")
Back to Journals » International Journal of Women's Health » Volume 14
Impact of Female Stress Urinary Incontinence on Quality of Life, Mental Health, Work Limitation, and Healthcare Seeking in China, Taiwan, and South Korea (LUTS Asia): Results from a Cross-Sectional, Population-Based Study
Authors Chow PM, Chuang YC, Hsu KCP, Shen YC , Liu SP
Received 25 July 2022
Accepted for publication 17 November 2022
Published 28 December 2022 Volume 2022:14 Pages 1871—1880
DOI https://doi.org/10.2147/IJWH.S383651
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Po-Ming Chow,1 Yao-Chi Chuang,2 Karina Chin Po Hsu,3 Yuan-Chi Shen,2 Shih-Ping Liu1
1Department of Urology, National Taiwan University Hospital and College of Medicine, Taipei, Taiwan; 2Department of Urology, Kaohsiung Chang Gung Memorial Hospital, Chang Gung University College of Medicine, Kaohsiung, Taiwan; 3Medical Affairs Department, Former Employee of Astellas Pharma Taiwan, Inc., Taipei, Taiwan
Correspondence: Shih-Ping Liu, Department of Urology, National Taiwan University Hospital and College of Medicine, No. 7, Chung Shan South Road, Taipei, 10002, Taiwan, Tel +886 2 2312-3456 ext. 62135, Fax +886 2 2321-9145, Email [email protected]
Background: Stress urinary incontinence (SUI) is common among adult women with negative effects on psychosocial well-being, mental health, and health-related quality of life. The purpose of the research is to determine if SUI in women is a factor implicated in changes in health-related quality of life (HRQoL) in both physical and mental health domains and in work difficulties.
Methods: Data of women 40 years or older from a cross-sectional, population-based, internet survey were examined post-hoc. The effect of SUI frequency on HRQoL (SF12 score), in physical and mental health domains, was assessed. In addition, multivariate and univariate analyses were used to show the influence of SUI on HADS (Hospital Anxiety and Depression Scale) depression score and HADS anxiety score. The effects of demographic factors and physical ailments and SUI on work difficulties were similarly analyzed using multivariate logistic regression.
Results: A total of 4208 women with mean age of 60 were included in the analysis. The more frequent SUI episodes were associated with a greater reduction of HRQoL in both physical and mental health domains. In addition, both multivariate and univariate analyses showed that SUI could be correlated with a negative effect on HADS anxiety score (OR 1.617, CI 1.335– 1.958, p=0.000) and HADS depression score (OR 1.263, CI 1.044– 1.527, p=0.016). Univariate analyses suggested that work difficulties were correlated with SUI. Available data revealed that many sufferers, including up to 40% of individuals with SUI frequency rating 1 (less than once a month) to 3 (a few times a week), failed to seek treatment.
Conclusion: SUI, common in women ≥ 40 years of age, impairs quality of life in both physical and mental health domains. SUI is an independent risk factor for anxiety and depression and has been linked to significant work dysfunctions.
Trial Registration: This study is registered at ClinicalTrials.gov: NCT02618421 (Date of registration: December 1, 2015).
Keywords: stress urinary incontinence, quality of life, China, South Korea, Taiwan
Plain Language Summary
This is a summary of a secondary analysis of an internet-based survey called LUTS Asia. In total, 8284 adults aged at least 40 years from China, Taiwan and South Korea took part in the one-time survey. The purpose of the survey was to determine how commonly adults experience bother originating in the lower urinary system. A key type of lower urinary bother is called stress urinary incontinence, and it is common in women. The current research aimed to aid the understanding about how stress urinary incontinence affects quality of life and mental health and diminishes work productivity among the female respondents included in the LUTS Asia survey.
Research results showed that stress urinary incontinence was the reason the affected women experienced anxiety and depression. In addition, the more severe the symptoms of stress urinary incontinence were, the more negative impact to both physical and mental aspects of health-related quality of life was seen. Analyses also showed that stress urinary incontinence tended to negatively affect work productivity. Despite these unfavorable effects, many women with stress urinary incontinence still do not seek behavioral counselling or medical treatments that may improve their condition.
Introduction
Stress urinary incontinence (SUI) is the complaint of involuntary leakage of urine on exertion, sneezing or coughing1 and is linked to major negative economic, emotional and health-related quality of life issues.2,3 The condition occurs when the pelvic floor muscles that support the urethra weaken or the urinary sphincter muscles that control the release of urine lose strength. Vaginal delivery is one factor predisposing to SUI; additional risk factors include age, body weight, and hysterectomy. Most women with incontinence, including SUI, have been shown to improve with either pharmacologic or nonpharmacologic treatments.4,5
Large cohort studies for female SUI, however, are scarce. An earlier EpiLUTS study,3 published in 2009, from the US, UK, and Sweden, was a large cohort study that provided comprehensive data correlating lower urinary tract symptoms (LUTS) to various aspects of quality of life, but it did not offer a correlation of the physical aspects of health-related quality of life with SUI. Other large studies of patients with LUTS likewise have not provided a separate analysis of SUI; these include the EPIC study, released in 2006;6 a 2006 UK study of women visiting primary care providers;7 and a more recent research based on the Brazil LUTS database.8
The current database (LUTS Asia) provides data on LUTS in males and females and can be analyzed to provide information highlighting the impact of female SUI on quality of life, mental health, work limitation, and healthcare seeking behaviors. Leveraging the LUTS Asia database, this study attempted to elaborate on the impact of female SUI on the psychosocial wellbeing of those affected. A significant advantage of LUTS Asia is that confounding factors such as age, diabetes, hypertension, and hyperlipidemia (see Tables 1 and 2 and Supplementary Table 1) can be controlled.
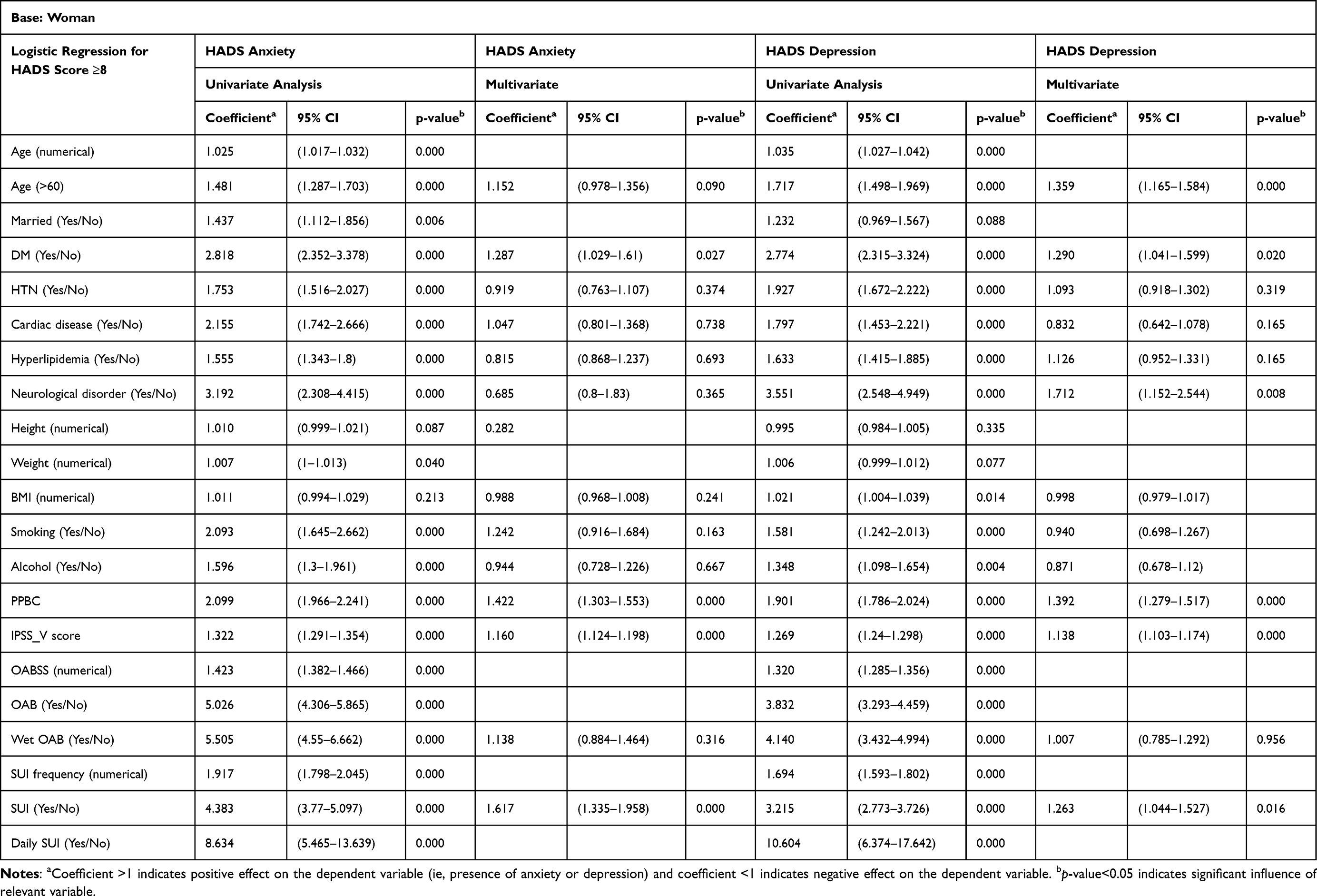 |
Table 1 Univariate and Multivariate Logistic Regression Analysis of Factors Determining HADS Score ≥8 |
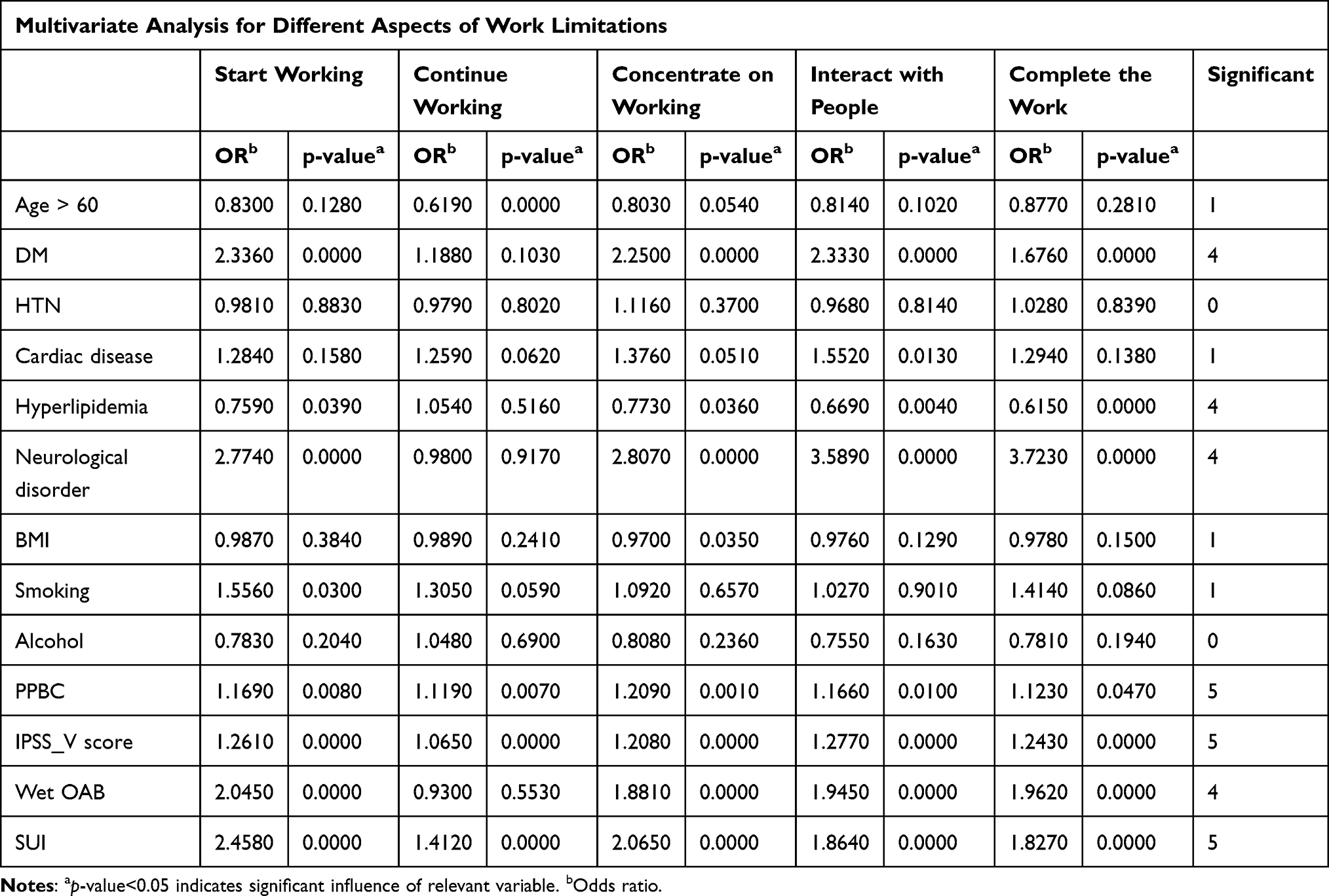 |
Table 2 Impact on Work Limitations |
This analysis took the women cohort (51% of 8284 male and female participants) included in the cross-sectional, population-based study of LUTS in China, South Korea, and Taiwan. The study aimed to evaluate prevalence of female SUI, to determine whether SUI in women is an effector of changes in health-related quality of life (HRQoL) in both the physical and mental domains and in work difficulties, and to analyze healthcare seeking behaviors.
Methods
Study Design
An internet-based survey was conducted in 2015 in a cross-sectional, population-based study group comprising individuals at least 40 years.9 Exclusion criteria included pregnancy at the time of the survey and/or a urinary tract infection within the preceding month. Information about confidentiality and the voluntary nature of participation was included in the introduction to the survey, and informed consent was obtained from all patients being included in the study. The conduct of survey adhered to the principles of the Declaration of Helsinki.10 Quality checks and survey management were previously described by Chapple et al.9
Data Collection
Part of the general demographic information constituting the analysis included age and marital status. The following key general health and medical comorbidity data were collected: BMI, diabetes mellitus, hypertension, cardiac disease, hyperlipidemia, neurological disorder, smoking and alcohol consumption. Topics relating to LUTS were probed using established survey instruments, including the International Prostate Symptoms Score (IPSS), other International Continence Society (ICS) symptom questions (related to splitting/spraying, hesitancy, terminal dribble, urgency), the Overactive Bladder Symptom Score (OABSS), and a single-item global measure called the Patient Perception of Bladder Condition (PPBC). SUI, whose severity was scored from 1 to 5, was derived from Q31 in the questionnaire (see Supplementary Tables 2–4). Altogether, parameters derived from these survey tools included IPSS voiding subscore (IPSS_V), presence of wet OAB, PPBC and SUI score, all of which were considered pertinent risk factors for diminished quality of life, mental stress and impaired work productivity.
Other standard survey instruments used included the WLQ (Work Limitation Questionnaire – 8 items); generic HRQoL_SF12v2 (with the 12-item short form Health Survey version 2)11 and HADS (Hospital Anxiety and Depression Scale – 14 items).12 Further description of these survey instruments is provided in Appendix 1.
Primary and Secondary Outcomes
The primary outcome of the female SUI arm of LUTS Asia was the effect of SUI frequency on HRQoL, mental and emotional factors, and work difficulty. The specific dependent variables were three-fold: (1) HRQoL for the physical domain and HRQoL for the mental health domain; (2) HADS anxiety score (numerical) greater than or equal to 8 (categorical) and HADS depression score (numerical) greater than or equal to 8 (categorical); and (3) difficulty in working greater than or equal to 50% of the time as defined by Q46 in the questionnaire (see Supplementary Table 5).
The secondary outcomes were as follows: (1) to determine the effect of SUI on the adoption of various treatment options; (2) to reveal the effect of SUI on healthcare seeking behaviors; and (3) to delineate how often female SUI occurs by leakage-inducing movement.
Statistical Analysis
In the female SUI arm of this study, descriptive statistical analysis and multivariate and univariate logistic regression models were used to demonstrate how various risk factors deemed clinically relevant by the urologist investigators from the questionnaire, including SUI, PPBC, IPSS_V score and presence of wet OAB, influenced quality of life, work productivity, and mental health. The influence of important patient factors and SUI on the HADS anxiety and depression scores was correlated using logistic regression models. The confounders were controlled by multivariate analysis. Treatment seeking behaviors, both pharmacologic and nonpharmacologic, were delineated with logistic regression models. An analysis of how often SUI occurred in relation to leakage-inducing movements was also provided.
Results
Survey Sample
In the original LUTS Asia study, 7.0% of e-mail survey invitation recipients responded, 5.4% provided informed consent and 1.7%, which amounted to 8284 participants, ultimately completed the survey and constituted the final valid sample.9
Age
A total of 4208 women with mean age of 60 were included in the analysis. The overall prevalence of SUI in women greater than or equal to 40 years old was 23% (979/4208). The age distribution favors older women, and 42.3% of women with SUI in this study were greater than or equal to 60 years of age. The percentage of married women was higher in the SUI group, possibly related to childbirth, which is a major cause of SUI (see Supplementary Table 1). There was a clear increase in SUI prevalence and overall frequency with increasing age. Prevalence of SUI “a few times a month” or greater increased from 14% in women aged 40–44 years to 30% in women aged 50–59 years (Figure 1).
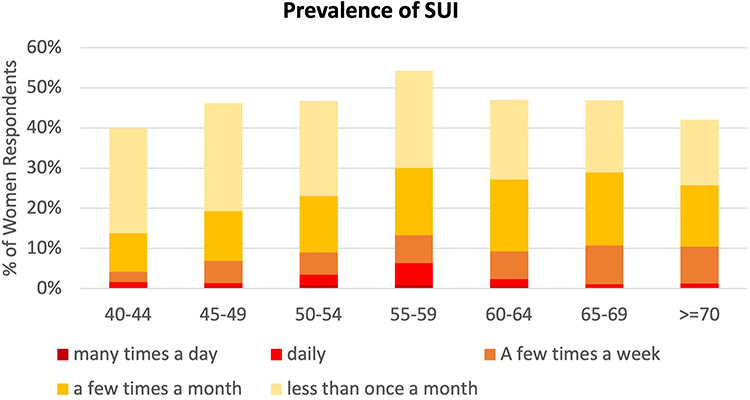 |
Figure 1 SUI prevalence by age group - highest frequency of any of the SUI. Abbreviation: SUI, stress urinary incontinence. |
Quality of Life
Study results showed that the quality of life, in both the physical and mental domains, was significantly affected by SUI. The average transformed SF12 score for the physical health domain decreased from 73 for women without SUI to 40 in women reporting SUI frequency of “many times a day”. Average transformed SF12 score for mental health domain decreased from 42 for women without SUI to 22 in women reporting SUI frequency of “many times a day” (Figure 2). The results of multivariate analyses indicated fewer factors with significant influence on HADS anxiety and depression scores, ie, SUI, PPBC score, IPSS-V score, and presence of diabetes. Age and presence of neurological disorder were significant factors with respect to depression, but not anxiety (Table 1).
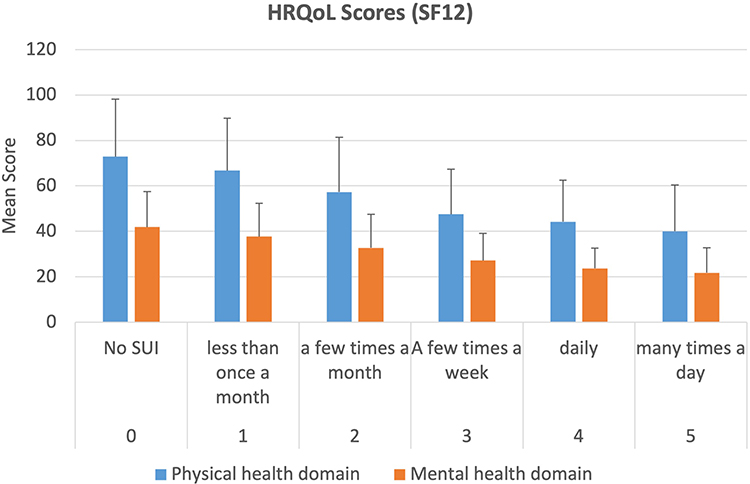 |
Figure 2 Avg. transformed SF12 scores by highest frequency of any of the SUI. The SF-12 is a general HRQoL survey in the 12-item short form from Health Survey version 2, and it measures general health status in 8 domains (physical functioning, role limitations due to physical problems, bodily pain, general health, vitality, social functioning, role limitations due to emotional problems, and mental health).10 Abbreviation: SUI, stress urinary incontinence. |
Work Limitation
SUI significantly impacted work limitation across WLQ measures. SUI, wet OAB, and neurological disorders showed the highest impact on work limitation in terms of starting working, continuing working, staying focused at work, interacting with people and completing work (Table 2).
Management Approaches
Utilization of prescription medications increased with the increase in frequency of SUI. Among participants showing 1–3 frequency rating of SUI, use of prescription medications was 27%; use of prescription medicines increased to 34% among participants reporting an SUI frequency rating of ≥4. Up to 40% of participants who reported SUI frequency rating of 1–3 did not follow any treatment/management approach (Figure 3).
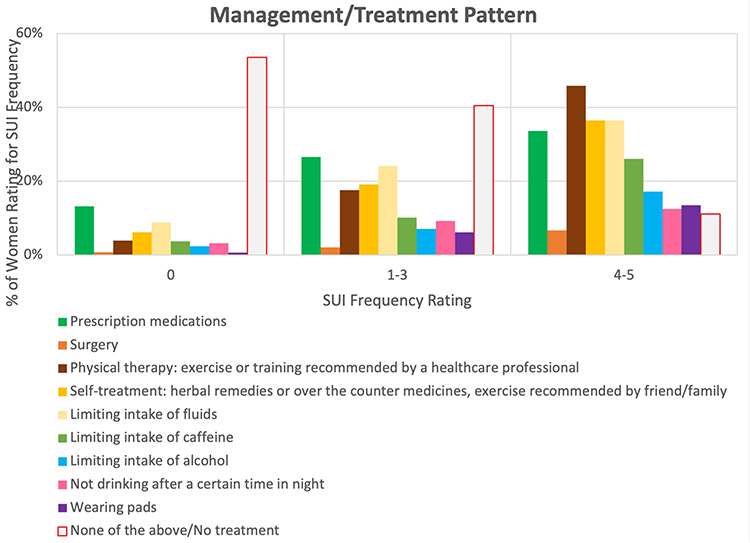 |
Figure 3 Frequency of SUI and management approaches. The definition of SUI frequency rating is as follow: 0 = “no SUI”, 1 = “less than once a month”, 2 = “a few times a month”, 3 = “A few times a week”, 4 = “daily”, 5 = “many times a day”. Abbreviation: SUI, stress urinary incontinence. |
Leakage-Inducing Movements
The role of various leakage-inducing movements in SUI is illustrated in Figure 4. The percentage of patients experiencing SUI symptoms many times a day, daily, a few times a week, or a few times a month was shown for each of the five leakage-inducing movements: sneezing, coughing, exercise, laughing, and lifting heavy objects. Sneezing and coughing are the more prominent triggers of incontinence, with a prevalence of 14% and 12%, respectively. Exercise, laughing, and lifting heavy objects, with prevalence of 7%, 5%, and 5%, respectively, played minor roles.
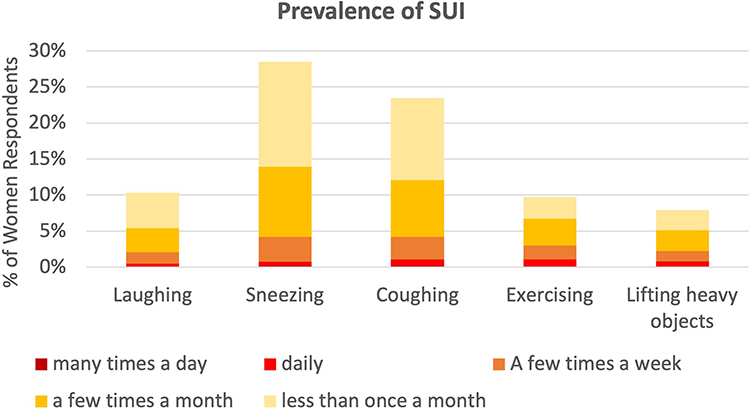 |
Figure 4 Frequency of SUI by leakage-inducing movement. Abbreviation: SUI, stress urinary incontinence. |
Discussion
The results of this post hoc analysis of 4208 women with LUTS in China, South Korea, and Taiwan showed that SUI reduced quality of life in both the physical and mental health domains and that the condition was an independent risk factor for anxiety and depression and could negatively impact work function.
Prevalence
SUI is a common condition in women ≥40 years of age, and in this analysis set of 4208 women, the overall prevalence was 23.3%. A similar overall prevalence of SUI of 25% was observed in a small study of women studying nursing.13 In women aged 50–59 years of age in the current analysis, the prevalence was highest at 30%, and SUI remained at high prevalence at 26–27% in women over 60 years old. In another large study from the USA, UK and Sweden, SUI occurred at high percentages in more than 4000 female patients; SUI from laughing, sneezing and coughing occurred in 55.9% of female patients and SUI from physical activities occurred in 28.3% of patients.14
Quality of Life
This study uniquely examined the impact of SUI on QoL issues from two-pronged vantage points of both physical and mental domains. A small-scale study involving 120 Malaysian women with SUI similarly showed that females suffering from the condition have significantly poorer quality of life compared with continent women when measured using both condition-specific and generic quality of life measures.15
Mental and Emotional Health: Anxiety and Depression
Comparable studies, not necessarily using the HADS, likewise showed the impact of SUI on emotional state. A recent controlled study of 177 women (80 patients with SUI and 97 control individuals) showed that women with SUI had a higher level of depression (50% vs 11%) and anxiety (29% vs 3.1%).16 In the large EpiLUTS study out of the US, UK, and Sweden, SUI was among the urinary tract conditions associated with increased anxiety and depression.17 In a third study of 275 women with SUI, nearly every third woman (28.7%) felt great mental discomfort related to the disease symptoms, 31.7% a considerable discomfort and 33.1% a moderate discomfort.18
Work Function
This study expectedly demonstrated that SUI has a significant impact on work function. In another study involving more than 2000 working women, 88% of those with more severe incontinence symptoms, including but not limited to SUI, reported at least some negative impact on concentration, performance of physical activities, self-confidence or the ability to complete tasks without interruption.19
Healthcare Seeking
Although SUI has major effects on quality of life, physical and mental health, and work functioning, in this analysis, up to 40% of female patients with a 1–3 SUI frequency rating did not seek treatment of any type. In the EpiLUTS study, patients with LUTS symptoms of any type sought treatment in fewer than one-third of instances.17 In both large studies of patients with LUTS, and specifically with SUI, many sufferers did not seek intervention that would have been likely to alleviate their symptoms.5 In addition, lack of apparent correlation between objective diagnostic findings of urodynamic voiding phase dysfunction, a common manifestation among female patients with SUI, and subjective complaints of LUTS20 would mean that chance of incidental diagnosis of SUI is low unless female patients bothered by the condition proactively seek medical intervention.
Strengths and Limitations
Strengths of the study included the large sample size and the use of well-validated instruments. Online surveys are suitable for extracting information on private, sensitive personal issues but also tend to favor individuals of higher socioeconomic status. An additional drawback was that information on prior medications was not collected as part of the LUTS Asia database. In addition to the general study design limitations described in the Chow et al paper,21 for this analysis of SUI in females, the exclusion of pregnant women meant that the time of vaginal delivery, often a particularly important determinant of female SUI, was not captured in the analysis. Since this study was a post-hoc secondary analysis, research was constrained by parameter availability and data quality of the original LUTS Asia database not purposely created for the current research question of interest. A critical facet of such constraint was the lack of comprehensive medical history from survey respondents, including surgical history, which hampered the attempt of risk factor analysis for SUI as it is well recognized that prior pelvic surgery is strongly linked to the development of SUI.
The lack of confirmed SUI diagnosis among survey respondents could cloud the interpretation of SUI as a culprit in reduction in QoL, decline in work productivity and relative passivity in seeking treatment. Our study indicates that QoL was clearly reduced with an increase in SUI frequency, and that the impact of SUI on work productivity is as significant as other factors, such as wet OAB and neurological disorders, in multivariate analysis. Probing of healthcare seeking behavior involved all aspects of urinary symptoms, which were confounders that could not be adjusted by statistical methods. Regardless if these patients might seek treatment for LUTS of other nature, we can still conclude that a large portion of women with SUI (with or without other LUTS) did not receive any management.
Conclusion
SUI is common in women over 40 years old. SUI has a negative impact on quality of life in both the physical and mental health domains. Along with some other urinary dysfunctions, it is an independent risk factor for anxiety and depression and may cause significant work limitations. Despite these negative effects, many women still do not seek pharmacologic or nonpharmacologic treatments for SUI and other LUTS that might improve their condition.
Abbreviations
BMI, body mass index; DM, diabetes mellitus; HADS, Hospital Anxiety and Depression Scale; HRQoL, health-related quality of life; HTN, hypertension; ICS, International Continence Society; IPSS_V score, International Prostate Symptom Score – voiding; IRB, Institutional Review Board; LUTS, lower urinary tract symptoms; PPBC, Patient Perception of Bladder Condition; OABSS, Overactive Bladder Symptoms Score; OAB, overactive bladder; SF12, a measure of HRQoL (with the 12-item short form Health Survey version 2); SUI, stress urinary incontinence; WLQ, Work Limitations Questionnaire.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article as Supplementary Information files.
Ethics Approval and Informed Consent
The National Taiwan University Hospital Research Ethics Committee waived the oversight of retrospective analyses using de-identified secondary database. The original survey was performed in compliance with Good Clinical Practice and the World Association for Social, Opinion and Market Research (ESOMAR) guidelines that enshrine legal and ethical considerations of consumer panel research. All procedures followed were in accordance with the Helsinki Declaration of 1964, as revised in 2013. Informed consent was obtained from all patients being included in the study.
Acknowledgments
The authors would like to thank Ravi Prakash Koni (Stratycon Business Solutions Pvt. Ltd., Bangalore, India) for statistical analyses. Medical writing support was provided by Adele S Lubell, PhD of St. John’s University, Queens, New York in collaboration with SDL.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by Astellas Pharma Singapore Pte Ltd. under a General Research Grant.
Disclosure
SP Liu has received research support from Astellas Pharma Singapore Pte. Ltd. KCP Hsu is a former employee of Astellas Pharma Taiwan, Inc. PM Chow, YC Chuang and YC Shen declare no conflicts of interest.
References
1. Abrams P, Cardozo L, Fall M, et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 2002;21(2):167–178. doi:10.1002/nau.10052
2. Chong EC, Khan AA, Anger JT. The financial burden of stress urinary incontinence among women in the United States. Curr Urol Rep. 2011;12(5):358–362. doi:10.1007/s11934-011-0209-x
3. Coyne KS, Sexton CC, Thompson CL, et al. The prevalence of lower urinary tract symptoms (LUTS) in the USA, the UK and Sweden: results from the Epidemiology of LUTS (EpiLUTS) study. BJU Int. 2009;104(3):352–360. doi:10.1111/j.1464-410X.2009.08427.x
4. Balk EM, Rofeberg VN, Adam GP, Kimmel HJ, Trikalinos TA, Jeppson PC. Pharmacologic and nonpharmacologic treatments for urinary incontinence in women: a systematic review and network meta-analysis of clinical outcomes. Ann Intern Med. 2019;170(7):465–479. doi:10.7326/M18-3227
5. Haylen BT, de Ridder D, Freeman RM, et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourol Urodyn. 2010;29(1):4–20. doi:10.1002/nau.20798
6. Irwin DE, Milsom I, Hunskaar S, et al. Population-based survey of urinary incontinence, overactive bladder, and other lower urinary tract symptoms in five countries: results of the EPIC study. Eur Urol. 2006;50(6):1306–14;discussion 1314–1315. doi:10.1016/j.eururo.2006.09.019
7. Shaw C, Gupta RD, Bushnell DM, et al. The extent and severity of urinary incontinence amongst women in UK GP waiting rooms. Fam Pract. 2006;23(5):497–506. doi:10.1093/fampra/cml033
8. Soler R, Gomes CM, Averbeck MA, Koyama M. The prevalence of lower urinary tract symptoms (LUTS) in Brazil: results from the epidemiology of LUTS (Brazil LUTS) study. Neurourol Urodyn. 2018;37(4):1356–1364. doi:10.1002/nau.23446
9. Chapple C, Castro-Diaz D, Chuang YC, et al. Prevalence of lower urinary tract symptoms in China, Taiwan, and South Korea: results from a cross-sectional, population-based study. Adv Ther. 2017;34(8):1953–1965. doi:10.1007/s12325-017-0577-9
10. World Medical Association. World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. World Medical Association; 2013:2191–2194.
11. Ware J, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
12. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
13. Opara J, Czerwinska-Opara WE. The prevalence of stress urinary incontinence in women studying nursing and related quality of life. Prz Menopauzalny. 2014;13(1):32–35. doi:10.5114/pm.2014.41086
14. Sexton CC, Coyne KS, Kopp ZS, et al. The overlap of storage, voiding and postmicturition symptoms and implications for treatment seeking in the USA, UK and Sweden: epiLUTS. BJU Int. 2009;103(Suppl 3):12–23. doi:10.1111/j.1464-410X.2009.08369.x
15. Lim R, Liong ML, Leong WS, Lau YK, Khan NAK, Yuen KH. The impact of stress urinary incontinence on individual components of quality of life in Malaysian women. Urology. 2018;112:38–45. doi:10.1016/j.urology.2017.10.019
16. Steibliene V, Aniuliene R, Aniulis P, Raskauskiene N, Adomaitiene V. Affective symptoms and health-related quality of life among women with stress urinary incontinence: cross-sectional study. Neuropsychiatr Dis Treat. 2020;16:535–544. doi:10.2147/NDT.S236234
17. Coyne KS, Wein AJ, Tubaro A, et al. The burden of lower urinary tract symptoms: evaluating the effect of LUTS on health-related quality of life, anxiety and depression: EpiLUTS. BJU Int. 2009;103(Suppl 3):4–11. doi:10.1111/j.1464-410X.2009.08371.x
18. Stadnicka G, Lepecka-Klusek C, Pilewska-Kozak A, Jakiel G. Psychosocial problems of women with stress urinary incontinence. Ann Agric Environ Med. 2015;22(3):499–503. doi:10.5604/12321966.1167723
19. Fultz N, Girts T, Kinchen K, Nygaard I, Pohl G, Sternfeld B. Prevalence, management and impact of urinary incontinence in the workplace. Occup Med. 2005;55(7):552–557. doi:10.1093/occmed/kqi152
20. Chang Y-C, Fan Y-H, Lin ATL, Chen -K-K. Do female patients with predominant voiding symptoms really have objective voiding-phase dysfunction? Urol Sci. 2017;28(3):152–155. doi:10.1016/j.urols.2016.10.002
21. Chow PM, Liu SP, Chuang YC, et al. The prevalence and risk factors of nocturia in China, South Korea, and Taiwan: results from a cross-sectional, population-based study. World J Urol. 2018;36(11):1853–1862. doi:10.1007/s00345-018-2329-0
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.