Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Impact of Different Exercise Modalities on Physical Function and Quality of Life in Patients with Heart Failure
Received 23 February 2024
Accepted for publication 7 May 2024
Published 23 May 2024 Volume 2024:17 Pages 2551—2559
DOI https://doi.org/10.2147/JMDH.S465578
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pavani Rangachari
Jiangying Li,1 Lu Chen,2 Lichun Wang3
1Department of Cardiology, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, Taizhou, 225300, People’s Republic of China; 2Department of Emergency, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, Taizhou, 225300, People’s Republic of China; 3Department of Nursing, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, Taizhou, 225300, People’s Republic of China
Correspondence: Lichun Wang, Department of Nursing, The Affiliated Taizhou People’s Hospital of Nanjing Medical University, Taizhou School of Clinical Medicine, Nanjing Medical University, No. 366 Taihu Road, Taizhou Pharmaceutical High-Tech Zone, Taizhou, 225300, People’s Republic of China, Tel +86 13775704547, Email [email protected]
Abstract: Heart failure, a chronic condition, often manifests with reduced physical function and an overall decline in quality of life. It is considered critical that patients with heart failure recover as soon as possible; exercise training, which includes aerobic exercise, resistance exercise, inspiratory muscle training, traditional mind-body exercise, and combined training, facilitates this. The research progress on the impact of various exercise modalities on the physical function and quality of life of patients with heart failure is systematically reviewed in this article. The objective is to augment the understanding of healthcare personnel regarding the status of implementation and outcomes associated with varied exercise modalities. This endeavor seeks to provide a point of reference for the development of exercise rehabilitation programs tailored to individuals contending with heart failure.
Keywords: exercise modalities, heart failure, physical function, quality of life, review
Introduction
Heart failure (HF) encompasses a variety of clinical syndromes characterized by reduced ventricular ejection and/or ejection capacity caused by anatomical and/or functional abnormalities in the heart.1 This condition is characterized by typical symptoms such as dyspnea, fatigue, and fluid retention. Global reports indicate that approximately 40 million individuals are affected by HF,2 with around 8.9 million cases reported in China alone.3 HF is associated with high morbidity, mortality, and re-hospitalization rates, contributing to a substantial disease burden and diminished quality of life.4
While medications play a crucial role in HF management, guidelines emphasize the effectiveness of exercise as a treatment that can enhance symptoms and cardiac function in patients with HF.5 Exercise therapy has also been shown to alleviate fatigue, improve sleep quality, and enhance overall life quality in patients with HF.6,7 Various exercise modalities, including aerobic exercise, resistance exercise, inspiratory muscle training (IMT), traditional mind-body exercise, and combinations of these modalities, are commonly available. Exercise training is a fundamental component of cardiac rehabilitation for individuals with cardiovascular disease. However, there is still ongoing debate regarding the most effective training program for HF treatment.
The objective of this study is to examine the advancements in research about the effects of various exercise methods on the physical function and quality of life of patients with HF. The goal is to provide medical professionals with a reference for developing a scientifically sound, safe, and feasible exercise program for patients with HF.
Aerobic Exercise
Aerobic exercise, also referred to as endurance exercise, involves the rhythmic movement of large muscle groups over an extended period.8 This form of exercise raises heart rates and breathing rates, enhancing cardiopulmonary function and the efficiency of the respiratory and circulatory systems. The goal is to supply adequate oxygen and nutrients to the body’s tissues and organs. Common aerobic exercises include brisk walking, swimming, running, stair climbing, and cycling.
According to the 2021 JACC Expert Consensus on Cardiac Rehabilitation in Patients with Heart Failure, published by the Journal of the American College of Cardiology, aerobic exercise is the primary mode of exercise.9 Numerous studies support the positive impact of aerobic exercise on the physical function and quality of life of patients with HF. For instance, a study investigated the effect of an aerobic exercise intervention program (five times a week for seven months) on 38 patients with HF.10 The study revealed a significant increase in exercise tolerance and a marked improvement in the left heart function index in the observation group. This evidence underscores the constructive influence of aerobic exercise on cardiovascular rehabilitation in patients, aligning with the findings reported by Delgado et al.11 Another study also revealed significant improvements in physical function indexes and quality of life in the aerobic exercise group at 16 weeks of follow-up.12 In contrast, Gary et al observed that there were no statistically significant improvements in the results of the 6-minute walking test (6MWT) after a 12-week schedule of aerobic exercise training for patients with HF.13 This observation may be correlated with the study’s substantial inclusion of female participants and patients with obesity, each exhibiting three or more comorbidities. Therefore, healthcare professionals should comprehensively assess patients’ conditions, age, gender, physical fitness, exercise history, and other factors before designing an exercise plan to maximize the benefits of exercise.
Contemporary guidelines advocate for moderate continuous training (MCT), consisting of sessions lasting up to 60 minutes, to be undertaken 3 to 5 days per week, as a recommended approach for patients diagnosed with HF.14 However, some individuals may face difficulties in sustaining long-term aerobic exercise training because of symptoms they experience, such as leg soreness and difficulty breathing, which can worsen with lengthy periods of aerobic activity.15 High-intensity interval training (HIIT) involves alternating periods of high-intensity with low-intensity exercise periods to improve metabolism and cardiopulmonary function. This modality is increasingly being adopted in clinical practice. Sowa et al conducted a randomized trial where patients were allocated into HIIT, MCT, and control groups.16 The results indicated that both the HIIT and MCT groups exhibited substantial improvements in exercise capacity in comparison to their respective baseline measurements. Benda et al17 scrutinized the influence of HIIT on patients with chronic heart failure (CHF). The study revealed that HIIT not only increased the exercise capacity of the patients but also improved their physical fitness and quality of life. In contrast, Lundgren et al conducted a study that investigated the effects of a 3-month home-based high-intensity interval training (HIIT) program on patients with heart failure (HF). The results showed that the telerehabilitation group experienced an increase in walking distance of 19.1 meters, whereas the control group had an increase of 15.3 meters from the beginning to the end of the intervention.18 However, no statistically significant differences between the two groups were observed, attributed to poor patient compliance. Home-based exercise rehabilitation, integrated with patients’ daily activities and not constrained by location, is gradually gaining popularity among patients. However, monitoring the effectiveness of the exercise poses challenges, with patients at risk of dropping out. Therefore, special attention needs to be paid to patients’ adherence issues during implementation.
In addition, growing attention is being paid to comparing the differences between HIIT and MCT. A study conducted in China indicated that HIIT increases VO2peak, 6MWT, and left ventricular ejection fraction in patients with HF compared to MCT.19 Donelli et al reported that after 3 months of exercise training, HIIT was more effective than MCT in elevating peak oxygen uptake (VO2peak).20 On the contrary, a multicenter trial compared the intervention effects of 12 weeks of HIIT, MCT, or regular exercise. The results showed that HIIT was not superior to MCT in improving left ventricular remodeling, aerobic capacity, and VO2peak, but both were superior to regular exercise. However, these improvements were not sustained in the follow-up at 52 weeks.21 Similarly, Valborgland et al, report no significant differences between the effects of HIIT and MCT on left ventricular remodeling and exercise capacity in patients.22 The differences in the analysis results of HIIT and MCT in the patients with heart failure suggest that we need to pay attention to: (1) the uncertainty of result variations caused by differences between the actual training intensity and the target training intensity in the exercise program; (2) differences in the populations included in various trial studies, including age, gender, heart function classification, comorbidities, etc.
Resistance Exercise
Resistance exercise, also known as strength training, involves active efforts to overcome external resistance during muscle contraction, and involves various equipment such as dumbbells, barbells, and elastic bands.8 While traditional rehabilitation has predominantly focused on aerobic exercise, emerging evidence supports the muscle hypothesis, indicating skeletal muscle abnormalities in patients with HF and a correlation between low skeletal muscle mass and poor clinical outcomes.23 The reduction in muscle mass and strength is closely linked to diminished physical function, frailty, and disease progression.24 A significant fraction of persons with acute decompensated heart failure had frailty or sub-frailty in a recent clinical experiment, and almost one-third displayed significant weakness in their lower limbs.25 The American Physical Therapy Association recommends resistance exercise in HF management guidelines.26
Multiple studies underscore the efficacy of resistance training in augmenting both muscle mass and strength, thereby playing a pivotal role in averting muscle atrophy and improving exercise tolerance. A study demonstrated positive outcomes in lower and upper extremity muscle strength, VO2peak, and 6-minute walking distance (6MWD) without adverse effects on left ventricular parameters.27 Additional researches have demonstrated the effectiveness of resistance exercise rehabilitation interventions in improving cardiopulmonary exercise function and quality of life in patients with HF, suggesting its broad potential in clinical use.28,29 Studies on elderly patients with HF have confirmed the definitive effectiveness of resistance exercise training in enhancing exercise tolerance and cardiac function, emphasizing its clinical value.30 A meta-analysis of 10 studies indicated that resistance exercise, as a standalone intervention, improved muscle strength, aerobic capacity, and quality of life in patients with CHF, offering an alternative for those unable to participate in aerobic training.31 Despite these findings, there is a notable lack of research on resistance exercise in elderly patients and those with advanced HF, necessitating further investigation to optimize their inclusion. In a separate investigation, individuals diagnosed with heart failure participated in a three-month regimen of resistance exercise, which led to enhanced ability to engage in physical activity, without notable alterations in muscle strength.32 This may be related to the patient’s lack of severe muscle dysfunction and their average age (usually around 57 years old).
In conclusion, incorporating resistance exercise as part of comprehensive rehabilitation for patients with HF can contribute to more holistic care and an improved quality of life. There are rehabilitation guidelines33 that classify the intensity of resistance exercise into three levels: low intensity: 20% to 30% of one repetition maximum test (1RM), ratings of perceived exertion (RPE) levels of 10 to 11; moderate intensity: 40% to 60% of 1RM, RPE levels of 11 to 13; high intensity: 80% of 1RM, RPE levels of 13 to 16. It is recommended to perform 8 to 15 repetitions per set, 1 to 3 sets per day, 2 to 3 days per week, with adjustments to the program based on the patient’s condition. Further research is needed to determine the specific intensity, frequency, mode, and duration of resistance exercise that can improve physical function and quality of life in patients with heart failure.
IMT
Inspiratory muscle weakness is acknowledged as a key factor by which ventilation is limited in patients with HF.34 The presence of inspiratory muscle weakness is recognized in 50% of patients with HF, and symptoms like dyspnea and fatigue may be induced, consequently impacting the prognosis of patients.35,36 IMT facilitates the reduction of risk factors for cardiovascular disease by using breathing and relaxation techniques, as well as improving strength and endurance in the inspiratory muscle groups.37 This constitutes an effective strategy for improving cardiopulmonary function, exercise capacity, and quality of life in patients with HF. The effectiveness of IMT in ameliorating dyspnea in patients with HF was observed by Gaikar et al.38 Another study demonstrated marked improvement in pulmonary function parameters and inspiratory muscle strength when IMT was added to standardized cardiac rehabilitation for patients with HF.39
In a study by Tanriverdi et al, patients with HF with reduced ejection fraction underwent high-intensity interval-based IMT with an intensity of at least 70% of maximal inspiratory pressure for 8 weeks (21 min each time, three times a week).40 The results highlighted the positive effects of IMT on inspiratory muscle strength, quadriceps strength, inspiratory muscle endurance, dyspnea, and quality of life in patients with HF, aligning with the findings of Wu et al.41 Nevertheless, despite some studies reporting increased functional capacity in patients with HF due to IMT, there is insufficient evidence to support its positive impact on cardiovascular parameters, blood biomarkers, or quality of life.42
Sadek et al conducted a meta-analysis comprising seven studies employing diverse training regimens.43 The results indicated that Inspiratory Muscle Training (IMT), particularly when conducted at 60% of the maximum inspiratory pressure for a duration of 12 weeks, with a frequency of 6 sessions per week, led to notable improvements in the strength of the muscles involved in inhalation, walking distance, and a decrease in difficulty in breathing among patients with Congestive Heart Failure (CHF). However, the study acknowledged the presence of inspiratory muscle weakness in some participants and not in others, introducing potential biases. Another meta-analysis revealed that IMT alone resulted in increased inspiratory muscle strength, functional capacity, and quality of life, especially in patients with inspiratory muscle weakness who trained at a load higher than 60% for a longer duration.44 However, when combined with another intervention, IMT only marginally elevated inspiratory muscle strength.
In conclusion, as a non-invasive and effective intervention, IMT has demonstrated promising results in enhancing physical function and quality of life in patients with HF. Despite varied study outcomes, there is general support for the use of IMT in patients with HF. However, further research is needed to address issues such as comparisons of the effects of IMT alone or in combination with another intervention, optimal training load, intervention duration, long-term effects, and indications. Moreover, most randomized controlled trials exhibit a substantial risk of bias, contributing to a low level of evidence for most outcomes. Therefore, high-quality studies are essential to elevate the level of evidence for IMT in patients with HF.
Traditional Mind-Body Exercise
Traditional mind-body exercise, such as Tai Chi Chuan, Baduanjin and Yoga, is deemed suitable for middle-aged and elderly patients with HF, as it constitutes a form of low- and moderate-intensity exercise characterized by slow and gentle movements and a moderate level of exercise intensity. In contrast to contemporary exercise rehabilitation therapies, traditional mind-body therapies not only offer the advantages of simplicity, ease of acquisition, flexibility in space and time utilization, and favorable adherence, but also align with the daily exercise needs of individuals with HF. Tai Chi Chuan is a traditional Chinese martial art that emphasizes the principles of overcoming hardness with softness and using stillness to control movement. Before practicing Tai Chi Chuan, it is important to first maintain balance and relaxation with the correct standing posture. During the movements, focus on relaxing the body, concentrating the mind, and directing attention to the details and inner sensations of each movement. Tai Chi Chuan emphasizes slow and continuous movements, avoiding stiffness and rigidity, aiming to improve the body’s coordination and stability through practice. A meta-analysis revealed that exercise capacity and quality of life significantly increased in patients practicing Tai Chi Chuan.45 Similar conclusions were drawn by Hui et al, who found that Tai Chi Chuan alleviated depressive symptoms and improved sleep quality, with no significant impact on VO2peak.46 Redwine et al investigated a 16-week Tai Chi Chuan exercise program, observing noteworthy reductions in depressive symptoms in comparison to conventional treatment.47 Nevertheless, no noticeable disparities in the 6-minute walk distance (6MWD) were seen, which could be attributed to constraints such as the relatively small number of participants, the elderly age of the individuals involved, and the existence of other medical conditions that would have hindered their ability to walk. Existing studies mostly focused on short-term interventions, underscoring the need for further research to explore the effects of regular, long-term Tai Chi Chuan exercise on exercise tolerance, cardiac function, and patient prognosis.
Baduanjin is an independent and complete set of fitness exercises with a history of over 800 years. In Traditional Chinese Medicine, Baduanjin is believed to promote the circulation of qi and blood, harmonize the functions of the internal organs, relieve fatigue, enhance physical fitness, and improve respiratory function. The exercises are divided into eight sections, with each section consisting of a specific movement, hence the name “Baduanjin”. When practicing Baduanjin, it is important to perform the movements gently and slowly, with rounded and smooth transitions; a balance of relaxation and tension, a combination of movement and stillness; the mind in harmony with the body, and qi infused throughout. Previous studies indicate that Baduanjin enhances exercise capacity and quality of life.48,49 Chen et al analyzed a 12-week Baduanjin intervention program for patients with HF, revealing marked improvements in fatigue and quality of life at weeks 4, 8, and 12 compared to the control group.50 Although there is a scarcity of research on the impacts of Baduanjin in patients with HF, additional investigation is necessary to comprehend its influence on physical function and quality of life. This will establish a foundation for its therapeutic promotion and implementation.
Yoga is a form of exercise that combines meditation, relaxation, visualization, controlled breathing, and body stretching. It is characterized by gentle, soothing movements, simplicity, and accessibility to individuals of all ages, physical abilities, and environments. Hägglund et al conducted a 12-week yoga intervention, consisting of two sessions per week lasting 45–60 minutes each, for 40 heart failure patients.51 The results indicated that yoga could improve the health-related quality of life in heart failure patients and potentially alleviate depressive symptoms. Another study showed that yoga can significantly improve the cardiac function and quality of life in heart failure patients.52 However, the overall research on the effects of yoga on heart failure patients is not extensive at present. This is reflected in the small number of studies and the scarcity of high-quality randomized controlled trials. Further research is needed to determine the impact of yoga on heart failure patients.
In conclusion, both Tai Chi Chuan, Baduanjin and Yoga are recognized as effective exercise modalities for the treatment of HF. Nonetheless, the precise distinction in their efficacy for managing patients with HF has yet to be conclusively determined. Therefore, there is a need for extensive, high-quality randomized controlled studies to clarify the effects of traditional mind-body workouts on patients with HF, considering diverse types, causes, and New York Heart Association Functional categories. Such studies are essential for furnishing compelling evidence that can aid patients in making informed decisions regarding the selection of a more suitable exercise rehabilitation program. Despite the numerous benefits of traditional mind-body exercise for patients with HF, attention must be given to two key points: (1) Exercise intensity should be moderate, adjusting it moderately according to the individual situation of patients with HF to prevent increased heart burden from over-exercise. (2) Emphasis should be placed on strengthening rehabilitation guidance, ensuring that patients with HF engage in traditional mind-body exercise under professional guidance to exercise correctly and safely, thus avoiding injury or worsening of the condition.
Combined Training
The exercise regimen known as combined training is characterized by the incorporation of two or more exercise modalities, including aerobic exercise, resistance exercise, IMT, and HIIT. This approach is gradually finding application in clinical practice. The question of whether combined training yields a more pronounced improvement effect compared to a single modality of exercise is a matter of concern. A study revealed that, in comparison to aerobic exercise alone, the combination of aerobic exercise and resistance exercise resulted in substantial improvements in the physical function, muscle strength, and quality of life of patients.53 Similarly, in a study by Liu et al involving 60 patients with HF, it was demonstrated that 12 weeks of aerobic exercise combined with resistance exercise enhanced exercise tolerance, quality of sleep, and overall quality of life in patients with HF with preserved ejection fraction when compared to conventional treatment.54
Saeidi et al observed that high-intensity resistance exercise combined with aerobic exercise (75%1-RM) significantly increased 6MWD compared to low-intensity resistance exercise combined with aerobic exercise (50%1-RM), suggesting that higher exercise intensities should be judiciously considered in cardiac rehabilitation programs.55 Another study indicated that, in comparison to high-intensity aerobic interval training or IMT alone, a combined intervention of high-intensity aerobic interval training and IMT markedly improved inspiratory muscle function, exercise capacity, and quality of life in patients.56
In a study by Laoutaris et al, 88 patients with CHF were allocated into four groups:57 aerobic exercise, aerobic exercise combined with resistance exercise, aerobic exercise combined with IMT, and a combination of aerobic exercise, resistance exercise, and IMT. The results demonstrated that the combination of aerobic exercise, resistance exercise, and IMT surpassed the other exercise regimens in improving 6MWD, muscle strength, dyspnea, and quality of life in patients. Nevertheless, it is crucial to acknowledge that this study was constrained by certain limitations, including a limited sample size and a low proportion of female participants. Therefore, expanding the sample size and increasing the representation of female patients in future studies is crucial to further validate the effects of combined training programs on patients with HF.
Despite the positive findings suggesting the benefits of combined training for patients with HF, there are still unresolved issues. For instance, the optimal combined training program and training intensity remain undetermined, highlighting the need to explore effective ways to promote and apply this program in actual clinical settings. Furthermore, some studies have limitations, including small sample sizes and short follow-up durations. Hence, future research should aim to address these issues to enhance understanding and validate the effects of combined training on patients with HF.
Summary and Prospects
Exercise rehabilitation for patients with heart failure has attracted considerable attention. Current research indicates that exercise rehabilitation can improve symptoms, cardiac function, and quality of life for patients. Aerobic exercise, with minimal joint impact, is simple to learn and often does not require specialized equipment or specific locations, making it a common choice for heart failure patients. Nevertheless, elderly individuals engaging in aerobic activity could encounter various levels of muscular tiredness and necessitate an extended period of adjustment. Consequently, older patients engaging in aerobic exercise may have a higher dropout rate. Resistance training provides an alternative for patients who cannot engage in aerobic exercise and is suitable for those who can overcome gravity and external resistance to perform joint movements. Resistance exercise is more effective in improving muscle strength and preventing muscle atrophy, but it requires professional guidance and supervision to avoid muscle injuries and excessive cardiac burden. Inspiratory muscle training is simple to learn, convenientto implement, and not constrained by time or location, making it especially suitable for patients who cannot adhere to regular cardiac rehabilitation or engage in exercise. Traditional mind-body exercises help alleviate stress, enhance mental health, and promote mind-body balance. Currently, their application in heart failure is limited, requiring further, larger-scale, and longer-duration studies to validate their effects on patients with heart failure. Combination training can improve patients’ cardiopulmonary function and enhance muscle strength. Due to the high exercise volume, it places greater demands on patients’ physical fitness. Therefore, patients’ endurance and exercise intensity should be fully considered. And Table 1 shows strengths and limitations of various forms of exercise.
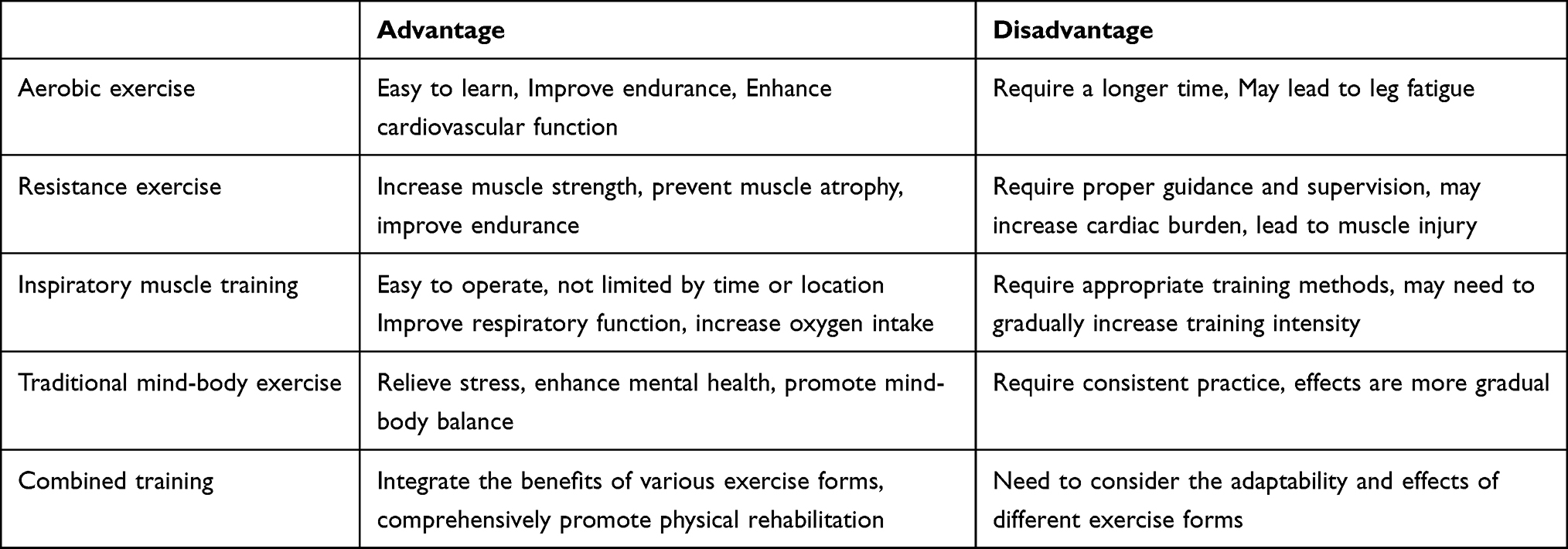 |
Table 1 Advantages and Disadvantages of Different Forms of Exercise |
In summary, the current situation disregards the development of standardized exercise rehabilitation programs for patients with heart failure and the therapeutic impacts of exercise over the long term. Subsequent research should focus on establishing the optimal exercise rehabilitation program and tracking the long-term therapeutic effects. Additionally, low participation rates and poor compliance are common issues in the exercise rehabilitation process for heart failure patients, necessitating more effective methods to improve patient compliance.
Abbreviations
HF, Heart Failure; JACC, Journal of the American College of Cardiology; 6MWT, 6-min walking test; MCT, moderate continuous training; HIIT, high-intensity interval training; CHF, Chronic heart failure; VO2peak, Peak oxygen uptake; 6MWD, 6-minute walking distance; IMT, Inspiratory muscle training; NYHA, New York Heart Association; 1RM, one repetition maximum test; RPE, Ratings of perceived exertion.
Data Sharing Statement
The data and materials used to support the findings of this study are available from the corresponding author Lichun Wang on reasonable request.
Funding
This research was supported by Application of nursing intervention based on IMB model in family caregivers of elderly patients with chronic heart failure (No. ZD202223).
Disclosure
The authors declare that they have no conflicts of interest regarding this work.
References
1. Wang X, Zhang C.; Cardiovascular Group, Geriatrics Branch, Chinese Medical Association; Editing Group of the Chinese Expert Consensus on the Diagnosis and Treatment of Chronic Heart Failure in Elderly Patients. Chinese expert consensus on the diagnosis and treatment of chronic heart failure in elderly patients (2021). Aging Med. 2022;5(2):78–93. PMID: 35792618; PMCID: PMC9245176. doi:10.1002/agm2.12215
2. Baman JR, Ahmad FS. Heart Failure. JAMA. 2020;324(10):1015. PMID: 32749448. doi:10.1001/jama.2020.13310
3. Liu J. Summary of China cardiovascular health and disease report 2022. Chin Circ J. 2023;38(06):583–612.
4. Patti A, Merlo L, Ambrosetti M, Sarto P. Exercise-based cardiac rehabilitation programs in heart failure patients. Heart Fail Clin. 2021;17(2):263–271. PMID: 33673950. doi:10.1016/j.hfc.2021.01.007
5. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. Erratum in: Eur Heart J. 2016 Dec 30. PMID: 27206819. doi:10.1093/eurheartj/ehw128
6. Taylor RS, Long L, Mordi IR, et al. Exercise-based rehabilitation for heart failure: cochrane systematic review, meta-analysis, and trial sequential analysis. JACC Heart Fail. 2019;7(8):691–705. PMID: 31302050. doi:10.1016/j.jchf.2019.04.023
7. Chan E, Giallauria F, Vigorito C, Smart NA. Exercise training in heart failure patients with preserved ejection fraction: a systematic review and meta-analysis. Monaldi Arch Chest Dis. 2016;86(1–2):759. PMID: 27748473. doi:10.4081/monaldi.2016.759
8. Piercy KL, Troiano RP, Ballard RM, et al. The physical activity guidelines for Americans. JAMA. 2018;320(19):2020–2028. PMID: 30418471; PMCID: PMC9582631. doi:10.1001/jama.2018.14854
9. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2022;145(18):e876–e894. PMID: 35363500. doi:10.1161/CIR.0000000000001062
10. Wen ZB, Zhang TW. Exercise resistance effects on adverse reaction rate in heart failure. Revista Brasileira de Medicina do Esporte. 2022;28:532–535. doi:10.1590/1517-8692202228052022_0016
11. Delgado B, Novo A, Lopes I, et al. The effects of early rehabilitation on functional exercise tolerance in decompensated heart failure patients: results of a multicenter randomized controlled trial (ERIC-HF study). Clin Rehabil. 2022;36(6):813–821. PMID: 35313751; PMCID: PMC9082976. doi:10.1177/02692155221088684
12. Brubaker PH, Avis T, Rejeski WJ, Mihalko SE, Tucker WJ, Kitzman DW. Exercise training effects on the relationship of physical function and health-related quality of life among older heart failure patients with preserved ejection fraction. J Cardiopulm Rehabil Prev. 2020;40(6):427–433. PMID: 32604218; PMCID: PMC7647941. doi:10.1097/HCR.0000000000000507
13. Gary RA, Paul S, Corwin E, et al. Exercise and cognitive training intervention improves self-care, quality of life and functional capacity in persons with heart failure. J Appl Gerontol. 2022;41(2):486–495. PMID: 33047625; PMCID: PMC8041896. doi:10.1177/0733464820964338
14. Pelliccia A, Sharma S, Gati S, et al. 2020 ESC Guidelines on sports cardiology and exercise in patients with cardiovascular disease. Eur Heart J. 2021;42(1):17–96. Erratum in: Eur Heart J. 2021 Feb 1;42(5):548–549. PMID: 32860412. doi:10.1093/eurheartj/ehaa605
15. Dubé BP, Agostoni P, Laveneziana P. Exertional dyspnoea in chronic heart failure: the role of the lung and respiratory mechanical factors. Eur Respir Rev. 2016;25(141):317–332. PMID: 27581831; PMCID: PMC9487213. doi:10.1183/16000617.0048-2016
16. Sowa PW, Winzer EB, Hommel J, et al. Impact of different training modalities on high-density lipoprotein function in HFpEF patients: a substudy of the OptimEx trial. ESC Heart Fail. 2022;9(5):3019–3030. PMID: 35747946; PMCID: PMC9715788. doi:10.1002/ehf2.14032
17. Benda NM, Seeger JP, Stevens GG, et al. Effects of high-intensity interval training versus continuous training on physical fitness, cardiovascular function and quality of life in heart failure patients. PLoS One. 2015;10(10):e0141256. PMID: 26517867; PMCID: PMC4627811. doi:10.1371/journal.pone.0141256
18. Lundgren KM, Langlo KAR, Salvesen Ø, et al. Feasibility of telerehabilitation for heart failure patients inaccessible for outpatient rehabilitation. ESC Heart Fail. 2023;10(4):2406–2417. PMID: 37221704; PMCID: PMC10375147. doi:10.1002/ehf2.14405
19. Li YZ, Liu D, Wu H, et al. A meta-analysis of the effects of high-intensity interval training and medium-intensity continuous training on cardiac rehabilitation in patients with heart failure. Chin J Evid Based Cardiovasc Med. 2022;14(11):1305–1309.
20. Donelli da Silveira A, Beust de lima J, da Silva Piardi D, et al. High-intensity interval training is effective and superior to moderate continuous training in patients with heart failure with preserved ejection fraction: a randomized clinical trial. Eur J Prev Cardiol. 2020;27(16):1733–1743. PMID: 31964186. doi:10.1177/2047487319901206
21. Ellingsen Ø, Halle M, Conraads V, et al. High-intensity interval training in patients with heart failure with reduced ejection fraction. Circulation. 2017;135(9):839–849. PMID: 28082387; PMCID: PMC5325251. doi:10.1161/CIRCULATIONAHA.116.022924
22. Valborgland T, Isaksen K, Munk PS, Larsen AI. Blood lactate AUC is a sensitive test for evaluating the effect of exercise training on functional work capacity in patients with chronic heart failure. Rehabil Res Pract. 2021;2021:6619747. PMID: 34631167; PMCID: PMC8497121. doi:10.1155/2021/6619747
23. Carbone S, Billingsley HE, Rodriguez-Miguelez P, et al. Lean mass abnormalities in heart failure: the role of sarcopenia, sarcopenic obesity, and cachexia. Curr Probl Cardiol. 2020;45(11):100417. PMID: 31036371. doi:10.1016/j.cpcardiol.2019.03.006
24. LeMaitre JP, Harris S, Hannan J, Fox KA, Denvir MA. Maximum oxygen uptake corrected for skeletal muscle mass accurately predicts functional improvements following exercise training in chronic heart failure. Eur J Heart Fail. 2006;8(3):243–248. PMID: 16185918. doi:10.1016/j.ejheart.2005.07.011
25. Kitzman DW, Whellan DJ, Duncan P, et al. Physical rehabilitation for older patients hospitalized for heart failure. N Engl J Med. 2021;385(3):203–216. PMID: 33999544; PMCID: PMC8353658. doi:10.1056/NEJMoa2026141
26. Shoemaker MJ, Dias KJ, Lefebvre KM, Heick JD, Collins SM. Physical therapist clinical practice guideline for the management of individuals with heart failure. Phys Ther. 2020;100(1):14–43. PMID: 31972027. doi:10.1093/ptj/pzz127
27. Fisher S, Smart NA, Pearson MJ. Resistance training in heart failure patients: a systematic review and meta-analysis. Heart Fail Rev. 2022;27(5):1665–1682. PMID: 34542742. doi:10.1007/s10741-021-10169-8
28. Huang XQ. Application of anti-resistance exercise in the treatment of coronary heart failure. Chin J Evid Based Cardiovasc Med. 2017;9(02):203–205+208.
29. Wang Y, Bian XW. Effect of exercise resistance rehabilitation intervention on heart function and quality of life in patients with chronic heart failure. Chin J Primary Med Pharm. 2020;27(23):2918–2921.
30. You ZN, Zhang L, Du YY. Effect of progressive resistance exercise training on elderly patients with chronic heart failure. J Community Med. 2023;21(16):843–847. doi:10.19790/j.cnki.JCM.2023.16.06
31. Giuliano C, Karahalios A, Neil C, Allen J, Levinger I. The effects of resistance training on muscle strength, quality of life and aerobic capacity in patients with chronic heart failure - A meta-analysis. Int J Cardiol. 2017;227:413–423. PMID: 27843045. doi:10.1016/j.ijcard.2016.11.023
32. Turri-Silva N, Vale-Lira A, Verboven K, Quaglioti Durigan JL, Hansen D, Cipriano G. High-intensity interval training versus progressive high-intensity circuit resistance training on endothelial function and cardiorespiratory fitness in heart failure: a preliminary randomized controlled trial. PLoS One. 2021;16(10):e0257607. PMID: 34597330; PMCID: PMC8486136. doi:10.1371/journal.pone.0257607
33. JCS Joint Working Group. Guidelines for rehabilitation in patients with cardiovascular disease (JCS 2012). Circ J. 2014;78(8):2022–2093. doi:10.1253/circj.CJ-66-0094
34. Nakagawa NK, Diz MA, Kawauchi TS, et al. Risk factors for inspiratory muscle weakness in chronic heart failure. Respir Care. 2020;65(4):507–516. PMID: 31822596. doi:10.4187/respcare.06766
35. Hamazaki N, Masuda T, Kamiya K, et al. Respiratory muscle weakness increases dead-space ventilation ratio aggravating ventilation-perfusion mismatch during exercise in patients with chronic heart failure. Respirology. 2019;24(2):154–161. PMID: 30426601. doi:10.1111/resp.13432
36. Yamada K, Kinugasa Y, Sota T, et al. Inspiratory muscle weakness is associated with exercise intolerance in patients with heart failure with preserved ejection fraction: a preliminary study. J Card Fail. 2016;22(1):38–47. PMID: 26505812. doi:10.1016/j.cardfail.2015.10.010
37. Wang MH, Yeh ML. Respiratory training interventions improve health status of heart failure patients: a systematic review and network meta-analysis of randomized controlled trials. World J Clin Cases. 2019;7(18):2760–2775. PMID: 31616691; PMCID: PMC6789387. doi:10.12998/wjcc.v7.i18.2760
38. Gaikar P, Kale M. A Study to assess the effectiveness of the inspiratory muscle training program on level of dyspnea among heart failure patients attending cardiac tertiary care centers, Maharashtra. Indian J Public Health Res Dev. 2023;14(1):190–195. doi:10.37506/ijphrd.v14i1.18832
39. Piotrowska M, Okrzymowska P, Kucharski W, Rożek-Piechura K. Application of inspiratory muscle training to improve physical tolerance in older patients with ischemic heart failure. Int J Environ Res Public Health. 2021;18(23):12441. PMID: 34886168; PMCID: PMC8657106. doi:10.3390/ijerph182312441
40. Tanriverdi A, Savci S, Ozcan Kahraman B, et al. Effects of high intensity interval-based inspiratory muscle training in patients with heart failure: a single-blind randomized controlled trial. Heart Lung. 2023;62:1–8. PMID: 37285766. doi:10.1016/j.hrtlng.2023.05.011
41. Wu J, Kuang L, Fu L. Effects of inspiratory muscle training in chronic heart failure patients: a systematic review and meta-analysis. Congenit Heart Dis. 2018;13(2):194–202. PMID: 29423938. doi:10.1111/chd.12586
42. Fernandez-Rubio H, Becerro-de-bengoa-vallejo R, Rodríguez-Sanz D, Calvo-Lobo C, Vicente-Campos D, Chicharro JL. Inspiratory muscle training in patients with heart failure. J Clin Med. 2020;9(6):1710. PMID: 32498445; PMCID: PMC7356942. doi:10.3390/jcm9061710
43. Sadek Z, Salami A, Joumaa WH, Awada C, Ahmaidi S, Ramadan W. Best mode of inspiratory muscle training in heart failure patients: a systematic review and meta-analysis. Eur J Prev Cardiol. 2018;25(16):1691–1701. PMID: 30073849. doi:10.1177/2047487318792315
44. Azambuja ACM, de Oliveira LZ, Sbruzzi G. Inspiratory muscle training in patients with heart failure: what is new? Systematic review and meta-analysis. Phys Ther. 2020;100(12):2099–2109. PMID: 32936904. doi:10.1093/ptj/pzaa171
45. Taylor-Piliae R, Finley BA. Benefits of Tai Chi exercise among adults with chronic heart failure: a systematic review and meta-analysis. J Cardiovasc Nurs. 2020;35(5):423–434. PMID: 32544110. doi:10.1097/JCN.0000000000000703
46. Hui J, Wang Y, Zhao J, Cong W, Xu F. Effects of Tai Chi on health status in adults with chronic heart failure: a systematic review and meta-analysis. Front Cardiovasc Med. 2022;9:953657. PMID: 36158796; PMCID: PMC9500215. doi:10.3389/fcvm.2022.953657
47. Redwine LS, Wilson K, Pung MA, et al. A randomized study examining the effects of mild-to-moderate group exercises on cardiovascular, physical, and psychological well-being in patients with heart failure. J Cardiopulm Rehabil Prev. 2019;39(6):403–408. PMID: 31397771; PMCID: PMC6832782. doi:10.1097/HCR.0000000000000430
48. Lai Q, Zhang J. Effects of traditional Chinese eight brocade exercise with same frequency and different durations on the quality of life, 6-min walk and brain natriuretic peptide in patients with chronic heart failure. Exp Gerontol. 2023;172:112059. PMID: 36526096. doi:10.1016/j.exger.2022.112059
49. Yang WY, Xu Y, Ye L, et al. Effects of Baduanjin exercise on quality-of-life and exercise capacity in patients with heart failure: a systematic review and meta-analysis. Complement Ther Clin Pract. 2023;50:101675. PMID: 36436262. doi:10.1016/j.ctcp.2022.101675
50. Chen DM, Yu WC, Hung HF, Tsai JC, Wu HY, Chiou AF. The effects of Baduanjin exercise on fatigue and quality of life in patients with heart failure: a randomized controlled trial. Eur J Cardiovasc Nurs. 2018;17(5):456–466. PMID: 29189045. doi:10.1177/1474515117744770
51. Hägglund E, Hagerman I, Dencker K, et al. Effects of yoga versus hydrotherapy training on health-related quality of life and exercise capacity in patients with heart failure: a randomized controlled study. Eur J Cardiovasc Nurs. 2017;16(5):381–389. doi:10.1177/1474515117690297
52. Jain AK, Subhash CM, Bhola SV, et al. Effect of yoga lifestyle in patients with heart failure: a randomized control trial. Int J Yoga. 2022;15(1):40–44. doi:10.4103/ijoy.ijoy_183_21
53. Volterrani M, Caminiti G, Perrone MA, et al. Effects of concurrent, within-session, aerobic and resistance exercise training on functional capacity and muscle performance in elderly male patients with chronic heart failure. J Clin Med. 2023;12(3):750. PMID: 36769399; PMCID: PMC9917949. doi:10.3390/jcm12030750
54. Liu SP, Zhou JG, Jin Y, et al. Therapeutic efficacy of shexiang baoxin pill combined with exercise in patients with heart failure with preserved ejection fraction: a single-center, double-blind, randomized controlled trial. Chin J Integr Med. 2023;29(2):99–107. PMID: 36484921; PMCID: PMC9734389. doi:10.1007/s11655-022-3627-3
55. Saeidi M, Ravanbod R, Pourgharib Shahi MH, et al. The acute effects of 2 different intensities of resistance exercise on autonomic function in heart failure patients: a randomized controlled trial. Anatol J Cardiol. 2023;27(5):266–273. PMID: 37119185; PMCID: PMC10160845. doi:10.14744/AnatolJCardiol.2022.2282
56. Sadek Z, Salami A, Youness M, et al. A randomized controlled trial of high-intensity interval training and inspiratory muscle training for chronic heart failure patients with inspiratory muscle weakness. Chronic Illn. 2022;18(1):140–154. PMID: 32370544. doi:10.1177/1742395320920700
57. Laoutaris ID, Piotrowicz E, Kallistratos MS, et al. Combined aerobic/resistance/inspiratory muscle training as the ‘optimum’ exercise programme for patients with chronic heart failure: ARISTOS-HF randomized clinical trial. Eur J Prev Cardiol. 2021;28(15):1626–1635. PMID: 33624071. doi:10.1093/eurjpc/zwaa091
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Factors Associated with Health-Related Quality of Life in Older Persons Residing in Nursing Homes
Boström AM, Cederholm T, Faxén-Irving G, Franzén E, Grönstedt H, Seiger, Vikström S, Wimo A
Journal of Multidisciplinary Healthcare 2022, 15:2615-2622
Published Date: 11 November 2022
Skin Barrier Repair and Nursing Care in Patients with Atopic Dermatitis: A Narrative Review
Chen X
International Journal of General Medicine 2025, 18:6803-6819
Published Date: 7 November 2025
Differential Effects of Telehealth on Psychological Outcomes in Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials
Sugiharto F, Trisyani Y, Nuraeni A, Abdullah KL
Therapeutics and Clinical Risk Management 2026, 22:617167
Published Date: 30 June 2026