")
Back to Journals » International Journal of General Medicine » Volume 16
Impact of COVID-19 Pandemic on Weight Change Among Adults in the UAE
Authors Al Zaman K , Ahmed S , Alshamsi A, Alshamsi A, Alshdaifat B, Alaleeli S, Mussa BM
Received 9 February 2023
Accepted for publication 18 April 2023
Published 5 May 2023 Volume 2023:16 Pages 1661—1670
DOI https://doi.org/10.2147/IJGM.S407934
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Khaled Al Zaman,1 Shahad Ahmed,1 Alya Alshamsi,1 Amna Alshamsi,1 Bashar Alshdaifat,1 Shamsa Alaleeli,1 Bashair M Mussa2
1College of Medicine, University of Sharjah, Sharjah, United Arab Emirates; 2Basic Medical Science Department, College of Medicine, University of Sharjah, Sharjah, United Arab Emirates
Correspondence: Bashair M Mussa, University of Sharjah, College of Medicine, Basic Medical Science Department, P.O. Box: 27272, Sharjah, United Arab Emirates, Tel +971-65057220, Fax +971-6558579, Email [email protected]
Background: The COVID-19 pandemic which started in November 2019 and since then has led to multiple lockdowns aimed towards controlling the pandemic, these lockdowns contributed to major changes in individuals’ lifestyles including eating patterns and restriction of physical activity due to continues house confinement. Such changes have significantly contributed to weight change, with increasing rates of obesity in the UAE, COVID-19 have posed a major concern to the country’s obesity levels.
Aim: To measure the prevalence and investigate the views related to weight change among adults in the UAE during the COVID-19 pandemic.
Methods: A cross-sectional study was conducted through a self-administered online questionnaire distributed using social media platforms between February 15th and March 14th, 2021. The sample size was 439 adults in the UAE (18– 59 years), collected by volunteer sampling. Analysis was done using SPSS with a significance of 5.0%. Exclusion criteria included pregnancy and bariatric surgeries history.
Results: 51.1% of participants gained weight, 36.2% lost weight and 12.7% maintained their weight. Meal consumption frequency and weight gain were correlated. Consuming fast food resulted in 65.7% of participants gaining weight. 66.2% of people who lost weight during the COVID-19 pandemic did exercise. Stress management and sleeping patterns were not contributing factors to the weight change. 64.4% of the participants who were not satisfied with their weight and believed that they need to make changes in their lifestyle received no guidance from professional personnel to reach their desired weight.
Conclusion: In this study, the majority of participants have witnessed an increase in weight. UAE health authorities must provide guidance and support to the population via structured nutritional programs and lifestyle awareness campaigns.
Keywords: United Arab Emirates, COVID-19, weight change, weight gain, weight loss, pandemic, dietary habits, physical activity
Introduction
COVID-19 restrictions and obligatory quarantine guidelines had limited opportunities for socializing and outdoor physical activities. This led to many challenges and lifestyle changes, including eating practices, physical activity patterns, sleeping habits, stress and anxiety caused by confinement during the pandemic and the fear of contracting COVID-19 infection.1 An American Psychological Association survey found that 42.0% of US adults reporting undesired weight gain since the start of the pandemic.2 A newly published research article in the UAE reported a 31.0% increase in weight among the 1012 participants in the study.3 Moreover, in an article conducted among adult Americans during the pandemic, pre-pandemic weight status was a statistically significant predictor of pandemic weight gain. Thus, weight gain was higher in the group who reported being very overweight before the pandemic.4 According to a recently released research study from Saudi Arabia, there was a significant change in weight between the pre-2020 and post-2020 periods, with almost 10.0% of the population shifting into either overweight or obese BMI categories. The results of this study were consistent with the results of the adult American study, as 4.8% of those with normal BMI pre-2020 had shifted to overweight or obese classes in post-2020, and 5.1% of those who were overweight had shifted to obese class.5
Obesity and overweight represent a worldwide concern that is significantly rising by the minute, according to the World Health Organization. In 2016, more than 1.9 billion adults, 18 years and older, were overweight; of these, over 650 million individuals were obese,6 and it is estimated that 2.7 billion adults are going to become overweight by the year 2025.7 Unfortunately, the United Arab Emirates is suffering from this uprising problem. In 2007, the obesity prevalence in the UAE adult population was 21.5%, then it jumped to 29.9% in 2016. It seems that the COVID-19 pandemic and home quarantine may have worsened these problems and aggravated their magnitude.8 Social distancing, protective actions and strategies undertaken by the UAE government to control and reduce the spread of COVID-19 infection negatively impacted the population’s physical activity and led to a more sedentary lifestyle. The government has urged the public to stay home unless it is necessary to perform essential jobs or obtain essential supplies. Individuals were also asked to use their own cars, with a maximum capacity of three people seated in each vehicle. People were also advised to avoid going to public places and maintaining social distancing rules when gathering with family members to ensure their safety. According to a recent study, this change promoted increased screen time exposure (e.g. computers and tablets in distant learning), limitation of outdoor physical activities (e.g. closure of gyms and physical training centers) that have caused a reduction in energy expenditure and had a strong association with weight change during the lockdown period. This can be seen in a study conducted in the UAE reporting that 38.5% of the study population did not engage in physical activity.3 Furthermore, this influenced the food and dietary choices related to daily life patterns, which were associated with adverse changes in body weight.9 On the contrary, another study conducted among 415 adults living in Kuwait reported a significant decrease in the frequency of fast-food and takeaway food consumption and an increase in the percentage of home-cooked food to adopt a healthier lifestyle and avoid any chance of infection transmission.10 In addition, the changes in daily life routines and stress during the lockdown and home quarantine affected the quality of sleep of individuals; resulting in sleep disturbances and abnormal sleeping patterns, that has been implicated in increasing late-night snacks and skipping of breakfast, which negatively influenced body weight compared to pre-COVID-19 period.1 In a recently released paper that systematically reviewed longitudinal studies on how eating habits changed throughout the pandemic, there was a decline in adherence to healthy diets. This was represented by an increase in the frequency and amount of food eaten, with greater consumption of snacks, sweets and processed foods and a decreased consumption of fruits, vegetables, and fresh food.11 It has been found that the unhealthy food habits and negative lifestyle changes such as increased screen time and decreased physical activity are the main contributors to weight change during the COVID-19 pandemic, with a higher risk of weight change reported in pre-COVID-19 obese individuals or people living in macroeconomic regions.12 Therefore, the present study aimed to investigate the prevalence and the views related to weight change among adults in the UAE during the COVID-19 pandemic.
Materials and Methods
Study Design, Setting and Population
The present cross-sectional study was conducted in Sharjah, UAE, and the targeted population included adults living in the UAE (age range 18–59 years). All pregnant females and individuals who underwent bariatric surgeries or gastric balloon procedures to lose weight during their lifetime were excluded. Using Cochran’s formula, a volunteer sample size of 385 was calculated but was increased to 425 to give a chance for potential incomplete responses that were expected to happen during data collection. This ensured that we reached the calculated sample size and in total 500 responses were received.
Ethical Consideration
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University of Sharjah (REC-21-02-09-04-S). Written informed consent has been obtained from the participants to publish this paper. Although this research was anonymous, confidentiality was achieved by ensuring that the participants data were safe and secure. All the data were kept in an encrypted drive, locked with a password, given only to the researchers and the research supervisor.
Data Collection
A structured self-administered online questionnaire was used; the primary investigators created it following a review of related literature.1,3,13 The studies whose questionnaires were used in developing this research instrument developed their Questions based on a previous national nutrition survey,14 the International Physical Activity Questionnaire Short Form (IPAQ-SF), to measure the physical activity intensity and estimate the levels of activity15 and the Copenhagen Psycho-social Questionnaire (COPSOQ-II) to asses mental stress and strains usually in the work environment.16 In addition, the investigators added some questions from the weight and lifestyle management questionnaire that was developed by Cleveland Clinic Canada.13 The questionnaire consisted of 31 questions, divided into 6 different sections: demographics which consisted of 10 questions including date of birth, sex, nationality, marital status, and education level. The next section was weight change which had 7 questions about participants’ weight, height, perception, and weight satisfaction. The third section asked about the participant’s eating habits, and it had 5 questions inquiring about the type of food consumed and the frequency of food consumption. The physical activities section had 2 questions about the type of activities practiced, their intensity and frequency. The fifth section asked about sleeping habits and consisted of 3 questions, including sleep quality and length. The last section was about stress and anxiety, which had 4 questions asking about stresses experienced during the pandemic and how they were managed. The questionnaire was piloted among a small number of participants to ensure that it was easy to understand and measure the time it took to answer . There were comments related to the wording of some questions. All recommendations and comments were considered, and the questionnaire was adjusted, then distributed among community members using social media platforms such as: Instagram, What’s app, Snapchat, Facebook and Twitter via a link accessed by everyone who received it and all participants were able to access it using their smartphones and fill it with complete privacy.
Anthropometry
Weight and height data were all self-reported by the participants through the online questionnaire. Nevertheless, there were no indications for participants on how to measure their weight or height. Two questions were used to obtain weight change-related information, the current weight refers to the weight of the participants at the time of data collection, on Feb 2021, whilst the weight before refers to the weight before the lockdown period in the UAE, on Feb 2020, with a year gap between the two. Then, the body mass index (BMI) was determined as the ratio of weight in kilograms to height in meters squared (kg/m2). Participants were divided into four categories of BMI classification according to WHO, which include, underweight (BMI <18.5), normal weight (BMI 18.5–24.9), overweight (BMI 25–29.9), and obese (BMI >30).6 Significant weight change was defined as the gain or loss of 10 pounds (4.5 kg) or more than 5% of the normal body weight over 6 to 12 months.17
Statistical Analysis
Data analysis was performed using the IBM SPSS 26. Uni-variate analysis was conducted using descriptive statistics like frequencies, the means and measures of variability, and bivariate analysis using inferential statistics tests, including Chi-square, t-test and Pearson correlation, was done. In all tests, P values less than 0.05 were considered statistically significant.
Results
Participant’s Demographics
A total of 439 responses that met the inclusion criteria were included, out of which 239 (66.7%) were females and 146 (33.3%) were males Figure 1. Participants’ ages ranged between 18 and 59 years, with almost half of the study population (50.8%) falling into the age group 18–25. Most participants were single (61.7%), had a university degree (59.7%) and worked or studied from home (64.0%) Table 1.
 |
Table 1 Participants’ Demographic Characteristics |
 |
Figure 1 In total, 500 responses were received and 61 were excluded according to our exclusion criteria. Therefore the study included the remaining 439 responses out of which 14 did not report their weight. *Did not report either their weight before or during COVID-19 pandemic. |
Weight Change
The mean weight before the COVID-19 pandemic in the sample was 71.07± 19.12 kg, and it became 71.46± 18.85 kg during the COVID-19 pandemic. Comparing the weight before and during the COVID-19 pandemic has revealed that half of the sample (51.1%) experienced weight gain, 36.2% lost weight, and 12.7% experienced no weight change Figure 2.
 |
Figure 2 Weight change during the pandemic. |
The mean BMI before covid-19 pandemic in the sample was 25.91 ±6.002. The BMI was used to classify the sample population into groups, underweight, healthy, overweight, and obese these groups accounted for 34 (8.4%), 164 (40.3%), 124 (30.5%), 85 (20.9%) of the sample population, respectively. During COVID-19 pandemic, the mean BMI was 26.062 ± 5.844. The percentages of each group were 28 (6.9%) underweight, 158 (38.8%) healthy, 125 (30.7%) overweight and 96 (23.6%) are obese Table 2.
 |
Table 2 BMI Groups Before and During COVID 19 Pandemic |
Lifestyles Pattern Changes Before and During the Pandemic
Certain lifestyle patterns, such as the frequency of meal consumption, have changed during the COVID-19 pandemic. There has been a considerable shift in meal frequency patterns from 1 to 2 meals per day to more than 5 meals per day, with the number of persons eating 1 to 2 meals per day decreasing from 160 to 124 and the number of people eating more than 5 meals per day increasing from 24 to 63 (P=0.014). Meanwhile, there was no significant difference between physical activity before and during the pandemic Table 3. The individuals’ sleep quality had deteriorated, as the mean quality of sleep was 7 before the COVID-19 pandemic and 6.77 during the pandemic. Furthermore, out of 439 participants, 161 had lower sleep quality, 116 had higher sleep quality, and 162 had the same sleep quality (P=0.032).
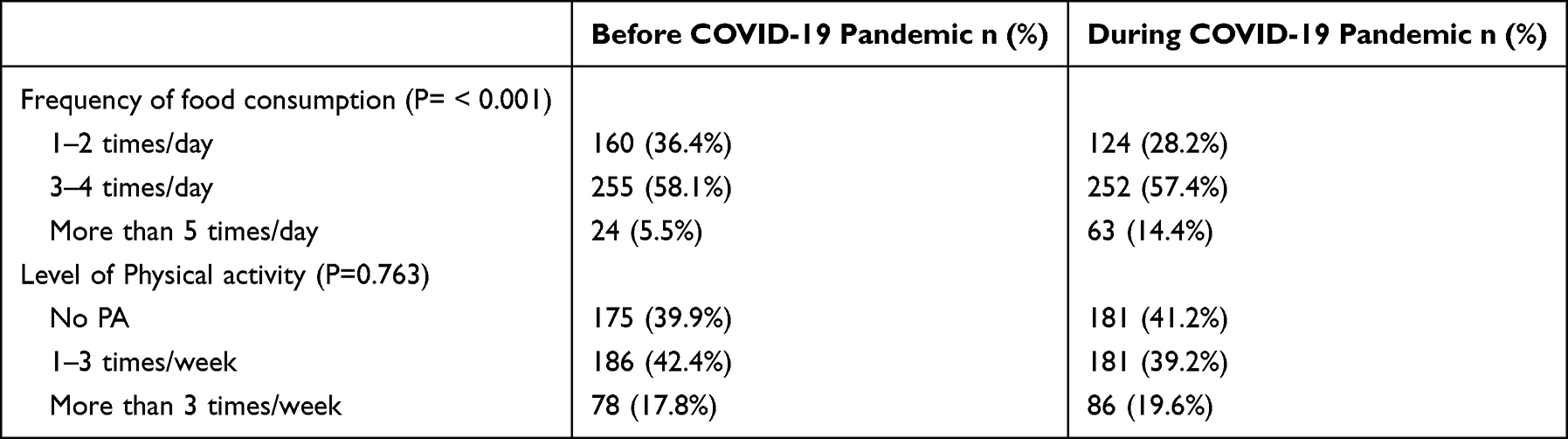 |
Table 3 Lifestyle Pattern Changes Before and During the Pandemic |
Factors Affecting Weight Change
67.0% of the 105 participants who ate fast food gained weight, while 27.6% lost weight. When compared to 368 participants who ate homemade food, 38.0% lost weight and 48.6% gained weight. 41.0% of those who ate (1–2) meals each day lost weight, whereas 42.6% gained weight. 37% of participants who ate three to four meals per day lost weight, whereas 50.6% of them gained weight. 70.0% of people who ate more than five meals per day gained weight. 44.7% of people who gained weight during the COVID-19 pandemic did not participate in any form of physical activity. At the same time, 66.2% of people who lost weight during the COVID-19 pandemic did participate in physical activity. In addition, other parameters were assessed, and the outcomes have shown that there was no significant relationship between stress management and the weight change; even though some participants reported a change in their eating habits when stressed, these changes did not have a significant effect on weight change Table 4. There was not an important correlation between the quality of sleep during the COVID-19 pandemic and weight change.
 |
Table 4 Factors Affecting Weight Change |
Individual’s Views Related to Their Weight and Body Image During the COVID-19 Pandemic
The majority of the study participants were unhappy with their present weight, believing that they needed to shed a few kilos or a large amount of weight (more than 5 kg), with a total percentage of 69.5%. It is noteworthy that 323 (73.6%) of the participants received no weight-loss advice, and of those 323 participants, only 28.8% were satisfied with their weight, 64.4% would like to lose weight (39.3% would like to lose a few kilograms and 25.1% believed they have a significant amount of weight to lose) and 6.8% believed they would like to gain weight Table 5.
 |
Table 5 Weight Satisfaction |
Discussion
The findings of the present study, conducted on UAE adults during COVID-19 (February and March 2021), demonstrated significant changes in lifestyle parameters and behaviors compared with prior to and post the outbreak of COVID-19. Regarding weight change, the results of this study indicated that 217 (51.1%) participants of the study sample have gained weight during COVID-19. In agreement with this finding, previous reports in UAE have shown that 31.0% of the subjects gained weight during the pandemic.3 Furthermore, studies by the World Obesity Federation and AlMughamis et al showed similar outcomes. This result is also consistent with other literature, which meets the expectations due to the significant alteration in daily life activities.7,18 In the current study, certain lifestyle behaviors were seen that could be attributed to the change in weight and may eventually increase the rates of obesity. Among the study participants, people who gained weight reported the highest frequency of food consumption (More than 5 times/day); this can be explained by the long home-stay duration due to online and distant learning and remote working, especially in the early COVID-19 pandemic. Additionally, in contrast to some literature, fast food consumption was reported to be the highest among the group of people who gained weight compared to homemade food.3,19 This factor was not significant in the previous studies. It can be justified that those studies were conducted during the early lockdown period and imposed restrictions, where most people shifted away from fast food as per restrictions and as a way of immune support due to the fear associated with contracting the disease. As our results suggest, this pattern did not stay the same by the time we collected our data, when the fear of food-borne COVID-19 transmission was reduced, people returned to fast food, which may explain why we got such results in comparison to the other studies. Furthermore, with increased stay-at-home duration, unhealthy eating patterns and behaviors have been reported in recent studies, including breakfast skipping and in-between meals and late-night snacking, which also had a significant influence on the increased rates of overweight and obesity.18,20 Emotional eating was not a significant factor in the current study; however, it was highly linked with weight gain during the pandemic.21
There was no significant difference between physical activity before and during the pandemic; a possible explanation for this is that the current study had a higher percentage of younger age groups who seemed to be healthy and physically active before the pandemic and, thus, continued to maintain the same trend during the pandemic. The lack of physical activity was more evident in the group who gained weight during the pandemic (44.7%). This behavior is consistent with the outcome seen in this study and the Papaspanos’s study (2020).20 On the contrary, 66.2% of participants who lost weight reported being physically active. The present study showed that 55.0% (239) of our participants can manage stress well; this might be because 50.8% of our participants were in the age group 18–25. Younger age groups tend to use online resources to cope with and relieve stress created by the pandemic through chatting and gaming. Individuals’ reactions to stress were influenced by their age and developmental stage. Most studies have found that older and younger age groups have different techniques to cope with stress. Elderly individuals were thought to have less influence over their surroundings than adults, which may impair their coping abilities.22 Our study showed no significant relationship between stress eating and weight loss or weight gain. However, 57.1% (250) of the participants stated that they occasionally tend to eat more when feeling stressed, unhappy, angry, or bored. In contrast, 49.7% (221) of the participants have chosen to eat less. This negative association was also observed in British civil servants aged 35–55 in a prospective cohort study.23 On the other hand, there was no correlation between the quality of sleep during the pandemic and weight change. In the questionnaire, participants had to choose a number from 1 to 10 to rate their sleep quality. The majority chose 8 (mode) as the rate of quality of sleep before the pandemic and after the pandemic. This explains why there was no correlation between sleep quality and weight change, as most participants did not have any change in their sleep quality. Also, there are several possible explanations why we find that the overall quality of sleep did not change during the pandemic. Due to semi-lockdown measures, daily living slowed down significantly for a broad portion of the population, perhaps reducing time pressure. There is also evidence that during a recession, individuals devote more time to leisure activities.24,25 Most of our participants were from the younger age group (18–25), so our results might be very subjective as they do not have to wake up early in the morning; hence, the quality of sleep did not change. Whereas, if the majority were from an older age group, they might have difficulties in sleeping as work stress and being confined at home might affect their psychological well-being. Regarding weight satisfaction, in the group who did not receive any healthcare guidance about weight and lifestyle changes, the majority were the least satisfied with their current weight and reported the need to lose weight. The reasons behind not receiving guidance can be explained by the less accessibility of resources and the fear of transmission of COVID-19, especially at the beginning of the pandemic. Our recommendation is to encourage people who are unsatisfied with their weight to seek professional guidance and support regarding lifestyle change plans and nutritional habits programs. Our study provides new insight into the relationship between the COVID-19 pandemic and the weight changes that have occurred due to the restrictions and quarantine guidelines. It aided in identifying individuals who may be most at risk for future adverse health outcomes on account of increased weight and BMI. Should another pandemic or lockdown be required in the future, people at high risk must be guided from the start to avoid future complications. An example of guidance in the UAE is the launch of the National Nutritional Strategy 2022–2030 by the Ministry of Health and Prevention; the objective of this strategy aims to develop and implement a variety of food systems that are designed to provide healthy diets and support the health systems and to provide comprehensive coverage of nutrition education and social protection measures for all age groups. The strategy is built on a participatory framework that includes a wide range of partners. It aims to develop a healthy food system through sustainable practices.26 We were able to support the findings of other studies conducted in different countries and regions that came up with the same conclusions as our study.
Limitations of the Study
There are several limitations to this study. A self-selection bias was introduced due to a volunteering sample approach. Since the weight and height were self-reported, there is a possibility that people under-reported their weight, resulting in an underestimation of the actual difference. There were no specific recommendations given as to when the participants were supposed to measure their weight. Furthermore, most of the research sample consisted of the younger population, which may have resulted in a minor variation in their physical activity. However, it might be due to the prolonged sitting hours spent working from home. Participants with comorbidities were not excluded. This study can be improved by measuring the participant’s height and weight instead of being self-reported. Further questions regarding use of weight loss supplements, medications that might affect weight change, stress management, sleep patterns and physical activity may be needed to understand better the factors affecting weight change.
Conclusion
According to the findings of this study, the COVID-19 pandemic lockdown altered the lifestyle habits of a proportion of adults in the UAE, resulting in a significant increase in weight. The COVID-19 pandemic still influences individuals’ lifestyle practices with a well-renowned impact on dietary habits and physical activity. COVID-19 restrictions and obligatory quarantine guidelines have limited opportunities for socializing and outdoor physical activities; it may be viewed as a new indirect factor that triggers various new behaviors that further influence lifestyle and body weight by default. Our findings might help establish nutrition and lifestyle guidelines for maintaining a healthy weight throughout the pandemic. The UAE’s health authorities must guide and support the population via structured nutritional programs and lifestyle awareness campaigns.
Abbreviations
UAE, United Arab Emirates; WHO, World Health Organization; BMI, Body Mass Index; SPSS, Statistical Package for Social Sciences.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of University of Sharjah (REC-21-02-09-04-S). Written informed consent has been obtained from the participants to publish this paper.
Acknowledgments
The authors would like to thank all people who were involved in the present study for their valuable participation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest, financial or otherwise.
References
1. Gallè F, Sabella EA, Ferracuti S, et al. Sedentary behaviors and physical activity of Italian undergraduate students during lockdown at the time of CoViD-19 pandemic. Int J Environ Res Public Health. 2020;17(17):6171. doi:10.3390/ijerph17176171
2. American Psychological Association. One year on: unhealthy weight gains, increased drinking reported by Americans coping with pandemic stress; 2021. Available from: https://www.apa.org/news/press/releases/2021/03/march-weight-change.
3. Cheikh Ismail L, Osaili TM, Mohamad MN, et al. Eating habits and lifestyle during COVID-19 lockdown in the United Arab Emirates: a cross-sectional study. Nutrients. 2020;12(11):3314. doi:10.3390/nu12113314
4. Khubchandani J, Price JH, Sharma S, Wiblishauser MJ, Webb FJ. COVID-19 pandemic and weight gain in American adults: a nationwide population-based study. Diabetes Metab Syndr. 2022;16(1):3314. doi:10.1016/j.dsx.2022.102392
5. Alshahrani SM, Alghannam AF, Taha N, et al. The impact of COVID-19 pandemic on weight and body mass index in Saudi Arabia: a longitudinal study. Front Public Health. 2022;9:775022. doi:10.3389/fpubh.2021.775022
6. Obesity and overweight; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
7. Prevalence of obesity. Available from: https://www.worldobesity.org/about/about-obesity/prevalence-of-obesity.
8. Department, P. & 26, A. UAE - prevalence of obesity in the adult population 2016; 2020. Available from: https://www.statista.com/statistics/978079/uae-prevalence-rate-obesity-adult-population/.
9. Reyes-Olavarría D, Latorre-Román PÁ, Guzmán-Guzmán IP, et al. Positive and negative changes in food habits, physical activity patterns, and weight status during COVID-19 confinement: associated factors in the Chilean population. Int J Environ Res Public Health. 2020;17(15):5431. doi:10.3390/ijerph17155431
10. Husain W, Ashkanani F. Does COVID-19 change dietary habits and lifestyle behaviours in Kuwait: a community-based cross-sectional study. Environ Health Prev Med. 2020;25(1):1–6. doi:10.1186/s12199-020-00901-5
11. González-Monroy C, Gómez-Gómez I, Olarte-Sánchez CM, Motrico E. Eating behaviour changes during the COVID-19 pandemic: a systematic review of longitudinal studies. Int J Environ Res Public Health. 2021;18(21):11130. doi:10.3390/ijerph182111130
12. Drywie ´n MŁE, Hamulka J, Zielinska-Pukos MA, Jeruszka-Bielak M, Górnicka M. The COVID-19 pandemic lockdowns and changes in body weight among Polish women. A cross-sectional online survey PLifeCOVID-19 study. Sustainability. 2020;12(18):7768. doi:10.3390/su12187768
13. Cleveland Clinic Canada. Weight and lifestyle management questionnaire; 2021. Available from: https://studylib.net/doc/8321024/weight-and-lifestyle-management-questionnaire.
14. Ng SW, Zaghloul S, Ali H, et al. Nutrition transition in the United Arab Emirates. Eur J Clin Nutr. 2011;65:1328–1337. doi:10.1038/ejcn.2011.135
15. Lee PH, Macfarlane DJ, Lam TH, Stewart SM. Validity of the international physical activity questionnaire short form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act. 2011;8(115):336. doi:10.1186/1479-5868-8-115
16. Pejtersen JH, Kristensen TS, Borg V, Bjorner JB. the second version of the Copenhagen psychosocial questionnaire. Scand J Public Health. 2010;38:8–24. doi:10.1177/1403494809349858
17. Jameson J, Fauci AS, Kasper DL, Hauser SL, Longo DL, Loscalzo J, editors. Unintentional Weight Loss., Harrison’s Principles of Internal Medicine. McGraw Hill; 2018.
18. AlMughamis N, AlAsfour S, Mehmood S. Poor eating habits and predictors of weight gain during the COVID-19 quarantine measures in Kuwait: a cross sectional study. F1000Res. 2020;12:914. doi:10.12688/f1000research.25303.1
19. Chenarides L, Grebitus C, Lusk JL, Printezis I. Food consumption behavior during the COVID-19 pandemic. Agribusiness. 2020;27(1):44–81. doi:10.1002/agr.21679
20. Papaspanos N. Effects of COVID-19 home confinement on eating behaviour and physical activity: results of the ECLB- COVID19 international online survey. Komp Nutr Diet. 2020;1(1):19–21. doi:10.1159/000512852
21. Borgatti AC, Schneider-Worthington CR, Stager LM, et al. The COVID-19 pandemic and weight management: effective behaviors and pandemic-specific risk factors. Obes Res Clin Pract. 2021;15(5):518–521. doi:10.1016/j.orcp.2021.06.007
22. Aldwin CM, Sutton KJ, Lachman M. The development of coping resources in adulthood. J Pers. 1996;64(4):837–871. doi:10.1111/j.1467-6494.1996.tb00946.x
23. Kivimäki M, Head J, Ferrie JE, et al. Work stress, weight gain and weight loss: evidence for bidirectional effects of job strain on body mass index in the Whitehall II study. Int J Obes. 2006;30(6):982–987. doi:10.1038/sj.ijo.0803229
24. Colman G, Dave D. Exercise, physical activity, and exertion over the business cycle. Soc Sci Med. 2013;93:11–20. doi:10.1016/j.socscimed.2013.05.032
25. de Quervain D. The Swiss corona stress study. open science framework; 2020. Available from: https://osf.io/jqw6a/.
26. National nutrition strategy 2030 - the official portal of the UAE Government; n.d.. Available from: https://u.ae/en/about-The-uae/strategies-initiatives-and-awards/strategies-plans-and-visions/health/national-nutrition-strategy-2030#:~:text=The%20National%20Nutrition%20Strategy%202030,nutrition%20to%20all%20age%20groups.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.