")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Impact of Opioid-Free Anesthesia on Postoperative Quality of Recovery in Patients After Laparoscopic Cholecystectomy-A Randomized Controlled Trial
Authors Hao C, Xu H, Du J, Zhang T, Zhang X, Zhao Z, Luan H
Received 11 September 2023
Accepted for publication 17 November 2023
Published 28 November 2023 Volume 2023:17 Pages 3539—3547
DOI https://doi.org/10.2147/DDDT.S439674
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Georgios Panos
Conghui Hao,1 Hai Xu,1 Jingjing Du,1 Tianyu Zhang,1 Xiaobao Zhang,2 Zhibin Zhao,2 Hengfei Luan2
1Department of Anesthesiology, Graduate Training Base of Lianyungang First People’s Hospital of Jinzhou Medical University, Lianyungang, Jiangsu, People’s Republic of China; 2Department of anesthesiology, The Affiliated Lianyungang Hospital of Xuzhou Medical University, The First People’s Hospital of Lianyungang, Lianyungang, Jiangsu, People’s Republic of China
Correspondence: Hengfei Luan, The Affiliated Lianyungang Hospital of Xuzhou Medical University, The First People’s Hospital of Lianyungang, No. 6 East Zhenhua Road, Lianyungang, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: Opioid analgesics may delay discharge and affect postoperative quality of recovery because of their significant adverse effects, such as hyperalgesia, postoperative nausea and vomiting (PONV), shivering and urine retention. We aimed to compare the quality of postoperative recovery (QoR) between patients undergoing laparoscopic cholecystectomy surgeries with opioid-free anesthesia (OFA) and those with opioid-based anesthesia (OA).
Patients and Methods: 80 adult patients undergoing laparoscopic cholecystectomy were randomly allocated to an opioid-free anesthesia group (Group OFA) or an opioid-based anesthesia group (Group OA). The primary outcome was the quality of postoperative recovery using QoR-15 scale on postoperative day 1 (POD 1) and 2 (POD 2). The secondary outcomes included the incidence of opioid-related adverse symptoms, perioperative hemodynamic data, duration of post-anesthesia care unit (PACU) stay and duration of extubation, and the incidences of hypotension and bradycardia.
Results: A statistically significant difference in total QoR-15 was observed between the two groups on POD 1 and POD 2 (91.00 (90.00, 92.00) vs 113.00 (108.25, 115.00), 106.00 (104.00, 112.00) vs 133.00 (130.00, 135.00), P < 0.001). The incidence of opioid-related symptoms was significantly different between the two groups on POD 1 (P < 0.05). There were between-group differences in systolic blood pressure (SBP) and diastolic blood pressure (DBP) at T3 (P < 0.001). There was also a significant difference in the incidence of hypotension between the two groups (P = 0.001). However, there were no significant differences in the duration of PACU stay, duration of extubation and the incidence of bradycardia (P > 0.05). There was no difference in heart rate between the two groups at all observed time points, either (P > 0.05).
Conclusion: We concluded that the quality of recovery of patients receiving OFA was superior to those receiving OA after laparoscopic cholecystectomy.
Keywords: opioid-free anesthesia, opioid-based anesthesia, postoperative recovery, laparoscopic cholecystectomy
Introduction
Laparoscopic cholecystectomy is an effective surgical approach for the treatment of abdominal gallbladder disorders such as cholecystitis, gallbladder stones or gallbladder polyps. Although the surgical technique for the treatment of cholecystitis with laparoscope shows some benefits compared to open surgery, postoperative complications such as abdominal incision pain, nausea and vomiting, or other complications are still challenging issues.1
To date, opioids are still used as the most potent and effective drugs to eliminate various kinds of pain in clinical practice.2 However, the widespread misuse of opioids, over-prescription or distribution without permission also leads to some kinds of perverse effects, such as hyperalgesia, nausea and vomiting, shivering, and urine retention. These side effects can result in prolonged hospitalization, increased treatment costs, prolonged return to daily activities and affect the quality of postoperative recovery for postsurgical patients.3 In recent years, with the introduction of the concept of enhanced recovery after surgery (ERAS), a new mode of perioperative analgesia strategy has been recommended, which is referred to as opioid-free anesthesia (OFA). It consists of a variety of non-opioid narcotic drugs and techniques with different mechanisms of action and different targets in the pain transduction pathways to obtain high-quality anesthesia, avoid opioid-related adverse reactions, relieve pain to the maximum extent and promote patient recovery.4 At present, OFA is increasingly promoted in clinical practice and widely used in gynecology, orthopedics and gastrointestinal laparoscopic surgeries.5 It can control postoperative pain effectively, decrease the incidence of long-term chronic pain, reduce opioid drug consumption, speed up postoperative recovery, relieve patient anxiety and shorten the length of hospital stay.6,7
Based on these considerations, we designed a prospective, randomized, single-blinded study to primarily evaluate the impact of OFA on postoperative quality of recovery as measured by the QoR-15 questionnaire on POD 1 and POD 2 after laparoscopic cholecystectomy. We aim to investigate whether OFA can promote postoperative quality of recovery, result in a lower incidence of opioid-related adverse symptoms, more stable intraoperative hemodynamic data, shorter duration of PACU stay and duration of extubation.
Materials and Methods
Participants
This prospective, randomized, single-blinded clinical study was conducted from November 2022 to August 2023, at the First People Hospital of Lianyungang, China. The study complied with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the First People’s Hospital of Lianyungang (KY-20220711001-01, on 26 Aug 2022). The study had been registered on ClinicalTrials.gov (ChiCTR2200065324). This study enrolled 84 adult patients with ASA physical status I or II, aged 20–60 years and were scheduled for laparoscopic cholecystectomy surgery. Non-inclusion criteria included: a. serious heart, lung disease and psychiatric disease. b. hypotension, bradycardia and atrioventricular block. c. allergy to study drugs. d. pregnancy, breastfeeding or menstruating women. e. BMI>30 kg/m2. Written informed consent was obtained from all patients.
Study Randomization
All patients in this study were randomly assigned to OFA group (Group OFA) or OA group (Group OA) based on a computer-generated list with a 1:1 allocation. The information regarding group assignment was hidden in sealed opaque envelopes. When the patients arrived in the operating room, the anesthesiologist opened these sequentially numbered envelopes, and the card inside determined which group the patient was placed. A specialist nurse who was not involved in the study prepared the study medication. The patients, surgeons, nurses, post-operative visitors, and the statistician were unaware of the group assignment. The attending anesthesiologist could not be blinded because of the different drug administration protocols.
Study Endpoints
The primary outcome was to evaluate the quality of recovery on POD 1 and POD 2 using the QoR-15 questionnaire for all patients. The QoR-15 questionnaire evaluates five dimensions of recovery and includes 15 items: physical comfort (5 items), emotional state (4 items), physical independence (2 items), psychological support (2 items), and pain (2 items). Each question is scored on a 10-point Likert scale ranging from 0 to 10. The sum of scores is the patient’s QoR-15 score. The total score ranged from 0 (poorest recovery quality) to 150 (best recovery quality).
The secondary outcomes included the following: the incidence of opioid-related adverse symptoms evaluated on POD 1, the opioid-related adverse symptoms include nausea, vomiting, constipation, difficulty urinating, difficulty concentrating, drowsiness or difficulty staying awake, dizziness, feeling sleepy, general fatigue or weakness, itching, dry mouth, and headache. The other outcomes included duration of PACU stay and extubation, the incidences of hypotension and bradycardia, and perioperative hemodynamic data including heart rate (HR), systolic and diastolic blood pressures (SBP, DBP) at baseline (T0), before intubation (T1), 1 min after endotracheal intubation (T2), 1 min before skin incision (T3), 1 min after skin incision (T4) and 1 min after extubation (T5).
Anesthetic Management Protocol
All patients presenting for elective cholecystectomy were identified and visited according to routine procedures by criteria for inclusion and exclusion. After arriving at the operating room, patients received routine preoperative vital sign monitoring including electrocardiogram (ECG), non-invasive blood pressure measurement (NIBP), pulse oximeter (SpO2) and body temperature. The depth of anesthesia was monitored using the bispectral index (BIS).
Pre-oxygenation was administered for 3 min before anesthesia induction. All patients received a bolus dose of IV propofol 1–2 mg/kg for the induction of general anesthesia. After confirmation of unconsciousness (BIS value < 60), absence of an eyelash reflex, and no response to verbal stimulation, a bolus dose of IV cisatracurium 0.1–0.2 mg/kg was administered, and 3 min after administering the muscle relaxant orotracheal intubation was performed using a direct laryngoscope. Additional cisatracurium was administered as needed. Group OFA received IV induction of dexmedetomidine 0.6 μg/kg for 10 min, and esketamine 0.2 mg/kg. Maintenance of anesthesia also included IV dexmedetomidine 0.5–0.7 μg/kg/h, and esketamine 0.2–0.5 mg/kg/h, which was separately adjusted in steps of 0.1μg/kg/h and 0.1 mg/kg/h to maintain SBP with ±30% of baseline. Immediately after induction of anesthesia, propofol was followed by a continuous dose of 4–8 mg/kg/h. Dexmedetomidine and esketamine infusions were stopped at the beginning of skin suturing. Group OA received sufentanil 0.3–0.5 μg/kg before the induction of general anesthesia followed by a continuous infusion of remifentanil 0.1–0.3 μg/kg/min. After induction of anesthesia, the remifentanil infusion was adjusted in increments of 0.1μg/kg/min to maintain the SBP with ±30% of the baseline. Remifentanil infusion was stopped at the end of the skin suturing.
After patients was endotracheally intubated, intraoperative mechanical ventilation in Pressure Control Volume Guaranteed Ventilation Mode (PCV-VG) was performed and the ventilation parameters were set as follows: tidal volume, 6–8 mL/kg; respiratory rate, 12–20 breaths/min; titrate sevoflurane concentrations (sevoflurane MAC 0.8–1.4) in the oxygen/air mixture (FiO2: 0.6, total gas flow: 2L/min) to maintain BIS values between 40 and 60; CO2 concentrations (PetCO2, 35–40 mmHg) and airway pressure < 30 cm H2O.
During the time from induction of anesthesia to discharge from the PACU, hypotension (defined as systolic blood pressure falling > 20% from preoperative baseline and/or systolic blood pressure < 90mmHg) was treated with 4–8 μg norepinephrine intravenously. Bradycardia (defined as heart rate falling > 20% from preoperative baseline and/or heart rate < 50bpm) was treated with 0.5mg atropine intravenously. Parecoxib 40mg via intravenous injection and acetaminophen 100mg via intravenous drip for 30 min were administered before the end of surgery. Ropivacaine was used for local infiltration anesthesia at the end of surgery. To prevent PONV, patients received azasetron 10mg at the end of surgery.
Statistical Analysis
Sample size was calculated based on previously reported values of the mean and standard deviation QoR-15 score in patients after general anesthesia and intermediate surgery (114 ± 18); an average difference of ≥ 12 in the global QoR-15 score was considered a clinically significant improvement.8 The estimated sample size was 42 participants per group with a power of 0.8, type 1 error of 0.05, and dropout rate of 10%. Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 25.0. The normality of the quantitative variables was tested using the Shapiro–Wilk test. Normally distributed data were expressed as means and standard deviations and analyzed using independent samples t-test. Skewed data were expressed as medians and interquartile ranges and analyzed using Mann–Whitney U-test. Categorical data were expressed as a number (percentage) and analyzed using Pearson’s Chi-square test. All tests were two-tailed and statistical significance was considered for P< 0.05.
Results
The details of the study cohort conduction are shown in Figure 1. Between Nov. 2022 to August 2023, 84 adult patients underwent laparoscopic cholecystectomy surgery were enrolled. Of these, 4 patients were excluded; 3 because of not meeting inclusion criteria, and 1 because of declining to participate. Among 80 patients included in this analysis, 40 received intraoperative OA anesthesia method and 40 received intraoperative OFA anesthesia method.
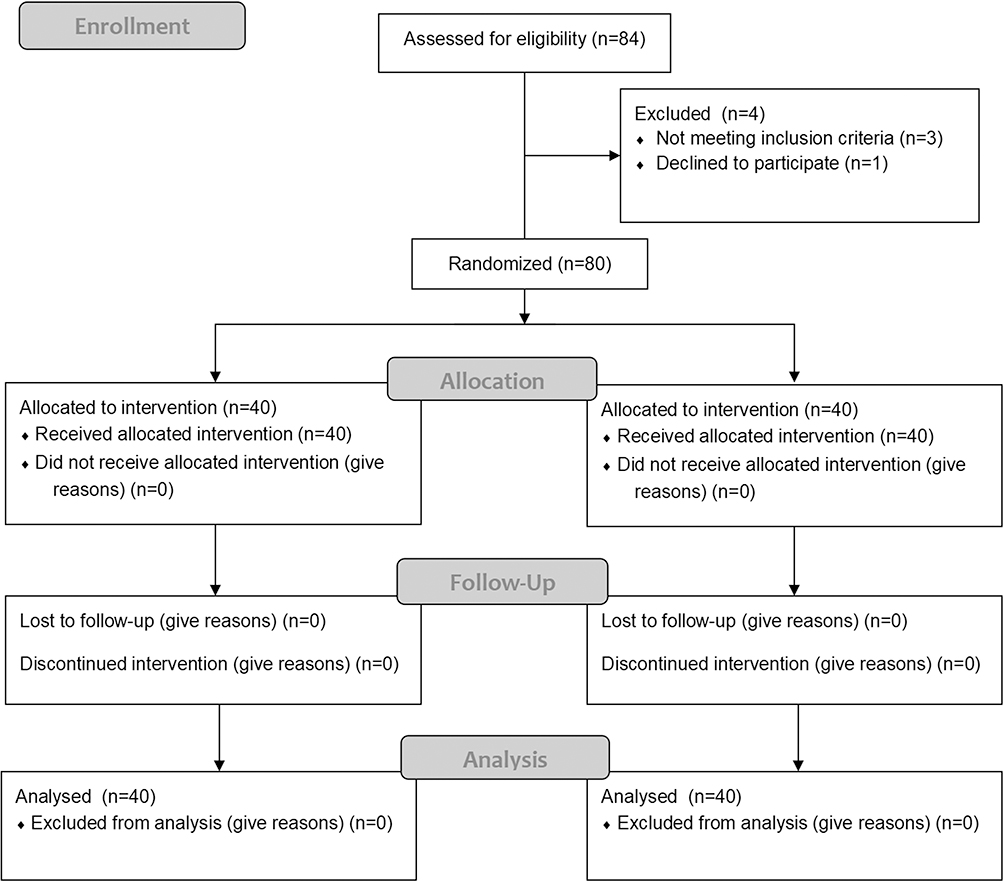 |
Figure 1 Flowchart of patient selection. |
No differences in age, gender, BMI, ASA physical status between the two groups. (Table 1).
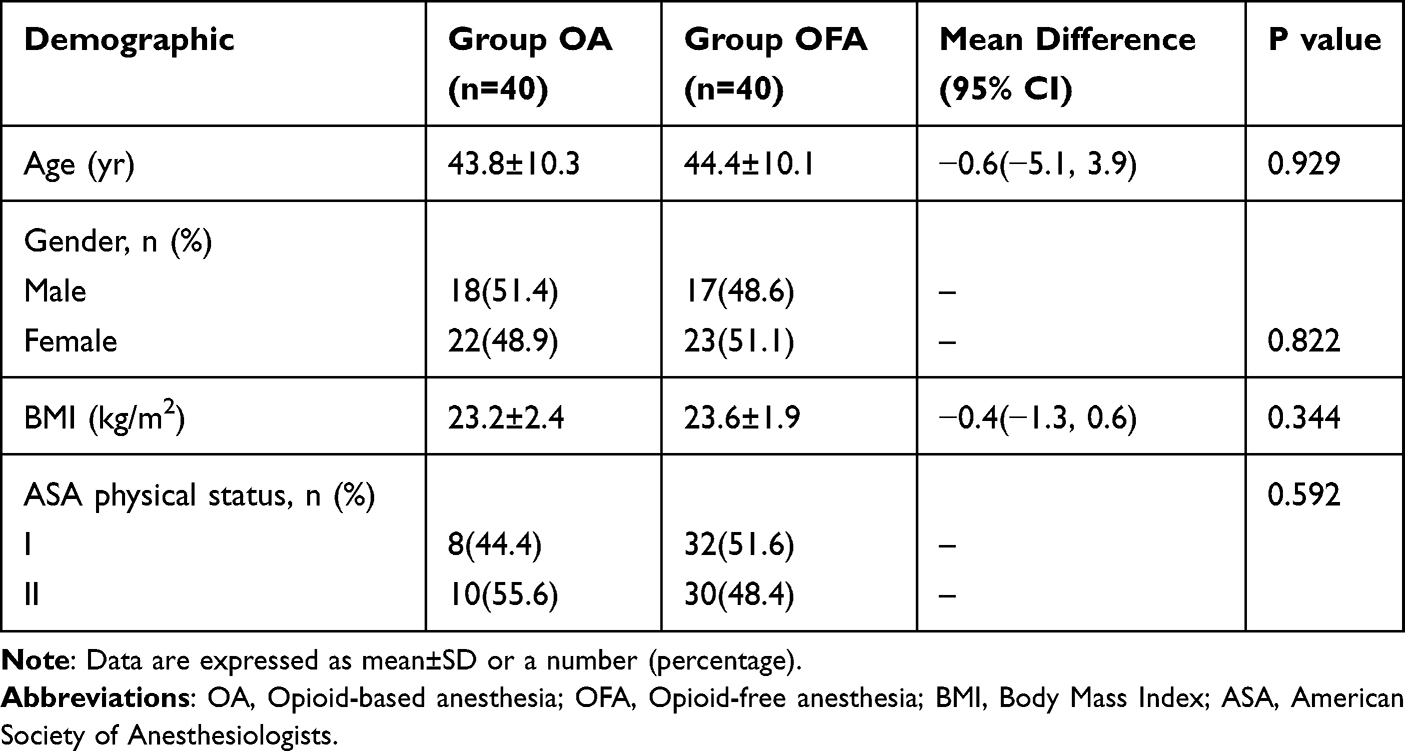 |
Table 1 Demographic Data |
There were no differences in the duration of surgery, duration of PACU stay and duration of extubation, and the incidence of bradycardia between the two groups. There was a significant difference in the incidence of hypotension (30.0% vs 2.5%) between the two groups (P = 0.001). (Table 2).
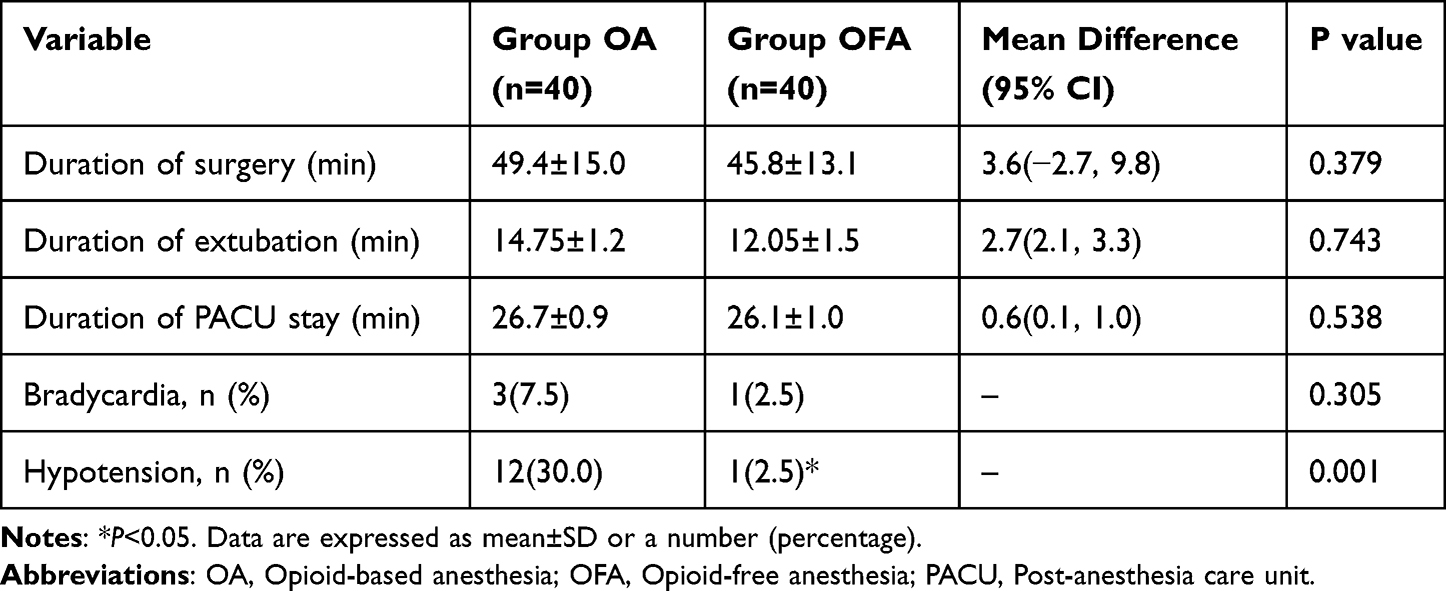 |
Table 2 Descriptive and Comparative Statistics on Perioperative Data of the Groups |
The QoR-15 score on POD 1 and POD 2 were significantly higher in Group OFA than those in Group OA (91.00 (90.00, 92.00) vs 113.00 (108.25, 115.00), 106.00 (104.00, 112.00) vs 133.00 (130.00, 135.00), P < 0.001).
All sub-scores on the QoR-15 questionnaire were significantly higher in the OFA group than those in the OA group on POD 1 (pain:12.00 (12.00, 12.00) vs 15.00 (14.00, 15.75), P < 0.001; physical comfort: 25.00 (25.00, 26.00) vs 30.00 (30.00, 32.00) P < 0.001; physical independence: 14.00 (13.00, 14.00) vs 16.00 (15.00, 16.75), P < 0.001; psychological support: 15.00 (14.00, 16.00) vs 16.00 (16.00, 17.00), P < 0.001; emotional state: 25.00 (24.00, 25.00) vs 35.00 (32.00, 37.00), P < 0.001).(Figure 2).
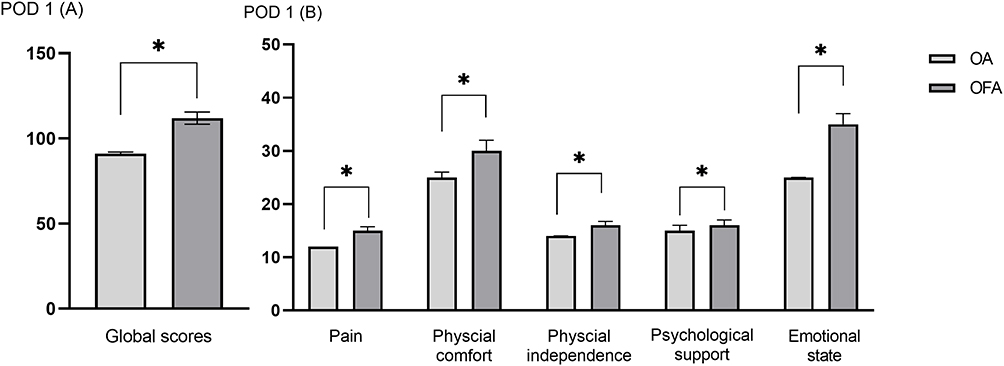 |
Figure 2 The Quality of Recovery-15 questionnaire scores obtained on postoperative day 1 (A) Global scores (B) Sub-dimension scores. *P<0.001. |
All sub-scores on the QoR-15 questionnaire were also significantly higher in Group OFA on POD 2 (pain: 12.50 (12.00, 13.00) vs 20.00 (18.25, 20.00), P < 0.001; physical comfort: 29.00 (28.00, 30.00) vs 39.00 (38.00, 39.00), P < 0.001; physical independence: 17.00 (17.00, 18.00) vs 18.00 (18.00, 18.00), P =0.001; psychological support: 19.00 (18.00, 19.00) vs 19.00 (19.00, 20.00), P =0.019; emotional state: 27.00 (26.00, 34.00) vs 38.00 (36.00, 39.00), P < 0.001). (Figure 3).
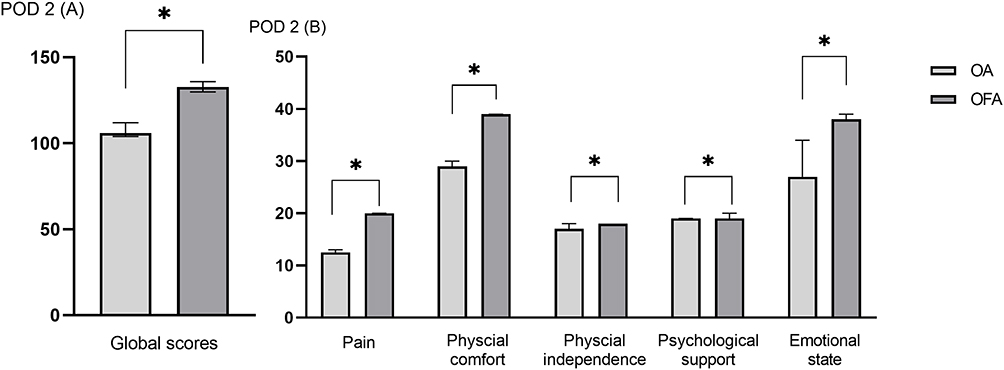 |
Figure 3 The Quality of Recovery-15 questionnaire scores obtained on postoperative day 2 (A) Global scores (B) Sub-dimension scores. *P<0.001. |
Except for constipation, difficulty passing urine, difficulty concentrating, itchiness, and feeling confused, the incidences of opioid-related adverse symptoms were significantly different between the two groups on POD 1 (P < 0.05). In terms of nausea (47.5% vs 22.5%), vomiting (42.5% vs 15.0%), drowsiness/difficulty staying awake (35.0% vs 10.0%), feeling lightheaded or dizzy (30.0% vs 10.0%), feelings of general fatigue or weakness (45.0% vs 20.0%), dry mouth (32.5% vs 20.0%) and headache (20.0% vs 5.0%) (P < 0.05). (Table 3).
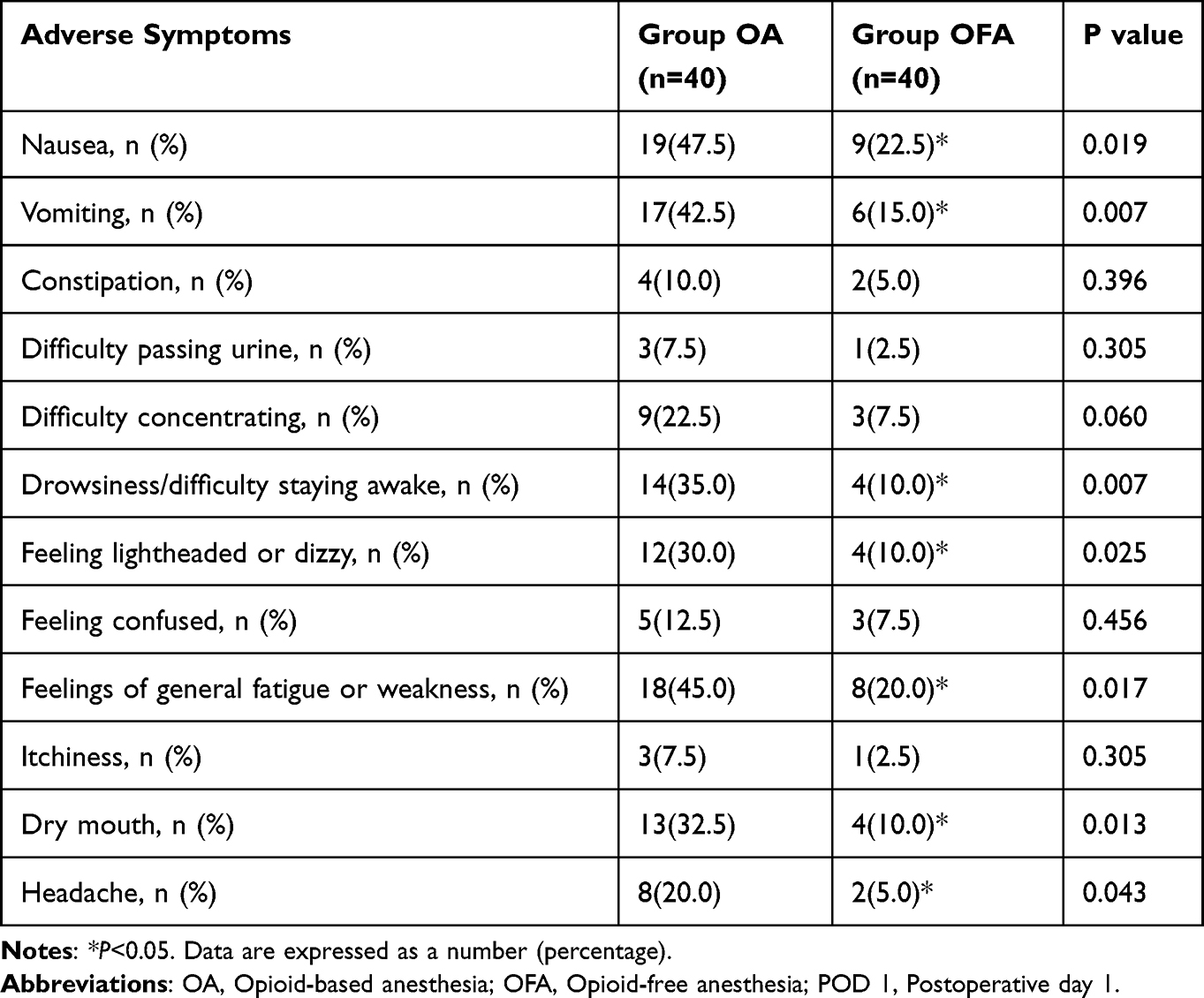 |
Table 3 Comparison of the Incidence of Opioid-Related Adverse Symptoms on POD 1 |
The SBP and DBP between the two groups were statistically different at T3 (117.1±9.9 vs 126.7±6.6, 70.8±6.2 vs 77.9±8.4) (P<0.05). There was no statistical difference in heart rate between the two groups at all points (P > 0.05). (Figure 4).
 |
Figure 4 Perioperative hemodynamic variables including (A) SBP, (B) DBP, (C) HR at baseline (T0), before intubation (T1), 1 min after endotracheal intubation (T2), 1 min before skin incision (T3), 1 min after skin incision (T4) and 1 min after extubation (T5); *P<0.05. Abbreviations: SBP, systolic pressure; DBP, diastolic blood pressure; HR, heart rate. |
Discussion
The results from the current study demonstrated that compared to OA, OFA resulted in higher QoR-15 scores in patients who underwent laparoscopic cholecystectomy surgery. Among the five domains of QoR-15, improvement in pain, psychological support, emotional state, physical comfort, and physical independence were all evident.
QoR-15 is a developed outcome and has been validated in various clinical settings. It is widely used for assessing patient comfort and quality of recovery after general anesthesia. Good recovery experience should prioritize subjective well-being and satisfaction of patients after surgery. It includes physical, mental and emotional status. The higher the QoR-15 scores, the better the quality of recovery.9
We found that the pain score of the QoR-15 questionnaire in Group OA was lower than in Group OFA on POD 1 and POD 2. This may be due to the continuous infusion of remifentanil resulting in a state of nociceptive sensitization or hyperpathia induced by remifentanil.10 In addition, low doses esketamine used in Group OFA has been established that it can increase the pain score of the QoR-15 questionnaire.11 We found a significant difference in the patients’ psychological support and emotional states between the two groups. The parameters used to assess psychological support and emotional states included needing help and talk and various feelings from general well-being to anxiety and depression. We found that patients in Group OFA felt better emotionally than those in Group OA. Studies have found that the antidepressant effect of esketamine may be related to its blocking of N Methyl D Aspartate receptor (NMDA-R), increasing the levels of 5-hydroxytryptamine (5-HT).12 In terms of physical discomfort and physical independence, the current results are consistent with the findings from a recent study, which revealed that the incidence of PONV in Group OA after gynecological surgery was higher than in Group OFA.13 Combined with our results, we speculate that intraoperative opioid use might increase the risk of PONV and may result in poor sleep quality and worse diet quality. Esketamine is a valid analgesic alternative to opioids to avoid opioid-related nausea and vomiting in the postoperative setting.14,15 Thus, we demonstrated that Group OFA in the current study had a lower incidence of drowsiness, weakness, dry mouth, headache and dizziness, which in turn may have contributed to promoting patient physical discomfort and physical independence scores.
Our findings were similar to those studies conducted by Berlier et al and Devine et al, where they demonstrated that OFA could reduce the incidence of opioid adverse symptoms compared with OA.16 In a systematic review and meta-analysis of clinical trials, Malo-Manso et al also supported that there was a clear benefit of OFA in pain control and PONV.17 We found that the better quality of recovery was accompanied by significant reductions in fewer opioid-related adverse symptoms. In our study, we observed a difference in the reduction of postoperative opioid-related adverse symptoms between the two groups, which can also be attributed to the use of multimodal analgesia, such as dexmedetomidine, esketamine, paracetamol, and non-steroidal anti-inflammatory drugs. Such reduction of symptoms is also linked to a better quality of recovery. Recent studies regarding enhanced recovery after surgery (ERAS) have shown that multimodal, opioid-free analgesia, could reduce stress mediators, improve perioperative management, and reduce functional and quality-of-life impairments.15 Furthermore, the incidence of constipation, difficulty concentrating, itchiness and feeling confused did not show any difference between the groups. This may be attributed to the shorter duration of laparoscopic cholecystectomy. More sophisticated studies on other types of operation are needed to compare the opioid adverse symptoms between the two anesthetic methods in this regard.
Moreover, the incidence of hypotension was lower in Group OFA. The advantage of esketamine and dexmedetomidine on maintaining intraoperative hemodynamic stability in OFA needed to be specifically spelled out. This may be partly related to the inhibitory effect of dexmedetomidine on neuronal discharge, sedation, analgesic and anti-sympathetic effects, so as to stabilize hemodynamics and decrease heart rate, blood pressure and cardiac output with a good protective effect on blood pressure and cardiac function.18,19 A second explanation could be related to the reduction of esketamine inhibits NMDA-R activation caused by the release of inflammatory mediators and glutamate that could effectively inhibit the stress response of endotracheal intubation.20 Studies have shown that hypotension is a common side effect of general anesthesia induction, especially when propofol is used as an induction agent, and its incidence in non-cardiac surgeries is reportedly 9–60%.21 In our study we found that SBP and DBP at 1 min before skin incision (T3) in Group OA were lower in Group OFA. It might be attributed that post-induction hypotension appears to result from arterial dilation with reduced systemic vascular resistance.22 Besides, because of the excitatory effect of esketamine on the circulatory system, the hemodynamics in Group OFA was more stable, and the incidence of hypotension was reduced during surgery. Beloeil et al concluded that balanced opioid-free anesthesia with dexmedetomidine, compared with remifentanil, would not result in fewer postoperative opioid-related adverse events; moreover, dexmedetomidine resulted in a higher incidence of serious adverse events, especially bradycardia. However, our study results were not consistent with the results of the above study.23 These discrepancies are probably due to the different doses of dexmedetomidine.
Our study presents several limitations. Firstly, in daily postoperative recovery quality assessment, the incidence of other adverse reactions after anesthesia may be underestimated due to the scattered postoperative evaluation time. Secondly, the sample size calculation is based on the total QoR-15 scores. The duration of PACU stay and other secondary outcomes should be interpreted as exploratory. Thirdly, it was conducted at a single center, limiting the generalizability of our results.
Conclusion
In conclusion, among patients undergoing laparoscopic cholecystectomy, patients receiving OFA with dexmedetomidine and es-ketamine had a better quality of recovery on POD 1 and POD 2 than those receiving opioid-based anesthesia. All five domains were scored higher in patients receiving OFA. OFA can be considered as an anesthetic method of choice for achieving a good QoR with less opioid-related side effects.
Data Sharing Statement
All data generated or analyzed during this study are included in the article. Further inquiries about the datasets can be directed to the corresponding author on reasonable request.
Acknowledgments
We thank the participants and clinic staff for their contributions to the study.
Funding
This study was funded by the Ph.D Science Research Startup Foundation of the First People’s Hospital of Lianyungang (BS202005).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Yayla A, Eskici Ýlgin V, Kýlýnç T, Karaman Özlü Z, Ejder Apay S. Nausea and vomiting after laparoscopic cholecystectomy: analysis of predictive factors. J Perianesth Nurs. 2022;37(6):834–841. doi:10.1016/j.jopan.2022.01.002
2. Sridharan K, Sivaramakrishnan G. Comparison of fentanyl, remifentanil, sufentanil and alfentanil in combination with propofol for general anesthesia: a systematic review and meta-analysis of randomized controlled trials. Curr Clin Pharmacol. 2019;14(2):116–124. doi:10.2174/1567201816666190313160438
3. Paul AK, Smith CM, Rahmatullah M, et al. Opioid analgesia and opioid-induced adverse effects: a review. Pharmaceuticals. 2021;14(11):1091. doi:10.3390/ph14111091
4. Gao C, Huang T, Wu K, et al. Multimodal analgesia for accelerated rehabilitation after total knee arthroplasty: a randomized, double-blind, controlled trial on the effect of the co-application of local infiltration analgesia and femoral nerve block combined with dexmedetomidine. Brain Sci. 2022;12(12):1652. doi:10.3390/brainsci12121652
5. Hoffman C, Buddha M, Mai M, et al. Opioid-free anesthesia and same-day surgery laparoscopic hiatal hernia repair. J Am Coll Surg. 2022;235(1):86–98. doi:10.1097/XCS.0000000000000229
6. Taylor C, Metcalf A, Morales A, Lam J, Wilson R, Baribeault T. Multimodal analgesia and opioid-free anesthesia in spinal surgery: a Literature Review [published online ahead of print, 2023 Jul 15]. J Perianesth Nurs. 2023. doi:10.1016/j.jopan.2023.04.003
7. Carnes KM, Ata A, Cangero T, Mian BM. Impact of enhanced recovery after surgery protocols on opioid prescriptions at discharge after major urological cancer surgery. Urol Pract. 2021;8(2):270–276. doi:10.1097/UPJ.0000000000000207
8. Myles PS, Myles DB, Galagher W, Chew C, MacDonald N, Dennis A. Minimal clinically important difference for three quality of recovery scales. Anesthesiology. 2016;125(1):39–45. doi:10.1097/ALN.0000000000001158
9. Massoth C, Schwellenbach J, Saadat-Gilani K, et al. Impact of opioid-free anaesthesia on postoperative nausea, vomiting and pain after gynaecological laparoscopy - A randomised controlled trial. J Clin Anesth. 2021;75:110437. doi:10.1016/j.jclinane.2021.110437
10. Koo JM, Chung YJ, Lee M, Moon YE. Efficacy of dexmedetomidine vs. remifentanil for postoperative analgesia and opioid-related side effects after gynecological laparoscopy: a prospective randomized controlled trial. J Clin Med. 2023;12(1):350. doi:10.3390/jcm12010350
11. Huang Z, Liu N, Hu S, Ju X, Xu S, Wang S. Effect of dexmedetomidine and two different doses of esketamine combined infusion on the quality of recovery in patients undergoing modified radical mastectomy for breast cancer - a randomised controlled study. Drug Des Devel Ther. 2023;17:2613–2621. doi:10.2147/DDDT.S422896
12. Chen HY, Meng XY, Gao H, et al. Esketamine-based opioid-free anaesthesia alleviates postoperative nausea and vomiting in patients who underwent laparoscopic surgery: study protocol for a randomized, double-blinded, multicentre trial. Trials. 2023;24(1):13. doi:10.1186/s13063-022-07003-3
13. Song JY, Choi H, Chae M, Ko J, Moon YE. The effect of opioid-free anesthesia on the quality of recovery after gynecological laparoscopy: study protocol for a prospective randomized controlled trial. Trials. 2021;22(1):207. doi:10.1186/s13063-021-05166-z
14. Zhu T, Zhao X, Sun M, et al. Opioid-reduced anesthesia based on esketamine in gynecological day surgery: a randomized double-blind controlled study. BMC Anesthesiol. 2022;22(1):354. doi:10.1186/s12871-022-01889-x
15. Wang D, Long YQ, Sun Y, et al. Opioid-free total intravenous anesthesia for thyroid and parathyroid surgery: protocol for a randomized, double-blind, controlled trial. Front Med. 2022;9:939098. doi:10.3389/fmed.2022.939098
16. Berlier J, Carabalona JF, Tête H, et al. Effects of opioid-free anesthesia on postoperative morphine consumption after bariatric surgery. J Clin Anesth. 2022;81:110906. doi:10.1016/j.jclinane.2022.110906
17. Malo-Manso A, Fontaneda-Heredia A, Romero-Molina S, et al. Opioid-Free anaesthesia improves anaesthesia recovery when compared with that of opioid-based anaesthesia. systematic review and meta-analysis of clinical trials. Curr Med Chem. 2023;30(14):1667–1681. doi:10.2174/0929867329666220907155612
18. Modir H, Moshiri E, Yazdi B, Kamalpour T, Goodarzi D, Mohammadbeigi A. Efficacy of dexmedetomidine-ketamine vs. fentanylketamine on saturated oxygen, hemodynamic responses and sedation in cystoscopy: a doubleblinded randomized controlled clinical trial. Med Gas Res. 2020;10(3):91–95. doi:10.4103/2045-9912.296037
19. Zhou N, Liang X, Gong J, et al. S-ketamine used during anesthesia induction increases the perfusion index and mean arterial pressure after induction: a randomized, double-blind, placebo-controlled trial. Eur J Pharm Sci. 2022;179:106312. doi:10.1016/j.ejps.2022.106312
20. Guo Y, Chen L, Gao Z, et al. Is esketamine-based opioid-free anesthesia more superior for postoperative analgesia in obstructive sleep apnea patients undergoing bariatric surgery? A study protocol. Front Med. 2022;9:1039042. doi:10.3389/fmed.2022.1039042
21. Yokose M, Takaki R, Mihara T, et al. Hypotension after general anesthesia induction using remimazolam in geriatric patients: protocol for a double-blind randomized controlled trial. PLoS One. 2022;17(9):e0275451. doi:10.1371/journal.pone.0275451
22. Jor O, Maca J, Koutna J, et al. Hypotension after induction of general anesthesia: occurrence, risk factors, and therapy. A prospective multicentre observational study. J Anesth. 2018;32(5):673–680. doi:10.1007/s00540-018-2532-6
23. Beloeil H, Garot M, Lebuffe G, et al. Balanced Opioid-free anesthesia with dexmedetomidine versus balanced anesthesia with remifentanil for major or intermediate noncardiac surgery. Anesthesiology. 2021;134(4):541–551. doi:10.1097/ALN.0000000000003725
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.