")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Impact of Isolation During the COVID-19 Pandemic on the Patient Burden of Parkinson’s Disease: A PMD Alliance Survey
Authors Hermanowicz N , Ospina MC , Torres-Yaghi Y, Gould S, Papesh K, Rivera JA, Miller S, Jones S, Musick K, May D
Received 13 December 2021
Accepted for publication 22 February 2022
Published 23 March 2022 Volume 2022:18 Pages 633—643
DOI https://doi.org/10.2147/NDT.S351691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Roger Pinder
Neal Hermanowicz,1 Maria Cristina Ospina,2 Yasar Torres-Yaghi,3 Sherrie Gould,4 Kelly Papesh,5 Jason A Rivera,6 Susan Miller,6 Sarah Jones,6 Kelli Musick,7 Damian May7
1Christus-St. Vincent Neurology Specialists, Santa Fe, NM, USA; 2Regional Parkinson Center, Phoenix, AZ, USA; 3MedStar Georgetown University Hospital, Washington, DC, USA; 4Scripps Clinic Movement Disorder Center, La Jolla, CA, USA; 5Cleveland Clinic Lou Ruvo Center for Brain Health, Las Vegas, NV, USA; 6Parkinson and Movement Disorder Alliance (PMD Alliance), Tucson, AZ, USA; 7ACADIA Pharmaceuticals Inc, San Diego, CA, USA
Correspondence: Neal Hermanowicz, Tel +1 (505) 913-3877, Email [email protected]
Purpose: As the COVID-19 pandemic resulted in social restrictions around the globe, this cross-sectional survey aimed to assess the impact of social isolation on self- or proxy-reported symptoms of Parkinson’s disease (PD) during the pandemic.
Patients and Methods: The survey was distributed among 7109 subscribers of the Parkinson and Movement Disorders Alliance (PMD Alliance) News and Information list and was open only to people with PD (PwP) and care partners (CP, defined as main caregivers of PwP and serving as proxy respondents). No attempt was made to identify PwP and CP pairs. The survey was distributed online using Survey Monkey between 01/06/2021 and 02/27/2021. Respondents were grouped by level of social support from outside of their household during the pandemic (decreased or maintained [ie, the same as pre-pandemic or increased]).
Results: Of 7109 invited participants, 718 responded to the survey (response rate 10.1%). PwP (self-reports) accounted for 70.6% of respondents and CP (proxy reports) for 29.4%. Decreased social support from outside of the household during the COVID-19 pandemic (58.5% of all responses) was significantly associated with increases in sadness/depression and anxiety, compared with maintained levels of social support (p < 0.0001 for both comparisons). It was also associated with increased burden of several non-motor (decline in memory, problem solving, or communication, p = 0.0009; new or worsening confusion, p < 0.0001; new or worsening delusions, p = 0.018) and motor PD symptoms.
Conclusion: Decline in social support from outside of the household during the COVID-19 pandemic showed a statistically significant and negative association with the burden of mood and non-motor symptoms of PD. These results call for increased vigilance towards non-motor symptoms in PwP experiencing social isolation and highlight the need for stronger provider focus on encouraging PwP and their CPs to build and maintain social connections and engagements.
Keywords: Parkinson’s disease, social isolation, anxiety, depression, non-motor symptoms, COVID-19
Plain Language Summary
- Parkinson’s Disease (PD) can be associated with many movement-related symptoms (eg shaking, stiffness, and slowness of movement) and symptoms unrelated to movement (called “non-motor symptoms”), such as anxiety, depression, confusion, hallucinations (false sensations, eg seeing something that is not there), and delusions (false beliefs, eg a belief someone is being spied on).
- As the COVID-19 pandemic led to severe restrictions on social interactions between households and social life in general, we surveyed people with PD and their care partners (who responded on behalf of the person with PD under their care) to find out what impact these social restrictions had on PD symptoms.
- Nearly 60% of survey respondents reported that the level of social support from outside of their household decreased during the pandemic. This decrease in social support was associated with an increase in non-motor PD symptoms such as anxiety; sadness and depression; confusion; delusions; and problems with problem solving, memory and communication. It was also associated with an increase in many movement-related symptoms, including difficulty in managing everyday activities.
- We propose that, during and beyond the COVID-19 pandemic, people with PD, their care partners, and others in their social environment should strive to build and maintain social connections and engagements, to help people with PD feel better and reduce the burden that PD symptoms have on their lives. In addition, healthcare providers, as well as people with PD and their care partners should pay increased attention towards detecting non-motor symptoms of PD and their prompt treatment.
Introduction
Parkinson’s Disease (PD) is estimated to affect approximately 110 per 100,000 people globally and approximately 188 per 100,000 people in the United States.1 The global prevalence of PD has increased by about 50% in the last 25 years1 and is projected to continue rising, driven primarily by population ageing.2 It is estimated that over 12 million people worldwide will be living with PD by 2040.2
PD is associated with a range of motor (eg tremor, rigidity, and bradykinesia) and non-motor symptoms, including sleep disturbances, cognitive decline, anxiety, depression, apathy, and psychosis, characterized by visual and/or auditory hallucinations, delusions, and illusions.3,4 Non-motor symptoms are common in PD. Up to 60% of people with PD (PwP) experience anxiety3 and approximately a third have clinically significant depression.5 Furthermore, a long-term prospective study in Norway reported that as many as 60% of PwP developed psychotic symptoms.6 Importantly, psychosis in PwP is associated with high morbidity and mortality, as well as notable caregiver stress and burnout.4
The psychological and social burden of PD is substantial, with PwP experiencing psychological distress, reduced life satisfaction, and impaired quality of life (QoL).7 Non-motor symptoms are associated with reduced QoL in PwP8,9 and contribute substantially to caregiver burden.10,11 PD symptoms can also adversely impact social functioning of PwP;12 however, perceived physical health in PwP has been reported to correlate with time spent on outdoor leisure activities.13 Moreover, loneliness has been linked to several conditions affecting mental and physical health.14,15 The COVID-19 pandemic resulted in restrictions on social contact across the globe, with variable severity of restrictions according to time period and location. However, throughout the pandemic, the Centers for Disease Control and Prevention promoted general awareness of the increased risk of serious infection or death to those who are older, immune compromised, and those with certain medical conditions, including dementia and other neurological conditions.16 Therefore, despite the uptake of online resources (such as medical provider visits, and physical and complementary therapy)17 and the availability of virtual support group meetings for both PwP and their Care Partners (CP),18 the pandemic brought about a risk of PwP entering a vicious circle of reduced social activity impacting their perceived health, which decline could precipitate further social withdrawal.
The objective of this cross-sectional survey was to assess the impact of the COVID-19 pandemic on the burden of motor and non-motor PD symptoms, using an online survey of PwP and their CP, who served as proxy respondents, reporting on the symptoms experienced by PwP under their care. This publication focuses specifically on the impact of social isolation on the respondent-perceived change in PD symptoms.
Materials and Methods
Participant Sample
The survey was distributed among 7109 subscribers of the Parkinson and Movement Disorders Alliance (PMD Alliance) News and Information list. Based on self-identification at the start of the survey, respondents were classified as PwP or CP (defined as a spouse, partner, or non-paid person caring and living with a PwP). CPs served as proxy respondents, completing the survey on behalf of the PwP under their care.
CPs responding to the survey were not necessarily the CPs of PwP respondents. Neither the survey itself nor the data analysis process attempted to identify PwP and CP pairs from the same household.
The survey was open to PwP and CP only. Any potential respondents who reported that they belonged to neither of the two groups (eg healthcare professionals involved in PD care) received a thank you note for their willingness to participate but could not proceed to complete the survey.
Survey Methodology and Characteristics
The survey was distributed using Survey Monkey® between January 6, 2021 and February 27, 2021. Potential respondents were invited to participate via e-mail, which was sent 3 times between January 13, 2021 and January 21, 2021. No incentives were offered to respondents for their participation. The survey was fully anonymous and, as no personal identifiers were collected, no ethical board approval was required.
Each respondent could only submit a single questionnaire entry to avoid duplicate responses being included in the analysis. The survey included 22 questions assessing demographic and disease characteristics; perceived change in social support since the onset of COVID-19 restrictions in April 2020; impact of COVID-19 disease on the PwP and their family; change in social engagements, activities, and support during the COVID-19 pandemic; impact of COVID-19 pandemic on motor and non-motor symptoms of PD; and participation and interest in PMD Alliance events. The complete survey is available in the Supplementary Material.
Analysis
Survey results were presented using descriptive statistics, including count and percentage for categorical variables and mean and standard deviation (SD) for continuous variables. The respondent-perceived impact of the COVID-19 pandemic on PD symptoms was assessed using a 3-point Likert scale with “no change” corresponding to 0 points, “slightly” to 1 point, “somewhat” to 2 points, and “significantly” to 3 points, and was analyzed as a continuous variable. Note, where self-reported “significant” impact of the pandemic on symptoms is described in text, the word “significant” is placed in parentheses to distinguish this from references to statistical significance.
Subgroup analyses are presented by respondent type (PwP self-reports or CP proxy reports), duration of PD (<5 years, 5–10 years, and >10 years), and the level of social support from outside of home or primary relationship during the COVID-19 pandemic (decreased, the same as pre-pandemic, or increased). Due to the small proportion of respondents experiencing an increase in social support during the pandemic, the last two categories were collapsed as “maintained social support from outside of home or primary relationship”. Under the assumption that Likert scale scores did not follow normal distribution, subgroup analyses utilized non-parametric methods. Wilcoxon rank-sum test was used for pairwise comparisons across respondent groups with a dichotomous classification (PwP vs CP, decreased vs maintained social support from outside of the household) and Kruskal–Wallis test was used for those groups with an ordinal classification (duration of PD). No adjustment for multiple comparisons was performed.
Due to a technical glitch, the survey was terminated early for 124 participants. A sensitivity analysis was performed in these partial responders, showing no significant difference from the primary analysis including all respondents. Therefore, results from the total respondent sample are presented in this manuscript.
Results
Participant Characteristics
Among 7109 invited participants, 718 responded to the survey, resulting in an overall response rate of 10.1%. Most respondents were PwP (n=507, 70.6%). CP providing proxy responses constituted approximately a third of the surveyed group (n=211, 29.4%). Respondent demographics are presented in Table 1. More than half of the respondents (61.4%) were aged >70 years and CP were significantly older than PwP (p=0.006, Chi-square test). Both genders were represented to a similar extent among PwP but, compared with PwP, CP were significantly more likely to be female (p<0.0001, Chi-square test). PD duration was significantly longer when reported by CP proxy respondents than for PwP self-respondents (p<0.0001, Chi-square test).
 |
Table 1 Demographic and Disease Characteristics of Survey Respondents |
Social Support During the COVID-19 Pandemic
Decreased social support from outside of the home or primary relationship during the COVID-19 pandemic was reported by 58.5% of respondents, while 31.1% of respondents stated that the level of support was the same as pre-pandemic and 10.5% experienced increased support. With regards to other types of social support, 20.2% of respondents reported decreased ability to rely on someone they could count on if they needed help. Similar proportions of respondents reported decreased ability reach out to someone on hard days (24.4%) and decreased ability to contact their PD medical provider (22.3%). Overall, respondents reported a decline in social support from outside of the home or primary relationship significantly more often than a decline in other types of social support (p<0.0001 for all comparisons, pairwise sign test).
COVID-19 Disease Experience
In terms of direct experience of COVID-19 disease, 41.6% of respondents reported that COVID-19 impacted them, their family, or their support group. Nearly a quarter of respondents (23.2%) stated that they, or someone in their family or support group, had been diagnosed with COVID-19 and 6.4% reported COVID-related deaths in their family or support group.
Mood Symptoms
An increase of any magnitude in sadness and depression during the COVID-19 pandemic was reported by 69.6% of respondents (70.7% among PwP and 66.9% among CP), while a “significant” increase in sadness and depression was reported by 16.5% of respondents (19.0% among PwP and 10.5% among CP) (Figure 1). An increase in anxiety during the pandemic was reported by 65.5% of respondents (63.1% among PwP and 71.3% among CP). The increase in anxiety was considered to be “significant” by 13.1% of respondents (12.1% among PwP and 15.5% among CP) (Figure 1). While increase in sadness and depression was reported significantly more often by PwP than CP (p=0.0183), the reverse applied to anxiety (p=0.0092).
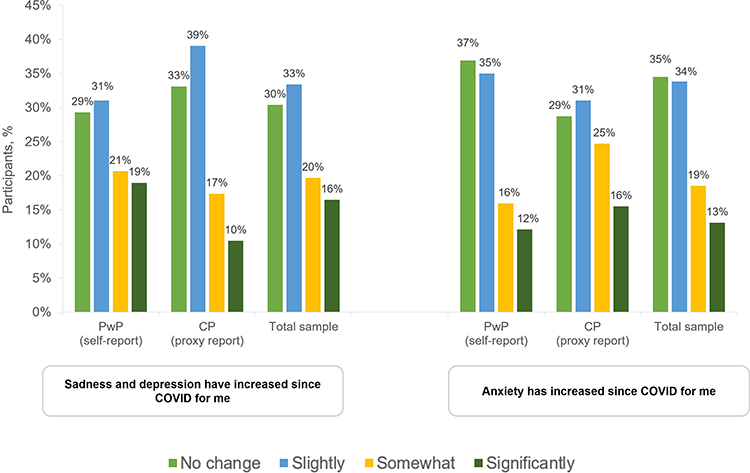 |
Figure 1 Change in sadness and depression (left panel) and anxiety (right panel) during the COVID-19 pandemic as reported by PwP, CP, and the total sample. |
Decreased social support from outside of their home or primary relationship during the COVID-19 pandemic was significantly associated with increased levels of both sadness and depression and anxiety, compared with maintained levels of social support (p<0.0001 for both comparisons, Figure 2). In contrast, duration of PD was not significantly associated with changes in sadness and depression (p=0.2078) or anxiety (p=0.5208) (data not shown).
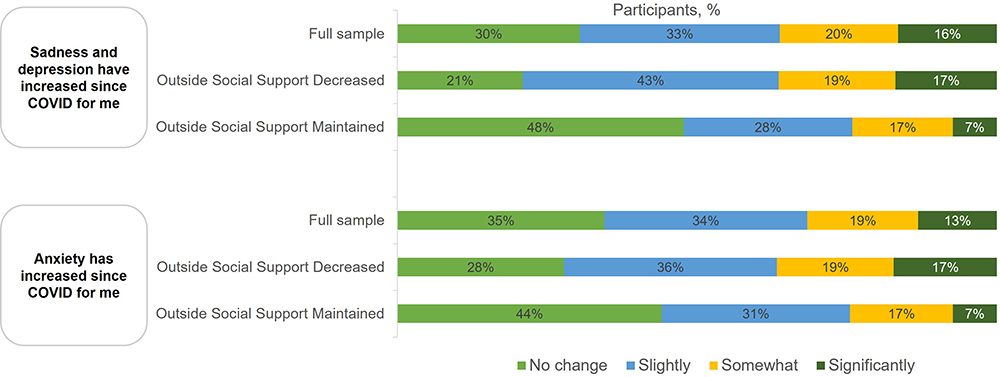 |
Figure 2 Association between the change in social support from outside of the home or primary relationship during the COVID-19 pandemic and sadness and depression (top panel) and anxiety (bottom panel). |
Other Non-Motor Symptoms
A decline in memory, problem solving, or communication during the COVID-19 pandemic was reported by 63.1% of respondents; 6.1% reported it to be “significant”. Other non-motor symptoms were less frequently exacerbated during the pandemic. New or worsening confusion was reported by 39.4% of respondents (considered to be “significant” in 5.2%), new or worsening hallucinations by 19.4% (“significant” in 4.4%), and new or worsening delusions by 16.2% (“significant” in 3.2%).
An increased burden of all four non-motor symptoms was significantly more likely to be reported by CP than by PwP (p<0.0001 for all symptoms, Figure 3).
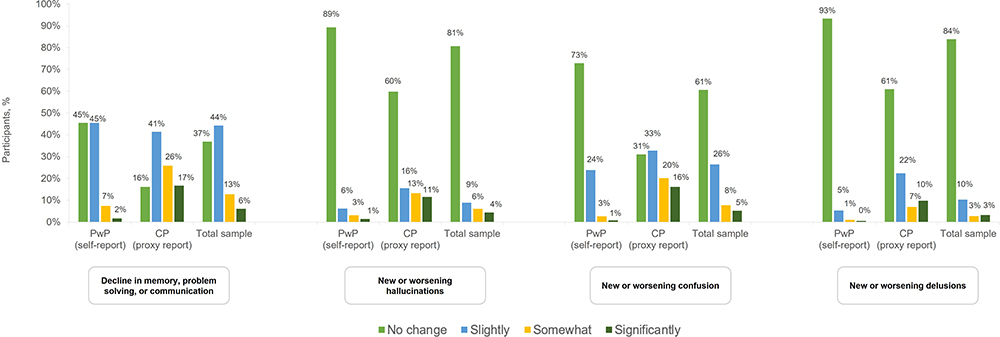 |
Figure 3 From left to right: 1) decline in memory, problem solving, or communication, 2) new or worsening hallucinations, 3) new or worsening confusion, 4) new or worsening delusions during the COVID-19 pandemic as reported by PwP, CP, and the total respondent sample. |
Decreased social support from outside of the home or primary relationship was significantly associated with decline in memory, problem solving, or communication (p=0.0009), new or worsening confusion (p<0.0001), and new or worsening delusions (p=0.018) (Figure 4). There was no significant association between a decline in this type of social support and the onset of new worsening of hallucinations (p=0.1278) (Figure 4). Longer duration of PD was associated with a significant worsening of all non-motor symptoms assessed (data not shown).
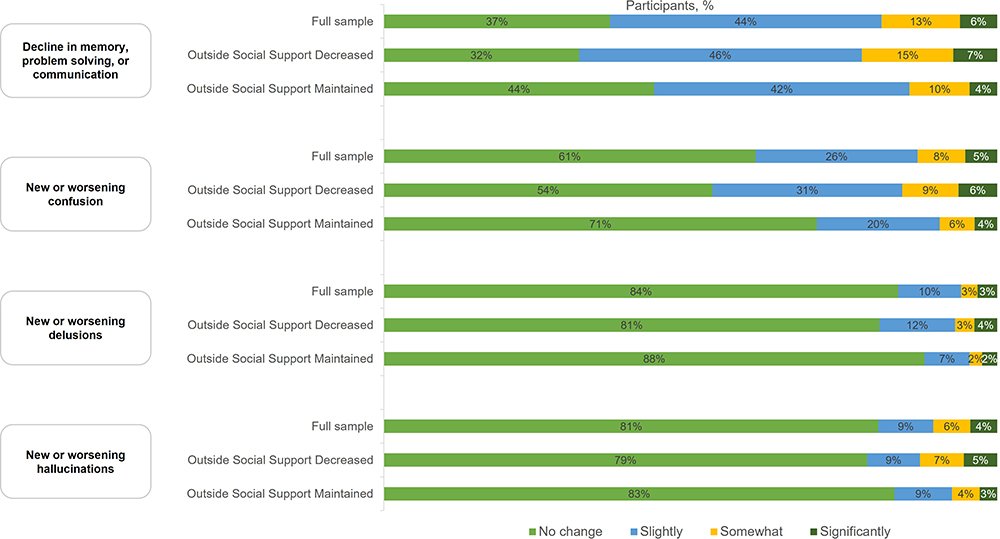 |
Figure 4 Association between the change in social support from outside of the home or primary relationship during the COVID-19 pandemic and, from top to bottom: 1) decline in memory, problem solving, or communication, 2) new or worsening confusion, 3) new or worsening delusions, 4) new or worsening hallucinations. |
Motor Symptoms
Motor symptoms reported in the survey are summarized in Figures 5 and 6. Change in motor symptoms, including new challenges or worsening symptoms of PD, decline in managing everyday activities, worsening sense of balance, more frequent falls, and difficulty maintaining regular exercise were reported significantly more often by CP than PwP (p<0.0001 for all comparisons, Figure 5).
 |
Figure 5 From left to right: 1) new challenges or worsening symptoms, 2) decline in managing everyday activities, 3) worsening sense of balance, 4) more frequent falls, and 5) difficulty maintaining regular exercise during the COVID-19 pandemic as reported by PwP, CP, and the total respondent sample. |
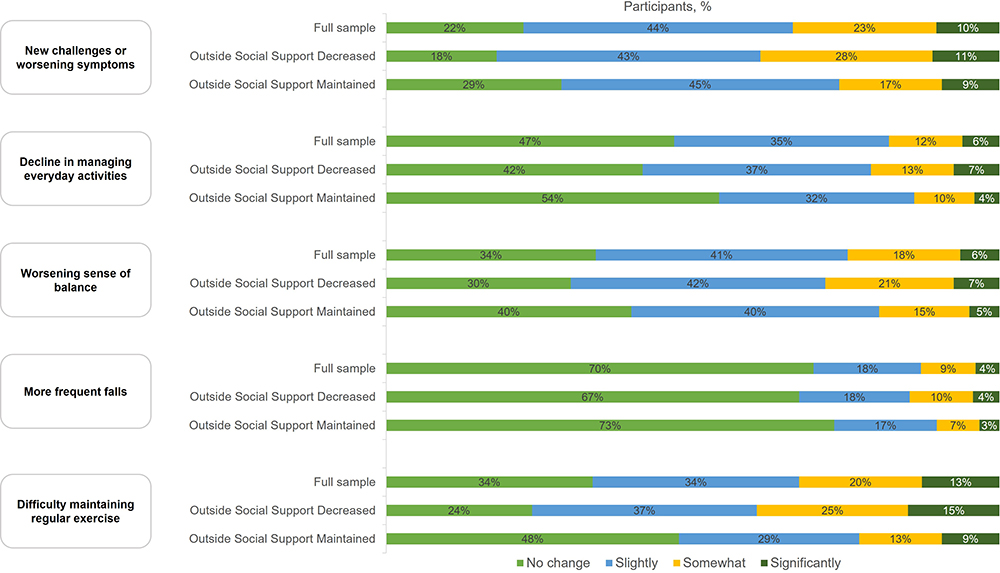 |
Figure 6 Association between the change in social support from outside of the home or primary relationship during the COVID-19 pandemic and, from top to bottom: 1) new challenges or worsening symptoms, 2) decline in managing everyday activities, 3) worsening sense of balance, 4) more frequent falls, and 5) difficulty maintaining regular exercise. |
Decreased social support from outside of the home or primary relationship was significantly associated with worsening of all motor symptoms studied except for an increase in the frequency of falls (Figure 6). Longer duration of PD was significantly associated with worsening of all motor symptoms assessed (data not shown).
Discussion
This study provides insights into the impact of the COVID-19 pandemic and the associated social restrictions on the symptoms of PD, as reported by PwP themselves or through CP proxies. The respondents reported a decline in social support from outside the home or primary relationship since the beginning of pandemic-related restrictions in April 2020 significantly more often than a decline in other forms or social support. Decreased social support from outside of the home or primary relationship was significantly associated with worsening mood symptoms (sadness/depression and anxiety), worsening of memory, problem solving, or communication, and worsening confusion and delusions.
Less than a quarter of respondents experienced a COVID-19 diagnosis themselves or within their close circle, and few reported COVID-related deaths in their family or support group. The worsening of PD symptoms reported in the survey could therefore be attributed mostly to the isolation and decreased social support during the pandemic rather than to the impact of COVID-19 disease itself.
In line with previous reports on PwP experience during COVID-related social restrictions, respondents to this survey reported reduced participation in regular exercise or rehabilitation during the pandemic,17,19,20 which can be expected to have a detrimental effect on PD symptoms, given the well-established benefits of physical exercise in PwP.21,22 Furthermore, the high prevalence of sadness/depression and anxiety, as well as general worsening of PD symptoms reported in this study is similar to the results from an online survey conducted in the US by the Parkinson’s Foundation and Columbia University Parkinson’s Disease Center of Excellence17 and from an online survey of community-dwelling PwP in Israel.20 Another online survey, conducted by the European Patient Forum, suggests that the feeling of anxiety and social isolation as well as experiencing challenges due to the pandemic, are shared by the wider population of people with health conditions.23
Progression of non-motor symptoms of PD does not necessarily follow motor deterioration24 and, given the burden non-motor symptoms pose on PwP8,9 and caregivers,10,11 increased attention towards prompt recognition and treatment of non-motor symptoms during the COVID-19 pandemic is warranted. PwP were generally less likely than CP proxies to report increased PD symptoms, but the difference was particularly prominent for non-motor symptoms. This suggests that PwP may under-recognize and/or under-report increases in non-motor symptoms. Engaging CPs during the visits could also improve the detection of non-motor symptoms. CPs have a detailed overview of the condition of the PwP under their care and may be able to provide a more accurate picture of PD symptoms and the effects of treatment than PwP themselves, particularly where symptoms such as apathy, cognitive impairment, or depression arise.25 Clinical experience of the authors also suggests that there is a reluctancy from both patients and providers to initiate new treatments during the pandemic-related restrictions limiting face-to-face health care visits. It is plausible that this reluctance to step-up treatment could also impact on non-motor and mood symptoms reported in this survey.
The findings of the survey reinforce previously established concepts on the wide ranging impact that social isolation has on physical and mental health, particularly among the elderly.26–28 PwP, already at risk for neuropsychiatric symptoms, may be especially susceptible to the consequences of reduced social connection and resultant loneliness. Indeed, a telephone study of PwP living in Luxembourg reported that, during the pandemic-related restrictions, PwP experienced unmet need associated with both the need to find alternative measures of pursuing normal daily activities participation in physiotherapy).29
Non-motor symptoms of PD profoundly add to caregiver burden, adversely affect caregivers’ mental health,10,11,30,31 and are associated with a reduced CP satisfaction from their relationship with the PwP.32 The increase in delusions and hallucinations reported by PwP in this survey are particularly worrisome, since, in addition to frequent hospitalizations and falls,33 it is these symptoms that have been found to be the main reason for placement in a long-term care facility.34 The reduced social support from outside of the household during the pandemic may contribute substantially to caregiver burnout and concerns about their own wellbeing, in addition to affecting PwPs care. All these factors have also been reported to contribute to the transition of the PwP to an institutional long-term care facility.33 It is therefore crucial that routine clinical follow-up in PD includes a thorough assessment of non-motor symptoms, particularly in PwP experiencing social isolation which may predispose to non-motor symptom intensification.
The results of the current study shed light on the impact that social isolation in general may have on PD symptoms, highlighting the need for ongoing engagement of PwP through patient organizations and encouragement of social activity by healthcare providers. While the scope of activities available to PwP and their CP is different than pre-pandemic, patient organizations stepped in to offer a number of activities, many of which lived past the height of the pandemic-related restrictions. These include web-based educational programs, online support groups, and virtual exercise groups, supplemented with training on online conferencing platforms that enables PwP and CP to take part in the aforementioned activities. Many health clinics also enable online access to medical providers and complementary therapies. However, it should be noted that while PwP enrolled in prior studies have expressed high levels of satisfaction with virtual medical provider visits conducted in the research setting,35,36 future research remains to determine if virtual support group meetings have the same benefits as meetings conducted in person.
Limitations of this survey include a restricted number of symptoms captured (eg gastrointestinal, sleep, and urinary symptoms were not included), and the fact that utilization of healthcare (including telemedicine, tele-rehabilitation, and complementary therapy) and medication adherence during the pandemic were not assessed, so that their impact on reported symptoms or their role as means of reducing social isolation remain unknown. Furthermore, CP and PwP pairs were not surveyed, which should be taken into account when interpreting the results. There was a significant association between longer PD duration and worsening of all motor and non-motor symptoms and PD duration reported by CP proxies was significantly longer than that self-reported by PwP. As PwP and CPs did not necessarily belong to the same family units, there is a possibility that some of the CP responses reflect more severely ill patients unable to fill in the survey themselves. This notion, however, could not be directly evaluated, as information on clinical features of PD, including symptom severity, was not collected as part of the survey. While PD duration was collected, disease duration alone is not an accurate proxy for severity, particularly regarding non-motor symptoms, which have been reported to progress slowly over >4 years and with different patterns of progression between individual symptoms.37–39 Finally, the real-world, descriptive nature of the study does not allow a definite causative effect between social isolation and PD symptom worsening to be established.
Strengths of the present survey include large respondent population and high relevance to PD care during and beyond the COVID-19 pandemic. As the social isolation habits acquired during the COVID-19 pandemic may persist beyond the duration of the restrictions, the results of the present survey draw attention into the likely challenges in PD care in the coming years and call for increased vigilance towards non-motor symptoms of PD.
Conclusion
During the COVID-19 pandemic, PwP experienced a decline in social support, which showed a statistically significant and negative association with the burden of mood and non-motor symptoms of PD, including neuropsychiatric symptoms. These results call for increased vigilance towards non-motor symptoms in PwP experiencing social isolation, with the aim to recognize and treat them promptly in order to reduce the burden they pose. They also highlight the need for stronger provider focus on encouraging PwP and their CPs to build and maintain social connections and engagements.
Abbreviations
CP, Care Partners; PD, Parkinson’s Disease; PMD Alliance, Parkinson and Movement Disorders Alliance; PwP, People with Parkinson’s Disease.
Ethics
The survey was fully anonymous, and the investigators did not collect any identifiable information on the respondents. Therefore, according to the US regulation 45 CFR §46.104d, this study meets the criteria for exemption from the policy regulating Institutional Review Board (IRB) approval. As no additional organizational policies of PMD Alliance required an IRB approval, this was not sought. Completion of the survey was considered as informed consent to participate.
Acknowledgments
Medical writing and editorial assistance with the preparation of this manuscript was provided by Karolina Badora, PhD of Maple Health Group and sponsored by Acadia Pharmaceuticals Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the submission to Neuropsychiatric Disease and Treatment; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by ACADIA Pharmaceuticals Inc.
Disclosure
NH received honoraria for Speakers Bureau from AbbVie, Acadia, Allergan, and Amneal, as well as honorarium for advisory board participation from AbbVie. YTY is an IP/Patent Holder for Mindsquare Technology, and received consulting fees from AbbVie, Acorda, Amneal, Acadia, Abbott, Sunovion, Teva, US World Meds, and Biogen. SG received honoraria for Speakers’ Bureau from AbbVie, Abbott, Amneal, and Sunovion. MCO has served as a consultant and/or speaker for AbbVie, Amneal, Acorda, Kyowa Kirin, Neurocrine, Supernus, Synovian, Teva, and Adamas. KP received honoraria for Speakers Bureau for Amneal, Acorda Therapeutics, and AbbVie. DM is a full-time employee of Acadia Pharmaceuticals. KM was a full-time employee of Acadia Pharmaceuticals at the time this work was conducted. SJ, JAR, and SM have no conflicts of interest to report.
References
1. Global Burden of Disease Study 2019. GBD results tool. Available from: http://ghdx.healthdata.org/gbd-results-tool?params=gbd-api-2019-permalink/edb233ab1438d2d99368d7bf1ee6c3ea.
2. Dorsey ER, Sherer T, Okun MS, Bloem BR. The emerging evidence of the Parkinson pandemic. J Parkinsons Dis. 2018;8(s1):S3–S8. doi:10.3233/JPD-181474
3. Armstrong MJ, Okun MS. Diagnosis and treatment of Parkinson disease: a review. JAMA. 2020;323(6):548–560. doi:10.1001/jama.2019.22360
4. Samudra N, Patel N, Womack KB, Khemani P, Chitnis S. Psychosis in Parkinson disease: a review of etiology, phenomenology, and management. Drugs Aging. 2016;33(12):855–863. doi:10.1007/s40266-016-0416-8
5. Sveinbjornsdottir S. The clinical symptoms of Parkinson’s disease. J Neurochem. 2016;139(Suppl 1):318–324. doi:10.1111/jnc.13691
6. Forsaa EB, Larsen JP, Wentzel-Larsen T, et al. A 12-year population-based study of psychosis in Parkinson disease. Arch Neurol. 2010;67(8):996–1001. doi:10.1001/archneurol.2010.166
7. Vescovelli F, Sarti D, Ruini C. Well-being and distress of patients with Parkinson’s disease: a comparative investigation. Int Psychogeriatr. 2019;31(1):21–30. doi:10.1017/s1041610217002575
8. Tibar H, El Bayad K, Bouhouche A, et al. Non-motor symptoms of Parkinson’s disease and their impact on quality of life in a cohort of Moroccan patients. Front Neurol. 2018;9:170. doi:10.3389/fneur.2018.00170
9. D’Iorio A, Vitale C, Piscopo F, et al. Impact of anxiety, apathy and reduced functional autonomy on perceived quality of life in Parkinson’s disease. Parkinsonism Relat Disord. 2017;43:114–117. doi:10.1016/j.parkreldis.2017.08.003
10. Mantri S, Klawson E, Albert S, et al. The experience of care partners of patients with Parkinson’s disease psychosis. PLoS One. 2021;16(3):e0248968. doi:10.1371/journal.pone.0248968
11. Martinez-Martin P, Rodriguez-Blazquez C, Forjaz MJ, et al. Neuropsychiatric symptoms and caregiver’s burden in Parkinson’s disease. Parkinsonism Relat Disord. 2015;21(6):629–634. doi:10.1016/j.parkreldis.2015.03.024
12. Perepezko K, Hinkle JT, Shepard MD, et al. Social role functioning in Parkinson’s disease: a mixed-methods systematic review. Int J Geriatr Psychiatry. 2019;34(8):1128–1138. doi:10.1002/gps.5137
13. Hitchcott PK, Fastame MC, Corona F, et al. Self-reported physical and mental health and motor functioning in elders with and without Parkinson’s disease. Psychol Health Med. 2019;24(7):788–798. doi:10.1080/13548506.2019.1574355
14. Quadt L, Esposito G, Critchley HD, Garfinkel SN. Brain-body interactions underlying the association of loneliness with mental and physical health. Neurosci Biobehav Rev. 2020;116:283–300. doi:10.1016/j.neubiorev.2020.06.015
15. Park C, Majeed A, Gill H, et al. The effect of loneliness on distinct health outcomes: a comprehensive review and meta-analysis. Psychiatry Res. 2020;294:113514. doi:10.1016/j.psychres.2020.113514
16. Centers for Disease Control and Prevention. COVID-19. People with certain medical conditions. 2022. Available from: https://www.cdc.gov/coronavirus/2019-ncov/need-extra-precautions/people-with-medical-conditions.html.
17. Feeney MP, Xu Y, Surface M, et al. The impact of COVID-19 and social distancing on people with Parkinson’s disease: a survey study. NPJ Parkinson’s Dis. 2021;7(1):10. doi:10.1038/s41531-020-00153-8
18. PMD Alliance. Virtual support groups. 2022. Available from: https://www.pmdalliance.org/virtual-support-groups/.
19. Cavallieri F, Sireci F, Fioravanti V, et al. Parkinson’s disease patients’ needs during the COVID-19 pandemic in a red zone: a framework analysis of open-ended survey questions. Eur J Neurol. 2021;28(10):3254–3262. doi:10.1111/ene.14745
20. Yogev-Seligmann G, Kafri M. COVID-19 social distancing: negative effects on people with Parkinson disease and their associations with confidence for self-management. BMC Neurol. 2021;21(1):284. doi:10.1186/s12883-021-02313-6
21. Bhalsing KS, Abbas MM, Tan LCS. Role of physical activity in Parkinson’s disease. Ann Indian Acad Neurol. 2018;21(4):242–249. doi:10.4103/aian.AIAN_169_18
22. Fayyaz M, Jaffery SS, Anwer F, Zil-E-Ali A, Anjum I. The effect of physical activity in Parkinson’s disease: a mini-review. Cureus. 2018;10(7):e2995–e2995. doi:10.7759/cureus.2995
23. European Patients Forum. Survey report. The impact of the COVID-19 pandemic on patients and patient organisations. Available from: https://www.eu-patient.eu/globalassets/covid19-survey-report_final.pdf.
24. Antonini A, Barone P, Marconi R, et al. The progression of non-motor symptoms in Parkinson’s disease and their contribution to motor disability and quality of life. J Neurol. 2012;259(12):2621–2631. doi:10.1007/s00415-012-6557-8
25. Hiseman JP, Fackrell R. Caregiver burden and the nonmotor symptoms of Parkinson’s disease. Int Rev Neurobiol. 2017;133:479–497. doi:10.1016/bs.irn.2017.05.035
26. Düzel S, Drewelies J, Gerstorf D, et al. Structural brain correlates of loneliness among older adults. Sci Rep. 2019;9(1):13569. doi:10.1038/s41598-019-49888-2
27. Cacioppo JT, Cacioppo S, Capitanio JP, Cole SW. The neuroendocrinology of social isolation. Annu Rev Psychol. 2015;66:733–767. doi:10.1146/annurev-psych-010814-015240
28. Prohaska T, Burholt V, Burns A, et al. Consensus statement: loneliness in older adults, the 21st century social determinant of health? BMJ Open. 2020;10(8):e034967. doi:10.1136/bmjopen-2019-034967
29. Hanff AM, Pauly C, Pauly L, et al. Unmet needs of people with Parkinson’s disease and their caregivers during COVID-19-related confinement: an explorative secondary data analysis. Front Neurol. 2020;11:615172. doi:10.3389/fneur.2020.615172
30. Oh Y-S, Lee JE, Lee PH, Kim J-S. Neuropsychiatric symptoms in Parkinson’s disease dementia are associated with increased caregiver burden. JMD. 2015;8(1):26–32. doi:10.14802/jmd.14019
31. Smith ER, Perrin PB, Tyler CM, Lageman SK, Villaseñor T. Parkinson’s symptoms and caregiver burden and mental health: a cross-cultural mediational model. Behav Neurol. 2019;2019:1396572. doi:10.1155/2019/1396572
32. Heine J, von Eichel H, Staege S, Höglinger GU, Wegner F, Klietz M. Relationship satisfaction in people with Parkinson’s disease and their caregivers: a cross-sectional observational study. Brain Sci. 2021;11(6):822. doi:10.3390/brainsci11060822
33. Jensen I, Lescher E, Stiel S, Wegner F, Höglinger G, Klietz M. Analysis of transition of patients with Parkinson’s disease into institutional care: a retrospective pilot study. Brain Sci. 2021;(11):11. doi:10.3390/brainsci11111470
34. Goetz CG, Stebbins GT. Risk factors for nursing home placement in advanced Parkinson’s disease. Neurology. 1993;43(11):2227–2229. doi:10.1212/wnl.43.11.2227
35. Myers TL, Tarolli CG, Adams JL, et al. Video-based Parkinson’s disease assessments in a nationwide cohort of Fox insight participants. Clin Parkinsonism Relat Disord. 2021;4:100094. doi:10.1016/j.prdoa.2021.100094
36. Tarolli CG, Andrzejewski K, Zimmerman GA, et al. Feasibility, reliability, and value of remote video-based trial visits in Parkinson’s disease. J Parkinsons Dis. 2020;10(4):1779–1786. doi:10.3233/jpd-202163
37. Ayala A, Triviño-Juárez JM, Forjaz MJ, Rodríguez-Blázquez C, Rojo-Abuin J-M, Martínez-Martín P. Parkinson’s disease severity at 3 years can be predicted from non-motor symptoms at baseline. Front Neurol. 2017;8. doi:10.3389/fneur.2017.00551
38. Erro R, Picillo M, Vitale C, et al. The non-motor side of the honeymoon period of Parkinson’s disease and its relationship with quality of life: a 4-year longitudinal study. Eur J Neurol. 2016;23(11):1673–1679. doi:10.1111/ene.13106
39. Chen Y-C, Chen R-S, Weng Y-H, et al. The severity progression of non-motor symptoms in Parkinson’s disease: a 6-year longitudinal study in Taiwanese patients. Sci Rep. 2021;11(1):14781. doi:10.1038/s41598-021-94255-9
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.