Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Impact of Exercise Capacity Upon Respiratory Functions, Perception of Dyspnea, and Quality of Life in Patients with Chronic Obstructive Pulmonary Disease
Received 29 March 2021
Accepted for publication 20 May 2021
Published 1 June 2021 Volume 2021:16 Pages 1529—1534
DOI https://doi.org/10.2147/COPD.S311221
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Wenjun Liu,1,2 Yufei Liu,1,2 Xiaolin Li1,2
1Department of Human Movement Science in Graduate School, Harbin Sport University, Harbin, 150000, People’s Republic of China; 2Department of Sports Science and Health, Harbin Sport University, Harbin, 150000, People’s Republic of China
Correspondence: Xiaolin Li Email [email protected]
Background: Chronic obstructive pulmonary disease (COPD) is associated with a high prevalence of morbidity and mortality worldwide. We investigated the effects of exercise capacity upon respiratory functions, perception of dyspnea, and quality of life (QoL) in patients with COPD.
Methods: A total of 512 COPD patients formed the study cohort. They were divided into four subgroups according to the distance walked in the 6-minute walking test (6MWT). We compared respiratory functions, perception of dyspnea, and QoL between groups.
Results: Patients who walked > 350 m had significantly better disease-specific QoL scores (p < 0.001) than those of other groups. A negative correlation was found between the walking distance and anxiety, depression, and dyspnea scores (p < 0.001).
Conclusions: In patients who walked < 350 m, the reduced walking distance adversely affected respiratory functions, psychological symptoms, and QoL.
Keywords: chronic obstructive pulmonary disease, exercise, quality of life, statistics
Introduction
Chronic obstructive pulmonary disease (COPD) is a prevalent disease worldwide and leads to a high prevalence of morbidity and mortality.1 It is characterized by irreversible, progressive airflow limitation, and repeated airway inflammation, which seriously affects the quality of life (QoL) of patients with COPD.2 Environmental factors and genetic mutations have roles in COPD. Exposure to cigarette smoking, occupational exposure to chemicals, and environmental pollution are risk factors for COPD.3 Furthermore, several studies have shown that genetic factors are involved in COPD pathogenesis.4 Dyspnea is an important contributor to QoL decline.5 The clinical symptoms of COPD also include sputum production, chronic cough, and wheezing. COPD is the fourth leading cause of death worldwide.6 Reduced activity due to dyspnea can also cause psychological problems (eg, anxiety, depression).7
The diagnosis of COPD is established through spirometry. A ratio of post-bronchodilator forced expired volume in one second/forced vital capacity (FEV1/FVC) <0.7 denotes persistent airflow obstruction.8 However, spirometry values are usually not a good predictor of QoL in patients with COPD, and also correlate weakly with dyspnea, exercise capacity, and health status.9 Therefore, we can measure the impact of chronic diseases and treatment efficacy by assessing QoL.10 Functional evaluations, such as assessment of exercise capacity, are useful tools. The 6-minute walk test (6MWT) can be used to measure exercise capacity.11 Several concomitant physiological variables, such as heart rate, workload, and oxygen consumption, can be monitored. At least partly due to systemic inflammation, extrapulmonary symptoms and anemia may occur, such as cachexia.12
COPD can be treated first by removal/modification of risk factors (eg, smoking cessation). Exercise training, typically to a pulmonary rehabilitation program, is efficacious treatment in COPD patients in terms of exercise capacity and health-related QoL.13
Studies have shown that COPD and its consequent daily activity restrictions affect QoL.14 Exercise ability can be reflected by exercise tests. However, the extent to which exercise testing accurately reflects QOL as assessed by clinical parameters is not clear. At present, there are few studies on the detailed and comprehensive analysis of the effect of exercise capacity on the clinical parameters of COPD patients.15,16
In this study, we wished to investigate the effects of exercise capacity on respiratory functions, perception of dyspnea, and QoL in patients with COPD. We used only the BODE Index as a reference for grouping of COPD patients. In this way, we could more clearly examine the impact of reducing the walking distance on patients with COPD. And reducing walking distance has a negative effect on the clinical indicators of COPD patients.
Methods
Ethical Approval of the Study Protocol
The study was conducted in accordance with the Declaration of Helsinki. The study protocol was approved by Graduate School of Harbin Sport University. The purpose of the assessment methods was detailed to patients. Written informed consent was obtained from all participants.
Characteristics of Patients
Demographic and clinical characteristics (eg, smoking history) were recorded. Pulmonary function tests, chest radiography, and arterial blood gases (ABG) were evaluated.
Bode Index
The BODE Index is a multidimensional grading system comprising the body mass index (BMI), airway obstruction, dyspnea scale, and exercise capacity. It is being used increasingly for COPD evaluation. The BODE Index is calculated based on the combination of four variables for each patient with COPD. The calculation rules are the evaluation score of the: (i) body composition (BMI): from 0 point to 1 point; (ii) intensity of airflow obstruction (FEV1% predicted post-bronchodilator): from 0 point to 3 points; (iii) subjective sensation of dyspnea (Medical Research Council (MRC) scale): from 0 point to 3 points; (iv) exercise capacity (walked distance in the 6MWT): from 0 point to 3 points. Therefore, the total score of the BODE Index ranges from 1 to 10. The closer the BODE Index score is to 10, the more severe is the condition. According to the 6MWT, patients with COPD can be divided into four groups: 1 (walked <150 m); (ii) 2 (walked between 150 m and 249 m); (iii) 3 (walked between 250 m and 349 m); (iv) 4 (walked ≥350 m). The reason for this grouping is to be able to more clearly examine the impact of reduced walking distance on COPD patients and follow-up statistical analysis. In addition, our grouping system also used the BODE Index as a reference. All parameters were compared again between these four groups.
Pulmonary Function
Body plethysmography was undertaken using a Zan 500 system (Belgium). Carbon‑monoxide diffusion capacity (TLCO) was measured using a Zan 300 system. Patients had to meet a postbronchodilator ratio of FEV1/FVC <0.7.
Evaluation of Dyspnea
Dyspnea severity was determined using the MRC dyspnea scale. A score of 1 was considered to denote perception of the mildest dyspnea. A score of 5 denoted perception of the most severe dyspnea.
QoL
The Saint George’s Respiratory Questionnaire (SGRQ) was used to assess disease‑specific QoL. The higher the score, the worse was the disease, and an increase in symptoms was likely.
Psychological Symptoms
The Hospital Anxiety and Depression (HAD) scale was used to determine mental status. There are 14 questions in the HAD scale. A score for anxiety and depression of 0−7 is “normal”, 8−11 is “borderline” and >11 indicates “anxiety or depression”.
Exercise Capacity
The 6MWT was employed to determine exercise capacity. Patients were asked to walk as fast as they could for 6 min, and the result was measured in meters. If the test result does not meet the requirements, multiple repeat tests can be undertaken.17
Statistical Analyses
Statistical analyses were undertaken using SPSS 20.0 (IBM, Armonk, NY, USA). The normality of the data distribution was checked by the Shapiro–Wilk test and Kolmogorov–Smirnov test. If the data distribution was not normal, continuous variables were expressed as the median (interquartile range) and categorical variables as percentages. Fisher’s exact test was used for variables determined with numbers. The Kruskal–Wallis H‑test was conducted to compare data between groups. The Mann–Whitney U‑test was employed to test the significance of pairwise differences. The Bonferroni correction was undertaken to adjust for multiple comparisons. p < 0.05 was considered significant.
Results
The demographic and clinical characteristics of 512 COPD patients are shown in Table 1. Except for sex, the other parameters tested were significantly different (p < 0.001 for all). The age of group-4 patients was significantly lower than that of patients in the other three groups (p < 0.001). BMI was significantly higher in group 4 than that in groups 1 (p = 0.035) and group 2 (p = 0.012). BMI of group 3 was significantly higher than that of group 1 (p = 0.041). The number of cigarettes consumed between group 1 and group 2 was comparable. Compared with the other three groups, the number of admissions to the emergency department and hospitalization within the previous year was significantly lower in group 4 (p < 0.001). According to admissions to the emergency department, the number was lower in group 3 (p = 0.021) and group 2 than those for group 1 (p = 0.035). FEV1 (%) and FEV1/FVC were comparable between group 1 and group 2, but significantly higher in group 4, compared with those in all other groups, and significantly higher in group 3 compared with those in group 1 and group 2 (p < 0.005). TLCO was comparable between group 1 and group 2, but significantly higher in group 4 compared with that in all other groups (p < 0.001), and significantly higher in group 3 compared with that in group 1 (p = 0.040) and group 2 (p = 0.035). Measurement of ABGs revealed that the partial pressure of oxygen (PaO2) and arterial oxygen saturation (SaO2) were significantly higher in group 4 compared with those in all other groups (p < 0.001). Comparison between group 1 and group 2 revealed PaO2 (p = 0.045) and SaO2 to be significantly higher than those in group 3 (p = 0.022).
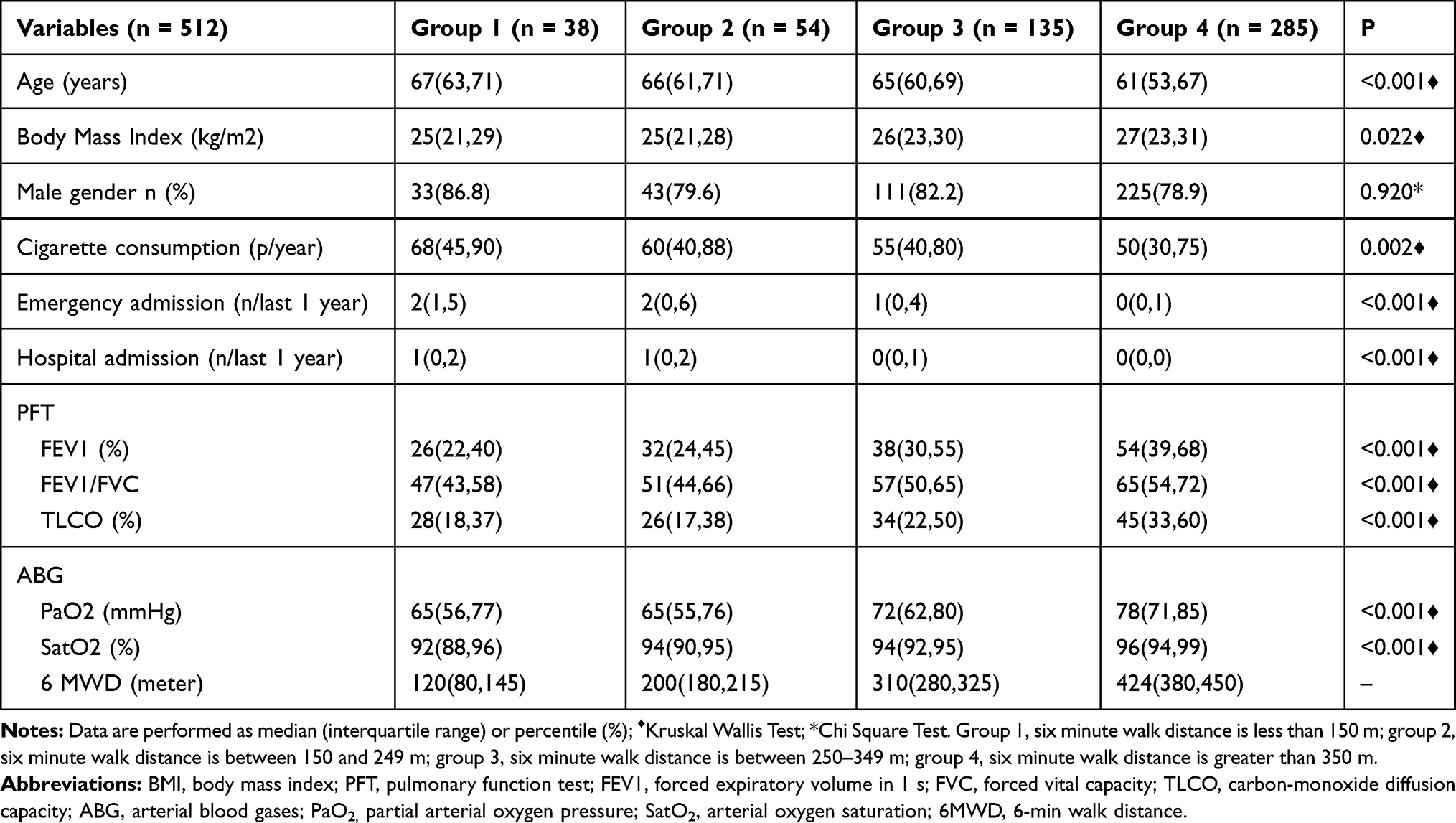 |
Table 1 Demographic and Clinical Characteristics of the Patients |
The perception of dyspnea was lower in group 4 compared with that in all other groups (p < 0.001) and it was significantly lower in group 3 compared with that in group 1 (p = 0.022) and group 2 (p = 0.035). Dyspnea scores were comparable between groups 1 and 2 (p = 0.561).
With regard to SGRQ scores, the symptom score, activity score, and effect score were significantly lower in group 4 compared with those in all other groups (p < 0.001). The total score in group 4 was significantly lower compared with that in the other three groups (p < 0.001). Table 2
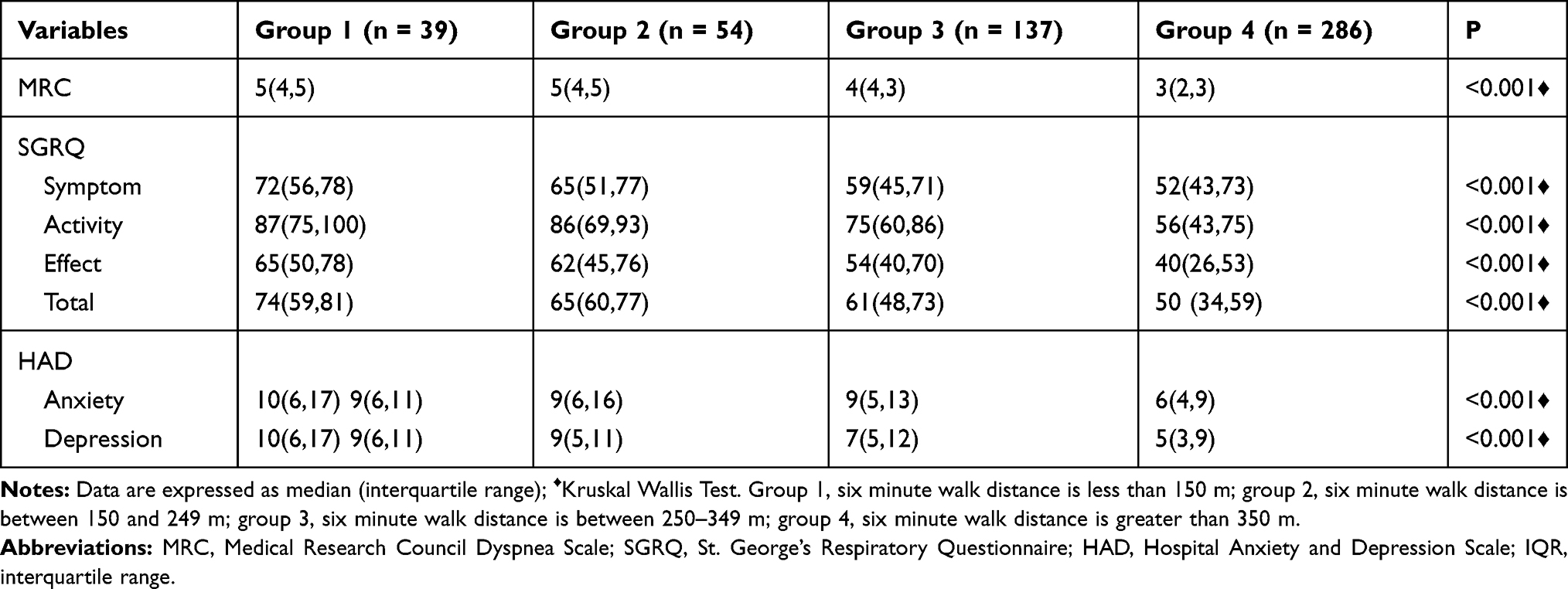 |
Table 2 Comparison of Dyspnea, Quality of Life, Anxiety, and Depression Among the Groups |
Discussion
We divided COPD patients into four groups based on the distance walked in the 6MWT. We found that the walking distance had a correlation with smoking, BMI, and age. As patients smoked more and became older, BMI decreased and patients walked shorter distances. A reduced walking distance also meant higher numbers of admissions to the emergency department and hospitalization during the previous year. Patients who had shorter walking distances had a higher perception of dyspnea and their psychological symptoms increased, which led to lower QoL.
Impact of Exercise Capacity Upon Respiratory Functions in Patients with COPD
COPD is characterized by airflow obstruction that is partially reversible. COPD not only causes an abnormal inflammatory response in the lungs, it also reduces exercise capacity.18 People who smoke are more likely to suffer from COPD than people who do not smoke, with 20–25% of smokers going on to develop COPD.19 The prevalence of COPD in people aged >40 years is higher than that in individuals aged <40 years, and is not related to sex.20 The FEV1 of patients with COPD decreases gradually as the disease progresses. The diagnosis is established through spirometry, so the FEV1 measurement can play an important part, but it cannot fully reflect the adverse effects of COPD.
Exercise capacity is a very important parameter to measure COPD. Recently, it has been used to evaluate the prognosis and the effect of therapeutic interventions.21 The 6MWT is usually employed for assessment of the functional status of patients. The walking distance will decrease gradually over time, but it is not associated with respiratory function.22 In our study, the average age of COPD patients who walked >350 m was significantly lower than that of the other patients. For patients who walked >350 m, the FEV1, FEV1/FVC, and TLCO in the respiratory function test also increased significantly. Studies have reported that the distance walked in the 6MWT is linearly related to COPD severity.23 In the present study, patients with a walking distance <150 m had significantly more severe COPD than that of other patients. Consistent with a study reporting a negative correlation between smoking and exercise capacity,24 most of our patients who consumed more cigarettes walked a shorter distance. We found that the BMI of patients who walked ≥350 m was significantly higher than that of the other groups: this result is consistent with the research results of Punekar and colleagues.9 The walking distance of COPD patients was significantly longer after presenting to the emergency department. Studies have shown that hospital admission reduces walking distances significantly, and there is a negative correlation between walking distances and the number of hospital admissions.21 In our study, the number of emergency hospital admissions and hospitalizations was significantly negatively correlated with the walking distance.
Impact of Exercise Capacity Upon Perception of Dyspnea with COPD
As one of the main symptoms of COPD, dyspnea can lead to decreased activities of daily living (ADL), physical deterioration, and exercise intolerance.25 Other studies have shown that the improvement of physical activity can make the patient’s lung function slightly better, less dyspnea, and better quality of life.26,27 A negative correlation between the walking distance and perception of dyspnea has been documented.9 In our study, the perception of dyspnea was significantly lower in patients whose walking distance was >350 m (ie, the walking distance decreased with an increase in perception of dyspnea). COPD also has a negative impact on a patient’s psychology and brings a heavy burden to society.28 Patients with COPD are confronted with social isolation and psychological symptoms due to reduced ADL.29 In the present study, the scores for anxiety and depression (the most common physical symptoms of COPD patients) increased significantly as the walking distance increased.
Impact of Exercise Capacity Upon Quality of Life in Patients with COPD
The QoL of COPD patients worsens and their exercise capacity decreases with time.23 Smoking, psychological symptoms, dyspnea, and decreased ADL lead to a decline in the QoL of patients.30 In sub-scores of the SGRQ, “activity” and “effect” scores have been shown to be negatively correlated with walking distance.9 We found a negative correlation between the SGRQ score and walking distance. Patients who walked >350 m had a significantly lower SGRQ score (sub-scores and the total score) than that for patients in the other groups. Table 2
With regard to the limitations of our study, we did not consider other influencing factors (eg, economic status, marriage, profession). Moreover, medication alone is not enough for COPD patients. Therefore, in the treatment plan for COPD, in addition to drug treatment, attention should also be paid to increasing walking distance, providing nutrition and psychological support, and improving the quality of life.
Conclusions
COPD patients were divided into four groups according to the walking distance. Patients who walked >350 m were significantly younger, had higher BMI, smoked less, and had better respiratory functions and oxygenation compared with those in the other groups. We discovered a negative correlation between the walking distance and dyspnea, psychological symptoms, and QoL. The shorter the distance the patient walked, the higher number of admissions to the emergency department and hospitalization. Increasing the walking distance, relieving dyspnea, smoking less, and improving QoL are very important parameters for the recovery of patients with COPD.
Acknowledgments
Special thanks to Xiao Lanlu for helping us with patient communication, patient privacy, etc.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang N, Wang Q, Du T, et al. The potential roles of exosomes in chronic obstructive pulmonary disease. Front Med. 2020;7:618506. doi:10.3389/fmed.2020.618506
2. Putcha N, Puhan MA, Hansel NN, Drummond MB, Boyd CM. Impact of co-morbidities on self-rated health in self-reported COPD: an analysis of NHANES 2001–2008. Copd. 2013;10(3):324–332. doi:10.3109/15412555.2012.744963
3. Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/s2213-2600(17)30293-x
4. Hobbs BD, Hersh CP. Integrative genomics of chronic obstructive pulmonary disease. Biochem Biophys Res Commun. 2014;452(2):276–286. doi:10.1016/j.bbrc.2014.07.086
5. Nici L, Donner C, Wouters E, et al. American thoracic society/European respiratory society statement on pulmonary rehabilitation. Am J Respir Crit Care Med. 2006;173(12):1390–1413. doi:10.1164/rccm.200508-1211ST
6. Hashemi SY, Momenabadi V, Faramarzi A, Kiani A. Trends in burden of chronic obstructive pulmonary disease in Iran, 1995–2015: findings from the global burden of disease study. Arch Public Health. 2020;78:45. doi:10.1186/s13690-020-00426-x
7. Bowers S, Cannizzaro K, Gregus J, Scott Q, Eason J. Outcomes in cardiopulmonary physical therapy: sickness impact profile. Cardiopulm Phys Ther J. 2009;20(1):19–24. doi:10.1097/01823246-200920010-00004
8. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Am J Respir Crit Care Med. 2017;195:557–582. doi:10.1183/13993003.50214-2017
9. Punekar YS, Riley JH, Lloyd E, Driessen M, Singh SJ. Systematic review of the association between exercise tests and patient-reported outcomes in patients with chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2017;12:2487–2506. doi:10.2147/copd.S100204
10. Ahmed MS, Neyaz A, Aslami AN. Health-related quality of life of chronic obstructive pulmonary disease patients: results from a community based cross-sectional study in Aligarh, Uttar Pradesh, India. Lung India. 2016;33(2):148–153. doi:10.4103/0970-2113.177438
11. Butland RJ, Pang J, Gross ER, Woodcock AA, Geddes DM. Two-, six-, and 12-minute walking tests in respiratory disease. Br Med J. 1982;284(6329):1607–1608. doi:10.1136/bmj.284.6329.1607
12. Choudhury G, Rabinovich R, MacNee W. Comorbidities and systemic effects of chronic obstructive pulmonary disease. Clin Chest Med. 2014;35(1):101–130. doi:10.1016/j.ccm.2013.10.007
13. Rochester CL, Vogiatzis I, Holland AE, et al. An official American thoracic society/European respiratory society policy statement: enhancing implementation, use, and delivery of pulmonary rehabilitation. Am J Respir Crit Care Med. 2015;192(11):1373–1386. doi:10.1164/rccm.201510-1966ST
14. Lu Y, Nyunt MS, Gwee X, et al. Life event stress and chronic obstructive pulmonary disease (COPD): associations with mental well-being and quality of life in a population-based study. BMJ Open. 2012;2(6):e001674. doi:10.1136/bmjopen-2012-001674
15. Kortianou EA, Aliverti A, Louvaris Z, et al. Limitation in tidal volume expansion partially determines the intensity of physical activity in COPD. J Appl Physiol. 2015;118(1):107–114. doi:10.1152/japplphysiol.00301.2014
16. Louvaris Z, Kortianou EA, Spetsioti S, et al. Intensity of daily physical activity is associated with central hemodynamic and leg muscle oxygen availability in COPD. J Appl Physiol. 2013;115(6):794–802. doi:10.1152/japplphysiol.00379.2013
17. Holland AE, Spruit MA, Troosters T, et al. An official European respiratory society/American thoracic society technical standard: field walking tests in chronic respiratory disease. Eur Respir J. 2014;44(6):1428–1446. doi:10.1183/09031936.00150314
18. King PT. Inflammation in chronic obstructive pulmonary disease and its role in cardiovascular disease and lung cancer. Clin Transl Med. 2015;4(1):68. doi:10.1186/s40169-015-0068-z
19. Lundbäck B, Lindberg A, Lindström M, et al. Not 15 but 50% of smokers develop COPD?–Report from the obstructive lung disease in Northern Sweden studies. Respir Med. 2003;97(2):115–122. doi:10.1053/rmed.2003.1446
20. Fabbri L, Pauwels RA, Hurd SS. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease: GOLD executive summary updated 2003. Copd. 2004;1(1):105–141. doi:10.1081/copd-120030163
21. Ramon MA, Gimeno-Santos E, Ferrer J, et al. Hospital admissions and exercise capacity decline in patients with COPD. Eur Respir J. 2014;43(4):1018–1027. doi:10.1183/09031936.00088313
22. Pinto-Plata VM, Cote C, Cabral H, Taylor J, Celli BR. The 6-min walk distance: change over time and value as a predictor of survival in severe COPD. Eur Respir J. 2004;23(1):28–33. doi:10.1183/09031936.03.00034603
23. Agrawal SR, Joshi R, Jain A. Correlation of severity of chronic obstructive pulmonary disease with health-related quality of life and six-minute walk test in a rural hospital of central India. Lung India. 2015;32(3):233–240. doi:10.4103/0970-2113.156231
24. Mesquita R, Gonçalves CG, Hayashi D, et al. Smoking status and its relationship with exercise capacity, physical activity in daily life and quality of life in physically independent, elderly individuals. Physiotherapy. 2015;101(1):55–61. doi:10.1016/j.physio.2014.04.008
25. Corhay JL, Dang DN, Van Cauwenberge H, Louis R. Pulmonary rehabilitation and COPD: providing patients a good environment for optimizing therapy. Int J Chron Obstruct Pulmon Dis. 2014;9:27–39. doi:10.2147/copd.S52012
26. Osadnik CR, Loeckx M, Louvaris Z, et al. The likelihood of improving physical activity after pulmonary rehabilitation is increased in patients with COPD who have better exercise tolerance. Int J Chron Obstruct Pulmon Dis. 2018;13:3515–3527. doi:10.2147/COPD.S174827
27. Kerti M, Balogh Z, Kelemen K, Varga JT. The relationship between exercise capacity and different functional markers in pulmonary rehabilitation for COPD. Int J Chron Obstruct Pulmon Dis. 2018;13:717–724. doi:10.2147/COPD.S153525
28. Ekici A, Bulcun E, Karakoc T, Senturk E, Ekici M. Factors associated with quality of life in subjects with stable COPD. Respir Care. 2015;60(11):1585–1591. doi:10.4187/respcare.03904
29. Balcells E, Gea J, Ferrer J, et al. Factors affecting the relationship between psychological status and quality of life in COPD patients. Health Qual Life Outcomes. 2010;8:108. doi:10.1186/1477-7525-8-108
30. Nagata K, Tomii K, Otsuka K, et al. Evaluation of the chronic obstructive pulmonary disease assessment test for measurement of health-related quality of life in patients with interstitial lung disease. Respirology. 2012;17(3):506–512. doi:10.1111/j.1440-1843.2012.02131.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.