Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Impact of Medical-Prevention Integration on Resource Utilization Efficiency in Chronic Disease Management Among Older Adults: Ethical and Economic Perspectives
Authors Huang XM, Zhao JF, Wang YW, Gong ZF, Li J, Li ZL
Received 16 September 2025
Accepted for publication 9 December 2025
Published 25 December 2025 Volume 2025:18 Pages 8237—8247
DOI https://doi.org/10.2147/JMDH.S564477
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Charles V Pollack
Xiao-Meng Huang,1,2 Jing-Fan Zhao,3 Yan-Wei Wang,4 Zhi-Fu Gong,5 Jun Li,6 Zhen-Liang Li7
1Medical Department, the First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, 075000, People’s Republic of China; 2Chengde Medical University, Chengde, Hebei Province, 067000, People’s Republic of China; 3Technology Department, the First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, 075000, People’s Republic of China; 4Quality Management Department, the First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, 075000, People’s Republic of China; 5Discipline Inspection and Supervision Office, the First Affiliated Hospital of Hebei North University, Zhangjiakou, Hebei Province, 075000, People’s Republic of China; 6General Practice Medicine Department, Affiliated Hospital of Chengde Medical University, Chengde, Hebei Province, 067000, People’s Republic of China; 7Higher Education Research Office, Hebei North College, Zhangjiakou, Hebei Province, 075000, People’s Republic of China
Correspondence: Zhen-Liang Li, Higher Education Research Office, Hebei North College, 11 Zuanshi South Road, Economic Development Zone, Zhangjiakou, Hebei Province, 075000, People’s Republic of China, Tel +8618931316690, Email [email protected] Jun Li, General Practice Medicine Department, Affiliated Hospital of Chengde Medical University, 36 Nanyingzi Avenue, Chengde, Hebei Province, 067000, People’s Republic of China, Tel +8618503147726, Email [email protected]
Objective: This study examined the impact of the medical-prevention integration model on the efficiency of medical resource utilization in the management of chronic diseases (primarily hypertension and diabetes) among older adults. The analysis focused on its ethical implications (eg, progress in urban-rural equity of resource allocation, residual disparities in underdeveloped regions, and potential biases in service access for disadvantaged groups) and economic effects, with the goal of informing evidence-based health policies to support the “Healthy China” strategy.
Methods: We included 10,236 adults aged ≥ 60 with chronic diseases from six counties in Guangdong, two rural counties in Sichuan, and one suburban area in Jiangsu. A mixed-methods approach was applied: quantitative analysis of medical costs and related indicators using the Heckman two-stage model, supplemented by qualitative case studies and semi-structured interviews. Indicators for economic performance, efficiency, and equity were constructed, with subgroup analyses by age and education.
Results: Model implementation was associated with significant efficiency gains: average annual per capita outpatient costs fell by 18.1%, hospitalization costs by 18.3%, chronic disease control rates rose by 13.6% (p< 0.001), and emergency visits declined by 27.4%. The urban-rural control rate gap narrowed from 12.7% to 5.9% (53.2% reduction), though disparities remained (5% in Guangdong, 3% in Jiangsu, 11% in rural Sichuan). Subgroup analysis showed greater cost reductions for ages 60– 70 (20.1%, p< 0.01) than > 70 (15.3%, p< 0.05), and higher control rates among more educated participants (75.2% vs 59.7%, p< 0.001).
Conclusion: The integration model improves efficiency and equity in chronic disease management, generating economic savings and reducing disparities. However, persistent regional gaps and barriers among vulnerable subgroups (eg, limited mobility in > 70, low health literacy) require targeted interventions. Findings are generalizable to similar aging middle-income settings and support strengthening primary care and equitable resource allocation.
Keywords: chronic disease, chronic disease management, ethics, medical-prevention integration, medical resources
Introduction
Chronic non-communicable diseases (NCDs) have risen a major public health problem worldwide that poses serious threats to human health. The prevalence of chronic diseases has increased remarkably in China due to economic development and the aging population, which puts a heavy burden on public health.1 The percentage of population of age over 65 was slowly rising, and had reached 2% by 2022, caused by the presence of hypertension and diabetes as an aging disease, and requires an elevated level of health-care.2 Existing models of healthcare delivery have limitations in addressing chronic disease management—specifically, the traditional siloed approach, where hospitals prioritize acute episode treatment and public health agencies focus on population-level prevention. This separation leads to fragmented care (eg, no continuity between hospital discharge and community follow-up), poor patient adherence to long-term management plans, and inefficient resource use (eg, redundant examinations across institutions). The siloed hospital-centric model focused on acute episodes and the public health department’s public health-prevention population mindset has proven to be less-than-optimal for the management of chronic disease, resulting in fractured care, lapses in the continuity of care, ineffective resource utilization and hence calls for more effective and impactful new service delivery models.
In order to strategically deal with the challenges, the medical-prevention integration model was suggested for integrating clinical care function with public health functions so that healthcare shifted to a mechanism that emphasizes both prevention and treatment instead of only treatment. The objective of this project is to strengthen the connection between medical treatment and preventive healthcare, facilitating the closure of the gap of separation between “treatment organized by health institutions” and “prevention by disease prevention institutions”,3 and pilot programs conducted in some regions have been recently promised with promising developments. Improved chronic disease management workflow, enhanced primary healthcare services, and increased access and quality of healthcare services—especially among chronically diseased elderly population—are some of the outputs from these projects.4 While the medical-prevention integration model aims to improve efficiency, it carries an ethical risk: populations with higher health literacy (eg, more educated individuals) and better service access (eg, urban residents) may disproportionately benefit, exacerbating existing health inequities. An equity-focused evaluation—tracking urban-rural and socioeconomic disparities—is therefore essential to ensure the model adheres to fair resource distribution principles.
In this study, we aim to evaluate the impact of the medical-prevention integration model on the efficiency of medical resource utilization for chronic diseases among older adults. The “efficiency” includes “economic efficiency” (reducing direct medical costs, such as outpatient and hospitalization expenses, and indirect social costs, such as family caregiver labor loss) and “health efficiency” (improving health outcomes per unit of resource input, measured by chronic disease control rates and reduced emergency department visits). This study will proceed by detailing the mixed-methods study design, presenting results on economic and equity outcomes, discussing the challenges and implications, and concluding with targeted policy recommendations.
Methods
Study Design
A mixed-methods design incorporating a “deep integration of qualitative and quantitative research” was adopted. This definition aligns with the indicators detailed in the Methods section. The study followed a sequential analytical framework comprising “mechanism exploration, effect verification, and different analysis,” while incorporating both ethical and economic perspectives.
The qualitative component focused on elucidating the underlying mechanisms driving observed effects. Implementation pathways across different regions were examined, with attention to resource integration strategies and policy support, and the lived experiences of disadvantaged groups, including participants with lower educational attainment and older adults residing in rural areas. Case studies and semi-structured interviews were employed to support variable screening and to inform the interpretive framework for the quantitative analysis.
The quantitative component assessed the generalizability and effect size of qualitative findings. The impact of the model on resource allocation efficiency was assessed using core indicators such as outpatient and inpatient rates, per capita medical costs, and chronic disease control rates. Differences were further analyzed according to sociodemographic characteristics.
The methods were interconnected to establish an iterative analytic process. Initially, the quantitative data were used to demonstrate overall effects. These findings were then interpreted using qualitative cases, such as examples of county-level data sharing practices that reduced duplicate examination fees. Finally, qualitative insights such as the influence of education attainment on participation in chronic disease management, guided stratified quantitative analyses. This integrative approach facilitated the integration of “quantitative verification and qualitative interpretation.”
Data Collection and Sample Selection
Sample Selection and Geographical Coverage
To improve sample representativeness and overcome the limitations of a single-site design, the study included participants from three types of representative regions. The final sample comprised 10,236 older adults (≥60 years) with chronic diseases, primarily hypertension and diabetes. The specific distribution was as follows:
- Counties in Guangdong Province: Six counties were included, comprising three economically developed counties in the Pearl River Delta and three less-developed counties in eastern and western Guangdong. These sites represented varying stages of medical-prevention integration implementation, including the pilot period (1 county), promotion period (3 counties), and maturity period (2 counties). This regional selection allowed for the analysis of how differing levels of economic development influenced the model’s effectiveness.
- Rural areas in central and western China: Two counties in Sichuan Province, designated as key national rural revitalization areas, were included to examine the challenges of implementation in resource-limited settings.
- Suburban area of an eastern developed region: One district in Jiangsu Province, located within the Yangtze River Delta urban agglomeration, was included to assess the effect of urbanization level on implementation outcomes.
The inclusion criteria were as follows: a confirmed diagnosis of hypertension or diabetes for ≥6 months, age ≥60 years, and continuous residence in the study area for at least 5 years. Individuals with severe mental illness or cognitive impairment who were unable to participate in the investigation were excluded.
Data Collection Methods
Qualitative Data
- Case data: Implementation plans from 10 cases of medical-prevention integration were collected, including detailed rules for resource integration and evaluation indicators. Data sources included policy documents issued by local health commissions, institutional work reports, and media reports.
- Interview data: Semi-structured interviews were conducted with three categories of participants, with 30 to 50 individuals per group. (Supplementary material A): Semi-structured interview guides.
- Medical staff (primary care physicians and staff from centers for disease control and prevention): Interviews focused on the assignment of responsibilities and barriers to information exchange within the integration framework.
- Older adults with chronic diseases: Discussions emphasized perceived accessibility of services (eg, distance, cost) and perceived changes in self-management capabilities.
- Policymakers: Emphasis was placed on the effectiveness of local support policies (eg, financial subsidies and workforce incentive policies).
Quantitative Data
- Administrative Data from Medical institutions: Data on healthcare utilization among older adults with chronic diseases were extracted from institutional databases in the study areas, from 2019 to 2023. Variables included the number of outpatient visits, hospitalization days, total medical expenses, and indicators chronic disease control (eg, blood pressure and blood glucose compliance rates).
- Questionnaire survey: Information on sociodemographic characteristics (sex, age, educational level, and household income), health literacy, and satisfaction with medical-prevention integration services was collected through face-to-face surveys. The health literacy scale has good internal consistency (Cronbach’s α=0.86) and construct validity (confirmatory factor analysis: CFI=0.92, RMSEA=0.05), adapted from the Chinese Citizen Health Literacy Scale. (Supplementary material B: Measurement tools, including the full-dimensional Health Literacy Scale and the Patient Satisfaction Questionnaire with specific items for evaluating medical-prevention integration service).
Data Analysis Methods
Quantitative Analysis
The core analytical framework was based on the Heckman two-stage model, which was applied to correct for sample selection bias. In the first stage, a Probit model was used to examine the influence of participation in medical-prevention integration services, with independent variables including age, educational level, and regional economic status. In the second stage, multiple linear regression was conducted to assess the specific impact of the depth of participation, measured by monthly frequency of participation in chronic disease management, on key outcomes such as medical costs and hospitalization rates. (Supplementary material C: Technical details for quantitative analysis, such as a complete list of variables).
Subgroup analyses were performed to validate heterogeneity in model effects across different populations. Stratifications were made by regional classification (counties in Guangdong Province, rural areas in central and western regions, and eastern suburban districts) and sociodemographic characteristics (age stratification: 60–70 years vs >70 years; educational level: primary school or below vs secondary school and above). These analyses facilitated the identification of effect modifiers and potential confounding variables, such as the moderating effect of educational level on the relationship between health literacy and medical costs.
An indicator system was developed to evaluate the efficiency of medical resource utilization, comprising the following dimensions:
- Economic indicators: per capita annual outpatient costs, per capita annual hospitalization costs, and the proportion of costs allocated to medications.
- Efficiency indicators: outpatient follow-up compliance rate (≥4 visits per year), chronic disease control rate (blood pressure <140/90 mmHg, blood glucose <7.0 mmol/L), and emergency department visit rate.
- Equity indicators: differences in service participation rates among income groups and differences in chronic disease control rates between urban and rural populations.
Qualitative Analysis
Thematic analysis was applied to encode the interview transcripts and case data across three levels. First-level coding involved the identification of initial themes such as “resource integration”, “policy support”, and “patient experience.” Second-level coding summarized these into core themes, including “obstacles in medical-prevention coordination” and “demand gaps among disadvantaged groups.” Third-level coding produced higher-order categories, namely “key elements of model effectiveness” (eg, “information exchange” and “financial guarantees”) and “ethical risk points” (eg, “resource allocation skewed toward high-income groups”).
Cross-case comparisons were conducted to analyze the impact of economic development on implementation pathways of medical-prevention integration. In Guangdong Province, implementation relied primarily on “resource reallocation within medical alliances”, whereas in central and western regions it depended on “capacity enhancement of village doctors.” Comparisons based on interview data from individuals with different educational backgrounds further illustrated the mediating role of health literacy in influencing engagement and outcomes within the integrated service model. (Supplementary material D: An example of the qualitative analysis coding framework, with definitions and illustrative quotations for first-, second-, and third-level codes).
Qualitative Sampling & Reliability:
- Sampling strategy: Purposive sampling was used to select information-rich cases from each county, ensuring representation of different age groups (60–70 years vs >70 years), educational levels (primary school or below vs secondary school and above), and urban/rural areas. This strategy prioritized cases that could provide in-depth insights into regional implementation differences and subgroup-specific barriers.
- Coding team: Composed of 2 public health researchers (with 5+ years of qualitative research experience) and 1 medical management expert (specializing in chronic disease policy), all trained in thematic analysis and the study’s theoretical framework to ensure consistency in coding logic.
- Inter-coder reliability: Prior to formal analysis, 20% of interview transcripts were independently coded by two researchers. Cohen’s kappa coefficient was calculated to assess agreement, with a final score of κ=0.82—indicating substantial reliability (κ>0.75, per academic standards for qualitative research). Discrepancies in coding were resolved through group discussion led by the medical management expert, with decisions documented in a coding memo.
Method Integration
The integration of quantitative and qualitative data was designed to enhance the comprehensiveness and interpretive depth of the analysis. First, quantitative data were applied to demonstrate the overall effect of the model. For example, “the average hospitalization cost of older adults in Guangdong counties was reduced by 23%.” Subsequently, qualitative findings were used to explain the specific mechanisms underlying the effect. For example, duplicate examinations were reduced through the mutual recognition of examination results within a county-level medical alliance, leading to an average annual cost saving of RMB 580 per patient.
Finally, subgroup analyses results were interpreted in conjunction with patient interviews. For instance, “cost reduction among individuals over 70 years of age [15%] was lower than that observed in the 60–70 age group [28%].” “Older adults with limited mobility demonstrated lower rates of follow-up participation.” This integration supported the development of targeted recommendations for policy optimization.
Integration Framework
To systematically link quantitative and qualitative findings, joint display tables were used as the core integration tool. These tables structured quantitative subgroup results (eg, “20.1% cost reduction in 60–70-year-olds vs 15.3% in >70-year-olds”) alongside corresponding qualitative themes (eg, “83% of >70-year-old interviewees reported ‘limited mobility’ as a barrier to follow-up”). This approach enabled cross-validation: for example, quantitative data showing persistent urban-rural disparities in Sichuan was corroborated by qualitative insights that “62% of rural participants cited ‘inconvenient transportation’ as a primary service barrier.” Joint displays also helped identify unmeasured confounding factors (eg, low health literacy in lower-educated groups) that explained subgroup differences in quantitative outcomes.
Results
Current Progress in the Implementation of the Medical-Prevention Integration Model
Case analyses conducted in six counties in Guangdong Province, two rural counties in Sichuan Province, and one suburban district in Jiangsu Province revealed regional variability in the implementation of the medical-prevention integration model for chronic disease management among older adults. The corresponding quantitative and qualitative findings are presented in Table 1. Distinct implementation pathways were observed based on regional economic development. In economically developed areas, such as counties in Guangdong Province and the suburban district in Jiangsu Province, implementation primarily relied on “resource integration and digital health infrastructure.” In contrast, less-developed rural counties in Sichuan Province depended on “capacity enhancement at the primary level.”
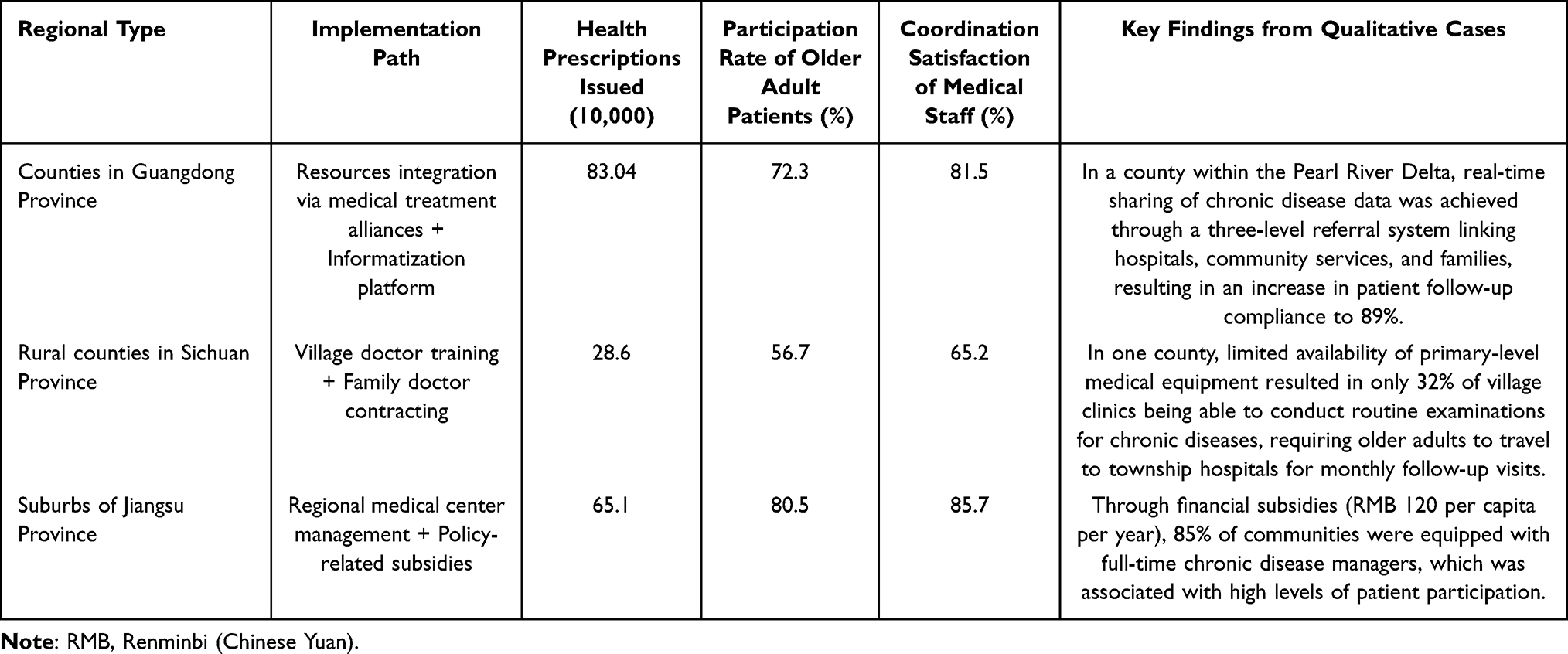 |
Table 1 Comparison of Core Indicators in the Implementation of the Medical-Prevention Integration Model Across Regions |
Regarding participation rates and satisfaction with collaboration, the suburban district in Jiangsu Province demonstrated the most favorable outcomes (participation rate: 80.5%; medical staff coordination satisfaction: 85.7%), attributable to policy subsidies and full-time personnel. In contrast, rural counties in Sichuan Province presented the lowest indicators (participation rate: 56.7%; coordination satisfaction: 65.2%), largely due to equipment shortages and human resource constraints. Notably, 83% of the interviewed village doctors reported “work overload” as a significant barrier to collaboration. Guangdong counties showed intermediate performance (participation rate: 72.3%; coordination satisfaction: 81.5%), with successful data-sharing through three-level referral systems.
Evaluation of Medical Resource Utilization Efficiency
Quantitative evaluation of medical resource utilization was conducted across three dimensions: economy, efficiency, and equity. Detailed findings are presented in Table 2.
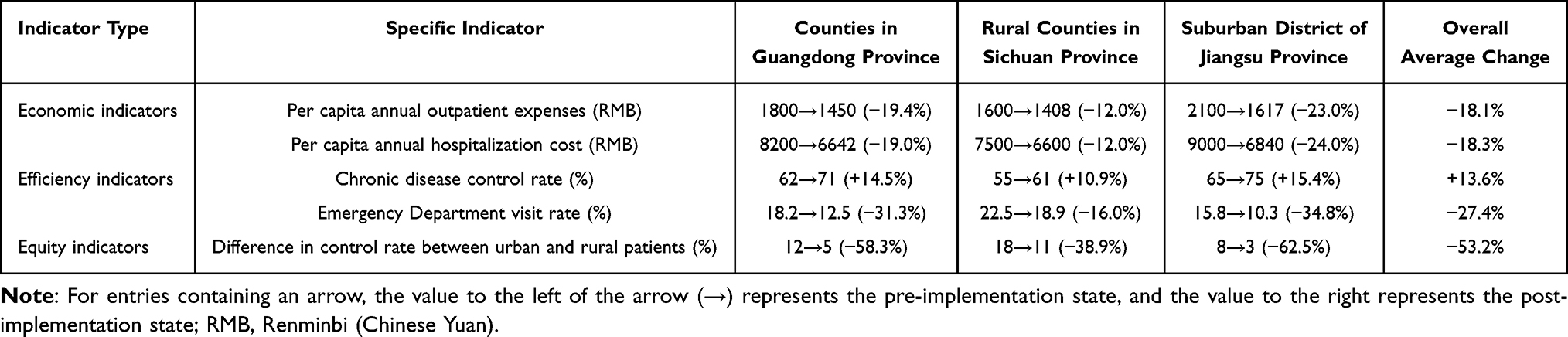 |
Table 2 Impact of the Medical-Prevention Integration Model on Medical Resource Utilization Efficiency: Pre- and Post-Implementation Comparison |
In terms of economic efficiency, the suburban district of Jiangsu Province demonstrated the most substantial improvements (outpatient cost reduction: 23.0%, hospitalization cost reduction: 24.0%), largely associated with reduced duplicate diagnostics (mutual recognition rate of examinations: 92%). Rural counties in Sichuan Province reported the smallest reductions (outpatient: 12.0%, hospitalization: 12.0%) due to inadequate equipment. On average, per capita annual outpatient costs decreased by 18.1% (range: 23.0%–12.0%) (p<0.001) and hospitalization costs by 18.3% (range: 24.0%–12.0%) (p<0.001) across all study sites.
In terms of health efficiency, the average chronic disease control rate improved by 13.6% (from 60.8% to 74.4%, p<0.001), while emergency department visit rates decreased by 27.4% (from 18.8% to 13.6%, 95% CI: −31.2% to −23.6%). The highest control rate was observed in Jiangsu’s suburban district (75.0%), followed by Guangdong counties (71.0%) and Sichuan rural counties (61.0%).
In terms of equity, the urban-rural chronic disease control rate gap narrowed from 12.7% (pre-intervention) to 5.9% (post-intervention), a 53.2% reduction. In Guangdong Province, the gap decreased from 12% to 5% (−58.3%), and in Jiangsu’s suburban district from 8% to 3% (−62.5%). However, an 11% gap persisted in Sichuan’s rural counties (down from 18% to 11%), with 62% of rural participants identifying “inconvenient transportation” as the primary barrier to service access.
In-Depth Economic Benefit Analysis
Building on the economic indicators in Evaluation of Medical Resource Utilization Efficiency, this section focuses on cost-benefit ratios and the breakdown of direct vs indirect savings.
Direct medical cost reductions varied by population subgroup: 60–70-year-olds achieved a 20.1% reduction (p<0.01) compared to 15.3% (p<0.05) in those over 70. Individuals with secondary education and above had a 22.4% cost reduction (p<0.001), while those with primary education or below had only a 12.8% reduction (p<0.05). These differences corresponded with follow-up participation rates: 78% in 60–70-year-olds, 58.9% in those over 70, 80.5% in higher-educated groups, and 54.3% in lower-educated groups.
Indirect social cost savings were primarily reflected in reduced labor loss for family caregivers, ranging from RMB 900 to 1,800 per year. The greatest indirect savings were observed in the over-70 age group (RMB 1,200/year) due to door-to-door services, while higher-educated groups achieved the highest direct cost savings (RMB 2,300/year) through independent medication adjustment. Lower-educated groups had limited indirect savings (RMB 900/year) because 65% relied on family members to interpret medical data. (Detailed data are presented in Table 3).
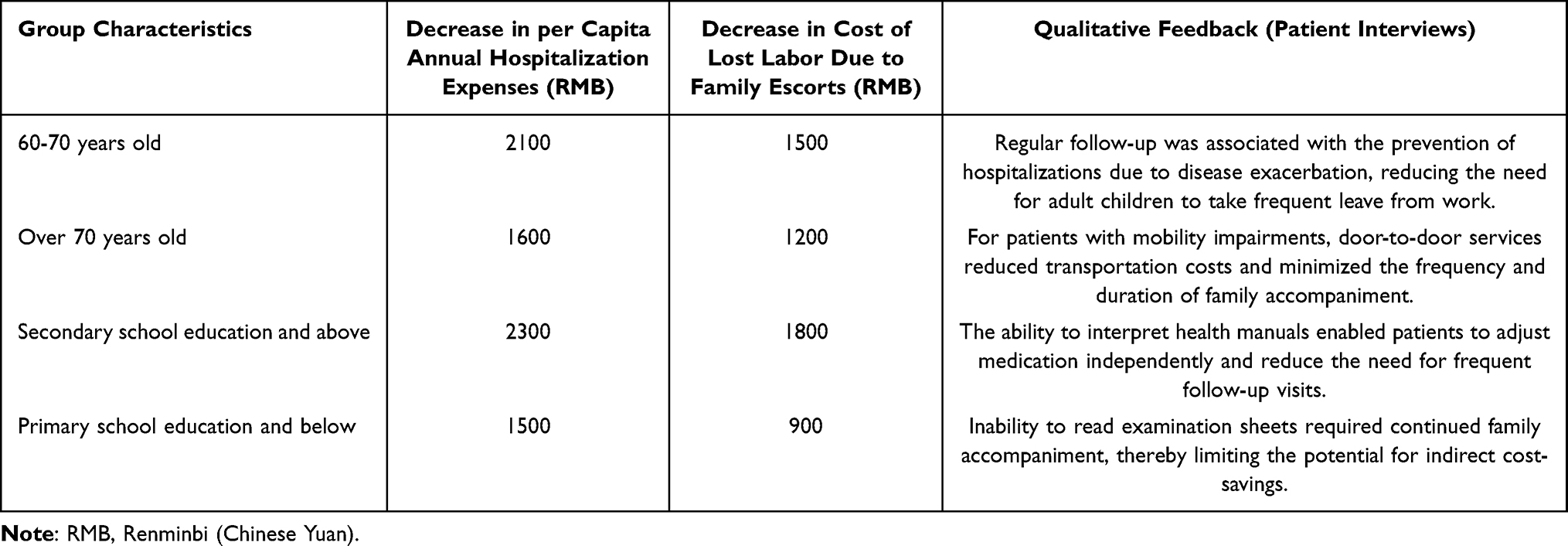 |
Table 3 Quantitative Results of Economic Benefits by Group Characteristics |
Influence of Sociodemographic Characteristics on the results
Stratified analyses by age group and educational attainment revealed significant variation in resource utilization efficiency.
As presented in Table 4, individuals aged over 70 years demonstrated lower control rates (62.8% vs 73.5% in 60–70-year-olds, p<0.001) and follow-up compliance rates (58.9% vs 76.2%, p<0.001). Qualitative interviews indicated limited mobility and solitary living (reported by 42% of participants aged over 70) as major barriers. This group also exhibited smaller cost reductions (15.3% vs 20.1%, p<0.05), reflecting rigid medical service demands.
 |
Table 4 Correlation Between Sociodemographic Characteristics and Core Indicators |
With respect to educational level, participants with higher education had higher health literacy scores (68.5 vs 45.2 points, p<0.001), stronger self-management capacity, and consequently higher control rates (75.2% vs 59.7%, p<0.001) and cost reductions (22.4% vs 12.8%, p<0.001). The follow-up compliance rate gap between higher and lower education groups reached 26.2 percentage points (80.5% vs 54.3%, p<0.001).
Notably, even within the highly educated group, regional economic differences influenced outcomes: the chronic disease control rate was 82.3% in Jiangsu’s suburban district (economically developed) compared to 68.5% in Sichuan’s rural counties (economically underdeveloped), highlighting the moderating role of resource accessibility.
Discussion
Advantages of the Medical-Prevention Integration Model: Multidimensional Effect Verification
This study sought to evaluate the impact of the medical-prevention integration model on medical resource utilization efficiency for older adults with chronic diseases, from both ethical and economic perspectives. Our findings confirm the model’s significant advantages in improving efficiency and equity, while also highlighting critical challenges that require targeted solutions. Our results validate the important advantages of medical-prevention combination model, while at the same time showing its fundamental challenge. The main objective of this work was to understand the impact on resource effectiveness from not only the moral perspective but also the economical dimension. The feasibility of the model was evaluated from economic, efficiency and social gain perspectives following studies of integrated management of chronic conditions.5,6
In terms of economic outcomes, per capita annual outpatient expenses decreased by 12.0%–23.0% and hospitalization costs by 12.0%–24.0%, consistent with Ningbo’s “integrated outpatient clinic for chronic diseases” results.5 The most substantial savings in Jiangsu’s suburban district underscore the importance of centralized resource allocation and financial support. Indirect social benefits included reduced family caregiver labor loss (RMB 900–1,800/year), alleviating care burdens as theoretically expected.
Comprehensive prevention and treatment may lower the prevalence of disease aggravation, as the chronic disease under control rate increased by 13.6%, the emergency visit rate decreased by 27.4% in terms of performance enhancement. Both in Guangdong and in Jiangsu, those subjects who were enrolled in digital health platforms and followed by fulltime staff were associated with a higher following rate, while age and education-related differences in the outcomes further evidence patient involvement as a key mediator-consistent with the literature associating health literacy with positive chronic disease management.6
In terms of equity, the 53.2% reduction in urban-rural control rate gaps demonstrates the model’s potential to promote health equity. Resource reallocation through medical alliances in Guangdong and policy subsidies in Jiangsu expanded rural access. However, the residual 11% gap in Sichuan reflects ethical risks of uneven resource distribution, emphasizing the need for region-sensitive implementation to avoid reinforcing inequities.7
Compared to Mayer et al’s8 research on comorbidity management, our study further clarifies that integration models achieve greater efficiency gains when combined with targeted subgroup interventions. Unlike Hirashima et al’s9 focus on biological mechanisms, we highlight the structural factors (eg, coordination mechanisms, resource allocation) that influence real-world implementation.
Implementation Challenges: Regional Differences and Mechanism Obstacles
Although proven in many advantages, its popularization still faces huge challenges, since the distribution of resources between different regions is uneven. In rural areas of Sichuan, the proportion of prescriptions from Guangdong was only 34.4%, and there was also a 15.6% lower share of involvement. The disparity distribution of resources in Guangdong and Jiangsu in the centralized resource model is very difficult to imitate in resource scarcity regions; therefore, low-cost imitations like mobile medical instrument were needed, as over 83% of village doctors said their equipment was not enough, but only 32% could offer routine chronic diseases examination village clinics.8
Coordination mechanism deficiencies also hinder effectiveness. Sichuan’s medical staff coordination satisfaction (65.2%) was significantly lower than in developed areas, with 76% citing ambiguous responsibilities and poor communication—consistent with findings that separation of medical and public health functions creates collaboration barriers.9 Even in developed areas, 23% of respondents expressed data-sharing security concerns, requiring technical (unified standards) and institutional (clarified data rights) improvements.
The absence of policy refinement does not address the specific population needs, as it was seen in the low follow-up compliance rates for people above 70 years old (58.9%) and lower education (54.3%), which can be explained through restrictions on mobility and disparities in health literacy, a result that correlates with Compton et al’s discovery. We reported that underserved populations benefit from the unique chronic disease prevention/screening modalities.10
Influence of Sociodemographic Factors on Outcomes and Intervention Strategies
Our model proves to be significantly affected by age and education status. Senior citizens at >70 had fewer control (62.8% vs 73.5%) and cost savings (15.3% vs 20.1%), whereas 42% were dependent on their family members in follow-up-consistent with previous studies related to physical limitations hinder medical adherence.10 Personalised interventions must include home visits, travel support for the population and virtual GP guidance to improve reach.
Educational level impacts outcomes through health literacy mediation. Higher-educated groups had 23-point higher health literacy scores, better self-management, and greater cost savings—supporting the theory that health literacy determines chronic disease self-management capacity.11 Peer-led education and scenario-based training are recommended for lower-educated populations.
The interaction between geography and economics also matters: even highly educated individuals in underdeveloped areas had lower control rates (68.5% vs 82.3% in developed areas). Telemedicine could compensate for resource limitations in these groups, avoiding a one-size-fits-all policy approach.
Balancing Ethics and Economics: A Coordinated Path Toward Equity and Efficiency
Our sustainability of the model mainly depends on a balanced balance between moral and economic impacts. Ethically, fairness should be at the top. Despite a large decline in the urban rural gap, the 11% urban rural gap in Sichuan and the smaller cost decline in lower-educated population (12.8% vs 22.4%) showed its unfairness. The qualitative data yielded results on rural elderly perceived that 38% of them thought that services are allocated preferentially for younger, more cooperative patients; hence, they reflected a possibility of a disadvantaged groups being marginalized).12 This violates the distributive justice and warrants the presence of equity appraisal indicators (eg, participation rates of the disadvantaged groups, differential urban-rural access to services) to ensure equitable resource allocation.
From an economic perspective, efficiency improvements require sustainable financing. Jiangsu’s suburban district achieved high participation through RMB 120/capita/year subsidies, but 67% of Sichuan’s township health centers struggled to maintain full-time managers without dedicated funding. Diversified financing (medical insurance allocation, social capital engagement) is needed. Notably, higher-educated groups had a favorable input-output ratio (RMB 2.3 hospitalization cost reduction per RMB 1 management investment), suggesting initial prioritization of these groups could generate demonstration effects, advancing “efficiency first with equity considered.”
The coordinating pathway develops equity with a sufficient base and enlarges efficiency to promote progress by giving free basic services (eg, free blood pressure examination and basic drug in rural counties that are under-developed) in Sichuan by transfer payment. Due to the combination and sharing of digital technology, efficient developed regions not only realize their efficiency but also use the savings to help the ineffective developing regions-making a win–win environment with an ascending spiral of equity by efficiency. This “efficiency-driving-equity” cycle is essential to maximizing the model’s contribution to the “Healthy China” strategy.
Research Limitations and Future Directions
Though such method mixtures and a large sample size are advantageous regarding reliability, constraints still exist. The sample does not involve citizens residing from the original city's downtowns or rural western pastoral regions, limiting the scope of the application. To guarantee the result application for various context, future works are recommend to involve these environments. Long period effects (eg) should also be considered. No long-term complication rates were tracked; follow-up cohort studies are required to assess cost effectiveness over time.
Second, SEM can be used to further examine how structural equation modeling moderates social support and family caregiving ability, so as to explore causal mechanisms further. Third, RCT must be done to determine whether intervention for the older or less-educated group could truly work. Among the identified future directions, two are most critical and urgent: (1) Expanding geographic representation to include first-tier city cores and western remote pastoral areas (to verify generalizability across diverse Chinese contexts); (2) Conducting long-term cohort studies to assess 5-year outcomes (eg, chronic disease complication rates and sustained cost savings), as short-term data (2019–2023) cannot fully capture the model’s long-term cost-effectiveness.
Conclusion
This study demonstrates that the medical-prevention integration model significantly improves the efficiency and equity of chronic disease management for older adults—reducing medical costs, improving health outcomes, and narrowing urban-rural gaps—yet its success is contingent on addressing critical regional disparities (eg, equipment shortages in Sichuan’s rural areas) and socioeconomic barriers (eg, low health literacy in less-educated groups). Economically, it reduces per capita annual outpatient costs by 18.1%, hospitalization costs by 18.3%, and emergency visits by 27.4%, while generating indirect social savings of RMB 900–1,800 annually for family caregivers; subgroups including 60–70-year-olds and those with secondary education or above benefited more. Ethically, it narrowed the urban-rural chronic disease control rate gap by 53.2%, though residual disparities remain, such as 11% in rural Sichuan.
To maximize the model’s value, targeted measures are needed: region-specific support, enhanced interventions for vulnerable groups (home visits for adults over 70, health literacy training for lower-educated populations), and optimized financing/equity monitoring. This model supports China’s “Healthy China” strategy and provides replicable insights for aging middle-income societies, with its core strength in balancing efficiency and equitable resource allocation for chronic disease care.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Hebei North College (No. K2025290). This study was conducted in accordance with the declaration of Helsinki. Written informed consent was obtained from all participants.
Acknowledgments
We thank the staff for their dedicated work in implementing the study’s intervention and evaluation.
Funding
The 2025 Annual Project Plan for Medical Scientific Research in Hebei Province: “Exploration of the Construction of the Medical Ethics Review Center in the Northwest Region of Hebei Province under the New Ethical Governance Model” (No.20250897).
Disclosure
The authors declare that they have no competing interests.
References
1. Bello AK, Okpechi IG, Levin A. et al. An update on the global disparities in kidney disease burden and care across world countries and regions. Lancet Glob Health. 2024;12(3):e382–e395. doi:10.1016/S2214-109X(23)00570-3
2. Zhong A, Bajaj SS, Stanford FC. Out of the frying pan into the fire: COVID-19 as a road map for integrated chronic disease prevention. J Public Health Manag Pract. 2023;29(2):117–119. doi:10.1097/PHH.0000000000001694
3. Thomas SA, Browning CJ, Charchar FJ, et al. Transforming global approaches to chronic disease prevention and management across the lifespan: integrating genomics, behavior change, and digital health solutions. Front Public Health. 2023;11:1248254. doi:10.3389/fpubh.2023.1248254
4. Pradhan N, Dobre M. Emerging preventive strategies in chronic kidney disease: recent evidence and gaps in knowledge. Curr Atheroscler Rep. 2023;25(12):1047–1058. doi:10.1007/s11883-023-01172-5
5. Wang Y, Deng R, Geng X. Exploring the integration of medical and preventive chronic disease health management in the context of big data. Front Public Health. 2025;13:1547392. doi:10.3389/fpubh.2025.1547392
6. Wesson DE, Mathur V, Tangri N, et al. Primary medical care integrated with healthy eating and healthy moving is essential to reduce chronic kidney disease progression. Am J Med. 2022;135(9):1051–1058. doi:10.1016/j.amjmed.2022.04.015
7. Aghnatios M, Darloy T, Dictor J, et al. Soins infirmiers en pratique avancée: représentations des acteurs de ce nouveau dispositif. Sante Publique. 2021;33(4):547–558. doi:10.3917/spub.214.0547
8. Mayer G, Dobrev D, Kaski JC, et al. Management of dyslipidaemia in patients with comorbidities: facing the challenge. Eur Heart J Cardiovasc Pharmacother. 2024;10(7):608–613. doi:10.1093/ehjcvp/pvae058
9. Hirashima Y, Nakano T, Torisu K, et al. SGLT2 inhibition mitigates transition from acute kidney injury to chronic kidney disease by suppressing ferroptosis. Sci Rep. 2024;14(1):20386.
10. Compton MT, Manseau MW, Dacus H, et al. Chronic disease screening and prevention activities in mental health clinics in new york state: current practices and future opportunities. Community Ment Health J. 2020;56(4):717–726. doi:10.1007/s10597-019-00532-3
11. Wilkinson AJK, Anderson G. Sustainability in Inhaled Drug Delivery. Pharmaceut Med. 2020;34(3):191–199. doi:10.1007/s40290-020-00339-8
12. Wu D, Liu W, Wang J, et al. Clinical application guideline of combination with traditional chinese medicine and western medicine in the prevention and treatment of chronic obstructive pulmonary disease. J Evid Based Med. 2025;18(2):e70024. doi:10.1111/jebm.70024
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.