Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Impact Of A Structured Emotional Well-Being Workshop On Psychological Outcomes And Patient Activation In Rheumatoid Arthritis And Spondyloarthritis: A Pilot Study
Authors Novella-Navarro M, Iniesta-Chamorro JM ![]() , Pavo-Blanco M, Plasencia-Rodríguez C
, Pavo-Blanco M, Plasencia-Rodríguez C
Received 28 April 2026
Accepted for publication 24 June 2026
Published 15 July 2026 Volume 2026:19 620714
DOI https://doi.org/10.2147/JMDH.S620714
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Veronica Swallow
Marta Novella-Navarro,1 Jose M Iniesta-Chamorro,2 María Pavo-Blanco,3 Chamaida Plasencia-Rodríguez1
1Rheumatology Department, University Hospital La Paz, Madrid, Spain; 2Biomedical Engineering and Telemedicine Centre, Center for Biomedical Technology, Universidad Politécnica de Madrid, Madrid, Spain; 3Rheumatology Department, Sanitas Hospitals, Madrid, Spain
Correspondence: Marta Novella-Navarro, Rheumatology Department, University Hospital La Paz, Paseo de la Castellana 261, Madrid, 28046, Spain, Tel +34917277020, Email [email protected]
Background: Patients with immune-mediated inflammatory diseases, such as rheumatoid arthritis (RA) and spondyloarthritis (SpA), frequently experience psychological distress and reduced well-being despite adequate control of inflammation with biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs). Psychosocial interventions may improve emotional health and self-management, although evidence within routine multidisciplinary care remains limited. This study evaluated the impact of a structured emotional well-being workshop on psychological outcomes and patient activation in RA and SpA.
Methods: We conducted a pilot study including patients with RA or SpA receiving b/tsDMARDs. Patients were invited to attend a structured emotional well-being workshop consisting of an initial face-to-face session, an eight-week online program, and a final face-to-face session. Psychological outcomes were assessed before and after the intervention using the WHO-5 Well-Being Index, the General Health Questionnaire (GHQ-12), and the Patient Activation Measure (PAM-13). Clinical outcomes included disease activity indices, physician global assessment (PhGA), patient global assessment (PGA), and pain visual analogue scale (VAS).
Results: Twenty-one patients participated. After the intervention, significant improvements were observed in PhGA and pain VAS. The frequency of moderate-to-high well-being increased from 71.4% to 95.2%, while high psychological distress decreased from 76.2% to 14.3%. Patient activation also improved, level of self-management was high in 71.4% of cases, with this percentage rising to 81.0%.
Conclusion: In this pilot study, a structured emotional well-being workshop integrated into multidisciplinary care was associated with improved psychological well-being and patient activation in patients with RA and SpA. These findings suggest the potential value of incorporating psychosocial interventions into routine rheumatology care, although confirmation in larger controlled trials is needed.
Keywords: psychological outcomes, immunomediated diseases, multidisciplinary management
Background
Immune-mediated inflammatory diseases (IMIDs), such as rheumatoid arthritis (RA) and spondyloarthritis (SpA), are chronic conditions that significantly impact patients’ physical, psychological, and social well-being.1,2 Beyond inflammation and structural damage, patients frequently experience emotional distress, anxiety, depressive symptoms, and reduced quality of life, which may persist even when disease activity is adequately controlled with biological or targeted synthetic disease-modifying antirheumatic drugs (b/tsDMARDs).3,4
Growing evidence supports the role of psychosocial factors in modulating perception of disease, adherence to treatment, self-management, and health-related outcomes in chronic rheumatic diseases.5 Emotional well-being and patient knowledge, skills, and confidence in health management have emerged as key components of patient-centered care. Mindfulness-based interventions, coaching programs, and emotional regulation strategies have demonstrated beneficial effects on psychological well-being and coping in chronic diseases.6,7 However, few data have been reported on structured emotional well-being interventions integrated into routine multidisciplinary care for patients with RA and SpA.
The present study aimed to evaluate the impact of a structured emotional well-being workshop, delivered within a multidisciplinary care model, on psychological well-being, mental health, and patient activation in patients with RA and SpA treated with b/tsDMARDs. Secondary objectives included exploring changes in disease activity indices and patient- and physician-reported outcomes, as well as potential correlations between psychological measures and disease activity.
Methods
Voluntary participation in the emotional well-being workshop was offered to patients with RA or SpA enrolled in the Mixed Attention Model (MAM) study for telemonitoring in IMIDs8 and who were undergoing treatment with b/tsDMARDs at the Multidisciplinary Unit for Immune-Mediated Diseases of La Paz University Hospital. Information about the workshop was disseminated through notifications and educational content delivered via the IMIDoc mobile App,9 which forms part of the online infrastructure supporting the MAM study. Interested patients self-registered using an electronic survey implemented in REDCap (Research Electronic Data Capture), a secure web-based platform designed to support data capture for research studies.10,11 All participants were already active users of the IMIDoc platform as part of the MAM telemonitoring program prior to enrollment in the workshop and continued to use the platform throughout the study period. Electronic informed consent was obtained, and contact details were recorded for study-related communications. Given logistic constraints related to the face-to-face components of the intervention, available places were allocated on a first-come, first-served basis.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki and was approved by the La Paz Ethics Committee (PI4519).
Workshop Structure and Schedule
The workshop was designed and delivered by a rheumatologist specialized in coaching (MP-B). It consisted of a three-part program. The first was an initial face-to-face session held in February 2025 and focused on engaging patients in what emotional well-being is, how to manage difficult emotions, self-regulation, and mindfulness. Attendance at this introductory session was recorded, and participants were subsequently granted access to online workshop materials through a personalized electronic distribution link, enabling structured participation in the online component of the intervention. The second part comprised an eight-week online program in which a series of topics were addressed on a weekly basis, with personal exercises and feedback from the coach.
The topics were as follows: Week 1, Identifying emotions (being aware); Week 2, Acceptance; Week 3, Mindfulness in your daily life; Week 4, Self-kindness; Week 5, Letting go; Week 6, Connection with the body, Self-care; Week 7, Resilience; Week 8, Gratitude.
The online component followed a structured temporal schedule in which educational videos and practical exercises were progressively released on a weekly basis. Participants were able to access cumulative content throughout the intervention period, enabling continuous engagement with previously delivered materials. The development of the workshop is shown in Figure 1.
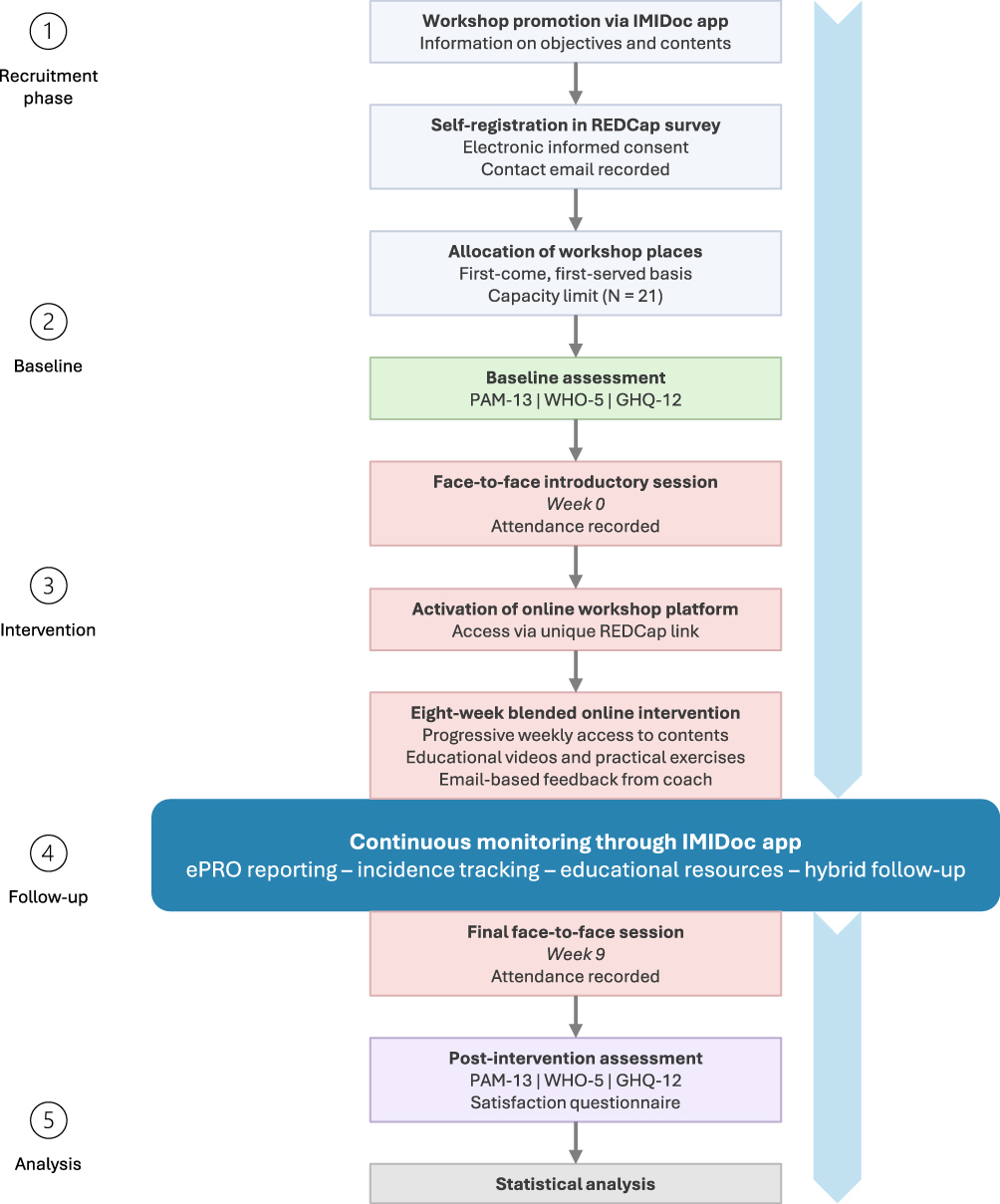 |
Figure 1 Flowchart of the emotional well-being workshop and participant pathway throughout the intervention. The diagram illustrates the recruitment process, registration and allocation of participants, baseline assessment, delivery of the blended intervention (face-to-face and online components), and post-intervention evaluation. The online component followed a structured weekly schedule with progressive release of educational content and exercises, accessible through a personalized REDCap link. |
The third part also consisted of a face-to-face session that took place in May 2025. The conclusions and lessons learned from the previous activities were shared, group dynamics were established, and wellness techniques were explored in greater depth. Attendance at this final session was recorded. Following completion of the workshop, participants were invited to complete post-intervention questionnaires to assess changes in psychological well-being, mental health, and patient activation.
Data Collection
The demographic and clinical characteristics collected included age, sex, level of academic achievement, age at diagnosis of RA or SpA, number of previous treatments, presence of structural damage, comorbidities (number and type), and anxiety-depression. These features related to medical history were obtained from the patient´s medical records. Clinical and patient-reported outcome data were obtained from the IMIDoc mobile App as part of routine monitoring within the MAM study. These included patient global assessment (PGA), physician global assessment (PhGA), and pain visual analogue scale (VAS). Data were collected prior to the workshop, between January and February 2025, and after the workshop, between May and June 2025. PhGA evaluations were performed by rheumatologists involved in routine clinical follow-up who were not involved in the design or delivery of the emotional well-being workshop. Similarly, disease activity indices were recorded, as follows: Disease Activity Index-28 (DAS28) for RA and for SpA; Ankylosing Spondylitis Disease Activity Score (ASDAS); and Bath Ankylosing Spondylitis Disease Activity Index (BASDAI).
Baseline psychological assessments were completed prior to the initial face-to-face workshop using electronic questionnaires distributed via REDCap. The same instruments were administered after completion of the intervention to enable pre–post comparisons of psychological outcomes. As a complement to the quantitative assessment of psychological outcomes, an ad hoc post-intervention questionnaire was administered to evaluate participant satisfaction and perceived usefulness of the workshop. This instrument consisted of five structured items using ordinal response scales to assess overall experience with the program, perceived emotional benefit, acquisition of practical coping strategies, perceived quality of interaction with the instructor, and willingness to recommend the intervention to other patients. In addition, two open-ended questions were included to capture qualitative feedback regarding participants’ experiences, perceived impact of the intervention, and suggestions for improvement.
Comprehensive Evaluation of Psychological Well-Being and Patient Engagement
Participants responded anonymously to three questionnaires to assess measures of subjective well-being, mental health, and patient activation. The scores obtained were collected before the initial and after the final workshop, and the changes between these two time points were analyzed.
A series of questionnaires were used. (1) The World Health Organization–Five Well-Being Index (WHO-5),12 which assesses general emotional well-being over the previous two weeks using five items scored 0–5, yielding a total score of 0–25, subsequently converted to a 0–100 scale; values below 50 suggest low well-being or possible depression, while scores above 50 indicate moderate-to-high well-being. (2) The General Health Questionnaire (GHQ-12),13 which measures psychological distress, stress, and recent emotional symptoms through 12 items scored either using a binary method (0–0–1–1; total 0–12) or a Likert format (0–1–2–3; total 0–36), with higher scores indicating greater psychological distress. (3) The Patient Activation Measure (PAM-13),14 which evaluates patients’ knowledge, skills, and confidence in the self-management of their health using 13 items, producing a raw score of 13–52, which is transformed into a standardized 0–100 activation score, and categorizing individuals into four activation levels: 1 (low activation), 2 (intermediate), 3 (moderate), and 4 (high self-management).
Improvement in these three questionnaires was defined as a change in score according to the following criteria: an increase of >10 points in the WHO-5, a reduction of >3 points in the GHQ-12, and an increase of >5 points in the PAM-13. These thresholds were used to facilitate the descriptive interpretation of clinically relevant changes in questionnaire scores and were considered exploratory measures within the context of this pilot study.
Statistical Analysis
Descriptive analyses of all patients were performed. Data are reported as absolute numbers and frequencies for qualitative variables and for quantitative variables, and as median and interquartile range (IQR) or mean and standard deviation (SD). Given the limited sample size and the small number of observations, normality could not be reliably established across all variables. Therefore, non-parametric methods were selected as a conservative analytical approach. Changes in quantitative variables were analyzed using the Wilcoxon test. Correlations between the scores of questionnaires and other quantitative variables (PGA, PhGA, VAS, DAS28, ASDAS, and BASDAI) were assessed using the Pearson and Spearman coefficients. P-values < 0.05 were considered statistically significant. Given the exploratory nature of this pilot study, no formal adjustment for multiple comparisons was performed. Therefore, statistical findings should be interpreted as exploratory and hypothesis-generating rather than confirmatory.
Statistical analyses were performed using IBM SPSS Statistics version 26 (IBM Corp., Armonk, NY, USA).
Results
A total of 21 patients participated in the emotional well-being workshop. Of these, 19 were female and two were male, with a mean (SD) age of 52.5 (8.4) years and a mean age at diagnosis of 42.5 (7.2) years. Thirteen patients (61.9%) had RA and eight (38.1%) had SpA. Seven patients (33.3%) were receiving their first b/tsDMARD, and only three patients had received ≥2 b/tsDMARDs (14.3%). Sixteen patients (76.2%) were educated to university level, four (19.0%) to secondary level, and one (4.8%) to elementary level. Regarding comorbidities, two thirds of participants (66.7%) had none, six patients (28.6%) had anxiety-depression syndrome, three (14.3%) had psoriasis, two had Sjögren syndrome (9.5%), and eight (38.1%) had structural damage.
With regard to activity indices and PGA, PhGA, and VAS scores, post-workshop scores were lower than the baseline scores, although these changes were statistically significant only in PhGA and VAS (see Table 1).
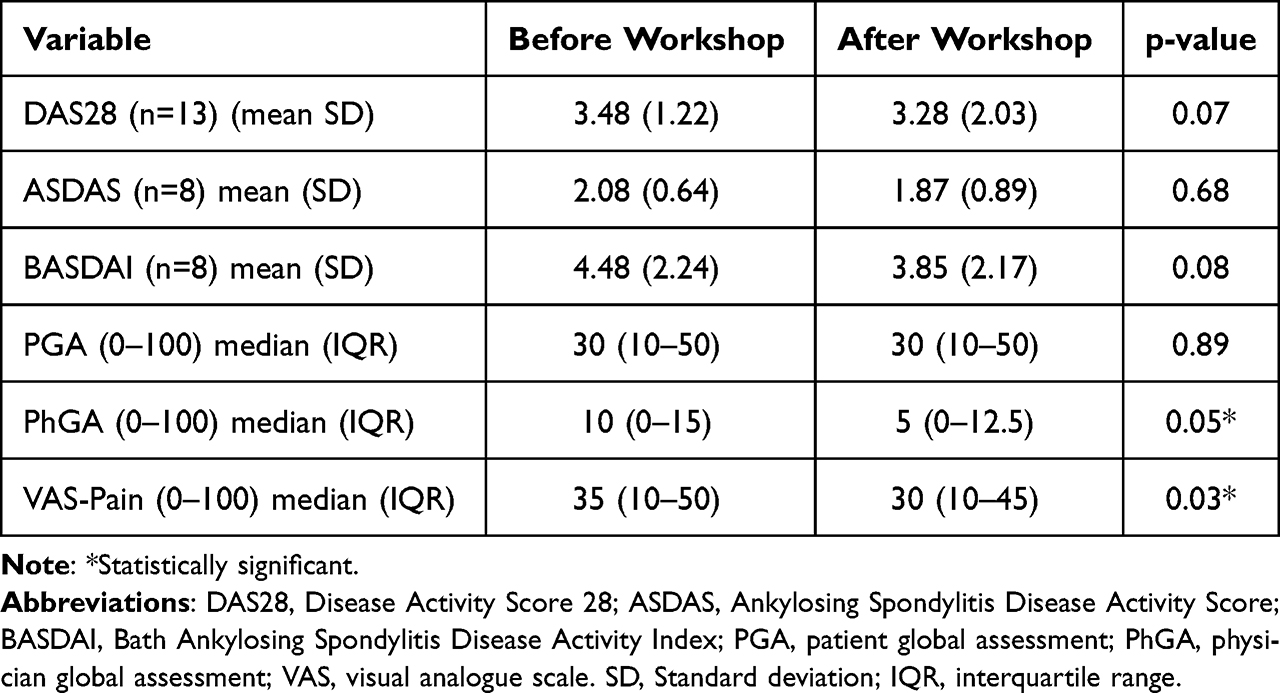 |
Table 1 Changes in Disease Activity Indices and Clinical Assessments Before and After Participation in the Emotional Well-Being Workshop |
According to WHO-5, well-being was moderate-to-high in 15 patients (71.4%) before the workshop; this percentage reached 95.2% at the end of the program, with significant changes in the scores in 66.7% of patients. Meanwhile, the results of the GHQ-12 showed that 16 participants (76.2%) had a high level of psychological distress at baseline; this frequency fell to 14.3% after the evaluation in the final session. The score in this questionnaire worsened in only two patients (9.5%), and a significant improvement in the average score of the items was recorded in 81.0%. Finally, the level of self-management among patients according to the PAM-13 questionnaire was high in 71.4% of cases, with this percentage rising to 81.0%. Even so, 52.4% of patients experienced significant changes in their knowledge and management skills in relation to their disease (Figure 2).
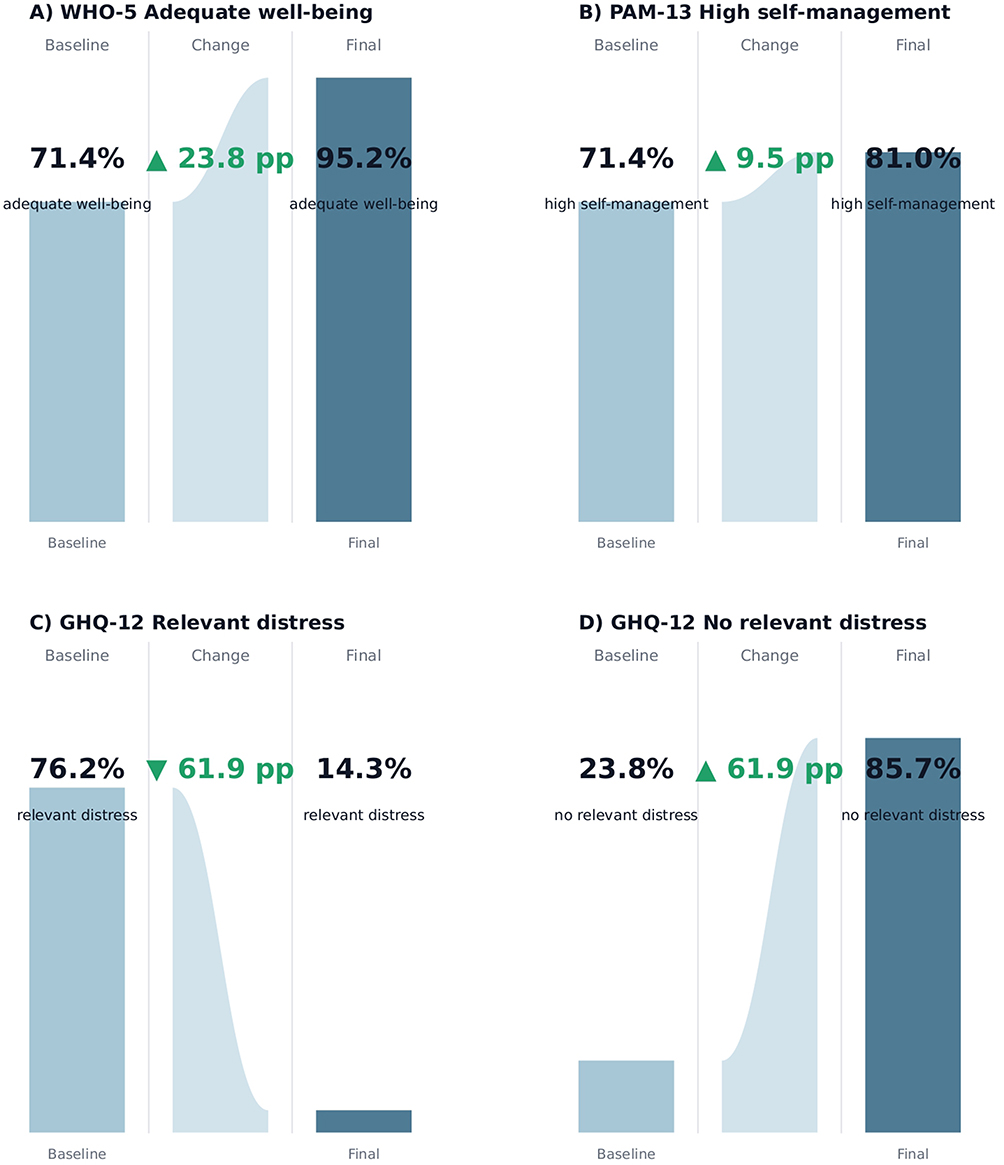 |
Figure 2 Changes in psychological well-being, psychological distress, and patient activation following participation in a structured emotional well-being workshop. Proportion of participants achieving clinically meaningful categories at baseline and post-intervention. (A) Percentage of participants with adequate well-being according to the WHO-5 index. (B) Percentage of participants with high self-management (level 4) according to the PAM-13 scale. (C) Percentage of participants presenting relevant psychological distress (high or moderate distress) according to the GHQ-12. (D) Percentage of participants with no relevant psychological distress according to the GHQ-12. Absolute percentage point changes between baseline and post-intervention assessments are graphically represented. The green arrows indicate the percentage-point change (increase or decrease) from baseline to post-intervention. Categories were defined according to established instrument-specific thresholds. |
No statistically significant correlations were found between the scores of the three different questionnaires and disease activity indexes.
Patient Satisfaction
Participant satisfaction with the emotional well-being workshop was high. All participants rated their overall experience positively, with 66.7% describing it as excellent and 33.3% as good. Most participants reported feeling consistently listened to and understood during the sessions (90.5% “always” and 9.5% “almost always”). A perceived benefit in emotional management was reported by 95.2% of participants, while all respondents indicated that they had acquired useful tools during the program. Notably, 100% of participants stated that they would recommend the workshop to other patients.
Discussion
This study shows that active participation in a structured emotional well-being program delivered by a professional coach was associated with meaningful improvements in psychological well-being, psychological distress, and patient activation among patients with RA and SpA receiving b/tsDMARDs.
Many studies have analyzed the association between IMIDs and symptoms of depression and anxiety, with the prevalence of these symptoms being higher than in the general population.15 Among patients with RA, major depressive disorder affected 16.8%, depressive symptoms 38.8%, and clinically relevant anxiety 22.1%;16 among those with SpA, moderate depression was reported in 15%.17 Furthermore, mental disorders in RA and SpA are closely associated with higher disease activity and unfavorable patient reported outcomes (PROs), while access to and acceptance of psychiatric care remain markedly insufficient.18 Although the WHO-5 questionnaire is a validated and widely used measure of emotional well-being, it continues to be infrequently used in patients with IMIDs.19
Following the intervention, a substantial increase in emotional well-being was observed, as measured by the WHO-5, with nearly all participants reaching moderate-to-high levels of well-being at the end of the program. The high proportion of patients achieving a significant improvement suggests that the intervention effectively enhanced positive emotional states.
Psychological distress assessed using the GHQ-12 decreased markedly after the workshop. Anxiety and depressive symptoms are increasingly taken into account when characterizing patients with SpA or RA. Moreover, these symptoms have been shown to influence adequate disease control and treatment response, further supporting a comprehensive, patient-centered approach and highlighting the importance of non-pharmacological strategies for management.1,3,4,20,21 Nevertheless, few studies have evaluated the impact of improvements in mental health using this type of questionnaire in patients with SpA or RA.22
Improvements were also observed in patient activation, assessed using the PAM-13, with over half of the participants experiencing a clinically relevant increase in activation scores. Higher PAM levels reflect greater confidence and competence in self-management, which may translate into improved adherence, lifestyle behaviors, and long-term outcomes. Some studies have concluded that strategies such as active coping, diversion, and self-encouragement were associated with better outcomes in RA and SpA patients.23–25
In addition, participants reported very high levels of satisfaction with the intervention. Most individuals perceived the workshop as helpful for emotional management and skill acquisition, and all participants expressed willingness to recommend the program to others. These findings suggest good acceptability and feasibility of structured emotional support interventions within routine multidisciplinary care for patients with IMIDs.
Qualitative feedback from participants highlighted three main thematic areas. First, participants reported an increased awareness and understanding of their emotional states, describing improvements in self-reflection and emotional regulation. Second, several respondents emphasized the acquisition of practical coping strategies that could be applied in daily life, including mindfulness techniques, stress management tools, and strategies to improve self-care. Third, participants valued the group experience and the supportive environment created during the workshop, which facilitated sharing experiences and feeling accompanied in the management of their chronic condition.
Changes in the disease activity indices (DAS28, ASDAS, BASDAI), on the other hand, did not reach statistical significance, although trends toward improvement were observed. This finding is not unexpected, given the short duration of follow-up, the small sample size, and the fact that most patients were already receiving stable b/tsDMARD therapy. Interestingly, patient-reported outcomes such as pain (VAS) and PGA improved significantly, suggesting that emotional well-being interventions may positively influence symptom perception and the clinical encounter, even without major changes in objective disease activity. This observation is biologically plausible, as emotional and psychological factors are known to influence pain perception through central mechanisms involved in attention, affective processing, and pain modulation. Improvements in emotional well-being, coping strategies, and self-regulation may therefore contribute to a more adaptive interpretation of symptoms and a reduced subjective burden of disease, even in the absence of substantial changes in inflammatory activity. This study is not without limitations. First, the study lacked a control group, which limits the ability to establish causal relationships between the intervention and the observed improvements. Consequently, the potential influence of factors such as natural fluctuations in psychological status, regression to the mean, placebo effects, or increased attention associated with study participation cannot be excluded. Second, the sample size was small, limiting statistical power and the generalizability of the findings. Third, the study was conducted at a single center, which may further limit external validity. Fourth, participants were volunteers, potentially introducing selection bias toward individuals who were more motivated and engaged in self-management activities. Moreover, the high satisfaction ratings observed may have been influenced by social desirability bias despite anonymous questionnaire administration. Finally, no long-term follow-up assessments were available, preventing evaluation of the sustainability of the observed benefits over time.
The study also has a series of strengths, including the use of validated instruments, a structured and reproducible intervention, and integration within routine multidisciplinary clinical care. Moreover, the study was conducted in the context of patient participation in a mixed care model (IMIDoc),8,9 where, in addition to the emotional well-being workshop, patient engagement was facilitated through an app that gave access to clinical monitoring and continuous reports, further supporting the need to integrate all possible tools in the management of chronic diseases.
In conclusion, this pilot study suggests that a structured emotional well-being workshop is feasible and associated with significant improvements in psychological well-being, mental health status, and patient activation in RA and SpA. These findings, together with the high levels of participant satisfaction and perceived usefulness of the intervention, support the potential value of incorporating psychosocial and emotional support interventions into multidisciplinary care strategies for patients with IMIDs.
Acknowledgments
This work was supported by the Fondo para la Investigación Sanitaria, Instituto de Salud Carlos III (PI22/00777). The emotional well-being workshop was made possible thanks to the collaboration of UCB Pharma, which provided unrestricted funding.
The authors thank the Spanish Foundation of Rheumatology for providing medical editorial assistance during the preparation of the manuscript (FERBT2026).
The authors acknowledge the Universidad Politécnica de Madrid for providing the computing infrastructure and technical resources necessary for the deployment and operation of the REDCap electronic data capture platform used in this study. The authors are also especially grateful to all the patients, who participated voluntarily in the emotional well-being workshop and contributed to the development of this initiative.
Funding
This work was supported by the Fondo para la Investigación Sanitaria, Instituto de Salud Carlos III (PI22/00777). The emotional well-being workshop was made possible thanks to the collaboration of UCB Pharma, which provided unrestricted funding.
Disclosure
M N-N has received research grants/honoraria from AbbVie, Alfasigma, and UCB outside the submitted work. Ch P-R has received research grants/honoraria from AbbVie, Pfizer, Novartis, Lilly, UCB, and Biogen outside the submitted work and meeting/travel support from Rovi, Johnson & Johnson, and Novartis, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sadovici-Bobeica V, Gupta L, Panagiotopoulos A, et al. Illness perception in axial spondylarthritis: bridging mind and joint. Int J Rheum Dis. 2026;29(2):e70579. doi:10.1111/1756-185x.70579
2. Doumen M, Gossec L, Ndosi M, et al. The positive perspective paradigm: proposal of a model to mitigate the impact of chronic inflammatory arthritis through comprehensive and early intervention. Ann Rheum Dis. 2026;S0003-4967(26):00002–9. doi:10.1016/j.ard.2026.01.001
3. Thiele T, Ahrenstorf G, Witte T, Kahl KG, Hirsch S. Prevalence and recognition gap of depressive and anxiety symptoms in patients with inflammatory-rheumatic diseases - a single center experience. J Psychiatr Res. 2026;196:257–262. doi:10.1016/j.jpsychires.2026.02.035
4. Roodenrijs NMT, van der Goes MC, Welsing PMJ, et al. Difficult-to-treat rheumatoid arthritis: contributing factors and burden of disease. Rheumatology. 2021;60(8):3778–3788. doi:10.1093/rheumatology/keaa860
5. Smolen JS, Gladman D, McNeil HP, et al. Predicting adherence to therapy in rheumatoid arthritis, psoriatic arthritis or ankylosing spondylitis: a large cross-sectional study. RMD Open. 2019;5(1):e000585. doi:10.1136/rmdopen-2017-000585
6. Tough H, Siegrist J, Fekete C. Social relationships, mental health and wellbeing in physical disability: a systematic review. BMC Public Health. 2017 May;17(1):414. BMC Public Health. 2017;17(1):580. doi:10.1186/s12889-017-4448-8
7. Landgren E, Mogard E, Bremander A, Lindqvist E, Nylander M, Larsson I. Belonging, happiness, freedom and empowerment-a qualitative study of patients’ understanding of health in early rheumatoid arthritis. BMC Rheumatol. 2024;8(1):29. doi:10.1186/s41927-024-00399-2
8. Novella-Navarro M, Iniesta-Chamorro JM, Benavent D, et al. Toward telemonitoring in immune-mediated inflammatory diseases: protocol for a mixed attention model study. JMIR Res Protoc. 2024;13:e55829. doi:10.2196/55829
9. Benavent D, Iniesta-Chamorro JM, Novella-Navarro M, et al. Digital health intervention for patient monitoring in immune-mediated inflammatory diseases: cocreation and feasibility study of the IMIDoc platform. JMIR Hum Factors. 2025;12:e58095. doi:10.2196/58095
10. Harris Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N. Conde JG.Research electronic data capture (REDCap)—a metadata-driven methodology and workflow process for providing translational research informatics support. J biomed informat. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
11. Harris PA, Taylor R, Minor BL, et al. The REDCap consortium: Building an International Community of Software Partners. J Biomed Informat. 2019;95:103208.
12. World Health Organization. The World Health Organization-Five Well-Being Index (WHO-5) (WHO-UCN-MSD-MHE-2024.01). 2024. Available from: https://www.who.int/publications/m/item/WHO-UCN-MSD-MHE-2024.01.
13. Lundin A, Hallgren M, Theobald H, Hellgren C, Torgén M. Validity of the 12-item version of the general health questionnaire in detecting depression in the general population. Public Health. 2016;136:66–74. doi:10.1016/j.puhe.2016.03.005
14. Hibbard JH, Mahoney ER, Stockard J, Tusler M. Development and testing of a short form of the patient activation measure. Health Serv Res. 2005;40(6 Pt 1):1918–1930. doi:10.1111/j.1475-6773.2005.00438
15. Cox N, Hawarden A, Kettle C, et al. The relationship between pain and depression and anxiety in people with inflammatory arthritis: a systematic review. Semin Arthritis Rheum. 2025;74:152808. doi:10.1016/j.semarthrit.2025.152808
16. Matcham F, Rayner L, Steer S, Hotopf M. The prevalence of depression in rheumatoid arthritis: a systematic review and meta-analysis: reply. Rheumatology. 2014;53(3):578–579. doi:10.1093/rheumatology/ket439
17. Zhao S, Thong D, Miller N, et al. The prevalence of depression in axial spondyloarthritis and its association with disease activity: a systematic review and meta-analysis. Arthritis Res Ther. 2018;20(1):140. doi:10.1186/s13075-018-1644-6
18. Husakova M, Balajkova V, Pavelka K, et al. Mental health in patients with rheumatoid arthritis and axial spondyloarthritis: a cross-sectional, case-control tertiary centre study from Czechia. BMJ Open. 2025;15(12):e103686. doi:10.1136/bmjopen-2025-103686
19. Englbrecht M, Alten R, Aringer M, et al. Validation of standardized questionnaires evaluating symptoms of depression in rheumatoid arthritis patients: approaches to screening for a frequent yet underrated challenge. Arthritis Care Res. 2017;69(1):58–66. doi:10.1002/acr.23002
20. Zhao SS, Webers C, Nikiphorou E, et al. Disease activity and mental health symptoms in axial spondyloarthritis: concordant or discordant? Rheumatology (Oxford). 2026;65(1):keaf506. doi:10.1093/rheumatology/keaf506
21. Rodríguez-Merlos P, Cabrera-Alarcon JL, Ruiz-Esquide V, et al. Early-onset difficult-to-treat rheumatoid arthritis: proposal of data-driven predictors and temporal threshold. Arthritis Res Ther. 2025;27:153. doi:10.1186/s13075-025-03621-9
22. Gaboury I, Dobkin PL, Gendron F, et al. Mindfulness-based stress reduction to improve depression, pain and high patient global assessment in controlled rheumatoid arthritis. Rheumatol Adv Pract. 2022;6(3):rkac074. doi:10.1093/rap/rkac074
23. Berner C, Erlacher L, Fenzl KH, Dorner TE. Medication adherence and coping strategies in patients with rheumatoid arthritis: a cross-sectional study. Int J Rheumatol. 2019;2019:4709645. doi:10.1155/2019/4709645
24. Bhatia O, Ahluwalia V, Pavlova V, Mulgund M. Patient engagement and empowerment using a mHealth application for management of inflammatory arthritis. J Rheumatol. 2025;52(Suppl 2):106–107. doi:10.3899/jrheum.2025-0314.129
25. Zhu X, Zheng N. The effect of continuous care on self-management and disease activity of patients with ankylosing spondylitis after discharge. J Pak Med Assoc. 2025;75(Suppl 2):S39–S46. doi:10.47391/JPMA.SRPH-07
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.