")
Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Impact of COVID-19 Pandemic on the Exacerbation Rates in COPD Patients in Southern India – A Potential Role for Community Mitigations Measures
Authors Acharya VK, Sharma DK, Kamath SK, Shreenivasa A , Unnikrishnan B , Holla R, Gautham M, Rathi P , Mendonca J
Received 20 March 2023
Accepted for publication 24 July 2023
Published 29 August 2023 Volume 2023:18 Pages 1909—1917
DOI https://doi.org/10.2147/COPD.S412268
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Richard Russell
Vishak K Acharya,1,2 Deepthi K Sharma,1,2 Sindhu K Kamath,1,2 A Shreenivasa,1,2 Bhaskaran Unnikrishnan,1,3 Ramesh Holla,1,3 Manish Gautham,2,4 Priya Rathi,1,3 Jane Mendonca1,2
1Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, India; 2Faculty in Department of Pulmonary Medicine, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, India; 3Faculty in Department of Community Medicine, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, India; 4Royal Liverpool University Hospital, Liverpool, UK
Correspondence: Vishak K Acharya, Department of Pulmonary Medicine, Kasturba Medical College, Mangalore, Manipal Academy of Higher Education, Manipal, Karnataka, 575001, India, Tel +91-9448331570, Email [email protected]
Introduction: The impact of the coronavirus 2 (SARS-CoV-2) pandemic and the effect of preventive health strategies on acute exacerbations of chronic obstructive pulmonary disease (AECOPD) are largely unknown. The public health model imposed during the pandemic and the lessons learnt have implications on recommending future preventive strategies for COPD care in general and exacerbations in particular.
Aim: This study endeavors to assess the role of preventive strategies of COVID-19 on exacerbation rates of COPD during the lockdown period compared to similar periods the previous year and assess the compliance to preventive strategies for COVID-19 among COPD patients.
Methods: This is a hospital-based descriptive cross-sectional study at a tertiary care center. AECOPD in patients during a period spanning five months in the pre-lockdown days was compared with exacerbation rates for a similar period during the national lockdown.
Results: Sixty-eight patients were recruited (mean age: 67.38) among whom 47 were males and 21 were females. There were only 7 (10.3%) reported admissions during the lockdown period of 5 months compared to 50 (73.5%) during the corresponding period pre-lockdown. Mild exacerbations reported during the lockdown period were also significantly less with only 17 (25%) against 58 (85.3%) during the pre-lockdown period. Adherence to measures such as donning of masks, hand hygiene, and social distancing was observed among COPD patients with good compliance to the health practices promulgated in the pandemic.
Discussion: A significant reduction in exacerbation rates among AECOPD patients during the period of lockdown was observed compared to a similar period the year prior. Noticeable were the findings that both community-based milder exacerbations and severe exacerbations necessitating hospitalizations showed a reduction during the period of lockdown. Adaptability, compliance and acceptance to usage of masks, hand hygiene measures, and norms such as physical distancing were observed in the majority of COPD patients.
Keywords: COPD, exacerbation, pandemic, physical distancing, face masks
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has affected millions of people around the world since the beginning of 2020. During the spate of this pandemic, there has been a lot of focus on its impact on those with comorbidities, as adverse outcomes in terms of hospitalizations and mortality were significantly higher in this group. However, surprisingly contrary to the general perception, prevalence of COPD and bronchial asthma among the COVID as a comorbidity is quite low1,2 compared to the quantum of their disease burden.3
COPD is the third leading cause of death worldwide.4 Most COPD deaths are due to acute exacerbation. Besides, acute exacerbations among COPD play a crucial role in disease progression, hospitalizations, morbidity, and health burden from the disease. Several risk factors and triggers are identified as acute exacerbations. These include smoking, air pollution, severe airflow limitation, bronchiectasis, prior exacerbations, comorbidities, high blood eosinophil counts and infections, both bacterial and viral.5
There has been a common clinical observation shared by pulmonologists worldwide on reduced acute exacerbation of COPD (AECOPD) and asthma in the last quarter, a juncture when the pandemic wreaked havoc in health care. This has not been backed by verifiable data as yet from scientific studies due to contextual limitations on account of acuteness of the COVID pandemic.
There is a likelihood that the basic measures practiced widely during this pandemic such as government-mandated lockdown, quarantine, hand washing and donning of face masks could be the reasons for better control of exacerbations in this pandemic season.
Aim
To assess the impact of the coronavirus 2 pandemic on AECOPD rates and assess the role of preventive measures practiced during the lockdown phase of the pandemic.
Objectives
1. To measure hospitalization rates due to acute exacerbation of COPD during the lockdown period in comparison with similar rates during the previous year period pre-lockdown.
2. To estimate mild to moderate exacerbation of COPD treated as outpatients during the lockdown period in comparison with similar rates during the previous year period pre-lockdown.
3. To assess the adherence, attitude, practice and perception of our COPD patients to the practices during the pandemic, of donning of masks, hand hygiene, and physical distance.
Methods
Study Design
The study was a hospital-based descriptive cross-sectional study carried out at a tertiary care teaching hospital in Mangalore, a coastal town in the state of Karnataka, southern India.
Ethics: The study was initiated after requisite approval from the research committee and institutional ethics committee Kasturba Medical College Mangalore on January 22, 2021. An information sheet with study details was provided to the patients and they were enrolled in the study after providing written informed consent for study participation.
Patients disgnosed with COPD who were being treated at the department of Pulmonary Medicine were enrolled for the study. The database was reviewed and patients who met the inclusion criteria for COPD and exacerbation states confirmed by clinical, radiological and spirometry criterion as per the global initiative of lung disease (GOLD) were included in the study. COPD patients with significant respiratory comorbidities such as bronchiectasis, lung malignancy, lung abscess, empyema, pleural effusions, active tuberculosis were excluded from the study.
Acute exacerbation among known COPD patients during 5 months of lockdown from April 2020 to August 2020 was captured and compared with similar exacerbation rates in the corresponding period of 5 months from April 2019 to August 2019. Outpatient exacerbations were defined as those resulting in a prescription for oral corticosteroids, increased use of rescue inhalers and/or antibiotics, but without hospital admission. Hospitalized exacerbations were defined as admissions to hospital with a documented discharge summary. We also assessed the awareness, practices, and compliance of our COPD patients to preventive strategies advocated for COVID-19 like usage of masks, hygiene, and social distancing.
Baseline data was collected in person from the patients attending as outpatients and in those hospitalized with exacerbations. Follow-up data was collected by a scripted periodic telephone survey. Data abstraction forms were used for collecting the data from the study subjects. It consisted of three sections.
Section 1 – Sociodemographic details
Section 2 – Clinical indicators for exacerbation
Section 3 – Awareness, practices and compliance to preventive strategies practiced during the pandemic
Statistical Analysis
Data were analyzed using SPSS version 25. Quantitative data were summarized as mean and SD while qualitative data were summarized as proportions. As a test of significance the chi-squared test was used to study the association. A P-value of 0.05 was considered a statistically significant difference.
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Results
Sixty-eight patients with COPD were included in the study with baseline characteristics (Table 1). Baseline COPD status assessment revealed that, 38 (60.3%) of patients were classed as GOLD 3 or 4 stage airflow obstruction and the remaining 25 (39.6%) were categorized as GOLD stage 1 and 2 airflow obstruction. Sixteen patients (23.5%) subjects were frequent exacerbators with a history of ≤ 2 admissions while 52 (76.5%) patients had 0–1 admission over the last one year. Thirty-two patients (47.1%) had COPD for more than 10 years, 27 (39.7%) had grade 3 and 4 mMRC scale of dyspnea, 7 (10.3%) patients were on domiciliary oxygen, and 17 (33.3%) had associated pulmonary hypertension (Table 2).
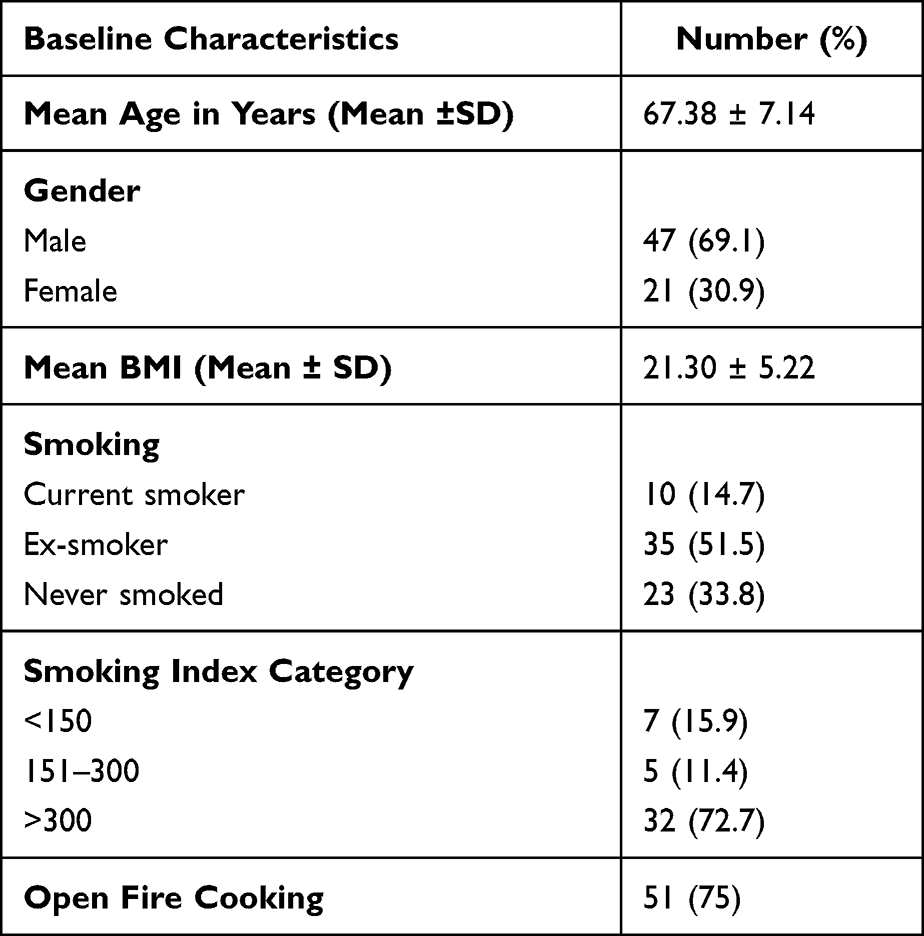 |
Table 1 Baseline Characteristics of Study Population (n=68) |
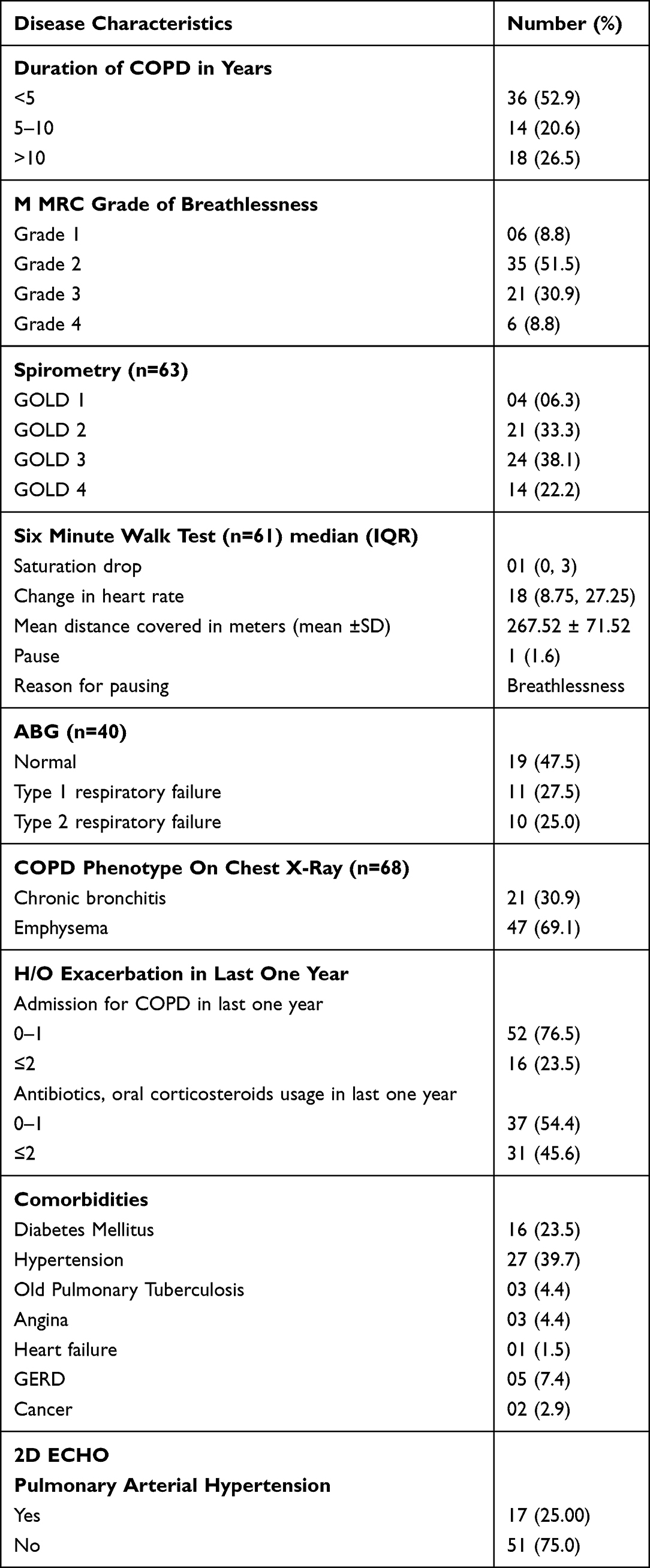 |
Table 2 Disease Characteristics of COPD Patients (n=68) |
Acute Exacerbations
Acute exacerbation of COPD during 5 months of lockdown (from April 2020 to August 2020) requiring hospital admissions were significantly reduced with only 7 (10.3%) reporting admissions compared to 50 (73.5%) during the corresponding period of 5 months’ pre-lockdown the previous year (April 2019 to August 2019). This difference observed in severe exacerbations requiring hospitalization assumed statistical significance (<0.0001) (Table 3).
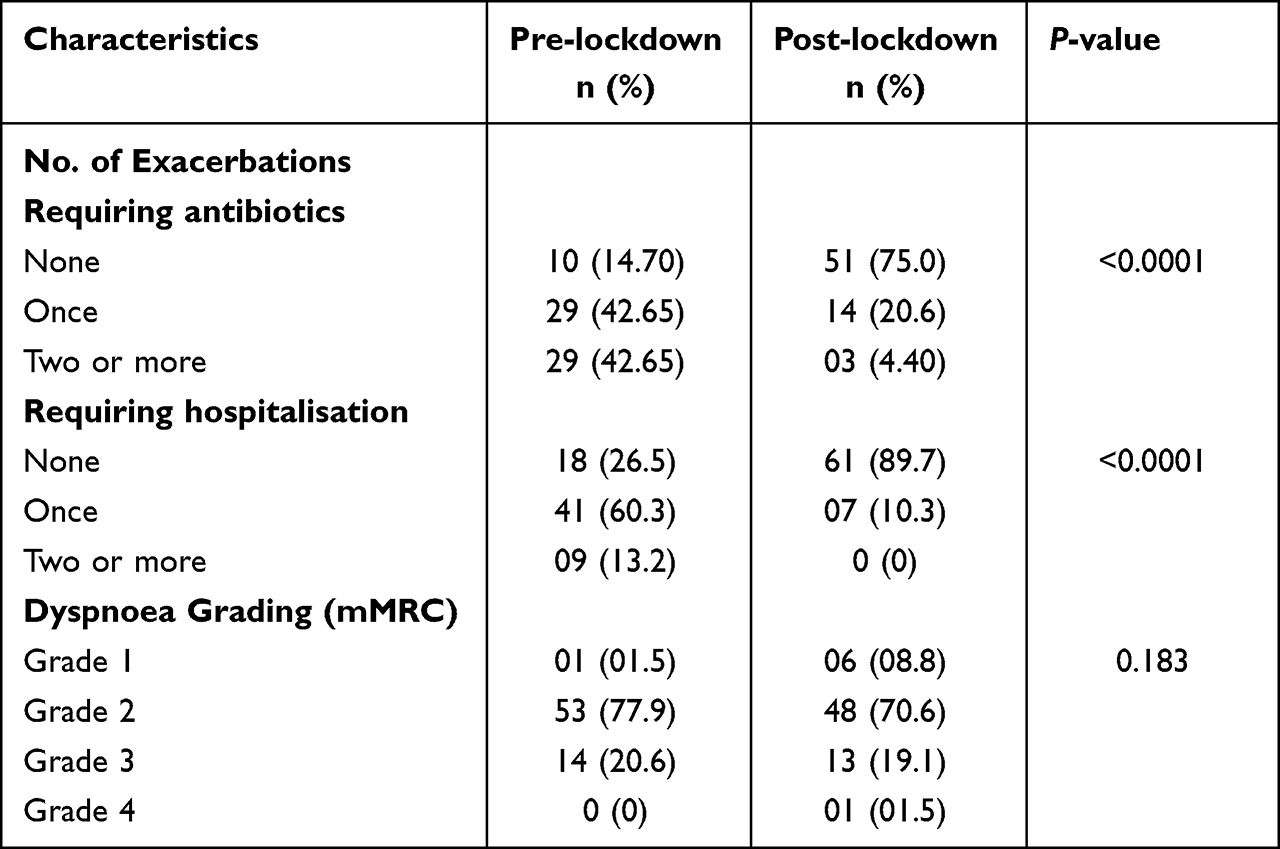 |
Table 3 Pre and Post Lockdown Comparison (n=68) |
Mild to moderate severe exacerbations treated as outpatients requiring antibiotics was also significantly less with only 17 (25%) against 58 (85.3%) in pre-lockdown.
Unsurprisingly, the majority of the exacerbations around 17 (25%) during the lockdown period were managed on an outpatient basis against 7 (10.3%) cases requiring admission.
Symptomatic grading of dyspnea on mMRC was not significantly different irrespective of COPD severity across both the groups in pre- and post-lockdown period.
Face masks, physical distancing, hygiene and health-care access
We assessed the adherence, attitude, practice and perception of our COPD patients to the recent and widely promulgated practices (during the pandemic) of donning of masks, hand hygiene, and physical distance. The majority of the COPD patients (97%) were compliant with face mask usage and most patients (80.3%) were comfortable with the new habit of regular mask usage in most settings whereas a minority (13%) were not comfortable with donning masks – the reason often reported was a feeling of suffocation. Unsurprisingly none of the COPD patients from our database had used face masks before and this was a novel habit for them. The most preferred face masks were cloth masks (78.8%) followed by surgical masks (19.7%) while only a few (1.5%) used N95 masks. Usage of masks was practiced mainly in an outdoor setting (95%) and masks offered most of the COPD patients (84%) a sense of well-being and attributed better COPD control to habit of mask usage.
All patients practiced frequent hand washing, while a minority used alcohol-based sanitizers (11.8%), soap and water solutions were preferred by most (88.2%). Interestingly all the COPD patients followed the norms of outdoor social distancing and avoided large and community gatherings whereas only a few (23.5%) followed physical distancing at homes.
Around half of our patients (52.8%) contacted health-care facilities during the lockdown period of 5 months with the majority of contacts being with the tertiary centers (58.3%) and some (41.7%) accessing local health care. On the contrary, only a few (18.2%) experienced difficulty in accessing health care while the majority (81.8%) had no difficulties in health-care access. Most patients preferred an in-person visit and only a few (5.56%) used video-consultations (Table 4).
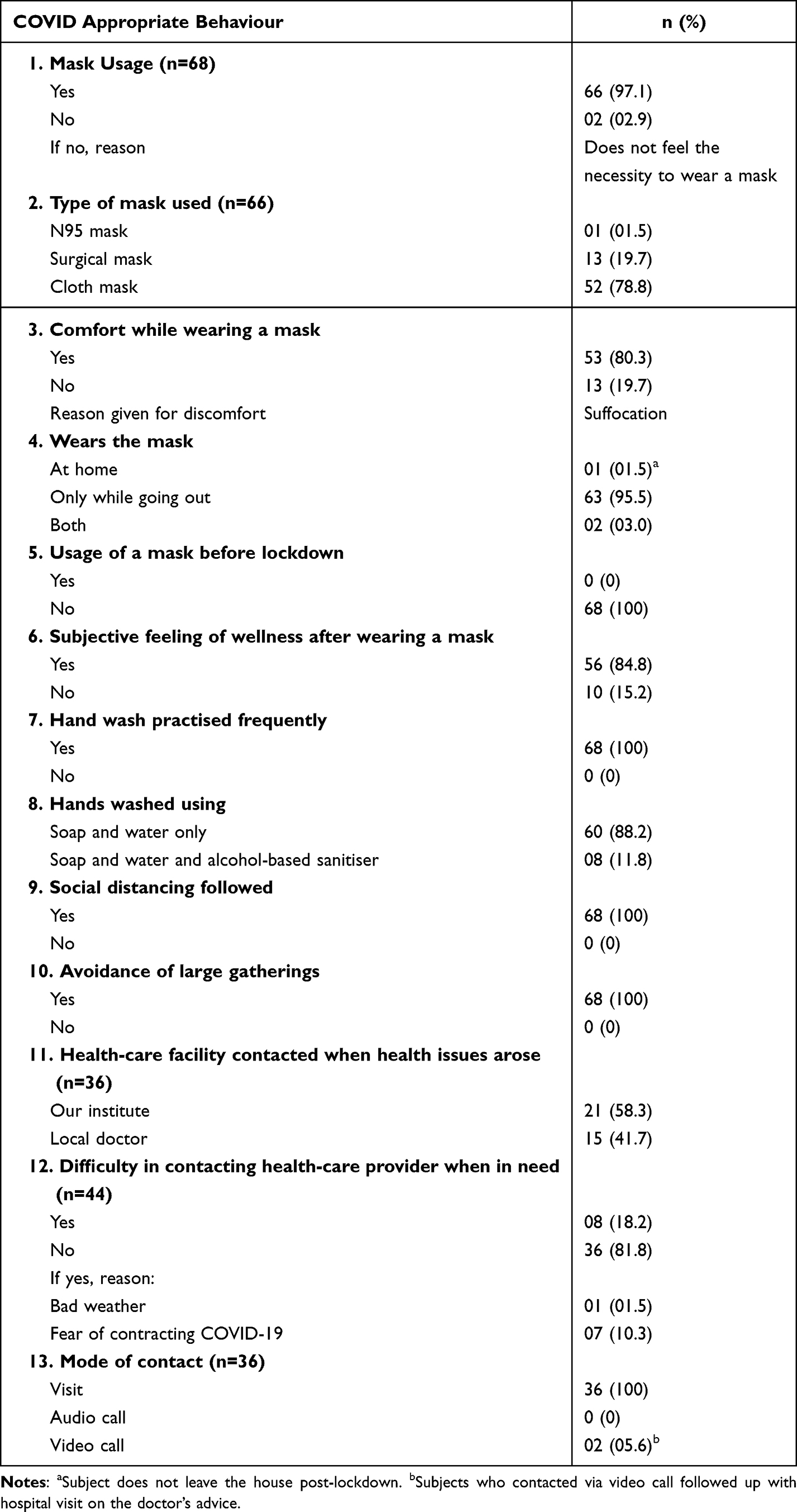 |
Table 4 COVID Appropriate Behaviour Among Study Participants (n=68) |
Discussion
The COVID-19 pandemic has had a telling impact on health care globally. Apart from the direct effect unleashed by the disease itself, there has been untold collateral damage specifically on the population suffering from chronic diseases. Presently, it is a known fact that comorbidities along with age are a definitive risk factor for COVID outcome. However, the impact of COVID on those with chronic respiratory comorbidities is shrouded by lack of clarity. The Global Initiative for Chronic Obstructive Lung Diseases (GOLD)5 has recently recognized that COPD patients are among the worst affected by COVID-19, but gives no mention of their infection rate. The Global Initiative for Asthma (GINA),6 however, has advised asthmatics to continue regular medications and avoid nebulization. The Center for Disease Control and Prevention (CDC)7 have recently noted that patients with COPD and a history of smoking are definitely at a higher risk, whereas patients with asthma might be at a higher risk for severe COVID-19 disease. Surprisingly COPD as a comorbidity has a lesser prevalence factoring in its disease burden compared to other comorbidities such as cardiovascular and systemic in those infected with COVID-19. In a systematic review by Emami et al, the incidence rate of COPD in hospitalized COVID-19 patients was only 0.95%.1 A slew of theories have been proposed, ranging from protective effects of inhaled corticosteroids, a different immune response in patients with chronic respiratory diseases, underdiagnosis of COPD, to the possible benefits due to better hygiene and isolation measures.8 However, emerging data reveals that mortality is much higher among COPD patients if infected with COVID-19.9 A meta-analysis carried out by Zhao et al showed that the risk of severe COVID‐19 in a patient with pre‐existing COPD was 4-fold higher than in patients without COPD.10 As per the existing data, though the mortality, severity and outcome among COPD patients when infected with COVID-19 is higher, the irony is the overall incidence rates of COPD among those infected with COVID-19 is less compared to its disease burden. A reduction in seasonal influenza due to certain community mitigation measures such as face mask wearing has led to the CDC considering that these might be useful adjuncts to influenza vaccination during influenza seasons, particularly for populations at highest risk for severe disease.11
The effect of COVID-19 and the indirect effects imposed by measures such as the lockdown, masks, hygiene, and social distancing on COPD patients has evoked interest and merits serious consideration. There has been a general perception among physicians of marked reduction in non-COVID-19 respiratory infections related exacerbations during the period of the pandemic. On the contrary, one recent study showed an increased number of community managed exacerbations in COPD attributed as due to likely behavioral changes while exacerbations requiring hospital admission showed a decline.12 A meta-analysis of nine pooled studies showed a 50% reduction in admissions for COPD exacerbations during the COVID-19 pandemic period compared to pre-pandemic times, those likely to be associated with a reduction in respiratory viral infections that trigger exacerbations.13 Concurrent with the available data, our observational study showed a significant reduction in exacerbation rates during the 5 months of lockdown compared to the corresponding 5-month period of the pre-pandemic year. These reductions were seen both among those with severe exacerbations requiring hospitalizations (10.3% lockdown v73.5% pre-lockdown) and in those with milder exacerbations managed on an outpatient basis (25% lockdown vs 85.3% pre-lockdown). Our study showed a significant proportion of severe COPD patients with GOLD stage 3 and 4 disease (60%) and some (10%) were on domiciliary oxygen. In spite of a subset of patients with high risk COPD in our study group, a reduction in overall exacerbation rates was a significant observation in our study.
A few extraneous factors may have possibly contributed to the marked low exacerbation rates reported during the lockdown period compared to the pre-lockdown period. These include difficulty in accessing health care and hesitancy in visiting hospitals due to the fear of contracting COVID-19. However as our patients were monitored by telephone and video-consultation services provided during this period it is unlikely that the impact of these factors are of great significance.
These unusual times have led to markedly better air quality partly on account of reduced pollution levels, decrease in the cross infections due to travel, crowd and movement restrictions imposed. It is plausible to assume that these may have contributed to reduction of exacerbation reported due to CRDs unrelated to COVID-19. Another possible explanation for reduced exacerbation rates is due to improved adherence to asthma and COPD medications by the patients as observed by the clinicians during this period of pandemic. Apprehensions over accessibility to health care and awareness among patients that optimized treatment of their lung disease lowers their risk of COVID-19 complications probably were factors leading to good adherence to prescribed medications.
Studies on adaptability, attitude and practices among COPD patients to widely imposed and practiced measures like social distancing, hygiene and face mask usage have been scarce. Our study addressing the behavioral aspects, attitude and the practices followed by the COPD patients also revealed some positive outcomes. The majority of the patients followed hand hygiene even though the methods varied. Social norms advocated during the pandemic such as physical distancing were met with good compliance. Surprisingly, as against the general perception, most of the COPD patients were comfortable with norms of face mask usage and only a minority complained of feeling suffocated. Reassuringly, most patients felt that the mask offered them a sense of protection and well-being that resulted in better control of their baseline COPD disease state. This perhaps ensured good compliance to the usage of face masks especially in outdoor and community settings. The pandemic with the lockdown and travel restrictions also opened up new avenues in health care, in a country like India where tele-medicine and medical informatics were still in their infancy. Patients were able to access health care both virtually and physically in spite of the restrictions and few used tele-consultations too. However, the majority still preferred an in-person visit to a tele-consult.
The conclusions derived from this study are limited by a relatively small sample size. Although the dataset of 68 patients provided adequate power for statistically significant differences in exacerbation between the two groups, a multicenter study with a larger dataset is essential, to validate the results from our study. Since the quantum of stringency of lockdown and compliance to usage of masks, social distancing and hygiene is not uniform across states and countries this may have influenced our study outcome. It warrants substantiation with multicenter studies with a larger representative patient database. Another limitation was the inability to document the reduced exacerbations with supporting evidence like baseline spirometry across both groups. The effect of these mitigation measures is intertwined and assessing their individual effect is a complex exercise beyond the scope of this study. In addition, assessing the individual efficacy of different types of mask on infective exacerbations will lead to meaningful practice recommendations. The study duration of 5 months is too short for a genuine assessment of exacerbations. Since the lockdown was imposed for that period, the study was time constrained. However, since data from correspondingly similar periods were drawn for both phases of the study, the seasonal impact was somewhat nullified.
Systematic review and meta-analysis support the evidence for physical distancing and provide quantitative estimates for models. Robust randomized studies are, however, needed to gauge and substantiate the quantum of evidence for these interventions. It is rational to presume that reduced respiratory infections causing exacerbations among patients with COPD and asthmatics over the last quarter is largely attributable to the current day practices being judiciously followed with use of masks, hygiene, and physical distancing. This pandemic has led to insightful evidence as shown with the decisive results of our study justifying the effectiveness of physical distancing, the safety net provided by the use of masks, and utility of hand hygiene practices. The landmark guidelines GOLD and GINA over the years, have been silent on general and respiratory hygiene measures in patients with chronic obstructive airway diseases. They have largely overlooked the role and utility of masks in certain specific settings. Recommendation on the use of masks in specified high-risk groups like COPD and in certain settings such as mass gathering may be judicious and a productive step that might have an impact on exacerbation rates among COPD patients. It would be prudent to include these basic lifestyle modification and preventive measures among the nonpharmacological interventions for COPD and asthma.14
A study on similar lines in the UK revealed that lockdown was associated with 48% pooled reduction in emergency admissions for COPD relative to the 5-year average. However, no statistical significant change in deaths due to COPD was observed. Lockdown was also associated with 39% reduction in primary care consultations for acute exacerbation of COPD.15
Our study is one of the few studies to assess both community and hospital exacerbations during the lockdown period in compared withthe same corresponding period the previous year, pre-lockdown. The study revealed a significant reduction in exacerbation rates during the period of lockdown compared to the corresponding period pre-pandemic. This reduction in exacerbation was significant as study subjects had a higher proportion of patients with moderate to severe COPD state. A reduction in exacerbation rates across the spectrum, both in patients with severe exacerbation requiring hospitalization and mild exacerbation was noticed. A novel attribute of our study was that it was conducted on stratified COPD severity groups and integrated with health approaches like adaptability, attitude and practices to the mitigation measures imposed during the lockdown. Data from the current pandemic-like findings from our study might help answer critical questions on the effect of community mitigation measures on transmission of infections and reduction in exacerbation rates in stable COPD and asthmatics. In addition, assessing acceptability, optimizing the stringency of these measures, and advocating these practices in special groups could pave the way for novel lifestyle interventions with impactful gains in COPD management.
Declaration
Our study complies with the Declaration of Helsinki.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
We have not received any funding or grants toward conducting the study.
Disclosure
None of the authors has anything to disclose and there is no conflict of interest in any form.
References
1. Emami A, Javanmardi F, Pirbonyeh N, Akbari A. Prevalence of underlying diseases in hospitalized patients with COVID-19: a systematic review and meta-analysis. Arch Acad Emerg Med. 2020;8(1):e35.
2. Grasselli G, Zangrillo A, Zanella A, et al.; COVID-19 Lombardy ICU Network. Baseline characteristics and outcomes of 1591 patients infected with SARS-CoV-2 admitted to ICUs of the Lombardy Region, Italy. JAMA. 2020;323(16):1574–1581. doi:10.1001/jama.2020.5394
3. Goyal P, Choi JJ, Pinheiro LC, et al. Clinical characteristics of Covid-19 in New York City. N Engl J Med. 2020;382(24):2372–2374. doi:10.1056/NEJMc2010419
4. Momtazmanesh S, Moghaddam SS, Ghamari S-H; GBD 2019 Chronic Respiratory Diseases Collaborators. Global burden of chronic respiratory diseases and risk factors, 1990–2019: an update from the Global Burden of Disease Study 2019. EClinicalMedicine. 2023;59:101936. doi:10.1016/j.eclinm.2023.101936
5. Viniol C, Vogelmeier CF. Exacerbations of COPD. Eur Respir Rev. 2018;27(147):170103. doi:10.1183/16000617.0103-2017
6. Global Initiative for Asthma (GINA). Global strategy for the diagnosis and prevention. Global Initiative for Asthma (updated 2020); 2020. Available from: http://ginasthma.org/wpcontent/uploads/2020/04/GINA-2020-full-report_-final.
7. Centers for Disease Control and Prevention. National Center for Health Statistics – homepage; 2020. Available from: https://www.cdc.gov/nchs/.
8. Halpin DMG, Faner R, Sibila O, Badia JR, Agusti A. Do chronic respiratory diseases or their treatment affect the risk of SARS-CoV-2 infection? Lancet Respir Med. 2020;8(5):436–438. doi:10.1016/S2213-2600(20)30167-3
9. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Prevalence, Severity and Mortality associated with COPD and Smoking in patients with COVID-19: a Rapid Systematic Review and Meta-Analysis. PLoS One. 2020;15(5):e0233147. doi:10.1371/journal.pone.0233147
10. Zhao Q, Meng M, Kumar R, et al. The impact of COPD and smoking history on the severity of COVID-19: a systemic review and meta-analysis. J Med Virol. 2020;92(10):1915–1921. doi:10.1002/jmv.25889
11. Olsen SJ, Azziz-Baumgartner E, Budd AP, et al. Decreased Influenza Activity During the COVID-19 Pandemic - United States, Australia, Chile, and South Africa, 2020. MMWR Morb Mortal Wkly Rep. 2020;69(37):1305–1309. doi:10.15585/mmwr.mm6937a6
12. McAuley H, Hadley K, Elneima O, et al. COPD in the time of COVID-19: an analysis of acute exacerbations and reported behavioural changes in patients with COPD. ERJ Open Res. 2021;7(1):00718–2020. doi:10.1183/23120541.00718-2020
13. Alqahtani JS, Oyelade T, Aldhahir AM, et al. Reduction in hospitalised COPD exacerbations during COVID-19: a systematic review and meta-analysis. PLoS One. 2021;16(8):e0255659. doi:10.1371/journal.pone.0255659
14. Vishak AK, Unnikrishnan B, Sindhu K, et al. Have guidelines been oblivious to the obvious? Unmasking the positives from the COVID-19 pandemic. NPJ Prim Care Respir Med. 2021;31(1):11. doi:10.1038/s41533-021-00224-0
15. Alsallakh MA, Sivakumaran S, Kennedy S, et al. Impact of COVID-19 lockdown on the incidence and mortality of acute exacerbations of chronic obstructive pulmonary disease: national interrupted time series analyses for Scotland and Wales. BMC Med. 2021;19(1):124. doi:10.1186/s12916-021-02000-w
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.