Back to Journals » Clinical Epidemiology » Volume 17
Impact of Changes in Patient Reported Outcomes on Healthcare Use After a Self-Management Supportive Intervention for Individuals with Low Back Pain
Authors Grøn S ![]() , Kongsted A, Olsen KR, Koes B, Johansson MS
, Kongsted A, Olsen KR, Koes B, Johansson MS ![]()
Received 21 June 2025
Accepted for publication 12 November 2025
Published 28 November 2025 Volume 2025:17 Pages 1011—1023
DOI https://doi.org/10.2147/CLEP.S548659
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor H Sorensen
Søren Grøn,1 Alice Kongsted,1,2 Kim Rose Olsen,3 Bart Koes,3,4 Melker S Johansson1,3
1Departments of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense M, Denmark; 2Chiropractic Knowledge Hub, Odense M, Denmark; 3Department of Public Health, University of Southern Denmark, Odense M, Denmark; 4Department of General Practice, Erasmus MC, University Medical Center, Rotterdam, The Netherlands
Correspondence: Søren Grøn, Center for Muscle and Joint Health, Departments of Sports Science and Clinical Biomechanics, University of Southern Denmark, Campusvej 55, Odense M, 5230, Denmark, Email [email protected]; [email protected]
Purpose: To investigate the potential impact of changes in patient reported outcome measures (PROMs) on subsequent healthcare use following a self-management supportive program for low back pain.
Patients and methods: Clinical data from a cohort of 2803 participants enrolled in a self-management supportive intervention for LBP (2018 to 2022) was linked with Danish national registry data. PROMs (predictors) were collected at baseline and at 3-months follow-up (end of intervention), including pain intensity, disability, illness perceptions, self-efficacy, and health-related quality of life. Healthcare use (outcome) was measured as the total use in the year before and after the intervention for i) visits to physiotherapists or chiropractors and ii) analgesics use. Associations between standardized changes in PROMs and changes in healthcare use were analyzed using zero-inflated negative binomial regression models and reported as incidence rate ratios (IRRs) with 95% confidence intervals (CIs). Subgroup analyses were conducted for low, medium, and high baseline use of each outcome.
Results: Across PROMs, improvements from baseline to 3-months follow-up were associated with reductions in subsequent healthcare use. For example, one standard deviation improvement in back pain, disability, and self-efficacy were associated with 6– 8% reductions in visits (adjusted IRRs [95% CI], back pain: 0.92 [0.88, 0.97]; disability: 0.94 [0.90, 0.99]; self-efficacy: 0.92 [0.87, 0.96]). For analgesic use, improvements in back pain and self-efficacy were related to a 4% reduction (adjusted IRR [95% CI], back pain: 0.96 [0.92, 1.01], self-efficacy 0.96 [0.91, 1.00]). Stronger associations were observed in subgroups with medium visit use and medium or low analgesic use at baseline.
Conclusion: On a group-level, improvements across PROMs were associated with reductions in subsequent healthcare use following participation in a self-management supportive intervention. The strength of the associations varied across subgroups and additional factors not measured by the PROMs are likely to also influence changes in healthcare use.
Keywords: low back pain, healthcare utilization, self-management
Introduction
Low back pain (LBP) is a prevalent condition affecting approximately 619 million people worldwide, with numbers expected to increase due to increased aging of the population.1 Globally, it is the leading cause of years lived disability and it is associated with high healthcare use (HCU), contributing to the burden of LBP on society.1–4
For most individuals with LBP, no specific structure can be identified as the nociceptive driver for the pain, this is often referred to as non-specific LBP.5 Many individuals experience recurrent episodes, and LBP is often viewed as a long-lasting condition with a fluctuating course rather than a series of isolated, unrelated occurrences.6,7 To embrace this complexity, LBP is best understood within a biopsychosocial framework, which acknowledges that multiple interacting factors contributes to the pain experience.8 Moreover, there is currently no curative treatment for LBP, and as a result, many individuals continue to seek care over time. Proposed actions to improve care for LBP include teaching individuals to self-manage their condition.9 This approach is endorsed by the World Health Organization (WHO) in its guideline for non-surgical management of chronic LBP, which recommends education that guides self-management.10
In this context, teaching individuals to self-manage means to empower people by equipping them with the knowledge, skills, and confidence to manage their condition independently, potentially reducing reliance on healthcare providers.11 While this does not preclude the use of healthcare, it is plausible that such support could lead to a change in healthcare-seeking behavior reducing future HCU, thereby alleviating pressure on healthcare systems.
It has been suggested that the decision to seek healthcare is influenced by an interplay between three domains: 1) predisposing characteristics (eg, demographics, social structures, and health beliefs), 2) enabling factors (eg, access to healthcare), and 3) a perceived need for care.12,13 Especially perceived needs, expressed as high pain intensity, disability, or concerns about worsening of symptoms, are linked to high HCU for people with LBP.14–17
The influence of self-management supportive interventions on HCU may be mediated through clinical outcomes (eg, disability and self-efficacy) that shape the perceived need for care. Self-management supportive interventions have demonstrated small but positive effects on clinical outcomes such as pain intensity, disability, and self-efficacy.18–20 However, for HCU the evidence is inconclusive.21 Yet, no previous studies have examined whether changes in these outcomes are associated with subsequent changes in HCU. Understanding this relationship is crucial for identifying modifiable drivers of HCU and optimizing self-management supportive interventions.
The aim of this study was to investigate the potential impact of changes in clinical outcomes on future HCU following a self-management supportive program for LBP. We hypothesized that improvements in patient-reported outcome measures (PROMs) were associated with reductions in HCU. Specifically, the study objectives were to 1) investigate the association between changes in PROMs and changes in a) primary care visits to physiotherapists and chiropractors, and b) redeemed prescriptions of analgesics from before to after participation in a self-management supportive program for individuals with LBP, and 2) to examine whether these associations differ between subgroups of participants with a low, medium, or high use of primary care visits and analgesics prior to the program, respectively.
Methods
This observational cohort study was based on data from the clinical registry “GLA:D® Back” linked with Danish national registry-data using the civil registration number. The study has been reported according to Strengthening the Reporting of Observational studies in Epidemiology (STROBE) guidelines.22
Participants and Setting
Participants included in the study were individuals above 18 years with non-specific LBP who enrolled in GLA:D Back between March 1st, 2018, and August 31st, 2022. They had to live in Denmark for at least 1 year before and 16 months after their enrollment in GLA:D Back for HCU data to be available.
The GLA:D Back Program
A detailed description of the GLA:D Back program, including development, content, theoretical framework, and implementation is provided elsewhere.23–25 In short, GLA:D Back is a structured 10-week self-management supportive program based on a cognitive behavioral approach. It consists of two individual session, two group sessions of education, and two weekly sessions of supervised exercise over eight weeks Throughout the program, participants work with individual goals for re-engagement in activity. The education focuses on key messages such as “the back is made for movement” and “pain does not equal harm”, aiming for participants to engage with activity and understand pain as less threatening. Themes of the education are discussed at the exercise sessions based on the participants’ experiences. The clinician facilitates discussions and guide participants in problem-solving during exercises to foster self-efficacy and sense of safety with movement. The program is underpinned by a theoretical model suggesting that acquiring new knowledge and skills can lead to changes in beliefs and behaviors. These changes are proposed to reduce pain interference and enhance self-efficacy, quality of life, and daily functioning.
There are no strict inclusion criteria, but the target group is individuals with persistent or recurrent non-specific LBP. It is delivered in primary care by chiropractors and physiotherapists nationwide in Denmark and participants pay around 400 Euros for the program, unless it is offered from a municipality rehabilitation center where there is no fee. Upon enrollment participants are registered in the GLA:D Back registry via REDCap, provided and supported by the Odense Patient data Explorative Network (OPEN). Data is collected using questionnaires at baseline, and after 3- (approximately end of treatment), 6- and 12 months. For this study, we used data collected at baseline and at the 3-months follow-up.
Variables
Predictors: PROMs
The following PROMs were used: Pain intensity (numerical rating scale, range 0–10, higher scores indicating higher pain intensity),26 disability (Oswestry Disability Index [ODI], range 0–100, higher scores indicating higher levels of disability),27,28 illness perceptions (Brief Illness Perception Questionnaire [IPQ], range 1–80, higher scores indicating worse perceptions, eg more worries),29,30 self-efficacy (The Arthritis Pain Self-Efficacy Scale [ASES], pain subscale, range 1–10, higher scores indicating higher self-efficacy),31 health-related quality of life (EQ-5D®, range 0–100, higher scores indicating higher health-related quality of life). PROMs were chosen based on the proposed determinants of change in the GLA:D Back program23,24 to cover domains of symptoms, knowledge and beliefs about LBP, ability to manage pain, and quality of life.
Outcomes: HCU
Number of visits to primary care was defined as the total number of all-cause consultations with a physiotherapist or chiropractor in a 12-month period before and after the intervention. The before period (baseline) refers to the total use in the 12 months preceding the date of enrollment in the intervention (index date). The after period included total use 4 to 16 months after enrollment, to ensure most participants had completed the program. Only one visit per provider type per day was counted. Data on visits were obtained from the Danish National Health Insurance Registry, which contains information on all services provided by physiotherapists and chiropractors reimbursed by the national health insurance.32
Analgesics use was defined as the total sum of defined daily doses (DDD) of prescriptions for paracetamol, non-steroidal anti-inflammatory drugs (NSAIDs), and opioids redeemed 12 months before and 12 months after the program, respectively. Data was obtained from the Danish National Prescription Registry, which contains information on all drug prescriptions redeemed at pharmacies in Denmark.33,34 A complete list of Anatomical Therapeutic Chemical Classification (ATC) codes can be found in Supplementary Table S1.
Additional variables
Additional baseline variables obtained from GLA:D Back included age, sex, body mass index (BMI, weight divided by squared height), and duration of the current LBP episode (less than a year, more than a year). From national registries, we obtained information on other chronic conditions (asthma, dementia, chronic obstructive lung disease, rheumatoid arthritis, osteoporosis, schizophrenia, diabetes type 1 or 2), level of education (primary school/high school, skilled worker/short-term education, long/medium term higher education),35 job situation (affiliated to the labor market, student, retired, unemployed, welfare payment, or other),36 and whether a participant had received a hospital diagnosis for LBP or MRI scan for LBP in the year before enrollment or the intervention had ended.37 All administrative data were obtained from January 2016 to December 2023.
Statistical Analysis
The characteristics of the study population were described with percentages, means with SDs, or medians with 25th and 75th percentiles. Multiple imputations were performed to account for missing data in PROMs. The imputations were based on predictive mean matching for numerical variables and logistic regression for binary variables and included: PROMs, HCU outcomes, additional variables, and baseline measurements of fear avoidance beliefs, Start Back Screening Tool and quality of life short form (SF-36).
Associations between changes in PROMs and HCU were investigated in longitudinal regression models with two time points. To account for excess zeroes and overdispersion of data, a zero-inflated negative binomial regression (ZINB) model was chosen. The ZINB model is a two-part model, in which the first part estimates the odds of being a structural non-user, while the other part estimates the incidence rate ratio (IRR) for HCU across the full sample.38 Given the study objectives, the interpretation was only based on the count component (IRR). In the models for visits, random intercepts were included for each unique ID and clinic, but removed in models for analgesic use as they did not improve model fit.
The modelling was conducted in three steps, separately for each PROM. First, crude models with an interaction between each PROM and time were fitted (model 1). Second, for each PROM, adjusted models were fitted that included age, sex, level of education, duration of pain, baseline HCU (visits or analgesics), and year of enrollment in addition to the PROM-time-interaction (model 2). Lastly, fully adjusted models were fitted, in which all PROMS were added to model 2 (model 3). PROMs’ scales were standardized to ensure comparability and inversed where needed to ease interpretation (higher scores reflect improvement for all PROMs). For each model, the estimate of interest was the interaction between a given PROM and time, reflecting the association between changes in HCU and PROM from baseline to follow-up.
All analyses were performed in the total sample and in subgroups of high, medium, and low users, based on tertiles of baseline use of visits and DDD, respectively. For analgesics use, subgroups were created based on a sample without “non-users” (no use at baseline and follow-up). The model estimates for the PROM-time-interaction were presented as IRR with 95% confidence intervals (CIs) and p-values.
All analyses were performed using R version 4.3.2,39 utilizing the mice40 and glmmTMB41 packages.
User Involvement
Previous participants from the GLA:D Back were invited as patient representatives to help interpret the results. In a 1-hour online group meeting, three participants provided their perspectives on 1) factors influencing healthcare seeking, 2) interpretation of findings, 3) limitations in the chosen predictors and outcomes.
Results
Study Sample
In total, 2803 participants were included in the analysis (Figure 1). Overall, 68% were female, mean age was 58 years, and 59% reported their LBP to have lasted for more than one year (Table 1). On a group level, all PROMs improved, although the mean change was close to zero in self-efficacy (Table 2). On average, the number of visits was reduced by 3 (SD 14) from baseline to follow-up. Analgesic use showed a mean reduction of 20 DDD (SD 133). HCU before and after the intervention is described in Table 3. Participants lost to follow-up were generally similar to the included participants but had slightly worse scores on all PROMs at baseline (Supplementary Table S2).
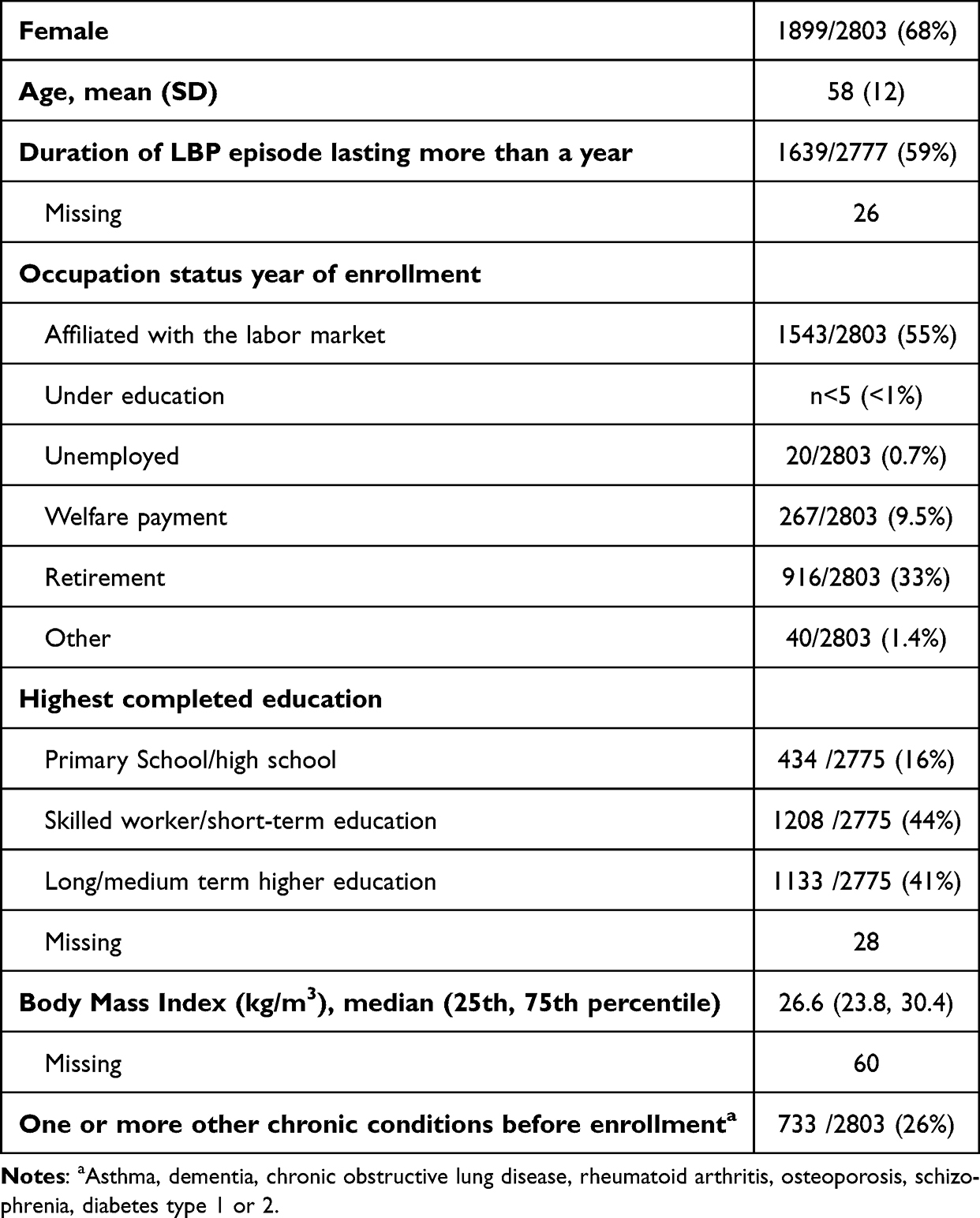 |
Table 1 Characteristics of the Study Sample N = 2803 |
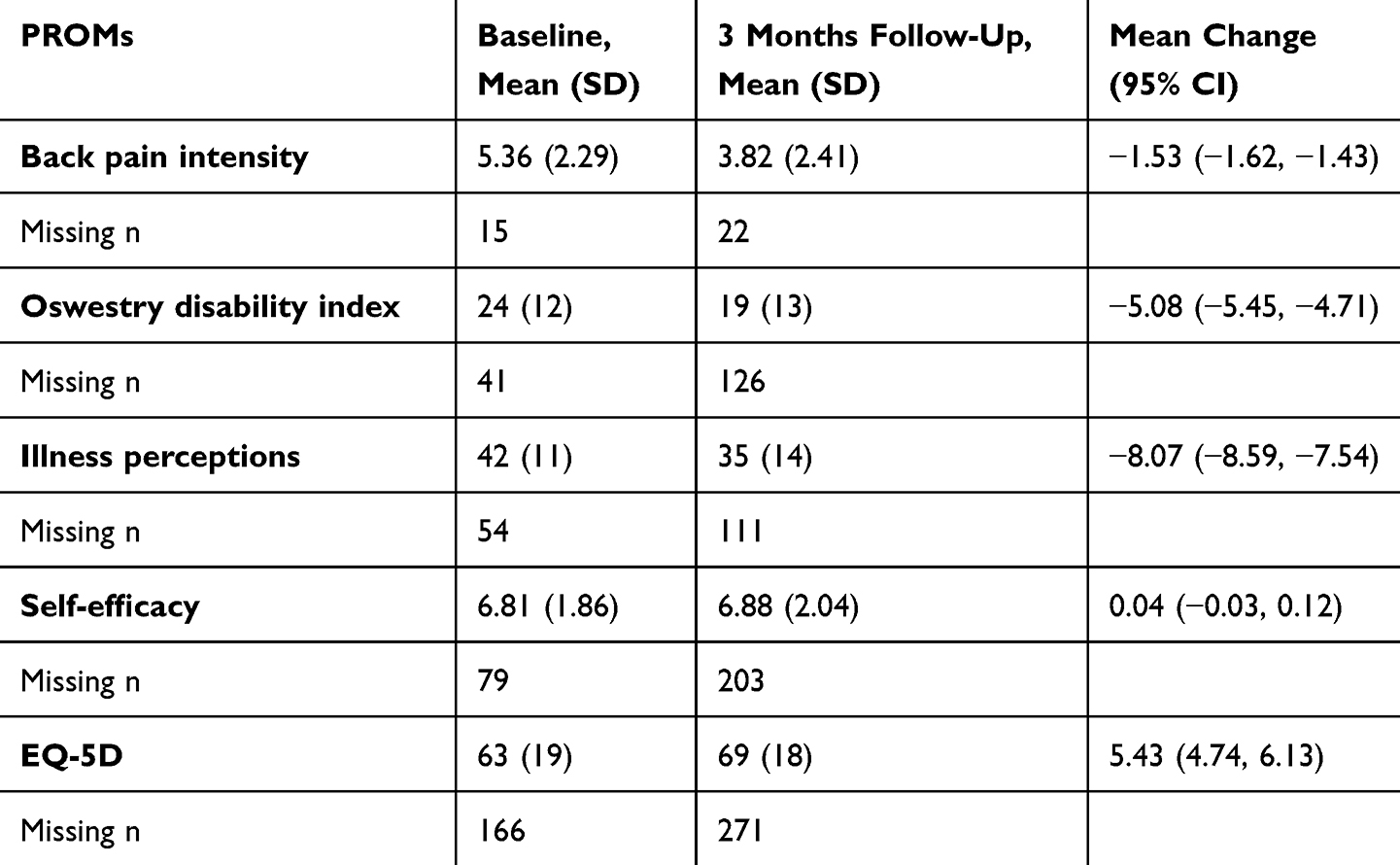 |
Table 2 Patient Reported Outcome Measures (PROMs) at Baseline and Follow-Up. N = 2803 |
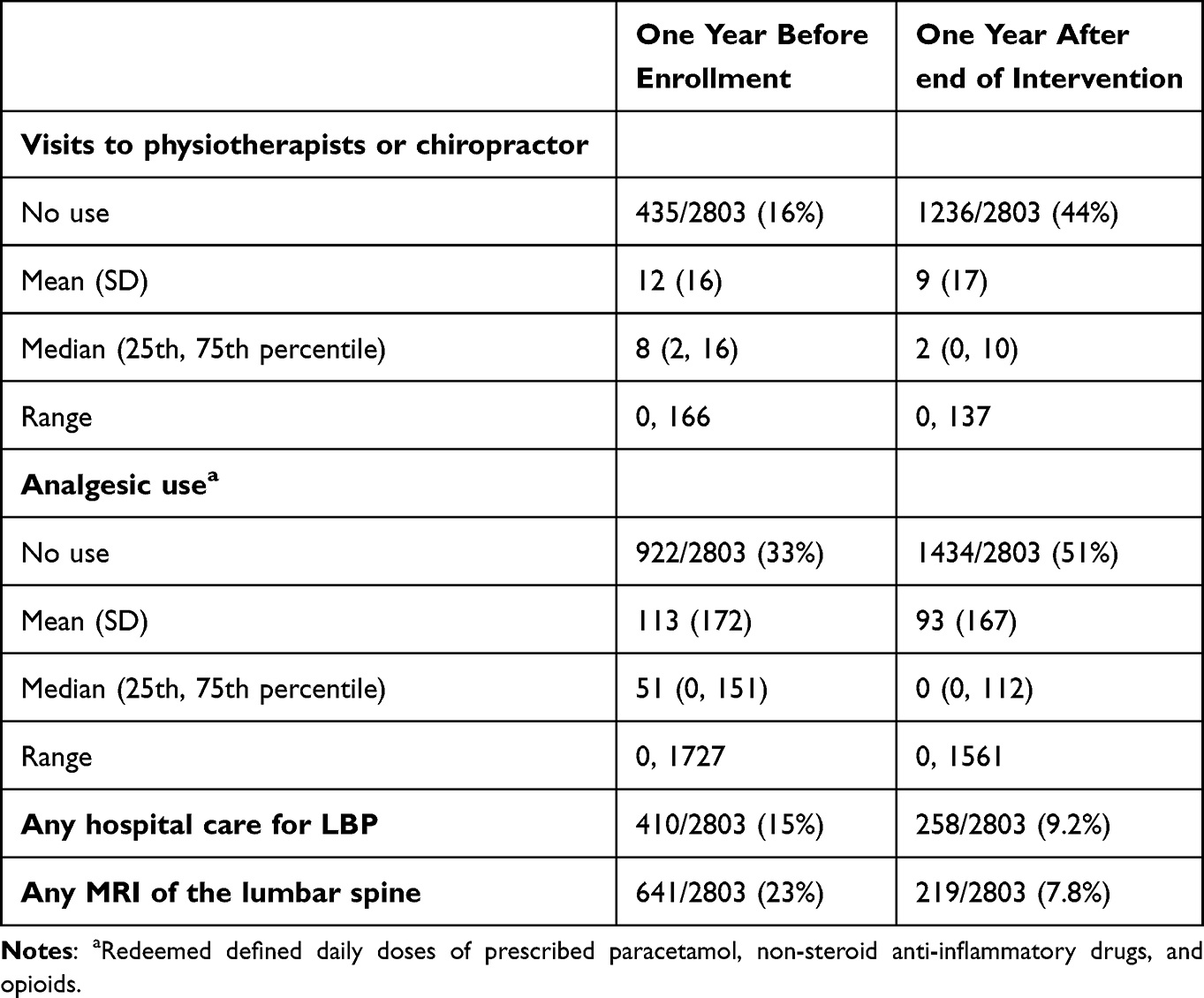 |
Table 3 Healthcare Use Before and After the Intervention |
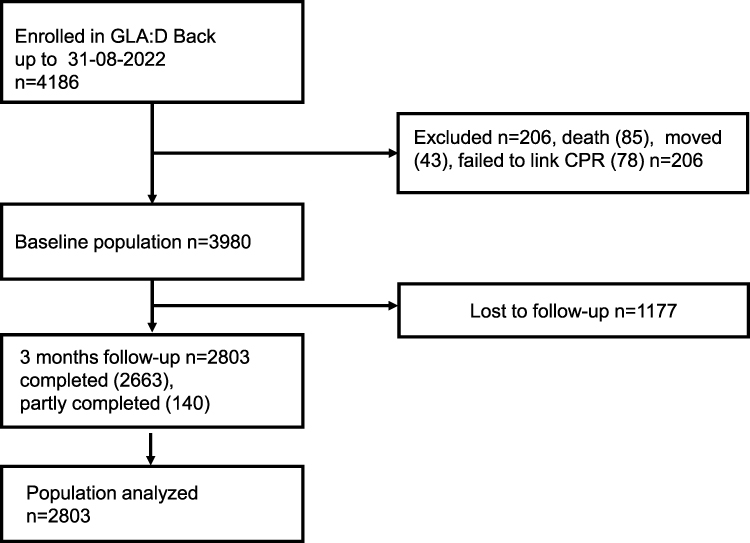 |
Figure 1 Flow chart for included participants. Follow-up refers to surveys collecting the patient-reported outcomes measures used as predictors. |
Association Between Changes in PROMs and Visits
Across PROMS, the three models yielded similar results, except for self-efficacy in model 1 which had an IRR closer to 1 than models 2 and 3 (Supplementary Table S3 and Figure S1). All results reported from hereon are therefore based on the fully adjusted model 3. Improvements in all PROMs from baseline to follow-up were associated with a reduction in number of visits, although CIs for illness perceptions and EQ-5D included 1 (Figure 2 and Table 4). The strongest associations were observed for back pain intensity and self-efficacy reflecting an 8% reduction in visits at follow-up per SD improvement (back pain intensity, IRR: 0.92, 95% CI: 0.88, 0.97; self-efficacy, IRR: 0.92, 95% CI: 0.87, 0.96), followed by a 6% reduction for ODI (IRR: 0.94, 95%: CI 0.90, 0.99). This corresponds to a reduction of 1 visit for a 2.3-point improvement in back pain (on a 0–10 scale) from baseline to follow-up.
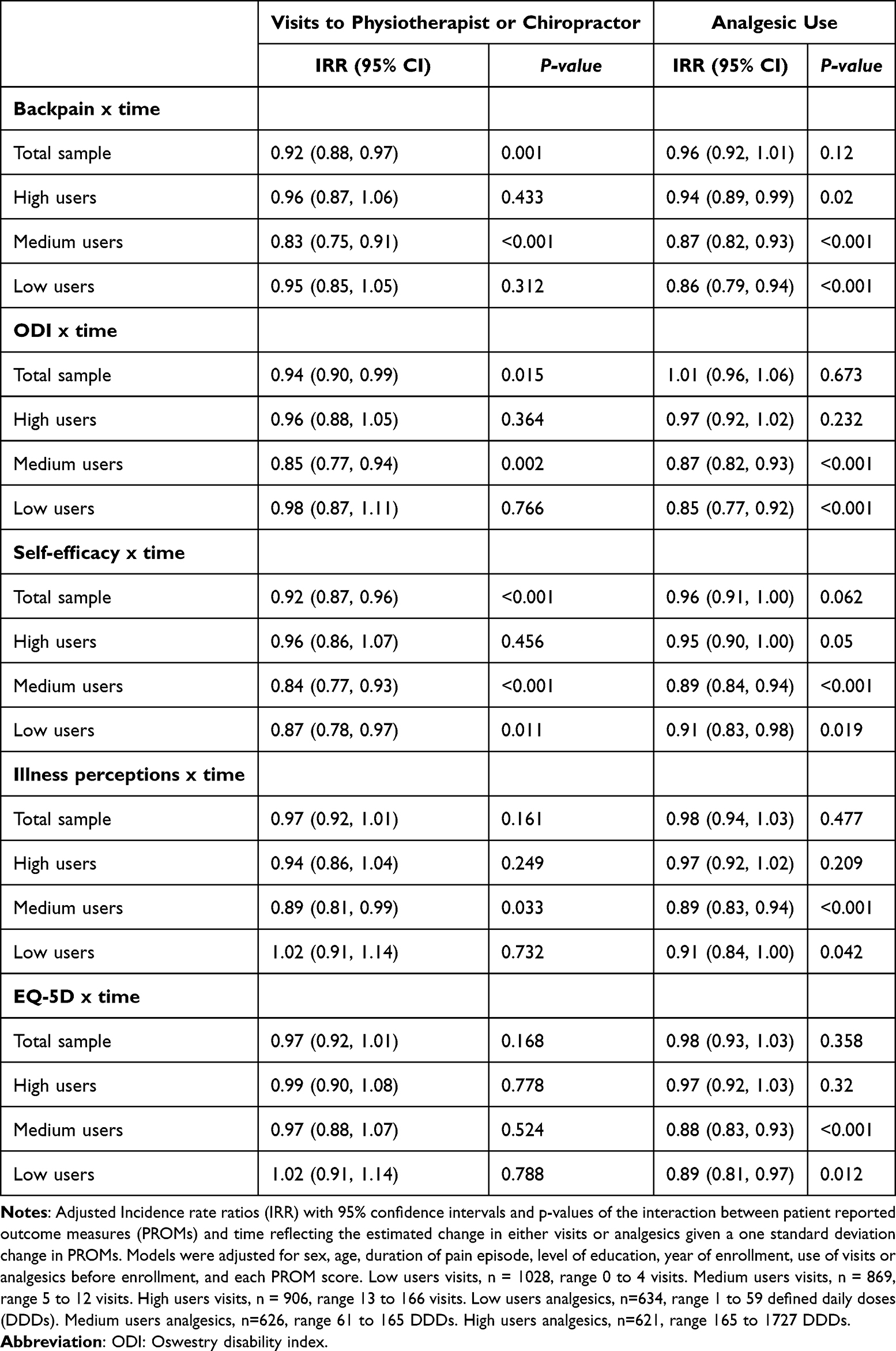 |
Table 4 Associations Between Changes in PROMs and Visits or Analgesic Use at Follow-up |
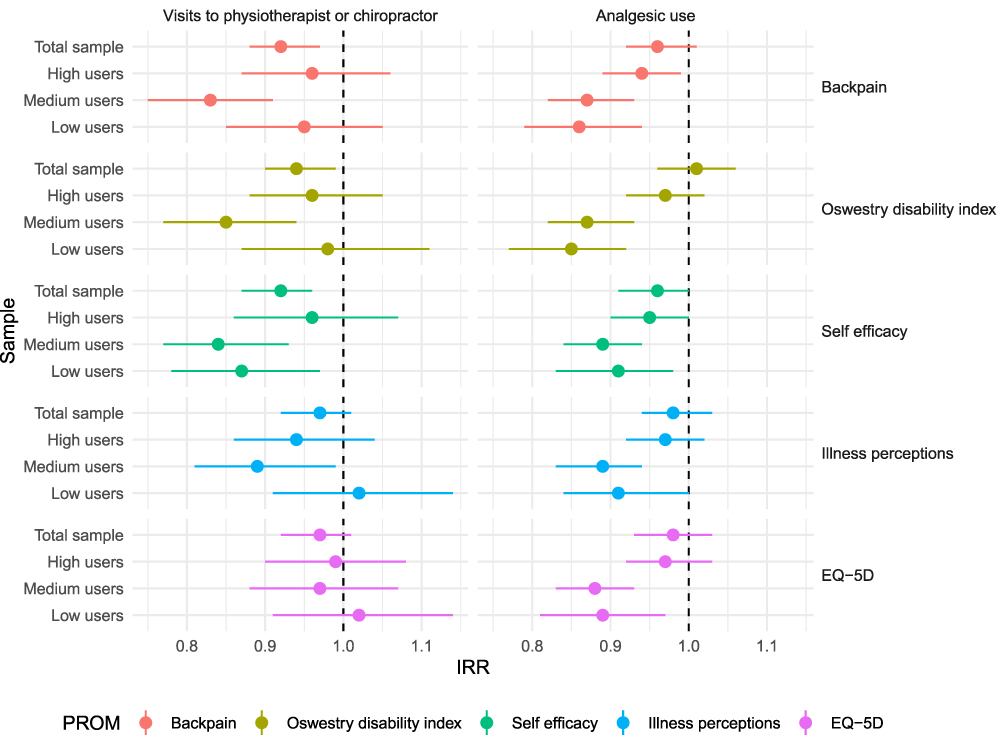 |
Figure 2 Adjusted incidence rate ratios (IRR) with 95% confidence intervals of the interaction between patient reported outcome measures (PROMs) and time, reflecting the estimated change in either visits or analgesics given a one standard deviation change in PROMs. Models were adjusted for sex, age, duration of pain episode, level of education, year of enrollment, use of visits or analgesics before enrollment, and each PROM score. |
Association Between Changes in PROMs and Analgesic Use
In the fully adjusted model 3, IRRs for all PROMs except for ODI indicated that improvements were related to reductions in analgesic use, but associations were uncertain with 95% CIs including 1 (Figure 2 and Table 4). For example, one SD improvement in back pain intensity was related to a 4% reduction in analgesic use (IRR: 0.96, 95% CI: 0.92, 1.01). Model 2 yielded similar results, while more uncertainty was observed for the crude model 1 (Supplementary Table S3 and Figure S2).
Subgroup Analyses
Overall, subgroups had similar baseline characteristics except for high users of analgesics that were older, had lower socioeconomic status, more chronic conditions, and worse PROMs at baseline (Supplemental Tables S4 and S5). Changes in PROMs from baseline to follow-up were similar across subgroups.
Associations between changes in PROMs and changes in HCU followed the same direction as in the total sample (Figure 2 and Table 4). For visits, the associations were stronger for medium users than for the other subgroups (Figure 2). For example, there was a reduction in visits by 17% per SD improvement in back pain intensity among the medium users (IRR: 0.83, 95% CI: 0.75, 0.91). For analgesic use, the strongest associations were observed for low and medium users with estimates for high users being similar to the total sample. For example, high users reduced analgesic use by 6% (IRR: 0.94, 95% CI: 0.89, 0.99) per SD improvement in back pain, while the reduction was 13% for medium users (IRR: 0.87, 95% CI: 0.82, 0.93). Although the relative changes (IRRs) were smaller for high users, the absolute changes were comparable to medium users. For example, a one SD improvement in back pain corresponded to a reduction of 14 DDD for medium users and 22 DDD for high users.
Discussion
This is the first study to examine the association between improvements in PROMs following a self-management supportive intervention for LBP and subsequent HCU. Improvements in pain intensity, disability, illness perceptions, self-efficacy, and quality of life were observed to be associated with reductions in both the number of visits and analgesic use. However, the estimated reductions in HCU given improvements in PROMs were small and the certainty varied across the PROMs. This suggests that other factors such as predisposing characteristics or enabling factors also influence HCU, in line with the Behavioral Model of Health Services Use.12,13 Associations were most consistent and pronounced for reductions in visits following improvement in back pain intensity, disability, and self-efficacy implying that, on a group level, improvements in LBP clinical outcomes lead to reduced HCU.
Despite the intention of the intervention to improve self-efficacy, average self-efficacy scores changed little over time. However, our findings suggested that when self-efficacy increases, it is likely to influence healthcare seeking behavior leading to a reduction in HCU to the same extent as reductions in pain intensity. Furthermore, self-efficacy has been found to be an important mediator for reducing pain and disability.42 This highlights the relevance of targeting self-efficacy in interventions for LBP.
A key message in GLA:D Back is that hurt does not equal harm, and that multiple factors influence pain. Changes in the understanding of pain could potentially lead to reduced HCU, by reducing individuals’ search for a specific structural explanation for their pain or which is a recurring theme for individuals with high HCU due to pain.43 Thus, it was somewhat surprising that the associations for illness perceptions were more uncertain. This may be due to the intervention not successfully altering participants’ perceptions or that the brief IPQ does not quantify perceived causes of LBP and thus may not fully have captured changes in the understanding of pain.44,45
For EQ-5D, the uncertain associations, especially with reduction in visits, may be explained by the fact that EQ-5D measures an individual’s general health-related quality of life. Multiple factors not related to the individual’s LBP condition can hence affect this measure. While poorer general health may increase the perceived need for medical treatment overall, it may not directly reflect a need for consulting a chiropractor or physiotherapist.
In the subgroup analyses, larger and more consistent associations were observed among participants with a medium use of visits prior to enrolment in the intervention, and among those with low or medium analgesic use. The variation in the magnitude of the strength of the association across subgroups indicates that factors related to initial healthcare-seeking behavior may have a strong interplay with perceived needs for healthcare. Thus, improvements in PROMs like symptom severity is not enough to explain why individuals use healthcare or not.
Estimates for the total sample were close to those of the high users, which indicates that these were mainly influenced by high users. This is likely a result of high users having a low probability of being a structural zero (ie, related to weights used in the ZINB model). High users, particularly of analgesics, differed on several baseline characteristics from those using less analgesics, and may represent a more complex population requiring tailored deprescribing interventions. For high users of visits, regular HCU may serve as preventive, social, or habitual functions, making it less sensitive to symptom improvements. While the relative changes per SD improvement in PROMs were smaller in the high use groups, the absolute reductions were similar or greater due to the higher use at baseline.
Strengths and Limitations
The combination of high quality HCU data from national registries (highly accurate and not prone to recall bias) and PROMs from a large primary care clinical registry is unique and not generally available when conducting registry based research.32,33
In Denmark, general practitioners (GPs), physiotherapists, and chiropractors are the primary care providers of care for LBP.4 Thus, not including visits to GPs in the study does not yield the complete picture of primary care visits. The reason we did not include GP visits was a concern that many of the consultations would not be LBP-related, since there are no diagnostic codes linked to visits in primary care in the national registries. Also, the lack of diagnostic codes may have overestimated the number of visits to physiotherapists and chiropractors, if participants stopped seeking care for LBP but still used this type of healthcare for other conditions.
Another limitation of the study was that over-the-counter medication and visits not reimbursed by the national health insurance are not part of national registries and hence not included in this study. This means that HCU was likely underestimated. When individuals transition between registered and unregistered healthcare services, the association with changes in clinical outcomes can become distorted, especially if such shifts are related to PROMs. Additionally, as confirmed by the patient representatives, individuals with LBP use many different healthcare related services like massage therapy or other non-reimbursed services (eg, yoga or home exercises). While changes in such services or management strategies would be relevant to include, no registry data was available to account for this.
Also, unmeasured confounding should be kept in mind when interpreting the results. We had a specific focus on need factors depicted by the PROMs, as these were the ones hypothesized to change through the intervention. Thus, we did not consider all relevant enabling factors or predisposing factors that are likely to also affect changes in HCU. Especially given the long follow-up, changes in general health, socioeconomic status, and other domains will inevitably have happened for some participants.
The PROMs chosen for the analysis resonated well with the patient representatives, who emphasized the importance of including the domains related to thoughts and perceptions in addition to pain and disability. However, measures reflecting coping strategies and the acceptance of pain, may be additional factors affected by a self-management supportive intervention that could influence future HCU.
The study sample likely underrepresents individuals with low socioeconomic status based on the out-of-pocket expense to enter the program and the low proportion of individuals with only a primary school/ high school education. Additionally, the study sample represents a clinical population of individuals with mostly minimal to moderate disability who are motivated to engage in a structured group-based intervention. Therefore, findings may not be generalized to individuals with more severe or medically complex presentations of LBP. The context of the Danish healthcare system, where there is relatively easy access to primary care physiotherapy and chiropractic services, may also limit generalizability to other healthcare systems.
Conclusion
Among individuals with LBP participating in a self-management supportive intervention, improvements across PROMs were associated with reduced use of physiotherapy, chiropractic care, and analgesics in the following year. Most prominent associations were observed for improvements in pain intensity, disability and self-efficacy, which highlight the importance of addressing multiple aspects of pain when aiming to reduce HCU. Large variation in the strength of associations between PROMs and HCU across subgroups suggests that factors beyond those captured by PROMs likely contribute to variation in HCU. The interplay between factors such as socioeconomics, access to healthcare and cultural influences therefore warrants further investigation.
Use of Generative Artificial Intelligence
During the preparation of this work the authors used Microsoft Copilot in order to improve readability, language, and grammar of some of the text in the submitted manuscript, as well as help with syntax for some of the coding of statistical analysis. After using these tools, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Data Sharing Statement
The data from the GLA:D Back cohort can be accessed on reasonable request by contacting Alice Kongsted, [email protected], leader of the GLA:D Back research program.
The data from the national registries used in this study is based on micro-data that are analyzed at a server on Statistics Denmark. Data cannot be shared outside the server but are available for Danish Research Institutions following applicable regulations for application to Statistics Denmark.
Ethics
This study complies with the Declaration of Helsinki. The data collection for GLA:D Back has obtained authorization from the Danish Data Protection Agency (DPA) as part of the University of Southern Denmark’s institutional authorization (DPA no. 2015–57-0008 SDU no. 17/30591). The Regional Committees on Health Research Ethics for Southern Denmark decided that the study did not need ethical approval (file number S-20172000-93). When registered by the clinician, the patient receives an Email with link to a patient reported survey. Written information about the study, data protection and participants’ rights are in the survey with a request to confirm consent for using data for research purposes. A yearly safety report is conducted which evaluates outcomes and patient reported side effects. The Report is overviewed by an external safety board.
Acknowledgments
We would like to acknowledge the Odense Patient data Explorative Network (OPEN) for their support in collecting data for the GLA:D Back Registry, RYGDATA:SDU for providing secure registry data access, and patient representatives for contributing with their perspectives on the results.
Funding
Søren Grøn’s position is funded by a stipend from the University of Southern Denmark, and grants from The Danish Rheumatism Association (R202-A7472.) and the Danish Foundation for Chiropractic Research and Post Graduate Education (R185-A4190).
Disclosure
This manuscript is based on work that is part of the PhD thesis by Søren Grøn titled Self-management and healthcare use for people with low back pain. The full thesis is available at: https://portal.findresearcher.sdu.dk/da/publications/self-management-and-healthcare-use-for-people-with-low-back-pain. Alice Kongsted is a co-developer of GLA:D Back and part of the clinician training team. All other authors declare no conflict of interest. GLA:D is a non-profit initiative hosted at the University of Southern Denmark and the GLA:D® trademark is property of the University of Southern Denmark. The researchers do not have any personal financial benefits from working with the project. The authors report no conflicts of interest in this work.
References
1. NCBI. Global, regional, and national burden of low back pain, 1990–2020, its attributable risk factors, and projections to 2050: a systematic analysis of the Global Burden of Disease Study 2021 - PMC. Available from: https://www-ncbi-nlm-nih-gov.proxy1-bib.sdu.dk/pmc/articles/PMC10234592/.
2. Fatoye F, Gebrye T, Ryan CG, Useh U, Mbada C. Global and regional estimates of clinical and economic burden of low back pain in high-income countries: a systematic review and meta-analysis. Front Public Health. 2023;11:1098100. doi:10.3389/fpubh.2023.1098100
3. Fatoye F, Gebrye T, Mbada CE, Useh U. Clinical and economic burden of low back pain in low- and middle-income countries: a systematic review. BMJ Open. 2023;13(4):e064119. doi:10.1136/bmjopen-2022-064119
4. Sundhedsstyrelsen. Resultater Fra Rapporterne Sygdomsbyrden i Danmark 2022 - Sygdomme Og Risikofaktorer. 2022.
5. Maher C, Underwood M, Buchbinder R. Non-specific low back pain. The Lancet. 2017;389(10070):736–747. doi:10.1016/S0140-6736(16)30970-9
6. Dunn KM, Hestbaek L, Cassidy JD. Low back pain across the life course. Best Pract Res Clin Rheumatol. 2013;27(5):591–600. doi:10.1016/j.berh.2013.09.007
7. Kongsted A, Kent P, Axen I, Downie AS, Dunn KM. What have we learned from ten years of trajectory research in low back pain? BMC Musculoskelet Disord. 2016;17:220. doi:10.1186/s12891-016-1071-2
8. Hartvigsen J, Hancock MJ, Kongsted A, et al. What low back pain is and why we need to pay attention. The Lancet. 2018;391(10137):2356–2367. doi:10.1016/S0140-6736(18)30480-X
9. Buchbinder R, Underwood M, Hartvigsen J, Maher CG. The Lancet Series call to action to reduce low value care for low back pain: an update. Pain. 2020;161(1):S57–S64. doi:10.1097/j.pain.0000000000001869
10. WHO. WHO Guideline for Non-Surgical Management of Chronic Primary Low Back Pain in Adults in Primary and Community Care Settings. World Health Organization. 2023.
11. Jonkman NH, Schuurmans MJ, Jaarsma T, Shortridge-Baggett LM, Hoes AW, Trappenburg JCA. Self-management interventions: proposal and validation of a new operational definition. J Clin Epidemiol. 2016;80:34–42. doi:10.1016/j.jclinepi.2016.08.001
12. Andersen RM. Revisiting the Behavioral Model and Access to Medical Care: does it Matter? J Health Soc Behav. 1995;36(1):1–10. doi:10.2307/2137284
13. Andersen R. A Behavioral Model of Families’ Use of Health Services. Center for Health Administration Studies, University of Chicago; 1974.
14. Talty FT, Roberts ME, Dang C, Clewley DJ, Horn ME. Using a behavioral model to identify factors associated with choice of provider for neck and low back pain: a systematic review. Musculoskelet Sci Pract. 2020;49:102223. doi:10.1016/j.msksp.2020.102223
15. Ferreira ML, Machado G, Latimer J, Maher C, Ferreira PH, Smeets RJ. Factors defining care-seeking in low back pain--a meta-analysis of population based surveys. Eur J Pain Lond Engl. 2010;14(7):
16. Esteve R, López-Martínez AE, Ruíz-Párraga GT, Serrano-Ibáñez ER, Ramírez-Maestre C. Pain Acceptance and Pain-Related Disability Predict Healthcare Utilization and Medication Intake in Patients with Non-Specific Chronic Spinal Pain. Int J Environ Res Public Health. 2020;17(15):5556. doi:10.3390/ijerph17155556
17. Huysmans E, Leemans L, Beckwée D, et al. The Relationship between Cognitive and Emotional Factors and Healthcare and Medication Use in People Experiencing Pain: a Systematic Review. J Clin Med. 2020;9(8):2486. doi:10.3390/jcm9082486
18. Scholz C, Schmigalle P, Plessen CY, et al. The effect of self-management techniques on relevant outcomes in chronic low back pain: a systematic review and meta-analysis. Eur J Pain. 2024;28:532–550. doi:10.1002/ejp.2221
19. Elbers S, Wittink H, Pool JJM, Smeets RJEM. The effectiveness of generic self-management interventions for patients with chronic musculoskeletal pain on physical function, self-efficacy, pain intensity and physical activity: a systematic review and meta-analysis. Eur J Pain Lond Engl. 2018;22(9):1577–1596. doi:10.1002/ejp.1253
20. Oliveira VC, Ferreira PH, Maher CG, Pinto RZ, Refshauge KM, Ferreira ML. Effectiveness of self-management of low back pain: systematic review with meta-analysis. Arthritis Care Res. 2012;64(11):1739–1748. doi:10.1002/acr.21737
21. Grøn S, Johansson M, Schiphof D, Koes B, Kongsted A. Do self-management supportive interventions reduce healthcare utilization for people with musculoskeletal pain conditions? - A systematic review. Public Health. 2024;238:152–161. doi:10.1016/j.puhe.2024.10.021
22. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34. doi:10.4103/sja.SJA_543_18
23. Kjaer P. GLA: D® Back Group-Based Patient Education Integrated with Exercises to Support Self-Management of Back Pain - Development, Theories and Scientific Evidence. 2018.
24. Kongsted A, Ris I, Kjaer P, Vach W, Morsø L, Hartvigsen J. GLA:D® Back: implementation of group-based patient education integrated with exercises to support self-management of back pain - protocol for a hybrid effectiveness-implementation study. BMC Musculoskelet Disord. 2019;20(1):85. doi:10.1186/s12891-019-2443-1
25. Kongsted A, Hartvigsen J, Boyle E, et al. GLA:D® Back: group-based patient education integrated with exercises to support self-management of persistent back pain — feasibility of implementing standardised care by a course for clinicians. Pilot Feasibility Stud. 2019;5(1):65. doi:10.1186/s40814-019-0448-z
26. Strong J, Ashton R, Chant D. Pain intensity measurement in chronic low back pain. Clin J Pain. 1991;7(3):209–218. doi:10.1097/00002508-199109000-00007
27. Lauridsen HH, Hartvigsen J, Manniche C, Korsholm L, Grunnet-Nilsson N. Danish version of the Oswestry Disability Index for patients with low back pain. Part 1: cross-cultural adaptation, reliability and validity in two different populations. Eur Spine J. 2006;15(11):1705–1716. doi:10.1007/s00586-006-0117-9
28. Lauridsen HH, Hartvigsen J, Manniche C, Korsholm L, Grunnet-Nilsson N. Danish version of the Oswestry disability index for patients with low back pain. Part 2: sensitivity, specificity and clinically significant improvement in two low back pain populations. Eur Spine J. 2006;15(11):1717–1728. doi:10.1007/s00586-006-0128-6
29. Leysen M, Nijs J, Meeus M, et al. Clinimetric properties of illness perception questionnaire revised (IPQ-R) and brief illness perception questionnaire (Brief IPQ) in patients with musculoskeletal disorders: a systematic review. Man Ther. 2015;20(1):10–17. doi:10.1016/j.math.2014.05.001
30. Broadbent E, Wilkes C, Koschwanez H, Weinman J, Norton S, Petrie KJ. A systematic review and meta-analysis of the Brief Illness Perception Questionnaire. Psychol Health. 2015;30(11):1361–1385. doi:10.1080/08870446.2015.1070851
31. Primdahl J, Wagner L, Hørslev-Petersen K. Self-efficacy in rheumatoid arthritis: translation and test of validity, reliability and sensitivity of the Danish version of the Rheumatoid Arthritis Self-Efficacy Questionnaire (RASE). Musculoskeletal Care. 2010;8(3):123–135. doi:10.1002/msc.172
32. Andersen JS, Olivarius NDF, Krasnik A. The Danish National Health Service Register. Scand J Public Health. 2011;39(7 Suppl):34–37. doi:10.1177/1403494810394718
33. Kildemoes HW, Sørensen HT, Hallas J. The Danish National Prescription Registry. Scand J Public Health. 2011;39(7 Suppl):38–41. doi:10.1177/1403494810394717
34. Pottegård A, Schmidt SAJ, Wallach-Kildemoes H, Sørensen HT, Hallas J, Schmidt M. Data Resource Profile: the Danish National Prescription Registry. Int J Epidemiol. 2017;46(3):798–798f. doi:10.1093/ije/dyw213
35. Jensen VM, Rasmussen AW. Danish Education Registers. Scand J Public Health. 2011;39(7 Suppl):91–94. doi:10.1177/1403494810394715
36. Baadsgaard M, Quitzau J. Danish registers on personal income and transfer payments. Scand J Public Health. 2011;39(7 Suppl):103–105. doi:10.1177/1403494811405098
37. Lynge E, Sandegaard JL, Rebolj M. The Danish National Patient Register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
38. Greene WH. Accounting for Excess Zeros and Sample Selection in Poisson and Negative Binomial Regression Models. Available from: https://papers.ssrn.com/abstract=1293115.
39. R Core Team. R: A Language and Environment for Statistical Computing. Vienna, Austria: R Foundation for Statistical Computing. 2025. Available from: https://www.R-project.org/.
40. van Buuren S. Groothuis-Oudshoorn K. mice: multivariate Imputation by Chained Equations in R. J Stat Softw. 2011;45:1–67. doi:10.18637/jss.v045.i03
41. Brooks ME, Kristensen K, van Benthem KJ, et al. glmmTMB Balances Speed and Flexibility Among Packages for Zero-inflated Generalized Linear Mixed Modeling. R J. 2017;9(2):378–400.
42. Alaiti RK, Castro J, Lee H, et al. What Are the Mechanisms of Action of Cognitive–Behavioral, Mind–Body, and Exercise-based Interventions for Pain and Disability in People With Chronic Primary Musculoskeletal Pain?: a Systematic Review of Mediation Studies From Randomized Controlled Trials. Clin J Pain. 2022;38(7):502–509. doi:10.1097/AJP.0000000000001047
43. Mose S, Budtz CR, Rønn Smidt H, et al. How do people with chronic pain explain their use, or non-use, of pain-related healthcare services? A qualitative study of patient experiences. Disabil Rehabil. 2023;45(25):4207–4217. doi:10.1080/09638288.2022.2147589
44. Grøn S, Bülow K, Jonsson TD, Degn J, Kongsted A. What do people believe to be the cause of low back pain? A scoping review. Braz J Phys Ther. 2023;27(6):100562. doi:10.1016/j.bjpt.2023.100562
45. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.