older and younger patients.15 Rates of discontinuations were somewhat higher in younger patients. This finding is not uncommon, and it has been postulated that this is due to greater disease severity and greater awareness of their health status in older patients.16
Opioid analgesics are often prescribed for the management of moderate-to-severe pain in patients with cancer.17,18 Other approaches to treat constipation, such as lifestyle modification and some types of laxatives, are often not practical for patients with cancer with OIC.19 Additionally, these approaches may be less effective because the underlying opioid receptor–mediated mechanism remains untargeted.18,20,21 This is exemplified by the fact that patients in these studies met eligibility criteria despite the use of multiple laxatives. However, constipation in patients with cancer is often multifactorial and may arise from several sources in addition to opioid use.19 Thus, patients with cancer may respond to PAMORA treatment differently than those with noncancer pain. As has been described previously, rates of rescue-free laxation were similar in patients with and without cancer who were receiving methylnaltrexone.22 This analysis also showed that rates of rescue-free laxation with methylnaltrexone were similar between patients with lower (better) and higher (worse) ECOG performance status scores, although there was a slight numerical trend toward higher response rates in patients with lower scores. Overall, rates of TEAEs and rates of gastrointestinal TEAEs were somewhat higher in patients with cancer than those without but similar between patients treated with methylnaltrexone and placebo. Unexpectedly, patients with ECOG performance status scores ≤2 receiving methylnaltrexone also tended to have higher rates of overall TEAEs, gastrointestinal TEAEs, and abdominal pain than those receiving placebo and those with ECOG performance status scores >2. It is unclear why this may be.
The efficacy of methylnaltrexone did not appear to vary with baseline treatment. Significant treatment differences in the achievement of rescue-free laxation in favor of methylnaltrexone versus placebo were observed across all baseline opioid dose ranges, although there was a trend toward increased rates of rescue-free laxation with increasing OED. Rates of TEAEs were mostly similar between methylnaltrexone and placebo groups across dose ranges. However, patients in the methylnaltrexone 80 to <150 mg/day category showed slightly higher rates of overall TEAEs and gastrointestinal TEAEs than those in the same dose category receiving placebo. Achievement of rescue-free laxation was highly consistent across types of laxatives used at baseline. Slightly higher incidences of overall TEAEs and gastrointestinal TEAEs were seen in patients using osmotic laxatives who received methylnaltrexone versus placebo, but rates of TEAEs were consistent between treatment groups for patients using stimulants and stool softeners.
Taken together, these results can help inform the decision to treat patients with methylnaltrexone. The findings of this study support the use of methylnaltrexone to manage OIC even in patients with factors that can complicate treatment such as greater age and cancer. This study also indicates that the efficacy of methylnaltrexone is not impacted by the type of laxative previously used. Based on these findings, methylnaltrexone can be used in a wide variety of patient populations, and factors of age, cancer status, opioid dose, and prior type of laxative used are not expected to affect the efficacy or safety of methylnaltrexone.
There are several limitations to this analysis due to its post hoc nature. Importantly, the two studies pooled in this analysis were not initially designed to compare outcomes for these subgroups of patients stratified by baseline characteristics and statistical comparisons were not made. In addition, the trials were of short duration; however, this was a necessity due to the nature of the patients’ advanced illness. Given that this was a patient population with advanced illness, the underlying disease may have significantly affected the occurrence of TEAEs.
Conclusion
Overall, methylnaltrexone treatment was superior to placebo for achievement of rescue-free laxation, irrespective of patients’ cancer status, baseline ECOG performance status, or baseline opioid or laxative use. Methylnaltrexone remained consistently safe across different baseline clinical and demographic characteristics with abdominal discomfort being the most likely adverse event. These findings demonstrate that methylnaltrexone provides effective, tolerable, and safe relief of OIC in patients with advanced illness regardless of baseline demographic or clinical characteristics, therefore supporting methylnaltrexone as a valuable treatment in patients with OIC.
Abbreviations
ECOG, Eastern Cooperative Oncology Group; OED, opioid equivalent dose; OIC, opioid-induced constipation; PAMORA, peripherally acting μ-opioid receptor antagonists; QOD, every other day; TEAE, treatment-emergent adverse event.
Study 302
Schulman Associates Institutional Review Board, Cincinnati, Ohio, USA
Research Ethics Board, McGill University Health Centre, Montreal, Quebec, Canada
University of British Columbia, British Columbia Cancer Agency Research Ethics Board, Vancouver, British Columbia, Canada
San Diego Hospice IRB, San Diego Hospice, San Diego, California, USA
University of Utah Institutional Review Board, University of Utah Health Sciences Center, Salt Lake City, Utah, USA
Henry Ford Health System Institutional Review Board, Henry Ford Health System, Detroit, Michigan, USA
Human Subjects Protection Office, The Penn State University/Milton S Hershey Medical Center, Hershey, Pennsylvania, USA
City of Hope IRB, City of Hope, Duarte, California, USA
Study 4000
Schulman Associates Institutional Review Board, Cincinnati, Ohio, USA
The University of Texas IRB, M.D. Anderson Cancer Center, Houston, Texas, USA
Division of Research Integrity & Compliance, Moffitt Cancer Center, Tampa, Florida, USA
Fox Chase Cancer Centre Institutional Review Board, Fox Chase Cancer Centre, Rockledge, Pennsylvania, USA
Regonala Etikprövningsnämnden i Linköping, Palliative Unit Vrinnevi Hospital, Linköping, Sweden
Ethics Committee CEIC, CSUB Ciutat Sanitaria Universitaria Bellvitge, Spain
Bellberry Limited, Dulwich, South Australia, Australia
Azienda Sanitaria Locale di Asti - ASL AT Sede, Asti, Italy
Comitato Etico Dell`Azienda Ospedaliera Guido Salvini di Garbagnate Milanese, Milan, Italy
Comitato Etico Indipendente Della Fondazione IRCCS Istituto Nazionale dei Tumori di Milano, Milan, Italy
St Vincent’s Hospital Human Research Ethics Committee (HREC), St Vincent’s Hospital, Darlinghurst, New South Wales, Australia
Ethik-Kommission an der Medizinischen Fakultät Technischen Hochschule Aachen, University of Aachen, Aachen, Germany
Ethik-Kommission bei der Medizinischen Fakultät der Ludwig-Maximilians Universität München, Munich, Germany
The Peter Mac Ethics Committee, Peter MacCallum Cancer Center, East Melbourne, Victoria, Australia
CIUSSS Research Ethics Board, The Jewish General Hospital, Montreal, Quebec, Canada
Bannatyne Campus Research Ethics Board, University of Manitoba, Winnipeg, Manitoba, Canada
Ethics Committee Research Leuven, UZ Leuven, Leuven, Belgium
Comité de Protection des Personnes – Sud Est V, Centre Hospitalier Universitaire de Grenoble, Grenoble, France
Hamilton Health Sciences, Hamilton, Ontario, Canada
London – Central MREC, London, United Kingdom
CHUQ Research Ethics Committee, Centre Hospitalier Universitaire de Quebec, Quebec City, Quebec, Canada
Western Institutional Review Board, Olympia, Washington, USA
Comitê de ética em Pesquisa em seres Humanos da Fundação Antônio Prudente, A.C. Camargo Cancer Center, São Paulo, Brazil
University of Utah Institutional Review Board, University of Utah Health Sciences Center, Salt Lake City, Utah, USA
Alberta Cancer Research Ethics Committee, University of Alberta, Edmonton, Alberta, Canada
Comité Bioético para la Investigación Clínica, Mexico City, Mexico
VA New Jersey Healthcare System Institutional Review Board, VA New Jersey Healthcare System, East Orange, New Jersey, USA
Data Sharing Statement
The datasets generated and/or analyzed during the current study are not publicly available at this time due to the proprietary nature of this information. Requests for additional information should be made to the corresponding author.
Ethics Approval and Informed Consent
Patients or their legally acceptable representatives provided written informed consent to participate before any study specific procedures were conducted. The specific ethical review boards that provided approval and oversight are listed above for study 302 and study 4000.
Acknowledgment
This work was supported by Salix Pharmaceuticals, a division of Bausch Health US, LLC, Bridgewater, NJ, USA, which has licensed the rights to develop and commercialize Relistor® from Progenics Pharmaceuticals, Inc., North Billerica, MA, USA, a wholly owned subsidiary of Lantheus Holdings, Inc., North Billerica, MA, USA. Progenics Pharmaceuticals had a role in the study design, implementation of the study, and data collection. Salix had a role in the data collection, data analysis, and the decision to publish. Technical editorial and medical writing assistance was provided under the direction of the authors by Drayton Hammond, PharmD, of Echelon Brand Communications, LLC, an OPEN Health company, Parsippany, NJ, USA. Funding for this assistance was provided by Salix Pharmaceuticals. The abstract of this paper was presented at the American College of Gastroenterology Annual Scientific Meeting in 2022 and the Society of Hospital Medicine Converge meeting in 2023 as a poster presentation. The poster’s abstract was published in The American Journal of Gastroenterology (https://journals.lww.com/ajg/Fulltext/2022/10002/S165_Impact_of_Patient_Subgroups_on_the_Efficacy.165.aspx) and in Journal of Hospital Medicine (https://shmpublications.onlinelibrary.wiley.com/toc/15535606/2023/18/S1).
Author Contributions
- Made a significant contribution to the work reported: conception, study design, execution, acquisition of data, analysis, and interpretation. All authors
- Have drafted or written, or substantially revised or critically reviewed the article. All authors
- Have agreed on the journal to which the article will be submitted. All authors
- Reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication, and any significant changes introduced at the proofing stage. All authors
- Agree to take responsibility and be accountable for the contents of the article. All authors
Disclosure
NM: Salix Pharmaceuticals – advisory boards. NES: Salix Pharmaceuticals – employee. RJI: Bausch Health US, LLC – employee. NS: Progenics Pharmaceuticals, Inc. – employee; Lantheus Holdings, Inc. – shareholder. EDS: Ardelyx, Mahana, Bausch Health/Salix, GI Supply/Laborie, Sanofi, Mylan – personal fees; Takeda and Neuraxis – non-financial supports, outside the submitted work.
References
1. Argoff CE. Opioid-induced constipation: a review of health-related quality of life, patient burden, practical clinical considerations, and the impact of peripherally acting μ-opioid receptor antagonists. Clin J Pain. 2020;36(9):716–722. doi:10.1097/AJP.0000000000000852
2. Johnson DA, Argoff CE. Hot topics in primary care: management of opioid-induced constipation. J Fam Pract. 2015;64(12 Suppl):S4–9.
3. Rogers E, Mehta S, Shengelia R, Reid MC. Four strategies for managing opioid-induced side effects in older adults. Clin Geriatr. 2013;21(4):1.
4. Panchal SJ, Muller-Schwefe P, Wurzelmann JI. Opioid-induced bowel dysfunction: prevalence, pathophysiology and burden. Int J Clin Pract. 2007;61(7):1181–1187. doi:10.1111/j.1742-1241.2007.01415.x
5. Iyer S, Davis KL, Candrilli S. Opioid use patterns and health care resource utilization in patients prescribed opioid therapy with and without constipation. Manag Care. 2010;19(3):44–51.
6. Crockett SD, Greer KB, Heidelbaugh JJ, Falck-Ytter Y, Hanson BJ, Sultan S. American Gastroenterological Association Institute guideline on the medical management of opioid-induced constipation. Gastroenterology. 2019;156(1):218–226. doi:10.1053/j.gastro.2018.07.016
7. Relistor (methylnaltrexone bromide) prescribing information; 2018. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/021964s019,208271s003lbl.pdf.
8. Slatkin N, Thomas J, Lipman AG, et al. Methylnaltrexone for treatment of opioid-induced constipation in advanced illness patients. J Support Oncol. 2009;7(1):39–46.
9. Thomas J, Karver S, Cooney GA, et al. Methylnaltrexone for opioid-induced constipation in advanced illness. N Engl J Med. 2008;358(22):2332–2343. doi:10.1056/NEJMoa0707377
10. Bull J, Wellman CV, Israel RJ, Barrett AC, Paterson C, Forbes WP. Fixed-dose subcutaneous methylnaltrexone in patients with advanced illness and opioid-induced constipation: results of a randomized, placebo-controlled study and open-label extension. J Palliat Med. 2015;18(7):593–600. doi:10.1089/jpm.2014.0362
11. ECOG performance status scale; 2022. Available from: https://ecog-acrin.org/resources/ecog-performance-status.
12. Michna E, Blonsky ER, Schulman S, et al. Subcutaneous methylnaltrexone for treatment of opioid-induced constipation in patients with chronic, nonmalignant pain: a randomized controlled study. J Pain. 2011;12(5):554–562. doi:10.1016/j.jpain.2010.11.008
13. Slatkin NE, Lynn R, Su C, Wang W, Israel RJ. Characterization of abdominal pain during methylnaltrexone treatment of opioid-induced constipation in advanced illness: a post hoc analysis of two clinical trials. J Pain Symptom Manage. 2011;42(5):754–760. doi:10.1016/j.jpainsymman.2011.02.015
14. Chokhavatia S, John ES, Bridgeman MB, Dixit D. Constipation in elderly patients with noncancer pain: focus on opioid-induced constipation. Drugs Aging. 2016;33(8):557–574. doi:10.1007/s40266-016-0381-2
15. Movantik (naloxegol) prescribing information. Wilmington, DE: AstraZeneca Pharmaceuticals; 2020.
16. Kim SJ, Kwon OD, Han EB, et al. Impact of number of medications and age on adherence to antihypertensive medications: a nationwide population-based study. Medicine. 2019;98(49):e17825. doi:10.1097/MD.0000000000017825
17. van den Beuken-van Everdingen MH, Hochstenbach LM, Joosten EA, Tjan-Heijnen VC, Janssen DJ. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manage. 2016;51(6):1070–1090.e1079. doi:10.1016/j.jpainsymman.2015.12.340
18. Pappagallo M. Incidence, prevalence, and management of opioid bowel dysfunction. Am J Surg. 2001;182(suppl 5A):11S–18S. doi:10.1016/S0002-9610(01)00782-6
19. Wickham RJ. Managing constipation in adults with cancer. J Adv Pract Oncol. 2017;8(2):149–161.
20. Kumar L, Barker C, Emmanuel A. Opioid-induced constipation: pathophysiology, clinical consequences, and management. Gastroenterol Res Pract. 2014;2014:1–6. doi:10.1155/2014/141737
21. Nee J, Zakari M, Sugarman MA, et al. Efficacy of treatments for opioid-induced constipation: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2018;16(10):1569–1584. doi:10.1016/j.cgh.2018.01.021
22. Chamberlain BH, Rhiner M, Slatkin NE, Stambler N, Israel RJ. Subcutaneous methylnaltrexone for treatment of opioid-induced constipation in cancer versus noncancer patients: an analysis of efficacy and safety variables from two studies. J Pain Res. 2021;14:2687–2697. doi:10.2147/JPR.S312731
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.